1. Introduction
Surgical cholecystostomy has been established as a surgical option for acute calculous cholecystitis for more than a century; today, the indications of temporary/definitive cholecystostomy have expanded to a broad spectrum of pathologies (including malignancy or miscellaneous), boosted by the possibility of minimally invasive access. Similar to all interventional techniques, cholecystostomy may be associated with early/late side effects and complications, depending on the therapeutic strategy for each pathology.
We report a late (21 years) complication of a temporary cholecystostomy in a previously normal (acalculous) gallbladder (GB), performed during open surgery for a complicated postbulbar ulcer; the patient was lost to follow-up. The cholecystostomy was a predisposing factor for subsequent late hazards and unfavorable outcomes, such as gallstone (GS) formation, emphysematous calculous cholecystitis, an abdominal abscess in the right hypochondrium, cholecystocutaneous fistula, unintentional incomplete, partial/subtotal cholecystectomy, partial remnant GB, and retained GS.
Late complications of temporary cholecystostomy in a normal gallbladder are rare (for obvious physiopathological reasons). To the best of our knowledge, this possibility has not been reported before; the case is unusual, so we decided to discuss all relevant issues. A thorough literature review was conducted using PubMed and Web of Science databases to contextualize this rare clinical scenario. Relevant publications were screened for case reports, retrospective analyses, systematic reviews, and meta-analyses published in English literature up to 2025.
2. Case Presentation
A 75-year-old female was urgently admitted (September 2024) for acute pain in the right upper quadrant of the abdomen and fever, in an apparently stable condition. She previously presented to an ambulatory institution; an abdominal ultrasound (US), 10 days before admission, visualized a GB with normal walls, no GS, also a 101x53 mm inhomogeneous, irregularly shaped (with imprecise limits) image in the right flank.
A voluminous cystic mass was observed on palpation of the right hypochondrium region, which was tender and painful, and also overlying cellulitis centered by a small spontaneous purulent discharge that had occurred only one day before (the main reason for presentation). Later on, bacterial culture examination identified Escherichia coli.
Laboratory demonstrated an inflammatory syndrome: CRP 153.42mg/L (normal values: 0-5/ mg/L), Fibrinogen 612 mg/dL (normal values: 170-420 /mg/dL), without other abnormalities.
Apart from high blood pressure, the medical history included surgery for a duodenal ulcer in 2003. She could not provide further details based on medical documents, but remembered that she was operated on by the first author of this study; she never presented for control afterwards. We were able to recover the surgical protocol, which demonstrated that the patient was unaware of previous biliary surgery; it was a crucial element for diagnosis in the situation of incomplete data and poor recall of medical history. This aspect highlights the importance of data regarding previous biliary surgery, available to us but potentially not available to other practitioners. The patient was operated (open surgery) in May 2003 for a complicated postbulbar ulcer: stenosis with gastric outlet obstruction; penetration in the common bile duct (CBD). Open surgery consisted of: troncular vagotomy, ½ distal gastric resection, Roux-en-Y gastroenterostomy. The duodenal papilla was in close vicinity (0.5-0.7 mm) to the transection line of the duodenum, so a Ch. 8 catheter was inserted in the CBD for its protection before closure of the duodenal stump with separate sutures; it was considered mandatory to prevent ampullary disconnection, transection of the confluence of the CBD and pancreatic ducts [
1]. Although total duodenal diversion (Roux-en-Y gastroenterostomy) provides a protective effect on duodenal stump leakage, external biliary drainage was added as a supplementary precaution. Cholecystostomy in a normal, acalculous GB, using a Ch. 24 Foley catheter, was used as a temporary biliary drainage for 13 days.
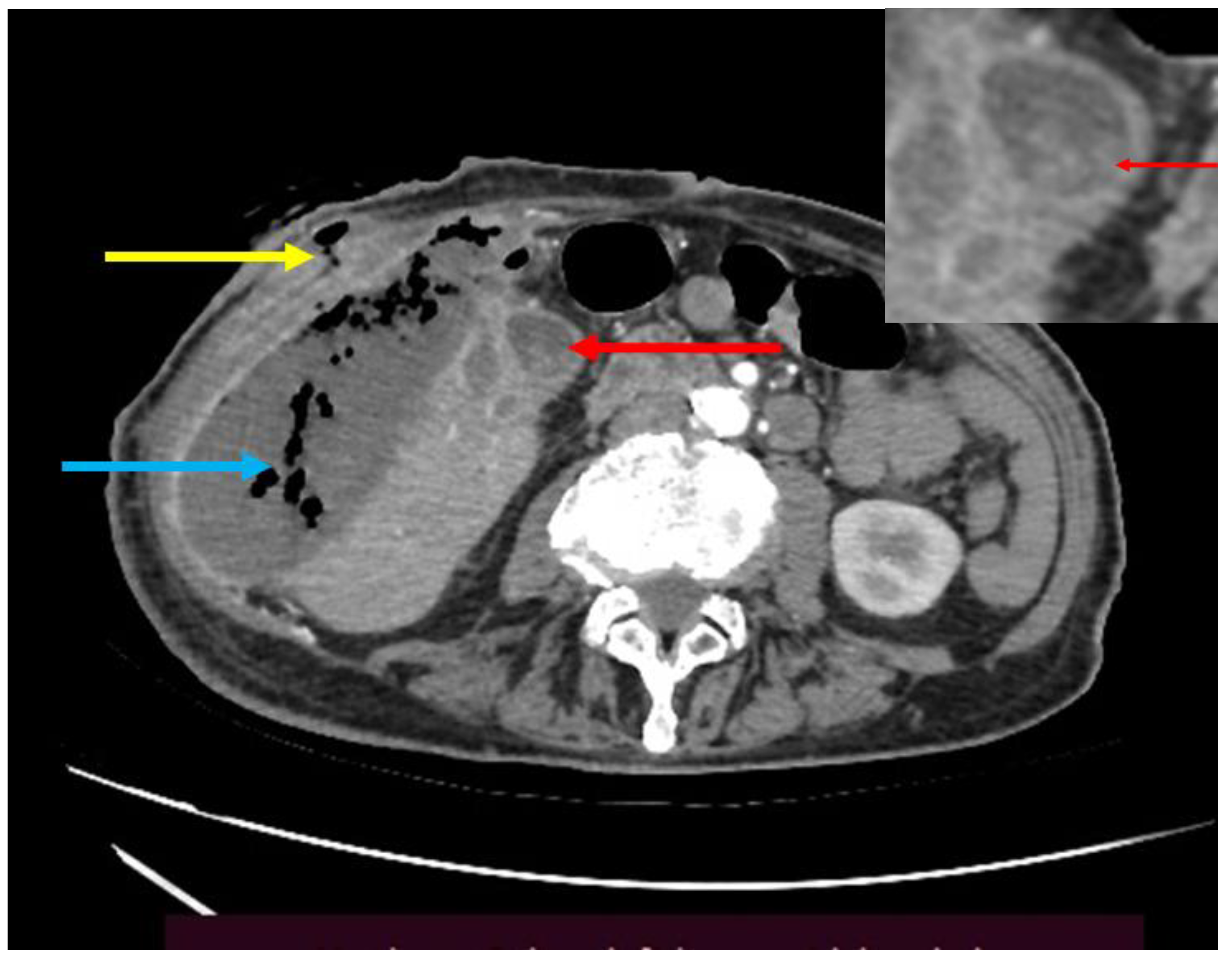
Computed tomography (CT) with IV and oral contrast offered further details (
Figure 1). A voluminous (70x130 mm), parafluid collection with multiple gas bubbles located in the right flank; a fistulous tract exteriorized to the skin with several extensions infiltrating the muscular abdominal wall and the subcutaneous soft tissues. The collection communicated with multiple microabscesses in the GB fossa and also with a structure that resembled a GB with thick walls (in close vicinity to a normal duodenal stump), containing multiple opaque calculi (maxim 12 mm in diameter) and a gaseous image. Dilated intrahepatic bile ducts with pneumobilia were encountered. It was concluded that the abscess was secondary to a calculous cholecystitis and originated in the GB fossa.
In the immediate post-admission period, the patient’s general status deteriorated, with arterial hypotension (BP 82/50 mmHg) and tachyarrhythmia (173 bpm), prompting urgent cardiological consultation. The patient was diagnosed with supraventricular tachycardia (SVT) and was successfully converted with intravenous beta-blocker administration. The patient underwent surgery 7 hours after admission, performed by the corresponding author. A transverse incision, centered on the cutaneous fistulous orifice, was followed by abundant discharge of fetid pus (> 500 mL), as well as multiple yellowish, frail calculi (3-5 mm), later on identified by the pathological report as cholesterol calculi. An extensive debridement was necessary for parietal tissues affected by cellulitis and necrotizing fasciitis, as well as for the removal of abdominal debris from the abscess cavity. A specimen resembling a gangrenous gallbladder tissue was extracted (
Figure 2). The abscess cavity was washed with hydrogen peroxide (H
2O
2) to dislodge small debris and irrigated with saline; two silicone tube drains were placed, one in the abscess cavity and the other in the subhepatic area. The abscess cavity was packed with a hemostatic (gauze) cotton mesh impregnated with Iodoform (triiodomethane, CHI
3 ).
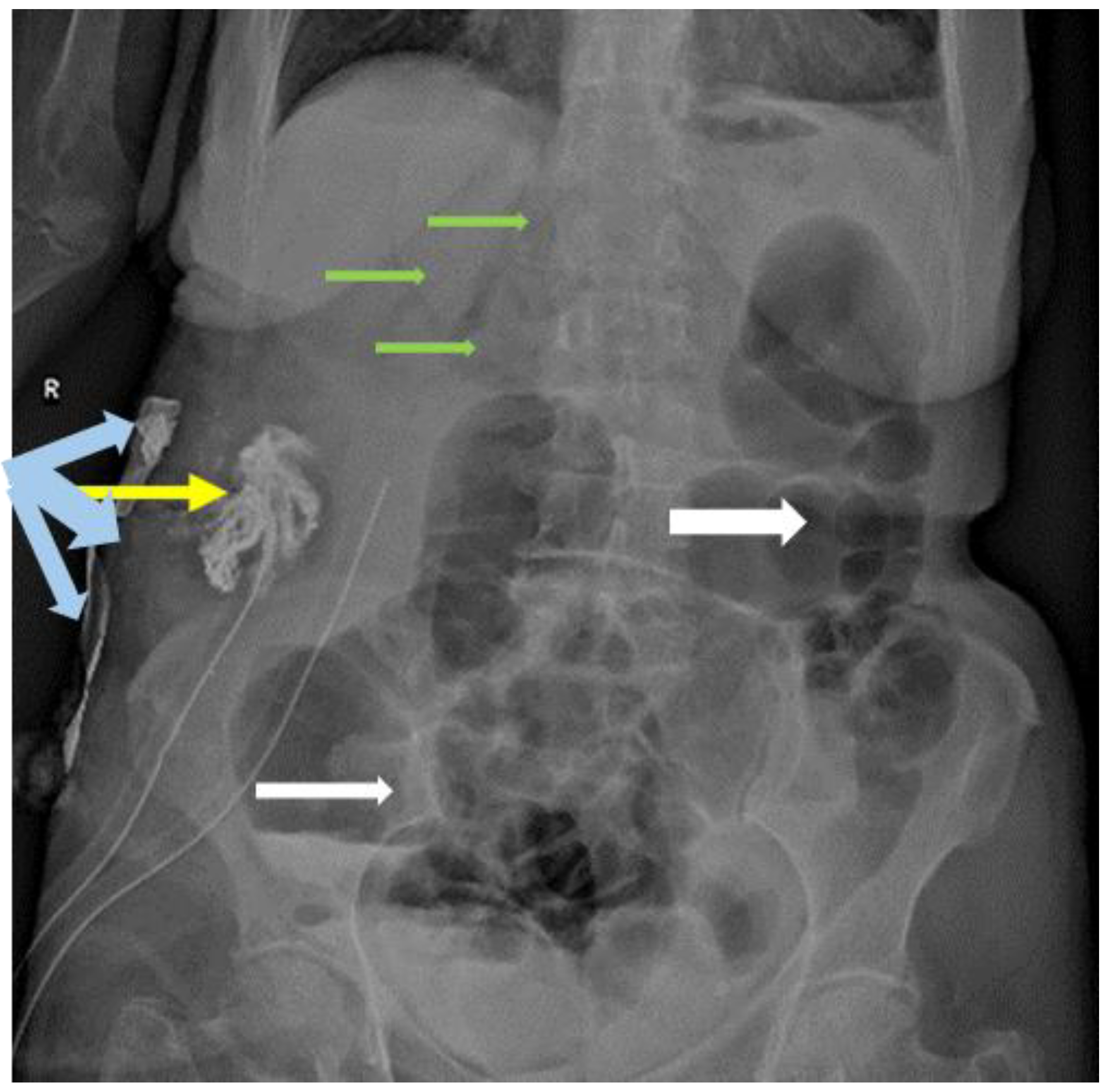
Abdominal X-ray with injection of water-soluble contrast through the abscess drain was used on postoperative day 3, to evaluate the size of the abscess cavity (
Figure 3); intrahepatic pneumobilia was still visible, without any evident communication with the CBD.
The abscess cavity was surgically inspected, and the mesh and the subhepatic drain were extracted. However, the following day, bile drainage (150 mL) appeared on the drain placed in the abscess cavity; it ceased spontaneously, so the drain was also removed on postoperative day 7. Minimal bile contamination of the dressing continued until day 12.
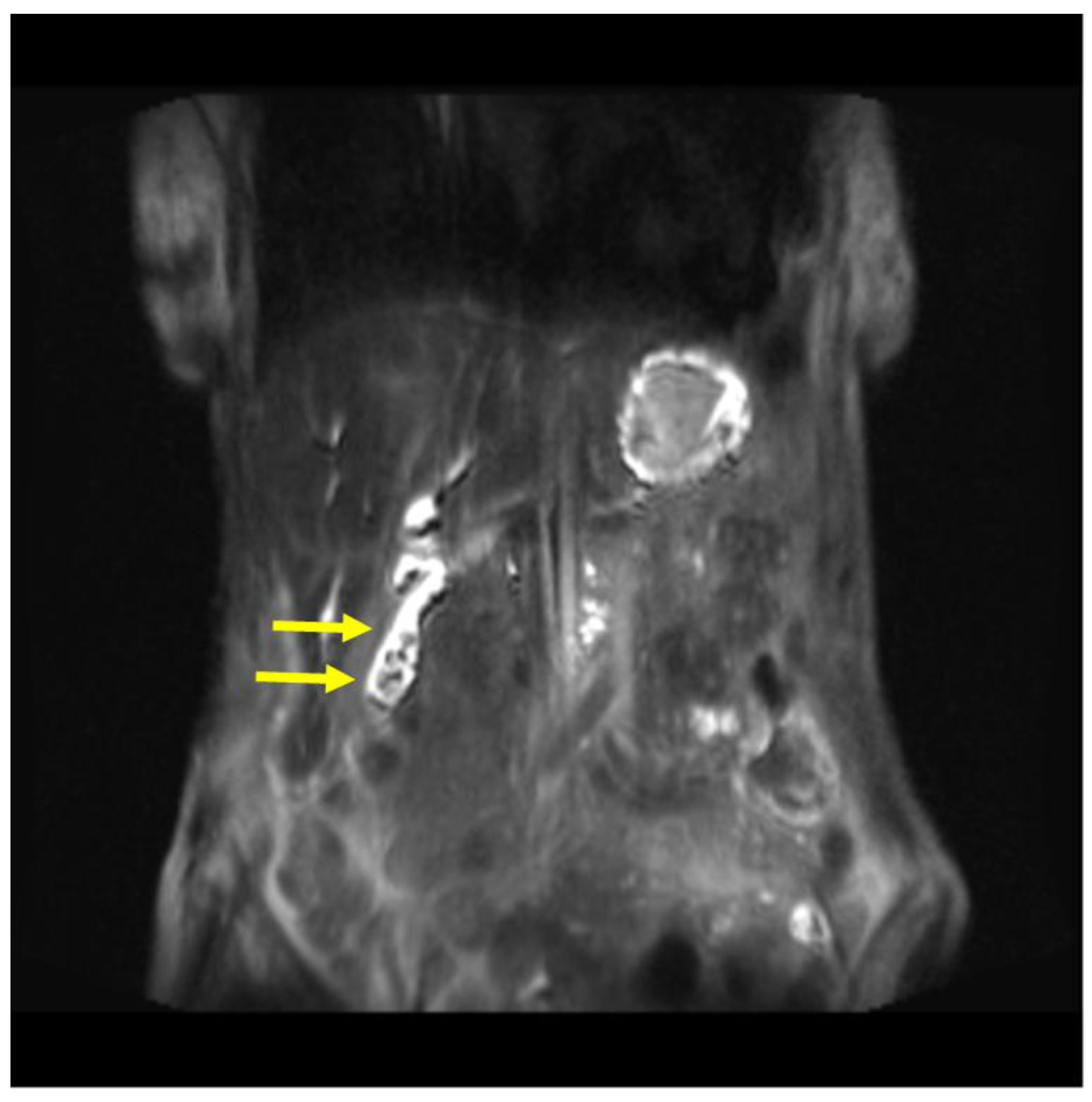
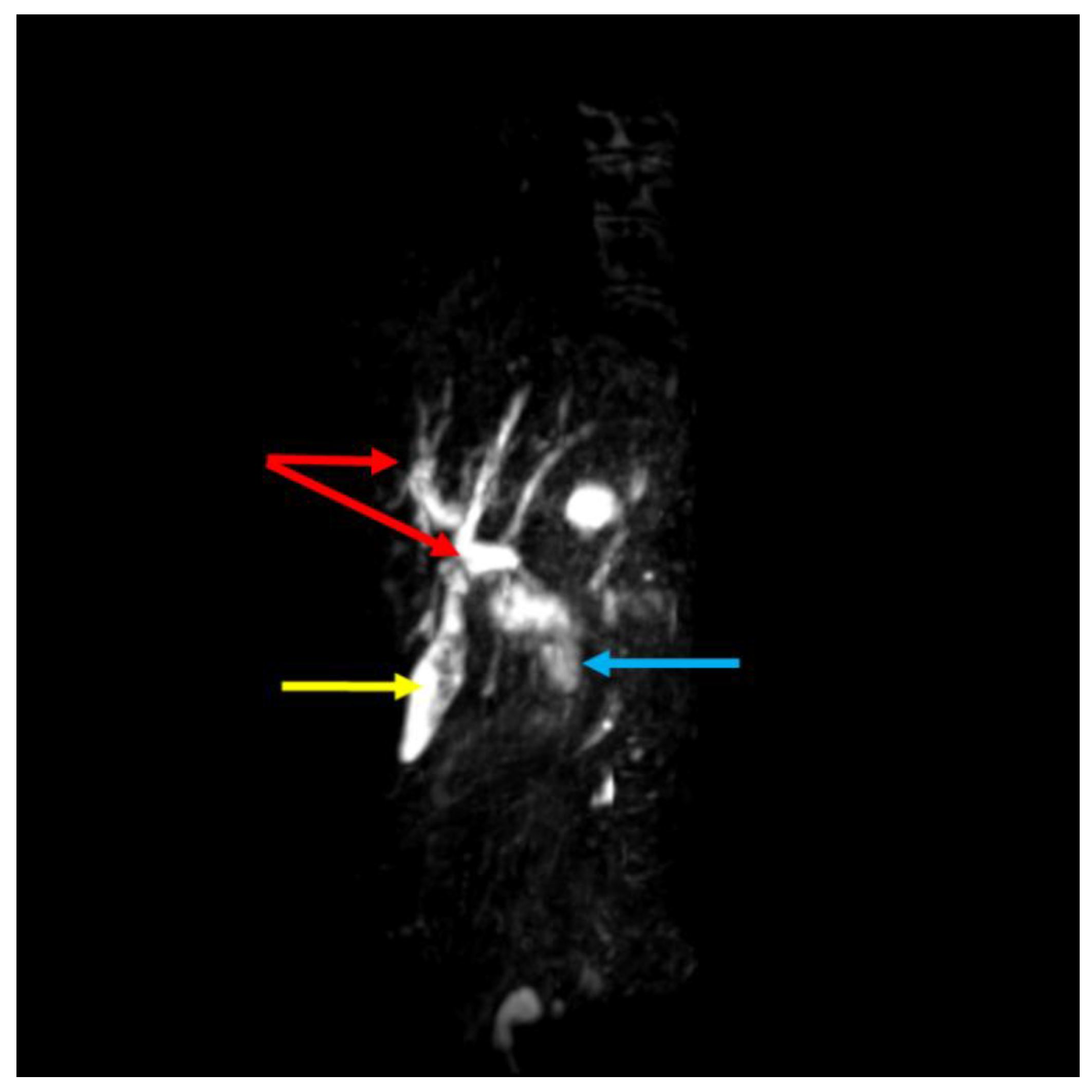
Magnetic resonance cholangiopancreatography (MRCP) on postoperative day 17 demonstrated the presence of a remnant gallbladder (GB) containing multiple calculi (
Figure 4,
Figure 5). In conclusion, debridement resulted in an inadvertent subtotal cholecystectomy. The patient was discharged on postoperative day 21 with a recommendation for completion cholecystectomy. She neglected this indication and, once again, was lost for follow-up for more than one year.
3. Discussion with Literature Review
3.1. Pathogenesis of Gallstone Formation Secondary to Temporary Cholecystostomy, Without Previous Gallbladder Disease, in the Context of Gastric Surgery
Except for highly selective vagotomy, all antiulcer procedures greatly disturb the pattern, the onset, and the rate of GB emptying; truncal vagotomy seems to disrupt vagally mediated preduodenal mechanism, resulting in delayed onset and reduced rate [
2]. Conversion of Billroth II to Roux-en-Y gastroenterostomy severely disturbs all parameters of the emptying of the gallbladder [
3]. Surgery for elective antiulcer procedures declined steadily in recent years. It is expected that the incidence of GS after gastric resection for duodenal ulcer (a benign pathology associated with a long survival) is higher than after gastrectomy for gastric cancer.
Diagnosis of early gastric cancer changed the prognosis; quality of life has gained importance due to the extended life expectancies. A study reported an 18.8% incidence of GS at 5 years after curative surgery for early gastric cancer (Billroth I, Billroth II, Roux-en-Y reconstruction) due to sectioning of the hepatic branch of the vagus nerve, which plays an important role in regulating GB tonicity, also to changes of endogenously released cholecystokinin (CCK), followed by changes in GB kinetics leading to bile stasis [
4]. Real-time US demonstrated a significantly reduced ejection fraction of GB in gastrectomized patients with/without vagotomy compared to healthy controls; thus, gastric surgery is a risk factor of GB dysmotility (biliary stasis), and subsequent GS formation [
5]. Total gastrectomy followed by Roux-en-Y reconstruction for gastric cancer leads to an increased risk of cholelithiasis, so that prophylactic cholecystectomy was suggested in patients without GS before surgery [
6]. One study reported a 25.7% incidence of GS formation after gastrectomy for gastric cancer (usually within two years, but in most cases asymptomatic); simultaneous prophylactic cholecystectomy was recommended in all patients with GS, and in those undergoing extended lymph-node dissection involving the hepatoduodenal ligament wich carries a high risk of damaging the hepatic branch of the vagus nerve resulting in reduced GB contractility [
7]. This study was based on a previous one [
8].
Another study reported a high incidence (32.02%) of GS (within two years) secondary to Roux-en-Y reconstruction in radical gastrectomy for gastric cancer: more often in total gastrectomy than distal gastrectomy because during a total gastrectomy, the vagal trunk is completely severed, resulting in the loss of hepatic branch function of the vagus nerve which plays a critical role in biliary function. Partial gastrectomy severed the vagus nerve to a lesser extent [
9]. Roux-en-Y in gastrectomy for gastric cancer is associated with a higher risk of GS formation compared to other types of gastrointestinal reconstruction [
9,
10]. This is a side-effect of total duodenal diversion (exclusion of duodenum during reconstruction, reduced CCK secretion; food passage through the duodenum serves as a stimulus for CCK secretion (a hormone responsible for contraction of the GB through the humoral regulation system), resulting in reduced GB contractility with increased risk of GS formation [
11]. Roux-en-Y is associated with a significantly higher incidence of clolecystolitiasis compared to Billroth I or II reconstruction [
12].
A
left-in-situ cholecystostomy (on a Foley catheter) for a prolonged period of 3 months can impair GB motility due to GB wall fibrosis [
13], predisposing to GS. GB contractility, calculated by US diameter measurement with provocation tests, is reduced to 62% [
14]. One study noted that after cholecystostomy in a previously normal GB, function will return to normal in most patients, despite adhesions impairing motility of the GB; if no GB disease develops within the first year after cholecystostomy, the risk of late complications (in the absence of GS) is minimal [
15]. However, this was an obsolete study based on only six cases.
Our study demonstrated that, in the long term, temporary cholecystostomy in a disease-free GB and gastric
surgery (troncular vagotomy; gastric resection/gastrectomy; total duodenal diversion - Roux-en-Y) may represent independent but synergistic factors responsible for the late
GS
formation
and secondary complications.
3.2. Emphysematous Cholecystitis
Neo-formation of GS was followed, 21 years later, by a peculiar form of acute calculous cholecystitis: emphysematous cholecystitis. This is an uncommon and severe form of acalculous or calculous gangrenous acute cholecystitis, associated with high mortality [
16]. The symptoms are nonspecific; the main characteristics are related to gas formation in the GB lumen, in the GB walls, the surrounding tissues, biliary ducts (pneumobilia), the abdominal cavity (pneumoperitoneum), and in the retroperitoneum, without any communication with the gastrointestinal tract [
16,
17,
18,
19,
20,
21]. Many studies demonstrated that translocation of gas-forming bacteria, especially anaerobes (such as
Escherichia coli, Klebsiella spp, Clostridium spp, Aerobacter aerogens, Salmonella spp), is implicated in etiology. Diagnosis is a challenging dilemma, and is presumed if the presence of gas is suspected using various imaging techniques, in the lumen or walls of the GB or adjacent structures (cavities). The amount of gas is also an important factor. An abdominal US may be inaccurate, so CT is considered more efficient due to higher sensitivity and specificity compared with other radiological modalities [
22]. A final diagnosis is demonstrated by bacterial culture examination, identifying anaerobic bacteria.
3.3. Cholecystostomy
Cholecystostomy (gallbladder drainage, gallbladder tube placement) is a reasonable alternative to cholecystectomy (open or laparoscopic) in acute calculous cholecystitis, mainly in elderly, high-surgical risk patients with significant comorbid conditions (critical illness or multiple medical comorbidities), who are not suitable for general anesthesia to undergo a complete cholecystectomy. It is a safe, effective, and temporary treatment of acute cholecystitis, allowing drainage of infected bile, decompression of the GB, and sepsis control. Today, surgical (open) cholecystostomy is considered obsolete; temporary decompression can be achieved using minimally invasive approaches (percutaneous or transhepatic) guided by US or CT, under local anesthesia.
Cholecystostomy may be curative in some cases of acalculous acute cholecystitis, but not for acute calculous cholecystitis because it may be associated with a high recurrence rate or complications related to retained GS or recurrent biliary disease. It is considered that retained GS are a nidus for sepsis. The interval for safe removal of the catheter and the necessity of interval (laparoscopic) cholecystectomy are variably reported [
23]. Catheter removal before 7 days may be associated with an increase in recurrent disease [
24]. Recurrent biliary events are common after percutaneous cholecystostomy for severe acute calculous cholecystitis, compared to interval (laparoscopic) cholecystectomy, so that the latter is indicated for patients fit for surgery after resolution of acute cholecystitis and sepsis; percutaneous cholecystostomy is a bridge to definitive management (cholecystectomy) [
25]. Retained GS in
left-in-situ cholecystostomy may be responsible for various complications, even gallstone ileus [
26]. Interval cholecystectomy is indicated after temporary cholecystostomy for acute calculous cholecystitis.
This may be a valid assertion, also related to our case report; late complications of neo-formed GS secondary to cholecystostomy (in a normal, acalculous GB) could have been prevented by cholecystectomy. Although cholecystostomy was not initially indicated for an acute cholecystitis, late complications and their prevention may overlap between the two conditions. We consider that continuous follow-up of a left-in situ GB after cholecystostomy (regardless of its initial indication) is mandatory; loss of follow-up and delayed diagnosis may lead to consecutive complications.
3.4. Cholecystocutaneous Fistula After Cholecystostomy
Spontaneous cholecystocutaneous fistula in the right hypochondrium after cholecystostomy for acute calculous cholecystitis (in the absence of definitive cholecystectomy) is a rare late complication that may occur months or even years later, sometimes associated with cellulitis, necrotizing fasciitis, and even sepsis [
27]. It may be preceded by an abdominal wall/cholecystocutaneous abscess [
28]. The pre-existing drain tract (the old drain tube tract is a point of least resistance) facilitates discharge through a cholecystocutaneous fistula and spontaneous passage (extrusion) of GS [
29], even years later [
30], including following cholecystostomy for acute emphysematous cholecystitis [
31].
In our case report, temporary cholecystostomy was not performed for acute calculous cholecystitis; rather, the fistula represented a late complication of neo-formed GS and acute emphysematous cholecystitis, following the same pattern through the pre-existing drain tract. One may conclude that, similar to the natural evolution of acute calculous cholecystitis, patients with a history of a left in-situ GB after cholecystostomy (in the absence of definitive cholecystectomy) are also prone to develop cholecystocutaneous fistula.
3.5. Incomplete, Partial/Subtotal Cholecystectomy
Today, laparoscopic cholecystectomy is the gold standard surgical procedure for definitive treatment of symptomatic GS. In selected cases, other techniques such as cholecystostomy or incomplete, subtotal/partial cholecystectomy may be recommended as the first step (as an exceptional definitive solution), mainly for acute severe cholecystitis. Similar to percutaneous cholecystolithotomy [
32], partial cholecystectomy should be considered a temporary option in severe acute calculous cholecystitis. Both techniques, in contrast to complete cholecystectomy, may be followed by symptoms related to residual or recurrent gallstones.
Partial cholecystectomy is indicated (as a bailout operation) in difficult laparoscopic cholecystectomy (“difficult gallbladder”) associated with poor visualisation of the hepatocystic or Calot’s triangle due to fibrosis, acute ductal inflamation or vascular variants, to prevent common bile duct (CBD) or vascular injury; it is considered a safe effective alternative surgical technique in difficult cholecystectomies, to decrease conversion to open cholecystectomy [
33]. A retrospective analysis and review [
34] suggested that laparoscopic subtotal cholecystectomy may offer advantages compared with open cholecystectomy in terms of immediate perioperative outcomes. Although subtotal laparoscopic cholecystectomy is less often associated with early complications
vs conversion to open surgery, long-term outcomes may differ and depend on surgical expertise [
35]. A systematic review and meta-analysis [
36] concluded that laparoscopic subtotal cholecystectomy is a reasonable alternative to laparoscopic cholecystectomy in acute cholecystitis. Although an incomplete operation, a systematic review [
37] concluded that laparoscopic subtotal cholecystectomy is an acceptable alternative for difficult gallbladders, in patients with a difficult Calot’s triangle; however it may be associated with a relative high incidence of morbidity and readmissions in the perioperative interval (90 days) [
38] and high-risk patients should be counseled to acknowledge this potential risk [
39].
A major concern in performing laparoscopic cholecystectomy is the avoidance of CBD injury, which is associated with considerable morbidity and even mortality [
40]. Principles of safe laparoscopic cholecystectomy were published by Gupta
et al [
41], including bailout techniques/strategies (such as cholecystostomy or subtotal cholecystectomy). Subtotal cholecystectomy may be performed laparoscopically; there are two major variants (types) to terminate the operation after clearance of GS and ablation of the remnant mucosa, depending on whether the biliary stump is closed or left open [
40,
42]. The fenestrating type leaves the posterior wall of the GB attached to the liver bed (the GB
fossa) exposed (left open), with/without closure of the cystic duct; the reconstituting type implies closure of the GB remnant (as small as possible) and/or the cystic duct. Accordingly, a literature review [
43] suggested using the terms subtotal open-tract
vs subtotal closed-tract in partial cholecystectomies. A classification based on four types was also published [
44]: Type A- the posterior wall of the GB is left attached to the liver bed, the GB stump is left open with placement of a drain; Type B- same as A with closure of the GB stump, with/without drain placement; Type C- resection of both anterior and posterior walls of the GB, stump closure without drain placement; Type D- same as C, but the stump is left open with drain placement.
Several studies and systematic reviews concerning safe laparoscopic techniques for subtotal cholecystectomy in difficult GB or acute cholecystitis, aimed at avoiding early or late complications (e.g., bile leakage, recurrent acute cholecystitis of the remnant GB, retained calculi), were published in recent years [
37,
38,
45,
46,
47,
48]. A systematic review and meta-analysis [
49] revealed that the fenestrating type prevents CBD injury but may be complicated by a higher rate of immediate bile leakage and the necessity of biliary decompression using endoscopic retrograde cholangiopancreatography (ERCP); in contrast, closure of the remnant GB creates a residual GB that may generate neoformation of calculi. Emergency laparoscopic cholecystectomy for acute cholecystitis during the acutely symptomatic phase of the index emergency admission is the best option when the cystic duct can be safely closed. Residual calculi in the GB remnant or cystic duct (whether closed or left open and drained) should be regarded as a bailout strategy and “suboptimal treatment”, not a definitive cholecystectomy, given the long-term risk of subsequent gallstones-related events [
50]. Therefore, there is a formal indication for a subsequent completion (redo) cholecystectomy for symptomatic GS and prevention of associated biliary complications after the index surgery.
The concept of the post-cholecytectomy syndrome is still ill-defined, with extrabiliary or biliary etiologies. The biliary etiology is usually associated with retained (residual) GS (in the cystic duct or the GB remnant) following an inadvertent incomplete cholecystectomy. It is possible after elective laparoscopic or open surgery, but is more frequent in an emergency setting, such as the reconstituting type of subtotal cholecystectomy for acute calculous cholecystitis. Mishaps (biliary complications) may occur at any time, even decades later [
51,
52,
53,
54,
55,
56]. Gallstones in the residual GB are associated with more complications than typical GS, due to diagnosis challenges and treatment delays [
57]. Despite a lack of standardized treatment guidelines, several studies dedicated to definitive (curative) surgical treatment concluded that laparoscopic completion cholecystectomy is feasible [
57,
58,
59,
60,
61,
62,
63,
64,
65]. According to the safety-first principle, the lowest morbidity is reported in centers with adequate experience in advanced laparoscopic procedures (skilled surgeons, experienced teams).
In our case report, debridement of the abscess cavity resulted in an inadvertent partial (incomplete) cholecystectomy for an acute calculous gangrenous (emphysematous) cholecystitis, with retained GS in the GB remnant. According to the current status, completion cholecystectomy was indicated; the patient was informed but neglected medical advice, once again, for more than one year (as well as the previous 21 years after the initial operation for postbulbar ulcer), and was lost for follow-up; the outcome is not known.
4. Conclusions and Further Directions
Cholecystostomy has been established as a temporary option in acute calculous cholecystitis for more than a century, but, like any interventional technique, it is associated with late side effects and complications. Late complications of temporary or left-in-situ cholecystostomy in patients with acute calculous cholecystitis are related to retained calculi and are ultimately resolved by cholecystectomy.
Temporary cholecystostomy in a disease-free (acalculous) gallbladder, associated with gastric surgery (troncular vagotomy; gastric resection/gastrectomy; total duodenal diversion, Roux-en-Y gastrojejunostomy), leads to gallbladder dysmotility and neoformation of gallstones. We report several late complications due to gallstones that occurred 21 years after open surgery for a complicated postbulbar ulcer: emphysematous cholecystitis; abdominal abscess in the right hypochondrium; cholecystocutaneous fistula; inadvertent subtotal cholecystectomy; a partial remnant gallbladder with retained calculi. To the best of our knowledge, this possibility was not reported before; there are several lessons to be learned.
The presence of clinically silent, undetected neo-formatted calculi after temporary cholecystostomy in an acalculous gallbladder may be overlooked because of a low index of suspicion, until the occurrence of late, potentially lethal, biliary complications; this may be a challenging diagnosis, especially in elderly patients with poor recall of biliary history and in the absence of medical documents.
Regular surveillance of a left-in-situ gallbladder after temporary cholecystostomy in a disease-free (acalculous) gallbladder is mandatory; loss of follow-up and delayed diagnosis may result in subsequent complications. The incidence of neo-formatted calculi appears higher than expected, compared with common gallstones.
Prophylactic cholecystectomy for asymptomatic neo-formatted gallstones is a reasonable choice; similarly, there is a clear indication for definitive/interval cholecystectomy after temporary cholecystostomy (for acute calculous cholecystitis) and for completion cholecystectomy after incomplete, partial/subtotal cholecystectomy (for cholelithiasis).
Author Contributions
I.N.M. and M.G. contributed equally to this study, read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical concerns, but are available from the corresponding author on reasonable request.
Acknowledgments
Publication of this paper was supported by the Carol Davila University of Medicine and Pharmacy, through the institutional program Publish not Perish. The authors sincerely appreciate all participants involved in the multidisciplinary treatment of these particular cases.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CT |
Computed tomography |
| GB |
Gallbladder |
| MRCP |
Magnetic resonance cholangiopancreatography |
| ERCP |
endoscopic retrograde cholangiopancreatography |
| GS |
Gallstone |
| CRP |
C-reactive protein |
| CBD |
common bile duct |
| Ch |
Charrier |
| IV |
intravenous |
| BP |
blood pressure |
| SVT |
supraventricular tachycardia |
| H2O2
|
oxygen hydroperoxide |
| CHI3
|
triiodomethane |
| RX |
radiography |
| CCK |
cholecystokinin |
| US |
ultrasonography |
References
- Ehrlich, E.W.; Howard, J.M. Ampullary disconnection during gastrectomy. Ann. Surg. 1969, 170, 961–968. [Google Scholar] [CrossRef]
- Pechlivanides, G.; Xynos, E.; Chrysos, E.; Tzovaras, G.; Fountos, A.; Vassilakis, J.S. Gallbladder emptying after antiulcer gastric surgery. Am. J. Surg. 1994, 168, 335–339. [Google Scholar] [CrossRef]
- Vassilakis, J.S.; Pechlivanides, G.; Fountos, A.; Zoras, O.J.; Xynos, E. Roux-en-Y gastroenterostomy severely disturbs emptying of the gallbladder. J. Am. Coll. Surg. 1994, 179, 313–317. [Google Scholar] [PubMed]
- Inoue, K.; Fuchigami, A.; Higashide, S.; Sumi, S.; Kogire, M.; Suzuki, T.; Tobe, T. Gallbladder sludge and stone formation in relation to contractile function after gastrectomy: A prospective study. Ann. Surg. 1992, 215, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hahm, J.; Park, J.; Cho, Y.; Eun, C.; Lee, Y.; Choi, H.; Yoon, B.; Lee, M.; Kee, C.; Park, K.; Lim, H.; Kwon, S. Changes in gallbladder motility in gastrectomized patients. Korean J. Intern. Med. 2000, 15, 1–6. [Google Scholar] [CrossRef]
- Pezzolla, F.; Lantone, G.; Guerra, V.; Misciagna, G.; Prete, F.; Giorgio, I.; Lorusso, D. Influence of the method of digestive tract reconstruction on gallstone development after total gastrectomy for gastric cancer. Am. J. Surg. 1993, 166, 6–10. [Google Scholar] [CrossRef]
- Fukagawa, T.; Katai, H.; Saka, M.; Morita, S.; Sano, T.; Sasako, M. Gallstone formation after gastric cancer surgery. J. Gastrointest. Surg. 2009, 13, 886–889. [Google Scholar] [CrossRef] [PubMed]
- Kodama, I.; Yoshida, C.; Kofuji, K.; Ohta, J.; Aoyagi, K.; Takeda, J. Gallstones and gallbladder disorder after gastrectomy for gastric cancer. Int. Surg. 1996, 81, 36–39. [Google Scholar] [PubMed]
- Zhang, B.; Nie, P.; Lin, Y.; Ma, Z.; Ma, G.; Wang, Y.; Ma, Y.; Zhao, J.; Zhang, J.; Yue, P.; et al. High incidence of gallstones after Roux-en-Y reconstruction gastrectomy in gastric cancer: A multicenter, long-term cohort study. Int. J. Surg. 2024, 110, 2253–2262. [Google Scholar] [CrossRef]
- Fujita, S.; Kimata, M.; Matsumoto, K.; Sasakura, Y.; Terauchi, T.; Furukawa, J.; Ogata, Y.; Kobayashi, K.; Shinozaki, H. Important risk factors for gallstones after laparoscopic gastrectomy: A retrospective study. BMC Surg. 2022, 22, 5. [Google Scholar] [CrossRef]
- Kobayashi, T.; Hisanaga, M.; Kanehiro, H.; Yamada, Y.; Ko, S.; Nakajima, Y. Analysis of risk factors for the development of gallstones after gastrectomy. Br. J. Surg. 2005, 92, 1399–1403. [Google Scholar] [CrossRef]
- Jun, K.H.; Kim, J.-H.; Kim, J.J.; Chin, H.M.; Park, S.M. Retrospective analysis of gallstone disease after gastrectomy for gastric cancer. Gastroenterol. Res. Pract. 2015, 2015, 827864. [Google Scholar] [CrossRef]
- Sinha, M.; Das, A. Effect of cholecystostomy on gallbladder motility. Gastroenterology 1995, 108, 1332. [Google Scholar] [CrossRef]
- Berger, H.; Leibl, A.; Kohz, P.; Briegel, T.; Pratschke, E. Results of long-term follow-up of patients with percutaneous cholecystostomy. Rofo 1993, 159, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Krom, R.A.; Pols, J.; Kingma, L.M.; Strake, L.T. Long-term effects of cholecystostomy on gallbladder function. Neth. J. Surg. 1984, 36, 121–123. [Google Scholar] [PubMed]
- Mentzer, R.M.; Golden, G.T.; Chandler, J.G.; Horsley, J.S. A comparative appraisal of emphysematous cholecystitis. Am. J. Surg. 1975, 129, 10–15. [Google Scholar] [CrossRef]
- Papavramidis, T.S.; Michalopoulos, A.; Papadopoulos, V.N.; Paramythiotis, D.; Karadimou, V.; Kokkinakis, H.; Fahantidis, E. Emphysematous cholecystitis: A case report. Cases J. 2008, 1, 73. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, H.; Shida, D.; Matsunaga, H.; Takahama, Y.; Miyamoto, S. Emphysematous cholecystitis with massive gas in the abdominal cavity. World J. Gastroenterol. 2013, 19, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Zeebregts, C.J.; Wijffels, R.T.; de Jong, K.P.; Peeters, P.M.; Slooff, M.J. Percutaneous drainage of emphysematous cholecystitis associated with pneumoperitoneum. Hepatogastroenterology 1999, 46, 771–774. [Google Scholar] [PubMed]
- Yagi, Y.; Sasaki, S.; Terada, I.; Yoshikawa, A.; Fukushima, W.; Kitagawa, H.; Fujimura, T.; Izumi, R.; Saito, K. Massive pneumoretroperitoneum arising from emphysematous cholecystitis: A case report and literature review. BMC Gastroenterol. 2015, 15, 114. [Google Scholar] [CrossRef]
- Delgado-Plasencia, L.; Gonzalez-Garcia, I.; Rodriguez-Gonzalez, D.; Torres-Monzon, A.E. Pneumomediastinum as a complication of emphysematous cholecystitis: Case report. BMC Gastroenterol. 2010, 10, 99. [Google Scholar] [CrossRef]
- McMillin, K. Computed tomography of emphysematous cholecystitis. J. Comput. Assist. Tomogr. 1985, 9, 330–332. [Google Scholar] [CrossRef]
- Er, S.; Berkem, H.; Ozden, S.; Birben, B.; Cetinkaya, E.; Tez, M.; Yuksel, B.C. Clinical course of percutaneous cholecystostomies: A cross-sectional study. World J. Clin. Cases 2020, 8, 1033–1041. [Google Scholar] [CrossRef]
- Di Martino, M.; Miguel Mesa, D.; Lopesino Gonzalez, J.M.; de la Hoz Rodriguez, A.; Martin-Perez, E. Safety of percutaneous cholecystostomy early removal: A retrospective cohort study. Surg. Laparosc. Endosc. Percutan. Tech. 2020, 30, 410–415. [Google Scholar] [CrossRef]
- Ragathaa, R.; Khalil, I.; Jones, R.; Manzelli, A.; Reece-Smith, A.; Oub, Y.; Wajed, S.; Di Mauro, D. Clinical evolution of gallstones following percutaneous cholecystostomy in patients with severe acute calculous cholecystitis: A single-center analysis of 102 cases. Ann. Gastroenterol. 2024, 37, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Siriwardana, P.N.; Weerasekara, D.; De Silva, M. Cholecystostomy does not prevent gallstone ileus: A case report. Cases J. 2009, 2, 6790. [Google Scholar] [CrossRef]
- Kasper, P.; Kaminiorz, J.; Schramm, C.; Goeser, T. Spontaneous cholecystocutaneous fistula: An uncommon complication of acute cholecystitis. BMJ Case Rep. 2020, 13, e238063. [Google Scholar] [CrossRef]
- Lofgren, D.H.; Vasani, S.; Singzon, V. Abdominal wall abscess secondary to cholecystocutaneous fistula via percutaneous cholecystostomy tract. Cureus 2019, 11, e4444. [Google Scholar] [CrossRef] [PubMed]
- Pripotnev, S.; Petrakos, A. Cholecystocutaneous fistula after percutaneous gallbladder drainage. Case Rep. Gastroenterol. 2014, 8, 119–122. [Google Scholar] [CrossRef]
- Gerrard, A.; Date, R. Delayed spontaneous passage of gallstones via cholecystocutaneous fistula. ACG Case Rep. J. 2017, 4, e102. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, M.; Goh, B.; Strauss, P.; Nyandowe, M. Spontaneous expulsion of a gallstone from a cholecystocutaneous fistula following percutaneous cholecystostomy. Cureus 2025, 17, e79282. [Google Scholar] [CrossRef]
- Donald, J.J.; Cheslyn-Curtis, S.; Gillams, A.R.; Russell, R.C.G.; Lees, W.R. Percutaneous cholecystolithotomy: Is gallstone recurrence inevitable? Gut 1994, 35, 692–695. [Google Scholar] [CrossRef]
- Kulen, F.; Tihan, D.; Duman, U.; Bayam, E.; Zaim, G. Laparoscopic partial cholecystectomy: A safe and effective alternative technique in difficult cholecystectomies. Ulus. Cerrahi Derg. 2016, 32, 185–190. [Google Scholar] [CrossRef]
- Aloraini, A.; Alburakan, A.; Alhelal, F.S.; Alabdi, G.; Elmutawi, H.; Alzahrani, N.S.; Alkhalife, S.; Alanezi, T. Subtotal vs. open cholecystectomy as a bailout procedure for difficult gallbladders: A retrospective tertiary care experience. Medicina 2024, 60, 1642. [Google Scholar] [CrossRef]
- Ramirez Giraldo, C.; Monroy, D.C.; Isaza Restrepo, A.; Ayala, D.; Gonzalez Tamayo, J.; Vargas Patino, A.M.; Trujillo Guerrero, L.; Van Londono, I.; Rojas Lopez, S. Subtotal laparoscopic cholecystectomy versus conversion to open as a bailout procedure: A cohort study. Surg. Endosc. 2024, 38, 4965–4975. [Google Scholar] [CrossRef] [PubMed]
- Koo, S.J.; Krishnan, R.J.; Ishikawa, K.; Matsunaga, M.; Ahn, H.J.; Murayama, K.M.; Kitamura, R.K. Subtotal vs. total cholecystectomy for difficult gallbladders: A systematic review and meta-analysis. Am. J. Surg. 2024, 229, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Al-Azzawi, M.; Abouelazayem, M.; Parmar, C.; Singhal, R.; Amr, B.; Martinino, A.; Atici, S.D.; Mahawar, K. Laparoscopic subtotal cholecystectomy for difficult gallbladders: A lifesaving bailout or an incomplete operation? A systematic review. Ann. R. Coll. Surg. Engl. 2024, 106, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.; Abdalkoddus, M.; Mahendran, B.; Mownah, O.A.; Nawara, H.; Aroori, S. Subtotal cholecystectomy: Is it a safe option for difficult gallbladders? Ann. R. Coll. Surg. Engl. 2023, 105, 455–460. [Google Scholar] [CrossRef]
- Lucocq, J.; Hamilton, D.; Scollay, J.; Patil, P. Subtotal cholecystectomy results in high perioperative morbidity: Risk profile should be emphasized during consent. World J. Surg. 2022, 46, 2955–2962. [Google Scholar] [CrossRef]
- Strasberg, S.M.; Pucci, M.J.; Brunt, L.M.; Deziel, D.J. Subtotal cholecystectomy: Fenestrating vs. reconstituting subtypes and prevention of bile duct injury. J. Am. Coll. Surg. 2016, 222, 89–96. [Google Scholar] [CrossRef]
- Gupta, V.; Jain, G. Safe laparoscopic cholecystectomy: Adoption of universal culture of safety. World J. Gastrointest. Surg. 2019, 11, 62–84. [Google Scholar] [CrossRef] [PubMed]
- Elshaer, M.; Gravante, G.; Thomas, K.; Sorge, R.; Al-Hamali, S.; Ebdewi, H. Subtotal cholecystectomy for difficult gallbladders: Systematic review and meta-analysis. JAMA Surg. 2015, 150, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Lunevicius, R. Review of the literature on partial resections of the gallbladder, 1898–2022: Outline of the conception of subtotal cholecystectomy and proposed terminology. Clin. Med. 2023, 12, 1230. [Google Scholar] [CrossRef]
- Henneman, D.; da Costa, D.W.; Vrouenraets, B.; van Wagensveld, B.A.; Lagarde, J.M. Laparoscopic partial cholecystectomy for the difficult gallbladder: A systematic review. Surg. Endosc. 2013, 27, 351–358. [Google Scholar] [CrossRef]
- Toro, A.; Teodoro, M.; Khan, M.; Schembari, E.; Di Saverio, S.; Catena, F.; Di Carlo, I. Subtotal cholecystectomy for difficult acute cholecystitis: How to finalize safely by laparoscopy—A systematic review. World J. Emerg. Surg. 2021, 16, 45. [Google Scholar] [CrossRef]
- Ramirez-Giraldo, C.; Torres-Cuellar, A.; Van-Londono, I. State of the art in subtotal cholecystectomy: An overview. Front. Surg. 2023, 10, 1142579. [Google Scholar] [CrossRef]
- Haldeniya, K.; Krishna, S.R.; Raghavendra, A.; Singh, P.K. Laparoscopic subtotal cholecystectomy in difficult gallbladder: Experience from a tertiary care center. Ann. Hepatobiliary Pancreat. Surg. 2024, 28, 214–219. [Google Scholar] [CrossRef]
- Abdallah, H.S.; Sedky, M.H.; Sedky, Z.H. The difficult laparoscopic cholecystectomy: A narrative review. BMC Surg. 2025, 25, 156. [Google Scholar] [CrossRef]
- Ravendran, K.; Elmoraly, A.; Thomas, C.S.; Job, M.L.; Vahab, A.A.; Khanom, S.; Kam, C. Fenestrating versus reconstituting subtotal cholecystectomy: Meta-analysis of bile leak, bile duct injury, and outcomes. Cureus 2024, 16, e72769. [Google Scholar] [CrossRef]
- Tebala, G.D.; Shabana, A.; Patel, M.; Samra, B.; Chetwynd, A.; Nixon, M.; Pradhan, S.; Elhag, B.; Mok, G.; Mighiu, A.; Antunes, D.; Slack, Z.; Cirocchi, R.; Bond-Smith, G. Prognostic factors and predictive models in hot gallbladder surgery: A prospective observational study. Ann. Hepatobiliary Pancreat. Surg. 2024, 28, 203–213. [Google Scholar] [CrossRef]
- Calhoun, S.K.; Piechowiak, R.L. Recurrent cholecystitis and cholelithiasis in a gallbladder remnant 14 years after converted cholecystectomy. Radiol. Case Rep. 2015, 5, 332. [Google Scholar] [CrossRef]
- Sahoo, M.R.; Kumar, A. Stump stone six years after cholecystectomy: A possibility. BMJ Case Rep. 2013, 2013, bcr2012007957. [Google Scholar] [CrossRef]
- Maynard, W.; McGlone, E.M.; Deguara, J. Unusual etiology of abdominal wall abscess: Cholecystocutaneous fistula presenting 20 years after open subtotal cholecystectomy. BMJ Case Rep. 2016, 2016, bcr2015213326. [Google Scholar] [CrossRef] [PubMed]
- Zahedian, A.; Ahangar, S.K.; Asghari, Y. Post-cholecystectomy syndrome requiring redo laparoscopic completion surgery: A case report. Int. J. Surg. Case Rep. 2018, 42, 145–147. [Google Scholar] [CrossRef]
- Hmida, W.B.; Jerraya, H.; Nasseh, S.; Haloui, N.; Khalfallah, M.; Nouira, R. Complications of subtotal cholecystectomy: A case report. Int. J. Surg. Case Rep. 2021, 83, 105950. [Google Scholar] [CrossRef]
- Mateja, H.L.; Rowe, D.A.; Tsai, A.; Giuseppucci, P. Remnant cholecystitis after subtotal cholecystectomy: A case report. Cureus 2024, 16, e71719. [Google Scholar] [CrossRef]
- Gadiyaram, S.; Nachiappan, M. The second “gallbladder operation”. J. Minim. Access Surg. 2022, 18, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Kar, A.; Gulati, S.; Mohammed, S.; Valappil, M.V.; Sarala, B.B.; Ghatak, S.; Bhattacharyya, A. Surgical management of cystic duct stump stone or gallbladder remnant stone. Indian J. Surg. 2018, 80, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kapoor, A.; Singh, R.K.; Prakash, A.; Behari, A.; Kumar, A.; Kapoor, V.K.; Saxena, R. Management of residual gallbladder: A 15-year experience at a tertiary center. Ann. Hepatobiliary Pancreat. Surg. 2018, 22, 36–41. [Google Scholar] [CrossRef]
- Gupta, V.; Sharma, A.K.; Kumar, P.; Gupta, M.; Gulati, A.; Sinha, S.K.; Kochhar, R. Residual gallbladder: An emerging disease after safe cholecystectomy. Ann. Hepatobiliary Pancreat. Surg. 2019, 23, 353–358. [Google Scholar] [CrossRef]
- Grossman, J.G.; Johnston, W.R.; Fowler, K.J.; Williams, G.A.; Hammill, C.W.; Hawkins, W.G. The symptomatic gallbladder remnant: A diagnosis reconsidered. J. Hepatobiliary Pancreat. Sci. 2019, 26, 137–143. [Google Scholar] [CrossRef]
- Cawich, S.O.; Mohanty, S.K.; Bonadie, K.; Simpson, L.; Ramnarace, R.; Fa Si Oen, P.; Singh, Y.; Naraynsingh, V.; Francis, W. Laparoscopic completion cholecystectomy: Audit from the AHPBA Caribbean Chapter. Cureus 2020, 12, e11126. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Kurian, N.; Singh, R.K.; Chidipotu, V.R.; Kumar, S.; Raj, A.K.; Mandal, M. Surgical management of cystic duct stump calculi causing post-cholecystectomy syndrome: A prospective study. J. Minim. Access Surg. 2023, 19, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Nafea, M.A.; Elshafey, M.H.; Hegab, A.; Seleem, A.; Rafat, W.; Khairy, M.; Elaskary, H.; Mohamed, Y.M.; Monazea, K.; Salem, A. Open versus laparoscopic completion cholecystectomy after prior open partial cholecystectomy: A retrospective study. Ann. Med. Surg. 2024, 86, 5688–5695. [Google Scholar] [CrossRef]
- Mohtashami, A.; Ziaziaris, W.A.; Lim, C.S.H.; Bhimani, N.; Leibman, S.; Hugh, T.J. Surgical options for retained gallstones after cholecystectomy. Surg. Laparosc. Endosc. Percutan. Tech. 2024, 34, 625–629. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).