
Submitted:
07 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
Liver fibrosis, the progressive accumulation of scar tissue resulting from chronic liver disease, is increasingly recognized as a multi-system condition whose effects transcend the liver, affecting brain health. In parallel, dementia determining progressively impaired cognition severe enough to impede daily functioning, is a significant global health issue whose risk factors and pathogenic precursors are incompletely defined. Increasing evidence suggests that certain pathophysiological correlates of chronic liver disease may negatively affect neuronal health through incompletely defined pathophysiological mechanisms. With this background, we appraise our current understanding of the relationship between liver fibrosis and cognitive impairment/dementia, using a variety of different methodologies. Firstly, the pathophysiology and clinical significance of liver fibrosis are discussed. Next, we describe the various types of dementia and related risk factors. We then present research evidence supporting the association between cognitive impairment/dementia and liver fibrosis. We highlight both consistency and heterogeneity of findings, including the degree of association being affected by liver fibrosis severity. We thoroughly examine potential causal mechanisms, comprising the role of chronic systemic and neuroinflammation, insulin resistance, vascular dysfunction, and intestinal microbiota-liver-brain axis as potential connectors of liver health with cognitive impairment and dementia. We briefly analyze how sex and age may modify the above associations, how liver fibrosis and cognitive function should be diagnosed, and those potential preventive/treatment strategies based on the shared metabolic/inflammatory pathways associating liver fibrosis, cognitive impairment and dementia. Finally, major research gaps are identified, together with matching proposals for prioritizing advancements in our understanding of the increasingly identified connections between liver fibrosis and dementia/cognitive impairment.
Keywords:
cognitive impairment
; dementia
; liver–brain axis
; liver fibrosis
; metabolic dysfunction
; neuroinflammation
; MASLD
; gut–liver–brain axis
; vascular dysfunction
; non‐invasive biomarkers
1. Introduction
Liver fibrosis is the final consequence of repeated cycles of tissue damage and repair associated with chronic liver disease (CLD) regardless of etiology and is now being recognized as an important global health issue. Its incidence is increasing with the growing prevalence of metabolic dysfunction, older populations, and the burden of CLD related to alcohol and viral hepatitis [1]. Although historically described as a disease of exclusive hepatological significance, liver fibrosis exerts a considerable systemic impact on metabolic, cardiovascular, immune, and renal health, which largely transcends the liver [2,3] and may also participate in central nervous system outcomes, including cognitive dysfunction and dementia [4].
Dementia, including Alzheimer's disease and vascular dementia, is now one of the greatest public health challenges worldwide, affecting over 57 million individuals in 2019 and expected to rise to approximately 152 million by 2050 [5]. The pathophysiology of dementia is complex and multifactorial, including amyloid deposition, tau aggregation, neuroinflammation, microvascular dysfunction, and metabolic dysfunction [6]. Numerous underlying mechanisms are characterized by common biological pathways that become activated in cases of chronic liver injury, thereby providing a logical foundation for the existence of a liver–brain connecting axis [7]. For example, systemic inflammation, impaired ammonia metabolism, altered lipid and glucose pathways, and intestinal dysbiosis are not only well-characterized occurrences in advanced CLD but are also considered factors contributing to neurodegeneration and cerebrovascular injury [8].
Only recently have studies specifically focused on the association between asymptomatic fibrosis detected by non-invasive methods in individuals without clinically overt cirrhosis (namely subclinical liver fibrosis) and long-term cognitive outcomes.
Several large population studies now indicate that liver fibrosis, even with the backset of non-cirrhotic livers, can be potentially associated with and increased risk of more rapidly progressive cognitive impairment and dementia [9,10]. This observation conceptualizes liver fibrosis as an important systemic determinant of brain aging rather than a condition of exclusive hepatological interest. However, our understanding of the putative pathophysiological mechanisms, the epidemiological evidence for the strength of association, and the degree to which liver-related biomarkers can refine dementia risk stratification, remains limited. Accordingly, the purpose of this review is to summarize the existing epidemiological, mechanistic, and clinical evidence to clarify the relationship between liver fibrosis and dementia, and to identify relevant future directions that may potentially enhance early identification and treatment options in research and practice.
2. Methods
We conducted a thorough literature search on PubMed to find studies that examine the connection between liver fibrosis and cognitive outcomes, including dementia and related neurodegenerative conditions. To ensure comprehensive and methodologically sound coverage, controlled vocabulary (MeSH terms) was utilized along with a wide range of titles and abstract keywords related to both liver fibrosis diagnostics and major dementia syndromes.
In the search for liver-related studies, we included the MeSH term “liver” along with MeSH headings on elasticity imaging techniques, biopsy, and fibrosis. Additionally, we used title and abstract keywords to capture non-invasive fibrosis methods and related terms such as biopsy, fibrosis, cirrhosis, stiffness, elastography, acoustic radiation force impulse imaging, FibroScan, acoustography, vibroacoustography, and sonoelastography.
For cognitive and neurodegenerative outcomes, the MeSH term “Dementia” was incorporated and the search expanded to include a wide range of dementia-related conditions and synonyms used in the title and abstract fields. This encompassed common ley words such as Alzheimer’s disease, vascular dementia, and frontotemporal lobar degeneration, as well as less common neurodegenerative, prion-related, and hereditary dementias such as CADASIL, Binswanger encephalopathy, Creutzfeldt–Jakob disease, progressive aphasia, tauopathies, neuronal ceroid lipofuscinosis, fatal familial insomnia, Huntington disease, and related disorders. These terms were chosen to ensure that all forms of cognitive impairment potentially linked to hepatic pathology were included.
The search was limited to human studies, publications in English, and adult populations, with no restrictions on study design. To cover historical evidence while including the most recent research a publication date filter from January 1, 1900, to November 30, 2025 was applied. The research was structured using Boolean operators to maximize the retrieval of studies on the intersection of liver fibrosis and cognitive impairment, maintaining specificity using MeSH terms and targeted keywords such as illustrated analytically in Table A1.
3. Liver Fibrosis: Pathophysiology and Clinical Relevance
3.1. Stages
Liver fibrosis involves excessive buildup of extracellular matrix (ECM) proteins like collagen. While reversible, it may progress to cirrhosis, portal hypertension, and liver failure [11,12]. Fibrosis stages range from F0 (none) through F4 (cirrhosis) [13], with significant fibrosis at F≥2 and advanced fibrosis at F≥3—important for comparing assessment methods [14].
3.2. Prevalence and Risk Factors
The prevalence rates of advanced fibrosis and cirrhosis in both sexes are shown in Table 1.
Additionally, the prevalence of cirrhosis varies significantly among continents [1]. Figure 1 illustrates the principal risk factors for advanced liver fibrosis and cirrhosis [1]. Alarmingly, the prevalence of advanced fibrosis has increased over time from 2.0% before 2010 to 4.7% after 2016 [1] indicating an increasing burden at the level of the general population and clinically.
3.3. Pathomechanisms of Liver Fibrosis
Extra-hepatic and hepatic determinants drive liver fibrosis by activating hepatic stellate cells (HSCs) through their differentiation into myofibroblasts and secretion of ECM [17]. Visceral obesity contributes to hepatic fibrogenesis through lipotoxic and proinflammatory pathomechanisms involving genetics and epigenetics, altered adipokine profile, oxidative stress, endoplasmic reticulum stress, and apoptosis [18,19]. The gut-liver axis significantly contributes to the histogenesis of cirrhosis through increased intestinal permeability, facilitated by gut dysbiosis, enabling bacteria to flow to the liver via the portal route [20], activating Kupffer cells via Toll-like receptor 4, and eventually leading to cytokine production, HSC activation, and liver fibrosis [21].
During fibrosis, immune cells and HSCs interact bi-directionally. Activated macrophages and neutrophils release signals that trigger HSC activation via inflammation [22]. “Hot” fibrosis exhibits immune cell infiltration and inflammation, while “cold fibrosis” is defined by minimal immune presence [23]. Gene variants like PNPLA3 and cell stress responses play key roles in both development and reversal of fibrosis [24,25]. HSCs experience stressors such as the unfolded protein response and oxidative stress, which prompt compensatory signaling [25]. Of concern, liver fibrosis also increases the risk of hepatocellular carcinoma [26].
3.4. Liver Fibrosis and Extrahepatic Outcomes
Liver fibrosis dictates the natural course of liver-related outcomes and is a key modifier of systemic health and extra-hepatic events [27], including all-cause mortality [28], incident diabetes [29,30], major adverse cardiovascular events [31], extra-hepatic cancers [32-34] and chronic kidney disease [35]. In this evolving scenario, Jamalinia et al. have recently found that liver fibrosis is associated with a 32% long-term increased risk of dementia, irrespective of confounders, and that the severity of fibrosis worsens this risk [4].
4. Dementia: Overview
4.1. Definitions and Spectrum
Dementia is characterized by a progressive impairment in cognitive abilities, including deficits in memory, executive function, language, visuospatial skills, and behavior. These impairments are significant enough to compromise daily independence, impacting essential activities such as self-care, monetary management, and household maintenance [36]. Rather than a disease in itself, dementia, is a heterogeneous syndrome of distinct disorders that are characterized by distinct pathophysiologic processes [37].
Alzheimer's disease (AD) is the most common subtype of dementia, comprising two-thirds of cases, and is defined by the presence of β-amyloid plaques and neurofibrillary tangles formed from hyperphosphorylated tau [38]. Vascular dementia (VaD), the second most common type of dementia, results from microvascular cerebral pathology that encompassing small vessel disease, lacunar infarcts, and microbleeds [39]. Several other subtypes of dementia, including dementia with Lewy bodies [40], frontotemporal dementia [41], and mixed dementias, are particularly common in older individuals in whom processes of neurodegeneration and vascular pathology often coexist [42]. Parkinson's disease (PD), the second most common neurodegenerative disorder after AD, is primarily a movement disorder. Many patients later develop PD dementia (PDD), usually years after PD diagnosis, particularly in those with late-onset, severe PD, mild cognitive impairment (MCI), depression, or sleep disorders[43-45]. Figure 2. Schematically illustrates the principal dementia subtypes.
Legend to Figure 2. – Spectrum of the main subtypes of dementia based on references cited in the text. Original illustration created using Servier Medical ART (SMART) and is licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0).
4.2. Pathophysiology and Risk Factors
The pathophysiology of dementia is multifactorial and involves complex interactions of neurodegenerative, inflammatory, and vascular processes [38]. In the case of AD, the accumulation of extracellular β-amyloid initiates a cascade of synaptic toxicity, oxidative stress, and microglial activation [46]. The abnormal phosphorylation of tau leads to impaired axonal transport, eventually inducing neuron dysfunction and death [47]. Neuroinflammation has emerged as a crucial player across the spectrum of dementia subtypes, as activated microglia and astrocytes secrete pro-inflammatory cytokines, enhancing neuron injury and impairing the clearance of toxic proteins [48,49]. Vascular pathology, including endothelial dysfunction, breakdown of the blood-brain barrier (BBB), cerebral hypoperfusion, and microvascular remodeling, plays an important role not only in VaD but also in accelerating cognitive impairment in AD [50,51]. Although each of these biological processes does not operate in isolation, they work together to alter neuronal health, synaptic connectivity, and brain network function, ultimately manifesting as clinical dementia.
There is also a wide range of modifiable and non-modifiable conditions that influence an individual’s progression to dementia. The strongest contributor remains age, with prevalence nearly doubling every 5 years after 65 [52]. Genetic risk, most commonly associated with the APOE ε4 allele genotype, significantly contributes to the risk of AD [53,54]. Cardio-metabolic risk factors and lifestyle habits, including atrial fibrillation, arterial hypertension, diabetes, dyslipidemia, obesity, and smoking, contribute to both AD and VaD, largely due to processes involving vascular injury, inflammation, and brain tissue hypoperfusion [55]. Other well-established risk factors include educational achievement, physical inactivity, social isolation, sensory deprivation, depression, and chronic systemic inflammation [56]. In addition to these established factors, metabolic dysfunction-associated steatotic liver disease (MASLD), through its associated metabolic dysfunction, systemic inflammation, and gut-liver-brain interactions, is increasingly identified as an emerging contributor to cognitive impairment, prompting research into the role of the liver in the pathogenesis of dementia [57,58].
5. Evidence Linking Liver Fibrosis and Dementia
5.1. Epidemiological Evidence
The epidemiological evidence linking liver fibrosis to dementia has significantly expanded over the past few years. Early insights came from cross-sectional studies showing that individuals with liver fibrosis perform poorly in cognitive domains relevant to dementia, such as executive function, attention, and memory. Additionally, they exhibit neuroimaging abnormalities like reduced cortical thickness, white-matter microstructural changes, and markers of cerebral small-vessel disease [59-62] (Table 2). These initial observations laid the groundwork for subsequent longitudinal cohort analyses.
In recent years, an increasing number of population-based cohort studies have investigated whether liver fibrosis predicts incident dementia [4]. However, these studies have not produced entirely consistent results [4]. While some large cohorts have reported a significant positive association between fibrosis and later dementia [9,10,63,64], others have found non-significant relationships [66-68]. These discrepancies likely reflect differences in population characteristics, methods of diagnosing fibrosis (e.g., non-invasive scores vs. imaging-based assessment), duration of follow-up, methods used to ascertain dementia, and residual confounding [4].
To address the uncertainties arising from these diverse findings, a recent meta-analysis was conducted, providing the most comprehensive and statistically powerful evaluation to date [4]. This analysis included eight cohort studies, involving approximately 1.1 million individuals, with around ~ 31,000 having liver fibrosis at baseline. Over an average follow-up period of 14 years, approximately 30,000 incident dementia cases were recorded [4]. The combined results showed that liver fibrosis was linked to a roughly 30% increased risk of dementia (pooled HR 1.32; 95% CI 1.08–1.61), independent of demographic, socioeconomic, anthropometric, and cardiometabolic factors [4].
Importantly, the risk of dementia increased progressively in parallel with the severity of liver fibrosis [4]. Pooled estimates revealed rising hazard ratios across fibrosis stages: HR 1.06 (95% CI 0.67–1.68) for ≥F2, HR 1.32 (95% CI 1.06–1.64) for ≥F3, and HR 1.69 (95% CI 1.01–2.83) for F4 [4]. Sensitivity analyses, limited to studies with maximum covariate adjustments confirmed the strength and independence of this association (n=5 studies; pooled HR 1.29, 95% CI 1.07–1.56) [4]. Overall, these findings establish liver fibrosis as an independent and clinically significant predictor of long-term dementia risk, providing the most compelling epidemiological evidence to date for this emerging liver-brain pathogenic axis [4].
5.2. Mechanistic Insights
Liver fibrosis contributes to dementia through interconnected pathways involving neuroinflammation, insulin resistance, vascular dysfunction, oxidative stress, and perturbed gut–liver–brain axis. These heterogeneous pathomechanisms are schematically illustrated in Figure 3.
5.2.1. Liver-Brain Axis: Neuroinflammation, Insulin Resistance, and Vascular Dysfunction
Fibrotic liver injury triggers a chronic inflammatory environment in which activated Kupffer and HSCs release tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and C-reactive protein (CRP) [68,69]. These substances can easily pass through the BBB and activate microglia, tipping the balance towards a pro-inflammatory state. Microglial activation accelerates the aggregation and deposition of β-amyloid and hyperphosphorylation of tau, which promotes an Alzheimer-type pathology [70]. Additionally, systemic insulin resistance, a hallmark of metabolic dysfunction-associated steatotic liver disease (MASLD), impairs insulin receptor signaling in neurons, decreases brain glucose uptake, and exacerbates mitochondrial dysfunction. Cerebrovascular damage acts as a third contributing factor [71]. Specifically, portal hypertension and endotoxemia increase levels of vasoconstrictors like endothelin-1, while reducing nitric oxide availability [68]. This results in endothelial dysfunction and small vessel disease, leading to clinical manifestations such as white matter hyperintensities and lacunar infarcts [69]. These combined processes create an unfavorable cerebral environment that heightens the risks of neurodegeneration, explaining why more severe stages of fibrosis are linked with a higher risk of dementia in epidemiological studies [63,72].
5.2.2. Metabolic Dysregulation and Oxidative Stress
Beyond its inflammatory effects, chronic liver injury is often accompanied by profound alterations in systemic metabolic function that vary based on the etiology of CLD. MASLD, for example, the prototypic hepatic manifestation of metabolic dysfunction, disrupts lipid handling, resulting in atherogenic dyslipidemia characterized by elevated very-low-density lipoprotein particles (VLDL), low HDL-cholesterol, and oxidized low-density lipoprotein (LDL)[73,74]. These lipoproteins can accumulate in cerebral vessels and brain parenchyma, further amplifying oxidative stress [75]. Meanwhile, impaired hepatic β-oxidation leads to the spill-over of free fatty acids, which activate NADPH oxidase and produce reactive oxygen species (ROS) both in the liver and peripherally [76,77]. ROS rapidly deplete antioxidants such as glutathione and superoxide dismutase, leaving neurons susceptible to peroxidative injury [78,79]. Compounding this vulnerability, fibrotic livers exhibit impaired capacity to synthesize ceruloplasmin and transferrin, resulting in dysregulated iron and copper metabolism. These elements catalyze Fenton reactions and exacerbate oxidative DNA damage in neural tissue [80]. Collectively, these metabolic derangements create a systemic pro-oxidant state that synergizes with neuroinflammation to accelerate neuronal apoptosis and synaptic loss [70].
5.2.3. Gut-Liver-Brain Axis: Intestinal Microbiota, Endotoxins, and Ammonia
The intestinal microbiota serves as an increasingly recognized connection between hepatic and cerebral pathology [81]. During liver fibrosis, intestinal permeability increases due to portal hypertension and mucosal congestion, allowing bacterial products like lipopolysaccharide (LPS) and peptidoglycan to invade the portal and systemic circulation [81]. LPS activates Toll-like receptor-4 on Kupffer cells, intensifying hepatic inflammation while simultaneously weakening the BBB through cytokine-mediated disruption of tight junctions [82]. Gut dysbiosis also leads to the overgrowth of urease-producing bacteria that release ammonia. Although blood levels of ammonia do not necessarily predict clinical symptoms, chronic low-grade exposure can interfere with astrocytic glutamine synthetase and disrupt neurotransmission [83]. Additionally, microbial metabolites like trimethylamine-N-oxide (TMAO) can increase platelet reactivity and vascular inflammation, connecting gut changes to both hepatic and cerebrovascular damage [84]. The decreased production of short-chain fatty acids such as butyrate eliminates an essential anti-inflammatory and neurotrophic signal, further shifting the balance towards neurodegeneration [85,86]. Therefore, the gut-liver-brain axis offers a biologically plausible mechanistic explanation for how liver fibrosis can impact cognitive health to a substantial extent.
5.3. Sex and Age Differences
Sex and age are key factors in shaping the relationship between liver fibrosis and dementia, influencing both conditions through biological, hormonal, and lifestyle mechanisms. Sex plays a role in the development of common types of CLD, such as MASLD, while also affecting the risk of dementia. Meanwhile age is a significant risk factor for both conditions, interacting with hormonal and genetic factors to influence the progression of dementia.
Sex and gender impact liver fibrosis through various factors like genetics, hormones, immune response, metabolism, and lifestyle factors, including alcohol consumption, diet, physical activity, and hormone therapy [87]. Women have a higher risk and prevalence of AD compared to men, with notable differences in disease progression and response to treatment [88].
Age can accelerate liver disease progression and worsen cognitive issues by reducing liver volume and blood flow, impairing detoxification, and affecting metabolic function. These factors increase the risk of conditions like hepatic encephalopathy and neurodegenerative diseases [72,89]. Additionally, age-related hormonal changes, such as declining of androgens in men, can impact both liver and brain health simultaneously [90-93]. Aging also increases susceptibility to acute liver injury, fibrosis, and poor outcomes in CLD due to various factors [94]. Similarly, aging raised the risk of neurodegenerative diseases like AD and Parkinson's due to genomic instability, telomere shortening, epigenetic changes, proteostasis loss, mitochondrial dysfunction, cellular senescence, disrupted nutrient sensing, stem cell depletion, and altered cell communication [95]. Liver fibrosis may affect dementia risk differently based on age and sex [4]. Hormones like estrogen and androgen play a role in the risk of liver disease and dementia as individuals age [96,97]. In women, hormonal changes after menopause largely explain the increased risk of dementia in older age [98].
6. Diagnostic Considerations
6.1. Fibrosis Assessment
The risks and limitations of liver biopsy, an invasive diagnostic procedure that has been the standard for histological fibrosis assessment throughout the history of hepatology, have prompted research and validation of noninvasive tests (NITs) that can detect fibrosis and cirrhosis at asymptomatic stages [99-101]. The recent FDA initiative to consider proposals for using non-invasive test instead of liver histology as reference standard endpoints (RLSEs) provides strong motivation for the adoption of non-invasive tests in drug development for metabolic dysfunction-associated steatohepatitis [102]. Figure 4 categorizes NITs for fibrosis as either blood-based or based on imaging techniques.
6.1.1. Blood-Based Non-Invasive Tests
The most thoroughly validated blood-based noninvasive tests include APRI, FIB-4, and ELF [101]. The practical benefits of these methods include applicability to over 95% of patients, reliable reproducibility, extensive accessibility, and, specifically for APRI and FIB-4, cost-effectiveness due to their calculation from routine blood tests[101]. However, these scores can be affected by confounding variables, such as age with FIB-4 and both age and extrahepatic fibroinflammatory changes with ELF [101,103]. A decreased accuracy of NIT is also observed among subjects with type 2 diabetes (T2D) because of different characteristics of this patient population, and owing to the effects of T2D itself on some NIT biomarkers of fibrosis[104]. Furthermore, the ELF test, being commercially available, is comparatively costly[101]. Table 3 summarizes the principal features of the blood-based indirect NITs.
6.1.2. Elastometry
Liver stiffness can be assessed through various ultrasound-based elastography techniques or magnetic resonance elastography (MRE) [109]. Liver stiffness measurements are reported in kilopascals (kPa), with values below 5 kPa considered within the normal range. These measurements are more prone to producing false positives than false negatives [101].
The practical benefits of VCTE include its point-of-care accessibility, straightforward learning curve, and consistent reliability, exceeding 95% when an extra-large probe is applied in patients without morbid obesity [110]. Nonetheless, it is essential to thoroughly account for potential confounding factors to prevent an inaccurate assessment of fibrosis [101].
6.1.3. Sequential Non-Invasive Assessment of Liver Fibrosis
A two-step protocol is typically applied to triage individuals displaying “red flags” for CLD. The protocol includes initial testing (APRI for individuals with viral hepatitis and FIB-4 for others) followed by secondary testing based on history, laboratory liver tests, and ultrasonography scanning [101]. The FIB-4 index uses low and high cutoffs to rule out or confirm advanced fibrosis, with values in between considered indeterminate[101,112,113]. Sequential combinations of markers with lower thresholds to exclude advanced fibrosis and higher thresholds to confirm cirrhosis can decrease the need for liver biopsies[114].
Patients with indeterminate or high FIB-4 scores should undergo further noninvasive testing (VCTE/MRE) or biopsy. VCTE is the most validated elastography method for detecting advanced fibrosis [101,115]. A liver stiffness under 15 kPa with platelet counts above 150,000/mm³ excludes significant portal hypertension, while stiffness over 25 kPa confirms portal hypertension in cirrhotic patients [101].
7. Cognitive Assessment and Biomarkers
7.1. Mini-Mental State Examination and Montreal Cognitive Assessment
The primary methods for diagnosing dementia include cognitive assessments such as the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA), which evaluate memory, orientation, and language abilities [116]. Both the MMSE and MoCA are appropriate cognitive assessment tools for monitoring changes in cognition [117]. A study of 803 German-speaking Memory Clinic outpatients discovered that MoCA scores were consistently lower than MMSE scores. The study also introduced a simple conversion table for comparing cognitive test results in patients with neurocognitive disorders [116].
7.2. Additional Diagnostic Techniques
Additional diagnostic approaches commonly involve neurological examinations, neuroimaging techniques such as CT and MRI scans, and, in certain cases, cerebrospinal fluid or blood tests to exclude alternative diagnoses and determine potential underlying causes [118].
Recent advances highlight fluid biomarkers as effective tools for detecting and characterizing cognitive impairment in clinical settings. These biomarkers may aid in earlier diagnosis, especially in cases of MCI or with comorbidities such as T2D. Table 4 presents recent meta-analytic reviews relevant to this subject.
7.3. Risk Prediction Models
Risk prediction models serve as validated clinical instruments designed to assess an individual's likelihood of developing dementia.
By utilizing demographic, metabolic, vascular, and lifestyle factors, these models help clinicians ranking patients based on their future cognitive risk. Validated dementia risk algorithms that assist clinicians in stratifying patients are listed in Table 5. It is important to note that none of these widely used models currently include any liver-related biomarkers or fibrosis measurements. However, a recent meta-analysis has shown that liver fibrosis is linked to cognitive impairment independently of the variables already used in these scores [4], suggesting that incorporating liver fibrosis parameters (such as VCTE-based stiffness values) into future risk models could lead to early identification of individuals at a heightened risk of dementia. Future studies should investigate whether incorporating liver fibrosis parameters could enhance risk prediction models.
8. Therapeutic and Preventive Implications
8.1. Liver-Directed Interventions: Lifestyle, Pharmacological, and Bariatric Approaches
Lifestyle modifications remain the cornerstone of antifibrotic therapy [130]. Sustained weight loss of 7-10%, achieved through Mediterranean-style diets and structured aerobic-resistance exercise regimens, can induce histologic fibrosis regression in up to one-third of patients [131]. Additionally, this approach improves executive function and memory scores on Montreal Cognitive Assessment (MoCA) testing [132]. Pharmacologically, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have become a primary focus. For example, semaglutide has been shown to reduce the histological activity of steatohepatitis, lower FIB-4 scores, and demonstrate preliminary slowing of cognitive impairment in T2D cohorts [133]. Farnesoid-X-receptor agonists like obeticholic acid and fibroblast growth factor-19 analogues (e.g., aldafermin) are currently undergoing phase III evaluation with secondary neurocognitive endpoints [134-136]. Bariatric surgery is the most effective and durable option for patients with morbid obesity and advanced fibrosis. Meta-analyses have indicated that Roux-en-Y gastric bypass and sleeve gastrectomy can reduce excess weight, total weight, cirrhosis progression, and decrease incident dementia by roughly 25-30% over a decade [137,138]. These effects are mediated by improvements in insulin sensitivity, reduced systemic inflammation, and favorable alterations in gut microbiota. It is crucial to monitor post-operative micronutrient levels to prevent B-vitamin deficiencies that could potentially negate cognitive gains [139,140].
8.2. Neuroprotective Potential of Liver-Focused Therapies
Mounting evidence suggests that therapies aimed at the liver can have direct and indirect neuroprotective effects. Resolving hepatic inflammation reduces systemic cytokine burden, decreases microglial activation, and preserves synaptic integrity[71]. Improved insulin sensitivity also boosts cerebral glucose uptake, supporting neuronal energy metabolism[141]. In animal models, GLP-1 RAs have been shown to cross the BBB, increase cyclic-AMP response-element binding protein (CREB) levels, and stimulate hippocampal neurogenesis [142]. Antioxidant agents like N-acetyl-cysteine, S-adenosyl-L-methionine, and manganese porphyrins are being investigated for their antifibrotic properties, as they can simultaneously reduce ROS levels in both the liver and brain [143,144]. Modulating the intestinal microbiota through high-fiber diets, prebiotics or, potentially, fecal microbiota transplantation can increase short-chain fatty acid production, which binds to G-protein-coupled receptors on microglia and promotes an anti-inflammatory response [145,146]. Taken together, these findings suggest that targeting hepatic fibrosis could potentially delay the onset or slow the progression of both AD type and vascular dementias. This hypothesis is currently being tested in umbrella trials that assess hepatic, metabolic and cognitive outcomes [147].
8.3. Multidisciplinary Care: Integrating Hepatology and Cognitive Medicine
Given the multifactorial nature of the fibrosis-dementia nexus, siloed care models are insufficient. An integrated pathway should begin with dual screening: non-invasive fibrosis assessment (using transient elastography or serum panels such as FIB-4) alongside cognitive testing (such as MoCA or digital neuropsychological batteries) in primary-care or diabetology settings [9,148]. Patients with either abnormality should be referred to combined hepatology-neurology clinics, where liver ultrasonography, MRE, and brain MRI with diffusion-tensor sequences can be ordered during a single visit.
Multidisciplinary teams, comprised of hepatologists, neurologists, endocrinologists, dietitians, and clinical psychologists, should collaborate to develop personalized care plans that address lifestyle factors (such as healthy diets, increased physical activity, and reduced sedentary time), pharmacotherapy, and psychosocial support [149,150]. Electronic health record dashboards should support real-time monitoring of liver stiffness, metabolic parameters, and cognitive scores, allowing for prompt adjustments to therapy. This integrated approach not only enhances the patient experience but also has the potential to identify treatable factors (such as obstructive sleep apnea or vitamin D deficiency) that impact both liver and cognitive function [151,152]. Additionally, public health campaigns focused on viral hepatitis vaccination, alcohol harm reduction, and metabolic syndrome screening could result in decreased rates of cirrhosis and dementia at a population-level, underpinning the interconnected nature of liver and brain health [153-156].
9. Gaps in Knowledge and Future Directions
Although evidence links liver fibrosis to increased dementia risk, key information is still missing to fully understand these connections and apply them clinically.
A key challenge is that the majority of existing epidemiological studies are based on indirect and non-invasive assessments of liver fibrosis [e.g., FIB-4 or NAFLD fibrosis score (NFS), which represent a significant potential for misclassification, and fail to capture changes in the temporal course of CLD, thus being exposed to the risk of under-representing the real relationship between liver fibrosis and cognitive impairment [4,157].
Establishing the temporal course of liver fibrosis development through longitudinal cohort studies with repeated, accurate and easily accessible assessments of fibrosis (with an emphasis on elastography) is necessary to characterize the relationship between liver fibrosis progression and cognitive loss [158].
Currently, the precise pathomechanisms by which liver fibrosis contributes to the development of dementia remain incompletely characterized.
Only a limited number of studies have examined the contribution of inflammatory, vascular, metabolic dysregulation, and gut-liver-brain pathways [159] although many potential mechanisms may be at play. We believe that multi-omic and imaging approaches may help determine the causal mediators of the relationship between liver disease and cognitive impairment, as well as the common pathways connecting them and identifying early biomarkers indicating susceptibility to neurodegeneration.
Another important unanswered question is related to patient population heterogeneity. The distribution of variables associated with sex, age, hormonal status, and genetic background in the population, which will affect liver disease development over time and the risk of developing dementia, is infrequently taken into account during the study design or analyses of the existing literature [4,160]. Additionally, the impact of various causes of CLD [MASLD, Alcohol-related Liver Disease (ALD) Metabolic dysfunction and ALD (MetALD)], viral hepatitis, and more rare etiologies) [161,162] is not well defined in existing studies, and stratified analyses based on the etiology of liver disease will likely uncover different risk characteristics and distinct disease mechanisms.
There are also more areas of therapeutic implications in need of investigation. It is unclear if lifestyle modifications, newer antifibrotic therapies, metabolic agents and/or bariatric surgery used to improve the liver's fibrotic state will reduce cognitive impairment. Therefore, studies with cognitive endpoints/cognition-related biomarkers should acertain test whether liver-based therapies would provide neuroprotective effects.
Another emerging area of data analytics is the utilization of machine learning and big data methodologies. By utilizing large data set approaches, which include electronic medical records with neuroimaging, genetic, and longitudinal cognitive data, we can improve predictive models of dementia risk in individuals with liver disease [163-165]. Nevertheless, thorough validation and standardization of these models is required prior to their implementation in routine clinical practice.
Bridging knowledge gaps on the link between fibrosing CLD and progressive cognitive impairment or dementia is essential for clarifying causality, improving risk assessment, and guiding prevention and treatment strategies for both liver and brain health.
10. Conclusions
The notion considering liver fibrosis as a fundamental parameter estimating uniquely the severity of hepatic injury is outdated. Presently, liver fibrosis is considered as a distinct systemic disorder with systemic implications, potentially impacting brain health. Growing evidence based on epidemiological and biological studies supports a substantive and non-chance association between the severity of liver fibrosis (notably including non-cirrhotic stages) and increased long-term risks of manifesting deteriorated cognitive functions/dementia, biological plausibility supports the association of these disorders. Shared mechanistic pathways involving chronic inflammation, metabolic dysfunction, endothelial/blood vessel damage, oxidative damage, and disruption of the gut-brain/liver axis highlight the interconnectedness of the aging liver and the dysfunctional brain.
The available data highlight the importance of early diagnosis of liver fibrosis, comprehensive risk assessment that considers the liver-brain axis as a functional organ unit, and extensive usage of non-invasive testing for fibrosis, advanced neuroimaging, and new biomarker technology to optimize risk stratification while guiding targeted preventive strategies.
Emerging therapies for MASLD and liver fibrosis, combined with lifestyle changes and metabolic optimization, may offer neuroprotection by reducing liver inflammation, improving metabolism and endothelial function, and supporting the gut-brain/liver axis.
While considerable progress has been made in understanding the relationship between liver and brain health, numerous gaps exist in our knowledge regarding the relationship between liver fibrosis and cognitive impairment/dementia, as well as the timing, duration, and type of exposure to liver damage associated with an increased risk of dementia/cognitive impairment, sex and age of the affected individual, and genetic factors. Further research, also including Mendelian Randomization Analysis, will be necessary to identify the exact relationship, casual or causal, and the specific mechanisms that link these two diseases. Moreover, effective clinical interventions must be investigated to prevent cognitive impairment and/or dementia among individuals living with liver fibrosis. Strong evidence in this field will indeed be provided by follow-up assessment of cognitive abilities in individuals submitted to interventions aimed at improving or reversing advanced liver fibrosis [166].
Author Contributions
Conceptualization, M.J., R.W., and A.L.; validation, M.J., R.W., and A.L.; formal analysis, M.J., R.W., and A.L.; resources, M.J., R.W., and A.L.; data curation, M.J., R.W., and A.L.; writing—original draft preparation, M.J., R.W., and A.L.; writing—review and editing, M.J., R.W., and A.L.; visualization, M.J. and A.L.; supervision, M.J., R.W., and A.L.; project administration, M.J., R.W., and A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were generated.
Acknowledgments
During the preparation of this manuscript, the authors utilized the free online tool “Edit My English” to enhance readability and ensure error-free language in terms of grammar, spelling, punctuation, and tone. Additionally, “Microsoft Copilot” was used to identify the most relevant and current references for specific statements. Following the use of these tools, the authors carefully reviewed and edited the content as necessary, taking full responsibility for the published article’s content.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| β | Regression coefficient |
| AD | Alzheimer’s disease |
| AF | Atrial fibrillation |
| ALD | Alcohol-related liver disease |
| ALT | Alanine aminotransferase |
| APOE | Apolipoprotein E |
| APRI | aminotransferase–platelet ratio index |
| AST | Aspartate aminotransferase |
| AST/ALT | Aspartate aminotransferase / alanine aminotransferase ratio |
| BBB | Blood–brain barrier |
| CI | Confidence interval |
| CLD | Chronic liver disease |
| DBil | Direct bilirubin |
| ECM | Extracellular matrix |
| FHS | Framingham Heart Study |
| ELF | enhanced liver fibrosis score |
| FA | Fractional anisotropy |
| FIB-4 | Fibrosis-4 index |
| GGT | Gamma-glutamyl transpeptidase |
| GLP-1 RAs | glucagon-like peptide-1 receptor agonists |
| HOMA | Homeostatic model assessment |
| HR | Hazard ratio |
| HSC | Hepatic stellate cell |
| MASH | Metabolic dysfunction-associated steatohepatitis |
| MASLD | Metabolic dysfunction-associated steatotic liver disease |
| MD | Mean diffusivity |
| MetALD | Metabolic dysfunction and ALD |
| MMSE | Mini-Mental State Examination |
| MoCA | Montreal Cognitive Assessment |
| MRE | Magnetic Resonance Elastography |
| MRI | Magnetic resonance imaging |
| MRI-PDFF | Magnetic resonance imaging–proton density fat fraction |
| NFS | NAFLD fibrosis score |
| PDD | Parkinson’s Disease Dementia |
| PET | Positron emission tomography |
| PFDR | False discovery rate–adjusted p-value |
| PNPLA3 | Patatin-like phospholipase domain-containing protein 3 |
| RS | Rotterdam Study |
| SHIP | Study of Health in Pomerania |
| TBil | Total bilirubin |
| T2D | Type 2 diabetes |
| TMAO | trimethylamine-N-oxide |
| UK | United Kingdom |
| VaD | Vascular dementia |
| VCTE | Vibration-controlled transient elastography |
| WMH | White matter hyperintensity |
Appendix A

Table A1.
Search syntax used to identify studies evaluating the association between liver fibrosis and dementia.
Table A1.
Search syntax used to identify studies evaluating the association between liver fibrosis and dementia.
| Database | Syntax |
| PubMed | (("liver"[Mesh] AND ("Elasticity Imaging Techniques"[Mesh] OR "biopsy"[Mesh] OR "fibrosis"[Mesh])) OR “Liver Cirrhosis”[Mesh] OR (("liver"[tiab] OR "hepatic"[tiab]) AND ("biops*"[tiab] OR "fibros*"[tiab] OR "cirrhos*"[tiab] OR "stiffness*"[tiab] OR "puncture"[tiab] OR "elastogra*"[tiab] OR "elasticit*"[tiab] OR "acoustography"[tiab] OR "vibroacoustography"[tiab] OR "vibro-acoustography"[tiab] OR "sonoelastograph*"[tiab] OR "fibroscan"[tiab] OR "acoustic radiation force impulse imaging"[tiab] OR "arfi imaging*"[tiab]))) AND ("Dementia"[Mesh] OR "Dementia*"[tiab] OR "Alzheimer*"[tiab] OR "Binswanger encephalopathy"[tiab] OR "CADASIL"[tiab] OR "Lewy body disease"[tiab] OR "Neurofibrillary tangles with calcification"[tiab] OR "Primary progressive aphasia"[tiab] OR "Progressive nonfluent aphasia"[tiab] OR "Hereditary diffuse leukoencephalopathy with spheroids"[tiab] OR "Huntington chorea"[tiab] OR "Kluver-Bucy syndrome"[tiab] OR "Mental deterioration"[tiab] OR "Nasu-Hakola disease"[tiab] OR "Neuronal ceroid lipofuscinosis"[tiab] OR "Prion disease"[tiab] OR "Bovine spongiform encephalopathy"[tiab] OR "Chronic wasting disease"[tiab] OR "Creutzfeldt-Jakob disease"[tiab] OR "Feline spongiform encephalopathy"[tiab] OR "Fatal familial insomnia"[tiab] OR "Gerstmann-Straussler-Scheinker syndrome"[tiab] OR "Kuru"[tiab] OR "Scrapie"[tiab] OR "Transmissible mink encephalopathy"[tiab] OR "Variably protease-sensitive prionopathy"[tiab] OR "Pseudodementia"[tiab] OR "Rett syndrome"[tiab] OR "Senility"[tiab] OR "Tauopathy"[tiab] OR "Creutzfeldt-Jakob syndrome"[tiab] OR "Diffuse neurofibrillary tangles with calcification"[tiab] OR "Frontotemporal lobar degeneration"[tiab] OR "Huntington disease"[tiab] OR "Amentia*"[tiab]) AND ("1900/01/01"[Date - Publication] : "2025/11/30"[Date - Publication]) AND (humans[Filter]) AND(english[Filter]) AND (alladult[Filter]) |
Note: MeSH = Medical Subject Headings; [tiab] = search in title/abstract; [Date - Publication] = publication date filter; [Filter] = population/language filter; Boolean operators: AND = include both terms, OR = include any term; parentheses () = group terms; * (asterisk) = wildcard to capture multiple word endings; search limited to humans, English, and adults, from inception through November 30, 2025.
References
- Zamani, M.; Alizadeh-Tabari, S.; Ajmera, V.; Singh, S.; Murad, M.H.; Loomba, R. Global Prevalence of Advanced Liver Fibrosis and Cirrhosis in the General Population: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2025, 23, 1123–1134. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Tilg, H. MASLD: a systemic metabolic disorder with cardiovascular and malignant complications. Gut 2024, 73, 691–702. [Google Scholar] [CrossRef]
- Tsomidis, I.; Voumvouraki, A.; Kouroumalis, E. Immune Checkpoints and the Immunology of Liver Fibrosis. Livers 2025, 5, 5. [Google Scholar] [CrossRef]
- Jamalinia, M.; Zare, F.; Lonardo, A. Liver Fibrosis and Risk of Incident Dementia in the General Population: Systematic Review With Meta-Analysis. Health Sci Rep 2025, 8, e71530. [Google Scholar] [CrossRef] [PubMed]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T.; et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Wang, X. Alzheimer’s disease: insights into pathology, molecular mechanisms, and therapy. Protein & Cell 2024, 16, 83–120. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, A.C.D.; Kjærgaard, K.; Schapira, A.H.V.; Mookerjee, R.P.; Thomsen, K.L. The liver-brain axis in metabolic dysfunction-associated steatotic liver disease. Lancet Gastroenterol Hepatol 2025, 10, 248–258. [Google Scholar] [CrossRef]
- Ayala, V.; Fontdevila, L.; Rico-Rios, S.; Povedano, M.; Andrés-Benito, P.; Torres, P.; Serrano, J.C.E.; Pamplona, R.; Portero-Otin, M. Microbial Influences on Amyotrophic Lateral Sclerosis: The Gut–Brain Axis and Therapeutic Potential of Microbiota Modulation. Sclerosis 2025, 3, 8. [Google Scholar] [CrossRef]
- Weinstein, G.; Schonmann, Y.; Yeshua, H.; Zelber-Sagi, S. The association between liver fibrosis score and incident dementia: A nationwide retrospective cohort study. Alzheimers Dement 2024, 20, 5385–5397. [Google Scholar] [CrossRef]
- Parikh, N.S.; Kamel, H.; Zhang, C.; Kumar, S.; Rosenblatt, R.; Spincemaille, P.; Gupta, A.; Cohen, D.E.; de Leon, M.J.; Gottesman, R.F.; et al. Association between liver fibrosis and incident dementia in the UK Biobank study. Eur J Neurol 2022, 29, 2622–2630. [Google Scholar] [CrossRef]
- Bataller, R.; Brenner, D.A. Liver fibrosis. J Clin Invest 2005, 115, 209–218. [Google Scholar] [CrossRef]
- Sultana, M.; Islam, M.A.; Khairnar, R.; Kumar, S. A guide to pathophysiology, signaling pathways, and preclinical models of liver fibrosis. Mol Cell Endocrinol 2025, 598, 112448. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Brol, M.J.; Drebber, U.; Luetkens, J.A.; Odenthal, M.; Trebicka, J. “The pathogenesis of hepatic fibrosis: basic facts and clinical challenges”—assessment of liver fibrosis: a narrative review. Digestive Medicine Research 2022, 5. [Google Scholar] [CrossRef]
- Gan, C.; Yuan, Y.; Shen, H.; Go, J.; Kong, X.; Che, Z.; Guo, Y.; Wang, H.; Dong, E.; Xiao, J. Liver diseases: epidemiology, causes, trends and predictions. Signal Transduct Target Ther 2025, 10, 33. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Romagnoli, D.; Lonardo, A. The independent predictors of non-alcoholic steatohepatitis and its individual histological features.: Insulin resistance, serum uric acid, metabolic syndrome, alanine aminotransferase and serum total cholesterol are a clue to pathogenesis and candidate targets for treatment. Hepatol Res 2016, 46, 1074–1087. [Google Scholar] [CrossRef]
- Lan, R.; Lin, J.; Chen, S.; Lu, Z.; Gong, Y.; Tan, S.; Liu, X.; He, W. Communication initiated by hepatocytes: The driver of HSC activation and liver fibrosis. Hepatol Commun 2025, 9. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Weiskirchen, R. Liver and obesity: a narrative review. Exploration of Medicine 2025, 6, 1001334. [Google Scholar] [CrossRef]
- Nowak, K.; Paluch, M.; Cudzik, M.; Syska, K.; Gawlikowska, W.; Janczura, J. From steatosis to cirrhosis: the role of obesity in the progression of liver disease. J Diabetes Metab Disord 2025, 24, 227. [Google Scholar] [CrossRef]
- Guan, H.; Zhang, X.; Kuang, M.; Yu, J. The gut-liver axis in immune remodeling of hepatic cirrhosis. Front Immunol 2022, 13, 946628. [Google Scholar] [CrossRef] [PubMed]
- Maslennikov, R.; Poluektova, E.; Zolnikova, O.; Sedova, A.; Kurbatova, A.; Shulpekova, Y.; Dzhakhaya, N.; Kardasheva, S.; Nadinskaia, M.; Bueverova, E.; et al. Gut Microbiota and Bacterial Translocation in the Pathogenesis of Liver Fibrosis. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Huang, Y.; Yu, Y.; Jin, W.; Zhang, X.; Yu, F. Interactions between hepatic stellate cells and immune cells: Implications for liver fibrosis. Biochim Biophys Acta Mol Basis Dis 2026, 1872, 168062. [Google Scholar] [CrossRef] [PubMed]
- de Zawadzki, A.; Leeming, D.J.; Sanyal, A.J.; Anstee, Q.M.; Schattenberg, J.M.; Friedman, S.L.; Schuppan, D.; Karsdal, M.A. Hot and cold fibrosis: The role of serum biomarkers to assess immune mechanisms and ECM-cell interactions in human fibrosis. J Hepatol 2025, 83, 239–257. [Google Scholar] [CrossRef]
- Weiskirchen, R.; Lonardo, A. PNPLA3 as a driver of steatotic liver disease: navigating from pathobiology to the clinics via epidemiology. J Transl Genetics Genomics 2024, 8, 355–377. [Google Scholar] [CrossRef]
- Hanquier, Z.; Misra, J.; Baxter, R.; Maiers, J.L. Stress and Liver Fibrogenesis: Understanding the Role and Regulation of Stress Response Pathways in Hepatic Stellate Cells. Am J Pathol 2023, 193, 1363–1376. [Google Scholar] [CrossRef]
- Lugari, S.; Baldelli, E.; Lonardo, A. Metabolic primary liver cancer in adults: risk factors and pathogenic mechanisms. Metabolism and Target Organ Damage 2023, 3, 5. [Google Scholar] [CrossRef]
- Lonardo, A.; Ballestri, S.; Baffy, G.; Weiskirchen, R. Liver fibrosis as a barometer of systemic health by gauging the risk of extrahepatic disease. Metabolism and Target Organ Damage 2024, 4, 41. [Google Scholar] [CrossRef]
- Seo, Y.G.; Polyzos, S.A.; Park, K.H.; Mantzoros, C.S. Fibrosis-4 Index Predicts Long-Term All-Cause, Cardiovascular and Liver-Related Mortality in the Adult Korean Population. Clin Gastroenterol Hepatol 2023, 21, 3322–3335. [Google Scholar] [CrossRef]
- Ampuero, J.; Aller, R.; Gallego-Durán, R.; Crespo, J.; Calleja, J.L.; García-Monzón, C.; Gómez-Camarero, J.; Caballería, J.; Lo Iacono, O.; Ibañez, L.; et al. Significant fibrosis predicts new-onset diabetes mellitus and arterial hypertension in patients with NASH. J Hepatol 2020, 73, 17–25. [Google Scholar] [CrossRef]
- Ampuero, J.; Aller, R.; Gallego-Durán, R.; Crespo, J.; Calleja, J.L.; García-Monzón, C.; Gómez-Camarero, J.; Caballería, J.; Lo Iacono, O.; Ibañez, L.; et al. Erratum to: "Significant fibrosis predicts new-onset diabetes mellitus and arterial hypertension in patients with NASH (J Hepatol 2020; 73: 17-25). J Hepatol 2020, 73, 740–741. [Google Scholar] [CrossRef]
- Zhang, J.; Li, L.; Lin, L.; Wu, Y.; Hu, L.; Feng, Z.; Zhang, D.; Fu, T.; Zhao, H.; Yin, X.; et al. Prognostic value of FIB-4 and NFS for cardiovascular events in patients with and without NAFLD. BMC Public Health 2025, 25, 2747. [Google Scholar] [CrossRef]
- Lonardo, A. Extra-hepatic cancers in metabolic fatty liver syndromes. Exploration of Digestive Diseases 2023, 2, 11–17. [Google Scholar] [CrossRef]
- Friedman, S.L. Hepatic Fibrosis and Cancer: The Silent Threats of Metabolic Syndrome. Diabetes Metab J 2024, 48, 161–169. [Google Scholar] [CrossRef]
- Mantovani, A.; Lonardo, A.; Stefan, N.; Targher, G. Metabolic dysfunction-associated steatotic liver disease and extrahepatic gastrointestinal cancers. Metabolism 2024, 160, 156014. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A. Association of NAFLD/NASH, and MAFLD/MASLD with chronic kidney disease: an updated narrative review. Metabolism and Target Organ Damage 2024, 4, 16. [Google Scholar] [CrossRef]
- Cipriani, G.; Danti, S.; Picchi, L.; Nuti, A.; Fiorino, M.D. Daily functioning and dementia. Dement Neuropsychol 2020, 14, 93–102. [Google Scholar] [CrossRef]
- Burgueño-García, I.; López-Martínez, M.J.; Uceda-Heras, A.; García-Carracedo, L.; Zea-Sevilla, M.A.; Rodrigo-Lara, H.; Rego-García, I.; Saiz-Aúz, L.; Ruiz-Valderrey, P.; López-González, F.J.; et al. Neuropathological Heterogeneity of Dementia Due to Combined Pathology in Aged Patients: Clinicopathological Findings in the Vallecas Alzheimer’s Reina Sofía Cohort. Journal of Clinical Medicine 2024, 13, 6755. [Google Scholar] [CrossRef]
- Zhang, J.; Kong, G.; Yang, J.; Pang, L.; Li, X. Pathological mechanisms and treatment progression of Alzheimer's disease. Eur J Med Res 2025, 30, 625. [Google Scholar] [CrossRef]
- Inoue, Y.; Shue, F.; Bu, G.; Kanekiyo, T. Pathophysiology and probable etiology of cerebral small vessel disease in vascular dementia and Alzheimer’s disease. Molecular Neurodegeneration 2023, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, P.S.; Sweeney, A.; Passmore, A.P.; McCorry, N.K.; Kane, J.P.M. Research on the perspectives of people affected by dementia with Lewy bodies: a scoping review. Alzheimer's Research & Therapy 2025, 17, 117. [Google Scholar] [CrossRef]
- Dattola, S.; Ielo, A.; Varone, G.; Cacciola, A.; Quartarone, A.; Bonanno, L. Frontotemporal dementia: a systematic review of artificial intelligence approaches in differential diagnosis. Front Aging Neurosci 2025, 17, 1547727. [Google Scholar] [CrossRef]
- Custodio, N.; Montesinos, R.; Lira, D.; Herrera-Pérez, E.; Bardales, Y.; Valeriano-Lorenzo, L. Mixed dementia: A review of the evidence. Dement Neuropsychol 2017, 11, 364–370. [Google Scholar] [CrossRef]
- Szeto, J.Y.Y.; Walton, C.C.; Rizos, A.; Martinez-Martin, P.; Halliday, G.M.; Naismith, S.L.; Chaudhuri, K.R.; Lewis, S.J.G. Dementia in long-term Parkinson's disease patients: a multicentre retrospective study. NPJ Parkinsons Dis 2020, 6, 2. [Google Scholar] [CrossRef]
- Gibson, L.L.; Weintraub, D.; Lemmen, R.; Perera, G.; Chaudhuri, K.R.; Svenningsson, P.; Aarsland, D. Risk of Dementia in Parkinson's Disease: A Systematic Review and Meta-Analysis. Mov Disord 2024, 39, 1697–1709. [Google Scholar] [CrossRef]
- Pourzinal, D.; Elgey, C.; Bailey, D.X.; Yang, J.; Lehn, A.; Tinson, H.; Liddle, J.; Brooks, D.; Naismith, S.L.; Shrubsole, K. Diagnosis, evaluation & management of cognitive disorders in Parkinson's disease: A systematic review 10.1016/j.inpsyc.2025.100081. Int Psychogeriatr 2025, 100081. [Google Scholar] [CrossRef]
- Dias, D.; Socodato, R. Beyond Amyloid and Tau: The Critical Role of Microglia in Alzheimer’s Disease Therapeutics. Biomedicines 2025, 13, 279. [Google Scholar] [CrossRef]
- Ebrahimi, R.; Bordbar, S.; Azad, G.; Davoody, S.; Mahmoudi, M.; Esmaeilpour, K. Beyond Neuroinflammation: Microglia at the Crossroads of Amyloid, Tau, and Neurodegeneration in Alzheimer’s Disease. Neurological Sciences 2025, 46, 5591–5605. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Zhang, Z.; Zhang, P.; Yu, Q.; Cheng, Q.; Lu, Z.; Zong, S. The roles of microglia and astrocytes in neuroinflammation of Alzheimer’s disease. Front Neurosci 2025, 19–2025. [Google Scholar] [CrossRef]
- Shafi, A.; Akmal, M.; Sethi, A.; Chauhdary, Z. A mechanistic insight of neuro-inflammation signaling pathways and implication in neurodegenerative disorders. Inflammopharmacology 2025. [Google Scholar] [CrossRef] [PubMed]
- Alaqel, S.I.; Imran, M.; Khan, A.; Nayeem, N. Aging, vascular dysfunction, and the blood–brain barrier: unveiling the pathophysiology of stroke in older adults. Biogerontology 2025, 26, 67. [Google Scholar] [CrossRef] [PubMed]
- Preis, L.; Villringer, K.; Brosseron, F.; Düzel, E.; Jessen, F.; Petzold, G.C.; Ramirez, A.; Spottke, A.; Fiebach, J.B.; Peters, O. Assessing blood-brain barrier dysfunction and its association with Alzheimer’s pathology, cognitive impairment and neuroinflammation. Alzheimer's Research & Therapy 2024, 16, 172. [Google Scholar] [CrossRef]
- Kumar A, Sidhu J, Lui F, al. e. Alzheimer Disease. 2025 [cited 1 December 2025]. In: StatPearls [Internet]. Treasure Island (FL). (updated 2024 Feb 12). [cited 1 December 2025]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499922/.
- Huang, X.-T.; Huang, L.-Y.; Tan, C.-C.; Wei, J.-M.; Zhang, X.-H.; Tan, L.; Xu, W. The role of APOE ε4 in modulating the relationship between non-genetic risk factors and dementia: a system review and meta-analysis. Journal of Neurology 2025, 272, 690. [Google Scholar] [CrossRef]
- Ren, Z.; Guan, Z.; Guan, Q.; Guan, H.; Che, H. Association between apolipoprotein E ε4 status and the risk of Alzheimer’s disease: a meta-analysis. BMC Neuroscience 2025, 26, 5. [Google Scholar] [CrossRef]
- Smith, J.R.; Pike, J.R.; Gottesman, R.F.; Knopman, D.S.; Lutsey, P.L.; Palta, P.; Windham, B.G.; Selvin, E.; Szklo, M.; Bandeen-Roche, K.J.; et al. Contribution of Modifiable Midlife and Late-Life Vascular Risk Factors to Incident Dementia. JAMA Neurology 2025, 82, 644–654. [Google Scholar] [CrossRef]
- Mekonnen, T.; Skirbekk, V.; Håberg, A.K.; Engdahl, B.; Zotcheva, E.; Jugessur, A.; Bowen, C.; Selbaek, G.; Kohler, H.-P.; Harris, J.R.; et al. Mediators of educational differences in dementia risk later in life: evidence from the HUNT study. BMC Public Health 2025, 25, 1336. [Google Scholar] [CrossRef]
- Song, D.; Li, Y.; Yang, L.-L.; Luo, Y.-X.; Yao, X.-Q. Bridging systemic metabolic dysfunction and Alzheimer’s disease: the liver interface. Molecular Neurodegeneration 2025, 20, 61. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yang, R.; Miao, Y.; Zhang, X.; Paillard-Borg, S.; Fang, Z.; Xu, W. Metabolic Dysfunction-Associated Steatotic Liver Disease Is Associated With Accelerated Brain Ageing: A Population-Based Study. Liver Int 2025, 45, e70109. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.Y.; Ou, Y.N.; Wang, H.F.; Wang, Z.B.; Fu, Y.; He, X.Y.; Ma, Y.H.; Feng, J.F.; Cheng, W.; Tan, L.; et al. Associations of liver dysfunction with incident dementia, cognition, and brain structure: A prospective cohort study of 431 699 adults. J Neurochem 2024, 168, 26–38. [Google Scholar] [CrossRef]
- Weinstein, G.; O'Donnell, A.; Frenzel, S.; Xiao, T.; Yaqub, A.; Yilmaz, P.; de Knegt, R.J.; Maestre, G.E.; Melo van Lent, D.; Long, M.; et al. Nonalcoholic fatty liver disease, liver fibrosis, and structural brain imaging: The Cross-Cohort Collaboration. Eur J Neurol 2024, 31, e16048. [Google Scholar] [CrossRef]
- Weinstein, G.; O'Donnell, A.; Davis-Plourde, K.; Zelber-Sagi, S.; Ghosh, S.; DeCarli, C.S.; Thibault, E.G.; Sperling, R.A.; Johnson, K.A.; Beiser, A.S.; et al. Non-Alcoholic Fatty Liver Disease, Liver Fibrosis, and Regional Amyloid-β and Tau Pathology in Middle-Aged Adults: The Framingham Study. J Alzheimers Dis 2022, 86, 1371–1383. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Yang, S.; Wei, Y.; Tian, M.; Liu, Q.; Li, X.; Ding, J.; Li, X.; Mao, M.; Han, X.; et al. Characterization of brain morphology associated with metabolic dysfunction-associated steatotic liver disease in the UK Biobank. Diabetes Obes Metab 2025, 27, 3419–3430. [Google Scholar] [CrossRef]
- Lu, Y.; Pike, J.R.; Hoogeveen, R.C.; Walker, K.A.; Raffield, L.M.; Selvin, E.; Avery, C.L.; Engel, S.M.; Mielke, M.M.; Garcia, T.; et al. Liver integrity and the risk of Alzheimer's disease and related dementias. Alzheimers Dement 2024, 20, 1913–1922. [Google Scholar] [CrossRef]
- Tao, M.H.; Gordon, S.C.; Wu, T.; Trudeau, S.; Rupp, L.B.; Gonzalez, H.C.; Daida, Y.G.; Schmidt, M.A.; Lu, M. Antiviral Treatment and Response are Associated With Lower Risk of Dementia Among Hepatitis C Virus-Infected Patients. Am J Geriatr Psychiatry 2024, 32, 611–621. [Google Scholar] [CrossRef]
- Shang, Y.; Nasr, P.; Ekstedt, M.; Widman, L.; Stål, P.; Hultcrantz, R.; Kechagias, S.; Hagström, H. Non-alcoholic fatty liver disease does not increase dementia risk although histology data might improve risk prediction. JHEP Rep 2021, 3, 100218. [Google Scholar] [CrossRef]
- Solfrizzi, V.; Scafato, E.; Custodero, C.; Loparco, F.; Ciavarella, A.; Panza, F.; Seripa, D.; Imbimbo, B.P.; Lozupone, M.; Napoli, N.; et al. Liver fibrosis score, physical frailty, and the risk of dementia in older adults: The Italian Longitudinal Study on Aging. Alzheimers Dement (N Y) 2020, 6, e12065. [Google Scholar] [CrossRef]
- Xiao, T.; van Kleef, L.A.; Ikram, M.K.; de Knegt, R.J.; Ikram, M.A. Association of Nonalcoholic Fatty Liver Disease and Fibrosis With Incident Dementia and Cognition: The Rotterdam Study. Neurology 2022, 99, e565–e573. [Google Scholar] [CrossRef]
- Taru, V.; Szabo, G.; Mehal, W.; Reiberger, T. Inflammasomes in chronic liver disease: Hepatic injury, fibrosis progression and systemic inflammation. J Hepatol 2024, 81, 895–910. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.; Wu, J.; Rosenblatt, M.; Dai, W.; Rodriguez, R.X.; Sui, J.; Qi, S.; Liang, Q.; Xu, B.; Meng, Q.; et al. Elevated C-reactive protein mediates the liver-brain axis: a preliminary study. EBioMedicine 2023, 93, 104679. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Li, J.; Wang, X.; Tang, D.; Chen, R. Neuroimmune modulation in liver pathophysiology. J Neuroinflammation 2024, 21, 188. [Google Scholar] [CrossRef] [PubMed]
- Horn, P.; Tacke, F. Metabolic reprogramming in liver fibrosis. Cell Metab 2024, 36, 1439–1455. [Google Scholar] [CrossRef]
- Peng, Z.; Duggan, M.R.; Dark, H.E.; Daya, G.N.; An, Y.; Davatzikos, C.; Erus, G.; Lewis, A.; Moghekar, A.R.; Walker, K.A. Association of liver disease with brain volume loss, cognitive decline, and plasma neurodegenerative disease biomarkers. Neurobiol Aging 2022, 120, 34–42. [Google Scholar] [CrossRef]
- Chen, Y.; Lei, K.; Liu, Y.; Liu, J.; Wei, K.; Guo, J.; Su, Z. Metabolic Dysfunction-Associated Steatotic Liver Disease: From a Very Low-Density Lipoprotein Perspective. Biomolecules 2025, 15. [Google Scholar] [CrossRef]
- Hoebinger, C.; Rajcic, D.; Hendrikx, T. Oxidized Lipids: Common Immunogenic Drivers of Non-Alcoholic Fatty Liver Disease and Atherosclerosis. Front Cardiovasc Med 2021, 8, 824481. [Google Scholar] [CrossRef]
- Parola, M.; Robino, G. Oxidative stress-related molecules and liver fibrosis. J Hepatol 2001, 35, 297–306. [Google Scholar] [CrossRef]
- Ma, Y.; Lee, G.; Heo, S.Y.; Roh, Y.S. Oxidative Stress Is a Key Modulator in the Development of Nonalcoholic Fatty Liver Disease. Antioxidants (Basel) 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Delli Bovi, A.P.; Marciano, F.; Mandato, C.; Siano, M.A.; Savoia, M.; Vajro, P. Oxidative Stress in Non-alcoholic Fatty Liver Disease. An Updated Mini Review. Front Med (Lausanne) 2021, 8, 595371. [Google Scholar] [CrossRef] [PubMed]
- Houldsworth, A. Role of oxidative stress in neurodegenerative disorders: a review of reactive oxygen species and prevention by antioxidants. Brain Commun 2024, 6, fcad356. [Google Scholar] [CrossRef] [PubMed]
- Trofin, D.M.; Sardaru, D.P.; Trofin, D.; Onu, I.; Tutu, A.; Onu, A.; Onită, C.; Galaction, A.I.; Matei, D.V. Oxidative Stress in Brain Function. Antioxidants (Basel) 2025, 14. [Google Scholar] [CrossRef]
- Ma, Y.; Pu, Y.; Chen, H.; Zhou, L.; Yang, B.; Huang, X.; Zhang, J. The pathogenesis of liver fibrosis in Wilson's disease: hepatocyte injury and regulation mediated by copper metabolism dysregulation. Biometals 2025. [Google Scholar] [CrossRef]
- Albillos, A.; de Gottardi, A.; Rescigno, M. The gut-liver axis in liver disease: Pathophysiological basis for therapy. J Hepatol 2020, 72, 558–577. [Google Scholar] [CrossRef]
- Banks, W.A.; Gray, A.M.; Erickson, M.A.; Salameh, T.S.; Damodarasamy, M.; Sheibani, N.; Meabon, J.S.; Wing, E.E.; Morofuji, Y.; Cook, D.G.; et al. Lipopolysaccharide-induced blood-brain barrier disruption: roles of cyclooxygenase, oxidative stress, neuroinflammation, and elements of the neurovascular unit. J Neuroinflammation 2015, 12, 223. [Google Scholar] [CrossRef]
- Rocco, A.; Sgamato, C.; Compare, D.; Coccoli, P.; Nardone, O.M.; Nardone, G. Gut Microbes and Hepatic Encephalopathy: From the Old Concepts to New Perspectives. Front Cell Dev Biol 2021, 9, 748253. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Gregory, J.C.; Org, E.; Buffa, J.A.; Gupta, N.; Wang, Z.; Li, L.; Fu, X.; Wu, Y.; Mehrabian, M.; et al. Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell 2016, 165, 111–124. [Google Scholar] [CrossRef]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Front Endocrinol (Lausanne) 2020, 11, 25. [Google Scholar] [CrossRef]
- Dalile, B.; Van Oudenhove, L.; Vervliet, B.; Verbeke, K. The role of short-chain fatty acids in microbiota-gut-brain communication. Nat Rev Gastroenterol Hepatol 2019, 16, 461–478. [Google Scholar] [CrossRef] [PubMed]
- Jamalinia, M.; Lonardo, A.; Weiskirchen, R. Sex and Gender Differences in Liver Fibrosis: Pathomechanisms and Clinical Outcomes. Fibrosis 2024, 2, 10006. [Google Scholar] [CrossRef]
- Gabelli, C.; Codemo, A. Gender differences in cognitive decline and Alzheimer’s disease. The Italian Journal of Gender-Specific Medicine 2015, 1, 21–28. [Google Scholar] [CrossRef]
- Williams, S.N.; Ding, W.X. The impact of aging on liver health and the development of liver diseases. Hepatol Commun 2025, 9. [Google Scholar] [CrossRef]
- Biagetti, B.; Puig-Domingo, M. Age-Related Hormones Changes and Its Impact on Health Status and Lifespan. Aging Dis 2023, 14, 605–620. [Google Scholar] [CrossRef]
- Yeap, B.B.; Flicker, L. Testosterone, cognitive decline and dementia in ageing men. Rev Endocr Metab Disord 2022, 23, 1243–1257. [Google Scholar] [CrossRef]
- Lonardo, A.; Jamalinia, M.; Weiskirchen, R. Sex differences in MASLD. SciErixiv 2025. [Google Scholar] [CrossRef]
- Lonardo, A.; Suzuki, A. Sex differences in alcohol-related liver disease, viral hepatitis, metabolic dysfunction-associated steatotic liver disease, and hepatocellular carcinoma. Exploration of Digestive Diseases 2025, 4, 1005101. [Google Scholar] [CrossRef]
- Kim, I.H.; Kisseleva, T.; Brenner, D.A. Aging and liver disease. Curr Opin Gastroenterol 2015, 31, 184–191. [Google Scholar] [CrossRef]
- Hou, Y.; Dan, X.; Babbar, M.; Wei, Y.; Hasselbalch, S.G.; Croteau, D.L.; Bohr, V.A. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol 2019, 15, 565–581. [Google Scholar] [CrossRef]
- Weiskirchen, R.; Lonardo, A. The Ovary-Liver Axis: Molecular Science and Epidemiology. Int J Mol Sci 2025, 26. [Google Scholar] [CrossRef]
- Weiskirchen, R.; Lonardo, A. Sex Hormones and Metabolic Dysfunction-Associated Steatotic Liver Disease. Int J Mol Sci 2025, 26. [Google Scholar] [CrossRef] [PubMed]
- Saelzler, U.G.; Sundermann, E.E.; Foret, J.T.; Gatz, M.; Karlsson, I.K.; Pederson, N.L.; Panizzon, M.S. Age of menopause and dementia risk in 10,832 women from the Swedish Twin Registry. Alzheimers Dement 2025, 21, e70541. [Google Scholar] [CrossRef] [PubMed]
- Berger, D.; Desai, V.; Janardhan, S. Con: Liver Biopsy Remains the Gold Standard to Evaluate Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Clin Liver Dis (Hoboken) 2019, 13, 114–116. [Google Scholar] [CrossRef]
- Josh, B.; Daniel, J.C.; Christopher, D.B. Evolving models of care in patients with metabolic dysfunction-associated steatotic liver disease, recognising its population burden and the impact of metabolic dysfunction on incident rates of hepatic and extrahepatic outcomes. Artificial Intelligence Surgery 2025, 5, 27. [Google Scholar] [CrossRef]
- Castera, L.; Rinella, M.E.; Tsochatzis, E.A. Noninvasive Assessment of Liver Fibrosis. N Engl J Med 2025, 393, 1715–1729. [Google Scholar] [CrossRef]
- Anania, F.A.; Hager, R.; Higgins, K.; Makar, G.A.; Siegel, J.; Tran, T.T. Non-invasive tests: Establishing efficacy for metabolic dysfunction-associated steatohepatitis beyond the biopsy-Current perspectives from the Division of Hepatology and Nutrition, US Food and Drug Administration. Hepatology 2025. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Hardy, T.; Dufour, J.F.; Petta, S.; Romero-Gomez, M.; Allison, M.; Oliveira, C.P.; Francque, S.; Van Gaal, L.; Schattenberg, J.M.; et al. Age as a Confounding Factor for the Accurate Non-Invasive Diagnosis of Advanced NAFLD Fibrosis. Am J Gastroenterol 2017, 112, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Boursier, J.; Canivet, C.M.; Costentin, C.; Lannes, A.; Delamarre, A.; Sturm, N.; Le Bail, B.; Michalak, S.; Oberti, F.; Hilleret, M.N.; et al. Impact of Type 2 Diabetes on the Accuracy of Noninvasive Tests of Liver Fibrosis With Resulting Clinical Implications. Clin Gastroenterol Hepatol 2023, 21, 1243–1251.e1212. [Google Scholar] [CrossRef] [PubMed]
- Yue, W.; Li, Y.; Geng, J.; Wang, P.; Zhang, L. Aspartate aminotransferase to platelet ratio can reduce the need for transient elastography in Chinese patients with chronic hepatitis B. Medicine (Baltimore) 2019, 98, e18038. [Google Scholar] [CrossRef]
- Shaheen, A.A.; Myers, R.P. Diagnostic accuracy of the aspartate aminotransferase-to-platelet ratio index for the prediction of hepatitis C-related fibrosis: a systematic review. Hepatology 2007, 46, 912–921. [Google Scholar] [CrossRef]
- Xu, X.L.; Jiang, L.S.; Wu, C.S.; Pan, L.Y.; Lou, Z.Q.; Peng, C.T.; Dong, Y.; Ruan, B. The role of fibrosis index FIB-4 in predicting liver fibrosis stage and clinical prognosis: A diagnostic or screening tool? J Formos Med Assoc 2022, 121, 454–466. [Google Scholar] [CrossRef]
- Torres, L.; Schuch, A.; Longo, L.; Valentini, B.B.; Galvão, G.S.; Luchese, E.; Pinzon, C.; Bartels, R.; Álvares-da-Silva, M.R. New FIB-4 and NFS cutoffs to guide sequential non-invasive assessment of liver fibrosis by magnetic resonance elastography in NAFLD. Ann Hepatol 2023, 28, 100774. [Google Scholar] [CrossRef]
- Yin, M.; Venkatesh, S.K. Ultrasound or MR elastography of liver: which one shall I use? Abdom Radiol (NY) 2018, 43, 1546–1551. [Google Scholar] [CrossRef]
- Eilenberg, M.; Munda, P.; Stift, J.; Langer, F.B.; Prager, G.; Trauner, M.; Staufer, K. Accuracy of non-invasive liver stiffness measurement and steatosis quantification in patients with severe and morbid obesity. Hepatobiliary Surg Nutr 2021, 10, 610–622. [Google Scholar] [CrossRef]
- Sharpton, S.R.; Tamaki, N.; Bettencourt, R.; Madamba, E.; Jung, J.; Liu, A.; Behling, C.; Valasek, M.A.; Loomba, R. Diagnostic accuracy of two-dimensional shear wave elastography and transient elastography in nonalcoholic fatty liver disease. Therap Adv Gastroenterol 2021, 14, 17562848211050436. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Castera, L.; Mark, H.E.; Allen, A.M.; Adams, L.A.; Anstee, Q.M.; Arrese, M.; Alqahtani, S.A.; Bugianesi, E.; Colombo, M.; et al. Real-world evidence on non-invasive tests and associated cut-offs used to assess fibrosis in routine clinical practice. JHEP Rep 2023, 5, 100596. [Google Scholar] [CrossRef]
- Erratum Regarding Previously Published Articles. JHEP Rep 2024, 6, 101097. [CrossRef] [PubMed]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Diagnostic accuracy of non-invasive tests for advanced fibrosis in patients with NAFLD: an individual patient data meta-analysis. Gut 2022, 71, 1006–1019. [Google Scholar] [CrossRef]
- Salehi, H.; Salehi, A.M.; Ghamarchehreh, M.E.; Khanlarzadeh, E.; Sohrabi, M.R. Diagnostic Accuracy of Vibration Controlled Transient Elastography as Non-invasive Assessment of Liver Fibrosis in Patients with Non-alcoholic Fatty Liver Disease. Middle East J Dig Dis 2023, 15, 26–31. [Google Scholar] [CrossRef]
- Fasnacht, J.S.; Wueest, A.S.; Berres, M.; Thomann, A.E.; Krumm, S.; Gutbrod, K.; Steiner, L.A.; Goettel, N.; Monsch, A.U. Conversion between the Montreal Cognitive Assessment and the Mini-Mental Status Examination. J Am Geriatr Soc 2023, 71, 869–879. [Google Scholar] [CrossRef]
- Wang, G.; Estrella, A.; Hakim, O.; Milazzo, P.; Patel, S.; Pintagro, C.; Li, D.; Zhao, R.; Vance, D.E.; Li, W. Mini-Mental State Examination and Montreal Cognitive Assessment as Tools for Following Cognitive Changes in Alzheimer's Disease Neuroimaging Initiative Participants. J Alzheimers Dis 2022, 90, 263–270. [Google Scholar] [CrossRef]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and Management of Dementia: Review. Jama 2019, 322, 1589–1599. [Google Scholar] [CrossRef]
- Gaur, A.; Rivet, L.; Mah, E.; Bawa, K.K.; Gallagher, D.; Herrmann, N.; Lanctôt, K.L. Novel fluid biomarkers for mild cognitive impairment: A systematic review and meta-analysis. Ageing Res Rev 2023, 91, 102046. [Google Scholar] [CrossRef]
- Ma, Y.; Chen, Y.; Yang, T.; He, X.; Yang, Y.; Chen, J.; Han, L. Blood biomarkers for post-stroke cognitive impairment: A systematic review and meta-analysis. J Stroke Cerebrovasc Dis 2024, 33, 107632. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.D.; Deng, C.F.; Chen, P.F.; Li, A.; Wu, H.Z.; Ouyang, F.; Hu, X.G.; Liu, J.X.; Wang, S.M.; Tang, D. Non-invasive metabolic biomarkers in initial cognitive impairment in patients with diabetes: A systematic review and meta-analysis. Diabetes Obes Metab 2024, 26, 5519–5536. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Liao, L.; Liu, Q.; Ma, R.; He, X.; Du, X.; Sha, D. Blood biomarkers for vascular cognitive impairment based on neuronal function: a systematic review and meta-analysis. Front Neurol 2025, 16, 1496711. [Google Scholar] [CrossRef] [PubMed]
- Kivipelto, M.; Ngandu, T.; Laatikainen, T.; Winblad, B.; Soininen, H.; Tuomilehto, J. Risk score for the prediction of dementia risk in 20 years among middle aged people: a longitudinal, population-based study. Lancet Neurol 2006, 5, 735–741. [Google Scholar] [CrossRef]
- Farkas, K.; Lazar, T.; Becske, M.; Zsuffa, J.A.; Rosenfeld, V.; Berente, D.B.; Bolla, G.; Negyesi, J.; Horvath, A.A. The CAIDE dementia risk score indicates elevated cognitive risk in late adulthood: a structural and functional neuroimaging study. GeroScience 2025. [Google Scholar] [CrossRef] [PubMed]
- Anstey, K.J.; Cherbuin, N.; Herath, P.M. Development of a new method for assessing global risk of Alzheimer's disease for use in population health approaches to prevention. Prev Sci 2013, 14, 411–421. [Google Scholar] [CrossRef]
- Anatürk, M.; Patel, R.; Ebmeier, K.P.; Georgiopoulos, G.; Newby, D.; Topiwala, A.; de Lange, A.G.; Cole, J.H.; Jansen, M.G.; Singh-Manoux, A.; et al. Development and validation of a dementia risk score in the UK Biobank and Whitehall II cohorts. BMJ Ment Health 2023, 26. [Google Scholar] [CrossRef] [PubMed]
- Anstey, K.J.; Kootar, S.; Huque, M.H.; Eramudugolla, R.; Peters, R. Development of the CogDrisk tool to assess risk factors for dementia. Alzheimers Dement (Amst) 2022, 14, e12336. [Google Scholar] [CrossRef]
- Erratum. Alzheimers Dement (Amst) 2022, 14, e12387. [CrossRef]
- Rosenau, C.; Köhler, S.; van Boxtel, M.; Tange, H.; Deckers, K. Validation of the Updated "LIfestyle for BRAin health" (LIBRA) Index in the English Longitudinal Study of Ageing and Maastricht Aging Study. J Alzheimers Dis 2024, 101, 1237–1248. [Google Scholar] [CrossRef]
- Schon, H.T.; Weiskirchen, R. Exercise-Induced Release of Pharmacologically Active Substances and Their Relevance for Therapy of Hepatic Injury. Front Pharmacol 2016, 7, 283. [Google Scholar] [CrossRef]
- Arita, V.A.; Cabezas, M.C.; Hernández Vargas, J.A.; Trujillo-Cáceres, S.J.; Mendez Pernicone, N.; Bridge, L.A.; Raeisi-Dehkordi, H.; Dietvorst, C.A.W.; Dekker, R.; Uriza-Pinzón, J.P.; et al. Effects of Mediterranean diet, exercise, and their combination on body composition and liver outcomes in metabolic dysfunction-associated steatotic liver disease: a systematic review and meta-analysis of randomized controlled trials. BMC Med 2025, 23, 502. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yang, B.; Liu, Q.; Gao, M.; Luo, M. The long-term neuroprotective effect of MIND and Mediterranean diet on patients with Alzheimer's disease. Sci Rep 2025, 15, 32725. [Google Scholar] [CrossRef]
- Weiskirchen, R.; Lonardo, A. How 'miracle' weight-loss semaglutide promises to change medicine but can we afford the expense? Br J Pharmacol 2025, 182, 1651–1670. [Google Scholar] [CrossRef] [PubMed]
- Fiorucci, S.; Urbani, G.; Distrutti, E.; Biagioli, M. Obeticholic Acid and Other Farnesoid-X-Receptor (FXR) Agonists in the Treatment of Liver Disorders. Pharmaceuticals (Basel) 2025, 18. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Ratziu, V.; Loomba, R.; Anstee, Q.M.; Kowdley, K.V.; Rinella, M.E.; Sheikh, M.Y.; Trotter, J.F.; Knapple, W.; Lawitz, E.J.; et al. Results from a new efficacy and safety analysis of the REGENERATE trial of obeticholic acid for treatment of pre-cirrhotic fibrosis due to non-alcoholic steatohepatitis. J Hepatol 2023, 79, 1110–1120. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Abdelmalek, M.F.; Neff, G.; Gunn, N.; Guy, C.D.; Alkhouri, N.; Bashir, M.R.; Freilich, B.; Kohli, A.; Khazanchi, A.; et al. Aldafermin in patients with non-alcoholic steatohepatitis (ALPINE 2/3): a randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Gastroenterol Hepatol 2022, 7, 603–616. [Google Scholar] [CrossRef]
- Monteiro Delgado, L.; Fabretina de Souza, V.; Fontel Pompeu, B.; de Moraes Ogawa, T.; Pereira Oliveira, H.; Sacksida Valladão, V.D.C.; Lima Castelo Branco Marques, F.I. Long-Term Outcomes in Sleeve Gastrectomy versus Roux-en-Y Gastric Bypass: A Systematic Review and Meta-Analysis of Randomized Trials. Obes Surg 2025, 35, 3246–3257. [Google Scholar] [CrossRef]
- Custers, E.; Vreeken, D.; Kleemann, R.; Kessels, R.P.C.; Duering, M.; Brouwer, J.; Aufenacker, T.J.; Witteman, B.P.L.; Snabel, J.; Gart, E.; et al. Long-Term Brain Structure and Cognition Following Bariatric Surgery. JAMA Netw Open 2024, 7, e2355380. [Google Scholar] [CrossRef]
- Gasmi, A.; Bjørklund, G.; Mujawdiya, P.K.; Semenova, Y.; Peana, M.; Dosa, A.; Piscopo, S.; Gasmi Benahmed, A.; Costea, D.O. Micronutrients deficiences in patients after bariatric surgery. Eur J Nutr 2022, 61, 55–67. [Google Scholar] [CrossRef]
- Al Mansoori, A.; Shakoor, H.; Ali, H.I.; Feehan, J.; Al Dhaheri, A.S.; Cheikh Ismail, L.; Bosevski, M.; Apostolopoulos, V.; Stojanovska, L. The Effects of Bariatric Surgery on Vitamin B Status and Mental Health. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Song, D.; Li, Y.; Yang, L.L.; Luo, Y.X.; Yao, X.Q. Bridging systemic metabolic dysfunction and Alzheimer's disease: the liver interface. Mol Neurodegener 2025, 20, 61. [Google Scholar] [CrossRef]
- Moaket, O.S.; Obaid, S.E.; Obaid, F.E.; Shakeeb, Y.A.; Elsharief, S.M.; Tania, A.; Darwish, R.; Butler, A.E.; Moin, A.S.M. GLP-1 and the Degenerating Brain: Exploring Mechanistic Insights and Therapeutic Potential. Int J Mol Sci 2025, 26. [Google Scholar] [CrossRef]
- Weiskirchen, R. Hepatoprotective and Anti-fibrotic Agents: It's Time to Take the Next Step. Front Pharmacol 2015, 6, 303. [Google Scholar] [CrossRef]
- Galicia-Moreno, M.; Monroy-Ramirez, H.C.; Caloca-Camarena, F.; Arceo-Orozco, S.; Muriel, P.; Sandoval-Rodriguez, A.; García-Bañuelos, J.; García-González, A.; Navarro-Partida, J.; Armendariz-Borunda, J. A new opportunity for N-acetylcysteine. An outline of its classic antioxidant effects and its pharmacological potential as an epigenetic modulator in liver diseases treatment. Naunyn Schmiedebergs Arch Pharmacol 2025, 398, 2365–2386. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Cao, J.; Ma, Y.; Zhang, Y.; Liu, J.; Wang, H. Fecal Microbiota Transplantation Donor and Dietary Fiber Intervention Collectively Contribute to Gut Health in a Mouse Model. Front Immunol 2022, 13, 842669. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, G.; Guarnaccia, A.; Fancello, G.; Agrillo, C.; Iannarelli, F.; Sanguinetti, M.; Masucci, L. Fecal Microbiota Transplantation and Other Gut Microbiota Manipulation Strategies. Microorganisms 2022, 10. [Google Scholar] [CrossRef]
- Pujol, A.; Sanchis, P.; Tamayo, M.I.; Godoy, S.; Calvó, P.; Olmos, A.; Andrés, P.; Speranskaya, A.; Espino, A.; Estremera, A.; et al. Metabolic-Associated Fatty Liver Disease and Cognitive Performance in Type 2 Diabetes: Basal Data from the Phytate, Neurodegeneration and Diabetes (PHYND) Study. Biomedicines 2024, 12. [Google Scholar] [CrossRef]
- Mignot, V.; Chirica, C.; Tron, L.; Borowik, A.; Borel, A.L.; Rostaing, L.; Bouillet, L.; Decaens, T.; Guergour, D.; Costentin, C.E. Early screening for chronic liver disease: impact of a FIB-4 first integrated care pathway to identify patients with significant fibrosis. Sci Rep 2024, 14, 20720. [Google Scholar] [CrossRef]
- Chen, M.J.; Chen, Y.; Lin, J.Q.; Hu, R.; Liu, D.; Chen, J.Y.; Li, K.; Jiang, X.Y. Evidence summary of lifestyle interventions in adults with metabolic dysfunction-associated steatotic liver disease. Front Nutr 2024, 11, 1421386. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Zelber-Sagi, S.; Lazarus, J.V.; Wong, V.W.; Yilmaz, Y.; Duseja, A.; Eguchi, Y.; Castera, L.; Pessoa, M.G.; Oliveira, C.P.; et al. Global Consensus Recommendations for Metabolic Dysfunction-Associated Steatotic Liver Disease and Steatohepatitis. Gastroenterology 2025, 169, 1017–1032.e1012. [Google Scholar] [CrossRef]
- Preshy, A.; Brown, J. A Bidirectional Association Between Obstructive Sleep Apnea and Metabolic-Associated Fatty Liver Disease. Endocrinol Metab Clin North Am 2023, 52, 509–520. [Google Scholar] [CrossRef]
- Iruzubieta, P.; Terán, Á.; Crespo, J.; Fábrega, E. Vitamin D deficiency in chronic liver disease. World J Hepatol 2014, 6, 901–915. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Department for HIV T, Hepatitis and Sexually Transmitted Infections. Global Health Sector Strategies 2022–2030 Geneva: World Health Organization; 2022 [cited 2025 21 November]. Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/strategies/global-health-sector-strategies.
- Rehm, J.; Shield, K.D. Global Burden of Alcohol Use Disorders and Alcohol Liver Disease. Biomedicines 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- El Zibaoui, R.; Díaz, L.A.; Idalsoaga, F.; Arab, J.P. Public Health Policies and Strategies to Prevent Alcohol-Related Morbidity and Mortality. Current Hepatology Reports 2025, 24, 20. [Google Scholar] [CrossRef]
- de Jong, V.D.; Alings, M.; Bruha, R.; Cortez-Pinto, H.; Dedoussis, G.V.; Doukas, M.; Francque, S.; Fournier-Poizat, C.; Gastaldelli, A.; Hankemeier, T.; et al. Global research initiative for patient screening on MASH (GRIPonMASH) protocol: rationale and design of a prospective multicentre study. BMJ Open 2025, 15, e092731. [Google Scholar] [CrossRef]
- van Kleef, L.A.; Strandberg, R.; Pustjens, J.; Hammar, N.; Janssen, H.L.A.; Hagström, H.; Brouwer, W.P. FIB-4-based Referral Pathways Have Suboptimal Accuracy to identify Increased Liver Stiffness and Incident Advanced Liver Disease. Clin Gastroenterol Hepatol 2025. [Google Scholar] [CrossRef]
- Selvaraj, E.A.; Mózes, F.E.; Jayaswal, A.N.A.; Zafarmand, M.H.; Vali, Y.; Lee, J.A.; Levick, C.K.; Young, L.A.J.; Palaniyappan, N.; Liu, C.-H.; et al. Diagnostic accuracy of elastography and magnetic resonance imaging in patients with NAFLD: A systematic review and meta-analysis. Journal of Hepatology 2021, 75, 770–785. [Google Scholar] [CrossRef]
- Mikkelsen, A.C.D.; Kjærgaard, K.; Schapira, A.H.V.; Mookerjee, R.P.; Thomsen, K.L. The liver–brain axis in metabolic dysfunction-associated steatotic liver disease. The Lancet Gastroenterology & Hepatology 2025, 10, 248–258. [Google Scholar] [CrossRef]
- Pan, L.; Xie, L.; Yang, W.; Feng, S.; Mao, W.; Ye, L.; Cheng, H.; Wu, X.; Mao, X. The role of brain–liver–gut Axis in neurological disorders. Burns & Trauma 2025, 13. [Google Scholar] [CrossRef]
- Chiu, W.C.; Tsan, Y.T.; Tsai, S.L.; Chang, C.J.; Wang, J.D.; Chen, P.C. Hepatitis C viral infection and the risk of dementia. Eur J Neurol 2014, 21, 1068–e1059. [Google Scholar] [CrossRef]
- Bao, X.; Kang, L.; Yin, S.; Engström, G.; Wang, L.; Xu, W.; Xu, B.; Zhang, X.; Zhang, X. Association of MAFLD and MASLD with all-cause and cause-specific dementia: a prospective cohort study. Alzheimer's Research & Therapy 2024, 16, 136. [Google Scholar] [CrossRef]
- Javeed, A.; Dallora, A.L.; Berglund, J.S.; Ali, A.; Ali, L.; Anderberg, P. Machine Learning for Dementia Prediction: A Systematic Review and Future Research Directions. Journal of Medical Systems 2023, 47, 17. [Google Scholar] [CrossRef] [PubMed]
- Exarchos, T.P.; Dimakopoulos, G.A.; Lazaros, K.; Krokidis, M.; Vrahatis, A.; Grammenos, G.; Avramouli, A.; Skolariki, K.; Adams, R.; Mahairaki, V.; et al. Five-year dementia prediction and decision support system based on real-world data. Frontiers in Aging Neuroscience 2025, 17–2025. [Google Scholar] [CrossRef]
- Vemulapalli, B.; Ghattu, M.; Atluri, K.; Lee, J.; Rustgi, V. Artificial Intelligence and Machine Learning Applications in Liver Disease. Clinics in Liver Disease 2025, 29, 755–770. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Y.; Liu, S.; Yang, M. Treatment of liver fibrosis: Past, current, and future. World J Hepatol 2023, 15, 755–774. [Google Scholar] [CrossRef]
Figure 1.
Principal risk factors for advanced liver fibrosis and cirrhosis. Original illustration created using Servier Medical ART (SMART) and is licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0). The main risk factors for advanced liver fibrosis and cirrhosis are based on data from Zamani et.al [1]. Additionally, more rare causes of fibrosing liver disease include autoimmune, genetic, and drug-related etiologies of fibrosing chronic liver disease (CLD) [15]. In MASH, the independent predictors for significant and advanced fibrosis, respectively, are waist circumference, metabolic syndrome, and ALT; age, platelets, HOMA, diabetes, and total cholesterol, suggesting that systemic metabolic dysfunction is very closely associated with liver fibrosis [16].
Figure 1.
Principal risk factors for advanced liver fibrosis and cirrhosis. Original illustration created using Servier Medical ART (SMART) and is licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0). The main risk factors for advanced liver fibrosis and cirrhosis are based on data from Zamani et.al [1]. Additionally, more rare causes of fibrosing liver disease include autoimmune, genetic, and drug-related etiologies of fibrosing chronic liver disease (CLD) [15]. In MASH, the independent predictors for significant and advanced fibrosis, respectively, are waist circumference, metabolic syndrome, and ALT; age, platelets, HOMA, diabetes, and total cholesterol, suggesting that systemic metabolic dysfunction is very closely associated with liver fibrosis [16].
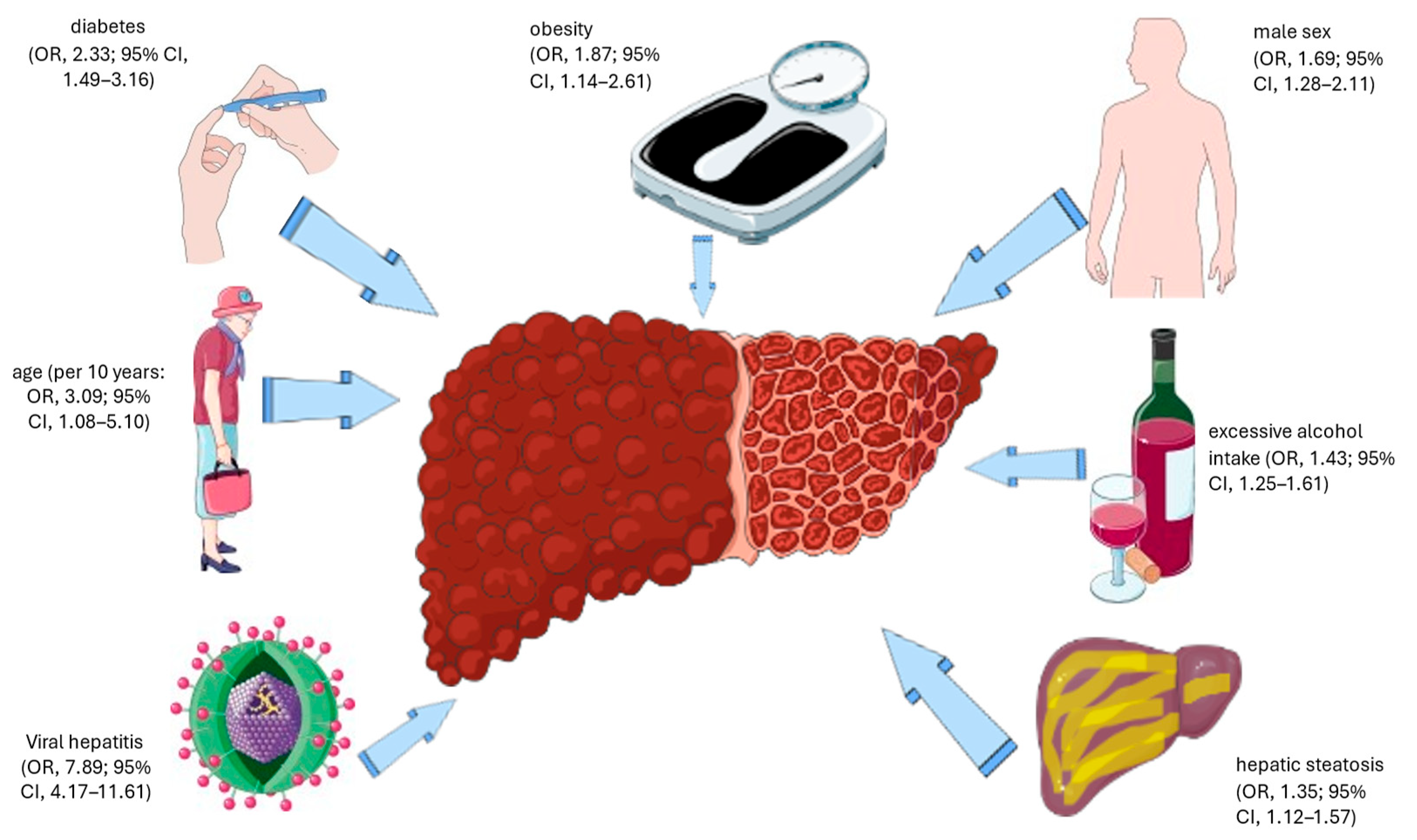
Figure 2.
Categorization of Dementia.
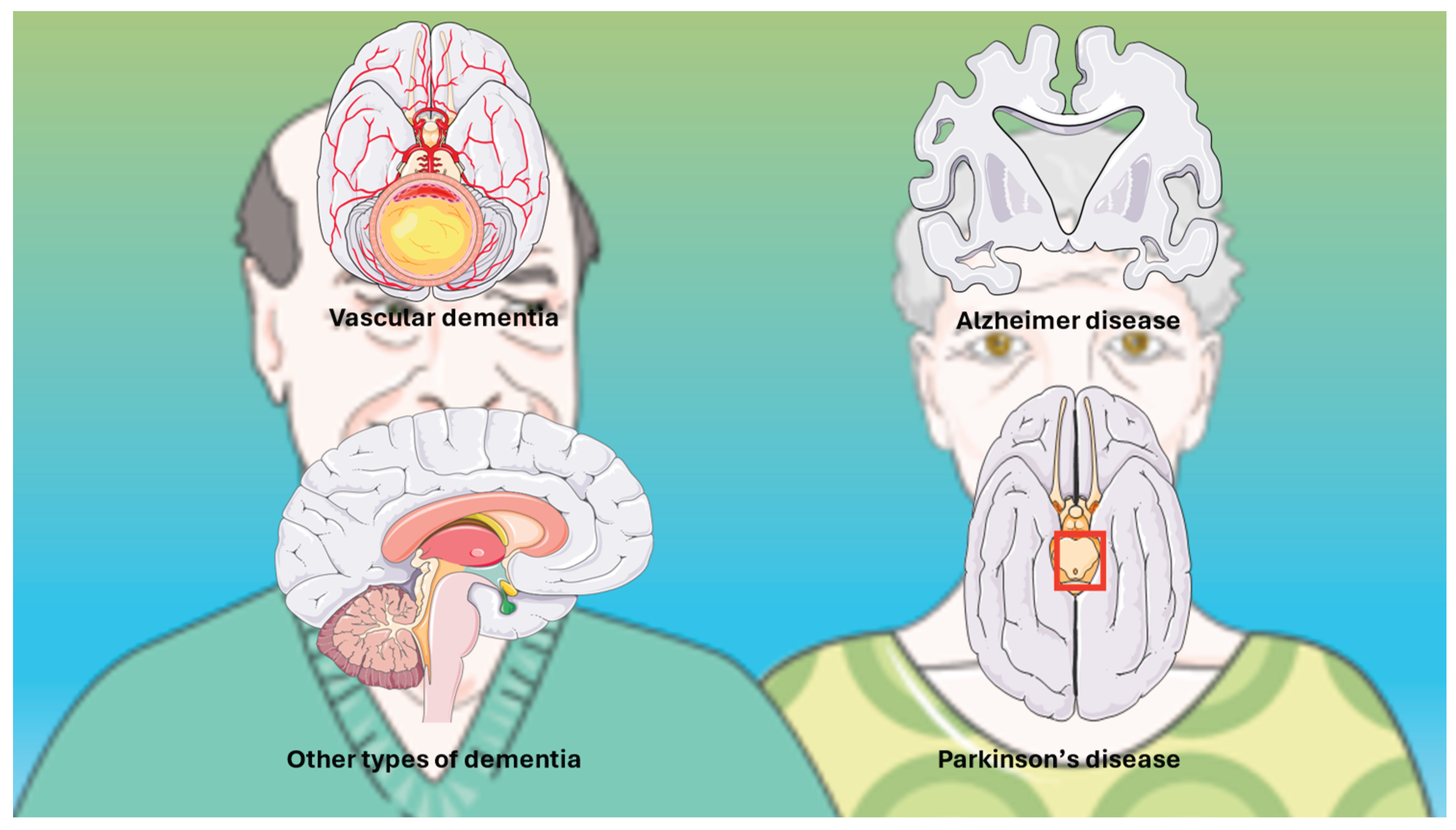
Figure 3.
Putative mechanistic pathways linking liver fibrosis with the risk of dementia. This figure illustrates the complex biological pathways through which liver fibrosis may contribute to accelerated brain aging and an increased risk of dementia. The pathways integrate metabolic, vascular, inflammatory, and neurotoxic mechanisms described throughout the manuscript, highlighting how hepatic dysfunction can influence cerebral structure, function, and neurodegenerative processes. Abbreviations: BBB, blood–brain barrier; WMH, white matter hyperintensity; AD, Alzheimer’s disease; VD, vascular dementia. Icons used in Figure 3 were sourced from flaticon.com.
Figure 3.
Putative mechanistic pathways linking liver fibrosis with the risk of dementia. This figure illustrates the complex biological pathways through which liver fibrosis may contribute to accelerated brain aging and an increased risk of dementia. The pathways integrate metabolic, vascular, inflammatory, and neurotoxic mechanisms described throughout the manuscript, highlighting how hepatic dysfunction can influence cerebral structure, function, and neurodegenerative processes. Abbreviations: BBB, blood–brain barrier; WMH, white matter hyperintensity; AD, Alzheimer’s disease; VD, vascular dementia. Icons used in Figure 3 were sourced from flaticon.com.
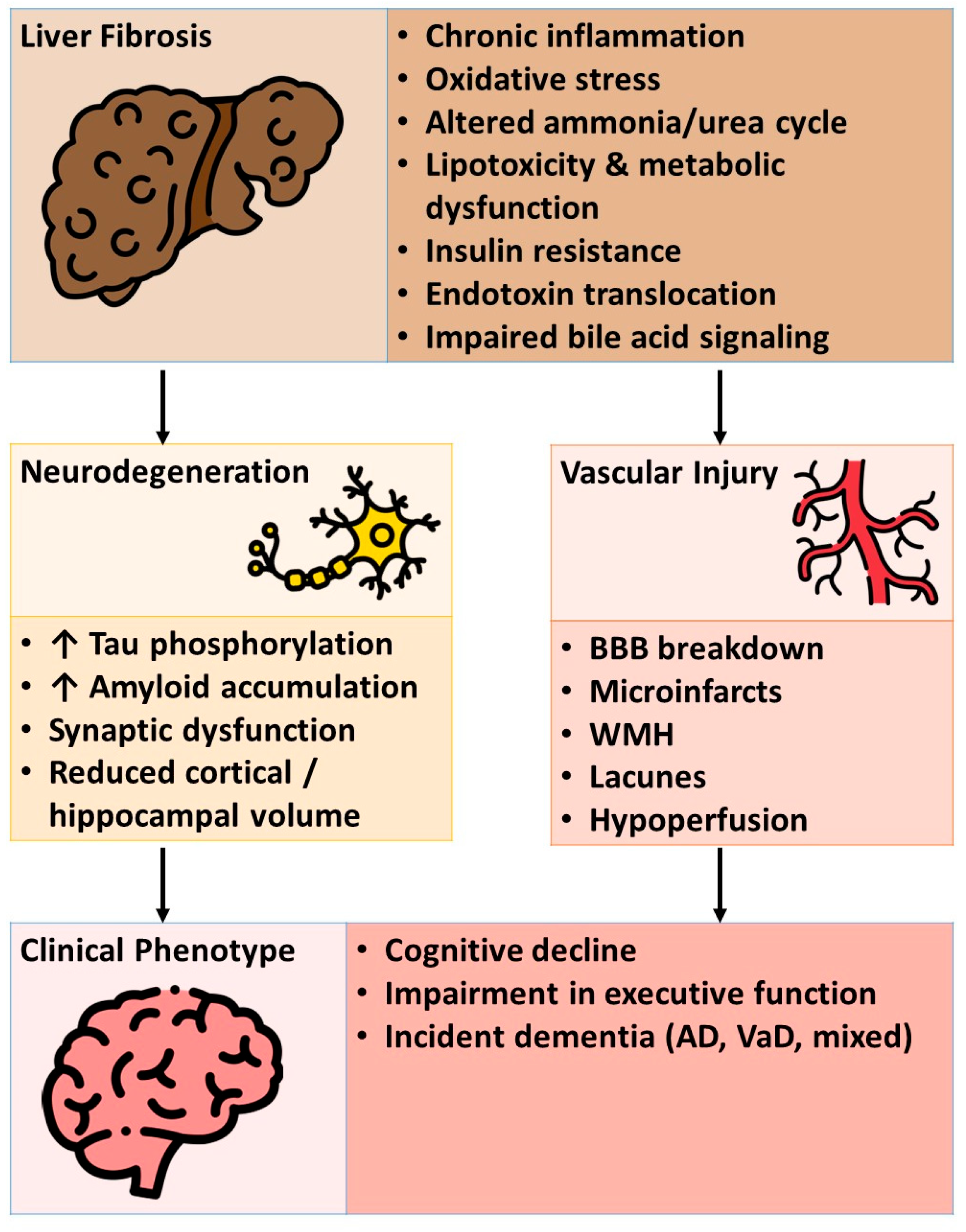
Figure 4.
Schematic illustration of the most used non-invasive tests for liver fibrosis. Original illustration created using Servier Medical ART (SMART) and licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0). Abbreviations: APRI, aminotransferase–platelet ratio index; ELF, enhanced liver fibrosis score; FIB-4, fibrosis-4 index; MRE, magnetic resonance elastography; NFS, NAFLD fibrosis score; PSWE, point shear wave elastography; 2DSWE, two-dimensional shear wave elastography; VCTE, vibration-controlled transient elastography.
Figure 4.
Schematic illustration of the most used non-invasive tests for liver fibrosis. Original illustration created using Servier Medical ART (SMART) and licensed under the Creative Commons Attribution 4.0 International License (CC BY 4.0). Abbreviations: APRI, aminotransferase–platelet ratio index; ELF, enhanced liver fibrosis score; FIB-4, fibrosis-4 index; MRE, magnetic resonance elastography; NFS, NAFLD fibrosis score; PSWE, point shear wave elastography; 2DSWE, two-dimensional shear wave elastography; VCTE, vibration-controlled transient elastography.
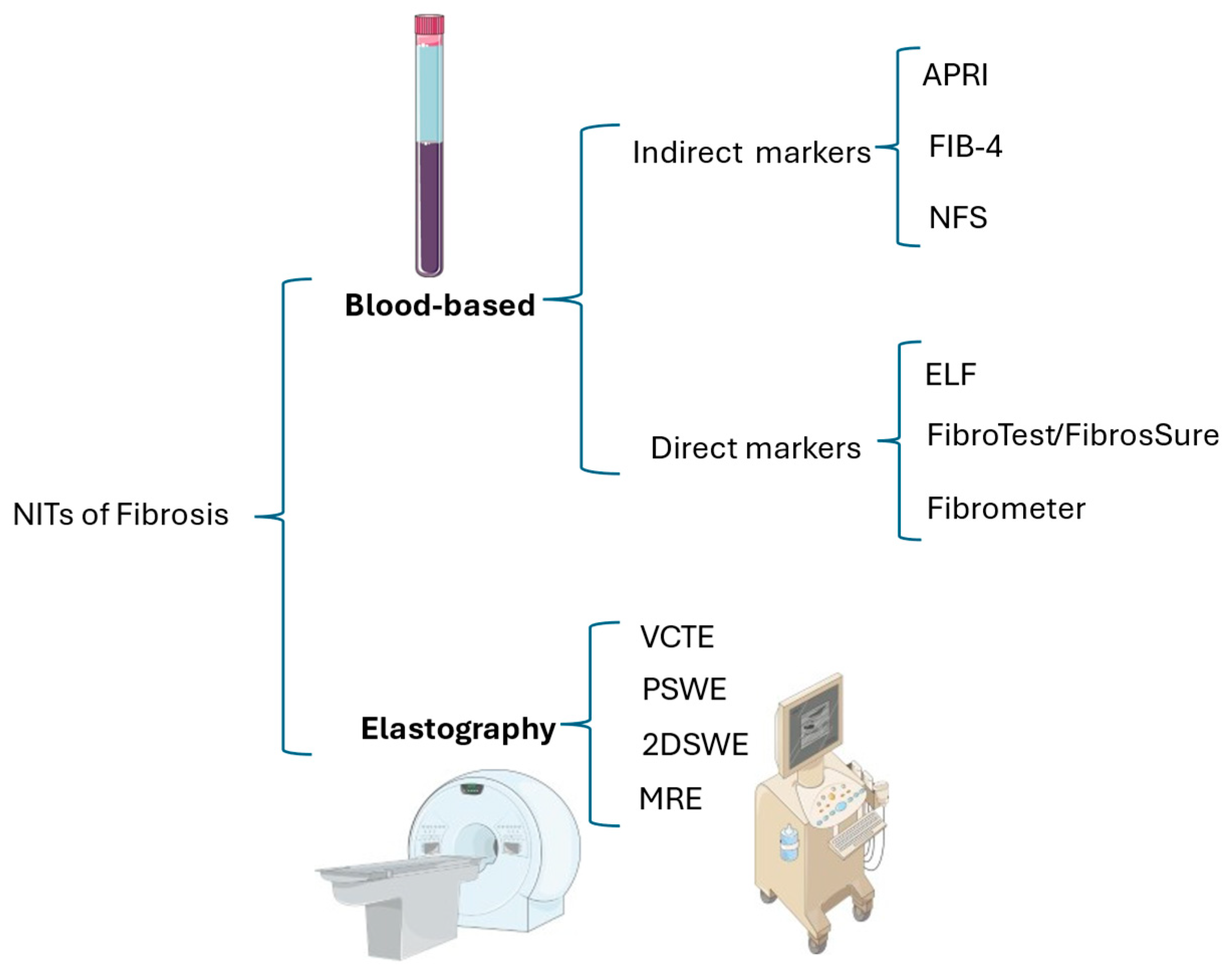
Table 1.
Meta-analytic estimates of advanced fibrosis and cirrhosis in men and women [1].
|
Global Prevalence of Advanced Fibrosis |
Global Prevalence of Cirrhosis |
|
| Overall | 3.3% (95% CI, 2.4–4.2) | 1.3% (95% CI, 0.9–1.7) |
| In men | 3.5% (95% CI, 2.6–4.5) | 2.5% (95% CI, 1.0–4.0) |
| In women | 2.2% (95% CI, 1.3–3.1) | 0.9% (95% CI, 0.0–1.8) |
Abbreviations: CI, confidence interval.
Table 2.
Summary of key studies linking liver fibrosis and metabolic liver disease to brain structure, cognition, and Alzheimer’s disease pathology.
Table 2.
Summary of key studies linking liver fibrosis and metabolic liver disease to brain structure, cognition, and Alzheimer’s disease pathology.
| Author, [Ref] | Method | Findings | Comment |
| Gao et al. [59] | Prospective cohort study of 431,699 UK Biobank participants with a mean follow-up of 8.65 ± 2.61 years. Cox proportional hazards analysis was used to assess associations of liver markers (ALT, AST, AST/ALT ratio, GGT), alcoholic liver disease, fibrosis, and cirrhosis with incident dementia. Additionally, linear regression was used to evaluate cognition and brain structure. | Each SD decrease in ALT is associated with a lower risk of all-cause dementia (HR 0.917, PFDR<0.001). Conversely, each SD increase in AST (HR 1.048, PFDR=0.010), AST/ALT ratio (HR 1.195, PFDR<0.001), GGT (HR 1.066, PFDR<0.001), alcoholic liver disease (HR 2.872, PFDR<0.001), and fibrosis/cirrhosis (HR 2.285, PFDR=0.002) increases the risk of dementia. Cognition shows a positive correlation with AST, AST/ALT, DBil, and GGT, and a negative correlation with ALT, albumin, and TBil. ALT, GGT, AST/ALT, and ALD are linked to cortical/subcortical changes in regions such as the hippocampus, amygdala, thalamus, pallidum, and fusiform (PFDR<0.05). | Large-scale evidence indicates that liver dysfunction predicts dementia and cognitive impairment, and is associated with cortical/subcortical changes |
| Weinstein et al. [60] | A cross-sectional meta-analysis was conducted on 5660 individuals with NAFLD and 3022 individuals with fibrosis, who were free of dementia and stroke, from the FHS, RS, and SHIP cohorts. NAFLD was assessed using abdominal imaging, while fibrosis was assessed using FibroScan. Linear regression was used to analyze total brain volume, gray matter volume, hippocampal volumes, and WMH. | NAFLD is associated with smaller total brain volume (β=-3.5, 95% CI -5.4 to -1.7), gray matter volume (β=-1.9, 95% CI -3.4 to -0.3), and cortical gray matter volume (β=-1.9, 95% CI -3.7 to -0.01). Fibrosis (liver stiffness ≥8.2 kPa) is linked to smaller total brain volume (β=-7.3, 95% CI -11.1 to -3.5). There is low heterogeneity. | This suggests that NAFLD and fibrosis may play a role in brain aging. |
| Weinstein et al. [61] | Participants from the Framingham Offspring and Third Generation cohorts underwent amyloid (11C-PiB) and tau (18F-Flortaucipir) PET scans, as well as abdominal CT scans or had FIB-4 data. Linear regression was used to assess associations of NAFLD and FIB-4 with regional tau and amyloid-β levels, adjusting for confounders. | FIB-4 is associated with increased rhinal tau levels (β=1.03±0.33, p=0.002). In NAFLD participants, higher FIB-4 levels are correlated with increased tau in regions such as the inferior temporal (β=2.01±0.47, p<0.001), parahippocampal (β=1.60±0.53, p=0.007), entorhinal (β=1.59±0.47, p=0.003), and rhinal cortex (β=1.60±0.42, p=0.001), as well as increased overall amyloid-β (β=1.93±0.47, p<0.001) and in regions like inferior temporal/parahippocampal. | Liver fibrosis, as opposed to NAFLD alone, could drive early Alzheimer’s pathology, including tau accumulation in certain brain regions. |
| Fan et al. [62] | A cross-sectional study was conducted on 29,195 UK Biobank participants aged 45–82 who underwent T1, T2 FLAIR, and DTI MRI scans. MASLD was defined as MRI-PDFF ≥5% plus ≥1 cardiometabolic criterion. Multiple linear regression was used to assess total and subcortical gray matter, AD-signature cortical thickness, WMH, FA, and MD. | MASLD is associated with smaller total/subcortical gray matter (p<0.05) and reduced cortical thickness in AD signature/regions (β=-0.04, 95% CI -0.07, -0.01). Higher total WMH volume (β=0.12, 95% CI 0.10, 0.15), increased global FA (β=0.05, 95% CI 0.03, 0.08), and reduced global MD (β=-0.04, 95% CI -0.07, -0.01). | MASLD affects gray and white matter integrity, further supporting a connection between liver metabolic dysfunction and brain structure. |
Abbreviations: β, regression coefficient; ACD, all-cause dementia; AD, Alzheimer’s disease; ALD, alcoholic liver disease; ALT, alanine transaminase; AST, aspartate transaminase; CI, confidence interval; FA, fractional anisotropy; FIB-4, fibrosis-4 index; GGT, gamma-glutamyl transpeptidase; HR, hazard ratio; MASLD, metabolic dysfunction-associated steatotic liver disease; MD, mean diffusivity; MRI, magnetic resonance imaging; MRI-PDFF, magnetic resonance imaging–proton density fat fraction; NAFLD, non-alcoholic fatty liver disease; PET, positron emission tomography; PFDR, false discovery rate–adjusted p value; VaD, vascular dementia; WMH, white matter hyperintensity.
Table 3.
Blood-based indirect NITs.
|
Test (calculation) |
Condition | Cutoff | Sensitivity (%) | Specificity/NPV% | Reference |
| APRI (AST level ÷ ULN ÷ platelet count) |
Significant fibrosis due to HBV Cirrhosis due to HCV |
> 0.35 >1.0 |
78 76 |
63 71 |
Yue et al. [105] Shaheen et al. [106] |
| FIB-4 (age × AST level) ÷ (platelet count × √ALT level) |
Significant fibrosis due to HCV | <1.45 >3.25 |
60-92 11-54 |
52-95 91-98 |
Xu et al. [107] |
| NFS (−1.675 + (0.037 × age) + (0.094 × BMI) + (1.13 × IR or diabetes [yes = 1, no = 0]) + (0.99 × AST:ALT ratio) − (0.013 × platelet count) − (0.66 × albumin) |
Identification of individuals with MASLD at risk of developing fibrosis | -0.835 | 100 | 70 | Torres et al. [108] |
Abbreviations used: BMI, body mass index; ALT, alanine transaminase; AST, aspartate transaminase; HBV, Hepatitis B Virus; HCV, Hepatitis C Virus; IR, insulin resistance; ULN, upper limit of normal. Cirrhosis defined as METAVIR F=4; Significant fibrosis defined as METAVIR F≥2.
Table 4.
Meta-analytic evidence supporting the use of biomarkers for diagnosing dementia.
| Author, year [Ref] | Method | Findings | Conclusion |
| Gaur, 2023[119] | Meta-analysis of 10 studies | In CSF, concentrations of NfL (SMD=0.69 [0.56, 0.83]), GFAP (SMD=0.41 [0.07, 0.75]), and HFABP (SMD=0.57 [0.26, 0.89]) were elevated in individuals with MCI. In blood, increased concentrations of T-tau (SMD=0.19 [0.09, 0.29]), NfL (SMD=0.41 [0.32, 0.49]), and GFAP (SMD=0.39 [0.23, 0.55]) were found in MCI. |
Levels of NfL and GFAP can be measured in both CSF and blood. Monitoring these biomarkers may provide valuable information about neurodegeneration in individuals with MCI. |
| Ma, 2024[120] | Meta-analysis of 63 studies | The following biomarkers were significantly higher in patients with PSCI compared to the non-PSCI group: Hcy (p<0.00001), CRP (p=0.0008), UA (p=0.02), IL-6 (p=0.005), Cys-C (p=0.0001), creatinine (p<0.00001) and TNF-α (p=0.02). | Integrating of neuroimaging and neuropsychological assessments with blood biomarker levels is crucial for evaluating the risk of PSCI. |
| Chen, 2024[121] | Meta-analysis of 13 studies | A notable elevation in MI concentration was found, along with reductions in Glu, Glx, and NAA/Cr ratios in DCI. | These biomarkers are highly sensitive metabolic indicators for assessing the progression of DCI. |
| Huang, 2025[122] | Meta-analysis of 30 studies | Peripheral Aβ42 levels, the Aβ42/Aβ40 ratio, NfL, and S100B show significant differences between VCI and non-VCI groups. | Peripheral Aβ42, the Aβ42/Aβ40 ratio, NfL, and S100B are potential blood biomarkers for VCI. |
Abbreviations: Aβ40, amyloid beta 40; Aβ42, amyloid beta 42; BDNF, brain-derived neurotrophic factor; CRP, C-reactive protein; CSF, cerebrospinal fluid; Cys-C, cystatin C; DCI, diabetic cognitive impairment; GFAP, glial fibrillary acidic protein; Glu, glutamate; Glx, composite of glutamate and glutamine; Hcy, homocysteine; IL-6, interleukin-6; TNF-α, tumor necrosis factor-α; HFABP, heart-type fatty acid binding protein; MCI, mild cognitive impairment; MI, myo-inositol; NAA/Cr, N-acetylaspartate/creatine; NfL, neurofilament light chain; PSCI, post-stroke cognitive impairment; p-tau 181, phosphorylated tau 181; SMDs, standardized mean differences; sRAGE, soluble receptor for advanced glycation end products; T-tau, total tau; UA, uric acid; VCI, vascular cognitive impairment.
Table 5.
Specific dementia risk algorithms.
| Risk Prediction Model | Parameters Included | Comment | References |
| CAIDE Dementia Risk Score | Age, sex, Education Level, Physical Inactivity, SBP, TChol, BMI. | Originally developed to predict the 20-year dementia risk among middle-aged Finnish individuals, this is the most established and frequently used mid-life risk score for predicting future dementia risk. | Kivipelto et al. [123] Farkas et al. [124] |
| ANU-ADRI | Age, sex, education level, BMI, diabetes, depression, TChol, traumatic brain injury, smoking, alcohol intake, social engagement, physical activity, cognitive activity, fish intake, and pesticide exposure. | In contrast to constructing risk indices using individual cohort studies, this methodology enables the inclusion of a broader range of risk factors, enhances the generalizability of outcomes, and facilitates the integration of interactions informed by research conducted across various stages of the life course. | Anstey et al. [125] |
| UKBDRS | Age, education, parental history of dementia, material deprivation, a history of diabetes, stroke, depression, hypertension, high cholesterol, household occupancy, and sex | This is an easy-to-use tool to identify individuals at risk of dementia in the UK. Further research is required to determine the validity of this score in other populations. | Anaturk et al. [126] |
| CogDrisk tool | Age, sex, education, HTN, midlife obesity, midlife high cholesterol, diabetes, insufficient physical activity, depression, TBI, AF, smoking, social engagement, cognitive engagement, fish consumption, stroke, and insomnia. | A comprehensive risk assessment tool for AD, VaD, and any other type of dementia, which will be applicable in high and low-resource settings. | Anstey et al. [127,128] |
| LIBRA and LIBRA2 | LIBRA focuses on 12 modifiable lifestyle and vascular risk factors, while the updated LIBRA2 version adds three more: hearing impairment, social contact, and sleep. | LIBRA2 demonstrates improved capability in identifying individuals at elevated risk for dementia and serves as an effective tool for public health initiatives focused on reducing dementia risk. | Rosenau et al. [129] |
Abbreviations: AD, Alzheimer’s disease; AF, atrial fibrillation; ANU-ADRI, Australian National University’s Alzheimer’s Disease Risk Index; BMI, body mass index; CAIDE, Cardiovascular Risk Factors, Aging, and Dementia; HTN, arterial hypertension; LIBRA, Lifestyle for Brain Health; SBP, systolic blood pressure; TBI, traumatic brain injury; TChol, total cholesterol; UKB-DRP, UK Biobank Dementia Risk Prediction; VaD, vascular dementia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



