
Submitted:
01 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
Background: Plasmablastic lymphoma (PBL) is a rare and highly aggressive B-cell neoplasm most often associated with immunodeficiency. Transformation of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) into PBL is exceptionally uncommon, particularly in immunocompetent individuals. This paper describes a rare synchronous SLL-to-PBL transformation and summarizes current knowledge on synchronous and metachronous cases reported in the literature. Methods: A 46-year-old immunocompetent woman presented with generalized lymphadenopathy and lumbar pain. Concurrent biopsies of an axillary lymph node and a retroperitoneal mass were obtained. Diagnostic evaluation included immunohistochemistry, fluorescent in situ hybridization (FISH), PCR-based assessment of IGH, IGK, and IGL loci, and next-generation sequencing (NGS) of IGHV to assess clonal relatedness. The patient was treated with six cycles of Dara-CHOP, followed by autologous stem cell transplantation and maintenance therapy with daratumumab and ibrutinib. Results: The axillary node showed SLL (CD20+, CD5+, CD23+), while the retroperitoneal mass demonstrated classic features of PBL (CD138+, MUM1+, MYC+, Ki-67 ~100%, CD20–). FISH detected MYC rearrangement in the PBL component. PCR and NGS confirmed identical IGHV1-69 rearrangements, establishing clonal relatedness and Richter transformation. Review of published cases shows that both synchronous and metachronous CLL/SLL-to-PBL transformations are exceedingly rare. The patient achieved partial metabolic remission after treatment and remains in sustained metabolic response 24 months after diagnosis. Conclusions: This case highlights a rare example of synchronous CLL/SLL-to-PBL transformation in an immunocompetent patient. Integration of detailed molecular diagnostics enabled early recognition and guided a personalized treatment approach incorporating CD38-targeted therapy and BTK inhibition, resulting in an excellent long-term clinical outcome.
Keywords:
SLL
; PBL
; NGS‐based clonal confirmation
; CD38 and BTK‐targeted therapy
1. Introduction
Richter’s transformation (RT) is the progression of chronic lymphocytic leukaemia/small lymphocytic lymphoma (CLL/SLL) into a more aggressive lymphoma, most often diffuse large B-cell lymphoma (DLBCL) [1]. Plasmablastic lymphoma (PBL) is a rare and aggressive transformation, especially uncommon in immunocompetent individuals [2]. It is most often seen in the context of immunodeficiency, such as HIV infection or prior exposure to chemotherapy [3,4,5]. We report a rare synchronous SLL and PBL case in an immunocompetent patient, and we additionally analyzed published cases CLL/SLL-to-PBL transformations, focusing on their clinical presentation, diagnostic features, and therapeutic approaches, highlighting patterns relevant for early recognition and management.
2. Case Report
We report a rare case of synchronous SLL and PBL in a 46-year-old woman, who presented in December 2023 with lower back pain, highlighting both diagnostic challenges and histopathological features. PET imaging revealed hypermetabolic retroperitoneal masses compressing the right ureter without renal impairment, along with bilateral pelvic lymph node involvement. In January 2024, an axillary lymph node biopsy was performed due to accessibility and significant lymphadenopathy on imaging, concurrently with a biopsy of a retroperitoneal lymph node. Biopsy specimens were analyzed histologically and immunohistochemically. Axillary and retroperitoneal nodes were examined for morphology and immunophenotype using standard panels (CD20, CD5, CD23, CD10, BCL6, cyclin D1, CD138, CD38, MUM1, c-myc, Ki67, light chains). FISH analysis was performed to detect MYC, BCL2, and BCL6 rearrangements. Clonal relatedness between SLL and PBL components was assessed by PCR-based analysis of IGH, IGK, and IGL loci, complemented by next-generation sequencing (NGS) of IGHV. In situ hybridization for EBV (EBER) and HHV8 (LANA1) was also performed. The patient was treated with Dara-CHOP chemotherapy (daratumumab, cyclophosphamide, doxorubicin, vincristine, prednisone) followed by autologous hematopoietic stem cell transplantation (AHSCT). Maintenance therapy consisted of monthly daratumumab and ibrutinib.
Overview of clinical and pathological features of reported transformation cases from CLL/SLL to PBL were analyzed separately for synchronous and metachronous transformations. Synchronous cases were defined as those in which CLL/SLL and PBL were diagnosed simultaneously or within a 6-month interval, while metachronous cases were defined as those in which transformation occurred more than 6 months after the initial CLL/SLL diagnosis.This distinction was made because synchronous transformations, occurring within a short temporal window, are more likely to originate from the same precursor clone, whereas metachronous cases may develop through later genetic divergence or therapy-driven clonal evolution, making their clonal relationship less predictable unless formally confirmed by molecular testing. For both groups, we collected and compared available clinical characteristics, pathological findings, immunophenotypic profiles, molecular data, treatment approaches, and patient outcomes, as reported in the literature.
3. Results
3.1. Morphological and Immunohistochemical Evaluation
Axillary lymph node biopsy revealed diffuse infiltration by small neoplastic cells with round to slightly irregular nuclei, condensed chromatin, and scant cytoplasm (Figure 1A). Immunohistochemistry confirmed SLL/CLL phenotype: CD20+, CD5+, CD23+, CD10−, BCL6−, cyclin D1−. Ki67 proliferation index was low (20–30%), with focal enhancement in proliferative centers (Figure 1B–F). Retroperitoneal lymph node histology showed a compact lymphoid proliferation of medium to large plasmacytoid cells with rounded/angular nuclei, decondensed chromatin, and prominent nucleoli. Apoptotic debris and mitoses were observed. Tumor cells were CD138+, CD38+, MUM1+, c-myc+, CD5−, CD10−, CD19−, CD20−, CD23−, CD45−, BCL2−, BCL6−, EMA−, cyclin D1−, ALK1−, IgA−, OCT2−, LANA1−. Ki67 index was nearly 100%. Tumor cells expressed lambda light chains, negative for kappa (Figure 2A,B).
3.2. Mollecular Analysis
3.3. Therapy
After two cycles of Dara-CHOP, PET in March 2024 showed no progression but persistent hypermetabolic lesions, prompting four additional cycles. By May 2024, a complete metabolic response was observed in the abdominal mass, though pelvic lymphadenopathy remained metabolically active. In July 2024, the patient underwent AHSCT. Chemotherapy was well tolerated; aplasia occurred on day +2, G-CSF started on day +7, with uneventful recovery. Maintenance therapy was initiated for residual SLL/CLL with daratumumab and ibrutinib.
3.4. Brief review of Synchronous Versus Metachronous Transformations Reported in the Literature
The results of our literature review are presented in Table 1 and Table 2. In summary, we identified four simultaneously diagnosed transformation cases within less than six months and ten non-simultaneously diagnosed cases. In both groups, patients were predominantly elderly males, with heterogeneous clinical presentations, diagnostic approaches, and treatment modalities. CHOP-based regimens were the most frequently applied therapy. In the synchronous group, only our patient achieved clinical stability with a daratumumab-based regimen targeting CD38 in addition to prior CHOP therapy, whereas in the metachronous group, one patient responded to combined localized therapy and chemotherapy.
4. Discussion
PBL is a rare and aggressive B-cell neoplasm first described by Delecluse et al. in 1997, predominantly affecting older male patients and immunocompromised individuals such as those with HIV, EBV infection, or post-transplant immunosuppression [3,4,6,7]. Extranodal involvement is common, while purely nodal PBL in immunocompetent patients remains exceedingly rare [3,8,9]. Transformation of CLL/SLL into PBL is particularly uncommon. The first reported case was described by Robak et al. in 2001 in an HIV- and EBV-negative woman [10]. Early (≤6 months) versus late (>6 months) transformations may reflect distinct biological mechanisms: early transformation could result from a pre-existing aggressive sub-clone or a common progenitor at the time of CLL diagnosis, whereas late transformation may arise from clonal evolution under therapeutic or micro-environmental pressure, as we revised the cases [4,7] (Table 1 and Table 2). Precise diagnosis typically involves lymph node biopsy, supported by ancillary studies such as IHC, FISH, PCR, and NGS to confirm clonality [2,16,18,19,20]. We report a rare case of a middle-aged woman who presented with lumbar pain, bilateral renal obstruction, and generalized lymphadenopathy. SLL and PBL were diagnosed simultaneously from axillary and retroperitoneal lymph nodes. While most reported patients are older males, only a few female cases—including ours—have been described [11,12]. The clinical presentation in our patient, with generalized lymphadenopathy and lumbar pain, aligns with the most commonly reported manifestations in the literature, which often also include B symptoms and pain associated with retroperitoneal or skeletal involvement [13,14]. Unlike most reported cases, the transformation in our patient was confined to lymph nodes, with no bone marrow involvement. This localized presentation may indicate an early stage of transformation or a nodal form of PBL with distinct biological behavior, and it may also reflect the benefit of rapid and accurate diagnostic evaluation. The diagnosis was established using a complete diagnostic workup—including imaging, immunohistochemistry, and FISH—with clonal relatedness confirmed by PCR and next-generation sequencing, representing, to our knowledge, the first such comprehensive approach reported in the literature. Histologically, the axillary lymph node showed classic SLL features with CD20 and CD5 expression. In contrast, the retroperitoneal lymph node demonstrated a diffuse proliferation of large plasmablast- and immunoblast-like cells with high mitotic activity and necrosis. These cells expressed plasma cell markers CD38, CD138, and MUM1, had a high Ki-67 index, and lacked B-cell markers such as CD20 and PAX5, consistent with typical PBL [3,4,7]. Because PBL can overlap morphologically and immunophenotypically with other entities—including immunoblastic DLBCL, plasmablastic myeloma, ALK-positive large B-cell lymphoma, and HHV-8–associated DLBCL—these diagnoses were carefully excluded. In our case, ALK positivity and paraproteinemia were absent, and lack of BCL2 and BCL6 expression helped rule out DLBCL and Burkitt lymphoma, while positivity for MYC and plasma cell markers supported the diagnosis of PBL [3,15]. Consistent with other reports, our patient tested negative for HIV, EBV, and HHV-8. Although HIV status is often negative or unreported in the literature, EBV positivity has been described by Khanna et al. and Martinez et al. ([2,12]; Table 1 and Table 2). These observations suggest that some cases of PBL may arise independently of viral infection, potentially driven by somatic mutations, genomic instability, and MYC-mediated transformation. Using FISH, we confirmed a MYC rearrangement, in line with the majority of previously reported cases ([2,10,16,17]). In contrast, Gasljevic et al. described a case without MYC rearrangement, highlighting potential diagnostic challenges, particularly as the antecedent disease was classical Hodgkin lymphoma rather than CLL/SLL ([11]; Table 2).
Confirming clonal relatedness through PCR and NGS was essential to establish this case as a true Richter transformation rather than two unrelated neoplasms ([2,16,18]). While Ramsay et al. and Chan et al. previously applied NGS, their analyses were limited to metachronous cases ([17,18]; Table 2). NGS is particularly valuable in synchronous transformations, where histopathological and immunophenotypic overlap can obscure disease evolution and where molecular confirmation is necessary to distinguish true transformation from the coexistence of two independent lymphoid neoplasms. In these instances, high-resolution genomic analysis provides definitive evidence of clonal relatedness, improves understanding of pathogenesis, and informs more tailored therapeutic strategies ([19,20]). Although additional synchronous transformation cases have been reported ([8,21,22]), they were excluded from our review due to lack of clonality confirmation, limiting their interpretive value.
Therapeutic management of PBL remains challenging due to its intrinsic chemo-resistance, MYC rearrangements, plasmacytic phenotype, and often low CD20 expression, which reduces rituximab efficacy [10,18]. In most reported cases, patients received R-CHOP or CHOP-like regimens and succumbed within six months, with only two exceptions: one patient survived 24 months, and another remained stable at the time of publication ([12,9]; Table 2). A particularly unusual case, reported by Mazumder et al. but not included in our review due to unconfirmed clonality, involved spontaneous regression of a gingival mass following biopsy [21]. However, the diagnostic work-up was limited to histology and EBV positivity, without molecular or phenotypic profiling, leaving its classification uncertain. In contrast to most reviewed cases, particularly synchronous transformations, our patient was diagnosed approximately 24 months ago and remains clinically stable after completing eight cycles of chemotherapy. She was treated with a daratumumab-based regimen targeting CD38, a marker highly expressed in PBL, which led to rapid resolution of lymphadenopathy, hepatosplenomegaly, and systemic symptoms. The patient subsequently underwent ASCT and is maintained on daratumumab and ibrutinib. This multimodal approach appears effective in controlling both plasmablastic and residual B-cell components. These observations emphasize the importance of tailoring treatment to the plasmablastic phenotype, particularly through the use of CD38-targeted therapy, BTK inhibitors, and stem cell transplantation.
5. Conclusions
This report describes a rare synchronous transformation of CLL/SLL into PBL in an immunocompetent woman, with nodal disease and clonal relatedness confirmed by PCR and NGS. Early molecular confirmation allowed prompt initiation of targeted multimodal therapy, resulting in a favorable outcome. These findings underscore the value of precise molecular diagnostics in synchronous transformations and the potential efficacy of CD38- and BTK-directed treatments in plasmablastic disease.
Author Contributions
Conceptualization: J.F., A.M.; Methodology: J.F., A.M.; Formal analysis and investigation: J.F., S.M., T.T., R.R., T.B., G.L., T.B.B., M.S., A.M.; Writing – original draft preparation: J.F., S.M.; Writing – review and editing: J.F., A.M., T.T.; Supervision: A.M.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to written informed consent that has been obtained from the patient to publish this paper.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy.
Acknowledgments
The authors have no acknowledgments to declare.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
RT Richter’s transformation
CLL/SLL Chronic lymphocytic leukemia / Small lymphocytic lymphoma
DLBCL Diffuse large B-cell lymphoma
PBL Plasmablastic lymphoma
HIV Human immunodeficiency virus
EBV Epstein–Barr virus
HHV-8 Human herpesvirus 8
SLL Small lymphocytic lymphoma
CD Cluster of differentiation
MUM1 Multiple myeloma oncogene 1
MYC MYC proto-oncogene
Ki-67 Marker of proliferation
FISH Fluorescent in situ hybridization
PCR Polymerase chain reaction
IGH Immunoglobulin heavy chain
IGK Immunoglobulin kappa light chain
IGL Immunoglobulin lambda light chain
NGS Next-generation sequencing
PET Positron emission tomography
HE Hematoxylin and eosin
EMA Epithelial membrane antigen
ALK1 Anaplastic lymphoma kinase 1
LANA1 Latency-associated nuclear antigen 1 (HHV8)
Dara-CHOP Daratumumab + Cyclophosphamide + Doxorubicin + Vincristine + Prednisone
AHSCT Autologous hematopoietic stem cell transplantation
BTK Bruton tyrosine kinase
References
- Petrackova, A; Turcsanyi, P; Papajik, T; Kriegova, E. Revisiting Richter transformation in the era of novel CLL agents. Blood Rev. 2021, 49, 100824. [Google Scholar] [CrossRef]
- Khanna, A; Drumheller, BR; Deeb, G; Tolbert, EW; Asakrah, S. Plasmablastic transformation of chronic lymphocytic leukemia: a review of literature and report on 2 cases. Lab Med. 2023, 54(6), e177-85. [Google Scholar] [CrossRef]
- Bailly, J; Jenkins, N; Chetty, D; Mohamed, Z; Verburgh, ER; Opie, JJ. Plasmablastic lymphoma: An update [published correction appears in Int J Lab Hematol. 2022 Dec; 44(6):1121. (doi: 10.1111/ijlh.13981)]. Int J Lab Hematol. 2022, 44 Suppl 1(Suppl 1), 54–63. [Google Scholar] [CrossRef] [PubMed]
- Teruya-Feldstein, J. Diffuse Large B-cell Lymphomas with Plasmablastic Differentiation. Curr Oncol Rep. 2005, 7, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Bhatt R, Naha K, Desai DS. Plasmablastic Lymphoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 17, 2024.
- Delecluse, HJ; Anagnostopoulos, I; Dallenbach, F; Hummel, M; Marafioti, T; Schneider, U; et al. Plasmablastic lymphomas of the oral cavity: a new entity associated with the human immunodeficiency virus infection. Blood 1997, 89(4), 1413–20. [Google Scholar] [CrossRef]
- Chen, BJ; Chuang, SS. Lymphoid Neoplasms With Plasmablastic Differentiation: A Comprehensive Review and Diagnostic Approaches. Adv Anat Pathol. 2020, 27(2), 61–74. [Google Scholar] [CrossRef] [PubMed]
- Hatzimichael, E; Papathanasiou, K; Zerdes, I; Flindris, S; Papoudou-Bai, A; Kapsali, E. Plasmablastic Lymphoma with Coexistence of Chronic Lymphocytic Leukemia in an Immunocompetent Patient: A Case Report and Mini-Review. Case Rep Hematol. 2017, 2017, 1–5. [Google Scholar] [CrossRef]
- Pan, Z; Xie, Q; Repertinger, S; Richendollar, BG; Chan, WC; Huang, Q. Plasmablastic transformation of low-grade CD5+ B-cell lymphoproliferative disorder with MYC gene rearrangements. Hum Pathol. 2013, 44(10), 2139–2148. [Google Scholar] [CrossRef]
- Robak, T; Urbańska-Ryś, H; Strzelecka, B; Krykowski, E; Bartkowiak, J; Bĺoński, JZ; et al. Plasmablastic lymphoma in a patient with chronic lymphocytic leukemia heavily pretreated with cladribine (2-CdA): an unusual variant of Richter’s syndrome. Eur J Haematol. 2001, 67(5-6), 322–327. [Google Scholar] [CrossRef]
- Gasljevic, G; Grat, M; Kloboves Prevodnik, V; Grcar Kuzmanov, B; Gazic, B; Lovrecic, L; et al. Chronic Lymphocytic Leukemia with Divergent Richter’s Transformation into a Clonally Related Classical Hodgkin’s and Plasmablastic Lymphoma: A Case Report. Case Rep Oncol. 2020, 13(1), 120–129. [Google Scholar] [CrossRef]
- Martinez, D; Valera, A; Perez, NS; Villegas, LFS; Gonzalez-Farre, B; Sole, C; et al. Plasmablastic transformation of low-grade B-cell lymphomas: report on 6 cases. Am J Surg Pathol. 2013, 37(2), 272–281. [Google Scholar] [CrossRef] [PubMed]
- Loghavi, S; Alayed, K; Aladily, TN; Zuo, Z; Ng, SB; Tang, G; et al. Stage, age, and EBV status impact outcomes of plasmablastic lymphoma patients: a clinicopathologic analysis of 61 patients. J Hematol Oncol. 2015, 8(1), 65. [Google Scholar] [CrossRef] [PubMed]
- Castillo, JJ; Guerrero--Garcia, T; Baldini, F; Tchernonog, E; Cartron, G; Ninkovic, S; et al. Bortezomib plus EPOCH is effective as frontline treatment in patients with plasmablastic lymphoma. Br J Haematol. 2019, 184(4), 679–682. [Google Scholar] [CrossRef] [PubMed]
- Grimm, KE; O’Malley, DP. Aggressive B cell lymphomas in the 2017 revised WHO classification of tumors of hematopoietic and lymphoid tissues. Ann Diagn Pathol. 2019, 38, 6–10. [Google Scholar] [CrossRef]
- Ronchi, A; Marra, L; Frigeri, F; Botti, G; Franco, R; De Chiara, A. Richter Syndrome With Plasmablastic Lymphoma at Primary Diagnosis: A Case Report With a Review of the Literature. Appl Immunohistochem Mol Morphol 2017, 25(6), e40-5. [Google Scholar] [CrossRef]
- Ramsey, MC; Sabatini, PJB; Smith, AC; Sakhdari, A. Molecular characterization and clonal evolution in Richter transformation: Insights from a case of plasmablastic lymphoma (RT--PBL) arising from chronic lymphocytic leukaemia (CLL) and review of the literature. EJHaem 2023, 4(4), 1203–1207. [Google Scholar] [CrossRef]
- Chan, KL; Blombery, P; Jones, K; et al. Plasmablastic Richter transformation as a resistance mechanism for chronic lymphocytic leukaemia treated with BCR signalling inhibitors. Br J Haematol. 2017, 177(2), 324–328. [Google Scholar] [CrossRef]
- Garcia-Reyero, J; Martinez Magunacelaya, N; Gonzalez de Villambrosia, S; Loghavi, S; Gomez Mediavilla, A; Tonda, R; et al. Genetic lesions in MYC and STAT3 drive oncogenic transcription factor overexpression in plasmablastic lymphoma. Haematologica 2021, 106(4), 1120–1128. [Google Scholar] [CrossRef]
- van den Brand, M; Möbs, M; Otto, F; Kroeze, LI; Gonzalez de Castro, D; Stamatopoulos, K; et al. EuroClonality-NGS Recommendations for Evaluation of B-Cell Clonality Analysis by Next-Generation Sequencing. J Mol Diagnostics 2023, 25(10), 729–739. [Google Scholar] [CrossRef]
- Mazumder, S; Jinkala, S; Gochhait, D; Manivannan, P; Amalnath, D. Concomitant diagnosis of plasmablastic lymphoma and chronic lymphocytic leukemia: A rare phenomenon. Int J Appl Basic Med Res. 2021, 11(3), 201. [Google Scholar] [CrossRef]
- Holderness, BM; Malhotra, S; Levy, NB; Danilov, A V. Brentuximab vedotin demonstrates activity in a patient with plasmablastic lymphoma arising from a background of chronic lymphocytic leukemia. J Clin Oncol. 2013, 31(12), e197-9. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, P; Nayak-Kapoor, A; Reid-Nicholson, M; Jones-Crawford, J; Ustun, C. Plasmablastic lymphoma with small lymphocytic lymphoma: clinico-pathologic features, and review of the literature. Leuk Lymphoma 2008, 49(10), 1999–2002. [Google Scholar] [CrossRef] [PubMed]
- Marvyin, K; Tjønnfjord, EB; Breland, UM; Tjønnfjord, GE. Transformation to plasmablastic lymphoma in CLL upon ibrutinib treatment. BMJ Case Rep. 2020, 13(9), e235816. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Histopathological and immunophenotypic features of SLL and its transformation into PBL. (A–F) Representative images of SLL showing: (A) diffuse infiltrate of small mature lymphocytes with clumped chromatin (H&E); (B) diffuse CD20 positivity; (C) co-expression of CD5; (D) CD23 positivity; (E) absence of CD10 expression; (F) low Ki-67 proliferation index exceeded in prolipherative centers (G–L) Corresponding images of the transformed PBL showing: (G) diffuse sheets of large atypical cells with plasmablastic morphology (H&E); (H) loss of CD20 expression; (I) partial expression of CD5; (J) strong expression of plasma cell marker CD138; (K) diffuse and strong nuclear expression of MYC; (L) diffuse nuclear positivity for MUM1; Abbreviations: SLL, small lymphocytic lymphoma; PBL, plasmablastic lymphoma; H&E, hematoxylin and eosin; magnification, 40x.
Figure 1.
Histopathological and immunophenotypic features of SLL and its transformation into PBL. (A–F) Representative images of SLL showing: (A) diffuse infiltrate of small mature lymphocytes with clumped chromatin (H&E); (B) diffuse CD20 positivity; (C) co-expression of CD5; (D) CD23 positivity; (E) absence of CD10 expression; (F) low Ki-67 proliferation index exceeded in prolipherative centers (G–L) Corresponding images of the transformed PBL showing: (G) diffuse sheets of large atypical cells with plasmablastic morphology (H&E); (H) loss of CD20 expression; (I) partial expression of CD5; (J) strong expression of plasma cell marker CD138; (K) diffuse and strong nuclear expression of MYC; (L) diffuse nuclear positivity for MUM1; Abbreviations: SLL, small lymphocytic lymphoma; PBL, plasmablastic lymphoma; H&E, hematoxylin and eosin; magnification, 40x.
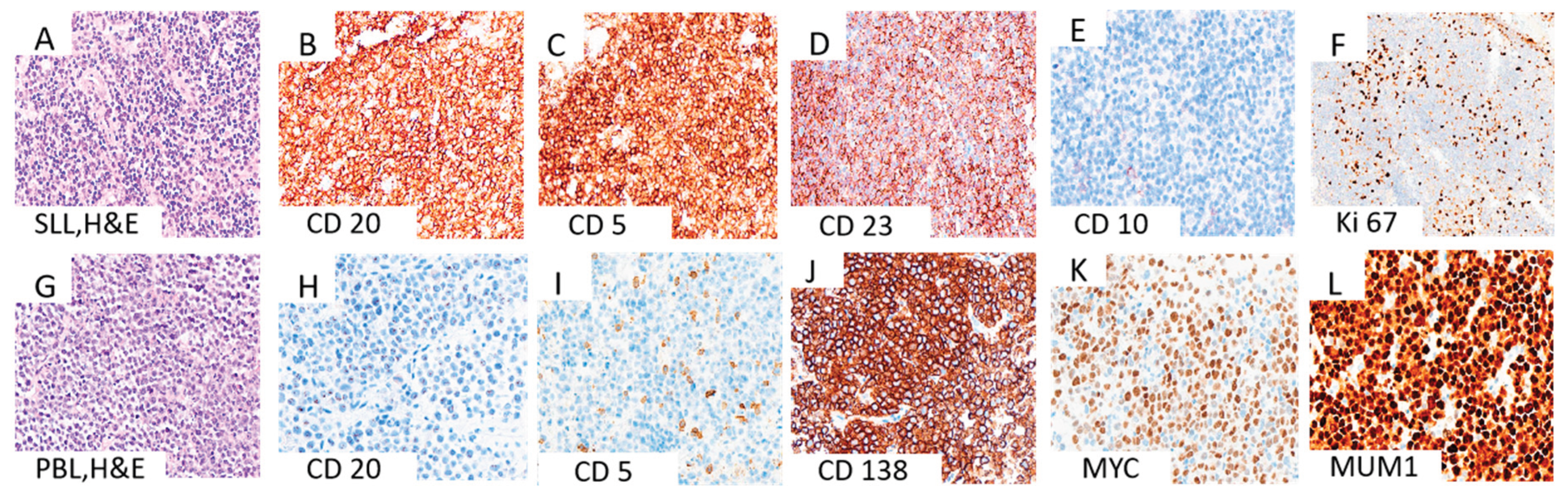
Figure 2.
A supportive finding for the diagnosis of PBL with kappa light chain restriction. Immunohistochemically, diffuse cytoplasmic staining for kappa light chain is observed in the majority of neoplastic cells (A), while no lambda expression is detected (B). Abbreviations: PBL, plasmablastic lymphoma; magnification, 40x.
Figure 2.
A supportive finding for the diagnosis of PBL with kappa light chain restriction. Immunohistochemically, diffuse cytoplasmic staining for kappa light chain is observed in the majority of neoplastic cells (A), while no lambda expression is detected (B). Abbreviations: PBL, plasmablastic lymphoma; magnification, 40x.
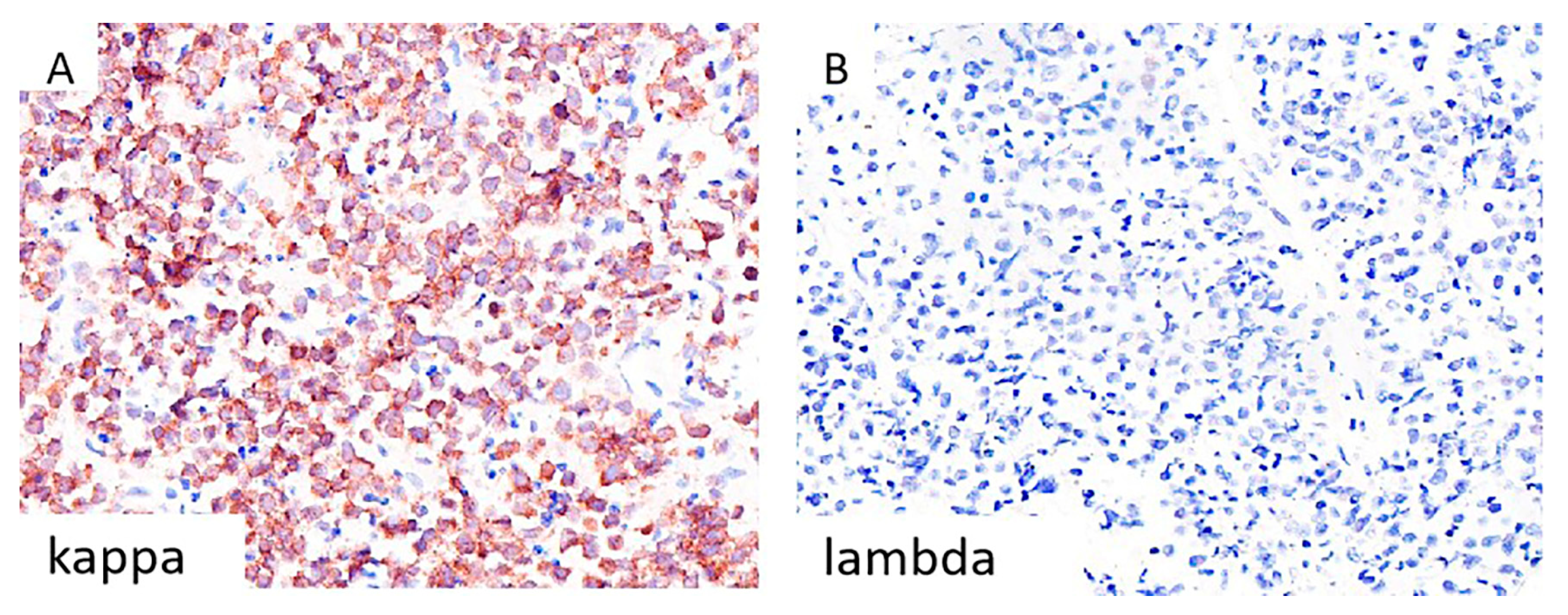
Figure 3.
Representative FISH images using break-apart probes (MetaSystems) for MYC (8q24), BCL6 (3q27), and BCL2 (18q21). A)The MYC probe demonstrates a break-apart signal pattern indicative of a MYC rearrangement. In contrast, B) the BCL6 and C) BCL2 probes show fused signals, consistent with the absence of BCL6 and BCL2 gene rearrangements; Abbreviation: FISH, fluorescence in situ hybridization;.
Figure 3.
Representative FISH images using break-apart probes (MetaSystems) for MYC (8q24), BCL6 (3q27), and BCL2 (18q21). A)The MYC probe demonstrates a break-apart signal pattern indicative of a MYC rearrangement. In contrast, B) the BCL6 and C) BCL2 probes show fused signals, consistent with the absence of BCL6 and BCL2 gene rearrangements; Abbreviation: FISH, fluorescence in situ hybridization;.
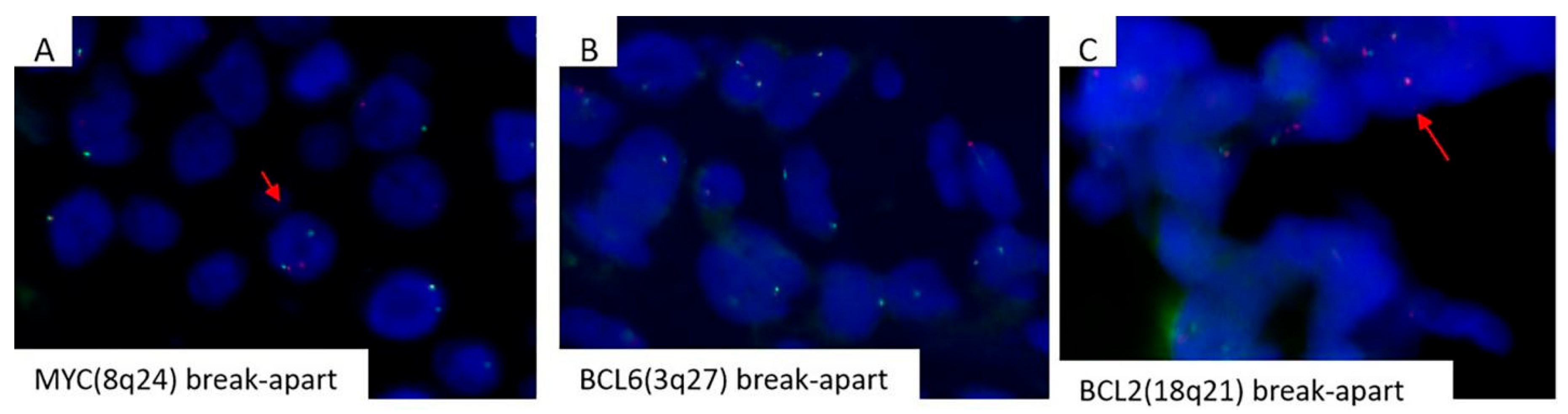
Figure 4.
Graphical representation of B clonality (IgH locus) results. Y axis: fragments height in fluorescence intensity ; X axis: fragments size in base-pairs (size of the expected fragments: VH-FR1-JH 310-360 ; VH-FR2-JH 250-295 ; VH-FR3-JH 100-170). Peak sizes are shown in boxes. A. Polyclonal control (Gaussian distribution of the size of the fragments amplified), B. Positive control (presence of a clonal rearrangement (1 peak) in the FR1, FR2 and FR3 region), C. Lymph-node biopsy (presence of a clonal rearrangement (2 peaks) in the FR1, FR2 and FR3 region), D. Retro-peritoneal biopsy (presence of the same clonal rearrangement (2 peaks of the same size) as in the lymph-node biopsy). Abbreviations: IgH, immunoglobulin heavy chain; VH, variable region of heavy chain; FR, framework region; JH, joining region of heavy chain.
Figure 4.
Graphical representation of B clonality (IgH locus) results. Y axis: fragments height in fluorescence intensity ; X axis: fragments size in base-pairs (size of the expected fragments: VH-FR1-JH 310-360 ; VH-FR2-JH 250-295 ; VH-FR3-JH 100-170). Peak sizes are shown in boxes. A. Polyclonal control (Gaussian distribution of the size of the fragments amplified), B. Positive control (presence of a clonal rearrangement (1 peak) in the FR1, FR2 and FR3 region), C. Lymph-node biopsy (presence of a clonal rearrangement (2 peaks) in the FR1, FR2 and FR3 region), D. Retro-peritoneal biopsy (presence of the same clonal rearrangement (2 peaks of the same size) as in the lymph-node biopsy). Abbreviations: IgH, immunoglobulin heavy chain; VH, variable region of heavy chain; FR, framework region; JH, joining region of heavy chain.
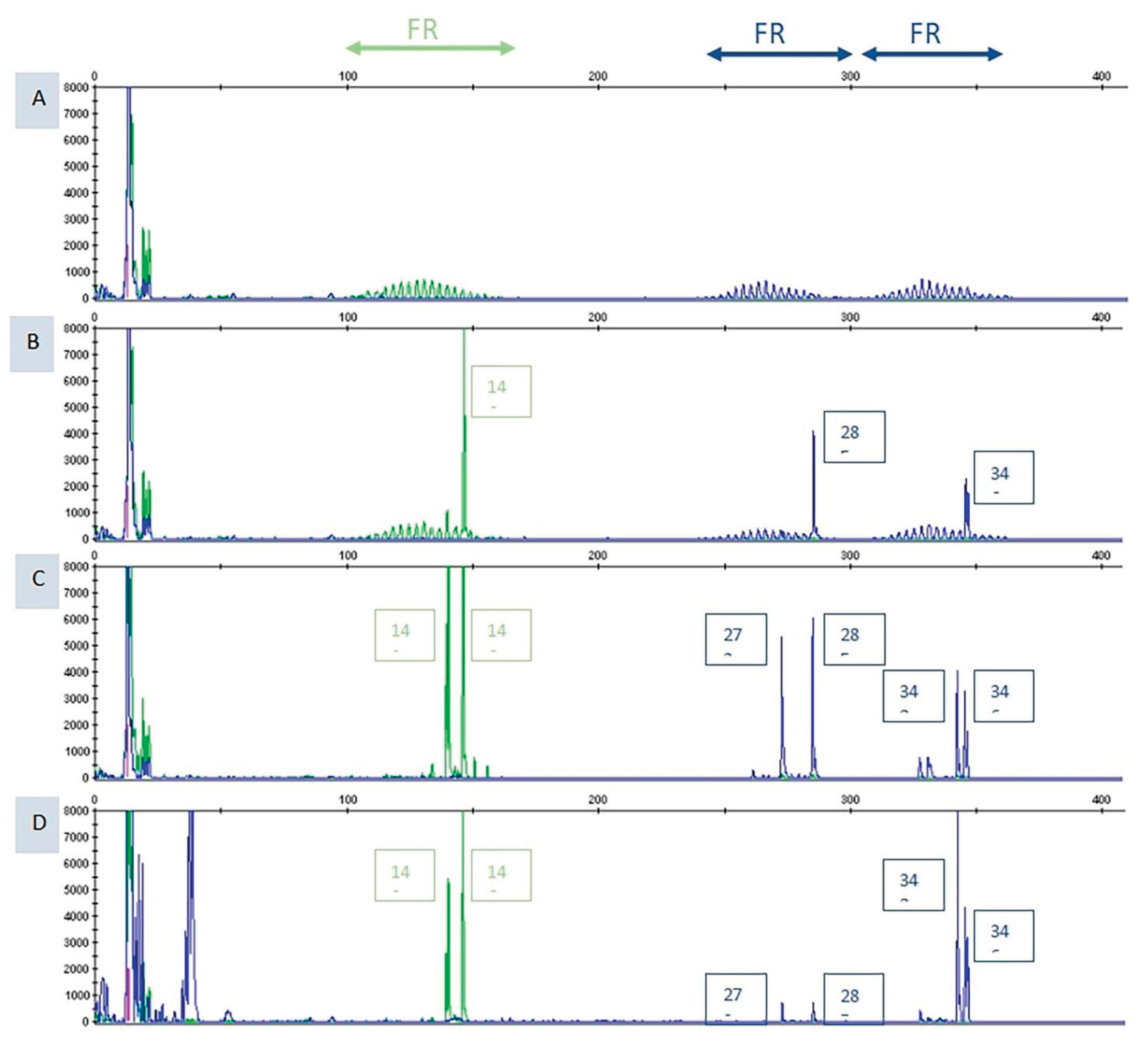

Table 1.
Overview of clinical and pathological features of reported transformation cases from CLL/SLL to PBL that were diagnosed simultaneously (under 6 months between diagnosis).
Table 1.
Overview of clinical and pathological features of reported transformation cases from CLL/SLL to PBL that were diagnosed simultaneously (under 6 months between diagnosis).
| Reference | Gender and age | HIV, EBV, HHV-8 | Diagnostic methods | Bone marrow involvement | FISH analysis (MYC rearrangements, bcl-2 and bcl-6) | Primary localisation | Therapy and outcome |
| Our case | Female, 46 yrs | Negative | PET, LN biopsy (HE, IHC), flow cytometry, ISH, FISH, NGS | N/A | MYC rearrangements | Concurrent diagnosis of CLL/SLL and PBL in same axillary LN | Dara-CHOP (6x), autologous bone marrow transplantation, Dara-CHOP (4x), daratumumab, ibrutinib |
| (Khanna et al., 2023) : 2 cases |
Case 1: Female, elderly patient |
Case 1: HIV others N/A | Case 1: BM biopsy (HE, IHC), flow cytometry, cytogenetic studies, FISH, transcriptome sequencing, PET | Consistent with CLL/SLL | Case 1: t (2;3) in CLL and PBL, MYC-IGH fusion t (8;14) and t (1;6) in PBL |
Case 1: 1 month, pleural fluid |
Case 1: daratumumab, R-CHOP -patient died, survilance N/A |
| (Ronchi et al., 2016) | Male, 61 yrs | Negative | Ultrasonography, axillary LN biopsy (HE, IHC), CT, PET, FISH | Both CLL/SLL and PBL | MYC gene rearrangement and translocation not documented | Concurrent diagnosis of CLL/SLL and PBL in same left supraclavicular LN | Hyper-C-PAD -patient died several months after initial diagnosis |
| (Martinez et al., 2012): 3 cases | Case 1: Male, 70 yrs | Negative | Biopsies (HE, IHC), ISH, cytogenetic analysis, FISH | Case 1: Yes | N/A |
Case 1: simultaneously, mesenteric LN | Case 1: R-CHOP (2x) -patient died 4 months after diagnosis |
| (Ramalingam et al., 2008) | Male, 42 yrs | HHV-8 positive | CT scan, MRI, mediastinal biopsy and BM (HE, IHC), flow cytometry, cytogenetic analysis | Yes | N/A | Concurrent diagnosis of CLL/SLL and PBL in bone marrow | High dose steroids, radiation of mediastinal mass, CHOP, hyper-CVAD, intrathecal cytarabine -patient died in 3 months |
Abbreviations: yrs – years; HIV – human immunodeficiency virus; EBV – Epstein–Barr virus; HHV-8 – human herpesvirus 8; PET – positron emission tomography; LN – lymph node; HE – haematoxylin and eosin; IHC – immunohistochemistry; ISH – in situ hybridisation; FISH – fluorescence in situ hybridisation; NGS – next-generation sequencing; BM – bone marrow; MYC – MYC proto-oncogene; BCL2 – B-cell lymphoma 2; BCL6 – B-cell lymphoma 6; CLL – chronic lymphocytic leukaemia; SLL – small lymphocytic lymphoma; PBL – plasmablastic lymphoma; Dara-CHOP – daratumumab plus cyclophosphamide, doxorubicin, vincristine, prednisone; R-CHOP – rituximab plus CHOP regimen; Hyper-C-PAD – hyperfractionated cyclophosphamide, cisplatin, doxorubicin, dexamethasone; Hyper-CVAD – hyperfractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone; RT – Richter’s transformation; N/A – not available.
Table 2.
Table 2. Overview of clinical and pathological features of reported transformation cases from CLL/SLL to PBL that were not diagnosed simultaneously (more than 6 months between diagnosis).
Table 2.
Table 2. Overview of clinical and pathological features of reported transformation cases from CLL/SLL to PBL that were not diagnosed simultaneously (more than 6 months between diagnosis).
| Reference | Gender and age | HIV, EBV, HHV-8 | Diagnostic methods | Bone marrow involvement | FISH analysis (MYC rearrangements, bcl-2 and bcl-6) | Time and localisation | Therapy and outcome |
| (Khanna et al., 2023): 2 cases | Case 2: elderly patient |
Case 2: EBV positive Others N/A |
Case 2: BM biopsy (HE, IHC), flow cytometry, PCR, CT scan | Consistent with CLL/SLL | Case 2: N/A | Case 2: Five years, pleural fluid |
Case 2: R-CHOP (1x), DA-R-Velcade EPOCH* patient died, survilance N/A |
| (Ramsey et al., 2023) | Male, 71 yrs | HIV N/A Others N/A |
BM biopsy, CT scan, LN biopsy, FISH, NGS | CLL/SLL | MYC rearrangement | 14 months, LN | CHOP (2x) -patient died after 4 months |
| (Marvyn et al., 2020) | Male, 53 yrs | HHV-8 Others N/A | LN and BM biopsies, genetic analysis, CT scan | Yes first CLL, later PBL | N/A | 7 years, bone marrow | COP regimen with added daratumumab from second cycle ** -patient died, survilance N/A |
| (Gasljevic et al., 2020) | Female, 74 yrs | HIV N/A, HHV-8 N/A | BM biopsy (HE, IHC), FISH, PCR, comparative genomic hybridization (CGH) | Yes CLL/SLL and later PBL |
No MYC rearrangements | 7 years cHL withmixed cellularity in inguinal LN but PBL in bone marrow | No therapy*** -patient died 2-3 weeks after LN biopsy |
| (Chan et al., 2017): 2 cases | Case 1: Male, 63 yrs Case 2: Male, 67 yrs |
Both cases: HIV N/A | BM and mass biopsy, FISH, NGS | Yes | N/A |
Case 1: 8 years, anal mass Case 2: 7 years, retroperitoneal LN |
Salvage chemotherapy -Case 1: patient died 2 weeks after PBL diagnosis -Case 2: patient died 12 weeks after PBL diagnosis |
| (Pan et al., 2013): 2 cases | Case 1: Male, 58 yrs Case 2: Male, 7 yrs |
Case 1: Negative Case 2: Negative |
LN and BM biopsy (HE, IHC), flow cytometry, cytogenetic studies, FISH, genetic studies | Case 1: Yes Case 2: Yes |
Case 1: CLL negative and PBL positive for MYC rearrangement Case 2: MYC rearrangement |
Case 1: 2 years, ulcerated mass at the gastroesophageal junction and bone marrow. Case 2: Diagnosed with low grade CD5+ LPD, after five years PBL left humerus |
Case 1: N/A -patient died after 3 months Case 2: localized radiotherapy and chemotherapy -patient stable |
| (Martinez et al., 2012) : 3 cases | Case 2: Male, 52 yrs Case 3: Female, 57 yrs |
EBV positive in case 2 | Biopsies (HE, IHC), ISH, cytogenetic analysis, FISH | Both cases: Yes | Case 2: N/A Case 3: N/A |
Case 2: 85 months, subcutaneous tissue Case 3:47 months, mandibula |
Case 2: R-CHOP (6x) -patient died 24 months after diagnosis of transformation Case 3: VAD (1x) and CHOP (3x) -patient died 6 months after diagnosis of transformation |
* Breast carcinoma treated with chemotherapy; therapy for SLL/CLL - bendamustine and rituxan. ** History of prostate cancer treated with hormone and radiotherapy; first therapy for CLL/SLL - fludarabine and cyclophosphamide; second therapy for CLL/SLL - fludarabine, cyclophosphamide and rituximab (6x) added ibrutinib. *** Early therapy - rituximab-chlorambucil with pegfilgrastim.for CLL/SLL. Abbreviations: yrs – years; HIV – human immunodeficiency virus; EBV – Epstein–Barr virus; HHV-8 – human herpesvirus 8; BM – bone marrow; HE – haematoxylin and eosin; IHC – immunohistochemistry; ISH – in situ hybridisation; FISH – fluorescence in situ hybridisation; NGS – next-generation sequencing; LN – lymph node; MYC – MYC proto-oncogene; BCL2 – B-cell lymphoma 2; BCL6 – B-cell lymphoma 6; cHL – classical Hodgkin lymphoma; PBL – plasmablastic lymphoma; CLL – chronic lymphocytic leukaemia; SLL – small lymphocytic lymphoma; LPD – lymphoproliferative disorder; COP – cyclophosphamide, vincristine, prednisone; CHOP – cyclophosphamide, doxorubicin, vincristine, prednisone; R-CHOP – rituximab plus CHOP regimen; DA-R-Velcade EPOCH – daratumumab, rituximab plus Velcade, etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin; VAD – vincristine, doxorubicin, dexamethasone; N/A – not available.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



