
Submitted:
15 December 2025
Posted:
16 December 2025
You are already at the latest version
Abstract
Tourist swimming pools are complex aquatic systems where operational failures can favour microbial growth and exposure to opportunistic pathogens. We conducted a four‑year surveillance (2016–2019) in hotel pools across Andalusia (Spain), analysing 2,053 water samples under Spanish regulation (Royal Decree 742/2013) with ISO methods (Pseudalert®/ISO 16266‑2 for Pseudomonas aeruginosa and Colilert‑18/ISO 9308‑2 for Escherichia coli). Overall non‑compliance reached 24.8%, and 2.0% of samples triggered immediate pool closure, most frequently due to P. aeruginosa. The bacterium was detected in 5.1% of samples, with heterogeneous distribution among installations: whirlpools (7.9%) > indoor pools (6.4%) > outdoor pools (4.5%) > cold wells (2.9%). No significant association was observed between use by children and P. aeruginosa detection (p > 0.05). Contamination occurred under both chlorine and bromine disinfection, with comparable prevalence (p = 0.18), and overlapping residual distributions indicated that single‑point disinfectant measurements alone did not predict contamination. Seasonality showed a bimodal pattern with winter (January) and summer (August) peaks, and prevalence markedly increased in 2019 compared with prior years. These findings highlight that P. aeruginosa contamination in tourist pools is driven less by momentary disinfectant levels than by structural and operational determinants (e.g., biofilm‑prone niches and hydraulic performance), underscoring the need for continuous surveillance, hydraulic optimization, routine mechanical cleaning, and robust monitoring across all seasons.
Keywords:
Pseudomonas aeruginosa
; recreational water
; swimming pools
; tourist facilities
; water microbiology
; disinfection systems
; public health surveillance
1. Introduction
Recreational water environments are an essential component of modern tourism and public health infrastructure. In regions with high tourist influx, swimming pools and spa facilities represent not only leisure amenities but also complex aquatic systems that require rigorous management to ensure user safety [1,2,3]. Proper maintenance of these systems is critical, as inadequate operation may lead to microbial proliferation, biofilm formation, and increased exposure to opportunistic pathogens [4]. Over the last two decades, several studies across Europe, North America and Australia have highlighted that swimming pool contamination remains a recurring issue, despite advances in disinfection technologies and increasingly stringent regulations [5,6,7,8].
Among the microorganisms of greatest concern in recreational waters, P. aeruginosa occupies a particularly relevant place. This Gram-negative opportunistic pathogen is well known for its ability to colonize aquatic environments, resist disinfection, and persist within biofilms in hydraulic systems and wet surfaces [9]. In addition to its environmental resilience, P. aeruginosa is a major clinical concern due to its intrinsic antimicrobial resistance and prevalence in healthcare-associated infections, which has led to its inclusion in international priority lists for surveillance and research [10,11,12]. Although infections acquired in swimming pools are relatively uncommon, they may include otitis externa, dermatitis, keratitis, hot-foot syndrome, or, in exceptional cases, more severe systemic disease [13,14,15,16]. For this reason, many countries include P. aeruginosa as a microbiological parameter in routine pool monitoring programs.
Tourist swimming pools, particularly those located in warm regions with high seasonal occupancy, may be especially prone to contamination. Factors such as user density, organic load, elevated water temperature, suboptimal hydraulic design, and insufficient mechanical cleaning are widely recognized contributors to increased microbial risk. Previous studies from the Balearic Islands and the Canary Islands demonstrated that these pressures could lead to measurable levels of P. aeruginosa contamination even in facilities operating under established regulatory frameworks [17,18]. These findings align with reports from Italy, Croatia, Northern Ireland, and Greece, suggesting that the issue is widespread across European tourist destinations [7,19,20,21].
Despite there is abundant literature on swimming pools, few studies have focused specifically on tourist facilities in southern Spain, a region with one of the highest concentrations of hotel pools in Europe. Moreover, international research has tended to emphasize free chlorine systems, leaving bromine-treated pools comparatively understudied, despite their relevance in spa settings and high-temperature installations. Additional uncertainty persists regarding the influence of user demographics (e.g., children), environmental seasonality, and the ability of disinfectant levels to predict P. aeruginosa contamination under real-world conditions. Addressing these gaps is essential for improving surveillance frameworks and guiding targeted interventions.
The present study provides a four-year assessment of the microbiological quality of tourist swimming pools in Andalusia, Spain, with a particular focus on P. aeruginosa. Building upon prior surveillance efforts in other Spanish regions, this work offers new insights into contamination patterns across different installation types, seasonal trends, and the comparative performance of chlorine and bromine disinfection. By integrating these findings, the study aims to contribute to a deeper understanding of the operational factors influencing P. aeruginosa persistence and to support evidence-based improvements in the management of recreational waters in high-occupancy tourist environments.
2. Materials and Methods
2.1. Study Design and Sampling Sites
A four-year surveillance study was conducted between 2016 and 2019 to assess the microbiological and physicochemical quality of recreational waters in tourist swimming pool installations located in Andalusia, southern Spain. All sampled facilities were hotel-based pools catering to tourists and subject to routine inspections under the regional surveillance program for compliance with Spanish national legislation [22] on swimming pool water quality.
Each facility was visited several times per year, covering all seasons to identify potential temporal variations in contamination and compliance.
2.2. Sampling Strategy
A total of 2,053 water samples were collected from the main pool basins following the standardized procedures defined in Royal Decree 742/2013. Sampling points were selected to ensure representative coverage of each installation and included outdoor pools, indoor pools, whirlpools (spas, jacuzzis), and cold wells.
Samples were obtained using sterile containers with sodium thiosulfate (for dichlorination) and were transported to the laboratory under refrigerated conditions for analysis within 24 hours.
2.3. Microbiological Analysis
The detection of P. aeruginosa was performed according to ISO 16266-2:2018, by using the Pseudalert® system (IDEXX Laboratories, USA) as an equivalent standardized method validated for recreational waters [23]. Briefly, 100 mL of each sample were mixed with the Pseudalert® reagent and incubated at 38 ± 0.5 °C for 24–28 hours. Fluorescence under UV light was considered positive for P. aeruginosa. As for E. coli analyses, they were performed using Colilert®-18 (IDEXX Laboratories), following manufacturer instructions and ISO 9308-2 standards.
2.4. Physicochemical Parameters
During each sampling event, free chlorine and combined chlorine or bromine (where applicable), pH, and temperature were measured in situ using portable digital meters (Hanna Instruments, Romania) calibrated daily according to the manufacturer’s specifications [24]. Measurements were performed simultaneously with microbiological sampling to enable correlation analyses between disinfectant levels, physicochemical conditions, and the presence of P. aeruginosa.
2.5. Compliance with National Standards
All microbiological and physicochemical results were evaluated in accordance with Royal Decree 742/2013, which sets operational and alert limits for swimming pool water quality in Spain. Samples exceeding those limits were classified as non-compliant.
Pools showing microbiological contamination or serious physicochemical deviations were subject to corrective actions or temporary closure by the corresponding facility manager or health authority.
2.6. Data Analysis
Descriptive statistics were used to calculate compliance rates and prevalence of P. aeruginosa. The D’Agostino–Pearson normality test was applied to assess the normal distribution of quantitative parameters, followed by the Mann–Whitney test for non-normally distributed data. Fisher’s exact test was employed for analysing qualitative parameters. Statistical significance was determined when the p-value was less than 0.05. All statistical analyses were performed using GraphPad Prism software version 9.4.1.
3. Results
3.1. Overall Compliance
Out of the 2,053 water samples analyzed, 24.8% did not comply with the quality criteria established in Royal Decree 742/2013. The most frequent causes of non-compliance were insufficient disinfectant concentration, inadequate water temperature, and the presence of P. aeruginosa. In 2.0% of all cases, the deviation was considered severe enough to warrant immediate pool closure.
P. aeruginosa was identified as the main cause of closure, highlighting its continued relevance as a public health concern in tourist swimming pools (see Table 1).
3.2. Prevalence of P. aeruginosa
P. aeruginosa was detected in 5.1% of all samples analyzed. This prevalence was comparable to those reported in other Spanish regions and Mediterranean countries. The observed rate was lower than previously reported for the Balearic Islands and Greece [17,20,25] but similar to values found in the Canary Islands, Croatia, Finland and Italy [7,18,19,26] (Table 2).
Contamination was not uniformly distributed among pool types. The highest prevalence was observed in whirlpools, where P. aeruginosa was detected in 7.9% of samples, followed by indoor pools (6.4%), outdoor pools (4.5%), and cold wells (2.9%).
3.3. Influence of Pool Use by Children
The potential influence of pool use by children on P. aeruginosa contamination was also evaluated (Table 3). Although some studies have suggested that young swimmers may increase the organic load and microbiological risk in recreational waters, no statistically significant association was found in this survey between the presence of children and the detection of P. aeruginosa (p > 0.05).
This finding indicates that microbial contamination is more closely linked to water management practices than to user demographics, reinforcing the importance of maintaining proper disinfection and maintenance protocols across all pool types.
3.4. Disinfection Systems
The study included both chlorine- and bromine-based disinfection systems, providing a broader comparison than most previous surveys (Table 4). P. aeruginosa was detected in pools treated with either disinfectant, with no significant differences in prevalence (p = 0.18). This is also illustrated in the frequency distribution of free chlorine levels (Figure 1). Most samples—both Pseudomonas-positive and -negative—clustered around 0.5–2 mg/L, which corresponds to the regulatory range. However, a small proportion of samples showed free chlorine levels below 0.5 mg/L, and these substandard values included several P. aeruginosa-positive cases, indicating insufficient disinfectant residual. Moreover, samples above 2 mg/L were relatively frequent and did not show a clear protective effect against contamination. A similar pattern was observed in bromine-treated facilities (Figure 2). Most values fell between 2 and 5 mg/L—within the recommended range—yet P. aeruginosa was detected across this entire interval. Suboptimal bromine concentrations (<2 mg/L) were also present in a minority of samples and were frequently associated with contamination. These findings suggest that both disinfectants can fail when residual concentrations fall below regulatory limits, while values within range, or even higher, do not fully guarantee microbiological safety.
3.5. Temporal Patterns (Seasonal and Annual Trends)
The monthly distribution of P. aeruginosa contamination revealed a heterogeneous pattern strongly influenced by the type of installation rather than a uniform seasonal trend (Figure 3). Although two apparent peaks were observed in January and August when all pool types were aggregated, the underlying data show that these increases were driven by specific installations. In January, contamination occurred exclusively in whirlpools (1/3 samples, 33%) and indoor pools (1/5 samples, 20%), whereas outdoor pools (0/4 samples) and cold wells (0 samples collected) showed no detections. This indicates that the “winter peak” does not represent a general increase across all facilities but is instead limited to indoor environments that remain active during the low season. The absence of contamination in outdoor pools and cold wells in winter reflects not a true zero risk but the reduced or absent sampling of these installations due to seasonal closure. In contrast, the August peak was broader and involved multiple pool types. Whirlpool contamination reached 9/45 samples (20%), while outdoor pools also showed increased positivity (21/193 samples, 10.9%). Cold wells showed 1/10 positives (10%), whereas indoor pools exhibited relatively low contamination (1/19 samples, 5.3%). This pattern aligns with the expected effects of high bather load, elevated temperatures, and increased organic input during the peak tourist season.
These results demonstrate that temporal variation is installation-dependent: whirlpools and indoor pools show intermittent contamination throughout the year, while outdoor pools and cold wells contribute mainly during summer months. Because sampling effort varied considerably across pool types and seasons, percentage-based heatmap patterns should be interpreted with caution, and the inclusion of absolute numbers clarifies that months with “0% contamination” often correspond to very low or absent sampling rather than confirmed absence of P. aeruginosa.
When analyzing yearly prevalence, contamination levels remained relatively stable during the first three years of surveillance (2016–2018), fluctuating around or below 5%. A marked increase was observed in 2019, when the prevalence more than doubled compared with previous years (Table 5). This pattern mirrors similar increases reported in other European regions during the same period and suggests that broader environmental or operational factors may have influenced contamination dynamics in multiple tourist facilities simultaneously [7]. However, analysis of the year-by-year distribution revealed that the marked increase observed in 2019 (11.4%) was not uniformly distributed across months or pool categories. Using the detailed monthly breakdown for 2019, most P. aeruginosa detections occurred between June and September, with August (n = 22) and September (n = 14) accounting for more than two-thirds of all positive samples. This indicates that the 2019 increase was driven by a pronounced summer peak rather than a true winter elevation.
When stratified by installation type, the rise was primarily attributable to whirlpools (15/78; 19.2%) and outdoor pools (34/346; 9.8%), whereas indoor pools and cold wells contributed minimally and exhibited very low sample numbers in winter months. Importantly, some installations (particularly cold wells and outdoor pools) had little or no sampling during the low season, explaining the apparent “winter peak” seen in aggregated heatmaps but not supported by 2019 data.
Overall, the annual increase in 2019 reflects a concentrated surge during the summer months in installation types that inherently present higher risk, rather than a uniform shift across seasons or facilities.
4. Discussion
The present study provides one of the most extensive datasets currently available on the microbiological quality of tourist swimming pools in southern Spain, with special emphasis on P. aeruginosa as a key indicator of water safety and operational performance. Overall, the prevalence observed (5.1%) is consistent with values reported in several European regions, supporting the notion that P. aeruginosa remains a persistent and widespread challenge in recreational waters [7,19,25]. In line with previous findings from the Balearic Islands and the Canary Islands, contamination rates in Andalusian tourist facilities followed a similar order of magnitude, reinforcing the idea that Pseudomonas problems in hotels are not region-specific but structurally linked to operational conditions common to most high-occupancy tourist environments [17,18].
The differences observed among installation types deserve particular attention. As in numerous international studies, whirlpools showed the highest prevalence of contamination [17,21,26,27]. Their combination of elevated water temperature, heavy bather load, high organic input, and the tendency to generate air–water mixing creates optimal conditions for bacterial proliferation and biofilm formation [28]. Conversely, cold-water installations, such as cold wells, exhibited lower contamination levels, which aligns with the well-known inhibitory effect of lower temperatures on P. aeruginosa growth and persistence.
One of the strengths of the present dataset is the inclusion of both chlorine- and bromine-treated installations, an aspect rarely addressed in comparative surveys. It is important to note that our previous regional studies found a higher prevalence of P. aeruginosa in bromine-treated pools [17,18]. In the current Andalusian series, we did not detect statistically significant differences in prevalence between chlorine and bromine systems (p > 0.05). This apparent discrepancy may be explained by differences in sampling composition, operational routines, monitoring frequency, or seasonal coverage between studies. Bromine systems in tourist settings can present greater variability in residuals due to less standardized dosing or monitoring practices; when poorly managed, this variability could translate into higher contamination risk, as previously observed [17,18] . Therefore, rather than attributing risk to the halogen itself, our combined evidence suggests that operational practices and monitoring quality (dose control, frequency of checks, shock treatments, and attention to hydraulic performance) largely determine the comparative effectiveness of chlorine and bromine in real-world conditions.
The analysis of free disinfectant levels provided additional insights into this relationship. The distribution patterns of free chlorine (and bromine) showed substantial overlap between contaminated and non-contaminated samples, indicating that punctual measurements of residual disinfectant alone cannot fully predict the presence of P. aeruginosa. This observation is consistent with previous literature demonstrating that biofilms, hydraulic dead zones, and protected niches within the system can harbor P. aeruginosa independently of momentary disinfectant levels [28,29]. Therefore, Pseudomonas contamination in pools is not merely a chemical control issue but also a structural and operational one, strongly influenced by system design, maintenance quality, and cleaning frequency [30].
Another relevant finding was the absence of association between P. aeruginosa presence and the use of installations by children. While children are often considered a higher-risk group for fecal contamination and accidental release of organic matter, Pseudomonas is primarily an environmental organism with strong affinity for surfaces, biofilms, and water systems. Several international studies have similarly concluded that contamination is driven far more by system conditions than by demography of pool users [17,18] . The present results reinforce this idea and highlight that preventive measures should prioritize hydraulic optimization and routine maintenance rather than user-related restrictions.
The temporal distribution of contamination also deserves comment. The temporal patterns observed in this study reveal that P. aeruginosa contamination in tourist pools does not follow a uniform seasonal trend but is strongly shaped by the type of installation and by sampling intensity. Although the aggregated heatmap suggested peaks in January and August, the underlying data show that the winter increase was restricted almost exclusively to whirlpools and indoor pools—facilities that remain active during the low season [31]. Outdoor pools and cold wells showed no detections in winter, but this reflected the absence or very low number of samples rather than a true reduction of risk. This underscores the importance of interpreting seasonal percentages considering the absolute number of samples collected per installation type. In contrast, the August peak represents a genuine seasonal increase, supported by large sample numbers across multiple pool types. Higher contamination in whirlpools and outdoor pools aligns with expected risk factors during peak tourist months, such as elevated temperatures, increased bather load, and higher organic input. Similar summer-associated increases have been documented in other regions [7,30,32,33].
The annual analysis further refines this interpretation. Prevalence remained stable from 2016 to 2018 but rose sharply in 2019. When examined in detail, this increase was concentrated almost entirely in the summer months—particularly August and September—and driven mainly by whirlpools and outdoor pools. Thus, the 2019 rise reflects an intensified summer peak rather than a year-round shift. Notably, a comparable increase in P. aeruginosa contamination was reported in the Balearic Islands and Croatia during the same year [7,17], suggesting that broader regional or operational pressures may have simultaneously affected tourist facilities in different Mediterranean areas.
Overall, these findings emphasize that temporal variability in P. aeruginosa contamination arises from the interplay of installation-specific vulnerabilities, operational dynamics, and seasonal patterns, rather than from climate or season alone. Surveillance and prevention strategies should therefore prioritize consistent year-round sampling and installation-specific risk assessment, particularly in high-risk environments such as whirlpools.
The finding that P. aeruginosa was the leading cause of immediate pool closures is particularly relevant for public health authorities and the tourism industry. Although clinical infections associated with swimming pools are relatively rare, P. aeruginosa has been implicated in folliculitis, otitis externa, keratitis, hot-foot syndrome, and, in exceptional cases, severe pneumonia among exposed individuals [13,14,15,16]. Given its well-known intrinsic and acquired antimicrobial resistance, some authors now consider this bacterium a pathogen of increasing relevance in both community and healthcare environments [34]. In the context of tourism, the occurrence of repeated closures may also have implications for consumer confidence and facility reputation, representing both health and an economic concern.
As with all surveillance-based studies, certain limitations should be acknowledged. First, the study relied on point-in-time sampling, which may underestimate transient contamination events. Second, only samples from the pool basin (not the recirculation circuit) were collected, preventing identification of possible system reservoirs. Third, information on occupancy dynamics, cleaning frequency, and hydraulic performance was not systematically available, which limits the ability to quantify their individual impact. Despite these constraints, the dataset is robust, spans multiple years, and shows remarkable consistency with previous regional studies in Spain and international literature.
Overall, this study contributes valuable evidence to the growing body of data on P. aeruginosa in tourist swimming pools. The findings consistently highlight that contamination patterns are shaped not only by disinfectant levels and temperature but—perhaps more importantly—by operational and structural factors that promote biofilm formation and hinder disinfectant efficacy. The similarities between the present results and those from other Spanish regions reinforce the generalizability of these conclusions and suggest that targeted interventions focused on hydraulic optimization, routine mechanical cleaning, and high-quality maintenance procedures may provide the greatest impact. Taken together, these insights underscore the need for continuous surveillance and improved management practices in tourist pools to safeguard public health and maintain high standards of safety and quality in recreational water environments.
In conclusion, the present study reinforces that P. aeruginosa remains a persistent microbiological challenge in tourist swimming pools, driven not only by disinfectant performance but by deeper structural and operational determinants. The consistency of our findings with previous data from other Spanish regions and international studies highlights the universal nature of these risks in high-occupancy recreational environments. By identifying whirlpools as the most vulnerable installations, demonstrating the limited discriminative power of residual disinfectant levels, and revealing seasonal patterns that extend beyond the summer season, this work underscores the need for comprehensive management strategies focused on hydraulic optimization, routine mechanical cleaning, and continuous surveillance. Strengthening these aspects will be essential to ensuring safer recreational waters and supporting the long-term quality and competitiveness of the tourism sector.
Author Contributions
Conceptualization, A.D-S. and S.A.; methodology, A.D-S, A.G-A and, M.M-B.; validation, S.A., A.G-A and, M.M-B.; formal analysis, A.D-S.; investigation, A.D-S, A.G-A and, M.M-B.; data curation, A.D-S.; writing—original draft preparation, A.D-S..; writing—review and editing, , S.A., A.G-A and, M.M-B.; supervision, A.D-S. and S.A.; project administration, A.D-S.; funding acquisition, A.D-S. and S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors would like to thank all the staff at the facilities visited who provided support during the sampling. During the preparation of this work the authors used ChatGPT to improve the readability and language of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- C. Coxon, K. Dimmock, and J. Wilks, “Managing Risk in Tourist Diving: A Safety-Management Approach,” New Frontiers In Marine Tourism: Diving Experiences, Sustainability, Management, pp. 201–220, Jan. 2007. [CrossRef]
- J. Wilks, “Tourism and aquatic safety: No lifeguard on duty-swim at your own risk,” Tourism in Marine Environ-ments, vol. 12, no. 3–4, pp. 211–219, 2017. [CrossRef]
- A. Papadakis, D. Chochlakis, E. Koufakis, V. Carayanni, and A. Psaroulaki, “Recreational Water Safety in Hotels: Lessons from the COVID-19 Pandemic and the Way Forward for a Safe Aquatic Environment,” Tourism and Hos-pitality 2024, Vol. 5, Pages 1167-1181, vol. 5, no. 4, pp. 1167–1181, Nov. 2024. [CrossRef]
- World Health Organization, Water recreation and disease. World Health Organization, 2005. Accessed: Jul. 11, 2017. [Online]. Available: http://www.who.int/water_sanitation_health/publications/water-recreation-and-disease/en/.
- A. Esterman et al., “Determinants of the microbiological characteristics of South Australian swimming pools.,” Appl Environ Microbiol, vol. 47, no. 2, p. 325, 1984. [CrossRef]
- M. C. Hlavsa et al., “Outbreaks Associated with Treated Recreational Water — United States, 2000–2014,” MMWR Morb Mortal Wkly Rep, vol. 67, no. 19, pp. 547–551, May 2018. [CrossRef]
- D. V. Lušić et al., “Occurrence of P. aeruginosa in Water Intended for Human Consumption and in Swimming Pool Water,” Environments 2021, Vol. 8, Page 132, vol. 8, no. 12, p. 132, Nov. 2021. [CrossRef]
- L. Dallolio et al., “Hygienic surveillance in swimming pools: Assessment of the water quality in Bologna facilities in the period 2010–2012,” Microchemical Journal, vol. 110, pp. 624–628, Sep. 2013. [CrossRef]
- S. Crone et al., “The environmental occurrence of Pseudomonas aeruginosa,” APMIS, vol. 128, no. 3, pp. 220–231, Mar. 2020. [CrossRef]
- M. Ahmad and A. U. Khan, “Global economic impact of antibiotic resistance: A review,” J Glob Antimicrob Resist, vol. 19, pp. 313–316, Dec. 2019. [CrossRef]
- “Antimicrobial resistance in the EU/EEA (EARS-Net) - Annual Epidemiological Report for 2020.” Accessed: Oct. 26, 2022. [Online]. Available: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-eueea-ears-net-annual-epidemiological-report-2020.
- S. L. Gellatly and R. E. W. Hancock, “Pseudomonas aeruginosa : new insights into pathogenesis and host defenses,” Pathog Dis, vol. 67, no. 3, pp. 159–173, Apr. 2013. [CrossRef]
- M. Hajjartabar, “Poor-quality water in swimming pools associated with a substantial risk of otitis externa due to Pseudomonas aeruginosa,” Water Science and Technology, vol. 50, no. 1, pp. 63–67, Jul. 2004. [CrossRef]
- Y. Yu, A. S. Cheng, L. Wang, W. M. Dunne, and S. J. Bayliss, “Hot tub folliculitis or hot hand-foot syndrome caused by Pseudomonas aeruginosa,” J Am Acad Dermatol, vol. 57, no. 4, pp. 596–600, Oct. 2007. [CrossRef]
- G. Pantazidou, M. E. Dimitrakopoulou, C. Kotsalou, J. Velissari, and A. Vantarakis, “Risk Analysis of Otitis Ex-terna (Swimmer’s Ear) in Children Pool Swimmers: A Case Study from Greece,” Water 2022, Vol. 14, Page 1983, vol. 14, no. 13, p. 1983, Jun. 2022. [CrossRef]
- G. F. Craun, R. L. Calderon, and M. F. Craun, “Outbreaks associated with recreational water in the United States,” Int J Environ Health Res, vol. 15, no. 4, pp. 243–262, Aug. 2005. [CrossRef]
- A. Doménech-Sánchez, E. Laso, and S. Albertí, “Environmental surveillance of Pseudomonas aeruginosa in recreational waters in tourist facilities of the Balearic Islands, Spain (2016–2019),” Travel Med Infect Dis, vol. 54, Jul. 2023. [CrossRef]
- A. Doménech-Sánchez, E. Laso, and S. Albertí, “Prevalence and Control of Pseudomonas aeruginosa in Tourist Facilities across the Canary Islands, Spain.,” Pathogens, vol. 13, no. 6, Jun. 2024. [CrossRef]
- M. Guida, F. Gallè, M. L. Mattei, D. Anastasi, and G. Liguori, “Microbiological quality of the water of recreational and rehabilitation pools: a 2-year survey in Naples, Italy,” Public Health, vol. 123, no. 6, pp. 448–451, Jun. 2009. [CrossRef]
- C. Papadopoulou et al., “Microbiological quality of indoor and outdoor swimming pools in Greece: Investigation of the antibiotic resistance of the bacterial isolates,” Int J Hyg Environ Health, vol. 211, no. 3–4, pp. 385–397, Jul. 2008. [CrossRef]
- J. E. Moore, N. Heaney, B. C. Millar, M. Crowe, and J. S. Elborn, “Incidence of Pseudomonas aeruginosa in recreational and hydrotherapy pools.,” Commun Dis Public Health, vol. 5, no. 1, pp. 23–6, Mar. 2002, Accessed: Oct. 14, 2021. [Online]. Available: http://www.ncbi.nlm.nih.gov/pubmed/12070972.
- Ministerio de Sanidad Servicios Sociales e Igualdad., “Real Decreto 742/2013, de 27 de septiembre, por el que se establecen los criterios técnico- sanitarios de las piscinas,” Boletín Oficial del Estado, vol. 244, no. I, pp. 83123–83135, 2013.
- S. DP, B. M, B. A, and S. D, “Evaluation of the Pseudalert/Quanti-Tray MPN Test for the Rapid Enumeration of Pseudomonas aeruginosa in Swimming Pool and Spa Pool Waters,” Curr Microbiol, vol. 71, no. 6, pp. 699–705, Dec. 2015. [CrossRef]
- M. Rosende et al., “Cost-Effectiveness Analysis of Chlorine-Based and Alternative Disinfection Systems for Pool Waters,” Journal of Environmental Engineering, vol. 146, no. 1, p. 04019094, Jan. 2020. [CrossRef]
- Tirodimos, M. Arvanitidou, T. Dardavessis, A. Bisiklis, and S. Alexiou-Daniil, “Prevalence and antibiotic resistance of Pseudomonas aeruginosa isolated from swimming pools in Northern Greece,” Eastern Mediterranean Health Journal, vol. 16, no. 7, pp. 783–787, 2010. [CrossRef]
- M. Vesaluoma, S. Kalso, L. Jokipii, D. Warhurst, A. Ponka, and T. Tervo, “Microbiological quality in Finnish public swimming pools and whirlpools with special reference to free living amoebae: a risk factor for contact lens wearers?,” British Journal of Ophthalmology, vol. 79, no. 2, pp. 178–181, Feb. 1995. [CrossRef]
- I. Tirodimos, E. P. Christoforidou, S. Nikolaidou, and M. Arvanitidou, “Bacteriological quality of swimming pool and spa water in northern Greece during 2011–2016: is it time for Pseudomonas aeruginosa to be included in Greek regulation?,” Water Supply, vol. 18, no. 6, pp. 1937–1945, Dec. 2018. [CrossRef]
- M. Guida et al., “Pseudomonas aeruginosa in Swimming Pool Water: Evidences and Perspectives for a New Control Strategy,” Int J Environ Res Public Health, vol. 13, no. 9, Sep. 2016. [CrossRef]
- M. Sigler Zekanović, G. Begić, A. Medić, I. Gobin, and D. Tomić Linšak, “Effects of a Combined Disinfection Method on Pseudomonas aeruginosa Biofilm in Freshwater Swimming Pool,” Environments 2022, Vol. 9, Page 103, vol. 9, no. 8, p. 103, Aug. 2022. [CrossRef]
- L. Lamere, E. Smith, H. Grieser, M. Arduino, M. C. Hlavsa, and S. Combes, “Pseudomonas Infection Outbreak Associated with a Hotel Swimming Pool — Maine, March 2023,” MMWR Morb Mortal Wkly Rep, vol. 73, no. 2, pp. 32–36, Jan. 2024. [CrossRef]
- N. Brousseau et al., “Contamination of public whirlpool spas: Factors associated with the presence of Legionella spp., Pseudomonas aeruginosa and Escherichia coli,” Int J Environ Health Res, vol. 23, no. 1, pp. 1–15, Feb. 2013. [CrossRef]
- S. Nikolaidou et al., “Microbiological water quality assessment of swimming pools and jacuzzis in Northern Greece: a retrospective study,” Int J Environ Health Res, 2024. [CrossRef]
- B. J, H. G, and S. J, “Pseudomonas aeruginosa in public swimming pools and bathroom water of patients with cystic fibrosis,” J Cyst Fibros, vol. 4, no. 4, pp. 227–231, Dec. 2005. [CrossRef]
- E. Tacconelli et al., “Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis,” Lancet Infect Dis, vol. 18, no. 3, pp. 318–327, Mar. 2018. [CrossRef]
Figure 1.
Frequency distribution of free chlorine levels in P. aeruginosa contaminated and not contaminated pool samples. Left, histogram showing the concentration of free chlorine in ranges of 0.5 mg L-1. Right, violin plot representing individual levels of free chlorine in pools contaminated or not with P. aeruginosa. (ns, p>0.05).
Figure 1.
Frequency distribution of free chlorine levels in P. aeruginosa contaminated and not contaminated pool samples. Left, histogram showing the concentration of free chlorine in ranges of 0.5 mg L-1. Right, violin plot representing individual levels of free chlorine in pools contaminated or not with P. aeruginosa. (ns, p>0.05).
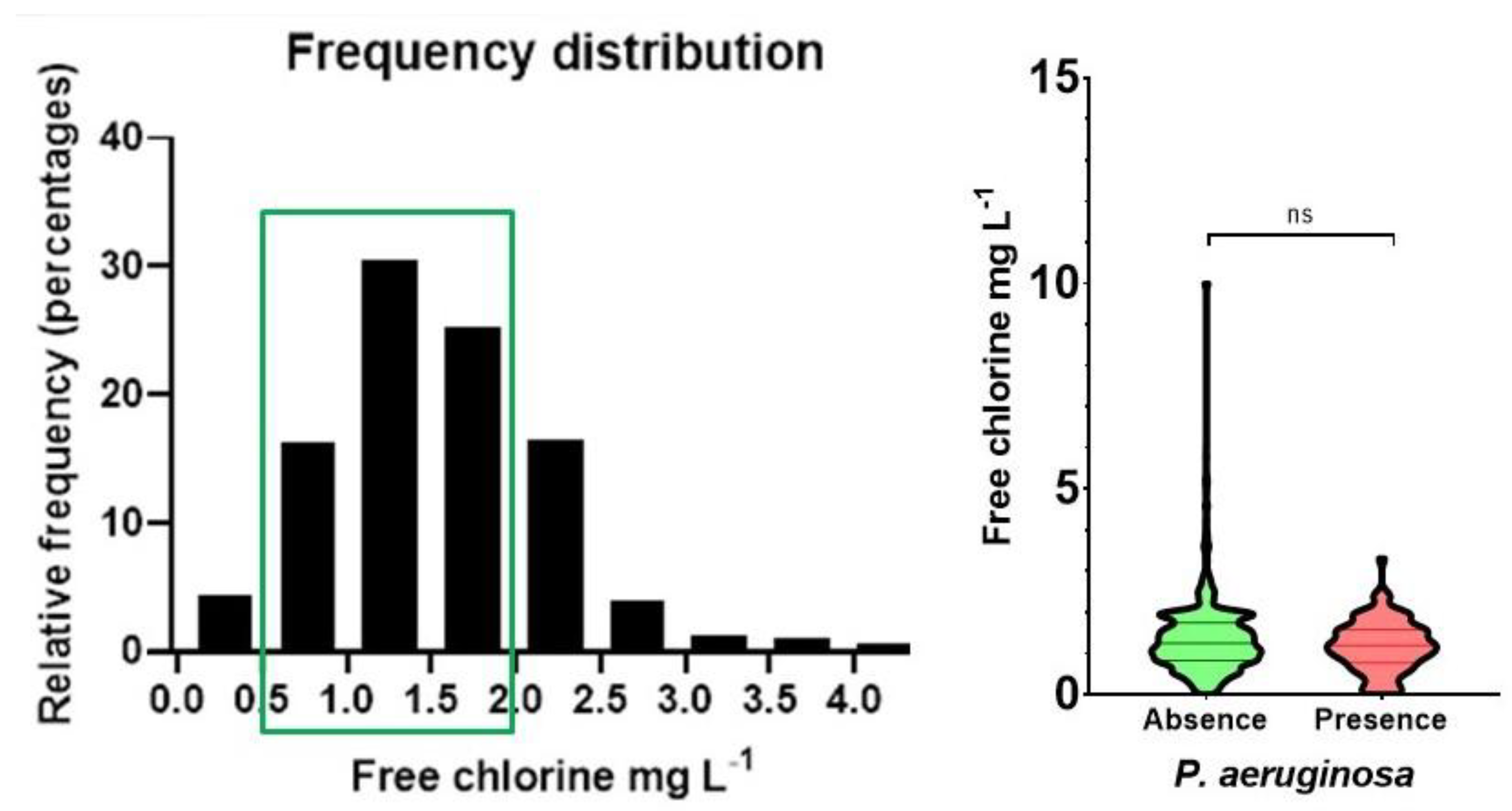
Figure 2.
Frequency distribution of bromine levels in P. aeruginosa contaminated and not contaminated pool samples. Left, histogram showing the concentration bromine in ranges of 1 mg L-1. Right, violin plot representing individual levels of bromine in pools contaminated or not with P. aeruginosa. (ns, p>0.05).
Figure 2.
Frequency distribution of bromine levels in P. aeruginosa contaminated and not contaminated pool samples. Left, histogram showing the concentration bromine in ranges of 1 mg L-1. Right, violin plot representing individual levels of bromine in pools contaminated or not with P. aeruginosa. (ns, p>0.05).
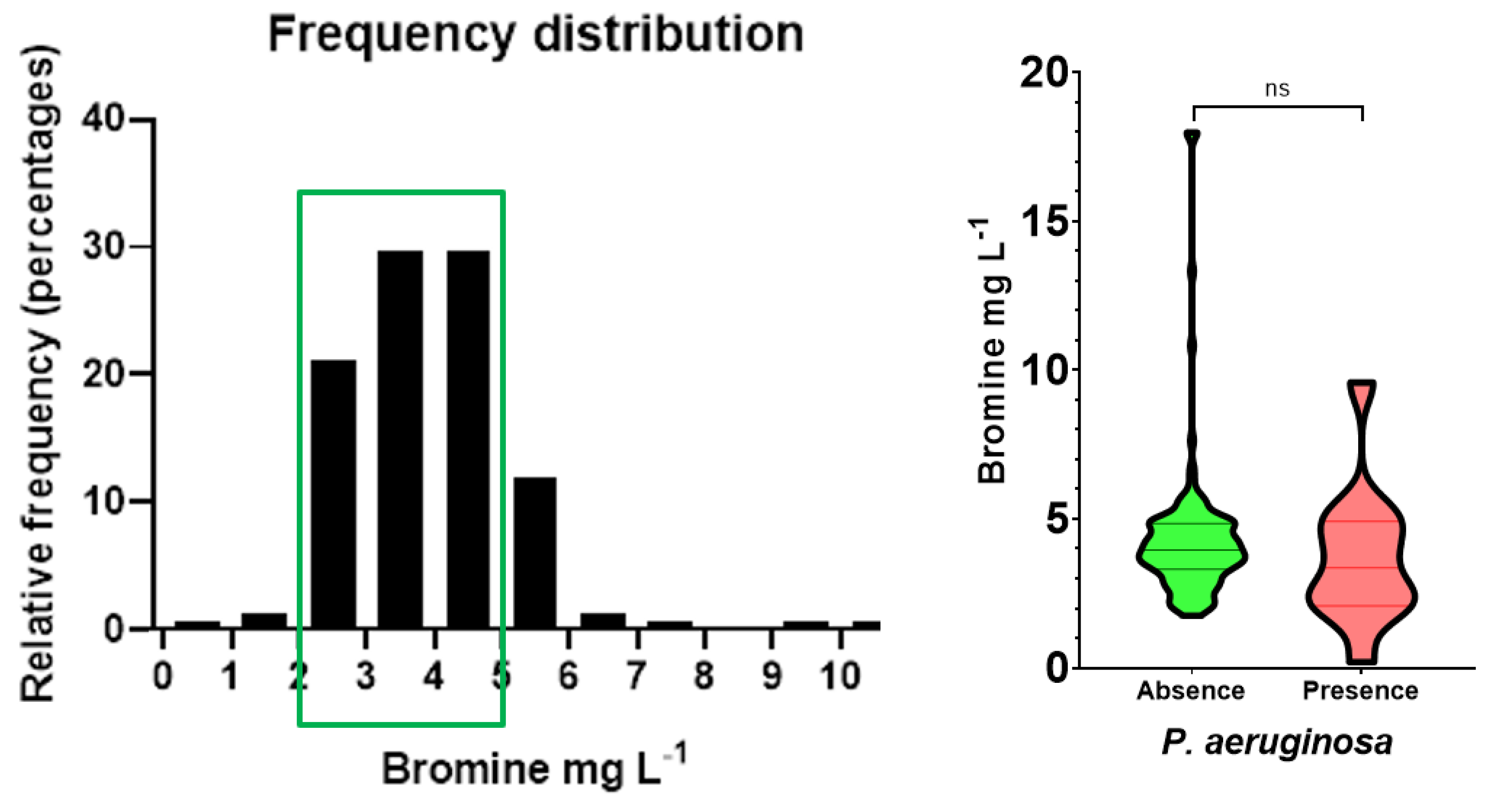
Figure 3.
Heatmap showing the seasonal frequency of P. aeruginosa contamination during the four years.
Figure 3.
Heatmap showing the seasonal frequency of P. aeruginosa contamination during the four years.
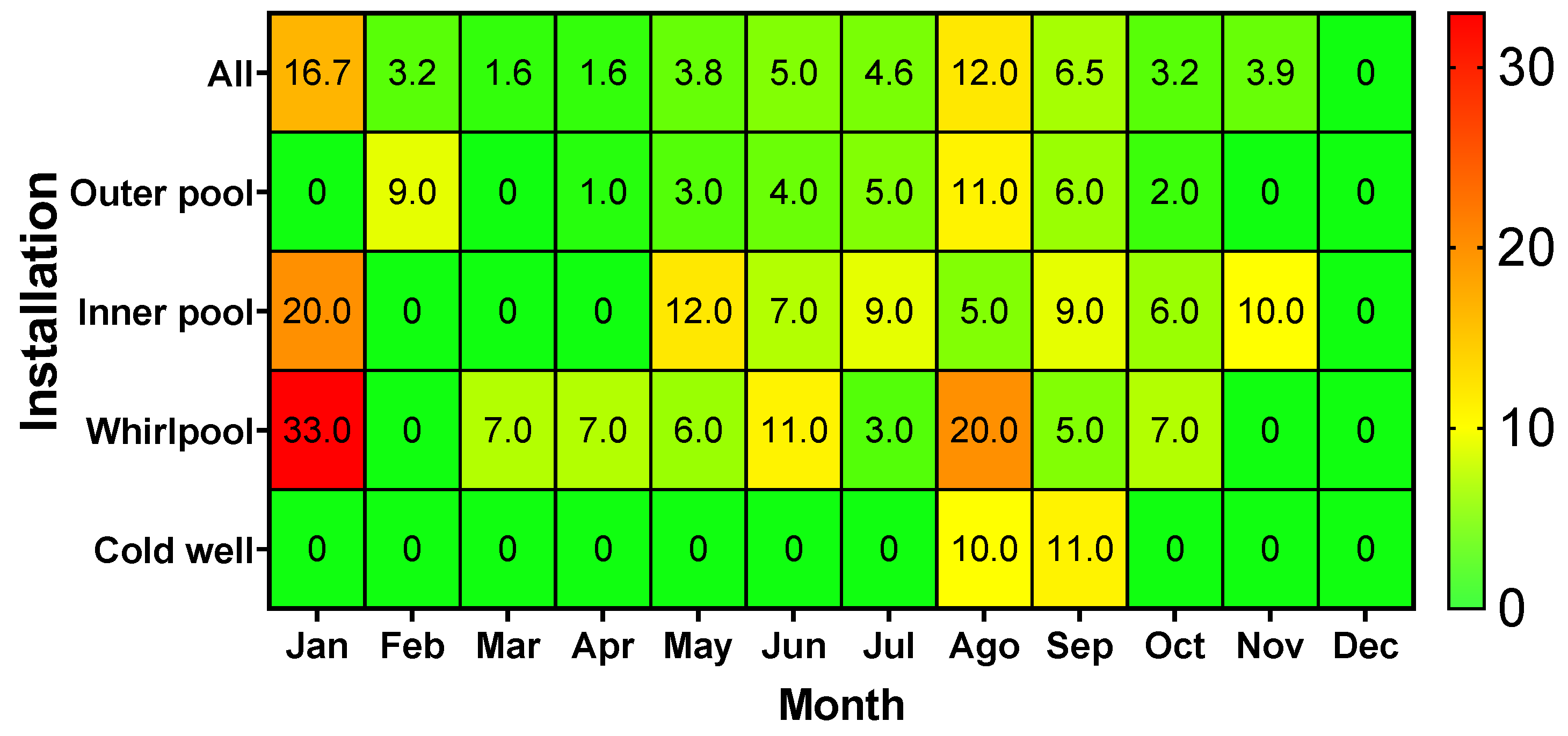

Table 1.
Compliance with water standards of legislated parameters in the pools investigated.
| Parameter | Parametric value | Total samples | Acceptable | Unacceptable | Closure1 | |||
| n | % | n | % | n | % | |||
| Temperature | 24-30°C2 | 5733 | 472 | 82.4 | 101 | 17.6 | 0 | 0.0 |
| pH | 7.2-8 | 2,053 | 1,946 | 94.8 | 107 | 5.2 | 6 | 0.3 |
| Turbidity | ≤5 | 2,053 | 2,047 | 99.7 | 6 | 0.3 | 0 | 0.0 |
| Free chlorine | 0.5-2 mg L-1 | 1,837 | 1,492 | 81.2 | 345 | 18.8 | 30 | 1.6 |
| Combined chlorine | ≤0.6 mg L-1 | 1,837 | 1,796 | 97.8 | 41 | 2.2 | 0 | 0.0 |
| Cyanuric acid | ≤75 mg L-1 | 1,837 | 1,827 | 99.5 | 10 | 0.5 | 2 | 0.1 |
| Bromine | 2-5 mg L-1 | 159 | 131 | 82.4 | 23 | 14.5 | 5 | 3.1 |
| P. aeruginosa | 0 CFU 100 mL-1 | 2,053 | 1,948 | 94.9 | 105 | 5.1 | 105 | 5.1 |
| E. coli | 0 CFU 100 mL-1 | 2,053 | 2,038 | 99.3 | 15 | 0.7 | 15 | 0.7 |
| Total | 2,053 | 1,543 | 75.2 | 510 | 24.8 | 41 | 2.0 | |
1 Unacceptable samples with values exceeding the limits established for the pool’s closure due to its dangerousness. 2 ≤36°C for whirlpools. 3 For whirlpools and inner pools.
Table 2.
Contamination by P. aeruginosa in the different types of investigated pools.
| Type of installation | Absence | Presence | Total | |||
| n | % | n | % | n | % | |
| Outer pools | 1,414 | 95.5 | 66 | 4.5 | 1,480 | 100 |
| Inner pools | 162 | 93.6 | 11 | 6.4 | 173 | 100 |
| Whirlpools | 304 | 92.1 | 26 | 7.9 | 330 | 100 |
| Cold wells | 68 | 97.1 | 2 | 2.9 | 70 | 100 |
| Total | 1,948 | 94.9 | 105 | 5.1 | 2,053 | 100 |
Table 3.
Contamination by P. aeruginosa in water samples from adults and children pools.
| Type of installation | Absence | Presence | Total | |||
| n | % | n | % | n | % | |
| Children pools | 267 | 94.7 | 15 | 5.3 | 282 | 100 |
| Adults’ pools | 1,681 | 94.9 | 90 | 5.1 | 1,771 | 100 |
| Total | 1,948 | 94.9 | 105 | 5.1 | 2,053 | 100 |
Table 4.
Contamination by P. aeruginosa in water samples with different disinfectant treatments.
| Type of installation | Absence | Presence | Total | |||
| n | % | n | % | n | % | |
| Bromine treated pools | 147 | 92.5 | 12 | 7.5 | 159 | 100 |
| Chlorine treated pools | 1,801 | 95.1 | 93 | 4.9 | 1,894 | 100 |
| Total | 1,948 | 94.9 | 105 | 5.1 | 2,053 | 100 |
Table 5.
Evolution of the contamination by P. aeruginosa over the years.
| Year | Absence | Presence | Total | |||
| n | % | n | % | n | % | |
| 2016 | 494 | 94.6 | 28 | 5.4 | 522 | 100 |
| 2017 | 508 | 96.9 | 16 | 3.1 | 524 | 100 |
| 2018 | 535 | 98.5 | 8 | 1.5 | 543 | 100 |
| 2019 | 411 | 88.6 | 53 | 11.4 | 464 | 100 |
| Total | 1,948 | 94.9 | 105 | 5.1 | 2,053 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



