
Submitted:
02 December 2025
Posted:
05 December 2025
You are already at the latest version
Abstract
Background: Bipolar disorder secondary to traumatic brain injury (TBI) is common, mechanistically distinct, and notoriously treatment-resistant. Rapid-acting glutamatergic antidepressants such as ketamine are effective in bipolar depression but remain inaccessible to most patients.Case presentation: We describe a woman in her mid-thirties with documented right frontal atrophy after a severe violence-related subdural hematoma in 2009, subsequent onset of cyclothymic-to-bipolar illness, and recent severe depressive relapse with insomnia, auditory hallucinations, PHQ-9 = 22 and GAD-7 = 14. Conventional treatment (valproate, low-dose risperidone, lemborexant, and Deanxit [flupentixol 0.5 mg + melitracen 15 mg]) produced minimal benefit. On 5 November 2025, low-dose dextromethorphan 30 mg nightly and piracetam 600 mg nightly were added. Melitracen, a moderate CYP2D6 inhibitor, inadvertently prolonged dextromethorphan exposure, effectively replicating the pharmacokinetic principle of Auvelity® while piracetam supplied AMPA positive allosteric modulation.Results: Within four weeks the patient reported marked mood stabilization and reduced ruminations. Transient mild hypomania with moria-like inappropriate laughter emerged, prompting spontaneous reduction of dextromethorphan to 22.5 mg nightly and upward titration of piracetam to 1 200 mg, after which euthymia was restored and maintained. No dissociation or worsening psychosis occurred.Conclusions: This case provides the first clinical illustration that an ultra-low-cost, fully oral glutamatergic oral regimen (dextromethorphan + unintended CYP2D6 inhibition + piracetam) can produce ketamine-class speed and magnitude of response in secondary bipolar depression after TBI, even at dextromethorphan doses far below those in licensed combinations. The narrow therapeutic window and hypomanic overshoot highlight the heightened glutamatergic sensitivity of the post-TBI brain.
Keywords:
bipolar disorder
; traumatic brain injury
; secondary bipolar disorder
; post-TBI mood disorder
; glutamatergic modulation
; dextromethorphan
; piracetam
; CYP2D6 inhibition
; Auvelity
; NMDA receptor antagonist
; AMPA positive allosteric modulator
; rapid antidepressant response
; hypomania
; treatment-resistant bipolar depression
; organic bipolar disorder
; frontal lobe atrophy
; ketamine-like effect
; over-the-counter augmentation
; case report
Introduction
Traumatic brain injury (TBI) is one of the most robust environmental risk factors for later-life mood disorders. Danish and Taiwanese registry studies report a three- to five-fold rise in new-onset bipolar disorder after moderate or severe head trauma [1,2]. When bipolar illness follows TBI it often carries a recognisable signature: marked irritability, emotional lability, cognitive impulsiveness, migraine comorbidity, and poor response to standard mood stabilisers—features thought to stem from chronic neuro-inflammation and damage to prefrontal–limbic circuits [3,4]. Because conventional monoaminergic drugs rarely deliver full remission in this subgroup, clinicians have begun to explore treatments that act further upstream on synaptic plasticity.
Intravenous ketamine paved the way by showing that a brief NMDA-receptor blockade, followed by a burst of AMPA throughput and mTOR-driven synaptogenesis, can lift mood within hours [5,6]. Yet ketamine's cost, need for monitoring, and dissociative side-effects limit its reach. An emerging alternative is the fully oral "Cheung glutamatergic regimen", which pairs dextromethorphan (DXM)—a σ₁-active NMDA antagonist—with a CYP2D6 inhibitor to slow DXM metabolism, then adds piracetam as an AMPA positive allosteric modulator and, optionally, L-glutamine to replenish presynaptic glutamate [7]. Early reports describe rapid, sometimes dramatic, benefit across refractory depression, schizoaffective disorder, obsessive–compulsive disorder, binge-eating disorder, trauma-related illness, and functional somatic syndromes, usually with inexpensive over-the-counter doses [8,9,10,11,12,13].
To our knowledge, no published case has examined this oral NMDA/AMPA stack in bipolar disorder that emerged after TBI. We therefore present the case of a woman in her mid-thirties with right-frontal atrophy from a domestic-violence subdural haematoma whose cyclothymic-bipolar course began immediately after the injury. During a severe depressive relapse she received low-dose DXM and piracetam on top of a regimen that inadvertently provided strong CYP2D6 inhibition. The intervention produced a rapid antidepressant response followed by a brief hypomanic overshoot, offering a window into both the promise and the risks of oral glutamatergic augmentation in post-TBI bipolarity.
Methods
This report describes the ordinary course of care for a single patient treated in a private outpatient psychiatry practice in Hong Kong SAR. Because no experimental procedures were added, the work took the form of a naturalistic, observational case study rather than a formal trial.
After a detailed discussion of risks and benefits, the patient gave written permission for her anonymised history, treatment, and outcome to be published. All potentially identifying information has been removed or modified.
Clinical status was reviewed at every visit through an unstructured interview and full mental-state examination, supplemented by three brief rating scales that the patient completed herself: the Patient Health Questionnaire-9 (PHQ-9) for depression, and the Generalised Anxiety Disorder-7 (GAD-7) for anxiety. Historical hospital notes and two magnetic-resonance imaging reports (2009 and 2019) documenting right-frontal atrophy were also available.
Medication changes were guided solely by day-to-day clinical judgment. On 21 October 2025 the baseline regimen consisted of sodium valproate 300 mg at night, risperidone 0.5 mg at night, lemborexant 5 mg for insomnia, as-needed alprazolam, and one morning tablet of Deanxit (flupentixol 0.5 mg + melitracen 15 mg). When mood and sleep had not improved by 5 November, dextromethorphan hydrobromide 30 mg at night and piracetam 600 mg at night were added. At the 2 December review the patient herself had reduced dextromethorphan to 22.5 mg nightly; piracetam was increased to 1 200 mg nightly and valproate to 500 mg nightly, while the remaining drugs were continued unchanged. No blood levels of dextromethorphan/dextrorphan were drawn and CYP2D6 genotyping was not performed.
The principal endpoints were change in PHQ-9 score, the patient's subjective sense of mood stability and sleep quality, and any emergence of hypomanic or manic features. Safety surveillance relied on both spontaneous reports and direct questioning about dissociative phenomena, psychotic symptoms, and possible serotonergic adverse effects. All observations were extracted retrospectively from the electronic chart, contemporaneous handwritten notes, and the patient's own diary entries.
Results
Ms. A is a woman in her mid-thirties who carries a diagnosis of bipolar disorder—currently judged to follow a cyclothymic course—and a documented traumatic brain injury (Figure 1). She arrived at the clinic on 21 October 2025 complaining of two months of relentless insomnia that had not responded to melatonin. Along with the sleeplessness she described pervasive insecurity, catastrophic ruminations, and, paradoxically, bursts of high energy during which her mind raced over unfinished tasks. Two days before the visit she heard child-like voices telling her, for example, that "if she is going, she needs to bring her daughter as well." Intake screening placed her PHQ-9 at 22, indicating severe depression, and her GAD-7 at 14, suggesting moderate anxiety.
Her medical background is notable for a traumatic subdural hematoma sustained during domestic violence. MRI in 2009 showed right frontal lobe atrophy, and repeat imaging ten years later confirmed progression, mirroring gradual changes in personality and emotional regulation observed by family. Psychiatric history goes back to a first depressive episode in 2009, followed by postpartum irritability and a spell in 2018 that looked hypomanic—compulsive shopping for items of specific colors and impairment at work—about which she remembers only fragments. A maternal grandmother had bipolar-spectrum symptoms.
Initial treatment on 21 October combined sodium valproate 300 mg, risperidone 0.5 mg, alprazolam as needed, lemborexant for sleep, and Deanxit (flupentixol + melitracen) one tablet daily. Two weeks later, on 5 November, Ms. A returned with worsening mood, irritability, and hypnagogic hallucinations; the PHQ-9 had fallen to 15, but her distress felt unchanged. A "glutamatergic regimen" was added: dextromethorphan 30 mg nightly alongside piracetam 600 mg, while Deanxit was continued. The choice was deliberate—melitracen inhibits CYP2D6, the enzyme that normally metabolises dextromethorphan, so keeping Deanxit on board was meant to raise DM's bioavailability and strengthen its NMDA-antagonist and sigma-1 agonist actions.
By 2 December, one month into the full combination, her presentation had shifted. Mood was mildly elevated with occasional, inexplicable laughter that gave a moria-like quality to her affect. She spontaneously cut her dextromethorphan from 30 mg to 22.5 mg and reported feeling "better and more stable" at the lower dose. The episode suggested that Deanxit had indeed boosted dextromethorphan to a level that, in the context of right frontal atrophy (a region associated with inhibitory control), pushed her into hypomanic territory.
At last review her daily medications were Deanxit one tablet, dextromethorphan 22.5 mg, piracetam 1 200 mg, sodium valproate 500 mg, and risperidone 0.5 mg, with alprazolam 0.25–0.5 mg available as needed.
Conclusion
Ms A's trajectory illustrates how a remote frontal head injury can colour the entire clinical picture of bipolar illness. Her right-frontal subdural haematoma, documented atrophy on serial MRI, late-onset mood lability and outsized irritability all echo the "organic" bipolar profile described in epidemiologic and cross-sectional work [1,3,4]. Such patients tend to show more disruptive affect, impulsivity and migraine than those with idiopathic bipolar disorder—each element readily recognisable in Ms A.
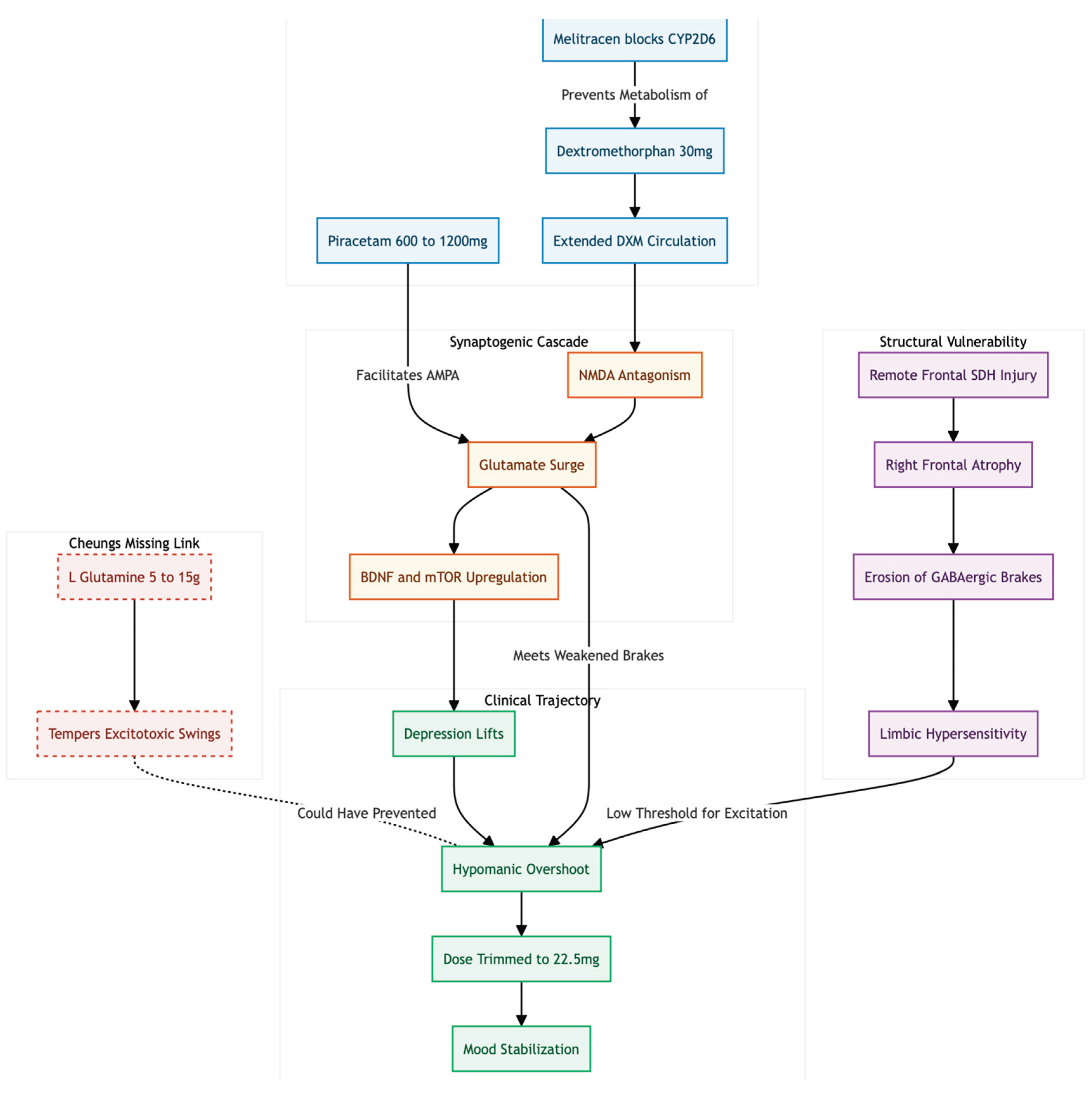
The therapeutic twist came when a low-cost glutamatergic stack was added (Figure 2): dextromethorphan (DXM) 30 mg plus piracetam 600–1 200 mg, layered on continuing Deanxit. Melitracen, one half of Deanxit, is a moderate CYP2D6 inhibitor; by remaining in the regimen it inadvertently duplicated the pharmacokinetic logic behind Auvelity®, keeping DXM in circulation far longer than usual [7,14]. Within weeks her depressive misery lifted—only to overshoot into a mild hypomanic state, a familiar hazard whenever NMDA antagonism "flips" cortical circuits too far toward excitation. Similar mood elevations are seen in 5–15 % of bipolar participants receiving ketamine or esketamine [15].
Why did such modest doses have so much punch? Chronic right-frontal damage is known to erode GABAergic brake systems, leaving limbic networks hypersensitive to any further disinhibition [3]. In that context, even low-level NMDA blockade can ignite the whole synaptogenic cascade—glutamate surge, AMPA throughput, BDNF/mTOR up-regulation—described in Cheung's oral ketamine-class hypothesis [7]. Ms A's own decision to trim DXM to 22.5 mg and the quick settling of her mood underscores how narrow the therapeutic window may be after frontal TBI.
One piece of Cheung's four-part concept was missing: supplemental L-glutamine. Because glutamine can both replenish presynaptic pools and temper excitotoxic swings, daily doses of 5–15 g might have softened the hypomanic rebound while preserving antidepressant speed [16]. Future trials should test that possibility, ideally with plasma DXM/dextrorphan ratios and serial mood scales to map dose-response more precisely.
Taken together, the case suggests that an inexpensive, entirely oral combination—DXM, a built-in CYP2D6 blocker, and an AMPA-facilitator—can deliver ketamine-like rapid relief in secondary bipolar depression. It also reminds us that structural brain vulnerability magnifies both benefit and risk; careful titration and close monitoring are essential whenever glutamatergic strategies follow a frontal TBI.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest and Source of Funding Statement
None declared.
Ethics Declaration
Not applicable.
References
- Orlovska, S.; Pedersen, M.S.; Benros, M.E.; et al. Head injury as risk factor for psychiatric disorders: a nationwide register-based follow-up study of 113,906 persons with head injury. Am J Psychiatry. 2014, 171, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.C.; Wu, H.L.; Chu, C.P.; et al. Traumatic brain injury and affective disorder: a nationwide cohort study in Taiwan, 2000–2010. J Affect Disord. 2016, 191, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Jorge, R.E.; Arciniegas, D.B. Mood disorders after TBI. Psychiatr Clin North Am. 2014, 37, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Drange, O.K.; Vaaler, A.E.; Morken, G.; et al. Clinical characteristics of patients with bipolar disorder and premorbid traumatic brain injury: a cross-sectional study. Int J Bipolar Disord. 2018, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Lee, B.; Liu, R.J.; et al. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science. 2010, 329, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Zanos, P.; Moaddel, R.; Morris, P.J.; et al. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Nature. 2016, 533, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N. DXM, CYP2D6-inhibiting antidepressants, piracetam, and glutamine: Proposing a ketamine-class antidepressant regimen with existing drugs. Preprints. 2025. [Google Scholar] [CrossRef]
- Cheung, N. Clinical experience and optimisation of the Cheung Glutamatergic Regimen for refractory psychiatric diseases. Preprints. 2025. [CrossRef]
- Cheung, N. An oral "ketamine-like" NMDA/AMPA modulation stack restores cognitive capacity in a young man with schizoaffective disorder—Case report. Preprints. 2025. [Google Scholar] [CrossRef]
- Cheung, N. Case series: Marked improvement in treatment-resistant obsessive–compulsive symptoms with over-the-counter glutamatergic augmentation in routine clinical practice. Preprints. 2025. [Google Scholar] [CrossRef]
- Cheung, N. Case report: Rapid remission of adolescent binge-eating disorder after over-the-counter glutamatergic augmentations to bupropion. Preprints. 2025. [Google Scholar] [CrossRef]
- Cheung, N. OTC glutamatergic augmentation resolves adolescent refractory somatic symptoms. Preprints. 2025. [Google Scholar] [CrossRef]
- Cheung, N. Oral glutamatergic augmentation for trauma-related disorders with fluoxetine- / bupropion- potentiated dextromethorphan ± piracetam: A four-patient case series. Preprints. 2025. [Google Scholar] [CrossRef]
- Preskorn, S.H.; Shah, R.; Neff, M.; et al. The potential for clinically significant drug-drug interactions involving the CYP 2D6 system: effects with fluoxetine and paroxetine versus sertraline. J Psychiatr Pract. 2007, 13, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Zarate CAJr Brutsche, N.E.; Ibrahim, L.; et al. Replication of ketamine's antidepressant efficacy in bipolar depression: a randomized controlled add-on trial. Biol Psychiatry. 2012, 71, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Son, H.; Baek, J.H.; Go, B.S.; et al. Glutamine has antidepressive effects through increments of glutamate and glutamine levels and glutamatergic activity in the medial prefrontal cortex. Neuropharmacology. 2018, 143, 143–152. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Case Presentation.
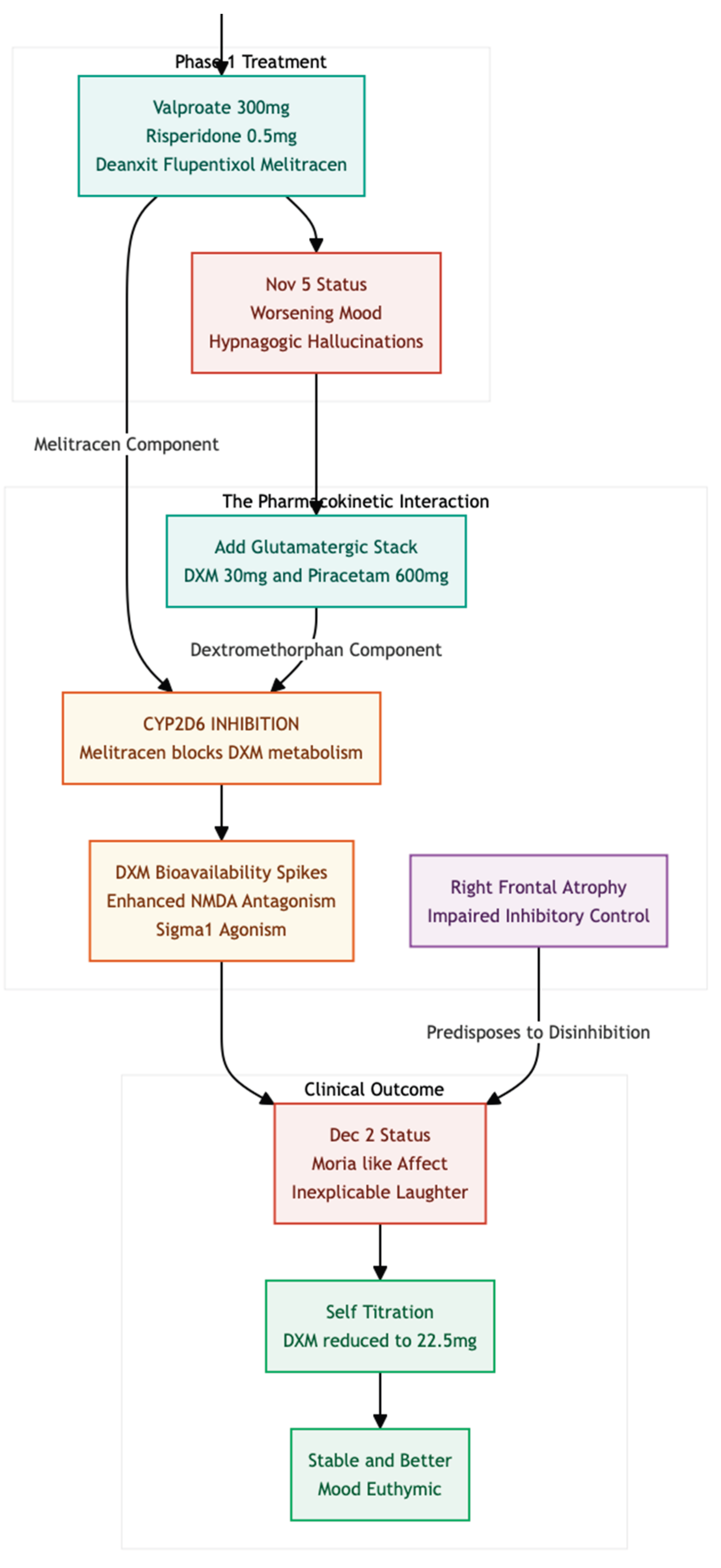
Figure 2.
Ms. A presents with an "Organic" Bipolar Profile consistent with secondary bipolarity following traumatic brain injury (TBI), where right frontal atrophy diminishes the brain’s GABAergic "brakes." This disinhibition results in a hypersensitive limbic system, manifesting as impulsivity and emotional lability that differ from idiopathic bipolar disorder. A Pharmacokinetic Twist occurred during treatment, inadvertently mimicking the mechanism of Auvelity®: Melitracen, a component of Deanxit, acts as a CYP2D6 inhibitor, impeding the metabolism of Dextromethorphan (DXM). This led to sustained DXM levels, triggering a strong glutamate surge and BDNF upregulation, which rapidly alleviated depression. However, The Missing Buffer—L-Glutamine—was notably absent. According to Cheung’s hypothesis, Glutamine replenishes presynaptic glutamate pools and acts as a buffer against excitotoxic spikes. Without this cushion, the unmitigated glutamate surge contributed to a hypomanic "overshoot," necessitating a reduction in the DXM dosage.
Figure 2.
Ms. A presents with an "Organic" Bipolar Profile consistent with secondary bipolarity following traumatic brain injury (TBI), where right frontal atrophy diminishes the brain’s GABAergic "brakes." This disinhibition results in a hypersensitive limbic system, manifesting as impulsivity and emotional lability that differ from idiopathic bipolar disorder. A Pharmacokinetic Twist occurred during treatment, inadvertently mimicking the mechanism of Auvelity®: Melitracen, a component of Deanxit, acts as a CYP2D6 inhibitor, impeding the metabolism of Dextromethorphan (DXM). This led to sustained DXM levels, triggering a strong glutamate surge and BDNF upregulation, which rapidly alleviated depression. However, The Missing Buffer—L-Glutamine—was notably absent. According to Cheung’s hypothesis, Glutamine replenishes presynaptic glutamate pools and acts as a buffer against excitotoxic spikes. Without this cushion, the unmitigated glutamate surge contributed to a hypomanic "overshoot," necessitating a reduction in the DXM dosage.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



