Submitted:
15 December 2025
Posted:
16 December 2025
Read the latest preprint version here
Abstract
Purpose: To evaluate the safety and efficacy of the eight-chop technique in phacoemulsification for white cataracts.Methods: The lens capsule was stained with brilliant blue G (BBG) and nucleus was cracked using the Eight-chopper. The best-corrected visual acuity (BCVA), corneal endothelial cell density (CECD), and intraocular pressure (IOP) were evaluated. The primary outcome measures were the mean operative time, mean phaco time, aspiration time, cumulative dissipated energy (CDE), and volume of fluid used.Results: The lens capsule visualization was sufficient with BBG. The mean (standard deviation, SD) operative time was 11.40 ± 4.42 minutes. The mean (SD) phaco time was 31.4 ± 15.3 seconds. The corresponding values for aspiration time, CDE, and volume of fluid used were 2.50 ± 0.72 minutes, 12.12 ± 7.07, and 61.9 ± 15.8 mL, respectively. The BCVA improved significantly (p<0.01). The CECD decreased by 5.5% at 7 weeks and 3.7% at 19 weeks postoperatively. The rate of IOP reduction was 7.3% at 7 weeks and 9.5% at 19 weeks postoperatively.Conclusions: The eight-chop technique is safe and effective in phacoemulsification and may reduce postoperative CECD loss and lower IOP in eyes with white cataracts. BBG staining may be safe for corneal endothelial cells.
Keywords:
cataract surgery
; phacoemulsification
; white cataract
; corneal endothelial cell
; eight-chop technique
Introduction
Akahoshi first developed the prechop technique in 1992 and presented it at the American Society of Cataract and Refractive Surgery Film Festival in 1994 [1]. The prechop technique manually divides the nucleus under ophthalmic viscosurgical device material prior to phacoemulsification [1]. Compared to conventional grooving, divide-and-conquer, and phaco-chop techniques, the total ultrasound energy required in the prechop technique is drastically reduced, and the operative time and volume of fluid used are significantly lower [2]. I developed the eight-chop technique in 2002 as an extension of the prechop technique and presented this technique at the 32nd Annual Meeting of the Japanese Society of Ophthalmic Surgery in 2009 [3,4]. The eight-chop technique is characterized by the division of the lens nucleus into eight segments, rather than four segments as in the prechop technique [2]. The Lance-chop technique is an eight-chop technique that uses the Lance-chopper and nucleus sustainer for cases with a hard lens nucleus and this technique was presented at the 42nd Annual Meeting of the Japanese Society of Ophthalmic Surgery in 2019. Since the Eight-chopper II cannot be inserted into a hard lens, the Lance-chop technique is used to divide the lens nucleus by inserting the Lance-chopper into the lens nucleus while supporting the lens equator with the nucleus sustainer and avoiding stress on the posterior lens capsule and zonules. Therefore, the eight-chop technique is safe and effective in dividing the hard lens nucleus. Since the lens nucleus of white cataract is often very hard, it is important to safely and efficiently emulsify the hard lens nucleus. The eight-chop technique is considered ideal for white cataracts. I attempted to verify the effectiveness of the eight-chop technique for the treatment of white cataracts. In this paper, to avoid confusion, the Lance-chop technique will be referred to as the eight-chop technique.
A white cataract is defined as a condition in which the crystalline lens is completely cloudy, and the fundus is invisible and lacks the red reflex. Advances in surgical techniques and phaco machines have increased the uptake of phacoemulsification in cataract treatment in developed countries. However, even for specialists with extensive surgical experience, phacoemulsification is difficult and associated with high rates of complications in eyes with white cataracts. Therefore, it is prudent to develop a safer and more effective surgical strategy for white cataracts.
An appropriate continuous curvilinear capsulorhexis (CCC) is critical for safe phacoemulsification, and complete CCC minimizes the risk of posterior capsular rupture and stabilizes the intraocular lens in the capsule. The incidence of incomplete capsulorhexis associated with white cataract surgery has been estimated in the range of 3.85% and 28.3% [5,6]. Therefore, in eyes with white cataracts, it is important to first complete CCC, which requires staining and visualization of the lens capsule. The use of brilliant blue G (BBG) has improved capsular visualization, enabling a complete capsulorhexis without evidence of toxicity in a rat model [7]. However, studies of eyes with white cataracts have used trypan blue for lens capsule staining, and BBG has not been used in any of the studies [5,8,9,10]. This study is the first to use BBG for staining in eyes with white cataracts. This study was conducted to evaluate the eight-chop technique based on intraoperative outcome measures and postoperative changes in corneal endothelial cell density (CECD) and intraocular pressure (IOP). Furthermore, this study is the first to report on intraoperative outcome measures such as operative time, phaco time, aspiration time, CDE, and volume of fluid used in eyes with white cataracts. Additionally, the lens capsules were stained with BBG, which has little effect on intraocular tissues, and the possibility of visualizing the lens capsule in eyes with white cataracts and its effect on corneal endothelial cells were examined.
Methods
This study included the eyes of patients with cataracts who had undergone phacoemulsification and posterior chamber intraocular lens (IOL) implantation between January 2010 and June 2022. Patients who had visited the clinic with a diagnosis of white cataracts were enrolled in the study. All eyes in white cataract patients lacked the red fundus reflex. Cataracts appearing white on slit-lamp examination were defined as white cataracts. The exclusion criteria were corneal disease or opacity, uveitis, and previous trauma or surgery.
The study protocol adhered to the guidelines of the Declaration of Helsinki and was approved by the review board. Informed consent for participation in this study was obtained from each patient. BBG has been approved by the European Union for human use and is in the process of being approved by the Ministry of Health and Welfare in Japan. Therefore, the use in this study was approved by the institutional review board.
Preoperatively, all patients underwent slit-lamp and retinal examinations, and their best-corrected visual acuity (BCVA) (Snellen) and IOP were measured. Endothelial cell density (cells/mm2) was measured using a noncontact specular microscope (EM-3000, Topcon, Hasunumacho, Tokyo, Japan). The firmness of the nucleus was graded using the Emery classification [11] by the surgeon intraoperatively during phacoemulsification. Phacoemulsification was performed by the same surgeon, who was experienced in the eight-chop technique, using the phacoemulsification unit (Alcon Labs Inc, Fort Worth, Texas, USA). All surgeries were captured by a video camera and recorded on a hard disk.
A new surgical instrument was designed and developed to perform the eight-chop technique [3,4]. The research team designed the eight-choppers and requested a manufacturing company to produce them. The Eight-chopper II (SP-8402; ASICO, Westmont, Illinois, USA) has a smaller tip (2.5 mm long and 0.8 mm wide) that is angled so that it can be inserted vertically into the lens nucleus for the Grade II group. The Lance-chopper (SP-9989; ASICO, Westmont, Illinois, USA) has a small tip with a length and width of 3.0 mm and 1.3 mm, respectively, as well as a sharper leading edge, and was used for the Grade III and IV groups. Normally, the Eight-chopper II is used for Grade III cases; however, due to the fragility of the lens capsule, the Lance-chopper was used for Grade III cases in this study.
In all operations, a temporal, clear, corneal incision was formed using a 3.0-mm steel keratome. BBG (0.025%) was used to improve visualization of the capsule in all cases. The staining of the lens capsule was confirmed by video recording in each case. A deliberately small CCC enlarged secondarily by the two-stage CCC technique [12] was used (Figure 1b). After the injection of sodium hyaluronate into the anterior chamber, a 6.2–6.5-mm CCC was created with a capsule forceps (Figure 1d). The soft-shell technique [13] was used in all cases. Hydrodissection was performed with a 27-G cannula. The lens nucleus was cracked into eight segments using the Eight-chopper II in five cases or the Lance-chopper in 76 cases (Figure 2). A one side-port incision was made using the 23-G microvitreoretinal knife at 90° from the main incision for the Grade III and IV groups. The eight segments were phacoemulsified and aspirated at the depth of the iris plane. The capsular bag was aspirated with the irrigation/aspiration tip to remove cortical material. Ophthalmic viscosurgical device was injected and a foldable IOL (Alcon Labs Inc, Fort Worth, Texas, USA) with polymethyl methacrylate haptics was inserted into the capsular bag with an injector system. The ophthalmic viscosurgical device was then aspirated. The phacoemulsification unit (Alcon Labs Inc, Fort Worth, Texas, USA) had a flow rate of 32 mL/min, a maximum ultrasound power of 80%, and a 1.1-mm flared tip. The wound was sealed using stromal hydration if necessary. At the end of the operation, the anterior chamber was replaced by balanced salt solution containing moxifloxacin (0.5 mg/mL).
The intraoperative outcome measures were operative time (minutes), phaco time (seconds), aspiration time (minutes), cumulative dissipated energy (CDE), volume of fluid used (mL), and the rate of intraoperative complications. The operative time was measured from the beginning of the corneal incision to the end of ophthalmic viscosurgical device aspiration. Patients were followed up on postoperative days 1 and 2 and at postoperative weeks 1, 3, 7, and 19. The postoperative outcome measures were BCVA, IOP measurements, and CECD (cells/mm2). Data on the outcome measures at 7 and 19 weeks postoperatively were used to conduct the present study.
Statistical analyses were performed to compare the results among the groups using either one-way analysis of variance (ANOVA) or the Kruskal-Wallis test, or the Kruskal-Wallis test followed by the Steel-Dwass post-hoc test using Excel Toukei® (version 7.0, Esumi Co. Ltd., Shimane, Japan). Values of p <0.05 were considered statistically significant.
Results
This study comprised 81 eyes of 78 cataract patients who had undergone phacoemulsification and posterior chamber IOL implantation. The patients’ characteristics and intraoperative parameters are shown in Table 1. There were significant differences in the mean ages and mean operative time among the groups (p<0.01, p=0.005, respectively, Kruskal-Wallis test). However, there was no significant difference in the mean operative time between Grade II and III cases (p=0.73, Steel-Dwass post-hoc test), and there was no significant difference in the mean operative time between Grade II and IV cases (p=0.084, Steel-Dwass post-hoc test), while the mean operative time in the Grade III group was significantly shorter than that in the Grade IV group (p=0.015, Steel-Dwass post-hoc test). There were significant differences in the mean phaco time among the groups (p<0.01, Kruskal-Wallis test). However, there was no significant difference in the mean phaco time between Grade II and Grade III groups (p=0.80, Steel-Dwass post-hoc test), and there was no significant difference in the mean phaco time between Grade II and IV groups (p=0.067, Steel-Dwass post-hoc test), while the mean phaco time in the Grade III group was significantly shorter than that in the Grade IV group (p<0.01, Steel-Dwass post-hoc test). There was no significant difference in the aspiration time among the groups (p=0.63, Kruskal-Wallis test). There were significant differences in the CDE among the groups (p<0.01, Kruskal-Wallis test); however, there was no significant difference in the CDE between Grade II and III groups (p=0.38, Steel-Dwass post-hoc test). The CDE values in the Grade III group were lower than those in the Grade IV group (p<0.01, Steel-Dwass post-hoc test), and the CDE values in the Grade II group were lower than those in the Grade IV group (p=0.016, Steel-Dwass post-hoc test). There was no significant difference in the volume of fluid used among the groups (p=0.27, Kruskal-Wallis test).
The changes in BCVA in each group are shown in Table 2. There were significant differences in the BCVA between the groups preoperatively and at 7 weeks postoperatively (p<0.01, one-way ANOVA). However, there was no significant differences in the BCVA between the groups at 7 weeks and 19 weeks postoperatively (p=1.00, one-way ANOVA). The BCVA between the groups also differed significantly preoperatively and at 19 weeks postoperatively (p<0.01, one-way ANOVA).
The changes in the CECD are shown in Table 2. The CECD decreased by 5.5% at 7 weeks and by 3.7% at 19 weeks postoperatively compared to the values preoperatively; this change was not statistically significant. (p=0.25, one-way ANOVA).
The changes in the IOP are shown in Table 2. The IOP was slightly lower at 7 and 19 weeks postoperatively than the preoperative IOP. The rate of IOP reduction was 7.3% at 7 weeks and 9.5% at 19 weeks postoperatively; however, the reduction in IOP was not statistically significant (p=0.070, one-way ANOVA).
The lens capsule visualization was sufficient and there was no incident of perioperative complications.
Intraocular complications included capsulorhexis tears in 2 (2.5%) eyes, posterior capsule rupture in 1 (1.2%) eye.
Discussion
This study revealed that the operative time for the eight-chop technique in eyes with white cataracts was 11.4 minutes; previous studies using other techniques have found operative times to be in the range of 12.2-22 minutes [9,10]. However, a comparison of operative times is not possible in studies of eyes with white cataracts because few studies to date have reported on operative times. This study also showed that the eight-chop technique has a shorter phaco time and less CDE, and requires only one-third to one-fourth the volume of fluid used compared to other techniques used in cases other than white cataracts [13,14,15,16,17,18,19,20]. In particular, the use of low fluid volume means that ultrasound and irrigation/aspiration tips are inserted into the eye for a short period of time, which may have little impact on ocular tissues other than corneal endothelial cells. Although operative time may be an important indicator of technical efficiency, few other studies, including those on white cataracts, have reported on the operative time. Comparator techniques are often required as a control condition in testing new techniques; however, we believe that surgical techniques may be evaluated using intraoperative outcomes and using these parameters when there are clinical difficulties.Phacoemulsification carries a significantly higher risk of severe cell loss in patients with hard cataracts relative to extracapsular cataract extraction [21]. Furthermore, CECD represents the true summation of intraocular insult during surgery, and its assessment is the key to its comparison between various techniques [22]. The percentage of ECD loss after routine phacoemulsification has been estimated in the range of 3.5% and 23.2% [18,21,23,24]. Studies of white cataracts have also reported reductions in ECD loss in the range of 8.5 to 18.6% [5,9,25,26]; however, herein, the reduction was only 3.7%, representing a non-significant change relative to baseline values. This finding suggests that the eight-chop technique may be useful in the treatment white cataracts.
BBG has been widely used for protein staining in the field of biology [27]. The efficacy of BBG was evaluated using enucleated pig eyes; the conclusion was that a concentration of 0.025 mg/mL or higher could sufficiently stain the anterior capsule [7]. In addition, the safety of BBG has been evaluated in rat eyes and 0.025 mg/mL BBG has shown lower toxicity than 1.0 mg/mL trypan blue or 5 mg/mL indocyanine green [7]. In contrast, indocyanine green and trypan blue showed degeneration of corneal endothelial cells on transmission and scanning electron microscopy [7]. Several studies have shown BBG to be a safer dye than indocyanine green or trypan blue for staining the inner limiting membrane [28,29,30]. Results from the present study regarding CECD are consistent with previous studies [7,28,29,30] suggesting that BBG is safe for staining the internal limiting membrane.
A decrease in the IOP after cataract surgery has been reported in both non-glaucoma and glaucoma patients [31,32,33,34]. Although changes in the IOP in eyes with white cataracts are clinically relevant, few other studies have evaluated them. The rate of IOP reduction in the present study was 7.3% at 7 weeks and 9.5% at 19 weeks postoperatively; however, this finding was not significant. The eight-chop technique is considered effective for cataract patients with concomitant glaucoma, given its extremely short operative time, and may be effective for patients with white cataracts given the IOP reduction; this application should be evaluated in future studies.
Table 3 shows the surgical technique, operative time, phaco time, and changes in corneal endothelial cells and IOP reported in previous studies on phacoemulsification in eyes with white cataracts [5,6,8,9,10,25,26,35].
Surgical techniques used in previous studies is not ideal for handling the hard lens nucleus of white cataracts, since the lens nucleus is first phacoemulsified with an ultrasound tip. Phacoemulsification of the hard lens nucleus with an ultrasound tip places strong stress on the posterior lens capsule and zonules, and there is a high risk of posterior capsule rupture or dialysis of the zonules. However, the eight-chop technique is extremely effective in dividing the hard lens nucleus. In addition, since a fragile lens capsule and weak zonules are often encountered in white cataracts, complications such as posterior capsule rupture and dialysis of the zonules are likely to occur with techniques such as divide-and-conquer and phaco-chop.
In contrast to previous studies, the eight-chop and prechop technique can safely divide the hard lens without stressing the zonules, making it possible to perform phacoemulsification surgery even in cases in which division of the lens nucleus is impossible with the phaco-chop or divide-and-conquer techniques. There are a few differences between the prechop and eight-chop techniques. First, in the prechop technique, the lens nucleus is usually divided into four sections [1,2], whereas in the eight-chop technique, the lens nucleus is always divided into eight sections; this is the main advantage of the eight-chop technique over the prechop technique as the smaller pieces of the divided lens nucleus allow for more efficient phacoemulsification and aspiration. The second difference is the development and use of special choppers with sharper and more delicate tips, such as the Eight-chopper II and Lance-chopper. These surgical instruments facilitate the eight-piece division of the lens nucleus, which is very difficult with the surgical instruments used in the prechop technique. Furthermore, these instruments are very useful in difficult cases because they reduce stress on the zonules and lens capsule.
Another advantage of the eight-chop technique over the divide-and-conquer and phaco-chop techniques is that it separates the division of the lens nucleus for phacoemulsification and aspiration, allowing the surgeon to concentrate on the individual procedures. In the divide-and-conquer and phaco-chop techniques, wherein lens nucleus division and phacoemulsification are performed simultaneously, the accuracy of each procedure may be compromised. If one procedure is given more attention, lens nucleus division and phacoemulsification and aspiration can be performed with more certainty.
The main limitation of this study is the lack of a control group consisting of patients undergoing cataract surgery by the divide-and-conquer technique or phaco-chop technique to directly compare postoperative outcomes. Nevertheless, this study demonstrates that the eight-chop technique is safe and efficient in the treatment of white cataracts. The main disadvantage of this technique is the delicate intraocular manipulation. However, once cataract surgeons become familiar with the use of our eight-choppers, they may use the eight-chop technique for the treatment of a variety of cataracts, including white cataracts, and in difficult cases.
Author Contributions
Tsuyoshi Sato wrote the main manuscript text and prepared all figures, tables and video. Tsuyoshi Sato reviewed the manuscript.
Funding
There was no funding for this study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Conflict of Interest
The author has no commercial or proprietary interest in any of the companies, products, or methods described in this article.
Abbreviation
BBG = brilliant blue G; BCVA = best-corrected visual acuity; CECD = corneal endothelial cell density; IOP = intraocular pressure; CDE = cumulative dissipated energy; SD = standard deviation; CCC = continuous curvilinear capsulorhexis; ANOVA = analysis of variance
References
- Akahoshi, T. Phaco Prechop. In Phaco Chop and Advanced Phaco Techniques, Second Edition ed.; Chang, D.F., Ed.; SLACK Incorporated: Thorofare, 2013; pp. 55-76.
- Akahoshi, T. Phaco Prechop: Re-evaluation of single-handed phacoemulsification using a new nucleofracture technique. Atarashii Ganka 1999, 16, 1219-1233.
- Sato, T. Efficacy and safety of the eight-chop technique in phacoemulsification for cataract patients. J Cataract Refract Surg 2023. [CrossRef]
- Sato, T. Effects of the eight-chop technique in phacoemulsification on intraocular pressure in patients with primary open-angle glaucoma and controls. EC Ophthalmology 2023, 14, 1–11.
- Jacob, S.; Agarwal, A.; Agarwal, A.; Agarwal, S.; Chowdhary, S.; Chowdhary, R.; Bagmar, A.A. Trypan blue as an adjunct for safe phacoemulsification in eyes with white cataract. J Cataract Refract Surg 2002, 28, 1819-1825. [CrossRef]
- Chakrabarti, A.; Singh, S. Phacoemulsification in eyes with white cataract. J Cataract Refract Surg 2000, 26, 1041-1047. [CrossRef]
- Hisatomi, T.; Enaida, H.; Matsumoto, H.; Kagimoto, T.; Ueno, A.; Hata, Y.; Kubota, T.; Goto, Y.; Ishibashi, T. Staining ability and biocompatibility of brilliant blue G: Preclinical study of brilliant blue G as an adjunct for capsular staining. Arch Ophthalmol 2006, 124, 514-519. [CrossRef]
- Ermisş, S.S.; Oztürk, F.; Inan, U.U. Comparing the efficacy and safety of phacoemulsification in white mature and other types of senile cataracts. Br J Ophthalmol 2003, 87, 1356-1359. [CrossRef]
- Wong, V.W.; Lai, T.Y.; Lee, G.K.; Lam, P.T.; Lam, D.S. Safety and efficacy of micro-incisional cataract surgery with bimanual phacoemulsification for white mature cataract. Ophthalmologica 2007, 221, 24-28. [CrossRef]
- Venkatesh, R.; Tan, C.S.; Sengupta, S.; Ravindran, R.D.; Krishnan, K.T.; Chang, D.F. Phacoemulsification versus manual small-incision cataract surgery for white cataract. J Cataract Refract Surg 2010, 36, 1849-1854. [CrossRef]
- Emery, J.M. Kelman phacoemulsification; patient selection. In Extracapsular Cataract Surgery, Emery, J.M., Mclyntyre, D.J., Eds.; CV Mosby: St Louis, 1983; pp. 95-100.
- Gimbel, H.V.; Willerscheidt, A.B. What to do with limited view: The intumescent cataract. J Cataract Refract Surg 1993, 19, 657-661. [CrossRef]
- Miyata, K.; Nagamoto, T.; Maruoka, S.; Tanabe, T.; Nakahara, M.; Amano, S. Efficacy and safety of the soft-shell technique in cases with a hard lens nucleus. J Cataract Refract Surg 2002, 28, 1546-1550. [CrossRef]
- Helvacioglu, F.; Yeter, C.; Tunc, Z.; Sencan, S. Outcomes of torsional microcoaxial phacoemulsification performed by 12-degree and 22-degree bent tips. J Cataract Refract Surg 2013, 39, 1219-1225. [CrossRef]
- Sato, M.; Sakata, C.; Yabe, M.; Oshika, T. Soft-shell technique using Viscoat and Healon 5: A prospective, randomized comparison between a dispersive-viscoadaptive and a dispersive-cohesive soft-shell technique. Acta Ophthalmol 2008, 86, 65-70. [CrossRef]
- Abdelmotaal, H.; Abdel-Radi, M.; Rateb, M.F.; Eldaly, Z.H.; Abdelazeem, K. Comparison of the phaco chop and drill-and-crack techniques for phacoemulsification of hard cataracts: A fellow eye study. Acta Ophthalmol 2021, 99, e378-e386. [CrossRef]
- Park, J.; Yum, H.R.; Kim, M.S.; Harrison, A.R.; Kim, E.C. Comparison of phaco-chop, divide-and-conquer, and stop-and-chop phaco techniques in microincision coaxial cataract surgery. J Cataract Refract Surg 2013, 39, 1463-1469. [CrossRef]
- Storr-Paulsen, A.; Norregaard, J.C.; Ahmed, S.; Storr-Paulsen, T.; Pedersen, T.H. Endothelial cell damage after cataract surgery: Divide-and-conquer versus phaco-chop technique. J Cataract Refract Surg 2008, 34, 996-1000. [CrossRef]
- Helvacioglu, F.; Yeter, C.; Sencan, S.; Tunc, Z.; Uyar, O.M. Comparison of two different ultrasound methods of phacoemulsification. Am J Ophthalmol 2014, 158, 221-226.e221. [CrossRef]
- Igarashi, T.; Ohsawa, I.; Kobayashi, M.; Umemoto, Y.; Arima, T.; Suzuki, H.; Igarashi, T.; Otsuka, T.; Takahashi, H. Effects of hydrogen in prevention of corneal endothelial damage during phacoemulsification: A prospective randomized clinical trial. Am J Ophthalmol 2019, 207, 10-17. [CrossRef]
- Bourne, R.R.; Minassian, D.C.; Dart, J.K.; Rosen, P.; Kaushal, S.; Wingate, N. Effect of cataract surgery on the corneal endothelium: Modern phacoemulsification compared with extracapsular cataract surgery. Ophthalmology 2004, 111, 679-685. [CrossRef]
- Upadhyay, S.; Sharma, P.; Chouhan, J.K.; Goyal, R. Comparative evaluation of modified crater (endonucleation) chop and conventional crater chop techniques during phacoemulsification of hard nuclear cataracts: A randomized study. Indian J Ophthalmol 2022, 70, 794-798. [CrossRef]
- Kosrirukvongs, P.; Slade, S.G.; Berkeley, R.G. Corneal endothelial changes after divide and conquer versus chip and flip phacoemulsification. J Cataract Refract Surg 1997, 23, 1006-1012. [CrossRef]
- Díaz-Valle, D.; Benítez del Castillo Sánchez, J.M.; Castillo, A.; Sayagués, O.; Moriche, M. Endothelial damage with cataract surgery techniques. J Cataract Refract Surg 1998, 24, 951-955. [CrossRef]
- Vasavada, A.; Singh, R.; Desai, J. Phacoemulsification of white mature cataracts. J Cataract Refract Surg 1998, 24, 270-277. [CrossRef]
- Vajpayee, R.B.; Bansal, A.; Sharma, N.; Dada, T.; Dada, V.K. Phacoemulsification of white hypermature cataract. J Cataract Refract Surg 1999, 25, 1157-1160. [CrossRef]
- Enaida, H.; Kumano, Y.; Ueno, A.; Yoshida, S.; Nakao, S.; Numa, S.; Matsui, T.; Ishibashi, T. Quantitative analysis of vitreous and plasma concentrations of brilliant blue g after use as a surgical adjuvant in chromovitrectomy. Retina 2013, 33, 2170-2174. [CrossRef]
- Ueno, A.; Hisatomi, T.; Enaida, H.; Kagimoto, T.; Mochizuki, Y.; Goto, Y.; Kubota, T.; Hata, Y.; Ishibashi, T. Biocompatibility of brilliant blue G in a rat model of subretinal injection. Retina 2007, 27, 499-504. [CrossRef]
- Baba, T.; Hagiwara, A.; Sato, E.; Arai, M.; Oshitari, T.; Yamamoto, S. Comparison of vitrectomy with brilliant blue G or indocyanine green on retinal microstructure and function of eyes with macular hole. Ophthalmology 2012, 119, 2609-2615. [CrossRef]
- Takayama, K.; Sato, T.; Karasawa, Y.; Sato, S.; Ito, M.; Takeuchi, M. Phototoxicity of indocyanine green and Brilliant Blue G under continuous fluorescent illumination on cultured human retinal pigment epithelial cells. Invest Ophthalmol Vis Sci 2012, 53, 7389-7394. [CrossRef]
- Irak-Dersu, I.; Nilson, C.; Zabriskie, N.; Durcan, J.; Spencer, H.J.; Crandall, A. Intraocular pressure change after temporal clear corneal phacoemulsification in normal eyes. Acta Ophthalmol 2010, 88, 131-134. [CrossRef]
- Steuhl, K.P.; Marahrens, P.; Frohn, C.; Frohn, A. Intraocular pressure and anterior chamber depth before and after extracapsular cataract extraction with posterior chamber lens implantation. Ophthalmic Surg 1992, 23, 233-237.
- Tennen, D.G.; Masket, S. Short-and long-term effect of clear corneal incisions on intraocular pressure. J Cataract Refract Surg 1996, 22, 568-570. [CrossRef]
- Chen, P.P.; Lin, S.C.; Junk, A.K.; Radhakrishnan, S.; Singh, K.; Chen, T.C. The effect of phacoemulsification on intraocular pressure in glaucoma patients: A report by the American Academy of Ophthalmology. Ophthalmology 2015, 122, 1294-1307. [CrossRef]
- Brazitikos, P.D.; Tsinopoulos, I.T.; Papadopoulos, N.T.; Fotiadis, K.; Stangos, N.T. Ultrasonographic classification and phacoemulsification of white senile cataracts. Ophthalmology 1999, 106, 2178-2183. [CrossRef]
Figure 1.
(a) The lens capsule is visualized by staining with brilliant blue G (0.025%), (b) A 3.0–4.0-mm continuous curvilinear capsulorhexis (CCC) is created with a capsule forceps, (c) Liquefied cortical matter is aspirated to reduce intralenticular pressure through the CCC and the anterior chamber is reformed, (d) A 6.2–6.5-mm CCC is created with a capsule forceps.
Figure 1.
(a) The lens capsule is visualized by staining with brilliant blue G (0.025%), (b) A 3.0–4.0-mm continuous curvilinear capsulorhexis (CCC) is created with a capsule forceps, (c) Liquefied cortical matter is aspirated to reduce intralenticular pressure through the CCC and the anterior chamber is reformed, (d) A 6.2–6.5-mm CCC is created with a capsule forceps.
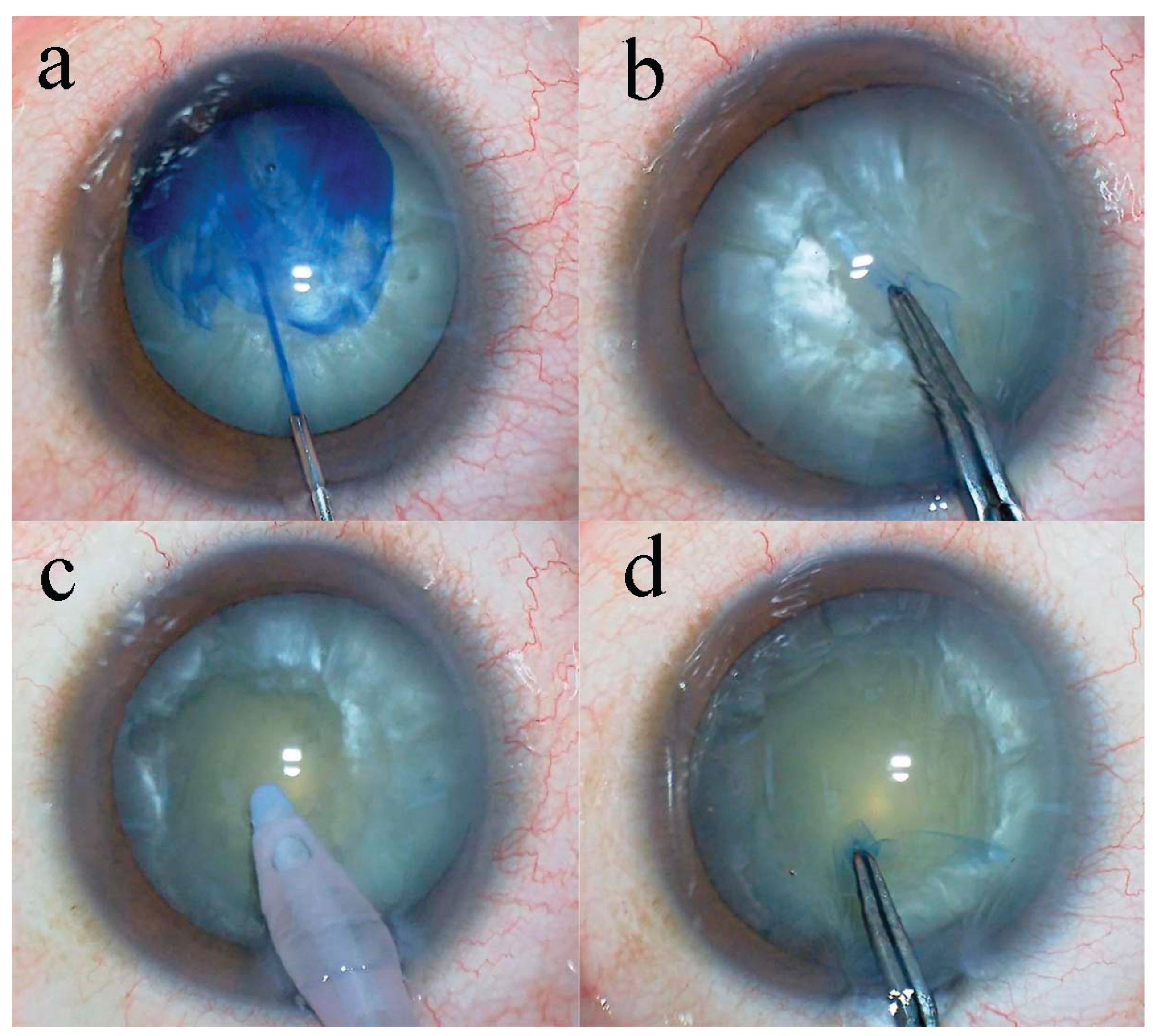
Figure 2.
(a) First, the lens nucleus is divided into hemispheres using the Lance-chopper while the nucleus sustainer (AE-2530; ASICO, Westmont, Illinois, USA) is inserted through the side port to support the equator of the lens nucleus, (b) Second, the lens nucleus is rotated 90° and divided into quadrants, (c) Third, the lens nucleus divided into quadrants is rotated 45° and divided into six segments, (d) Fourth, the remaining quarter of the lens nucleus is also divided to complete the eight-segmentation.
Figure 2.
(a) First, the lens nucleus is divided into hemispheres using the Lance-chopper while the nucleus sustainer (AE-2530; ASICO, Westmont, Illinois, USA) is inserted through the side port to support the equator of the lens nucleus, (b) Second, the lens nucleus is rotated 90° and divided into quadrants, (c) Third, the lens nucleus divided into quadrants is rotated 45° and divided into six segments, (d) Fourth, the remaining quarter of the lens nucleus is also divided to complete the eight-segmentation.
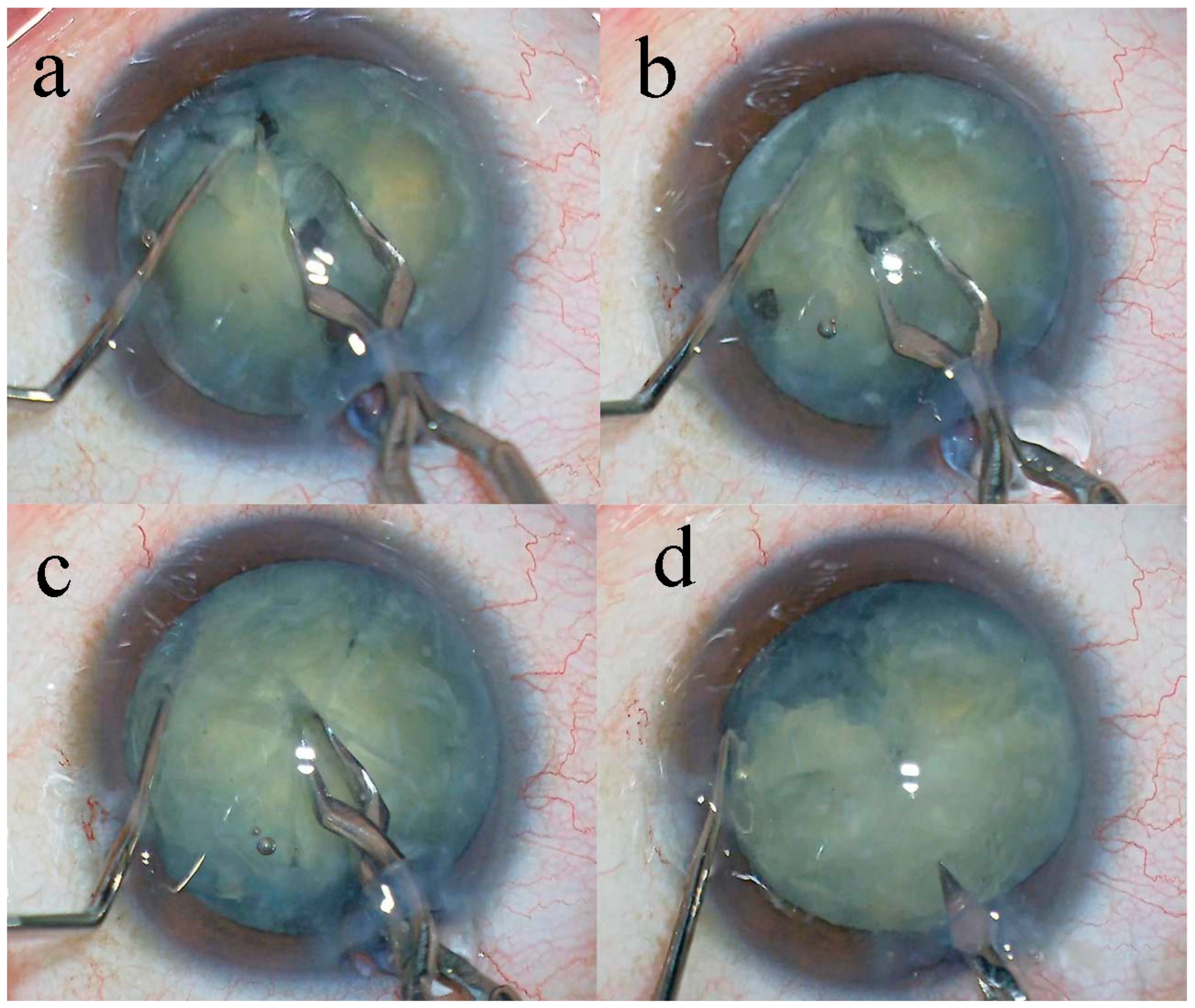

Table 1.
Preoperative characteristics and intraoperative parameters.
| Characteristics/Parameters | Grade II | Grade III | Grade IV | Total | PValue |
| Number of eyes | 5 (6%) | 24 (30%) | 52 (64%) | 81 | |
| Mean age (years) | 50.2 ± 5.2 | 62.9 ± 10.8 | 72.2 ± 9.1 | 68.1 ± 11.3 | 0.023†, 0.001†, 0.004† |
| Sex Male | 4 (80%) | 16 (67%) | 26 (50%) | 46 | |
| Female | 1 (20%) | 8 (33%) | 26 (50%) | 35 | |
| Mean operative time (minutes) | 8.20 ± 1.77 | 9.98 ± 4.37 | 12.35 ± 4.35 | 11.40 ± 4.42 | 0.73⁎, 0.015†, 0.084⁎, |
| Mean phaco time (seconds) | 17.8 ± 21.9 | 19.3 ± 12.8 | 31.9 ± 14.0 | 31.4 ± 15.3 | 0.80⁎, <0.01†, 0.067⁎ |
| Aspiration time (minutes) | 2.37 ± 0.85 | 2.38 ± 1.77 | 2.55 ± 0.75 | 2.50 ± 0.72 | 0.63⁎ |
| CDE | 5.02 ± 6.35 | 8.04 ± 5.97 | 14.69 ± 6.29 | 12.12 ± 7.07 | 0.38⁎, <0.01†, 0.016† |
| Volume of fluid used (mL) | 53.2 ± 17.5 | 58.6 ± 13.1 | 64.3 ± 16.5 | 61.9 ± 15.8 | 0.27⁎ |
Values are expressed as mean ± SD or number of patients unless otherwise noted. P-values, derived from the Steel-Dwass post hoc test are shown in the following order: Grade II and Grade III, Grade III and Grade IV, Grade II and Grade IV, respectively. CDE = cumulative dissipated energy. ⁎No significant difference among the groups (Kruskal-Wallis test). †Significant difference among the groups (Kruskal-Wallis test followed by Steel-Dwass post hoc test).
Table 2.
Pre- and postoperative BCVA, CECD, and IOP measurements of the study eyes.
| Preoperative | 7 Weeks Postoperatively | 19 Weeks Postoperatively | PValue | |
| BCVA (logMAR) n=36 | 2.20 ± 0.35 | 0.02 ± 0.14 | 0.01 ± 0.12 | <0.01†, 1.0⁎, <0.01† |
| CECD (cells/mm2) n=14 | 2577.5 ± 221.0 | 2435.1 ± 249.2 | 2478.8 ± 214.0 | 0.25⁎⁎ |
| CECD loss in % | NA | 5.5 ± 6.0 | 3.7 ± 5.9 | NA |
| IOP (mmHg) n=40 | 13.7 ± 2.6 | 12.7 ± 2.4 | 12.4 ± 2.4 | 0.070⁎⁎⁎ |
Values are expressed as mean ± SD unless otherwise noted. P-values, derived from the Steel-Dwass post hoc test are shown in the following order: preoperatively and 7 weeks postoperatively, 7 weeks and 19 weeks postoperatively, preoperatively and 19 weeks postoperatively, respectively. BCVA = best-corrected visual acuity. MAR = minimum angle of resolution. CECD = corneal endothelial cell density. IOP = intraocular pressure. NA = not applicable. †Significant difference among the groups (Kruskal-Wallis test followed by Steel-Dwass post hoc test). ⁎No significant difference among the groups (Kruskal-Wallis test followed by Steel-Dwass post hoc test). ⁎⁎No significant difference among the groups (Kruskal-Wallis test). ⁎⁎⁎No significant difference among the groups (one-way ANOVA).
Table 3.
Results in studies of phacoemulsification in eyes with mature cataracts.
| Study | Year | Number of Eyes | Surgical Technique | Operation Time (Minutes) |
Phaco Time (Seconds) |
CECD Loss in % | IOP Change |
| Vasavada23 | 1998 | 60 | Stop and chop | NR | NR | 18.6 | NR |
| Brazitikos33 | 1999 | 100 | D&C, Stop and chop | NR | 144 | NR | NR |
| Vajpayee24 | 1999 | 25 | Stop and chop | NR | 229.8 | 15.7 | NR |
| Chakrabarti4 | 2000 | 212 | D&C, Phaco-chop | NR | 121.8 | NR | NR |
| Jacob3 | 2002 | 52 | Karate-chop | NR | 132 | 8.5 | NR |
| Ermisş6 | 2003 | 82 | D&C | NR | 40.4 | NR | -4.2 % |
| Wong7 | 2007 | 25 | Stop and chop | 22 | 96 | 9.6 | NR |
| Venkatesh8 | 2010 | 113 | Phaco-chop | 12.2 | NR | NR | NR |
| Present | 2022 | 81 | Eight-chop | 11.4 | 31.4 | 3.7 | - 9.5 % |
NR = not reported. D&C = divide and conquer. CECD = corneal endothelial cell density. IOP = intraocular pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



