
Submitted:
16 December 2025
Posted:
16 December 2025
You are already at the latest version
Abstract
Background: Bladder adenocarcinoma (BA) is a rare malignancy, accounting for up to 2% of bladder cancers. Its molecular drivers remain poorly defined, limiting therapeutic options and prognostic assessment. This study characterizes the genomic landscape of BA using a large, multi-institutional sequencing database to identify recurrent alterations and potential therapeutic targets. Methods: Clinical and genomic data for BA were extracted from the AACR Project GENIE® database (accessed July 2025). Samples underwent targeted next-generation sequencing (50–555 genes, >500× coverage). Analyses included somatic mutation frequency, copy number alterations (CNAs), tumor mutational burden (TMB), and stratification by sex, race, and tumor site (primary vs. metastatic). Statistical comparisons used chi-squared, Student’s t-test, or Mann–Whitney U with Benjamini–Hochberg correction. Results: A total of 206 tumor samples from 195 patients were an-alyzed. The cohort was predominantly male (61%) and White (43%). Common somatic point mutations included TP53 (65.0%), KRAS (35.4%), PIK3CA (17.0%), SMAD4 (16.5%), and ARID1A (11.2%). CNAs were frequently affected by CDKN2A (11.6%), CDKN2B (11.6%), and SMAD4 (7.0%). Sex-stratified analysis revealed male enrichment in ARFGAP3, PTEN, LATS2, TSC2, and PRKDC, while CD40, FOXQ1, and WEE1 were observed only in females. Race-based differences included FANCD2 and EGFR en-richment in Asian patients. Co-occurring somatic point mutations were identified between ARID1A–TERT, NSD1–KDM6A, and KRAS–SMAD4, while SMAD4 and KDM6A point mutations demonstrated mutual exclusivity. Discussion: Findings confirm TP53, KRAS, and PIK3CA as recurrently mutated drivers in BA and highlight FGFR3 as a novel re-currently mutated gene, as well as frequent copy number losses involving SMAD4, CDKN2A, and CDKN2B. Subgroup analyses highlight sex- and race-associated muta-tional differences, suggesting potential biologic underpinnings of demographic dispari-ties. Co-occurrence and exclusivity analyses reveal previously unreported interactions, underscoring pathway redundancy and cooperation in tumor progression. Conclusion: This study provides one of the most comprehensive genomic characterizations of BA to date, identifying recurrent drivers, subgroup-specific alterations, and mutational inter-actions. These insights highlight TP53, KRAS, and PIK3CA pathway disruption as central in BA biology and support the development of targeted therapeutics and prospective validation in independent cohorts.
Keywords:
bladder adenocarcinoma
; bladder cancer
; AACR Project GENIE
; cancer genomics
; somatic point mutations
; copy number alterations
; TP53
; KRAS
; PIK3CA
; targeted therapy
1. Introduction
Bladder adenocarcinoma (BA) is a rare malignancy of the urinary bladder that arises most commonly in the trigone or posterior wall [1]. Histologically, five subtypes have been described: enteric, mucinous, signet ring cell, mixed morphology, and not otherwise specified (NOS) [2]. The most common presenting symptom is hematuria, with or without bladder irritation. Less frequently, patients may present with abdominal pain, dysuria, or mucusuria [1,2,3]. Due to its rarity and the limited size of existing studies, reported 5-year disease-free survival rates vary widely, ranging from 11% to 61% [4].
BA accounts for only 2% of all primary bladder tumors. Although rare globally, the largest number of reported cases originate from Egypt, while a U.S. study identified BA in only 0.8% of new bladder cancer diagnoses over a one-year period [4]. The disease typically presents in the fifth to seventh decade of life and is more common in males, with a reported male-to-female ratio of 3:1 [3]. Incidence increases significantly in regions where schistosomiasis is endemic [5]. Additional risk factors include endometriosis, bladder exstrophy, bladder augmentation, and various chronic irritative bladder conditions [5].
Diagnosis of BA requires careful exclusion of secondary involvement from adenocarcinomas of nearby organs. This is particularly challenging due to the histologic similarity between bladder adenocarcinomas, especially the enteric type, and colorectal adenocarcinomas. Cystoscopy, ultrasound, urinary cytology, and transurethral resection of bladder tumor (TURBT) are commonly used diagnostic tools [6]. BA is often present at an advanced stage, negatively impacting prognosis [8]. Diagnostic vigilance is critical, as emphasized in a case where multiple ultrasounds performed on a patient with recurrent UTIs led to early tumor detection [7].
Treatment typically involves total cystectomy with or without lymph node dissection [9,10]. The outcomes of chemotherapy and radiation remain controversial: some studies report poor tumor response or worsened outcomes, while others demonstrate survival benefits [6,7,11]. Recent evidence suggests that postoperative radiotherapy may improve 5-year disease-free survival, increasing rates from 37.5% to 61% [10]. Emerging evidence also highlights that frequent promoter methylation events in 14-3-3 σ and CAGE-1 genes play a key role in BA tumorigenesis [12]. Further sequencing has identified 18 pathogenic single-nucleotide variants (SNVs) across 68 genes, with TP53 (42%) and KRAS (25%) being the most altered [5,13]. Additional disruptions in p53, p21, p27, cyclin E, and Ki-67 proteins have also been observed. Co-alterations in p27 and Ki-67 have been strongly associated with increased disease recurrence and cancer-specific mortality [4]. Each of these molecular changes may offer potential targets for therapeutic development and improved prognosis.
Despite recent advancements, the full scope of genomic alterations driving BA remains poorly defined at the population level. Additionally, there is scarce existing data describing the influence of demographics on genomic alterations within BA, which warrants further study. This study aims to comprehensively characterize the mutational landscape and drivers of BA using a publicly accessible repository to identify prognostic biomarkers and novel therapeutic targets.
2. Materials and Methods
Ethical oversight for this study was waived by Creighton University (Phoenix, AZ, USA), as it involved publicly available data from the American Association for Cancer Research (AACR) Project GENIE® database. Clinical and genomic data were accessed through the cBioPortal platform (version 17.0-public) on July 20, 2025, encompassing records collected from 2017 onward.
The AACR GENIE® database collects genomic sequencing data from 19 international cancer centers, resulting in a heterogeneous dataset that reflects the diversity of sequencing technologies. Included platforms span whole-genome sequencing (WGS), whole-exome sequencing (WES), and targeted gene panels covering between 50 and 555 genes. All samples were sequenced using next-generation sequencing (NGS) technologies, with these targeted panels achieving coverage greater than 500×.
Each participating institution in GENIE uses its own bioinformatic pipeline for mutation calling and annotation; however, all adhere to GENIE harmonization standards facilitated by Genome NEXUS. Common tools such as GATK for variant detection and ANNOVAR are widely used, although versions may differ across different sites. While clinical outcome and therapeutic response data are available for select cancer types within the database, treatment information was not recorded for bladder adenocarcinoma, which limits analyses related to therapeutic efficacy. Variation in sequencing and annotation pipelines may occur both across and within contributing institutions, potentially introducing variability in the dataset.
Patients included in this study were those with a confirmed pathological diagnosis of bladder adenocarcinoma, selected from a pool of tumor cases. Tumor samples were classified as primary, referring to those taken from the original tumor site, or metastatic, those obtained from sites where the cancer had spread. To compare alteration frequencies between these two groups, a chi-squared test was performed, assessing differences based on the proportion of samples with mutations in each category.
This study draws on a large, publicly accessible genomic database to examine the somatic mutation profile of bladder adenocarcinoma in greater detail in order to gain insight that can further guide future diagnostic strategies and interventions.
The study utilized three main categories of data: genomic data (such as somatic mutations), histological subtype, and clinical demographics (including race, sex, and age). Although the design of targeted sequencing panels varied across participating institutions, most panels included coverage of key cancer-associated genes. Genes without known clinical relevance were typically excluded from these panels, and structural variants were not incorporated into the present analysis.
We assessed copy number alterations (CNAs) by identifying high-level amplifications and homozygous deletions, then calculating the frequency of recurrent events across the cohort. Tumor mutational burden (TMB) was quantified for each sample as the total number of somatic single-nucleotide variants, which include synonymous and nonsynonymous mutations, per megabase sequenced. TMB values were then normalized by the size of the targeted panel to account for differences. The normalized TMB estimates were converted to whole-exome sequencing (WES)–equivalent values using linear regression models developed by the AACR Project GENIE consortium. This incorporated panel size and potentially other factors to correct for heterogeneity. This two-step normalization and adjustment process minimizes bias from panel-specific characteristics and enhances the reliability of TMB comparisons across different sequencing platforms.
Samples with missing data were excluded from analysis. All statistical analyses were conducted in R/R Studio (R Foundation for Statistical Computing, Boston, MA, USA), with statistical significance set at p < 0.05. Continuous variables were summarized as means ± standard deviations (SD), and categorical variables were reported as frequencies and percentages. Associations between categorical variables were evaluated using the chi-squared test. For continuous variables, data distribution was assessed for normality; comparisons between two groups were performed using a two-sided Student’s t-test for normally distributed data or a Mann–Whitney U test for non-normal distributions. When applicable, p-values were adjusted for multiple comparisons using the Benjamini–Hochberg false discovery rate (FDR) method.
Somatic mutation analysis included only nonsynonymous variants, specifically missense, nonsense, frameshift, and splice-site mutations, that met a variant allele frequency threshold of ≥5% and sequencing coverage of ≥100×. Synonymous variants were excluded because these mutations are less likely to alter the amino acid sequence and have a functional impact. Variants of unknown significance were excluded as well. Final mutation calls were obtained from the AACR Project GENIE mutation annotation format files, which provide standardized gene and protein alteration annotations across all participating institutions, ensuring consistency and comparability of variant data.
3. Results
3.1. Patient Demographics of Bladder Adenocarcinoma
The demographic analysis combined data from both primary and metastatic tumor samples, given the rarity of BA and the smaller sample size of this cohort. Table 1 summarizes patient demographics. A total of 206 tumor samples were collected from 195 patients. Of these, 119 (61.0%) were male and 76 (39.0%) were female. Ethnically, 96 (49.2%) were non-Spanish/non-Hispanic, 15 (7.7%) were Spanish/Hispanic, and 84 (43.0%) were of unknown ethnicity. Racial composition included 9 (4.6%) Asian, 84 (43.1%) White, 20 (10.3%) Black, and 53 (27.2%) categorized as Other. Race data were unavailable for 23 (11.8%) individuals. All 195 patients (100%) were adults. Among the samples analyzed, 85 (41.3%) originated from primary tumors, 68 (32.9%) were from a metastatic site, and 53 (25.7%) had no available information regarding tumor site.
3.2. Most Common Somatic Point Mutations and Copy Number Alterations
Figure 1 highlights the landscape of the most frequent somatic point mutations and copy number alterations (CNAs) in the cohort. The most common somatic point mutations occurred in TP53 (n = 134; 65.0%), KRAS (n = 73; 35.4%), PIK3CA (n = 35; 17.0%), SMAD4 (n = 34; 16.5%), ARID1A (n = 23; 11.2%), KMT2D (n = 20; 9.7%), CDKN2A (n = 21; 10.2%), TERT (n = 20; 9.7%), FAT1 (n = 20; 9.7%), NSD1 (n = 12; 5.8%), ATM (n = 15; 7.2%), FGFR3 (n = 17; 8.3%), KDM6A (n = 18; 8.7%), and NF1 (n = 12; 5.8%).
In addition to point mutations, recurrent CNAs were detected in 86 samples. Loss of heterozygosity (LOH) events were common, particularly in tumor suppressor genes such as CDKN2A (n = 10; 11.6%), CDKN2B (n = 10; 11.6%), and SMAD4 (n = 6; 7.0%). In contrast, gene amplifications occurred less frequently and involved MYC, SMAD4, ERBB2, and CCND1.
3.3. Genetic Differences by Sex and Race
Sex-based stratification of somatic mutations demonstrated several genes enriched in male patients. Somatic point mutations in ARFGAP3 (n = 2; p = 3.84e-4), PTEN (n = 9; p = 0.0119), and LATS2 (n = 5; p = 0.0241) were observed exclusively in males. In contrast, somatic mutations in CD40, FOXQ1, LAMB4, LDLR, MCM2, PPP1R15A, and WEE1 were found only in female patients (n = 1 for each gene). Additionally, TSC2 and PRKDC mutations were significantly more frequent in males than in females (n = 10 vs. n = 1; p = 0.0256) and (n = 10 vs. n = 1; p = 0.0272), respectively.
Asian and Pacific Islander patients with bladder cancer tend to present with higher-grade tumors and worse overall 5-year survival compared to other groups [15]. Due to these trends, we specifically analyzed enriched somatic mutations in Asian patients. ANKRD26 (n = 1; p = 0.0220), EME1 (n = 1; p = 0.0435), NEIL3 (n = 1; p = 0.0435), FANCD2 (n = 2; p = 0.0301), and EGFR (n = 2; p = 0.0411) were each significantly enriched in Asian patients. Comparative frequencies between Asian and White patients are summarized in Table 2.
3.4. Co-Occurrence and Mutual Exclusivity of Mutations
Several statistically significant co-occurring somatic mutation pairs were observed in the cohort. Mutations in ARID1A co-occurred with TERT mutations (n = 5; p = 0.010), and NSD1 point mutations co-occurred with KDM6A (n = 4; p = 0.011). Additionally, KRAS point mutations were significantly associated with co-occurring mutations in SMAD4 (n = 8; p = 0.022) and FAT1 (n = 5; p = 0.025). One mutually exclusive relationship was identified between SMAD4 and KDM6A mutations (n = 18 vs. n = 16; p = 0.019).
3.5. Primary vs. Metastatic Mutations
The cohort included 85 primary and 68 metastatic tumor cases. In primary tumors, several genes harbored mutations, including CREBBP, CD40, FOXQ1, LDLR, PPP1R15A, and WEE1 (n = 1 each; p = 0.0274). In contrast, TRAF7 (n = 4; p = 0.0157), LAMB4 (n = 1; p = 0.0247), MCM2 (n = 1; p = 0.0247), NOTCH4 (n = 6; p = 0.0258), and FANCM (n = 3; p = 0.0444) somatic mutations were more frequently observed in metastatic tumors. While some genes harbored mutations exclusively in either primary or metastatic samples, the most recurrent mutations, such as those in KMT2D, ARID1A, and TP53, were observed across both groups, with no statistically significant differences in overall frequency.
4. Discussion
4.1. Demographic Trends and Subgroup Molecular Analysis
Existing epidemiologic data has demonstrated that bladder adenocarcinoma tends to present more frequently in males compared to females [1,14,15]. This known trend is reflected in our cohort as well, with a majority of patients being male (n=119). In addition to incidence, sex-stratified analysis revealed differences in mutation profiles. Specifically, somatic mutations in ARFGAP3 (n=2; p = 3.838e-4), PTEN (n=9; p = 0.0119), and LATS2 (n=5; p = 0.0241) were distinctly found in males. In contrast, CD40, FOXQ1, LAMB4, LDLR, MCM2, PPP1R15A, and WEE1 mutations were detected in only females (n=1 each). Additionally, mutations in TSC2 and PRKDC were present in both sexes; however, these alterations showed increased frequency in males compared to females (n = 10 vs. n = 1; p = 0.0256 and n = 10 vs. n = 1; p = 0.0272, respectively). While prior studies have demonstrated sex-based differences in urothelial carcinoma in genes such as RB1, CDKN2A, ERCC2, and the AR gene, comparable data is limited in BA. This study’s findings therefore represent a novel contribution to understanding sex-based genomic alterations in this cancer type.
Racial disparities are also well established in bladder cancer overall, with higher incidence reported in Caucasian groups when compared to other races [15]. Our findings were consistent with these trends, specifically with non-Spanish/non-Hispanic patient samples accounting for the largest group in our cohort (n=96). These results further support the influence of demographic factors on overall incidence.
Previous studies have shown that Asian and Pacific Islander patients with bladder cancer typically present with higher-grade tumors and worse overall 5-year survival compared to other groups [15]. As a result, we further compared genomic profiles between Asian and White patients. There were multiple somatic mutations that were observed with increased frequency in Asian patients, including ANKRD26 (p = 0.0220), EME1 (p = 0.0435), and NEIL3 (p = 0.0435), each identified once (n = 1), but absent in White patients. There was additional enrichment in FANCD2 (n = 2; p = 0.0301) and EGFR (n = 2; p = 0.0411) when compared to White counterparts. These results provide broader genomic context to previously observed trends in Asian populations with bladder adenocarcinoma and point to possible specific genetic mutations that may underlie these racial disparities.
4.2. Commonly Mutated Genes and Known Pathways
Substantial heterogeneity was observed throughout our cohort with respect to somatic genomic alterations. Known studies have identified various altered genes, including TP53, KRAS, PIK3CA, CTNNB1, APC, TERT, FBXW7, IDH2, and RB1, all of which play key roles in maintaining cancer hallmark characteristics [5]. Our study confirmed prior results, with somatic mutations in TP53 (65.0%), KRAS (35.4%), and PIK3CA (17.0%) being identified as the most common. While some prior studies have shown higher incidence of TERT mutation prevalence of up to 33% in some patient cohorts, our study showed a lower prevalence of TERT mutations (9.7%) [5].
Prior studies have noted an absence of alteration in FGFR in some BA cohorts [5]. This study identified FGFR3 alterations in 8.3% of samples, which is a novel finding in this tumor subtype. There is also limited information on the presence of loss of heterozygosity (LOH) events in bladder adenocarcinoma. Our cohort demonstrates that these loss-of-heterozygosity events were present and identified specific copy number losses in CDKN2A (n = 10; 11.6%), CDKN2B (n = 10; 11.6%), and SMAD4 (n = 6; 7.0%). The presence of these copy number alterations may underlie the disease’s proliferative capacity and aggressive nature, possibly pointing to a future therapeutic target.
4.3. p53 Pathway
Disruption of the TP53 pathway is one of the most common genetic alterations in cancer. In normal genetic landscapes, TP53 is an important tumor suppressor gene and plays a key role in pathways involving cell cycle progression and DNA repair mechanisms; however, when altered, this may contribute to tumorigenesis [16]. Across all cancers, TP53 disruption is frequently an early enabling event that weakens checkpoint surveillance and facilitates the accumulation of oncogenic mutations [17]. TP53 has been shown to be commonly altered in bladder adenocarcinoma as well, and TP53/RB1 pathways have been specifically implicated in its progression [5]. Our results confirm prior findings on the prevalence of TP53, with somatic mutations in TP53 present in 65% of our cohort. There are additional mutations observed in our cohort that overlap with TP53 signaling. Somatic mutations in CDKN2A, RB1, ATM, PTEN, and ARID1A all relate to the TP53 pathway by either functioning as a transcriptional target or serving roles in pathways that TP53 serves to regulate. Mutations in TERT and WEE1 further disrupt cell-cycle regulation, providing alternative mechanisms to bypass TP53-mediated control. These results highlight the influence of TP53 in the pathogenesis of bladder adenocarcinoma, specifically with respect to its roles in DNA repair, cell cycle regulation, and interconnectedness with chromatin remodeling networks.
Alterations in pathways involved with TP53 may hold potential for future therapeutic targets. Currently, there are no drugs specific to bladder adenocarcinoma that have been approved for p53-restoring therapy. However, there are several therapeutics under clinical investigation that are focused on p53 restoration. Specifically, mutant-p53 reactivators, such as eprenetapopt for leukemia (clinical trial: NCT03931291) and PC14586 for solid tumors (clinical trial: NCT04585750), have shown possible advances in therapeutics focused on p53 restoration. Further investigation should be performed into identifying methods of targeting TP53 and associated pathways therapeutically.
4.4. KRAS Pathway
KRAS is a commonly mutated oncogene found in most cancers and is involved in the regulation of cell division. KRAS is commonly found in BA as well throughout all stages and grades of the cancer [18]. KRAS effectively regulates the MAPK/ERK pathway, driving cell proliferation and survival [19]. Within BA, KRAS mutations are known to be early oncogenic events, fueling uncontrolled cellular growth. Our cohort saw KRAS mutations in 35.4% of samples, which is slightly higher than existing studies reporting KRAS mutation frequencies of 20–28% [5,20].
The important role of KRAS in oncogenesis in most cancers, including BA, underscores its potential as a future therapeutic target as well. Although there are no therapeutics in development focused on KRAS mutations in bladder adenocarcinoma, there are several drugs being developed and under investigation for similar pathways prevalent in colorectal cancer. Specifically, KRAS-G12C is now clinically druggable in colorectal cancer with adagrasib + cetuximab, which showed FDA accelerated approval in June 2024, and sotorasib + panitumumab, which received FDA approval in January 2025 [21,22].
4.5. PIK3CA Pathway
Generally, activating PIK3CA mutations drives PI3K-AKT-mTOR signaling to promote cellular growth, survival, and metabolic reprogramming [23]. Additionally, PI3K activation can function as an early or cooperating event in tumor initiation and progression, and this has been shown in urothelial tumorigenesis [24,25]. In BA specifically, PIK3CA has been identified within the PI3K/mTOR axis as one of the core pathways involved in pathogenesis. Our cohort found mutations in PIK3CA in 17% of our samples, which is consistent with literature rates of approximately 20% [5].
There are currently no therapies approved for targeting the PIK3CA pathway in bladder adenocarcinoma. However, agents targeting this pathway do exist for other diseases and have been evaluated in clinical trials. These include alpelisib, which is an FDA-approved drug that targets PIK3CA mutations in overgrowth syndrome and has demonstrated clinical benefit [26,27]. Additionally, inhibitors to the mTOR pathway such as everolimus (for PIK3CA amplification) and temsirolimus (for PI3K-pathway activation) have been investigated; however, their efficacy has been limited [28,29].
4.6. Co-Occurrence/Mutual Exclusivity and Functional Implications
Multiple co-occurring mutations were identified in bladder adenocarcinoma through this study. First, ARID1A mutations co-occurred with TERT mutations in 5 samples (p=0.01). Although this co-alteration has not been discussed in literature, prior functional studies provide supporting context. In human urothelial cell lines that were TERT immortalized, the inactivation of ARID1A induced p53/p21 expression, leading to dysregulation of the cell cycle and increased cell growth, likely due to co-mediation of c-Myc activity [30]. These findings suggest that the co-occurrence of alterations in ARID1A and TERT may cooperate to drive tumor progression by bypassing mechanisms of proliferative control and normal cellular senescence.
Another co-occurring mutation pair was observed between NSD1 and KDM6A, which was identified in 4 samples (p=0.010) and represents a unique and novel finding in bladder adenocarcinoma. The molecular mechanisms underlying this co-occurrence may be implicated in genomic stability. Prior studies have proposed that KDM6A maintains genomic stability by interacting with SND1, which establishes a protective state that limits replication fork collapse through the recruitment of RPA and Ku70 to the newly formed DNA strand [31].
Although KRAS mutations were previously described independently, co-occurrence was also demonstrated between KRAS and SMAD4 (n=8) and FAT1 (n=5). These co-occurrent patterns have not previously been reported in bladder adenocarcinoma. Prior studies have mainly demonstrated the possibility of co-occurrence between KRAS and SMAD4 in colorectal cancer.
Lastly, our analysis revealed a mutually exclusive relationship between SMAD4 and KDM6A somatic mutations, identified in 18 and 16 samples, respectively (p = 0.019). This finding has not been shown before in bladder adenocarcinoma; however, this may implicate possible redundancy in these two pathways. While SMAD4 has been shown to be integral to TGF-β signaling, cell growth, and differentiation, KDM6A mainly functions as a chromatin-modifying enzyme that influences tumor suppression and cell fate. These pathways being mutually exclusive may suggest that concurrent loss does not provide significant tumorigenic advantage when compared with a mutation of a single pathway [32,33].
4.7. Primary vs. Metastatic Tumors
The cohort included 85 primary and 68 metastatic tumor cases. In primary tumors, several genes harbored mutations, specifically in CREBBP, CD40, FOXQ1, LDLR, PPP1R15A, and WEE1 (n = 1 each; p = 0.0274). In contrast, TRAF7 (n = 4; p = 0.0157), LAMB4 (n = 1; p = 0.0247), MCM2 (n = 1; p = 0.0247), NOTCH4 (n = 6; p = 0.0258), and FANCM (n = 3; p = 0.0444) somatic mutations were more frequently observed in metastatic tumors.
4.8. Limitations
Despite notable findings, this study did contain limitations. One such limitation is the GENIE Database’s lack of treatment data. Treatment data within the database would have allowed for further subgroup analysis, primarily between primary and metastatic tumors, and may have also provided information regarding therapeutically induced genomic alterations. Another limitation lies in the lack of transcriptomic data, which may have limited analysis of downstream pathway targets and the potential identification of further miRNA-related therapeutic targets. A similar limitation is the lack of epigenetic alteration data within the cohort, which limited analysis and possible identification of additional epigenetic therapeutic targets. Incorporating such data would likely contribute to more detailed mechanistic understanding. A third limitation is due to the lack of clinical outcome data and survival endpoints within the patient cohort, which limited additional analyses. Another limitation inherent to the database itself is the grouping of overall bladder adenocarcinoma rather than stratifying by subtype. Another inherent limitation to the dataset itself is possible discrepancies between sequencing protocols across the multiple centers that the sequencing data was initially obtained from and later compiled into the GENIE database. Additionally, constraints were present in investigating connections between genetic mutations and trends within protein expression via techniques including immunohistochemistry. A limitation worth acknowledging as well is the smaller size of the cohort itself, which may impact the robust generalizability of results, and this necessitates subsequent investigations involving larger patient cohorts. Additionally, due to the inherent study design, it was difficult to identify and distinguish between driver as opposed to passenger mutations, which warrant further investigation in future studies as well. Furthermore, while a potential confounding variable may have been the presence of multiple tumor samples from the same patients in the cohort overall, this factor at best minimally skews the results. Despite these inherent limitations, our findings demonstrate novel and important information surrounding the genomic alterations and susceptible pathways in bladder adenocarcinoma. The results of this study underscore the importance of pathways TP53, KRAS, and PIK3CA and have identified possible novel therapeutic targets.
5. Conclusions
This study provides a broad genomic characterization and landscape of bladder adenocarcinoma. This study confirms TP53, KRAS, and PIK3CA as common recurrent mutations in BA and identified FGFR3 as an novel recurrently mutated gene, along with frequent copy number losses involving CDKN2A, CDKN2B, and SMAD4. Sex-stratified analyses demonstrated distinct patterns of somatic point mutations, with ARFGAP3, PTEN, TSC2, and LATS2 mutations enriched in male patients, while mutations in CD40, FOXQ1, LAMB4, LDLR, MCM2, PPP1R15A, and WEE1 were enriched in females. Race-stratified analyses revealed somatic point mutations in ANKRD26, EME1, NEIL3, FANCD2, and EGFR to be more frequently seen in Asian patients. Additionally, this study identified previously unreported co-occurring mutations between NSD1 and KDM6A, KRAS and SMAD4, and ARID1A and TERT. Notable mutational exclusivity of somatic point mutations was observed between SMAD4 and KDM6A. Future investigations should focus on the development of novel therapeutics to address molecular pathways unique to bladder adenocarcinoma pathophysiology, specifically those implicated by the genes TP53, KRAS, and PIK3CA. Furthermore, establishing clinical trials with independent cohorts using therapeutics could aid in treating bladder adenocarcinoma more comprehensively.
Author Contributions
Conceptualization A.S. and B.H.; data curation, A.S.; formal analysis, A.S.; methodology, S.R., S.O; project administration, T.M., A.S., S.P. and B.H.; supervision, A.S., T.M., S.P., B.H., G.S., A.T., and S.K.; visualization, A.S., S.R, S.O..; writing - original draft, A.S., S.R., and S.O.; writing - review & editing, A.S, T.M., S.O., S.R., G.S., S.P., B.H., S.K., and A.T. All authors have read and agreed to the published version of the manuscript. The authors would like to acknowledge the contributions of A.S and S.P as co-first authors of this study.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study as research exclusively utilized de-identified publicly available data through the AACR Project Genie database and therefore did not constitute human subjects research under federal regulations.
Informed Consent Statement
Patient consent was waived as research exclusively utilized de-identified publicly available data through the AACR Project Genie database, and this does not require individual informed consent.
Data Availability Statement
The data presented in this study are available from the AACR GENIE Database at https://genie.cbioportal.org/.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AACR | American Association for Cancer Research |
| ANKRD26 | Ankyrin Repeat Domain 26 |
| APC | Adenomatous Polyposis Coli |
| ARFGAP3 | ADP Ribosylation Factor GTPase Activating Protein 3 |
| ARID1A | AT-Rich Interaction Domain 1A |
| ATM | Ataxia Telangiectasia Mutated |
| BA | Bladder Adenocarcinoma |
| CCND1 | Cyclin D1 |
| CD40 | CD40 Molecule (TNF Receptor Superfamily Member 5) |
| CDKN2A | Cyclin-Dependent Kinase Inhibitor 2A |
| CDKN2B | Cyclin-Dependent Kinase Inhibitor 2B |
| CNAs | Copy Number Alterations |
| CREBBP | CREB-Binding Protein |
| CTNNB1 | Catenin Beta 1 |
| EGFR | Epidermal Growth Factor Receptor |
| EME1 | Essential Meiotic Structure-Specific Endonuclease 1 |
| ERBB2 | Erb-B2 Receptor Tyrosine Kinase 2 |
| ERCC2 | Excision Repair Cross-Complementation Group 2 |
| FANCD2 | Fanconi Anemia Complementation Group D2 |
| FANCM | Fanconi Anemia Complementation Group M |
| FAT1 | FAT Atypical Cadherin 1 |
| FDA | Food and Drug Administration |
| FGFR3 | Fibroblast Growth Factor Receptor 3 |
| FOXQ1 | Forkhead Box Q1 |
| GATK | Genome Analysis Toolkit |
| GENIE | Genomics Evidence Neoplasia Information Exchange (Project GENIE) |
| IDH2 | Isocitrate Dehydrogenase 2 |
| KDM6A | Lysine Demethylase 6A |
| KMT2D | Lysine Methyltransferase 2D |
| KRAS | Kirsten Rat Sarcoma Viral Oncogene Homolog |
| LAMB4 | Laminin Subunit Beta 4 |
| LATS2 | Large Tumor Suppressor Kinase 2 |
| LDLR | Low-Density Lipoprotein Receptor |
| LOH | Loss of Heterozygosity |
| MCM2 | Minichromosome Maintenance Complex Component 2 |
| NF1 | Neurofibromin 1 |
| NGS | Next-Generation Sequencing |
| NOTCH4 | Neurogenic Locus Notch Homolog 4 |
| NSD1 | Nuclear Receptor Binding SET Domain Protein 1 |
| PIK3CA | Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha |
| PRKDC | Protein Kinase, DNA-Activated, Catalytic Subunit |
| PTEN | Phosphatase and Tensin Homolog |
| RB1 | RB Transcriptional Corepressor 1 |
| SND1 | Staphylococcal Nuclease and Tudor Domain Containing 1 |
| SMAD4 | SMAD Family Member 4 |
| SNV | Single-Nucleotide Variant |
| TERT | Telomerase Reverse Transcriptase |
| TGF-β | Transforming Growth Factor Beta |
| TMB | Tumor Mutational Burden |
| TP53 | Tumor Protein p53 |
| TRAF7 | TNF Receptor Associated Factor 7 |
| TSC2 | TSC Complex Subunit 2 |
| TURBT | Transurethral Resection of Bladder Tumor |
| WEE1 | WEE1 G2 Checkpoint Kinase |
| WES | Whole-Exome Sequencing |
| WGS | Whole-Genome Sequencing |
References
- Dadhania, V.; Czerniak, B.; Guo, C.C. Adenocarcinoma of the urinary bladder. Am. J. Clin. Exp. Urol. 2015, 3, 51–63. [Google Scholar]
- Vasudevan, G.; Bishnu, A.; Singh, B.M.K.; Nayak, D.M.; Jain, P. Bladder Adenocarcinoma: A Per-sisting Diagnostic Dilemma. J. Clin. Diagn. Res. 2017, 11, ER01–ER04. [Google Scholar]
- Kamat, M.R.; Kulkarni, J.N.; Tongaonkar, H.B. Adenocarcinoma of the bladder: Study of 14 cases and review of the literature. Br. J. Urol. 1991, 68, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Kapur, P.; Lotan, Y.; King, E.; et al. Primary adenocarcinoma of the urinary bladder: Value of cell cycle biomarkers. Am. J. Clin. Pathol. 2011, 135, 822–830. [Google Scholar] [CrossRef]
- Roy, S.; Pradhan, D.; Ernst, W.L.; et al. Next-generation sequencing-based molecular characterization of primary urinary bladder adenocarcinoma. Mod. Pathol. 2017, 30, 1133–1143. [Google Scholar] [CrossRef] [PubMed]
- Alexander, R.E.; Lopez-Beltran, A.; Montironi, R.; et al. KRAS mutation is present in a small subset of primary urinary bladder adenocarcinomas. Histopathology 2012, 61, 1036–1042. [Google Scholar] [CrossRef]
- Santos, B.M.R.; de Souza, J.D.; Lima, R.S.B.C.; de Lima, E.M. Mucinous bladder adenocarcinoma: Case report and literature review. Case Rep. Urol. 2015, 2015, 783109. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.; Abdelrahman, I.; Abdelsalam, G. Survival of primary adenocarcinoma of the urinary bladder after radical treatment: National Cancer Institute, 5-years' experience. Egypt. J. Surg. 2019, 38, 429–438. [Google Scholar]
- Lu, H.; Zhu, W.; Mao, W.; et al. Trends of incidence and prognosis of primary adenocarcinoma of the bladder. Ther. Adv. Urol. 2021, 13, 17562872211018006. [Google Scholar] [CrossRef]
- Alexander, R.E.; Montironi, R.; Lopez-Beltran, A.; et al. EGFR alterations and EML4-ALK rear-rangement in primary adenocarcinoma of the urinary bladder. Mod. Pathol. 2014, 27, 107–112. [Google Scholar] [CrossRef]
- Yu, D.D.; Dong, H.; Chen, W.K.; et al. Development and validation of a nomogram for predicting sur-vival in patients with non-metastatic primary adenocarcinoma of the bladder. Transl. Cancer Res. 2020, 9, 5155–5165. [Google Scholar] [CrossRef]
- Kunze, E.; Schlott, T. High frequency of promoter methylation of the 14-3-3 σ and CAGE-1 genes, but lack of hypermethylation of the caveolin-1 gene, in primary adenocarcinomas and signet ring cell carcinomas of the urinary bladder. Int. J. Mol. Med. 2007, 20, 557–563. [Google Scholar] [CrossRef]
- Varadi, M.; Nagy, N.; Reis, H.; et al. Clinical sequencing identifies potential actionable alterations in a high rate of urachal and primary bladder adenocarcinomas. Cancer Med. 2023, 12, 9041–9054. [Google Scholar] [CrossRef]
- Wang, Y.; Chang, Q.; Li, Y. Racial differences in urinary bladder cancer in the United States. Sci. Rep. 2018, 8, 12521. [Google Scholar] [CrossRef]
- American Cancer Society. Key Statistics for Bladder Cancer. Available online: https://www.cancer.org/cancer/types/bladder-cancer/about/key-statistics.html (accessed on 26 November 2025).
- Donehower, L.A.; Soussi, T.; Korkut, A.; Liu, Y.; Schultz, A.; Cardenas, M.; et al. Integrated Analysis of TP53 Gene and Pathway Alterations in The Cancer Genome Atlas. Cell Rep. 2019, 28, 1370–1384.e5. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.; Pan, C.; Bei, J.-X.; Li, B.; Liang, C.; Xu, Y.; Fu, X. Mutant p53 in Cancer Progression and Targeted Therapies. Front. Oncol. 2020, 10, 595187. [Google Scholar] [CrossRef]
- Kompier, L.C.; Lurkin, I.; van der Aa, M.N.M.; van Rhijn, B.W.G.; van der Kwast, T.H.; et al. FGFR3, HRAS, KRAS, NRAS and PIK3CA Mutations in Bladder Cancer and Their Potential as Biomarkers for Surveillance and Therapy. PLoS ONE 2010, 5, e13821. [Google Scholar] [CrossRef] [PubMed]
- Uniyal, P.; Kashyap, V.K.; Behl, T.; Parashar, D.; Rawat, R. KRAS Mutations in Cancer: Understanding Signaling Pathways to Immune Regulation and the Potential of Immunotherapy. Cancers 2025, 17, 785. [Google Scholar] [CrossRef]
- Pires-Luis, A.S.; Martinek, P.; Alaghehbandan, R.; Trpkov, K.; Comperat, E.M.; Perez Montiel, D.M.; Bulimbasic, S.; Lobo, J.; Henrique, R.; Vanecek, T.; Pivovarcikova, K.; Michalova, K.; Pitra, T.; Hora, M.; Marques, A.; Lopes, J.M.; Rogala, J.; Mareckova, J.; Michal, M.; Hes, O. Molecular Genetic Features of Primary Nonurachal Enteric-type Adenocarcinoma, Urachal Adenocarcinoma, Mucinous Adenocarcinoma, and Intestinal Metaplasia/Adenoma: Review of the Literature and Next-generation Sequencing Study. Adv. Anat. Pathol. 2020, 27, 303–310. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. FDA grants accelerated approval to adagrasib with cetuximab for KRAS G12C-mutated colorectal cancer. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-adagrasib-cetuximab-kras-g12c-mutated-colorectal-cancer (accessed on 14 December 2025).
- U.S. Food and Drug Administration. FDA approves sotorasib with panitumumab for KRAS G12C-mutated colorectal cancer. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-sotorasib-panitumumab-kras-g12c-mutated-colorectal-cancer (accessed on 14 December 2025).
- Peng, Y.; Wang, Y.; Zhou, C.; Mei, W.; Zeng, C. PI3K/Akt/mTOR Pathway and Its Role in Cancer Therapeutics: Are We Making Headway? Front. Oncol. 2022, 12, 819128. [Google Scholar] [CrossRef]
- Payne, S.N.; Maher, M.E.; Tran, N.H.; Van De Hey, D.R.; Foley, T.M.; Yueh, A.E.; Leystra, A.A.; Pasch, C.A.; Jeffrey, J.J.; Clipson, L.; Matkowskyj, K.A.; Deming, D.A. PIK3CA mutations can initiate pancreatic tumorigenesis and are targetable with PI3K inhibitors. Oncogenesis 2015, 4, e169. [Google Scholar] [CrossRef]
- Faltas, B.M. Elucidating the Role of PIK3CA in Early-Stage Bladder Tumorigenesis: New Insights from a Novel Transgenic Mouse Model. Am. J. Pathol. 2023, 193, 1914–1915. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA approves alpelisib for PIK3CA-related overgrowth spectrum. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-alpelisib-pik3ca-related-overgrowth-spectrum (accessed on 14 December 2025).
- Chang, D.Y.; Ma, W.L.; Lu, Y.S. Role of Alpelisib in the Treatment of PIK3CA-Mutated Breast Cancer: Patient Selection and Clinical Perspectives. Ther. Clin. Risk Manag. 2021, 17, 193–207. [Google Scholar] [CrossRef]
- Kim, S.T.; Lee, J.; Park, S.H.; Park, J.O.; Park, Y.S.; Kang, W.K.; Lim, H.Y. Prospective phase II trial of everolimus in PIK3CA amplification/mutation and/or PTEN loss patients with advanced solid tumors refractory to standard therapy. BMC Cancer 2017, 17, 211. [Google Scholar] [CrossRef]
- Fleming, G.F.; Ma, C.X.; Huo, D.; Sattar, H.; Tretiakova, M.; Lin, L.; Hahn, O.M.; Olopade, F.O.; Nanda, R.; Hoffman, P.C.; Naughton, M.J.; Pluard, T.; Conzen, S.D.; Ellis, M.J. Phase II trial of temsirolimus in patients with metastatic breast cancer. Breast Cancer Res. Treat. 2012, 136, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Conde, M.; Frew, I.J. Therapeutic significance of ARID1A mutation in bladder cancer. Neoplasia 2022, 31, 100814. [Google Scholar] [CrossRef]
- Wu, J.; Jiang, Y.; Zhang, Q.; Mao, X.; Wu, T.; Hao, M.; Zhang, S.; Meng, Y.; Wan, X.; Qiu, L.; Han, J. KDM6A-SND1 interaction maintains genomic stability by protecting the nascent DNA and contributes to cancer chemoresistance. Nucleic Acids Res. 2024, 52, 7665–7686. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Mishra, L.; Deng, C.X. The role of TGF-β/SMAD4 signaling in cancer. Int. J. Biol. Sci. 2018, 14, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Hua, C.; Chen, J.; Li, S.; Zhou, J.; Fu, J.; Sun, W.; Wang, W. KDM6 Demethylases and Their Roles in Human Cancers. Front. Oncol. 2021, 11, 779918. [Google Scholar] [CrossRef]
Figure 1.
OncoPrint showing recurrently altered genes in the bladder adenocarcinoma cohort. This is with sequencing coverage of at least 100× (≥100×) and VAF of at least 5% (VAF ≥ 5%). Asterisks denote samples that lack complete genomic profiles.
Figure 1.
OncoPrint showing recurrently altered genes in the bladder adenocarcinoma cohort. This is with sequencing coverage of at least 100× (≥100×) and VAF of at least 5% (VAF ≥ 5%). Asterisks denote samples that lack complete genomic profiles.
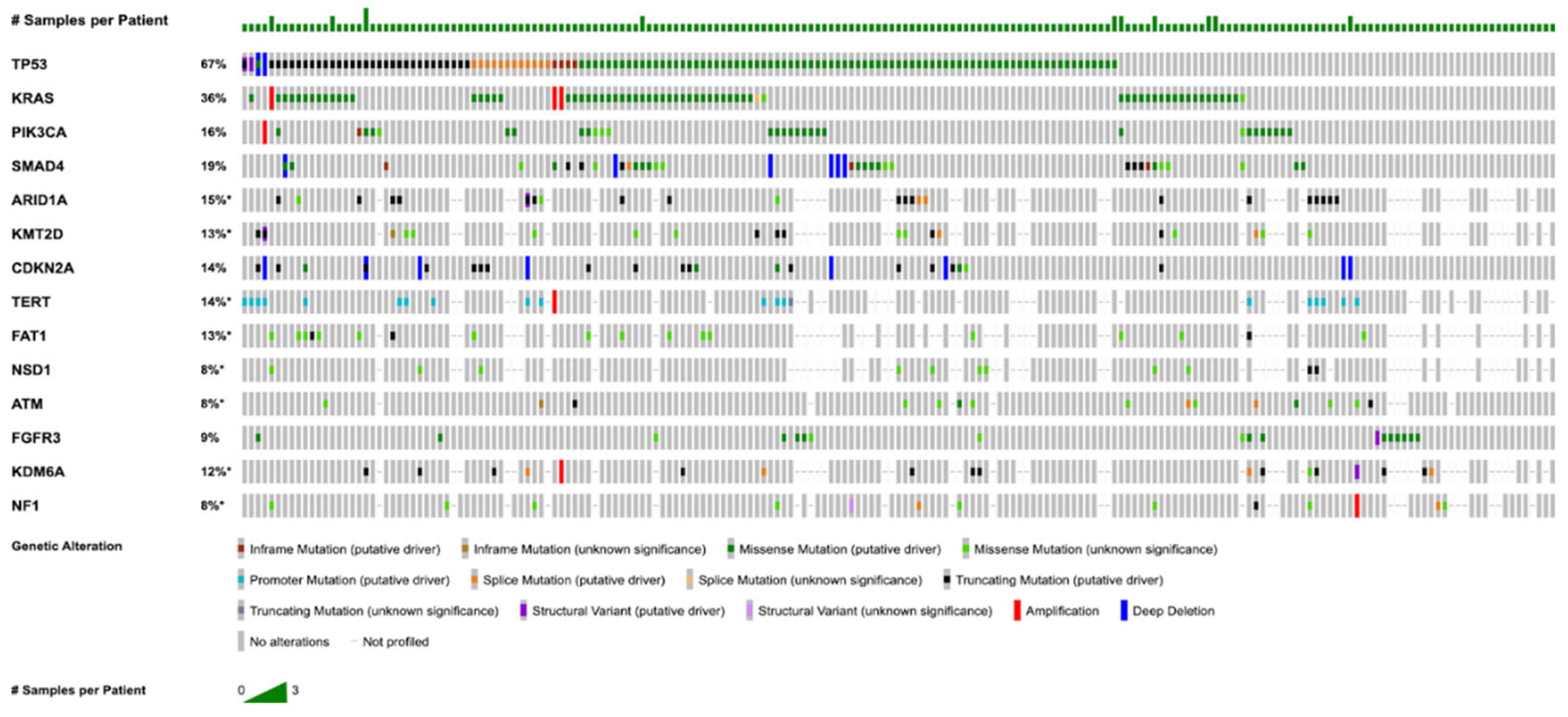

Table 1.
Bladder Adenocarcinoma Patient and Sample Characteristics.
| Demographics | Category | n (%) |
|---|---|---|
| Sex | Male Female |
119 (61.0%) 76 (39.0%) |
| Age Category | Adult Pediatric |
195 (100.0%) 0 (0.0%) |
| Ethnicity | Non-Hispanic Unknown/Not Collected Hispanic |
96 (49.2%) 84 (43.0%) 15 (7.7%) |
| Race | Asian White Black Other Unknown |
9 (4.6%) 84 (43.1%) 20 (10.3 %) 53 (27.2%) 23 (11.8%) |
| Sample Type | Primary Metastasis Not Collected |
85 (41.3%) 68 (32.9%) 53 (25.7%) |
Table 2.
Race and Associated Mutation Enrichment.
| Gene (Chi-squared) | Asian, n (%) | White, n (%) | p Value |
|---|---|---|---|
| ANKRD26 EME1 NEIL3 FANCD2 EGFR |
1 (50.00) 1 (100.00) 1 (100.00) 2 (50.00) 2 (22.22) |
0 (0.00) 0 (0.00) 0 (0.00) 2 (4.55) 2 (2.25) |
p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



