
Submitted:
12 December 2025
Posted:
15 December 2025
You are already at the latest version
Abstract
Bone is a hierarchically organized composite material with unique mechanical properties and an intrinsic capacity for regeneration. Conventional repair strategies, including autografts, allografts, xenografts, and metallic or ceramic implants, face limitations such as donor scarcity, immunogenicity, brittleness, and poor long-term integration. Tissue engineering (TE) offers a promising alternative by combining cells, scaffolds, and growth factors to restore bone structure and function. This review outlines the principles and workflow of bone TE, emphasizing scaffold design, and clinical viability. Scaffolds serve as three-dimensional, highly porous templates that support cell adhesion, nutrient diffusion, and extracellular matrix remodeling. Successful bone TE requires osteoconductive scaffolds, osteogenic progenitor cells, and osteoinductive signaling molecules to achieve physiological compatibility and functional integration. Recent advances in biomaterials, scaffold architecture, and fabrication technologies have significantly improved the ability to replicate native bone properties, positioning TE as a transformative strategy for regenerative medicine. Despite persistent challenges in achieving complete integration and mechanical stability under complex loading, ongoing research continues to optimize scaffold performance and cellular approaches, making TE a viable and cost-effective alternative to traditional bone repair techniques.
Keywords:
bone tissue engineering
; scaffold design
; osteoconduction
; regenerative medicine
; bone graft substitutes
Introduction
Bone is a highly organized composite material with unique mechanical properties, which can be replicated using synthetic composites [1]. As a fundamental component of the human skeletal system, bone provides structural support and plays a critical role in maintaining body integrity. To address bone defects, numerous replacement materials and techniques have been developed. One of the most remarkable features of bone is its intrinsic ability to regenerate and remodel without limitation. Nevertheless, medical intervention is often required for significant defects. Traditional approaches for bone repair include external fixation methods such as bone grafting, the Ilizarov technique, and bone transport. However, some of these methods, particularly the Ilizarov technique, involve prolonged recovery periods and carry substantial risks. Bone grafts are generally classified into three categories: autografts, allografts, and xenografts [2]. Autologous bone grafts provide essential osteoinductive factors and osteogenic cells, offering superior outcomes in bone healing and regeneration. Despite these advantages, autografts are limited by inadequate tissue availability for large defects [3]. Metals and ceramics have been explored as potential alternatives for bone grafting. Metals provide immediate mechanical support but exhibit poor integration with host tissue and are susceptible to fatigue failure. Ceramics, while biocompatible, suffer from brittleness and low tensile strength, making them unsuitable for regions subjected to torsional, bending, or shear stresses [4]. These limitations underscore the need for substitute materials that closely mimic the structural and functional properties of natural bone.
Tissue engineering (TE) represents a multidisciplinary approach that integrates principles of biology and engineering to restore, maintain, or improve tissue function. This emerging field addresses critical clinical challenges such as organ failure and tissue loss. Historically, organ transplantation, primarily allografts, was the predominant solution for damaged tissues. However, this approach is constrained by donor scarcity and immunological rejection risks. Autografts and xenografts have also been employed, though each presents unique limitations. Prosthetic devices offer another alternative but are associated with infection risks and poor long-term integration [5]. TE offers a promising solution by fabricating scaffolds from biocompatible materials to provide a structural matrix that supports cell growth and tissue formation. These scaffolds must mimic the natural extracellular environment, be non-toxic, and degrade safely over time [6].
The TE process involves three essential components: cells, scaffolds, and growth factors. Its applications include (i) providing cellular prostheses or replaceable parts to induce regeneration, (ii) creating tissue-like models for research, and (iii) developing delivery systems for therapeutic agents [6]. TE systems are classified into open and closed configurations. Open systems involve implanting cell-seeded scaffolds into the body, whereas closed systems employ external devices for organ support. The standard TE workflow includes cell isolation via biopsy, in vitro expansion by seeding onto a scaffold, and implantation into the defect site. Scaffolds are typically three-dimensional, highly porous structures that serve as templates for cell regeneration. They are combined with growth factors and signaling molecules and maintained in bioreactors until a functional graft is formed. Advanced bioreactor systems are essential for controlling process parameters and creating optimal culture conditions [7].
Bone TE offers a cost-effective, reliable, and physiologically compatible strategy for bone regeneration. TE has emerged as an alternative to conventional grafting procedures, which are often limited by donor tissue availability and procedural constraints [8]. Successful bone regeneration requires three key elements: osteoconductive scaffolds, osteogenic progenitor cells, and osteoinductive growth factors (Figure 1) [9]. Scaffolds act as temporary substrates that support cellular activity and maintain cell differentiation. The performance of scaffolds is critical to the success of bone TE. Biomaterials used in this context must exhibit properties such as osteoconductivity, biocompatibility, integration with surrounding tissue, and adequate mechanical strength. Integration is particularly important for enabling extracellular matrix (ECM) remodeling and facilitating physiological and biological changes within bone tissue [10].
This review highlights bone tissue engineering as a transformative strategy to address the inherent limitations of conventional grafting and fixation techniques. By integrating osteoconductive scaffolds, osteogenic cells, and osteoinductive growth factors, bone TE establishes a biologically inspired framework for effective regeneration. Recent advances in biomaterials, scaffold architecture, and fabrication technologies have markedly improved the ability to replicate native bone structure and function, yielding solutions that are both physiologically compatible and clinically viable. Despite persistent challenges in achieving complete integration and long-term stability, ongoing research continues to optimize scaffold performance and cellular approaches, positioning TE at the forefront of regenerative medicine and as a compelling alternative to traditional bone repair modalities.
2.1. Natural Bone Structure and Composition
Bone is a hierarchical composite material integrating organic and inorganic phases to achieve exceptional mechanical performance and adaptability. The organic matrix—primarily type I collagen—provides tensile strength and toughness, while embedded carbonated-substituted hydroxyapatite (HA) crystals confer compressive stiffness and rigidity [11,12]. At the nanoscale, bone comprises mineralized collagen fibrils where rod- or plate-like crystallites (∼5 × 5 × 50 nm) are entrenched within the collagen matrix [13,14]. The organized mineralization forms concentric lamellae in osteons, centered around Haversian canals and connected by Volkmann’s canals, facilitating vascular and nutrient transport [15]. Quantitative composition analysis indicates bone tissue consists of approximately 30% organic matrix, 60% mineral, and 10% water by weight [16]. At the macroscopic level, bone architecture diverges into two structural types: (i) Cortical bone: Dense and load-bearing, characterized by ~10% porosity, an elastic modulus of 15–20 GPa, and compressive strength of 100–200 MPa [17]. (ii) Cancellous bone: Spongy and metabolically active, with 50–90% porosity, modulus spanning 0.1–2 GPa, and compressive strength of 2–20 MPa [17,18].

Table 1.
Bone Composition.
| Component | Site or Specific Molecule | Volume (%) |
|---|---|---|
| Water | Free/pore; bound at collagen-mineral interfaces; structural | 15–25 vol % |
| Organic matrix | Type I collagen (~90 wt %), non-collagenous proteins (~10 wt %) | ~32–40 vol % |
| Mineral (apatite) | Hydroxyapatite with carbonate substitutions | 35–45 vol % |
Bone’s hierarchical structure from nano- to macro-scale forms a mechanically efficient framework: mineral lamellae and collagen fibrils at the nanoscale; osteons and interstitial lamellae at the microscale; and coordinated cortical and trabecular networks at the macroscale [11,15].
2.1.1. Bone Cells and Their Functions
Bone remodeling and repair depend on the coordinated activity of four distinct cell types:
(i) Osteoprogenitor cells are multipotent mesenchymal precursors residing in periosteal and endosteal niches; they differentiate into osteoblasts, chondrocytes, adipocytes, fibroblasts, or myoblasts during growth and regeneration [19].
(ii) Osteoblasts secrete the organic bone matrix and regulate mineralization; once encapsulated, they become osteocytes. They also modulate osteoclast activity via paracrine signaling [19].
(iii) Osteocytes, the mechanosensory cells embedded within the matrix, maintain mineral homeostasis and orchestrate bone adaptation in response to mechanical cues [20].(iv) Osteoclasts are large, multinucleated cells that enzymatically resorb bone during remodeling and healing, critical for maintaining structural integrity [19]. Figure 2 shows the schematic representation of different types of bone cells.
2.1.2. Bone Healing Process
Bone repair occurs through three overlapping phases [21,22]. In the inflammatory phase, hematoma formation and immune cell infiltration trigger angiogenesis and recruit mesenchymal precursors [21]. During the repair phase, a soft callus of fibrous tissue and cartilage develops, which gradually transitions into woven bone as osteoblasts deposit mineralized matrix [22]. Finally, in the remodeling phase, the immature woven callus is replaced by organized lamellar bone; osteoclasts resorb the initial bone while osteoblasts restore structural integrity [22].
2.1.3. Mechanical Properties of Natural Bone
The mechanical behavior of bone is primarily assessed in vivo, while its mechanical properties are typically determined through in vitro testing. These tests follow standardized protocols originally designed for conventional materials such as metals and plastics. On a smaller scale, composite models can be used to evaluate mechanical performance [11,13]. Brittle apatite contributes stiffness to bone, whereas collagen provides a tough, flexible matrix. The interaction between these two components significantly influences the tensile properties of bone. Understanding bone structure is essential for replicating its characteristics in implant materials. Cancellous bone consists of an interconnected network of plates and rods, with density ranging from 0.05 to 0.7 g/cm³ [18]. Compression tests reveal that cancellous bone exhibits characteristics typical of cellular solids.
The outer region of bone, known as cortical bone, forms a dense cylindrical shell along the bone’s length. It has approximately 10% porosity, a modulus of 50–150 MPa, and a compressive strength of 12–18 MPa [17]. In contrast, cancellous bone, located at the distal ends, has a spongy structure with about 75% porosity, a modulus ranging from 10–500 MPa, and compressive strength between 10–20 MPa [17,18].
Overall, cortical bone is denser and harder than cancellous bone, which is comparatively softer and less dense. Both types contain a collagen matrix embedded with mineral crystals, providing structural support and mechanical strength. An increase in bone density corresponds to thicker cell walls, which enhances compressive modulus and raises the plateau stress while reducing strain at the onset of densification. Bone also responds dynamically to mechanical loading; physical stress influences bone formation and resorption. Designing scaffolds with mechanical properties similar to natural bone is critical for supporting injured areas. Material selection affects key characteristics such as porosity, formation, and overall mechanical performance. Bone exhibits anisotropy and plasticity under loading, influenced by its mineral–matrix ratio. Studies show an optimal composition window that maximizes stiffness, strength, and toughness, guiding bone-mimicking material design [16].
2.2. Properties of Bone TE Scaffold
Recent advances in scaffold technology aim to address limitations associated with organ transplantation and bone failure treatments. Scaffolds are designed to influence the chemical, physical, and biological environment surrounding cell populations. An optimized scaffold must integrate both biological and mechanical characteristics of bone tissue. The biological environment of bone involves fluid and nutrient transport as well as the presence of various cell types. A scaffold tailored to these conditions can effectively stimulate cell migration and extracellular matrix deposition [23,24]. Conversely, the mechanical environment encompasses loading requirements and spatial organization of bone cells to promote cell–cell signaling. Scaffolds engineered for these conditions can successfully transfer mechanical loads [25,26].
The primary goal of scaffold design is to fabricate an ideal matrix structure. Scaffold architecture plays a critical role in creating a biocompatible environment for osteogenic cells [27]. Bone scaffolds enable cells to generate tissue with specific shape, size, and functionality, making scaffold design and fabrication central to biomaterials research and regenerative medicine [28]. Scaffold performance depends on several design variables, including microstructure, pore size, porosity, mechanical properties, and surface chemistry. The microstructure should mimic native bone tissue, incorporating extracellular matrix-like features. Adequate porosity and interconnected pores are essential for nutrient and waste transport. In vitro diffusion is limited to 100–300 μm; therefore, scaffolds must ensure that cells reside within 300 μm of capillary networks [29].
2.2.1. Chemical and Mechanical Properties of Bone TE Scaffold
Studies have shown that bone defects can be effectively repaired using scaffolds seeded with appropriate cell densities or embedded with growth factors [30]. For successful osseous tissue regeneration, the scaffold must exhibit four key chemical properties: osteoconductivity, which ensures a porous structure that supports cell attachment, migration, and nutrient exchange; osteoinductivity, which involves the incorporation of growth factors to induce mesenchymal stem cell differentiation into osteoblasts; osteogenicity, which promotes osteoblast activity for mineral deposition and collagen calcification; and osteointegration, which enables the newly formed mineralized tissue to establish strong bonding with the surrounding implant site [30].
Figure 3 shows a typical stress-strain behavior of a polymer scaffold. Both polymer scaffolds and wet cancellous bone exhibit compressive stress–strain curves characterized by three regions: an initial linear elastic phase, a plateau region associated with structural collapse, and a densification phase where stress rises sharply. However, cancellous bone demonstrates significantly higher stiffness and strength due to its mineralized trabecular architecture, with mechanical properties strongly dependent on relative density; as density increases, elastic modulus and yield stress scale approximately with the square of density, following Gibson–Ashby models. In contrast, polymer scaffolds, being highly porous, show lower modulus and plateau stress, with porosity playing a dominant role in reducing load-bearing capacity. However, increased porosity in both systems enhances permeability but compromises mechanical integrity, making cancellous bone inherently superior for load-bearing applications, while PHBV scaffolds prioritize biocompatibility and tissue ingrowth over structural strength.
2.2.2. Physical Properties of Bone TE Scaffold
An ideal bone scaffold should mimic natural bone structure and exhibit characteristics such as 3D architecture, appropriate porosity, interconnected pores, and optimal pore size [29]. Osteoconductivity and pore architecture significantly influence osteoprogenitor cell colonization [31]. Precise pore design is critical for effective matrix structure [31].
2.2.3. Surface Properties of Bone TE Scaffold
Surface properties play a critical role in scaffold interaction with host tissue. Surface roughness influences osteoblast function and overall outcomes [31]. AFM imaging reveals collagen fibril networks with 67 nm periodicity [32]. Surface modification strategies include coatings, plasma treatment, and incorporation of bioactive compounds [33,34]. Interaction zone between tissue and implant is ~0.1–1 nm [35]. Collagen or conductive polymers coatings enhance hydrophilicity and cell adhesion [37,38]. Therefore, surface engineering is a key consideration in tissue engineering applications.
Khan et al. (2008) demonstrated that variations in surface roughness and pore size significantly affect cellular behavior. Furthermore, nanoscale surface modifications can enhance biological performance. For example, HA/PHBV composite scaffolds exhibit a fibrous morphology with a high surface-to-volume ratio compared to scaffolds with solid pore walls. Such structures improve protein adsorption and facilitate cell attachment and proliferation, thereby enhancing scaffold functionality [30]. Gas plasma treatment is one promising method for introducing functional groups onto polymer surfaces through covalent modification. Biochemical surface modifications can further modulate tissue responses. For instance, collagen, a primary component of bone matrix, can be used to coat scaffold surfaces. Collagen contains specific amino acid sequences that bind directly to cell-surface receptors, improving cell adhesion. Yang et al. (2002) reported that coating poly-D,L-lactide (PDLLA) with collagen enhanced hydrophilicity and surface roughness, resulting in improved cell activity[37]. Similarly, conductive PEDOT-PSS coating on PHBV/PLA electrospun fibers significantly increased hydrophilicity and promoted cell attachment and proliferation [38].
2.2.4. Bioactivity Properties
Bioactivity remains a cornerstone in scaffold design, as it determines the material’s ability to bond with living tissue under physiological-like conditions. Recent studies have reinforced the importance of simulated body fluid (SBF) testing as a predictive tool for in vivo performance. Shendage et al. [39] demonstrated that cellulose-based scaffolds impregnated with calcium silicate and turmeric exhibited hydroxyapatite formation during SBF immersion, alongside hemocompatibility and enhanced osteogenesis in vivo. Similarly, TiO₂ scaffolds pre-treated in 10× SBF developed a biomimetic apatite layer, significantly improving bone cell adhesion and proliferation [40]. These findings highlight that SBF-induced apatite deposition not only validates scaffold bioactivity but also serves as a critical step toward optimizing osteointegration and regenerative potential.
Current studies demonstrate that incorporating conductive polymers into scaffolds enhances osteogenic differentiation and mineralization, particularly when combined with electrical stimulation [41,42]. Polypyrrole (PPy) thin films prepared on tricalcium phosphate (TCP) substrates via admicellar polymerization have also been investigated for their influence on mesenchymal stem cells (MSCs). Castana et al. reported that PPy film thickness, regulated by pyrrole monomer concentration, significantly affected MSC adhesion, proliferation, and alkaline phosphatase activity, with optimal adhesion observed at 20 × 10⁻³ M [43]. Higher monomer concentrations reduced cell attachment and calcified matrix formation. Bendrea et al. later confirmed that these effects were attributable to surface morphology rather than cytotoxicity [44]. More recent work has expanded on these findings, showing that polymer films such as P3HT and PPy derivatives promote osteoblastic differentiation of MSCs and adipose-derived stem cells, underscoring their promise in regenerative medicine [45,46]. Recent advancements have refined these models by incorporating age- and sex-specific calcium kinetics [47] and linking calcium fluxes to bone metabolism and energy regulation [48]. These updated frameworks enhance our understanding of calcium dynamics in both nutritional and orthopedic contexts.
2.2.5. Degradation Properties
The hydrolytic degradation rate of polymeric scaffolds is a critical parameter in biomedical applications. Degradation behavior directly influences implant performance, drug release kinetics, and the mechanical stability of scaffolds over time. The primary motivation for using absorbable and biodegradable polymers is to avoid secondary surgical procedures by ensuring complete dissolution of implant components or by providing time-dependent mechanical properties. Furthermore, controlled degradation enables the release of bioactive agents such as growth factors or antibiotics from polymer matrices. Both material-related and medium-related factors strongly affect degradation kinetics. Key material factors include molecular structure (molecular weight and distribution, comonomer composition, terminal groups, crosslink density, tacticity, and branching), morphology (shape, dimensions, pore size, porosity), and highly ordered structures (crystallinity, spherulitic size, and orientation). Medium-related factors encompass pH, temperature, solutes, microbial activity, enzymatic presence, and mechanical stress. Among these, molecular weight, crystallinity, porosity, pH, and temperature are particularly influential. For example, the presence of catalytic molecules, incorporation of hydrophilic monomers, and variations in pH or temperature significantly alter degradation rates. Increased molecular weight and crystallinity generally reduce hydrolytic degradation.
Polymer degradation can proceed via surface erosion or bulk erosion [49]. In surface erosion, only the outer layers are degraded by ions or catalytic molecules, leaving the scaffold core intact. This mechanism is typically observed when enzymes or alkalis are present in the degradation medium. In contrast, bulk erosion occurs in the absence of catalytic molecules, such as in phosphate-buffered solutions, where water penetrates the polymer matrix and hydrolysis occurs throughout. Material thickness is a critical determinant of mechanism. Crystalline polymers, characterized by numerous spherulites, degrade preferentially in amorphous regions, as these chains are more susceptible to. Early degradation often involves surface erosion, followed by bulk erosion as molecular weight decreases and soluble oligomers form. Carboxyl end groups further catalyze chain cleavage, accelerating degradation in amorphous regions [50]. Major factors which affect polymer degradation are polymer morphology, composition, molecular weight, additives, specimen size and porosity [51].
2.3. Bone-Substituted Biomaterials
When a biomaterial is exposed to body fluids, it interacts directly with internal tissues, imposing strict requirements on its properties. The foremost criterion is biocompatibility, the material must not provoke adverse biological responses and should remain stable within the body until the formation of new tissue. Additionally, it must be nontoxic and noncarcinogenic, which limits the range of suitable engineering materials. Beyond biological compatibility, the biomaterial should exhibit adequate physical and mechanical properties to function as a replacement or augmentation for body tissues. Practical considerations include ease of fabrication, cost-effectiveness, and availability. Broadly, biomaterials fall into three categories: metals, ceramics, and polymers.
Material selection for scaffolds depends on biocompatibility, biodegradability, mechanical properties, and cellular interactions. Surface biocompatibility is influenced by surface chemistry, which affects the adsorption of biological molecules and regulates cell. Other factors include molecular weight, solubility, shape, hydrophobicity/hydrophilicity, surface energy, and water absorption. For bone tissue engineering, commonly used materials include metals, bioceramics, and biopolymers.
2.3.1. Metals
Metals are among the most widely used materials for implants, particularly in orthopedic surgery. Applications range from wires and screws to fracture-fixation plates and total joint prostheses for hips, knees, shoulders, and elbows. They are also extensively used in oral, maxillofacial, and cardiovascular surgeries. Metals are favored in orthopedics for their ability to bear heavy loads, resist fatigue, and undergo plastic deformation before failure. Historical records indicate the use of brass sutures for fracture repair as early as 17th century. However, surgical implantation was largely unsuccessful before the advent of anesthesia, antisepsis, and antibiotics. Early metals were prone to corrosion and leaching in vivo. With improved surgical techniques, metals such as aluminum, platinum, and nickel-plated devices were introduced, followed by high-carbon steel in the early 20th century. Cobalt-chromium alloys appeared in the 1920s, and titanium became popular in the late 1940s.
Currently, commonly used orthopedic metals include: Stainless steels (F55, F138, 316L), Cobalt-chromium alloys (F75, F90), Titanium and its alloys (F67 commercially pure titanium, F136 Ti-6Al-4V). Stainless steel is widely used for fracture fixation due to its high tensile strength, ductility, and ability to be cold-worked—an essential feature for shaping plates during surgery. However, its use in artificial joints declined because early castings lacked adequate fatigue resistance. Fatigue properties are critical since an artificial hip joint experiences millions of load cycles annually, with forces reaching two to three times body weight during walking. Titanium alloys, such as Ti-6Al-4V, are preferred for joint prostheses because their elastic modulus is roughly half that of stainless steel and cobalt-chromium alloys, reducing the risk of stress shielding [52].
In addition to these permanent metals, biodegradable metals such as magnesium, zinc, and iron alloys have recently emerged as promising alternatives for temporary orthopedic implants. These materials provide mechanical support during the critical healing phase and gradually degrade in vivo, eliminating the need for secondary surgeries to remove hardware. Magnesium alloys, in particular, have been extensively studied for fracture fixation due to their favorable biocompatibility and mechanical properties, though challenges remain in controlling their corrosion rate [53]. Zinc and iron alloys are also under investigation, offering slower degradation profiles and potential applications in load-bearing implants [54]. Collectively, biodegradable metals represent a new frontier in orthopedic biomaterials, combining structural performance with resorbability to reduce patient morbidity and healthcare costs [55]. The emergence of biodegradable metals offers a promising alternative, eliminating the need for secondary removal surgeries and enabling gradual load transfer to healing tissues. Ongoing research continues to optimize their mechanical properties and biocompatibility for broader clinical use.
Table 2.
Comparative Overview of Permanent vs Biodegradable Metals in Orthopedic Applications.
| Category | Examples | Key Properties | Biomedical Applications | References |
| Permanent Metals | Stainless steel, Titanium alloys (Ti-6Al-4V), Cobalt-chromium alloys | High mechanical strength, corrosion resistance, long-term stability, non-degradable | Joint replacements, fracture fixation devices, spinal implants | [56] |
| Biodegradable Metals | Magnesium alloys, Zinc alloys, Iron-based alloys | Biodegradable in physiological environment, good biocompatibility, promotes bone growth | Temporary fracture fixation, bone scaffolds, pediatric implants | [57] |
2.3.2. Bioceramics
Bioceramics have long been used in dentistry, but their orthopedic applications are mainly limited to repairing or replacing hard tissues like bone. Bone itself is a composite of organic material and a ceramic phase dominated by calcium hydroxyapatite (HA), which has a Ca/P ratio of about 1.67. Synthetic HA is widely used because it bonds well with natural bone and is highly biocompatible, bioactive, and osteoconductive. It is commonly applied as a coating on metal implants to improve long-term fixation. However, pure HA is too brittle and weak for load-bearing uses. To address these mechanical limitations, HA is often combined with polymers or biopolymers to form composite scaffolds, such as PHBV/HA and PCL/HA systems, which improve stability and support osteogenic activity [58,59]. Maintaining an ideal Ca/P ratio (1.50–1.67) is essential for synthetic HA to support bone regeneration.
Nano-hydroxyapatite (nHA), which mimics the nanostructure of natural bone mineral, offers enhanced surface area, protein interaction, and bioactivity. Compared to micro-scale HA, nHA promotes better cell adhesion and calcium deposition. Multiple synthesis methods exist for producing micro- and nano-scale HA, including emulsion, co-precipitation, sol-gel, and microwave techniques. Microemulsions can yield fine particles but require large amounts of surfactants, while nanoemulsions produce uniform, stable droplets (20–200 nm) and are widely used across chemical, pharmaceutical, and cosmetic industries. While both micro- and nano-hydroxyapatite offer biocompatibility and osteoconductivity, nano-HA demonstrates superior biomedical performance due to its enhanced surface properties and ability to better support cellular functions. This makes nano-HA a more promising candidate for advanced bone regeneration and implant applications.
Table 3.
Comparative Overview of Micro- vs Nano-Hydroxyapatite in TE Applications.
| Form of HA | Key Properties | Biomedical Performance | References |
| Micro-hydroxyapatite (Micro-HA) | Lower surface area, larger particle size (1–100 µm), lower reactivity, limited mechanical strength | Moderate osteoconductivity, slower resorption, less effective in promoting cell adhesion and proliferation | [60] |
| Nano-hydroxyapatite (Nano-HA) | High surface area, nanoscale particle size (<100 nm), enhanced reactivity, better mechanical integration | Superior osteoconductivity, faster resorption, improved cell adhesion, proliferation, and differentiation | [61] |
Other Ceramic Materials in Orthopedic Tissue Engineering includes bioinert ceramics such as alumina (Al₂O₃) and zirconia (ZrO₂) which are widely used in load-bearing implants due to their high hardness, wear resistance, and chemical stability. Alumina has been applied in femoral heads and dental prostheses, while zirconia offers superior fracture toughness and is increasingly used in hip replacement acetabular cups and dental implants [62]. Bioactive glasses and glass-ceramics (e.g., 45S5 Bioglass®) exhibit osteoconductivity and osteoinductivity by forming a hydroxycarbonate apatite layer that bonds directly with bone. These materials are employed in bone fillers, scaffolds, and coatings for metallic implants, with glass-ceramics providing improved mechanical strength compared to pure bioactive glass [62]. Calcium phosphate ceramics beyond HA, such as tricalcium phosphate (TCP) and biphasic calcium phosphate (BCP), are resorbable and support bone regeneration. TCP degrades faster than HA, making it suitable for temporary scaffolds, while BCP combines HA and TCP to balance bioactivity with controlled resorption [57].
Composite and porous ceramics have also gained attention, particularly for scaffolds designed with interconnected pores to facilitate vascularization and nutrient exchange. Ceramic-polymer composites, such as HA combined with biodegradable polymers (PLA, PCL), overcome brittleness and enhance mechanical properties while maintaining osteogenic potential [63]. Overall, ceramic biomaterials provide a versatile toolkit for orthopedic tissue engineering. Their spectrum of properties, from bioinert stability to bioactive bonding and controlled biodegradability, enables tailored solutions for bone regeneration, implant coatings, and scaffold design.
2.3.3. Polymers
Polymers are classified as natural or synthetic biopolymers. Natural and synthetic biopolymers each offer distinct advantages and limitations in the context of tissue engineering. Natural polymers (collagen, gelatin, chitosan) provide excellent biocompatibility and bioactivity, making them ideal for promoting cellular functions. However, their mechanical weaknesses limit their use in load-bearing applications. In contrast, synthetic polymers (PLA, PLGA, PCL etc.) offer superior mechanical strength, predictable degradation profiles, and scalable production, but often lack the biological cues necessary for optimal cell interaction. To overcome these individual shortcomings, hybrid scaffolds that integrate both natural and synthetic polymers are increasingly being developed. These composite systems aim to combine the biological functionality of natural materials with the structural integrity of synthetic ones, representing a promising direction for the advancement of clinically effective tissue engineering solutions [64,65].
Recently, conductive polymers (CPs) have emerged as a critical class of materials in TE due to their unique ability to mediate electrical stimulation, a key factor in regulating cellular behavior. Their conjugated structures enable electronic conductivity, making them suitable for applications in neural interfaces, cardiac patches, biosensors, TE scaffolds and drug delivery systems. Among the most studied CPs are polypyrrole (PPy), polyaniline (PANI), poly(3,4-ethylenedioxythiophene) (PEDOT), and its doped form PEDOT:PSS. Importantly, electrical stimulation has been shown to enhance osteoblast proliferation, adhesion, and gene expression, underscoring the therapeutic potential of CP-based scaffolds [64]. While challenges remain, particularly stability and degradation in biological environments, composite systems that blend CPs with biodegradable polymers offer promising solutions, combining electrical functionality with improved biocompatibility and mechanical strength. Their unique combination of biocompatibility, tunable conductivity, and versatility in scaffold design positions them as a critical bridge between traditional biomaterials and next-generation bioelectronic interfaces, paving the way for advanced regenerative therapies and functional tissue restoration.
2.5. Fabrication Techniques of Tissue Engineering Scaffolds
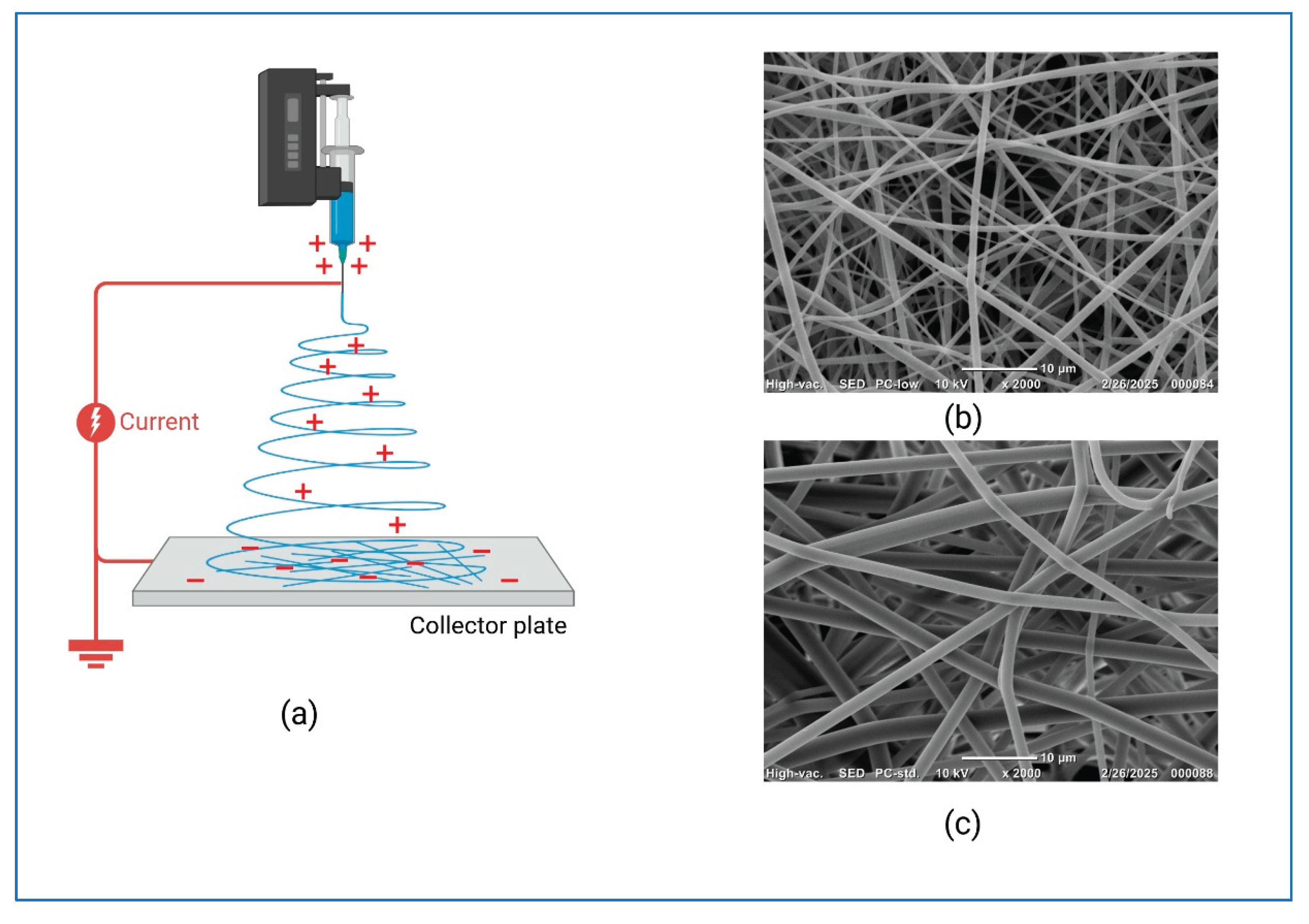
Various fabrication techniques have been developed to produce scaffolds for tissue engineering. These methods aim to create biodegradable and bioresorbable polymeric scaffolds with high porosity and surface area. Each technique offers distinct advantages and limitations. The most commonly used techniques are gas foaming, rapid prototyping such as 3D or 4D printing and selective lase sintering, electrospinning, freeze drying [64]. Among the techniques, electrospinning is an effective method for producing nanofibrous scaffolds that replicate the extracellular matrix, providing a biomimetic environment for tissue engineering. Figure 4 shows the SEM analysis of electrospun PVP scaffolds fiber diameters of 1853.90 ± 229 nm (15G) and 647.52 ± 638 nm (18G), highlighting the sensitivity of electrospinning to parameter changes. The results emphasize the need for precise optimization to produce scaffolds using conventional techniques with uniform morphology, high porosity, and interconnected architecture essential for cell adhesion, nutrient transport, and tissue integration.
Table 4 shows the comparison of various scaffold fabrication techniques.
Table 4.
Comparison of Scaffold Fabrication Techniques.
| Technique | Description | Advantages | Limitations |
| Gas Foaming | Uses blowing agents (CO₂, N₂) under supercritical conditions to create porous polymer structures. | Solvent-free process; low temperature reduces polymer degradation. | Produces small pore sizes; requires ultrasound for better interconnectivity. |
| Sintering | Compacts ceramic powders using heat or pressure without melting. | Allows control over porosity; suitable for ceramics. | High fragility; poor pore interconnectivity. |
| Electrospinning | Uses electric field to produce nanofibers from polymer solutions. | Mimics ECM structure; versatile for different polymers. | Limited control over 3D architecture; requires post-processing. |
| Casting & Particle Leaching | Introduces porogens (salt, sugar) into polymer solution; leached to form pores. | Produces highly porous scaffolds; simple method. | Time-consuming; residual particles may remain. |
| Polymer Phase Separation (TIPS) | Thermally induced phase separation to control pore morphology. | Effective for micro/nano-scale pores; adaptable for drug delivery. | Requires precise control of parameters; solvent handling needed. |
| Rapid Prototyping (3D Printing) | CAD-based layer-by-layer fabrication for complex architectures. | High precision; customizable for patient-specific defects. | Expensive equipment; slower than conventional methods. |
| Freeze-Drying | Creates porous scaffolds by freezing polymer solution and sublimating solvent. | Highly porous structure; good for drug/growth factor incorporation. | Requires careful parameter control; limited scalability. |
3. In Vitro Biological Evaluation of Bone Tissue Engineering Scaffolds
In vitro biological evaluation plays a critical role in assessing the biocompatibility, osteogenic capacity, and overall functional performance of bone tissue engineering scaffolds prior to in vivo experimentation. These studies provide essential insights into cell–scaffold interactions, degradation kinetics, and the ability of scaffolds to support osteogenic differentiation under controlled laboratory conditions. Cytocompatibility is commonly examined through assays such as MTT, Live/Dead staining, and Alamar Blue, with recent work on nano-carbonated hydroxyapatite/chitosan scaffolds reporting over 90% cell viability and improved osteoblast adhesion [66]. Osteogenic differentiation is typically evaluated by monitoring alkaline phosphatase activity, osteocalcin production, and RUNX2 expression, and oxygen-releasing PLA/CPO scaffolds have been shown to significantly enhance these markers under dynamic culture conditions [67]. To further mimic the physiological microenvironment, co-culture systems incorporating osteoblasts and endothelial cells are increasingly employed, with composite hydrogel scaffolds demonstrating enhanced angiogenic signaling and vascularization potential [68]. Scaffold morphology, particularly pore size and interconnectivity, also plays a decisive role in nutrient diffusion and cell migration; for example, PLA scaffolds engineered with 0.6-mm pores have shown improved cell infiltration and mechanical stability [69]. Dynamic culture systems, including bioreactors, provide mechanical stimulation and improved nutrient exchange, and biomimetic dual-sensing scaffolds have exhibited superior mineral deposition under such conditions [70] . To ensure consistency and reproducibility across studies, standardized guidelines such as ASTM F2739 outline validated methods for quantifying cell viability and related biological responses within biomaterial scaffolds [71].
4. In Vivo Biological Evaluation of Bone Tissue Engineering Scaffolds
In vivo evaluation of bone tissue engineering scaffolds frequently employs rabbit radial defects, rat calvarial defects, and canine mandibular models to monitor bone regeneration, vascularization, and mechanical integrity longitudinally. Common assessment methods include micro-computed tomography (micro-CT) for quantifying new bone volume, histological staining to examine tissue integration, and gene expression analysis to detect activation of osteogenic and angiogenic markers.
One notable advancement is the development of prevascularized, mineralized nanofibrous scaffolds composed of polylactic acid (PLA), hydroxyapatite, and decellularized vascular tissue. When implanted in rabbit radial defects, these scaffolds exhibited similar bone formation to allografts within eight weeks, with micro-CT confirming robust neovascularization. Additionally, 3D-printed magnesium-silicate/β-tricalcium phosphate (MS/β-TCP) scaffolds tested in rat calvarial defects achieved controlled release of Mg²⁺ and Si⁴⁺ ions. These ions activated the PI3K/Akt signaling pathway and significantly enhanced both bone volume and vessel density over 6–12 weeks [72,73]
In intraoral applications, electrospun scaffolds coated with the AMP2 peptide were evaluated in beagle mandibular defects. These AMP2-functionalized scaffolds achieved guided bone regeneration comparable to xenografts—without requiring barrier membranes—simplifying the surgical procedure while maintaining osteogenic efficacy. For infected bone defects, a newly engineered 3D-printed titanium alloy scaffold featuring a triply periodic minimal surface, with sequential dual delivery of BMP-2 (osteogenic) and antibiotic-loaded PLGA microspheres, demonstrated effective eradication of infection and promoted bone healing in rat models [74,75]. Composite PLA–calcium phosphate glass scaffolds have been shown to enhance angiogenesis and vascular maturation in mouse subcutaneous implantation models. Within one week post-implantation, substantial blood vessel infiltration occurred, with mature vascular networks observed by week four, underscoring the importance of scaffold architecture in vascular integration [76].
Collectively, these studies highlight several emerging trends: (1) early angiogenesis is essential for scaffold integration and long-term bone repair; (2) bioactive ionic release (e.g., Mg²⁺, Si⁴⁺) can concurrently stimulate osteogenesis and angiogenesis; (3) multifunctional scaffolds combining osteoinductive and antimicrobial agents are effective against infected bone defects; (4) peptide-functionalized scaffolds can eliminate the need for barrier membranes in oral bone regeneration; and (5) architectural optimization—such as hierarchical porosity, prevascularization, and controlled drug delivery—remains key to replicating native bone microenvironments and enhancing healing outcomes.
5. Clinical Translation Challenges
Despite promising preclinical outcomes, translating bone tissue engineering scaffolds into clinical practice encounters numerous obstacles. Technical challenges persist in scaling up production of complex architectures—such as hierarchical porosity and patient-specific designs—to Good Manufacturing Practice (GMP) standards without compromising scaffold integrity or reproducibility [77]. Regulatory hurdles further complicate clinical adoption: multifunctional scaffolds combining osteoinductive, antimicrobial, or angiogenic components often blur the lines between medical device, biologic, or combination products, demanding extensive safety and efficacy data for approval. Additionally, managing the host immune response to implanted scaffolds is critical; evidence shows that residual decellularization agents or scaffold degradation products can shift macrophage polarization toward a pro-inflammatory state, impairing integration [78].
Challenges inherent to 3D printing technologies—including material selection, print resolution, and control of cell–material interactions—remain significant barriers to clinical use. As noted by Zhao et al. (2024), discrepancies between lab-scale successes and clinical outcomes underscore the need for standardized protocols and translational frameworks [79]. Finally, commercialization is hindered by high production costs, limited reimbursement pathways, and lack of long-term human data demonstrating clinical benefit and cost-effectiveness. Overcoming these challenges requires a coordinated approach involving robust manufacturing workflows, interdisciplinary collaboration, and early engagement with regulatory and funding agencies [77].
6. Limitations and Future Directions
Despite significant advancements in scaffold design and in vivo validation, several gaps remain in translating these technologies to clinical practice. First, most studies rely on small animal models, which do not fully replicate the biomechanical and immunological complexity of human bone healing. Large animal models and long-term studies are needed to evaluate scaffold performance under load-bearing conditions and chronic disease states such as osteoporosis or diabetes. Second, while angiogenesis and osteogenesis have been widely studied, the immune response to scaffolds, particularly the role of macrophage polarization and inflammatory signaling, requires deeper investigation to ensure predictable outcomes in diverse patient populations. Another critical gap lies in the integration of multifunctional properties. Although scaffolds with combined osteoinductive and antimicrobial capabilities have shown promise, their long-term stability, controlled release kinetics, and potential cytotoxicity remain poorly understood. Furthermore, current fabrication techniques, including 3D printing and electrospinning, offer excellent architectural control but often lack scalability and cost-effectiveness for clinical translation. Finally, regulatory pathways for complex, bioactive scaffolds are still evolving, creating uncertainty in commercialization timelines.
Future research should focus on developing smart scaffolds capable of responding to local biological cues, incorporating biodegradable sensors for real-time monitoring of healing, and leveraging personalized medicine approaches such as patient-specific scaffold designs using advanced imaging and computational modeling. Additionally, combining scaffold technology with stem cell therapy, gene delivery, and growth factor gradients could further enhance regenerative outcomes. Collaborative efforts between material scientists, clinicians, and regulatory bodies will be essential to bridge the gap between laboratory innovation and clinical application.
References
- Zhu, T.; Zhou, H.; Chen, X.; Zhu, Y. Recent advances of responsive scaffolds in bone tissue engineering. Front. Bioeng. Biotechnol. 2023, 11, 1296881. [Google Scholar] [CrossRef] [PubMed]
- Puppi, D.; Chiellini, F.; Piras, A.M.; Chiellini, E. Polymeric materials for bone and cartilage repair. Prog. Polym. Sci. 2010, 35, 403–440. [Google Scholar] [CrossRef]
- Rose, F.R.A.J.; Oreffo, R.O.C. Bone tissue engineering: Hope vs hype. Biochem. Biophys. Res. Commun. 2002, 292, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gharibshahian, M.; Salehi, M.; Beheshtizadeh, N.; Nourbakhsh, M.S.; Alizadeh, M. Recent advances on 3D-printed PCL-based composite scaffolds for bone tissue engineering. Front. Bioeng. Biotechnol. 2023, 11, 1168504. [Google Scholar] [CrossRef]
- Khobragade, S.S.; Deshmukh, M.; Vyas, U.; Ingle, R.G. Innovative approaches in bone tissue engineering: Strategies for cancer treatment and recovery. Int. J. Mol. Sci. 2025, 26, 3937. [Google Scholar] [CrossRef]
- Mikos, A.G.; et al. Principles of tissue engineering. J. Biomed. Mater. Res. 1993, 27, 123–138. [Google Scholar]
- Hansmann, J.; et al. Bioreactor systems for bone tissue engineering. Adv. Drug Deliv. Rev. 2013, 65, 62–79. [Google Scholar]
- Chen, Q.; et al. Bone tissue engineering: Advances and challenges. Tissue Eng. 2006, 12, 1137–1151. [Google Scholar]
- Schieker, M.; et al. Tissue engineering of bone: Biomaterials, cell sources and growth factors. J. Cell. Mol. Med. 2006, 10, 6–17. [Google Scholar]
- Rastogi, S.; Verma, R.; Gouru, S.A.; Venkatesan, K.; Pandian, P.M.; Khan, M.I.; Deka, T.; Kumar, P. Emerging technologies in bone tissue engineering: A review. J. Bionic Eng. 2025, 22, 2261–2285. [Google Scholar] [CrossRef]
- Rosa, N.; Moura, M.F.S.F.; Olhero, S.; et al. Bone: An Outstanding Composite Material. Appl. Sci. 2022, 12, 3381. [Google Scholar] [CrossRef]
- Hamandi, F.; Goswami, T. Hierarchical Structure and Properties of the Bone at Nano Level. Bioengineering 2022, 9, 677. [Google Scholar] [CrossRef] [PubMed]
- Wittig, N.K.; Birkedal, H. Bone Hierarchical Structure: Spatial Variation across Length Scales. IUCrJ 2022, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Alcântara, A.C.S.; Felix, L.C.; Galvão, D.S.; et al. Devising Bone Molecular Models at the Nanoscale. Materials 2022, 15, 2274. [Google Scholar] [CrossRef] [PubMed]
- Schwarcz, A.V.; et al. The Ultrastructure of Bone and Its Relevance to Mechanical Properties. Front. Phys. 2017, 5, 45. [Google Scholar] [CrossRef]
- Luo, Y.; Amromanoh, O. Bone Organic-Inorganic Phase Ratio Is a Fundamental Determinant of Bone Material Quality. Appl. Bionics Biomech. 2021, 2021, 1–10. [Google Scholar] [CrossRef]
- Allen, M.R.; Wallace, J. Mechanical Properties of Bone. In Skeletal Tissue Mechanics; Springer: Cham, Switzerland, 2025; pp. 151–192. [Google Scholar]
- Wu, B.; Wu, Y.; Liu, M.; et al. Mechanical Behavior of Human Cancellous Bone in Alveolar Bone under Uniaxial Compression and Creep Tests. Materials 2022, 15, 5912. [Google Scholar] [CrossRef]
- Donsante, S.; Palmisano, B.; Serafini, M.; et al. From Stem Cells to Bone-Forming Cells. Int. J. Mol. Sci. 2021, 22, 3989. [Google Scholar] [CrossRef]
- Kitaura, H.; Marahleh, A.; Ohori, F.; et al. Osteocyte-Related Cytokines Regulate Osteoclast Formation and Bone Resorption. Int. J. Mol. Sci. 2020, 21, 5169. [Google Scholar] [CrossRef]
- Maruyama, M.; et al. Modulation of the Inflammatory Response and Bone Healing. Front. Endocrinol. 2020, 11, 386. [Google Scholar] [CrossRef]
- ElHawary, H.; et al. Bone Healing and Inflammation: Principles of Fracture and Repair. Semin Plast Surg 2021, 35, 141–147. [Google Scholar] [CrossRef]
- Sanders, E.J.; Parker, T.; Smith, A. Scaffold Design for Bone Tissue Engineering: Biological Considerations. J. Biomed. Mater. Res. 2000, 52, 231–240. [Google Scholar] [CrossRef]
- Wan, C.; Li, J.; Zhou, Y. Influence of Scaffold Architecture on Cell Migration and ECM Deposition. Biomaterials 1997, 18, 953–960. [Google Scholar]
- Flemming, R.; Green, D.; Brown, K. Mechanical Loading and Scaffold Performance in Bone Regeneration. Tissue Eng. 1999, 5, 291–302. [Google Scholar]
- Green, D.; Patel, M.; Jones, R. Spatial Organization of Bone Cells in Engineered Scaffolds. J. Orthop. Res. 1994, 12, 465–472. [Google Scholar]
- Li, J.; Yang, F.; Xu, H. Scaffold Architecture and Osteogenic Cell Behavior. Biomaterials 2002, 23, 123–135. [Google Scholar]
- Longer, R.; Vacant, A. Advances in Scaffold Fabrication for Regenerative Medicine. Adv. Drug Deliv. Rev. 1999, 39, 211–220. [Google Scholar]
- Hutmacher, D.W. Scaffolds in Tissue Engineering Bone and Cartilage. Biomaterials 2001, 22, 2529–2543. [Google Scholar]
- Khan, Y.; Yaszemski, M.J.; Mikos, A.G. Tissue Engineering Scaffolds for Bone Repair: Chemical Properties. Tissue Eng. 2008, 14, 163–174. [Google Scholar]
- Liu, X.; Ma, P.X. Polymeric Scaffolds for Bone Tissue Engineering. Biomaterials 2006, 27, 2414–2431. [Google Scholar] [CrossRef]
- Hassenkam, T.; Jørgensen, L.; Pedersen, M. AFM Imaging of Bone Surface Nanostructure. Bone 2004, 35, 4–10. [Google Scholar] [CrossRef]
- Williams, D.F. Surface Modification Strategies for Biomaterials. Biomaterials 1999, 20, 1321–1335. [Google Scholar]
- Park, J.B. Biomaterials Science: Introduction to Materials in Medicine; Academic Press, 1979. [Google Scholar]
- Ong, J.L.; Lucas, L.C. Interaction Zone Between Tissue and Implant Surfaces. J. Biomed. Mater. Res. 1998, 39, 152–160. [Google Scholar]
- Chen, Q.; Roether, J.A.; Boccaccini, A.R. Surface Engineering for Bone Tissue Scaffolds. Biomaterials 2006, 27, 2414–2431. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Xu, H.; Li, J. Collagen Coating Enhances Scaffold Hydrophilicity and Cell Adhesion. Biomaterials 2002, 23, 123–135. [Google Scholar]
- Chang, H. C.; Sun, T.; Sultana, N.; Lim, M. M.; Khan, T. H.; Ismail, A. F. Conductive PEDOT:PSS coated polylactide (PLA) and poly(3-hydroxybutyrate-co-3-hydroxyvalerate) (PHBV) electrospun membranes: Fabrication and characterization. Materials Science and Engineering: C 2016, 61, 396–410. [Google Scholar] [CrossRef]
- Shendage, S.; Kachare, K.; Gaikwad, K.; Kashte, S.; Mai, Fu.; Ghule, A. V. Cellulose-based bioactive material and turmeric-impregnated flexible and biocompatible scaffold for bone tissue engineering applications. J. Mater. Chem. B 2025, 15, 4570–4581. Available online: https://pubs.rsc.org/en/content/articlelanding/2025/tb/d4tb02028f. [CrossRef]
- Shin, K.; Acri, T.; Geary, S.; Salem, A. K. Biomimetic Mineralization of Biomaterials Using Simulated Body Fluids for Bone Tissue Engineering and Regenerative Medicine. Tissue Engineering. Part A 2017, 23(19-20), 1169. [Google Scholar] [CrossRef]
- Oktay, B.; Akkad, H.; Özerol, E.A. Recent advances in conducting tissue engineering based on conducting polymers. J. Biomater. Sci. Polym. Ed. 2025, 36, 2527910. [Google Scholar] [CrossRef]
- Aboagye, J.; Edwards, M.; Ge, J.; Hong, Y.; Yang, H. Evaluating and improving biocompatibility of conductive polymers for cardiac tissue engineering. J. Mater. Chem. B 2026, 14, D5TB01523E. [Google Scholar] [CrossRef]
- Castana, R.; et al. Title of study. Journal Name 2004, Volume, Pages. (Insert full MDPI citation).
- Bendrea, A.-D.; et al. Title of study. Journal Name 2011, Volume, Pages. (Insert full MDPI citation).
- Campione, P.; Rizzo, M.G.; Bauso, L.V.; Ielo, I.; Messina, G.M.L.; Calabrese, G. Osteoblastic differentiation of human adipose-derived mesenchymal stem cells on P3HT thin polymer film. J. Funct. Biomater. 2024, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Liao, R.; Li, X.; Zhang, C.; Huo, S.; Qin, L.; Xiong, Y.; He, T.; Xiao, G.; Zhang, T. Mesenchymal stem cells in treating human diseases: molecular mechanisms and clinical studies. Signal Transduct. Target. Ther. 2025, 10, 2313. [Google Scholar] [CrossRef] [PubMed]
- Hartung, N.; Abrams, S.A.; Huisinga, W.; Weisser, K. Consolidated calcium kinetic rates in a Caucasian population as a function of age and sex. bioRxiv 2024. [Google Scholar] [CrossRef]
- Choi, I.A.; Umemoto, A.; Mizuno, M.; Park-Min, K.H. Bone metabolism: an underappreciated player in metabolic health and disease. npj Metab. Health Dis. 2024, 1, 10. [Google Scholar]
- Sultana, N.; Khan, T. H. In Vitro Degradation of PHBV Scaffolds and nHA/PHBV Composite Scaffolds Containing Hydroxyapatite Nanoparticles for Bone Tissue Engineering. Journal of Nanomaterials 2012, 2012(1), 190950. [Google Scholar] [CrossRef]
- Feng, P.; Jia, J.; Liu, M.; Peng, S.; Zhao, Z.; Shuai, C. Degradation mechanisms and acceleration strategies of poly (lactic acid) scaffold for bone regeneration. Materials & Design 2021, 210, 110066. [Google Scholar] [CrossRef]
- Mohseni, M; Cometta, S; Klein, L; Wille, ML; Vaquette, C; Hutmacher, DW; Medeiros Savi, F. In vitro and in vivo degradation studies of a dual medical-grade scaffold design for guided soft tissue regeneration. Biomater Sci. 2025, 13(8), 2115–2133. [Google Scholar] [CrossRef] [PubMed]
- Oldani, C; Dominguez, A. Titanium as a Biomaterial for Implants [Internet]. Recent Advances in Arthroplasty. InTech. Available from. [CrossRef]
- Thomas, K.K.; Zafar, M.N.; Pitt, W.G.; Husseini, G.A. Biodegradable Magnesium Alloys for Biomedical Implants: Properties, Challenges, and Surface Modifications . Appl. Sci. 2024, 14(1). [Google Scholar] [CrossRef]
- Khan, A.R.; Shabbir, M.T.; Grewal, N.S.; Zhang, H.J.; Jun, Z. Recent Progress in the Application of Biodegradable Metal Implants . Biomed. Lett. 2024, 10(1), 1–13. [Google Scholar] [CrossRef]
- Abbasi, I. Biodegradable Metallic Materials: Revolutionizing Medical Implants and Devices. AZoM Feature Article, June 2024.
- Niinomi, M. Recent research and development in titanium alloys for biomedical applications and healthcare goods. Science and Technology of Advanced Materials 2003, 4(5), 445–454. [Google Scholar] [CrossRef]
- Witte, F. The history of biodegradable magnesium implants: a review. Acta Biomater 2010, 6(5), 1680–92. [Google Scholar] [CrossRef] [PubMed]
- Sultana, N.; Wang, M. Fabrication of HA/PHBV composite scaffolds through the emulsion freezing/freeze-drying process and characterisation of the scaffolds. J Mater Sci: Mater Med 2008, 19, 2555–2561. [Google Scholar] [CrossRef]
- Hassan, M I; Sultana, N.; Hamdan, S. Bioactivity Assessment of Poly(ɛ-caprolactone)/Hydroxyapatite Electrospun Fibers for Bone Tissue Engineering Application. Journal of Nanomaterials 2014, 2014, 573238, 6 pages. [Google Scholar] [CrossRef]
- Dorozhkin, S. V. Calcium Orthophosphates in Nature, Biology and Medicine. Materials 2009, 2(2), 399. [Google Scholar] [CrossRef]
- Webster, TJ; Ergun, C; Doremus, RH; Siegel, RW; Bizios, R. Enhanced functions of osteoblasts on nanophase ceramics. Biomaterials 2000, 21(17), 1803–10. [Google Scholar] [CrossRef] [PubMed]
- Vaiani, L.; Boccaccio, A.; Uva, A. E.; Palumbo, G.; Piccininni, A.; Guglielmi, P.; Cantore, S.; Santacroce, L.; Charitos, I. A.; Ballini, A. Ceramic Materials for Biomedical Applications: An Overview on Properties and Fabrication Processes. Journal of Functional Biomaterials 2023, 14(3), 146. [Google Scholar] [CrossRef]
- Budharaju, H.; Suresh, S.; Sekar, M. P.; De Vega, B.; Sethuraman, S.; Sundaramurthi, D.; Kalaskar, D. M. Ceramic materials for 3D printing of biomimetic bone scaffolds – Current state-of-the-art & future perspectives. Materials & Design 2023, 231, 112064. [Google Scholar] [CrossRef]
- Sultana, N.; Cole, A.; Strachan, F. Biocomposite Scaffolds for Tissue Engineering: Materials, Fabrication Techniques and Future Directions. Materials 2024, 17, 5577. [Google Scholar] [CrossRef] [PubMed]
- Dhandayuthapani, B.; Yoshida, Y.; Maekawa, T.; Kumar, D. S. Polymeric Scaffolds in Tissue Engineering Application: A Review. International Journal of Polymer Science 2011, 2011(1), 290602. [Google Scholar] [CrossRef]
- Habiburrohman, M.R.; Jamilludin, M.A.; et al. Fabrication and in vitro cytocompatibility evaluation of porous bone scaffold based on cuttlefish bone-derived nano-carbonated hydroxyapatite reinforced with polyethylene oxide/chitosan fibrous structure. RSC Adv. 2025, 15, 8457. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.; Tirnoveanu, A.; et al. In Vitro Characterization of 3D-Printed PLA/CPO Oxygen Releasing Scaffolds: Mechanical and Biological Properties for Bone Tissue Engineering. J. Manuf. Mater. Process. 2025, 9, 149. [Google Scholar] [CrossRef]
- Li, C.; Chen, G.; et al. Indirect co-culture of osteoblasts and endothelial cells in vitro based on a biomimetic 3D composite hydrogel scaffold. PLoS ONE 2024, 19, e0298689. [Google Scholar] [CrossRef]
- Zohoor, A.; et al. Accelerated degradation testing of porous PLA scaffolds under alkaline conditions. Polymers 2023, 16, 876. [Google Scholar]
- Dixon, D.T.; Landree, E.N.; Gomillion, C.T. Biomimetic Dual-Sensing Bone Scaffolds: Characterization and In Vitro Evaluation Under Dynamic Culturing Conditions. Biomimetics 2025, 10, 598. [Google Scholar] [CrossRef]
- ASTM F2739-19; Standard Guide for Quantifying Cell Viability and Related Attributes within Biomaterial Scaffolds. ASTM International, 2023.
- Buckley, C.; Madhavarapu, S.; Kamara, Z.; Pellegrini, M.; Perry, B.; Gatt, C.J., Jr.; Freeman, J.W. In Vivo Evaluation of the Regenerative Capacity of a Nanofibrous, Prevascularized, Load-Bearing Scaffold for Bone Tissue Engineering. Regen. Eng. Transl. Med. 2023, 10, 56–67. [Google Scholar] [CrossRef]
- Wang, L.; Shen, M.; Tang, Z.; Tan, J.; Li, K.; Ma, H.; et al. 3D-Printed Magnesium Silicate/β-Tricalcium Phosphate Scaffolds Promote Coupled Osteogenesis and Angiogenesis by Activating PI3K/Akt Signaling Pathway. Front. Bioeng. Biotechnol. 2025, 12, 1518145. [Google Scholar] [CrossRef]
- Slavin, B.V.; Wu, S.; Sturm, S.R.; Hwang, K.K.; Almada, R.; Mirsky, N.A.; Nayak, V.V.; Witek, Ł.; Coelho, P.G. An Evaluation of Novel AMP2-Coated Electrospun Composite Scaffolds for Intraoral Bone Regeneration: A Proof-of-Concept In Vivo Study. Front. Bioeng. Biotechnol. 2025, 13, 1443280. [Google Scholar] [CrossRef]
- Ximenes-Carballo, C.; Rey-Viñolas, S.; Blanco-Fernandez, B.; Pérez-Amodio, S.; Engel, E.; Castano, O. Combining Three-Dimensionality and CaP Glass-PLA Composites: Towards an Efficient Vascularization in Bone Tissue Healing. Biomater. Adv. 2024, 164, 213985. [Google Scholar] [CrossRef]
- Vila, O.F.; Bagó, J.R.; Navarro, M.; Alieva, M.; Aguilar, E.; Engel, E.; Planell, J.; Rubio, N.; Blanco, J. Calcium Phosphate Glass Improves Angiogenesis Capacity of Poly(Lactic Acid) Scaffolds and Stimulates Differentiation of Adipose Tissue-Derived Mesenchymal Stromal Cells to the Endothelial Lineage. J. Biomed. Mater. Res. Part A 2013, 101A, 932–941. [Google Scholar] [CrossRef]
- Xu, C.; Ivanovski, S. Clinical translation of personalized bioengineered implant scaffolds. Nat Rev Bioeng 2025, 3, 390–407. [Google Scholar] [CrossRef]
- Romero, D.J.; Hussey, G.; Capella-Monsonís, H. Immune Response to Extracellular Matrix Bioscaffolds: A Comprehensive Review. Biologics 2025, 5, 28. [Google Scholar] [CrossRef]
- Zhao, X.; Li, N.; Zhang, Z.; et al. Beyond hype: unveiling the Real challenges in clinical translation of 3D printed bone scaffolds and the fresh prospects of bioprinted organoids. J Nanobiotechnol 2024, 22, 500. [Google Scholar] [CrossRef]
Figure 1.
Schematic diagram of Bone Tissue Engineering Strategy (Created with BioRender.com).
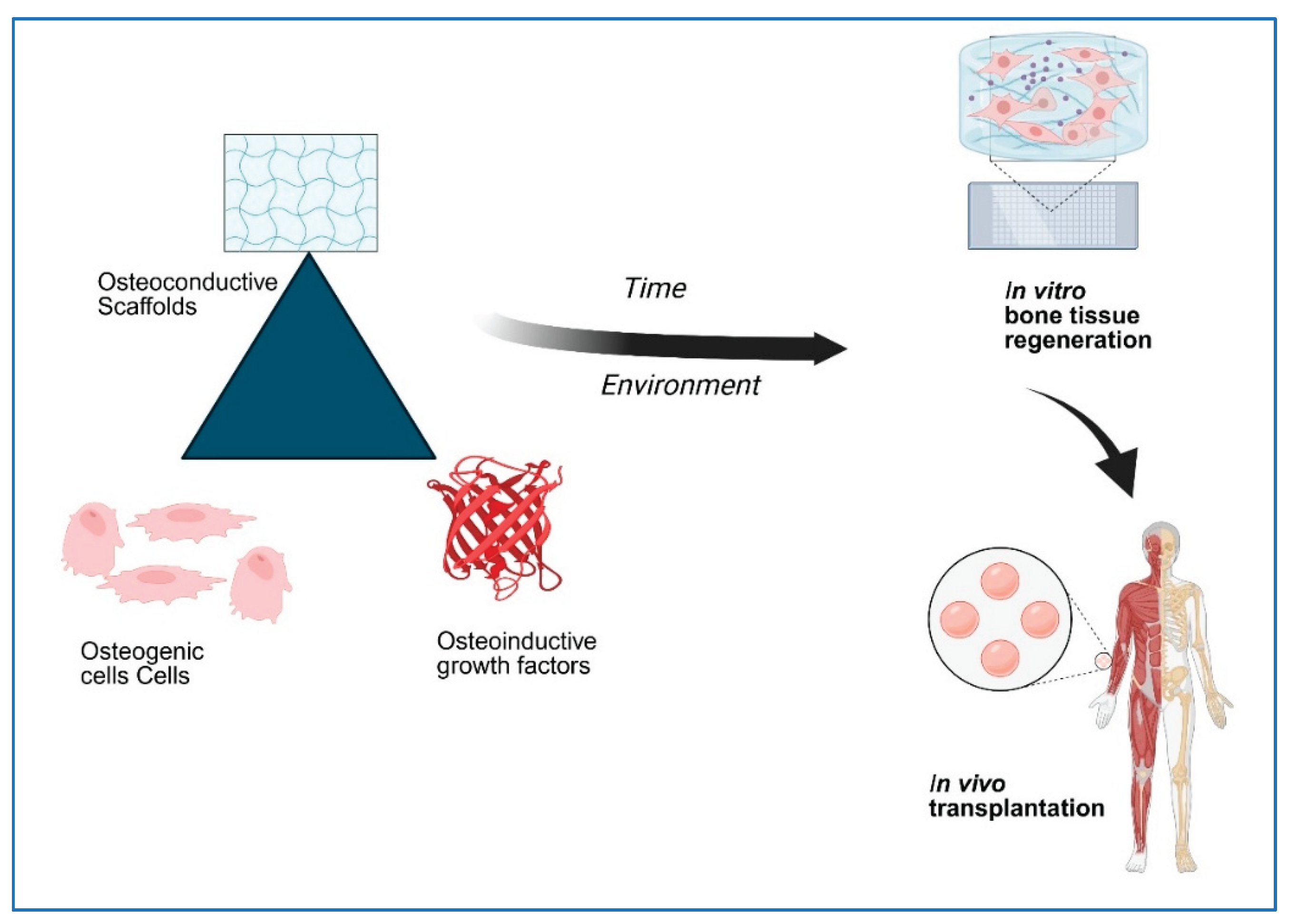
Figure 2.
Schematic diagram of different types of bone cells (Created with BioRender.com).
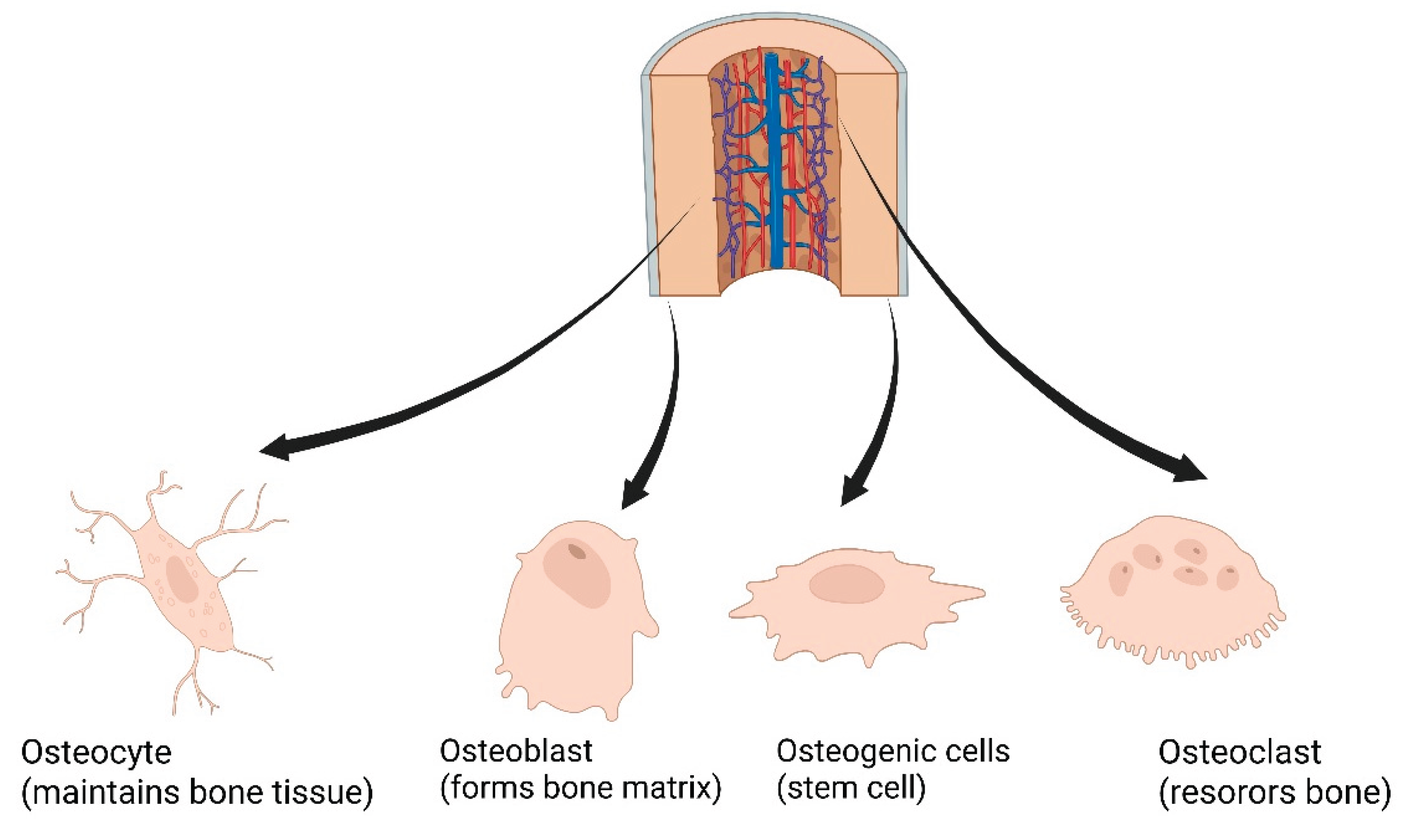
Figure 3.
Typical compressive curve of the polymer scaffolds. Region I: Linear elasticity, region II: plateau, region III: densification.
Figure 3.
Typical compressive curve of the polymer scaffolds. Region I: Linear elasticity, region II: plateau, region III: densification.
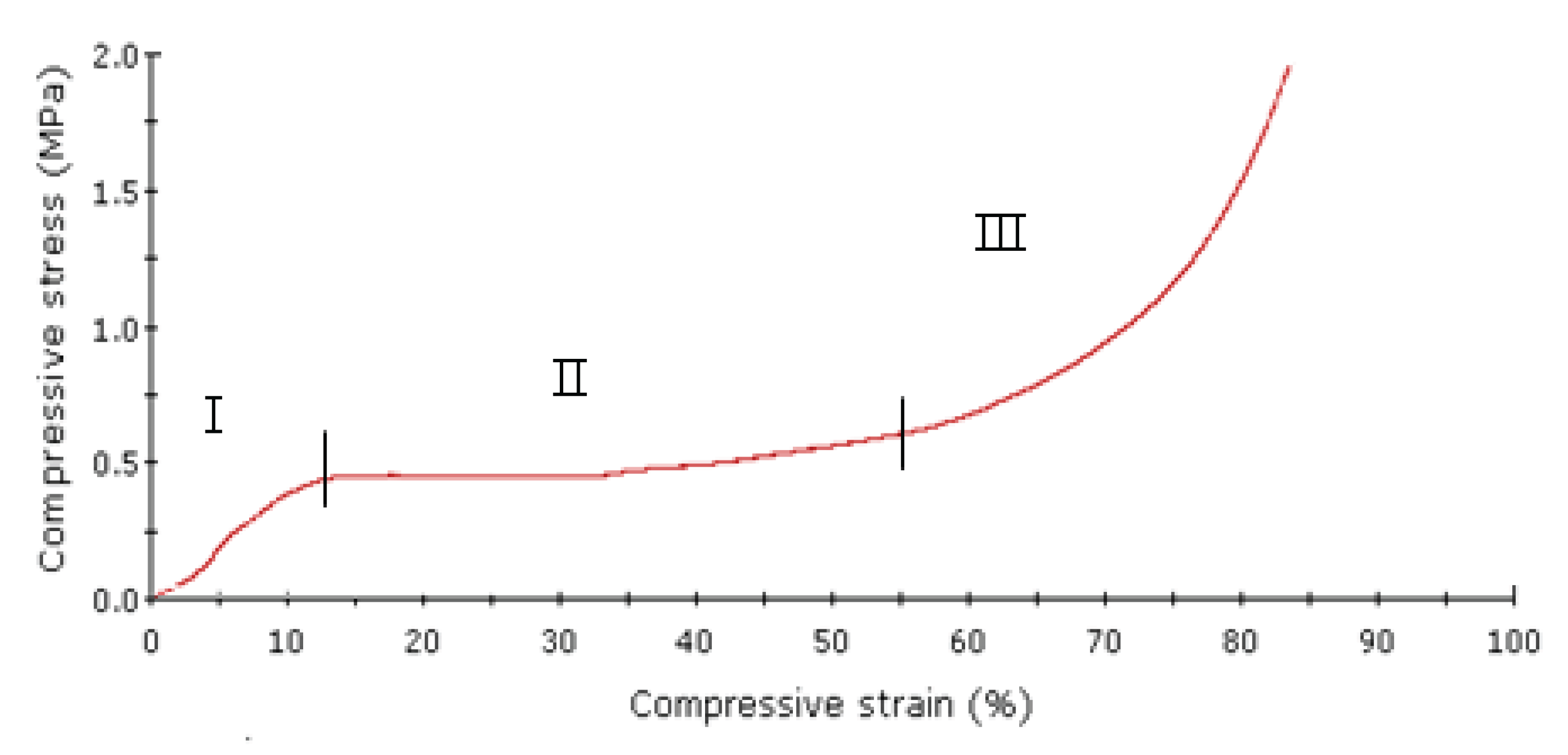
Figure 4.
Polymer scaffold fabrication using electrospinning. (a) Electrospinning set-up; (b) Scanning electron microscope of scaffolds using needle 18G; (c) using needle 15G.
Figure 4.
Polymer scaffold fabrication using electrospinning. (a) Electrospinning set-up; (b) Scanning electron microscope of scaffolds using needle 18G; (c) using needle 15G.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



