
Submitted:
12 December 2025
Posted:
15 December 2025
You are already at the latest version
Abstract
Objectives: Retrograde menstruation occurs in most women and could cause some peri-toneal irritation. The peritoneal cavity is a cavity outside the bloodstream, with a specific hormonal, immunological and microbiological micro-environment distinct from plasma. The mesothelial cells lining the peritoneal cavity react within seconds to minor trauma, such as blood, with retraction, causing acute inflammation and later inflammation. This mesothelial cell retraction exposes the basal membrane and facilitates implantation of tu-mour cells. The acute inflammation enhances adhesion formation after surgery, and causes pain. Design: A systematic review of menstrual C-reactive protein (CRP) concentrations, a non-specific marker of peritoneal inflammation (PROSPERO ID 536306). Results: All articles (n=8) showed a variable increase in CRP concentrations during the men-strual and early follicular phase of 80±36%. Conclusions: CRP concentrations are slightly increased during menstruation and the early follicular phase. This increase is likely due to retrograde menstruation, causing mesothelial cell retraction and acute pelvic inflamma-tion. It seems logical that the mesothelial cell retraction facilitates endometrial cell im-plantation and explains the anatomical distribution of endometriosis lesions. Acute pelvic inflammation may enhance postoperative adhesion formation.
Keywords:
dysmenorrhoea
; CRP
; postoperative adhesions
; acute inflammation
; retrograde menstruation
; endometriosis
1. Introduction
Retrograde menstruation occurs in most women [1], as recently reviewed. In the peritoneal fluid of women without and with endometriosis, endometrial cells were found in 54% and 75%, respectively [1], and peritoneal fluid is blood-stained in over 90% [2]. Retrograde menstruation, which contains viable endometrial cells with DNA similar to that of the endometrium [3], has been considered to support the implantation theory of endometriosis [3]. Also, dysmenorrhoea was suggested to be caused by retrograde menstruation and peritoneal inflammation [4]. Unfortunately, the volume of retrograde menstruation in individual women is unknown since difficult to measure, and it remains debated whether a more abundant menstruation, likely associated with more retrograde menstruation, increases the risk of endometriosis.
C-reactive protein (CRP) is an acute-phase protein secreted by the liver following interleukin-6 secretion by macrophages and T cells, signalling inflammation or tissue damage. It is a non-specific inflammation biomarker in many diseases, including cardiovascular, respiratory, gastrointestinal, musculoskeletal, neurological, autoimmune, and infectious diseases. Following gynaecologic or abdominal surgery, the increase in CRP concentrations is proportional to the severity of surgery, and CRP concentrations are used as a biomarker for postoperative complications associated with peritoneal inflammation [5,6,7].
The peritoneal cavity is a cavity outside the bloodstream, similar to the mouth, and is lined by the large and flat mesothelial cells of the peritoneum. The peritoneal cavity is a specific microenvironment, with the lining mesothelial cells actively regulating the transport of liquids, electrolytes, proteins, gases, and cells between plasma and peritoneal fluid [8]. In women without ovarian activity, transudation of peritoneal fluid is minimal. In ovulatory women, the peritoneal fluid volume increases exponentially during the follicular phase and remains high during the luteal phase by exudation from the growing follicle or the corpus luteum. This ovarian exudation explains that the estrogen and progesterone concentrations are much higher in peritoneal fluid than in plasma, with an acute increase after ovulation, by the release of the follicular content into the peritoneal cavity. The peritoneal cavity thus is a specific microenvironment with higher estrogen and progesterone concentrations than in plasma [9]. Also, the immunology is different [10], with distinct microbiota from the genital tract and the bowel, and a low grade inflammation in women with endometriosis [11,12,13,14,15,16,17,18].
The mesothelial cells lining the peritoneal cavity respond within seconds (Figure 1) to minor trauma by retracting and bulging of cells, thereby exposing the basal membrane between cells [19,20,21]. The retraction of mesothelial cells facilitates the implantation of cells, such as tumour cells [22], and is associated with acute inflammation [23], the body’s initial response to harmful stimuli, characterised by increased transudation of many substances from plasma and diapedesis of white blood cells [24]. Acute inflammation triggers the liver secretion of CRP , increasing after 6 hours. Acute inflammation of the peritoneal cavity also releases substances into the peritoneal fluid, which enhance adhesion formation between surgical lesions [8]. A surgical lesion starts a cascade of events to repair the mesothelial defect. If the mesothelial repair has not been completed by day 3, the fibroblasts start growing and form adhesions using any remaining fibrin as a scaffold [8]. Adhesion formation thus results from a slower repair because of infection, necrotic tissue, or suture material. However, quantitatively equally important for adhesion formation is the severity of the acute inflammation of the entire peritoneal cavity, which is always associated with surgery since caused by minor trauma such as the insufflation pressure [25], duration of mesothelial hypoxia by CO2 pneumoperitoneum, oxidative stress of open surgery, desiccation, irrigation liquids such as saline [26], surgical manipulation of tissues, or blood [27]. Blood is highly irritative, causing mesothelial cell retraction, pain and adhesion formation, and in a mouse model, as little as 0.125 mL of blood or plasma strongly increases adhesion formation [27].
Considering that retrograde menstruation occurs in most women [28], that minimal amounts of blood are highly irritative, causing mesothelial cell retraction and acute inflammation [27], that retrograde menstruation also contains microbiota from the upper genital tract, and that CRP secretion is a marker for acute inflammation and inflammation, we reviewed CRP concentrations during menstruation and the early follicular phase.
2. Materials and Methods
2.1. The Systematic Review
The PubMed database was searched for studies on menstrual and early follicular CRP concentrations or peritoneal inflammation. This systematic review was registered in PROSPERO (ID 536306), and PRISMA guidelines for a systematic review were followed [29]. Articles in English, Spanish or Italian published before November 24 2025, were considered. Exclusion criteria were any interfering diseases or surgery. The first search (menstruation OR menses) AND inflammation AND (C-reactive protein OR CRP) found 50 articles. The second search (menstruation OR menses) AND (postoperative adhesions) found 101 articles. Since only eight articles were found by searching manually (MMB and PRK ) the titles and abstracts for data on menstrual and early follicular CRP concentrations, an additional search was performed with (menstruation OR menses[Title/Abstract]) AND (inflammation OR C-reactive protein OR CRP[Title/Abstract]) AND human, but no additional data were found in these 988 articles.
Only 8 articles were found reporting menstrual CRP concentrations. The aim of the articles was heterogeneous and menstrual CRP concentrations were never the focus of the investigation. Therefore, although being complete, this review is not a systematic review permitting a meta-analysis and prisma guidelines to “appraise, and synthesize all available evidence using transparent, predefined rules to minimize bias and ensure reliability”. Most articles reported medians and interquartile ranges; two articles (Table 1) reported the means and SDs. The logarithmic distribution of plasma hormone concentrations [30,31,32] was never considered. One article with serial CRP measurements during the cycle only listed the percentage change compared to the mean CRP concentration [33]. In one article, data had to be extracted from the figure. Therefore, we focused on increases in CRP concentrations during menstruation rather than absolute concentrations.
2.2. Statistics
The retrieved data from the eight selected articles are listed in Table 1. The menstrual increase of CRP concentrations was calculated by dividing the menstrual early follicular concentrations (mean or median) by the respective late follicular or luteal phase concentrations.
3. Results
3.1. Menstruation and CRP
During menstruation and the early follicular phase, CRP concentrations consistently increase and almost double (Table 1 and Figure 2). This observation received little attention, as menstrual inflammation was never the primary aim of these publications. Blum et al. [33] focused on the relationship of CRP with obesity and insulin resistance. Puder et al. described the correlation between menstrual psychological and physical symptoms and CRP concentrations [40]. Wander et al. [39] focused on changes in a group of hormones and CRP concentrations during the entire menstrual cycle. Gaskins et al. [38] is the largest series showing median and interquartile ranges of CRP and other hormones during the menstrual cycle. The increased CRP concentrations in the early follicular phase were subsequently confirmed by Gursoy et al. [37], Chiareti et al. [36], Talebpour et al. [34] and Yama et al. [35], the latter focusing on premenstrual syndrome (PMS).
3.2. Menstruation, Inflammation and Adhesion Formation
No data were found describing the volume of retrograde menstruation. Therefore, there are no data demonstrating that the volume of retrograde menstruation is related to the menstrual increase in CRP concentrations.
No data were found, indicating that the menstrual increase in CRP concentrations might be associated with postoperative adhesion formation as suggested by indirect evidence [41]. Hellebrekers et al. demonstrated in patients undergoing abdominal myomectomy that, at second-look laparoscopy, CRP concentrations correlated with the incidence of adhesions, and the total amount of adhesions in the pelvis and to the uterus [41].
3.3. Logarithmic Distribution of CRP Concentrations
The logarithmic distribution of CRP concentrations can be concluded from the medians and quartile ranges and from means minus 3 SDs being below zero (Table 1).
4. Discussion
The menstrual increase in CRP concentrations is consistently reported across publications (Figure 1): CRP concentrations almost double, except in one study, which reported only a 33% increase [35]. Remarkably, this clear increase in menstrual CRP concentrations has received little attention, probably explained by these publications focusing on menstrual symptoms such as psychology, dysmenorrhea, cardiovascular accidents, premenstrual syndrome, polycystic ovarian syndrome (PCOS) and metabolic syndrome.
The increased CRP concentrations during menstruation and in the early luteal phase are likely caused by retrograde menstruation, since it is unlikely that blood from retrograde menstruation would not cause mesothelial cell retraction and acute inflammation in the pelvis (Figure 1), given the sensitivity of mesothelial cells to minor amounts of blood, as demonstrated in mice [27]. Since the increase in CRP concentrations persists during the early follicular phase, the uterine inflammation during menstruation [42,43] seems a less likely explanation. Unfortunately, no data describe the absence of increases in menstrual CRP concentrations in women with occluded tubes. The hypothesis that retrograde menstruation triggers mesothelial cell retraction, acute inflammation and elevated CRP concentrations is clinically important. First, the severity of the inflammatory reaction will vary with the amount of retrograde menstruation, and the consequences will be individually variable. Second, this hypothesis sheds new light on our understanding of the pathophysiology of endometriosis. Mesothelial cell retraction, exposing the basal membrane, will facilitate the implantation of endometrial cells or fragments, as demonstrated by the increased tumour cell implantation [22]. This facilitated implantation of endometrial cells is consistent with clinical observations, such as the widely held belief that women with endometriosis have more abundant menstruation, with a higher probability of having more retrograde menstruation and more pelvic pain. The hypothesis of retrograde menstruation, mesothelial cell retraction facilitating implantation, is also consistent with the anatomical localisation of endometriosis lesions, which are more frequent on the left side in the pelvis and on the right side of the diaphragm since peritoneal fluid circulates [44] clockwise from the pouch of Douglas over the right gutter to the right diaphragm. The lower recurrence rate of endometriosis after surgery in women taking medical therapy might be explained by the lower menstrual volume or absence of menstruation. We can only speculate to what extent the severity of dysmenorrhoea might reflect the volume of retrograde menstruation and the acute inflammation, at least in some women [45].
It is unclear whether the mildly elevated CRP concentration, reflecting retrograde menstruation and mild acute inflammation, could be a cofactor in adhesion formation after surgery. This seems unlikely since surgery itself will cause a much more important acute inflammation of the peritoneal cavity by exposing the mesothelial cells to CO2 or to the oxidative stress of air and surgical manipulation. However, in mice, mild manipulation of the bowels in the upper abdomen enhances adhesion formation between opposing lesions in the lower abdomen [46].
Microbiota from the uterine cavity and upper genital tract may contribute to peritoneal inflammation caused by retrograde menstruation, as women with endometritis foci have more postoperative adhesions [47]. Similarly, an association with vaginal infections or vaginoses [38], as suggested for endometriosis, cannot be excluded [11]. Women with foci of endometritis have more postoperative adhesions without clinical symptoms of pelvic infection [47]. Indirect evidence thus suggests a relationship between the upper genital tract microbiome and the peritoneal inflammatory reaction.
The clinical consequences of mildly elevated CRP levels during menstruation are unclear. The clinician could consider the mild average increase in the average woman as clinically irrelevant. However, it might be wise to consider measuring CRP concentrations in women with abundant menstruation and dysmenorrhoea and, although speculative, to offer a treatment reducing menstrual flow to the individual woman with much more pronounced CRP increases. Similarly, it might be wise to avoid surgery during menstruation in women with very high CRP concentrations. Unfortunately, we have no data on whether anti-inflammatory drugs [34] or other CRP-lowering agents [48] could be considered.
With a little imagination, retrograde menstruation and increased CRP concentrations could be discussed differently. In mammals, menstruation, which occurs only in humans, some primates, 2 mouse strains, and some bats, is the exception without clear benefits. Today, women have over 400 menstruations in a lifetime, which is much more than the estimated 30 to 40 menstruations, 100 years ago. Retrograde menstruation has, to the best of our knowledge, been demonstrated only in women. After occlusion of the cervix, baboons develop haematometra without retrograde menstruation [49]. We risk underestimating the importance of the abdominal cavity being directly connected to the vagina, and of sperm cells transporting microorganisms on their tails. Therefore, it has been discussed that menstruation and retrograde menstruation might have some reproductive advantages in embryo selection, but at a price. It could be discussed whether avoiding menstruation in all women who are not trying to conceive might be beneficial. Abolishing menstruation might reduce the risk of endometriosis, considered a consequence of many retrograde menstruations because of delaying childbirth, together with microbiota. It could be argued that oral contraception should be given continuously, knowing that the 21+7 regimens with bleeding were chosen mainly to exclude an eventual pregnancy. In women without a pregnancy wish, tubal ligation could be reconsidered, primarily since it can be performed as a 5-minute procedure under local anaesthesia [50]. Preventing menstruation and retrograde menstruation and preventing vaginal microbiota from reaching the abdominal cavity might turn out to reduce the risk of ovarian cancer since the incidence of ovarian cancer is decreased by 50% after tubal ligation [51,52] or long-term oral contraceptive use [53,54].
5. Conclusions
The CRP concentrations increase during menstruation in most women. Although probably related to the volume of retrograde menstruation, a contribution from microbiota in the upper genital tract, eventually the vagina, and from the inflammation associated with menstruation, cannot be excluded. The increase in CRP concentrations reflecting mesothelial cell retraction must facilitate endometrial cell implantation and can explain the localisation of endometriosis lesions. The clinical consequences of this menstrual increase in CRP are unclear. However, this observation could be used clinically to consider individualisation of those women with much higher CRP concentrations during menstruation. Individualisation could be considered to prevent endometriosis in women with heavy menstrual bleeding and dysmenorrhoea, to prevent recurrences of endometriosis after surgery, and maybe to avoid surgery during menstruation. Philosophically, it might be argued that avoiding menstrual bleeding could be beneficial for all women
Author Contributions
“Conceptualisation, MMB and PRK.; statistics, PRK.; draft manuscript MMB; formal analysis and writing, all authors. All authors have read and agreed to the published version of the manuscript.”.
Funding
“This research received no external funding”.
Institutional Review Board Statement
“Not applicable”.
Informed Consent Statement
“Not applicable.”.
Data Availability Statement
“Available with the authors on simple request”.
Conflicts of Interest
“The authors declare no conflicts of interest.”.
Abbreviations
The following abbreviations are used in this manuscript:
| CRP | C-reactive protein |
| SD | Standard deviation |
| PMS | Premenstrual syndrome |
| EF | Early follicular |
| LF | Late follicular |
| LL | Late luteal |
| SQR | Semi Quartile Range |
| PCOS | Polycystic ovarian syndrome |
References
- Koninckx, P.R.; Ide, P.; Vandenbroucke, W.; Brosens, I.A. New aspects of the pathophysiology of endometriosis and associated infertility. J Reprod. Med 1980, 24, 257-260, https://pubmed.ncbi.nlm.nih.gov/7420327/.
- Halme, J.; Hammond, M.G.; Hulka, J.F.; Raj, S.G.; Talbert, L.M. Retrograde menstruation in healthy women and in patients with endometriosis. Obstet Gynecol 1984, 64, 151-154.
- Sampson, J.A. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol 1927, 14, 422-469. [CrossRef]
- Kruitwagen, R.F. Menstruation as the pelvic aggressor. Baillieres Clin Obstet Gynaecol 1993, 7, 687-700. [CrossRef]
- Raimondo, D.; Raffone, A.; Aru, A.C.; Salucci, P.; Travaglino, A.; Maletta, M.; Ambrosio, M.; Borghese, G.; Iodice, R.; Casadio, P.; et al. C-reactive Protein for Predicting Early Postoperative Complications in Patients Undergoing Laparoscopic Shaving for Deep Infiltrating Endometriosis. Journal of Minimally Invasive Gynecology 2022, 29, 135-143. [CrossRef] [PubMed]
- Raimondo, D.; Raffone, A.; Aru, A.C.; Salucci, P.; Travaglino, A.; Maletta, M.; Ambrosio, M.; Borghese, G.; Iodice, R.; Casadio, P.; et al. C-reactive Protein for Predicting Early Postoperative Complications in Patients Undergoing Laparoscopic Shaving for Deep Infiltrating Endometriosis. J Minim Invasive Gynecol 2021. [CrossRef]
- De Cicco, C.; Schonman, R.; Ussia, A.; Koninckx, P.R. Extensive peritoneal lavage decreases postoperative C-reactive protein concentrations: a RCT. Gynecol Surg 2015, 12, 271-274. [CrossRef]
- Koninckx, P.R.; Gomel, V.; Ussia, A.; Adamyan, L. Role of the peritoneal cavity in the prevention of postoperative adhesions, pain, and fatigue. Fertil Steril 2016, 106, 998-1010. [CrossRef]
- Koninckx, P.R.; Ussia, A.; Adamyan, L.; Wattiez, A.; Vigano, P. Understanding Peritoneal Fluid Estrogen and Progesterone Concentrations Permits Individualization of Medical Treatment of Endometriosis-Associated Pain with Lower Doses, Especially in Adolescents Not Requiring Contraception. Journal of Clinical Medicine 2025, 14, 7196. [CrossRef] [PubMed]
- Mutsaers, S.E.; Pixley, F.J.; Prêle, C.M.; Hoyne, G.F. Mesothelial cells regulate immune responses in health and disease: role for immunotherapy in malignant mesothelioma. Curr. Opin. Immunol. 2020, 64, 88-109. [CrossRef] [PubMed]
- Koninckx, P.R.; Ussia, A.; Tahlak, M.; Adamyan, L.; Wattiez, A.; Martin, D.C.; Gomel, V. Infection as a potential cofactor in the genetic-epigenetic pathophysiology of endometriosis: a systematic review. Facts Views Vis Obgyn 2019, 11, 209-216.
- Tang, F.; Deng, M.; Xu, C.; Yang, R.; Ji, X.; Hao, M.; Wang, Y.; Tian, M.; Geng, Y.; Miao, J. Unraveling the microbial puzzle: exploring the intricate role of gut microbiota in endometriosis pathogenesis. Frontiers in cellular and infection microbiology 2024, 14, 1328419. [CrossRef]
- Guo, C.; Zhang, C. Role of the gut microbiota in the pathogenesis of endometriosis: a review. Front Microbiol 2024, 15, 1363455. [CrossRef]
- nervus vagus microbiota. 2024.
- Salmeri, N.; Sinagra, E.; Dolci, C.; Buzzaccarini, G.; Sozzi, G.; Sutera, M.; Candiani, M.; Ungaro, F.; Massimino, L.; Danese, S.; et al. Microbiota in Irritable Bowel Syndrome and Endometriosis: Birds of a Feather Flock Together-A Review. Microorganisms 2023, 11. [CrossRef]
- Lin, Q.; Duan, H.; Wang, S.; Guo, Z.; Wang, S.; Chang, Y.; Chen, C.; Shen, M.; Shou, H.; Zhou, C. Endometrial microbiota in women with and without adenomyosis: A pilot study. Front Microbiol 2023, 14, 1075900. [CrossRef]
- Kobayashi, H. Gut and reproductive tract microbiota: Insights into the pathogenesis of endometriosis (Review). Biomed Rep 2023, 19, 43. [CrossRef]
- Yuan, W.; Wu, Y.; Chai, X.; Wu, X. The colonized microbiota composition in the peritoneal fluid in women with endometriosis. Archives of Gynecology and Obstetrics 2022. [CrossRef] [PubMed]
- Binda, M.M.; Riiskjaer, M.; Koninckx, P.R. Pneumoperitoneum induced mesothelial cell changes in a laparoscopic mouse model. European Journal of Obstetrics & Gynecology and Reproductive Biology 2021, 265, 107-112. [CrossRef] [PubMed]
- Volz, J.; Koster, S.; Spacek, Z.; Paweletz, N. Characteristic alterations of the peritoneum after carbon dioxide pneumoperitoneum. Surg. Endosc 1999, 13, 611-614.
- Mutsaers, S.E.; Prele, C.M.; Pengelly, S.; Herrick, S.E. Mesothelial cells and peritoneal homeostasis. Fertil Steril 2016, 106, 1018-1024. [CrossRef]
- Binda, M.M.; Corona, R.; Amant, F.; Koninckx, P.R. Conditioning of the abdominal cavity reduces tumor implantation in a laparoscopic mouse model. Surg Today 2014, 44, 1328-1335. [CrossRef]
- Corona, R.; Verguts, J.; Schonman, R.; Binda, M.M.; Mailova, K.; Koninckx, P.R. Postoperative inflammation in the abdominal cavity increases adhesion formation in a laparoscopic mouse model. Fertil. Steril 2011, 95, 1224-1228. [CrossRef]
- Ryan, G.B.; Majno, G. Acute inflammation. A review. Am J Pathol 1977, 86, 183-276.
- Özdemir-Van Brunschot, D.M.D.; Van Laarhoven, K.C.J.H.M.; Scheffer, G.-J.; Pouwels, S.; Wever, K.E.; Warlé, M.C. What is the evidence for the use of low-pressure pneumoperitoneum? A systematic review. Surg. Endosc. 2016, 30, 2049-2065. [CrossRef] [PubMed]
- Breborowicz, A.; Oreopoulos, D.G. Is normal saline harmful to the peritoneum? Perit. Dial. Int 2005, 25 Suppl 4, S67-S70. [CrossRef]
- Corona, R.; Binda, M.M.; Mailova, K.; Verguts, J.; Koninckx, P.R. Addition of nitrous oxide to the carbon dioxide pneumoperitoneum strongly decreases adhesion formation and the dose-dependent adhesiogenic effect of blood in a laparoscopic mouse model. Fertil. Steril 2013, 100, 1777-1783. [CrossRef] [PubMed]
- Viganò, P.; Caprara, F.; Giola, F.; Di Stefano, G.; Somigliana, E.; Vercellini, P. Is retrograde menstruation a universal, recurrent, physiological phenomenon? A systematic review of the evidence in humans and non-human primates. Hum Reprod Open 2024, 2024, hoae045. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [CrossRef] [PubMed]
- Koninckx, P.R.; Heyns, W.; Verhoeven, G.; Van, B.H.; Lissens, W.D.; De, M.P.; Brosens, I.A. Biochemical characterization of peritoneal fluid in women during the menstrual cycle. J Clin. Endocrinol. Metab 1980, 51, 1239-1244. [CrossRef]
- Koninckx, P.; De Hertogh, R.; Heyns, W.; Meulepas, E.; Brosens, I.; De Moor, P. Secretion rates of LH and FSH during infusion of LH-FSH/RH in normal women and in patients with secondary amenorrhea: suggestive evidence for two pools of LH and FSH. J Clin Endocrinol Metab 1976, 43, 159-167. [CrossRef] [PubMed]
- Sollberger, S.; Ehlert, U. How to use and interpret hormone ratios. Psychoneuroendocrinology 2016, 63, 385-397. [CrossRef]
- Blum, C.A.; Müller, B.; Huber, P.; Kraenzlin, M.; Schindler, C.; De Geyter, C.; Keller, U.; Puder, J.J. Low-grade inflammation and estimates of insulin resistance during the menstrual cycle in lean and overweight women. J Clin Endocrinol Metab 2005, 90, 3230-3235. [CrossRef] [PubMed]
- Talebpour, A.; Mohammadifard, M.; Reza; Mahmoudzadeh, S.; Rezapour, H.; Saharkhiz, M.; Tajik, M.; Ferns, G.A.; Bahrami, A. Effect of curcumin on inflammatory biomarkers and iron profile in patients with premenstrual syndrome and dysmenorrhea: A randomized controlled trial. Physiological Reports 2023, 11. [CrossRef]
- Yama, K.; Asari, Y.; Ono, A.; Machida, M.; Miura, J. Plasma Interleukin-10 Levels Are Altered in Women with Severe Premenstrual Syndrome: A Preliminary Study. Women’s Health Reports 2020, 1, 73-79. [CrossRef]
- Chaireti, R.; Lindahl, T.L.; Byström, B.; Bremme, K.; Larsson, A. Inflammatory and endothelial markers during the menstrual cycle. Scand. J. Clin. Lab. Invest. 2016, 76, 190-194. [CrossRef]
- Gursoy, A.Y.; Caglar, G.S.; Kiseli, M.; Pabuccu, E.; Candar, T.; Demirtas, S. CRP at early follicular phase of menstrual cycle can cause misinterpretation for cardiovascular risk assessment. Interventional Medicine and Applied Science 2015, 7, 143-146. [CrossRef]
- Gaskins, A.J.; Wilchesky, M.; Mumford, S.L.; Whitcomb, B.W.; Browne, R.W.; Wactawski-Wende, J.; Perkins, N.J.; Schisterman, E.F. Endogenous Reproductive Hormones and C-reactive Protein Across the Menstrual Cycle: The BioCycle Study. Am. J. Epidemiol. 2012, 175, 423-431. [CrossRef]
- Wander, K.; Brindle, E.; O’Connor, K.A. C-reactive protein across the menstrual cycle. Am. J. Phys. Anthropol. 2008, 136, 138-146. [CrossRef] [PubMed]
- Puder, J.J.; Blum, C.A.; Mueller, B.; De Geyter, C.; Dye, L.; Keller, U. Menstrual cycle symptoms are associated with changes in low-grade inflammation. Eur J Clin Invest 2006, 36, 58-64. [CrossRef]
- Hellebrekers, B.W.J.; Trimbos-Kemper, T.C.M.; Boesten, L.; Jansen, F.W.; Kolkman, W.; Trimbos, J.B.; Press, R.R.; Van Poelgeest, M.I.E.; Emeis, S.J.; Kooistra, T. Preoperative predictors of postsurgical adhesion formation and the Prevention of Adhesions with Plasminogen Activator (PAPA-study): results of a clinical pilot study. Fertility and Sterility 2009, 91, 1204-1214. [CrossRef]
- Berbic, M.; Ng, C.H.; Fraser, I.S. Inflammation and endometrial bleeding. Climacteric 2014, 17 Suppl 2, 47-53. [CrossRef]
- Evans, J.; Salamonsen, L.A. Inflammation, leukocytes and menstruation. Rev Endocr Metab Disord 2012, 13, 277-288. [CrossRef]
- Bricou, A.; Batt, R.E.; Chapron, C. Peritoneal fluid flow influences anatomical distribution of endometriotic lesions: why Sampson seems to be right. Eur. J. Obstet. Gynecol. Reprod. Biol 2008, 138, 127-134.
- Kyathanahalli, C.N.; Tu, F.F.; Hellman, K.M. Inflammatory Mechanisms of Dysmenorrhea: Novel Insights From Menstrual Effluent in an Adolescent Cohort. BJOG: An International Journal of Obstetrics & Gynaecology 2025, 132, 1626-1634. [CrossRef]
- Schonman, R.; Corona, R.; Bastidas, A.; De, C.C.; Koninckx, P.R. Effect of Upper Abdomen Tissue Manipulation on Adhesion Formation between Injured Areas in a Laparoscopic Mouse Model. J. Minim. Invasive. Gynecol 2009, 16, 307-312. [CrossRef]
- Burke, R.K.; Hertig, A.T.; Miele, C.A. Prognostic value of subacute focal inflammation of the endometrium, with special reference to pelvic adhesions as observed on laparoscopic examination: An eight-year review. J. Reprod. Med 1985, 30, 646-650.
- Prasad, K. C-Reactive Protein (CRP)-Lowering Agents. Cardiovasc. Drug Rev. 2006, 24, 33-50. [CrossRef] [PubMed]
- Donnez, O.; A., V.L.; Defrere, S.; Colette, S.; O., V.K.; Dehoux, J.P.; Squifflet, J.; Donnez, J. Induction of endometriotic nodules in an experimental baboon model mimicking human deep nodular lesions. Fertil Steril 2013, 99, 783-789. [CrossRef] [PubMed]
- Koninckx, P.R.; Verguts, J.; Corona, R.; Adamyan, L.; Brosens, I. A mixture of 86% of CO2, 10% of N2O, and 4% of oxygen permits laparoscopy under local anesthesia: a pilot study. Gynecol Surg 2015, 12, 57-60. [CrossRef] [PubMed]
- Cibula, D.; Widschwendter, M.; Májek, O.; Dusek, L. Tubal ligation and the risk of ovarian cancer: review and meta-analysis. Hum Reprod Update 2011, 17, 55-67. [CrossRef] [PubMed]
- Magarakis, L.; Idahl, A.; Särnqvist, C.; Strandell, A. Efficacy and safety of sterilisation procedures to reduce the risk of epithelial ovarian cancer: a systematic review comparing salpingectomy with tubal ligation. The European Journal of Contraception & Reproductive Health Care 2022, 27, 230-239. [CrossRef]
- Jahanfar, S.; Mortazavi, J.; Lapidow, A.; Cu, C.; Al Abosy, J.; Morris, K.; Becerra-Mateus, J.C.; Steinfeldt, M.; Maurer, O.; Bohang, J.; et al. Assessing the impact of contraceptive use on reproductive cancer risk among women of reproductive age—a systematic review. Frontiers in Global Women’s Health 2024, 5. [CrossRef]
- Arshadi, M.; Hesari, E.; Ahmadinezhad, M.; Yekta, E.M.; Ebrahimi, F.; Azizi, H.; Esfarjani, S.V.; Rostami, M.; Khodamoradi, F. The association between oral contraceptive pills and ovarian cancer risk: A systematic review and meta-analysis. Bull. Cancer 2024, 111, 918-929. [CrossRef] [PubMed]
Figure 1.
The mesothelial cells lining the peritoneal cavity are large, flat cells with microvilli (A). These cells react within seconds to minor trauma by retracting, which results in cell bulging (B), exposure of the basal membrane (C), and acute inflammation. Reproduced with permission from [19]. .
Figure 1.
The mesothelial cells lining the peritoneal cavity are large, flat cells with microvilli (A). These cells react within seconds to minor trauma by retracting, which results in cell bulging (B), exposure of the basal membrane (C), and acute inflammation. Reproduced with permission from [19]. .
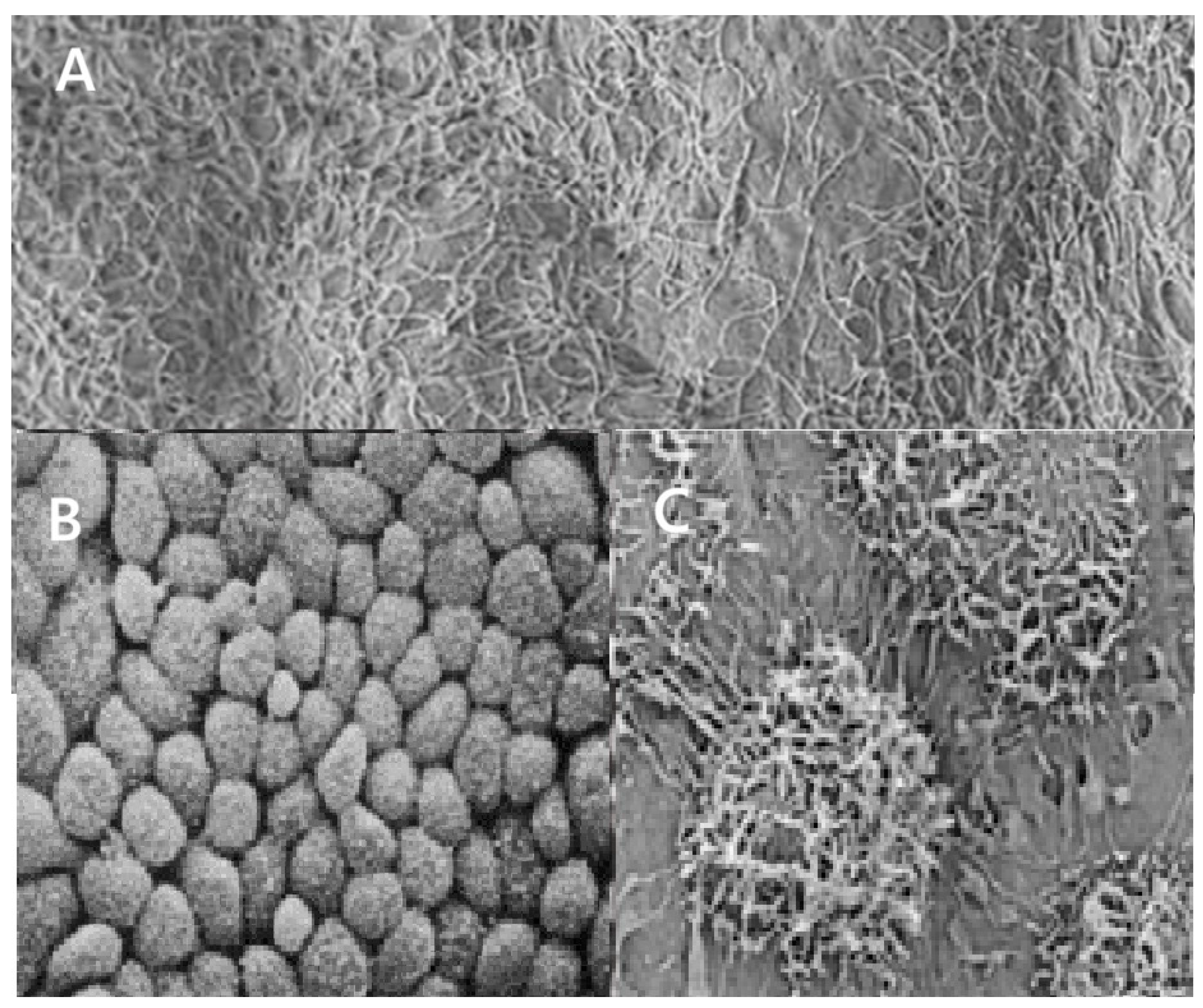
Figure 2.
Menstrual or early follicular (EF) increase in CRP concentrations in comparison with late follicular (LF) and late luteal (LL) concentrations. The size of the bubbles is proportional to the number of subjects included. The mean and standard error of the mean are indicated, but do not reflect the variable number of women included.
Figure 2.
Menstrual or early follicular (EF) increase in CRP concentrations in comparison with late follicular (LF) and late luteal (LL) concentrations. The size of the bubbles is proportional to the number of subjects included. The mean and standard error of the mean are indicated, but do not reflect the variable number of women included.
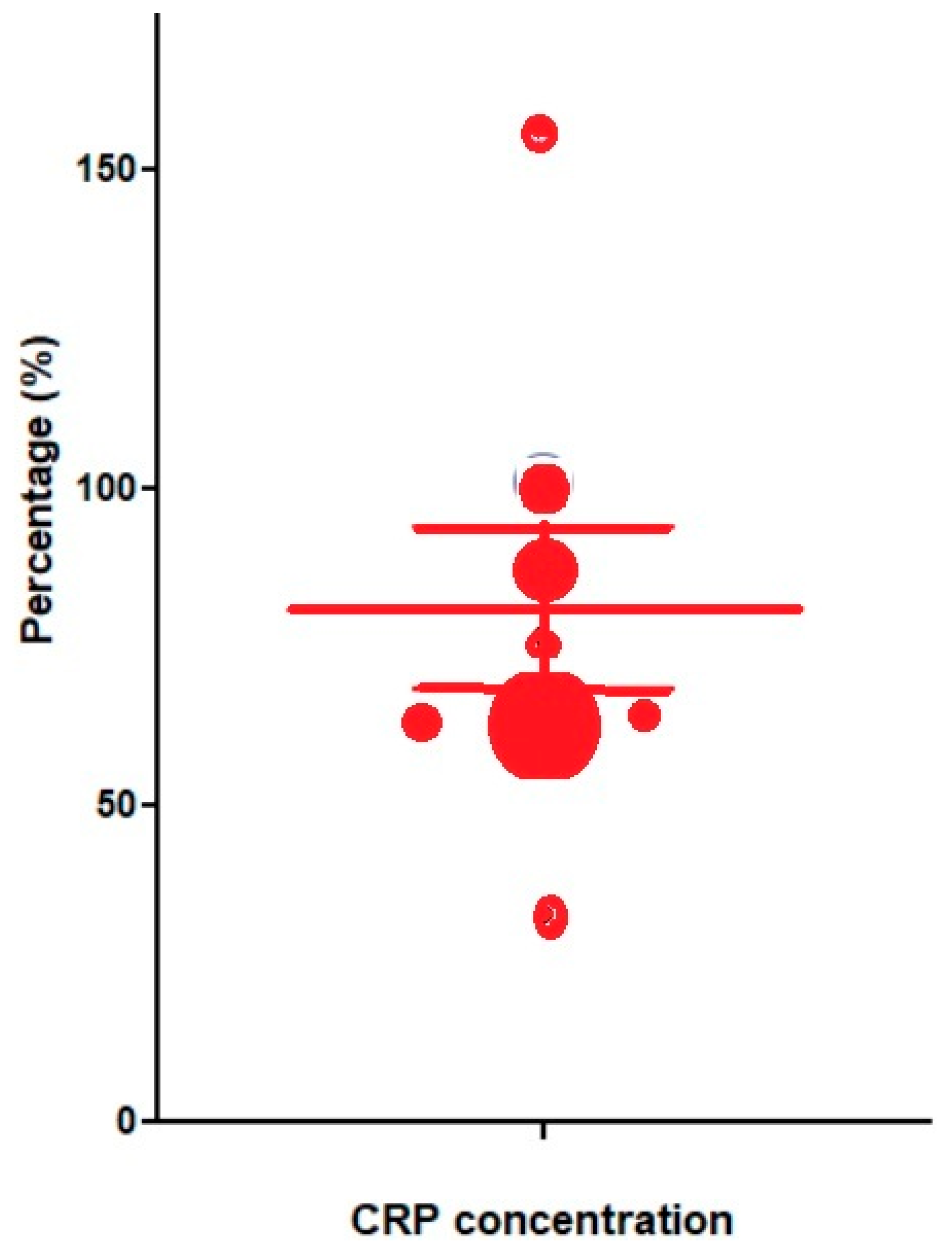

Table 1.
Menstrual or early follicular (EF) and late follicular (LF), and late luteal (LL) CRP concentrations and the reported p-values. Data were reported as mean and standard deviation (SD), median and interquartile range (IQR), or minimum and maximum values, reflecting the variability. The percentage increase during menstruation or the early follicular phase was calculated.
Table 1.
Menstrual or early follicular (EF) and late follicular (LF), and late luteal (LL) CRP concentrations and the reported p-values. Data were reported as mean and standard deviation (SD), median and interquartile range (IQR), or minimum and maximum values, reflecting the variability. The percentage increase during menstruation or the early follicular phase was calculated.
| Menstrual or EF | Late follicular or luteal | P value |
% increase (Mean±SD) |
|||||
| N |
Mean (Median) |
SD (SQR) [min -max] |
Mean (median) |
SD (SQR) [min -max] |
||||
| Talebpour et al. 2023 [34] | 111 | (0.4) | [0.0-4.0] | LL | (0.2) | [0.0-2.0] | - | 100 |
| Yama et al 2020 [35] | 21 | (0.24) | (0.1-0.4) | LL | (0.18) | (0.1-0.6) | NS | 33 |
| Chiareti et al 2015 [36] | 102 | 1.65 | 3 | LL | 0.89 | 1 | 0.025 | 85 |
| Gursoy et al 2015 [37] | 27 | (1.8) | [0.3-7.7] | LF | (0.7) | [0.1-8.3] | <0.001 | 157 |
| Gaskins et al. 2012 [38] | 509 | (0.75) | (0.4-1.7) | LF | (0.45) | (0.3-1.2) | 0.001 | 66 |
| Wander et al 2008 [39] | 72 | 2.8 | - | LF | 1.7 | - | 0.01 | 64 |
| Puder et al 2006 [40] | 15 | 1.4 | 1.3 | LF | 0.8 | 0.74 | 0.007 | 75 |
| Blum et al. 2005 [33] | 15 | 130%£ | 50% | LF | 78% | 30% | 0.00001 | 67 |
| 80±36 | ||||||||
£ In this article, CRP data were only presented as a percentage of each person’s mean concentration during the menstrual cycle.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



