
Submitted:
02 December 2025
Posted:
03 December 2025
You are already at the latest version
Abstract
Respiratory syncytial virus (RSV) is a leading cause of lower respiratory tract infection in young children, especially during infancy, resulting in substantial morbidity and mortality. Acknowledging the real-world evidence on RSV immunisation, the College of Paediatrics, Academy Medicine of Malaysia has appointed an expert panel to develop a position paper on recommendations for infant and/or maternal vaccination against childhood RSV specifically in the Malaysian context with year-round RSV activity. Recognising the potential constraints and limitations in the implementation process, the expert panel recommends targeted immunisation with long-acting RSV monoclonal antibody (mAb) for high-risk infants as a pragmatic first step, with subsequent scale-up to universal immunisation of infants when resources permit. Year-round maternal vaccination between 28- and 36-weeks’ gestation combined with immunisation at six months for all infants may potentially circumvent the unclear seasonality.
Keywords:
RSV
; nirsevimab
; RSVpreF
; maternal vaccination
; long-acting RSV monoclonal antibody
; seasonality
; immunisation
1. Introduction
Respiratory syncytial virus (RSV) infection is a major contributor to morbidity and mortality among young children. Globally, in 2019, 33 million cases of RSV-associated lower respiratory tract infection (LRTI) episodes were reported in children aged 0 to 60 months, with an estimated 3·6 million RSV-associated LRTI hospital admissions [1]. RSV infection accounted for 2% of all deaths in children aged 0 to 60 months; specifically, RSV infection contributes to 19% of RSV-related deaths within the first 6 months of life [1]. Notably, children in low-income and middle-income countries made up over 95% of RSV-related acute LRTIs and 97% of RSV-related deaths [1]. In the absence of effective therapy for RSV, prevention with monoclonal antibodies (mAbs) immunisation given to infants and maternal RSV prefusion F (RSVpreF) vaccination are proven interventions that could reduce case-related morbidity and mortality.
The advancement and real-world evidence on immunisation for RSV prevention necessitates local experts’ evaluation to inform its potential implementation within the Malaysian healthcare system. This position paper, developed by an expert panel of 12 members appointed by the College of Paediatrics, Academy Medicine of Malaysia, aims to provide recommendations on infant immunisation with long-acting mAbs and maternal vaccination against RSV in Malaysia. The expert panel includes key opinion leaders in paediatric respiratory medicine, neonatology, paediatric infectious disease and immunology, microbiology, as well as public health and bioethics. The recommendations were informed by literature search using PubMed and grey literature; cost-effectiveness analyses were incorporated where available.
2. Epidemiology of RSV in Malaysia
2.1. RSV as a Major Respiratory Pathogen in Children
Several Malaysian studies have demonstrated that RSV was among the most prevalent respiratory pathogens detected using respiratory samples [2,3,4,5]. In a 27-year retrospective study (1982–2008) of hospitalised children below 5 years in Kuala Lumpur, 26·4% of respiratory samples were tested positive by immunofluorescence or viral culture, of which 70·6% were RSV [2]. More recent studies from Peninsular Malaysia report similar RSV positivity rates of 15·9% (2015–2019, 23,000 cases tested via multiplex polymerase chain reaction [PCR]) [3], 17·1% (2017–2022, 4,084 samples tested via direct fluorescent antibody [DFA]) [4], and 14·3% (2017–2024, 45,884 samples tested via DFA) [6]. Meanwhile, in East Malaysia, RSV-A and RSV-B were detected from 19% and 8% of 438 nasopharyngeal samples using real-time reverse PCR or real-time reverse-transcription PCR, respectively, at Sibu and Kapit Hospitals, Sarawak over 12 months [5].
2.2. Age-Group Vulnerability
Younger children are more vulnerable to RSV infections, evidenced by a median age of 8 to 12 months reported across Malaysian studies [4,7,8,9]. Children under 2 years old are at the highest risk of RSV-related hospitalisation, with approximately 85% of admissions recorded for this age group [3,9]. Most of these children were previously healthy, with more than 80% of hospitalised children with no documented comorbidities [8]. Although a recent local study reported no RSV-related mortality over 3 months [8], a case fatality rate of 1·6% among Malaysian children below age 5 was observed in another study conducted from 2008 to 2013 [9].
2.3. Lack of Immunity Against RSV Virus and Disease
A Malaysian study reported a resurgence of RSV cases post-COVID-19 period, which increased sharply with a positivity rate of 36·3% in July-August 2022 following a sharp decline during the pandemic (8·3% in July-August 2020), surpassing pre-pandemic levels (20·6% during 2017–2019) [4]. This phenomenon is primarily attributed to immunity debt incurred during the COVID-19 period, described as decreased population immunity following an extended period of reduced exposure to circulating pathogens [10]. This raises concern as delayed RSV exposure may predispose children to more severe illness later in childhood [11], likely driven by immunological factors including: (i) lack of early-life mucosal priming [12], (ii) diminished secretory IgA and innate immune pattern recognition [13], (iii) waning of maternal antibodies in mothers who were not recently exposed to RSV [14], and (iv) the immaturity of the infant adaptive immune system at the time of first infection [15].
2.4. Seasonality of RSV Across Asia
Temperate countries such as China and Japan generally show well-defined peaks in the winter months [16], while non-temperate countries like Hong Kong [17], Taiwan [18], and Singapore [19] tend to experience less predictable outbreaks with residual RSV activity throughout the year. In Peninsular Malaysia, more pronounced infections peaks are observed either during the third quarter [3,20], or the end of the year [2,9,20,21,22]. As for East Malaysia, an earlier infection peak was observed in Sibu and Kapit, Sarawak from March to August [5]. RSV infection was independently associated with the rainy season in Kelantan (OR 3·31, 95% CI 1·44–3·69) [22]. A weak correlation between RSV infections and rain days was seen in epidemiological studies conducted in Kuala Lumpur [2,20,21]. While RSV patterns appear to vary across Malaysia, robust surveillance is warranted to better understand local transmission trends and guide effective prevention strategies.
3. Disease Burden of RSV
3.1. Impact on Resource Utilisation
RSV in younger children places a substantial strain on healthcare services, increasing demand for hospital beds and intensive care capacity. An average monthly bed occupancy of 115% in the paediatric ward was recorded at the Kuala Lumpur Women's and Children's Hospital, with RSV admissions accounting for 2–22% of total admissions; meeting inpatient demand would require 82 additional beds, at an estimated cost of RM188·6 million (RM2·3 million per bed) [23]. In the same facility, children with RSV infections also required critical care more often than those with non-RSV infections (23·1% vs. 15·4%, respectively), with a significantly longer median length of stay (4 days [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] vs. 3 days [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]) [24]. Across two local studies, the need for paediatric intensive care unit (PICU) admission ranged between 15–15·3%, non-invasive ventilation between 10·2–11·2%, and mechanical ventilation between 2·5–6·9% [8,9]. High RSV case volumes in younger children can overwhelm hospital services and limit PICU capacity, resulting in suboptimal care.
3.2. Healthcare and Societal Costs of RSV Admissions
Severe RSV illness and hospitalisation result in substantial expenditures. The median direct cost of admissions for children below 5 years with acute respiratory infection at a teaching hospital in Kuala Lumpur was estimated to be USD 756 for a median hospital stay of 4 days [25]. Despite government subsidies, the median direct out-of-pocket cost remained at USD 189, translating to 16·4% of monthly household income [25]. Lost parental productivity also adds to indirect costs, with each hospital admission associated with a median of three lost workdays, bringing the median societal cost to USD 871 [25]. Likely an underestimate of the current actual costs, a local audit conducted three decades ago, involving children under 2 years old hospitalised for RSV infection between 1995 and 1997, reported a median admission cost of USD 358 for general inpatient care and USD 4,114 for PICU care, with a median length of stay of 4 days [26,27]. These demands are significant financial burdens that could potentially overwhelm the government budget allocated for healthcare and as such, preventive strategies should be considered to ease healthcare resources utilisation.
3.3. High Risk Populations for Severe RSV Disease
A disproportionate burden of RSV infection is seen among at-risk patient populations. Preterm infants under 37 weeks gestational age (GA) accounted for 25% of RSV-LRTI hospitalisations; among infants below 6 months, admission rates is almost four-fold for below 32 weeks GA (RR 3·87) and two-fold for 32 to 37 weeks’ GA (RR 1·93) compared to all children below 2 years [28]. Local hospital admission data on RSV report a substantial proportion who were extremely preterm infants (26 to 28 weeks’ GA), with nearly half (45%) required PICU admission at the Kuala Lumpur Women's and Children's Hospital [29]. Meanwhile, the FLIP-2 Spanish prospective study involving hospitalised premature infants (32 to 35 weeks’ GA) reported that 17·8% were admitted to ICU and 7·4% required mechanical ventilation [30].
Infant risk stratification for RSV hospitalisation is a subject of interest, especially from an economic perspective in resource-limited settings, as it helps prioritise prophylaxis for those at highest risk of severe disease. The risk factors for severe RSV infection leading to hospitalisation are outlined in Box 1.
Box 1. Risk factors for severe RSV infection leading to hospitalisation
Prior to the recommendation of universal immunisation against RSV for all infants, palivizumab prophylaxis for preterm infants below 35 weeks’ gestation was the primary preventive strategy in many countries [34]. In Malaysia, while the Paediatric Pharmacy Services Guideline advises administering palivizumab to infants with chronic lung disease or a history of prematurity (< 35 weeks’ GA) [35], the Universiti Kebangsaan Malaysia teaching hospital reserves palivizumab for preterm neonates < 29 weeks’ GA, weighing 1,000 g and below, and/or diagnosed with bronchopulmonary dysplasia [36]. Although some settings secured budget allocation for infants at the highest risk of RSV disease [36], most Malaysian public hospitals administer palivizumab on an ad hoc basis without specific funding, reflecting the absence of a coordinated national policy.
3.4. Long-Term Clinical Sequelae Following RSV Infection
In children, clinical manifestations of RSV infection can range from mild respiratory symptoms to severe illness with acute and long-term consequences. That said, non-medically attended mild RSV infections can also have persistent symptoms beyond 15 days in half (50·5%) of healthy, term infants in the form of rhinitis (99%), cough (96·9%), and wheezing (66%) [37]. This can result in substantial social burden among parents, seen as impairment in usual daily activities (in 59·8% of episodes), worries (75·3%), anxiety (34%), and work absenteeism (10·8%) [37]. In more serious cases, infants who experience RSV bronchiolitis within their first 6 months of life have around 30% higher odds of developing pneumonia and otitis media, as well as requiring antibiotics in the following 6 months [38]. Early-life RSV LRTI can have long-term respiratory sequelae, including recurrent wheezing [39], asthma [40], abnormal lung function [41], and post-infection bronchiolitis obliterans [42]. Overall, RSV infections can result in substantial morbidity, often requiring medical attention in the long-term.
4. The Virus, Mechanism of Disease and Immune Defences
RSV (Figure 1a) is a single-stranded RNA virus that belongs to the Orthopneumovirus genus of the Pneumoviridae family, with two major subtypes—RSV A and RSV B [43]. Upon inhalation, RSV first infects the airway epithelial cells in the upper respiratory tract, then spreads to the bronchioles in the lower respiratory tract, where viral replication becomes more effective [44]. For viral entry into the host cells, the attachment glycoprotein (G) binds to the cell surface, while the fusion glycoprotein (F) facilitates membrane fusion [43]. RSV F protein then inhibits interferon-λ production, leading to continuous viral infection that becomes amplified [45]. This is accompanied by airway damage largely driven by immune-mediated response [45]. If confined to the upper airways, RSV infection typically presents with symptoms of an upper respiratory infection; however, in previously unexposed infants, the virus often spreads to the lower respiratory tract, causing LRTI [44].
Younger children are more vulnerable to severe illnesses from airway obstruction due to their smaller airways, reduced respiratory capacity, and lower respiratory reserve [44]. Additionally, protection against RSV infection in infants relies on maternal antibody levels, which wane rapidly after birth and are mostly absent at 6 months old [46]. These children are also susceptible to RSV reinfections, demonstrating primary infection rate of 86% and reinfection rate of around 35% in their first 3 years of life [46]. RSV reinfections could be attributed to short-lived primary RSV infection-induced antibody response, compounded by the immune system’s limited ability to develop efficient protective immunity against the virus, a rapid decline of antibody levels, and antigenic variations of RSV strains in subsequent epidemic seasons [46].
Efforts to develop active immunisation against RSV in infants have so far been unsuccessful, with progress remaining slow [47]. This is largely due to concerns about formalin-inactivated vaccine causing enhanced respiratory disease and the limited suitability of live attenuated vaccines in immunologically immature infants [48]. Interference from maternal antibodies in the first 6 months may also neutralise vaccine antigens before eliciting a strong immune response in infants [47]. Nonetheless, ongoing trials, mostly involving live attenuated vaccines administered intranasally, offer hope for safe and effective infant RSV immunisation [47].
At present, protection against severe RSV infection in children relies on passive immunisation, using mAbs and maternal RSV vaccines that target different antigenic sites of the RSV prefusion and postfusion proteins (Figure 1b) [47]. The RSV F glycoprotein is highly conserved and refolds from a metastable prefusion form to a stable postfusion form during viral entry, therefore an ideal candidate for passive prophylaxis development [49]. Palivizumab is an mAb that targets site II of the RSV F protein to neutralise the virus [50]; nirsevimab binds to site Ø, blocking the conformational change required for viral entry into host cells [50]; clesrovimab targets site IV of the F protein [51]. Meanwhile, the maternal vaccine is a bivalent subunit formulation containing prefusion antigens derived from RSV A and RSV B [52].
5. Current RSV Immunisation Approaches
5.1. Passive Immunisation
In June 1998, palivizumab became the first mAb approved by the US FDA for the prevention of RSV in high-risk children [53]. Infants who meet the criteria for prophylaxis may receive up to five monthly doses of palivizumab during their first RSV season, and at the start of their second season if indicated [54]. This schedule is based on its half-life of 20 days [55], which confers an estimated protection period of 28 days per dose [56]. A 2021 Cochrane review determined that palivizumab prophylaxis significantly reduces RSV-related hospitalisation in high-risk children (RR 0·44, 95% CI 0·3–0·64) [57]. Nonetheless, its short duration of action, the need for repeated monthly doses, and its high cost, support the recommendation for targeted immunisation of high-risk infants to reduce severe disease in a cost-effective manner [58].
Nirsevimab, the first long-acting mAb, was introduced in July 2023 to prevent RSV-associated LRTI in infants during their first RSV season and in high-risk children up to 24 months during their second RSV season [59,60]. With a half-life of 71 days, nirsevimab provides almost immediate protection after a single dose, which lasts for at least 5 months [55]. Its efficacy has been established in multiple pivotal trials (Table 1) [61,62,63,64,65], with a meta-analysis of 45,238 infants reporting a pooled efficacy of 88·4% (95% CI 84·7–91·2) against RSV-related hospitalisation [66]. The MEDLEY trial found that nirsevimab has a safety profile comparable to palivizumab [67]; there is also some evidence that the RSV protection could linger for a bit longer, with post-hoc analysis reporting nearly ten-fold higher and more sustained RSV-neutralising antibody levels up to 1 year [55].
The availability of nirsevimab has marked a paradigm shift in RSV prevention from targeted immunisation of high-risk infants to universal immunisation of all infants [68]. The NIRSE-GAL study in Galicia, Spain achieved 92% coverage, demonstrating 70·7% (95% CI 42·4–85·1) effectiveness against RSV-related LRTI hospitalisation and 80·3% (54·6–91·5) effectiveness in preventing RSV-related LRTI hospitalisation requiring oxygen support during the 2023-2024 season, with no new safety signals identified [69]. Similarly, Chile’s NIRSE-CL study achieved a coverage of 94% nationwide, resulting in effectiveness of 76·4% (72·6–79·7) against RSV-related LRTI hospitalisation and 84·9% (79·5–88·9) against ICU admissions [70]. Meanwhile, the REVIVE study conducted in Western Australia reported an adjusted effectiveness of 88·2% (73·5–94·7) against RSV-associated acute respiratory infection hospitalisations over 7 months [71]. The consistent effectiveness observed across real-world studies highlights the public health value of universal infant immunisation with nirsevimab.
A new mAb, clesrovimab, has recently received approval in June 2025 for prevention of RSV LRTI in infants born during or entering their first RSV season [72]. Despite clesrovimab having a shorter half-life than nirsevimab (44 days vs. 71 days), durable protection was observed across the typical five-month RSV season [73,74]. In the phase 2b/3 CLEVER trial (MK-1654-004), clesrovimab reduced RSV LRTIs at 150 days post-dose in healthy pre-term and full-term infants at birth to 1 year (efficacy 60·4%, 95% CI 44·1–71·9); even greater efficacy was observed in preventing LRTI hospitalisations (84·2%, 66·6–92·6) [73,75]. Additionally, the phase 3 SMART trial (MK-1654-007) found that clesrovimab is well tolerated in infants at high risk for RSV disease, with similar safety profile and RSV disease incidence rates comparable to monthly palivizumab through 150 days [74].
5.2. Maternal Vaccination
The RSVpreF vaccine is indicated for active immunisation of pregnant women to prevent RSV-associated LRTI in infants under 6 months old [76,77,78]. Although the European Medicines Agency approved its use for 24 to 36 weeks’ gestational period as per the MATISSE trial [52,78], slightly higher rates of preterm birth among RSVpreF recipients, though not statistically significant, perhaps led the US FDA to limit its use to 32 to 36 weeks’ gestation period in view of this potential risk [79,80]. Geographical variation was evident, with the vaccinated groups reporting a higher relative risk of preterm birth in Argentina and South Africa (significant in South Africa) [81]. A single RSVpreF dose between 32 and 36 weeks’ gestation period was also implemented in Canada and Argentina [82,83], while the UK and Australia recommend administration from 28 to 36 weeks [84,85].
Real-world data from Argentina’s BERNI study showed that maternal RSVpreF vaccination was effective against RSV-related LRTI hospitalisation from birth to 3 months (78·6%, 95% CI 62·1–87·9), with protection sustained up to 6 months (71·3%, 53·3–82·3) [83]. A modelling study in Australia suggests that achieving 70% year-round coverage of maternal RSVpreF vaccination could reduce infant hospitalisation under 3 months by 60% [86]. In Malaysia, the 2024 Malaysian Maternal Immunisation Consensus Guidelines positions RSVpreF as a highly efficacious vaccine and recommends its administration between 32 and 36 weeks gestation period [87].
5.3. Passive Immunisation vs. Maternal Vaccination
Both infant mAb immunisation and maternal RSVpreF vaccination offers distinct benefits and limitations, though no direct comparative data currently exist on their effectiveness in preventing RSV-associated LRTI in infants. Dosage and administration of infant mAb and maternal RSVpreF are outlined in File S1. Immunisation with mAb provides protective antibodies directly to the infant, unaffected by the variability in maternal response and transplacental transfer [79].
While maternal vaccination may offer immediate protection at birth and could be less susceptible to F protein mutations, its effectiveness might be compromised if antibody production or placental transfer is suboptimal, especially in immunocompromised mothers or if the infant is born prematurely within 14 days of vaccination [79]. RSVpreF induces robust immune responses in pregnant women, resulting in high RSV-neutralising titres in their newborns [88]. However, there is currently insufficient evidence on how sustained the antibodies in subsequent pregnancies are and whether they protect the pregnant women themselves against RSV infections.
6. Cost-Effectiveness of RSV Immunisation Approaches
Evaluating the cost-effectiveness of RSV prevention strategies in both targeted and universal approaches is essential to inform policymaking and optimise implementation. Table 2 outlines cost-effectiveness analyses of RSV prevention strategies conducted across countries.
6.1. Cost-Effectiveness for RSV Prevention in Malaysia
To support the expert panel’s deliberation, the study group performed a focused cost-effectiveness analysis of RSV prevention strategies in the Malaysian healthcare context. A decision tree model was used to account for direct and indirect medical costs related to RSV hospitalisation and mortality.
Findings from the cost-effectiveness analysis indicates that nirsevimab immunisation in high-risk infants prior to hospital discharge is the most affordable and costs substantially less than palivizumab, at almost one-tenth of its price. Nirsevimab alone or in combination with maternal vaccination is cost-effective compared to palivizumab; dominant strategies that are more cost-effective than palivizumab include i) nirsevimab for high-risk infants, ii) maternal vaccination with complementary nirsevimab for infants unprotected by maternal vaccination, and iii) maternal vaccination with complementary nirsevimab plus extended nirsevimab dosing for high-risk infants at 6 and 12 months. Nirsevimab for high-risk infants achieved the highest spending-to-savings ratio at 1:1·62, followed by maternal vaccination with complementary nirsevimab plus extended nirsevimab dosing for high-risk infants at 1:1·28. Further details of the cost-effectiveness analysis are outlined in File S2.
7. Ethics, Equity and Feasibility of RSV Immunisation
Historically, palivizumab has been reserved for high-risk infants due to cost issues, thereby excluding those at moderate risk and perpetuating preventable inequities in protection. The advent of new long-acting mAbs and maternal RSV vaccines now marks a critical ethical inflection point [95]. The true ethical imperative is not merely offering cheaper protection, but the systemic commitment to a universal access model, thereby dismantling the inequitable risk-stratification paradigm entirely. Policy discussions must pivot from cost-containment relative to the “palivizumab era” to assessing the absolute programme affordability required for universal deployment, acknowledging that even reduced per-course costs translate into significant, politically challenging budgetary demands on national health systems.
The concurrent emergence of maternal and infant immunisation strategies also raises uncertainties to which is the ethically preferable option beyond cost—should protection be delivered directly to infants via long-acting mAbs or indirectly via maternal immunisation? Long-acting mAbs may add to an already crowded paediatric vaccination schedule, potentially affecting adherence and raising concerns about pain, distress, and trust in healthcare services. Conversely, maternal vaccination avoids invasive procedures for the child but shifts the decision to the pregnant individual, invoking considerations of her own pain and distress, alongside parental responsibility and individual autonomy.
While existing national cold chain infrastructure is cited as supportive, potential limitations in system capacity and distribution topology can hinder the implementation of RSV prevention strategies. Maternal vaccination necessitates expanding cold chain access into antenatal clinics, while infant mAb delivery demands sufficient storage and seamless integration into community paediatric clinics. The challenge of achieving supply chain resilience extends particularly to last-mile delivery and comprehensive product tracking, which must bridge the infrastructural and administrative gaps between state-managed systems (e.g., National Immunisation Programme) and the often-decentralised private healthcare market, a divide common across diverse healthcare settings in countries with year-round RSV activity.
Healthcare workers should also be adequately trained, not only in clinical areas such as efficacy, contraindications, and adverse events, but also in operational competencies, including workflow integration and patient counselling. Additionally, parental acceptance remains crucial; as hesitancy is rarely resolved by simple “education”, public engagement must move beyond basic information, proactively addressing the unique scepticism surrounding a novel biologic through transparent dialogue and acknowledging the socio-political and experiential roots of distrust. Clinical efficacy must be actively validated and matched by deliberate, strategic efforts to build and maintain robust public trust.
8. Final Considerations and Position Statements
RSV prevention strategies should consider feasibility, administrative capacity, and budget constraints (Figure 2). With these considerations in mind, the expert panel advises targeted immunisation with long-acting mAbs for high-risk infants prior to hospital discharge as the pragmatic first step in the implementation of a national childhood RSV protection programme; immunisation may be repeated during the second year of life for eligible at-risk infants.
Complementary nirsevimab refers to nirsevimab given to infants: i) when the mother was not administered RSV vaccine during pregnancy, ii) when maternal vaccination status is unknown, or iii) when the infant is born less than 14 days after maternal vaccination.
Subsequent scale up of the programme to universal administration to protect all infants warrants serious consideration when resources permit. This can be achieved either through maternal vaccination with complementary long-acting mAbs or universal use of long-acting mAbs for all infants. As maternal vaccination is substantially less costly than long-acting mAbs, it may be worthwhile to explore the implementation of maternal vaccination for all mothers, especially in resource-limited settings.
Although real-world evidence showed effectiveness of long-acting mAbs for RSV prophylaxis as a seasonal strategy [69,70], the absence of clear seasonality in Malaysia, however, is a key limitation that complicates the optimisation of immunisation schedule for maximum protection. Therefore, the expert panel recommends addressing the issue of unclear seasonality with a combined strategy of maternal vaccination to protect infants from birth through 6 months, followed by universal infant immunisation with long-acting mAbs at 6 months to provide seamless protection across the first year of life. This strategy avoids potential interference that may occur with coadministration of other childhood vaccinations given at birth. Taken together, this addresses the high burden of disease in early infancy and the continued RSV circulation observed year-round (with peak incidence between 8 and 12 months of age) in a country with unclear RSV seasonality.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, FCC; Data curation, MRAM; Formal analysis, MRAM; Funding acquisition, FCC; Resources, FCC, EJK, AA, ZI, RAA, DCEN, PWKC, AAK, XYC, JICS, and AK; Supervision, FCC; Validation, FCC, EJK, AA, ZI, RAA, DCEN, PWKC, AAK, XYC, JICS, and AK; Writing – review & editing, FCC, EJK, AA, ZI, RAA, DCEN, PWKC, AAK, XYC, JICS, MRAM and AK.
Data Availability Statement
The authors confirm that the data supporting the finding of the cost-effectiveness analysis are available within File S2. Additional raw data that support the findings of this report are available from the corresponding author, upon reasonable request.
Acknowledgments
Medical writing support was provided by Jia Yin Lee, MPH, of Mediconnexions Consulting Sdn. Bhd., funded by the College of Paediatrics, Academy of Medicine of Malaysia. The authors would like to thank Dr David Chun-Ern Ng and Dr Asiah Kassim for providing unpublished data as clinical indicators and rationale to support the recommendations for RSV prophylaxis in Malaysia.
Conflicts of Interest
FCC has received payment for lectures from Sanofi and AstraZeneca, travel support for meeting attendance from Sanofi, and participation in advisory board from Sanofi and AstraZeneca. EJK is a Director for Baby and Beyond Child Specialist Clinic, Malaysia; some of EJK’s work was also supported by the FDA Scientific Conference Grant and the Institute of Medical Ethics Travel Grant, although EJK did not receive any payment for these contributions. AA has received consulting fees from AstraZeneca, as well as honoraria for lectures from AstraZeneca and MSD and participation in advisory board from MSD. ZI has received honorarium for lecture from Sanofi; ZI is also the Chairman of Immunise4Life Initiative and Positive Parenting Management Committee, as well as the past president of the Malaysian Paediatric Association. RAA has received honorarium for lecture from Sanofi. DCEN has received honoraria for lectures from Sanofi and Pfizer. AAK has received honorarium for lecture from Sanofi. XYC has received honorarium for lecture from AstraZeneca. JICS received research grant channelled to institution’s research unit from Sanofi. PWKC, MRAM, and AK declare no conflict of interests.
References
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Khor, C.S.; Sam, I.C.; Hooi, P.S.; Quek, K.F.; Chan, Y.F. Epidemiology and seasonality of respiratory viral infections in hospitalized children in Kuala Lumpur, Malaysia: a retrospective study of 27 years. BMC Pediatr 2012, 12, 32. [Google Scholar] [CrossRef]
- Low, Y.L.; Wong, S.Y.; Lee, E.K.H.; Muhammed, M.H. Prevalence of respiratory viruses among paediatric patients in acute respiratory illnesses in Malaysia. PLoS One 2022, 17, e0265288. [Google Scholar] [CrossRef]
- Chan, C.M.; Wahab, A.A.; Ali, A. Assessing the impact of COVID-19 on epidemiological changes of severe pediatric respiratory syncytial virus infections in Malaysia. Front Public Health 2024, 12, 1246921. [Google Scholar] [CrossRef]
- Toh, T.H.; Hii, K.C.; Fieldhouse, J.K.; Ting, J.; Berita, A.; Nguyen, T.T.; Wong, S.C.; Wong, T.M.; Lim, W.H.; Ha, S.J.; et al. High prevalence of viral infections among hospitalized pneumonia patients in equatorial Sarawak, Malaysia. Open Forum Infect Dis 2019, 6, ofz074. [Google Scholar] [CrossRef]
- Ng, D.C. Data from Hospital Tuanku Ja’afar, Seremban on RSV detection rate from hospitalised cases (unpublished work). 2025. [Google Scholar]
- Nathan, A.M.; Rani, F.; Lee, R.J.; Zaki, R.; Westerhout, C.; Sam, I.C.; Lum, L.C.; de Bruyne, J. Clinical risk factors for life-threatening lower respiratory tract infections in children: a retrospective study in an urban city in Malaysia. PLoS One 2014, 9, e111162. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.C.; Liew, C.H.; Tan, K.K.; Awang, E.H.B.; Nazri, F.; Maran, A.K.T.; Mohan, V.; Ramachandran, D.; Chok, M.; Teh, C.H.; et al. Clinical comparison of HMPV and RSV infections in hospitalised Malaysian children: A propensity score matched study. Clin Respir J 2024, 18, e13747. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.F.; Tan, K.K.; Sam, Z.H.; Ting, G.S.; Gan, W.Y. Epidemiology, clinical characteristics, laboratory findings and severity of respiratory syncytial virus acute lower respiratory infection in Malaysian children, 2008-2013. J Paediatr Child Health 2017, 53, 399–407. [Google Scholar] [CrossRef]
- Hatter, L.; Eathorne, A.; Hills, T.; Bruce, P.; Beasley, R. Respiratory syncytial virus: paying the immunity debt with interest. Lancet Child Adolesc Health 2021, 5, e44–e45. [Google Scholar] [CrossRef] [PubMed]
- Winthrop, Z.A.; Perez, J.M.; Staffa, S.J.; McManus, M.L.; Duvall, M.G. Pediatric respiratory syncytial virus hospitalizations and respiratory support after the COVID-19 pandemic. JAMA Netw Open 2024, 7, e2416852. [Google Scholar] [CrossRef]
- Ruckwardt, T.J.; Morabito, K.M.; Graham, B.S. Determinants of early life immune responses to RSV infection. Curr Opin Virol 2016, 16, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Attaianese, F.; Guiducci, S.; Trapani, S.; Barbati, F.; Lodi, L.; Indolfi, G.; Azzari, C.; Ricci, S. Reshaping our knowledge: advancements in understanding the immune response to human respiratory syncytial virus. Pathogens 2023, 12, 1118. [Google Scholar] [CrossRef]
- Abu-Raya, B.; Viñeta Paramo, M.; Reicherz, F.; Lavoie, P.M. Why has the epidemiology of RSV changed during the COVID-19 pandemic? EClinicalMedicine 2023, 61, 102089. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.V.C.; Openshaw, P.J.M.; Thwaites, R.S. Mucosal immune responses to respiratory syncytial virus. Cells 2022, 11. [Google Scholar] [CrossRef]
- Ponce, L.J.; Wu, T.; Sim, D.J.; Chow, J.Y.; Wee, L.E.; Chia, P.Y.; Lye, D.C.B.; Leo, Y.S.; Lim, J.T. Respiratory syncytial virus hospitalization costs, rates, and seasonality in Asia: a systematic review and meta-analysis. EClinicalMedicine 2025, 86, 103350. [Google Scholar] [CrossRef]
- Chan, P.K.; Sung, R.Y.; Fung, K.S.; Hui, M.; Chik, K.W.; Adeyemi-Doro, F.A.; Cheng, A.F. Epidemiology of respiratory syncytial virus infection among paediatric patients in Hong Kong: seasonality and disease impact. Epidemiol Infect 1999, 123, 257–262. [Google Scholar] [CrossRef]
- Lee, P.-I.; Liu, C.-C.; Hu, Y.-L.; Chen, J.-M. Seasonality and risk factor analysis of respiratory syncytial virus infection in children in Taiwan—a retrospective study from 1995 to 2005. J Med Virol 2023, 95, e29116. [Google Scholar] [CrossRef]
- Tan, K.W.J.; Yung, C.F.; Maiwald, M.; Saffari, S.E.; Thoon, K.C.; Chong, C.Y. Respiratory viral infections in hospitalised paediatric patients in the tropics. J Paediatr Child Health 2021, 57, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.M.; Wahab, A.A.; Ali, A. Determining the relationship of meteorological factors and severe pediatric respiratory syncytial virus (RSV) infection in Central Peninsular Malaysia. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef]
- Chan, P.W.; Chew, F.T.; Tan, T.N.; Chua, K.B.; Hooi, P.S. Seasonal variation in respiratory syncytial virus chest infection in the tropics. Pediatr Pulmonol 2002, 34, 47–51. [Google Scholar] [CrossRef]
- Teck, K.S.; Mac Guad, R.; Van Rostenberghe, A.H.; Hua, G.S. Prevalence, risk factors and clinical characteristics of respiratory syncytial virus-associated lower respiratory tract infections in Kelantan, Malaysia. J Med Virol 2019, 91, 1608–1615. [Google Scholar] [CrossRef] [PubMed]
- Kassim, A. Bed occupancy rate and RSV admissions at the Kuala Lumpur Women's and Children's Hospital (unpublished work). 2025. [Google Scholar]
- Kassim, A. Clinical characteristics and outcomes among children under 5 years old admitted for respiratory syncytial virus (RSV) compared to other common respiratory virus infections (unpublished work). 2025. [Google Scholar]
- Sam, I.C.; Ahmad Jaafar, N.; Wong, L.P.; Nathan, A.M.; de Bruyne, J.A.; Chan, Y.F. Socioeconomic costs of children <5 years hospitalised with acute respiratory infections in Kuala Lumpur, Malaysia. Vaccine 2021, 39, 2983–2988. [Google Scholar] [CrossRef]
- Chan, P.W.; Abdel-Latif, M.E. Cost of hospitalization for respiratory syncytial virus chest infection and implications for passive immunization strategies in a developing nation. Acta Paediatr 2003, 92, 481–485. [Google Scholar] [CrossRef]
- Wittenauer, R.; Pecenka, C.; Baral, R. Cost of childhood RSV management and cost-effectiveness of RSV interventions: a systematic review from a low- and middle-income country perspective. BMC Med 2023, 21, 121. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; Shi, T.; Bont, L.J.; Chu, H.Y.; Zar, H.J.; Wahi-Singh, B.; Ma, Y.; Cong, B.; Sharland, E.; et al. Global disease burden of and risk factors for acute lower respiratory infections caused by respiratory syncytial virus in preterm infants and young children in 2019: a systematic review and meta-analysis of aggregated and individual participant data. Lancet 2024, 403, 1241–1253. [Google Scholar] [CrossRef]
- Kassim, A. RSV admission versus total respiratory admission by gestational age (unpublished work). 2025. [Google Scholar]
- Figueras-Aloy, J.; Carbonell-Estrany, X.; Quero-Jiménez, J.; Fernández-Colomer, B.; Guzmán-Cabañas, J.; Echaniz-Urcelay, I.; Doménech-Martínez, E. FLIP-2 Study: risk factors linked to respiratory syncytial virus infection requiring hospitalization in premature infants born in Spain at a gestational age of 32 to 35 weeks. Pediatr Infect Dis J 2008, 27, 788–793. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Committee on Infectious Diseases, A.A.o.P.B.G.C. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics 2014, 134, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. RSV immunisation guidance for infants and young children. Available online: https://www.cdc.gov/rsv/hcp/vaccine-clinical-guidance/infants-young-children.html (accessed on 15 May 2025).
- Doering, G.; Gusenleitner, W.; Belohradsky, B.H.; Burdach, S.; Resch, B.; Liese, J.G. The risk of respiratory syncytial virus-related hospitalizations in preterm infants of 29 to 35 weeks' gestational age. Pediatr Infect Dis J 2006, 25, 1188–1190. [Google Scholar] [CrossRef]
- Carbonell-Estrany, X.; Simões, E.A.F.; Bont, L.; Manzoni, P.; Zar, H.J.; Greenough, A.; Ramilo, O.; Stein, R.; Law, B.; Mejias, A.; et al. Twenty-five years of palivizumab: a global historic review of its impact on the burden of respiratory syncytial virus disease in children. Expert Rev Anti Infect Ther 2025, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Malaysia. Paediatric Pharmacy Services Guidelines. Available online: https://pharmacy.moh.gov.my/sites/default/files/document-upload/paediatric-pharmacy-services-guideline.pdf (accessed on 3 October 2025).
- Kua, K.P.; Qureshi, N.; Kon Ken, W.; Bin, D.; Wu, D.B.C.; Lee, S.; Cheah, C. Impact of palivizumab immunization in controlling respiratory syncytial virus infections among preterm neonates after hospital discharge in the tropics. Perinatology 2019, 20, 1–9. [Google Scholar]
- Hak, S.F.; Venekamp, R.P.; Billard, M.N.; van Houten, M.A.; Pollard, A.J.; Heikkinen, T.; Cunningham, S.; Millar, M.; Martinón-Torres, F.; Dacosta-Urbieta, A.; et al. Substantial burden of nonmedically attended RSV infection in healthy-term infants: an international prospective birth cohort study. J Infect Dis 2024, 229, S40–s50. [Google Scholar] [CrossRef] [PubMed]
- Abreo, A.; Wu, P.; Donovan, B.M.; Ding, T.; Gebretsadik, T.; Huang, X.; Stone, C.A.; Turi, K.N.; Hartert, T.V. Infant respiratory syncytial virus bronchiolitis and subsequent risk of pneumonia, otitis media, and antibiotic utilization. Clin Infect Dis 2020, 71, 211–214. [Google Scholar] [CrossRef]
- McCready, C.; Haider, S.; Little, F.; Nicol, M.P.; Workman, L.; Gray, D.M.; Granell, R.; Stein, D.J.; Custovic, A.; Zar, H.J. Early childhood wheezing phenotypes and determinants in a South African birth cohort: longitudinal analysis of the Drakenstein Child Health Study. Lancet Child Adolesc Health 2023, 7, 127–135. [Google Scholar] [CrossRef]
- Zar, H.J.; Cacho, F.; Kootbodien, T.; Mejias, A.; Ortiz, J.R.; Stein, R.T.; Hartert, T.V. Early-life respiratory syncytial virus disease and long-term respiratory health. Lancet Respir Med 2024, 12, 810–821. [Google Scholar] [CrossRef]
- Korppi, M.; Piippo-Savolainen, E.; Korhonen, K.; Remes, S. Respiratory morbidity 20 years after RSV infection in infancy. Pediatr Pulmonol 2004, 38, 155–160. [Google Scholar] [CrossRef]
- Lui, C.S.; Che Daud, C.Z.; Mohammad, N.F.A.; Kamal, M.; Musa, A.; Sharibudin, N.K.; Zainuddin, H.; Mohd Hairi, F.; Gan, E.A.; Kailasam, P.D.; et al. Outcome of post-infectious bronchiolitis obliterans (PIBO) among children in Malaysia. Eur Respir J 2022, 60, 1561. [Google Scholar] [CrossRef]
- Gatt, D.; Martin, I.; AlFouzan, R.; Moraes, T.J. Prevention and treatment strategies for respiratory syncytial virus (RSV). Pathogens 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Kaler, J.; Hussain, A.; Patel, K.; Hernandez, T.; Ray, S. Respiratory syncytial virus: a comprehensive review of transmission, pathophysiology, and manifestation. Cureus 2023, 15, e36342. [Google Scholar] [CrossRef]
- Shang, Z.; Tan, S.; Ma, D. Respiratory syncytial virus: from pathogenesis to potential therapeutic strategies. Int J Biol Sci 2021, 17, 4073–4091. [Google Scholar] [CrossRef] [PubMed]
- Kutsaya, A.; Teros-Jaakkola, T.; Kakkola, L.; Toivonen, L.; Peltola, V.; Waris, M.; Julkunen, I. Prospective clinical and serological follow-up in early childhood reveals a high rate of subclinical RSV infection and a relatively high reinfection rate within the first 3 years of life. Epidemiol Infect 2016, 144, 1622–1633. [Google Scholar] [CrossRef]
- Babawale, P.I.; Martínez-Espinoza, I.; Mitchell, A.M.; Guerrero-Plata, A. Preventing RSV infection in children: current passive immunizations and vaccine development. Pathogens 2025, 14, 104. [Google Scholar] [CrossRef]
- Mejias, A.; Ramilo, O. RSV prevention within reach for older infants and toddlers: the role of active immunization. J Pediatric Infect Dis Soc 2024, 13, S125–s130. [Google Scholar] [CrossRef] [PubMed]
- McLellan, J.S.; Ray, W.C.; Peeples, M.E. Structure and function of respiratory syncytial virus surface glycoproteins. Curr Top Microbiol Immunol 2013, 372, 83–104. [Google Scholar] [CrossRef]
- Duan, Y.; Liu, Z.; Zang, N.; Cong, B.; Shi, Y.; Xu, L.; Jiang, M.; Wang, P.; Zou, J.; Zhang, H.; et al. Landscape of respiratory syncytial virus. Chin Med J (Engl) 2024, 137, 2953–2978. [Google Scholar] [CrossRef]
- Madhi, S.A.; Simões, E.A.F.; Acevedo, A.; Novoa Pizarro, J.M.; Shepard, J.S.; Railkar, R.A.; Cao, X.; Maas, B.M.; Zang, X.; Krick, A.; et al. A phase 1b/2a trial of a half-life extended respiratory syncytial virus neutralizing antibody, clesrovimab, in healthy preterm and full-term infants. J Infect Dis 2025, 231, e478–e487. [Google Scholar] [CrossRef]
- Kampmann, B.; Madhi, S.A.; Munjal, I.; Simões, E.A.F.; Pahud, B.A.; Llapur, C.; Baker, J.; Pérez Marc, G.; Radley, D.; Shittu, E.; et al. Bivalent prefusion F vaccine in pregnancy to prevent RSV illness in infants. N Engl J Med 2023, 388, 1451–1464. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Palivizumab product approval information - licensing action. Available online: https://web.archive.org/web/20160723194308/https:/www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/ucm093366.htm (accessed on 15 May 2025).
- US Food and Drug Administration. Synagis prescribing information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/103770s5200lbl.pdf (accessed on 15 May 2025).
- Wilkins, D.; Wählby Hamrén, U.; Chang, Y.; Clegg, L.E.; Domachowske, J.; Englund, J.A.; Muller, W.J.; Leach, A.; Kelly, E.J.; Villafana, T. RSV neutralizing antibodies following nirsevimab and palivizumab dosing. Pediatrics 2024, 154. [Google Scholar] [CrossRef]
- Gilca, R.; Billard, M.N.; Zafack, J.; Papenburg, J.; Boucher, F.D.; Charest, H.; Rochette, M.; De Serres, G. Effectiveness of palivizumab immunoprophylaxis to prevent respiratory syncytial virus hospitalizations in healthy full-term <6-month-old infants from the circumpolar region of Nunavik, Quebec, Canada. Prev Med Rep 2020, 20, 101180. [Google Scholar] [CrossRef]
- Garegnani, L.; Styrmisdóttir, L.; Roson Rodriguez, P.; Escobar Liquitay, C.M.; Esteban, I.; Franco, J.V. Palivizumab for preventing severe respiratory syncytial virus (RSV) infection in children. Cochrane Database Syst Rev 2021, 11, Cd013757. [Google Scholar] [CrossRef] [PubMed]
- Vittucci, A.C.; Antilici, L.; Dotta, A.; Cutrera, R.; Villani, A. Respiratory syncytial virus infection: new prevention strategies. Global Pediatrics 2024, 7, 100130. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Beyfortus prescribing information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761328s000lbl.pdf (accessed on 15 May 2025).
- US Food and Drug Administration. Beyfortus biologics license application approval. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2023/761328Orig1s000ltr.pdf (accessed on 15 May 2025).
- Griffin, M.P.; Yuan, Y.; Takas, T.; Domachowske Joseph, B.; Madhi Shabir, A.; Manzoni, P.; Simões Eric, A.F.; Esser Mark, T.; Khan Anis, A.; Dubovsky, F.; et al. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med 2020, 383, 415–425. [Google Scholar] [CrossRef]
- Hammitt Laura, L.; Dagan, R.; Yuan, Y.; Baca Cots, M.; Bosheva, M.; Madhi Shabir, A.; Muller William, J.; Zar Heather, J.; Brooks, D.; Grenham, A.; et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med 2022, 386, 837–846. [Google Scholar] [CrossRef]
- Muller, W.J.; Madhi, S.A.; Seoane Nuñez, B.; Baca Cots, M.; Bosheva, M.; Dagan, R.; Hammitt, L.L.; Llapur, C.J.; Novoa, J.M.; Saez Llorens, X.; et al. Nirsevimab for prevention of RSV in term and late-preterm infants. N Engl J Med 2023, 388, 1533–1534. [Google Scholar] [CrossRef]
- Drysdale Simon, B.; Cathie, K.; Flamein, F.; Knuf, M.; Collins Andrea, M.; Hill Helen, C.; Kaiser, F.; Cohen, R.; Pinquier, D.; Felter Christian, T.; et al. Nirsevimab for prevention of hospitalizations due to RSV in infants. N Engl J Med 2023, 389, 2425–2435. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Drysdale, S.B.; Cathie, K.; Flamein, F.; Knuf, M.; Collins, A.M.; Hill, H.C.; Kaiser, F.; Cohen, R.; Pinquier, D.; et al. 180-day efficacy of nirsevimab against hospitalisation for respiratory syncytial virus lower respiratory tract infections in infants (HARMONIE): a randomised, controlled, phase 3b trial. Lancet Child Adolesc Health 2025, 9, 404–412. [Google Scholar] [CrossRef]
- Riccò, M.; Cascio, A.; Corrado, S.; Bottazzoli, M.; Marchesi, F.; Gili, R.; Giuri, P.G.; Gori, D.; Manzoni, P. Impact of nirsevimab immunization on pediatric hospitalization rates: a systematic review and meta-analysis (2024). Vaccines (Basel) 2024, 12. [Google Scholar] [CrossRef]
- Domachowske, J.; Madhi, S.A.; Simões, E.A.F.; Atanasova, V.; Cabañas, F.; Furuno, K.; Garcia-Garcia, M.L.; Grantina, I.; Nguyen, K.A.; Brooks, D.; et al. Safety of nirsevimab for RSV in infants with heart or lung disease or prematurity. N Engl J Med 2022, 386, 892–894. [Google Scholar] [CrossRef]
- Morris, T.; Acevedo, K.; Alvarez Aldeán, J.; Fiscus, M.; Hackell, J.; Pérez Martín, J.; Sanchez Luna, M.; Weil-Olivier, C.; Tate, J. Lessons from implementing a long-acting monoclonal antibody (nirsevimab) for RSV in France, Spain and the US. Discover Health Systems 2025, 4, 21. [Google Scholar] [CrossRef]
- Mallah, N.; Pardo-Seco, J.; Pérez-Martínez, O.; Durán-Parrondo, C.; Martinón-Torres, F. Full 2023-24 season results of universal prophylaxis with nirsevimab in Galicia, Spain: the NIRSE-GAL study. Lancet Infect Dis 2025, 25, e62–e63. [Google Scholar] [CrossRef]
- Torres, J.P.; Sauré, D.; Goic, M.; Thraves, C.; Pacheco, J.; Burgos, J.; Trigo, N.; Del Solar, F.; Neira, I.; Díaz, G.; et al. Effectiveness and impact of nirsevimab in Chile during the first season of a national immunisation strategy against RSV (NIRSE-CL): a retrospective observational study. Lancet Infect Dis 2025. [Google Scholar] [CrossRef] [PubMed]
- Wadia, U.; Moore, H.C.; Richmond, P.C.; Levy, A.; Bell, L.; Pienaar, C.; Harvey, J.; Finucane, C.; van der Helder, E.; Bloomfield, L.; et al. Effectiveness of nirsevimab in preventing RSV-hospitalisation among young children in Western Australia 2024. J Infect 2025, 90, 106466. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Enflonsia prescribing information. Available online: https://www.merck.com/product/usa/pi_circulars/e/enflonsia/enflonsia_pi.pdf (accessed on 19 June 2025).
- Zar, H.J.; Simoes, E.; Madhi, S.; Ramilo, O.; Senders, S.; Shepard, J.S.; Laoprasopwattana, K.; Piedrahita, J.; Novoa Pizarro, J.M.; Vargas, S.L.; et al. 166. A phase 2b/3 study to evaluate the efficacy and safety of an investigational respiratory syncytial virus (RSV) antibody, clesrovimab, in healthy preterm and full-term infants. Open Forum Infect Dis 2025, 12. [Google Scholar] [CrossRef]
- Zar, H.J.; Bont, L.J.; Manzoni, P.; Munoz, F.M.; Ramilo, O.; Chen, P.-Y.; Novoa Pizarro, J.M.; Ordonez, G.A.; Tsolia, M.; Tapiero, B.; et al. 167. Phase 3, randomized, controlled trial evaluating safety, efficacy, and pharmacokinetics (PK) of clesrovimab in infants and children at increased risk for severe respiratory syncytial virus (RSV) Disease. Open Forum Infect Dis 2025, 12. [Google Scholar] [CrossRef]
- Zar, H.J.; Simões, E.A.F.; Madhi, S.A.; Ramilo, O.; Senders, S.D.; Shepard, J.S.; Laoprasopwattana, K.; Piedrahita, J.; Novoa, J.M.; Vargas, S.L.; et al. Clesrovimab for prevention of RSV disease in healthy infants. N Engl J Med 2025, 393, 1292–1303. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Abrysvo prescribing information. Available online: https://www.fda.gov/media/168889/download?attachment (accessed on 15 May 2025).
- US Food and Drug Administration. Abrysvo biologics license application approval. Available online: https://www.fda.gov/media/171492/download?attachment (accessed on 15 May 2025).
- European Medicine Agency. Abrysvo (respiratory syncytial virus vaccine (bivalent, recombinant)): an overview of Abrysvo and why it is authorised in the EU. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/abrysvo (accessed on 20 July 2025).
- Fleming-Dutra, K.E.; Jones, J.M.; Roper, L.E.; Prill, M.M.; Ortega-Sanchez, I.R.; Moulia, D.L.; Wallace, M.; Godfrey, M.; Broder, K.R.; Tepper, N.K.; et al. Use of the Pfizer respiratory syncytial virus vaccine during pregnancy for the prevention of respiratory syncytial virus-associated lower respiratory tract disease in infants: recommendations of the Advisory Committee on Immunization Practices - United States, 2023. MMWR Morb Mortal Wkly Rep 2023, 72, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Marchand, G.J.; Massoud, A.T.; Abdelsattar, A.T.; McCullough, P.A. RSVpreF vaccination in pregnancy: a meta-analysis of maternal-fetal safety and infant efficacy. Obstet Gynecol Sci 2024, 67, 511–524. [Google Scholar] [CrossRef]
- World Health Organization. Safety of maternal vaccination against RSV. Available online: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/rsv.
- Killikelly, A.; Siu, W.; Brousseau, N. Summary of the National Advisory Committee on Immunization (NACI) Statement on the prevention of respiratory syncytial virus (RSV) in infants. Can Commun Dis Rep 2025, 51, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Pérez Marc, G.; Vizzotti, C.; Fell, D.B.; Di Nunzio, L.; Olszevicki, S.; Mankiewicz, S.W.; Braem, V.; Rearte, R.; Atwell, J.E.; Bianchi, A.; et al. Real-world effectiveness of RSVpreF vaccination during pregnancy against RSV-associated lower respiratory tract disease leading to hospitalisation in infants during the 2024 RSV season in Argentina (BERNI study): a multicentre, retrospective, test-negative, case-control study. Lancet Infect Dis 2025. [Google Scholar] [CrossRef]
- UK Health Security Agency. Guidance: RSV vaccination of pregnant women for infant protection (information for healthcare practitioners). Available online: https://www.gov.uk/government/publications/respiratory-syncytial-virus-rsv-programme-information-for-healthcare-professionals/rsv-vaccination-of-pregnant-women-for-infant-protection-information-for-healthcare-practitioners (accessed on 20 July 2025).
- Australian Government Department of Health Disability and Ageing. Australian immunisation handbook: respiratory synctial virus. Available online: https://immunisationhandbook.health.gov.au/contents/vaccine-preventable-diseases/respiratory-syncytial-virus-rsv (accessed on 15 May 2025 ).
- Nazareno, A.L.; Newall, A.T.; Muscatello, D.J.; Hogan, A.B.; Wood, J.G. Modelling the epidemiological impact of maternal respiratory syncytial virus (RSV) vaccination in Australia. Vaccine 2024, 42, 126418. [Google Scholar] [CrossRef] [PubMed]
- Obstetrical & Gynaecological Society of Malaysia. Malaysian Maternal Immunisation Consensus Guidelines. Available online: https://www.ogsm.org.my/docs/Maternal-Immunisation-Guidelines.pdf (accessed on 15 May 2025).
- Simões, E.A.F.; Pahud, B.A.; Madhi, S.A.; Kampmann, B.; Shittu, E.; Radley, D.; Llapur, C.; Baker, J.; Pérez Marc, G.; Barnabas, S.L.; et al. Efficacy, safety, and immunogenicity of the MATISSE (Maternal Immunization Study for Safety and Efficacy) maternal respiratory syncytial virus prefusion F protein vaccine trial. Obstet Gynecol 2025, 145, 157–167. [Google Scholar] [CrossRef]
- Zeevat, F.; van der Pol, S.; Kieffer, A.; Postma, M.J.; Boersma, C. Cost-effectiveness analysis of nirsevimab for preventing respiratory syncytial virus-related lower respiratory tract disease in Dutch infants: an analysis including all-infant protection. Pharmacoeconomics 2025, 43, 569–582. [Google Scholar] [CrossRef]
- Langedijk, A.C.; van den Dungen, F.; Harteveld, L.; van den Boer, J.; Smit, L.; Averin, A.; Quinn, E.; Atwood, M.; Law, A.; Mendes, D.; et al. Cost-effectiveness of immunization strategies to protect infants against respiratory syncytial virus in the Netherlands. Hum Vaccin Immunother 2025, 21, 2521912. [Google Scholar] [CrossRef]
- Hutton, D.W.; Prosser, L.A.; Rose, A.M.; Mercon, K.; Ortega-Sanchez, I.R.; Leidner, A.J.; McMorrow, M.L.; Fleming-Dutra, K.E.; Prill, M.M.; Pike, J.; et al. Cost-effectiveness of maternal vaccination to prevent respiratory syncytial virus illness. Pediatrics 2024, 154. [Google Scholar] [CrossRef]
- Wang, Q.; Wu, J.; Li, L.; Guo, Z.; Zheng, B.; Zhang, S.; Xiang, C.; Li, M.; Qiao, X.; Lv, X.; et al. Cost-effectiveness analysis of nirsevimab for prevention of respiratory syncytial virus disease among infants in Shanghai, China: A modeling study. Hum Vaccin Immunother 2025, 21, 2506288. [Google Scholar] [CrossRef]
- Noto, S.; Kieffer, A.; Soudani, S.; Arashiro, T.; Tadera, C.; Eymere, S.; Lemański, T.; Wang, X. Cost-effectiveness and public health impact of universal prophylaxis with nirsevimab against respiratory syncytial virus (RSV) infections in all infants in Japan. Infect Dis Ther 2025, 14, 847–865. [Google Scholar] [CrossRef]
- Gebretekle, G.B.; Yeung, M.W.; Ximenes, R.; Cernat, A.; Simmons, A.E.; Killikelly, A.; Siu, W.; Rafferty, E.; Brousseau, N.; Tunis, M.; et al. Cost-effectiveness of RSVpreF vaccine and nirsevimab for the prevention of respiratory syncytial virus disease in Canadian infants. Vaccine 2024, 42, 126164. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Vittucci, A.C.; Antilici, L.; Pisani, M.; Scutari, R.; Di Maio, V.C.; Musolino, A.M.C.; Cristaldi, S.; Cutrera, R.; Perno, C.F. Prevention of RSV bronchiolitis: an ethical issue. Pediatr Infect Dis J 2024, 43, e296–e297. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
a) RSV structure and the b) RSV F glycoproteins. Modified from Akagawa M, et al. Viruses. 2022;14(11):2382. doi: 10.3390/v14112382. © 2022 The Authors. Licensed under CC BY 4.0. The RSV F glycoprotein is integral in the entry of virus into cells; during viral entry, the RSV F glycoprotein refolds from a prefusion to postfusion conformation, driving fusion of the viral and host membranes and enabling viral entry, after which viral replication proceeds. Passive prophylaxis targets several of the six sites on the RSV F glycoprotein: palivizumab, site II; nirsevimab, site Ø; clesrovimab, site IV.
Figure 1.
a) RSV structure and the b) RSV F glycoproteins. Modified from Akagawa M, et al. Viruses. 2022;14(11):2382. doi: 10.3390/v14112382. © 2022 The Authors. Licensed under CC BY 4.0. The RSV F glycoprotein is integral in the entry of virus into cells; during viral entry, the RSV F glycoprotein refolds from a prefusion to postfusion conformation, driving fusion of the viral and host membranes and enabling viral entry, after which viral replication proceeds. Passive prophylaxis targets several of the six sites on the RSV F glycoprotein: palivizumab, site II; nirsevimab, site Ø; clesrovimab, site IV.
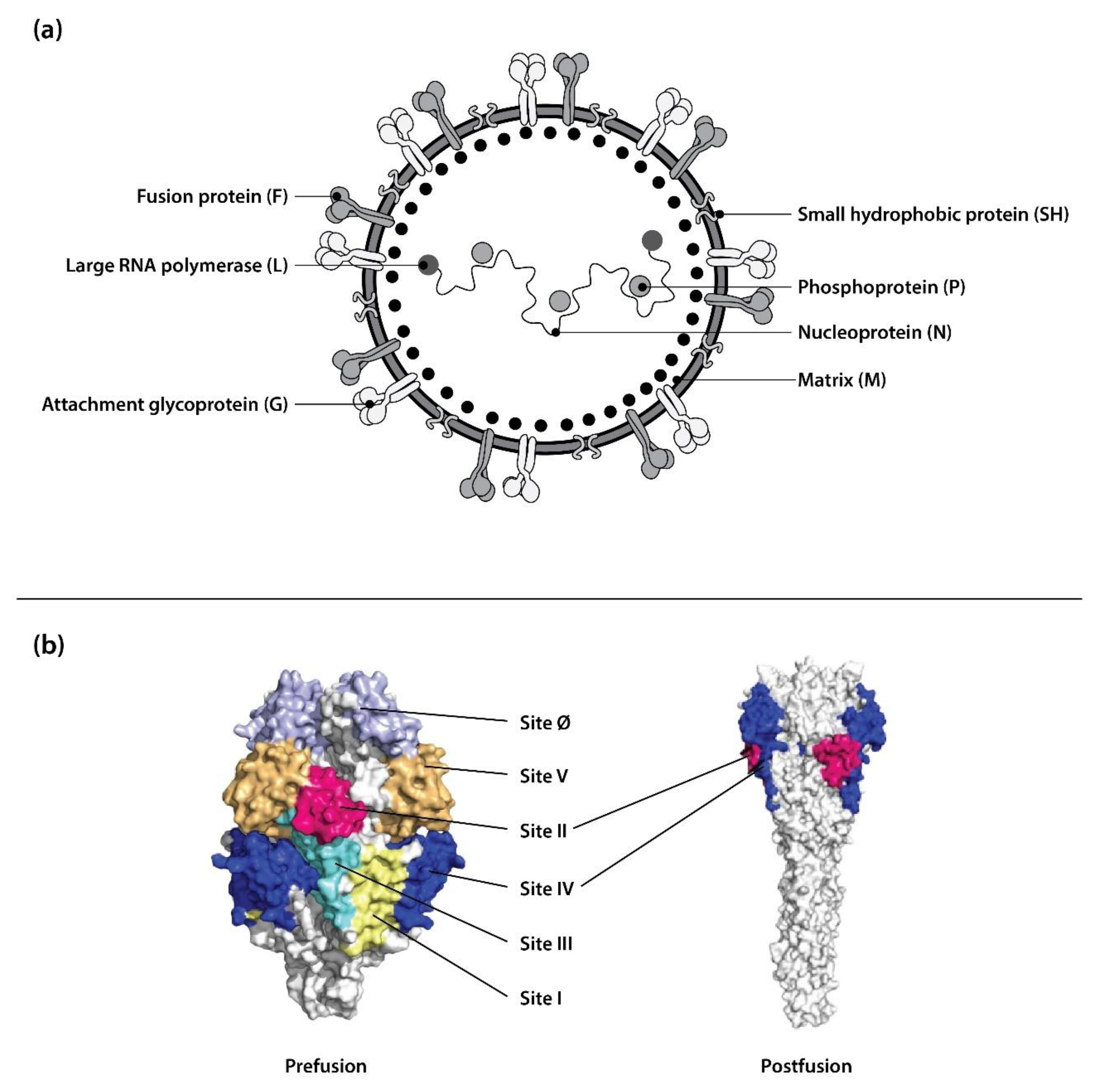
Figure 2.
Proposed RSV prevention strategies for Malaysian healthcare system.
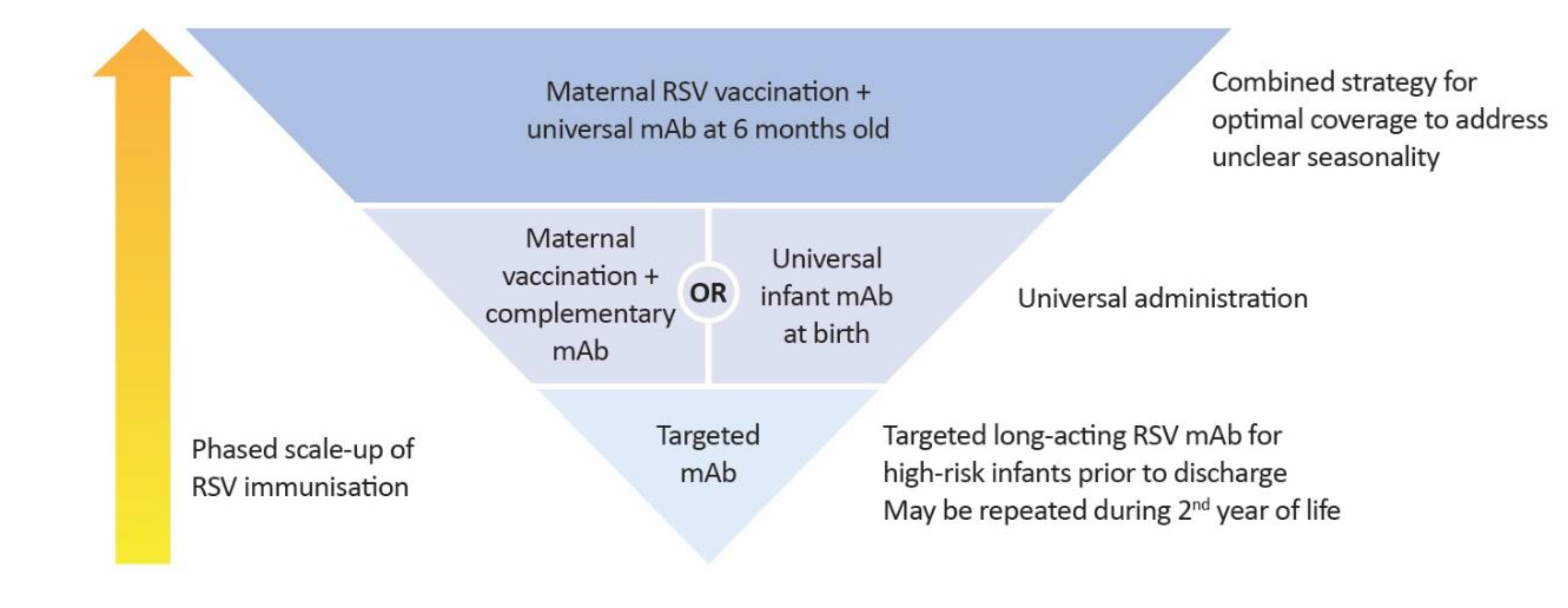

Table 1.
Efficacy outcomes from pivotal trials of nirsevimab.
| Trials | RSV MA-LRTI | RSV LRTI hospitalisation | Very severe RSV MA-LRTI | Very severe RSV LRTI hospitalisation |
|---|---|---|---|---|
| Phase 2b [61] (N = 1,453; nirsevimab = 969) |
70·1% (52·3–81·2) |
78·4% (51·9–90·3) |
- | - |
| MELODY, primary cohort [62] (N = 1,490; nirsevimab = 994) |
74·5% (49·6–87·1) |
62·1% (-8·6–86·6) |
- | - |
| MELODY, all subjects [63] (N = 3,012; nirsevimab = 2,009) |
76·4% (62·3–85·2) |
76·8% (49·4–89·4) |
78·6% (48·8–91) |
- |
| HARMONIE, through RSV season (~ 3 months) [64] (N = 8,058; nirsevimab = 4,037) |
- | 83·2% (67·8–92) |
- | 75·7% (32·8–92·9) |
| HARMONIE, through 180 days [65] (N = 8,058; nirsevimab = 4,037) |
- | 82·7% (67·8–91·5) |
- | 75·3% (38·1–91·8) |
Data presented as efficacy (95% CI). LRTI: lower respiratory tract infection; MA: medically attended; RSV: respiratory syncytial virus.
Table 2.
Cost-effectiveness analyses of RSV prevention strategies from other countries.
| Source | Strategy | Locality | Perspective | Price | WTP threshold | ICER |
|---|---|---|---|---|---|---|
| Zeevat, et al (2025) [89] | Universal nirsevimab (year-round) |
Netherlands | Societal | EJP: €220 | €50,000/QALY | €122,478/QALY (vs. palivizumab) |
| Universal nirsevimab (seasonal + catch-up) |
€50,000/QALY (vs. palivizumab) | |||||
| Langedijk, et al (2025) [90] | Universal nirsevimab | Netherlands | Societal | RSVpreF: €180 Nirsevimab: €547·23 (assumed) |
- | €592,404/QALY (vs. no intervention) |
| Maternal RSVpreF + complementary nirsevimab | €329,187/QALY (vs. no intervention) | |||||
| Hutton, et al (2024) [91] | Universal nirsevimab (seasonal + catch-up) | US | Societal | USD $445* | - | Universal: USD $153,517/QALY (vs. no intervention) High-risk children in second season: USD $308,468/QALY (vs. no intervention) |
| Wang, et al (2025) [92] | Universal nirsevimab (seasonal) | China | Societal | USD $263·83 | USD $26,866 | USD $13,073·79 (vs. no intervention) |
| Universal nirsevimab (year-round) |
USD $24,323·26 (vs. no intervention) | |||||
| Noto, et al (2025) [93] | Universal nirsevimab | Japan | Payer Societal |
¥45,000 EJP: ¥45,496 |
¥5,000,000 | Payer: ¥4,537,256/QALY (vs. palivizumab) Societal: ¥1,695,635/QALY (vs. palivizumab) |
| Gebretekle, et al (2024) [94] | Targeted nirsevimab for at-risk infants (seasonal + catch-up) | Canada | Health system and societal | Nirsevimab: CAD $110-190 RSVpreF: CAD $60-125 |
- | Infants at moderate/high-risk: CAD $27,891/QALY (vs. palivizumab) |
| Year-round maternal RSVpreF + nirsevimab for high-risk infants | CAD $50,000/QALY |
CAD $204,621/QALY (vs. seasonal nirsevimab for infants at moderate/high risk) |
||||
| Universal nirsevimab (seasonal + catch-up) | CAD 512,265 (vs. year-round maternal RSVpreF + nirsevimab for high-risk infants) |
*Assumption: With doses purchased through Vaccines for Children ($395) and commercial channel ($495), a weighted average of $445/dose was used as base-case cost. EJP: economically justifiable price; ICER: incremental cost-effectiveness ratio; QALY: quality-adjusted life-years; RSVpreF: RSV prefusion F; WTP: willingness-to-pay.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



