
Submitted:
29 November 2025
Posted:
02 December 2025
You are already at the latest version
Abstract
Abstract: Background: Academic health sciences libraries face organizational challenges because medical and health sciences schools are part of integrated academic health systems, yet there remains a lack of systematic guidance on structuring these libraries. Purpose: To create a mission-driven analytical framework that examines library organizational models within academic health systems, focusing on service delivery throughout the educational continuum and utilizing hub-spoke organizational principles from healthcare. Methods: We conducted a systematic literature review, thematic analysis, and iterative framework development grounded in organizational theory and healthcare delivery principles to develop a mission-driven decision framework. Results: Analysis reveals three main organizational models: independent (school-based), integrated (university library system), and hub-spoke (distributed). There is no single best model—success depends on institutional context, goals, resources, and stakeholder needs. Mission alignment should guide organizational design, with cost and feasibility considerations coming into play only after mission objectives are met. Hub-spoke models offer benefits for geographically dispersed systems, requiring higher initial investment but providing a strong return through reduced duplication and increased efficiency. Supporting the educational continuum from undergraduate to continuing medical education demands careful organizational planning to address service fragmentation during transitional phases. Conclusions: Choosing an organizational model involves a systematic, mission-driven analysis that aligns institutional missions with service needs and matches these needs to suitable organizational structures. This framework is the first to offer a comprehensive analytical method for making managerial decisions in complex academic health system environments, including practical guidance for implementation and economic validation. It shows that structures aligned with the mission can lead to positive returns on institutional investment.
Keywords:
academic health systems
; health sciences libraries
; organizational models
; hub-spoke model
; educational continuum
; mission-driven organizational design
; library administration
; implementation science
Key Terminology
Throughout this manuscript, we use specific terms consistently:

Table 1.
Core Terminology and Definitions.
| Term | Definition | Key Distinguishing Features |
| Academic Health System (AHS) | Integrated organization combining medical education, biomedical research, clinical care delivery, and community health missions under unified or coordinated governance | Multiple missions, complex stakeholder ecosystem, distributed operations |
| Organizational Model | One of three archetypal structural frameworks (independent, integrated, hub-spoke) characterized by reporting relationships, resource allocation, and service delivery patterns | Conceptual framework used for analysis and comparison |
| Organizational Structure | The actual implemented arrangement of reporting, governance, and operations at a specific institution | May combine elements from multiple models; context-specific implementation |
| Independent (School-Based) Model | Library operates as unit within medical school with director reporting to dean, school-funded budget, and governance within school administration | Autonomy within school, direct educational alignment, single-site focus |
| Integrated (University Library) Model | Health sciences library services provided as part of comprehensive university library system with shared infrastructure and centralized operations | Economies of scale, shared services, potential for specialized positions |
| Hub-Spoke Model | Organizational structure featuring centralized specialized expertise and coordination functions (hub) connected to distributed service points (spokes) providing local access | Combines specialization with geographic reach; requires coordination infrastructure |
| Mission-Driven Design | Analytical approach determining organizational structure through systematic translation: institutional missions → essential services → service delivery characteristics → enabling organizational structures | Mission alignment is PRIMARY principle; other considerations are subordinate |
| Educational Continuum | The complete trajectory of physician development from undergraduate medical education (UME) through graduate medical education/residency (GME) through continuing medical education (CME) and lifelong learning | Emphasizes progressive competency development requiring coordinated support |
1. Introduction
1.1. The Problem and Its Strategic Importance
Over the past thirty years, academic health systems have evolved from simple, single-campus medical schools into complex, distributed networks. These now include multiple clinical sites, diverse health professions programs, geographically dispersed training environments, and intricate stakeholder ecosystems. Libraries, initially designed for medical students on a single campus, now must support a wide range of users: residents at community hospitals, research center faculty, clinicians at satellite clinics, nursing and pharmacy students at various locations, and alumni participating in continuing education while working. Despite these changes, many institutions' organizational structures still reflect outdated models focused on geographical concentration and traditional education cores.
Although the importance of library organizational structure in achieving an institution's mission is evident, there is surprisingly limited comprehensive guidance to inform evidence-based decision-making [1,5,6]. Library directors often lack detailed frameworks for evaluating options and predicting outcomes when considering organizational changes [7]. Similarly, administrators in academic health systems often lack access to comparative data on costs, benefits, and organizational effectiveness [8]. For new academic health systems, particularly those in international contexts where integrated systems are built from scratch rather than through consolidation, guidance on the optimal library organizational structure is scarce [9]. The field generally relies on institutional tradition, reactive budgeting, and peer imitation rather than on systematic analysis of how organizations can best support institutional goals and missions [10].
1.2. Purpose and Research Questions
This research addresses a gap in systematic knowledge by developing an evidence-based analytical framework to support decision-making in library organizations within academic health systems. The framework emphasizes mission-driven analysis as the fundamental principle of organizational design and provides structured approaches for translating institutional missions into requirements for organizational structure.
This study investigates four interconnected questions to facilitate a structured analysis of organizations. First, it assesses the organizational models adopted by academic health sciences libraries within academic health systems and the institutional factors that influence their success across contexts [3,4]. Second, it explores how healthcare delivery models, particularly hub-and-spoke structures that combine centralized expertise with broader access, can inform the organization of library services in academic health systems [12,13]. Third, it considers how libraries can design services to support the entire educational continuum—from undergraduate medical education to residency, continuing medical education, and lifelong professional development [14,15]. Fourth, it identifies principles that underpin mission-driven organizational design, applicable systematically across various institutional contexts, while acknowledging that specific organizational solutions must be adapted to local conditions [16].
1.3. Scope and Significance
This study investigates academic health sciences libraries within integrated academic health systems that include educational, research, clinical, and community service roles [17]. It examines the organizational structure, governance, service delivery models, resource allocation, and the process of organizational transformation. Although primarily focused on North American examples, the study develops adaptable frameworks for different regional contexts [18].
The significance of this work operates at multiple levels. For library practice, it provides systematic frameworks enabling directors and administrators to analyze organizational options, make strategic decisions grounded in mission requirements, and implement organizational transformations effectively. [7,19] For academic health system leadership, it clarifies how library organizational structure affects institutional mission achievement and provides economic analysis supporting resource allocation decisions. [8] In the library and information science field, it advances organizational knowledge by integrating organizational theory, implementation science, and mission-driven analysis. [11,20] For healthcare education broadly, it demonstrates how information service infrastructure can be organized strategically to support distributed educational, research, and clinical operations. [21]
2. Conceptual Framework and Literature Foundations
2.1. Mission-Driven Organizational Design: Establishing the Foundational Principle
This research emphasizes mission alignment as the central principle guiding how libraries are organized within academic health systems [22,23]. It proposes that the organizational structure should be developed through a systematic analysis that starts with the institution's mission, identifies essential services and delivery needs, and finally designs the organizational frameworks to support these elements [24]. This mission-centered approach represents a significant departure from traditional organizational analysis, which often relies on existing models—such as peer institutions' structures, prescriptive theories, or conventional practices based on tradition or convenience [10].
The mission-driven framework challenges the conventional method by initially asking, "What must this library do to support the achievement of the institutional mission?" before contemplating, "What organizational structure best supports those key functions?" [25] This viewpoint regards organizational structure as a variable influenced by mission needs rather than a choice based on theory or the success of peers [26]. It suggests that organizational analysis should be customized for each institution's specific mission, since different goals require different services and potentially different structures [27]. Additionally, this method offers a straightforward way to evaluate effectiveness: does the organizational structure enable the delivery of services essential for fulfilling the institutional mission?
2.1.1. The Mission-to-Structure Translation Process
The mission-driven framework functions via a four-stage translation process that systematically transforms abstract institutional mission statements into tangible organizational structure requirements [22].
Figure 1 illustrates this convergent process, showing how broad institutional missions progressively narrow through systematic analysis to a derived organizational structure. The funnel shape visually communicates the core principle: structure is a dependent variable determined by mission requirements, not an independent choice.
Stage 1: Mission Analysis begins with a comprehensive review of the academic health system's actual functions, avoiding generic mission statements [29]. The education mission needs a clear definition: which educational programs are offered, their levels, student numbers, teaching methods, and program locations [30]. Similarly, the research mission requires detailed specifics: research funding amounts, main research areas, key methodological approaches, and existing infrastructure [31]. The clinical mission analysis examines the patient populations served, clinical specialties and services, the geographic scope of clinical activities, and quality-improvement priorities [32]. The community mission assessment details commitments to community involvement, population health initiatives, and public education roles [33].
Stage 2: Service Requirements Mapping systematically determines the key library services needed to accomplish the specific missions outlined in the earlier analysis [34].
Table 2.
Service Requirements by Mission Domain.
| Mission Domain | Primary Stakeholders | Essential Library Services | Consequence of Absence | Mission Criticality |
| Undergraduate Medical Education (UME) | Medical students, educational faculty | Curriculum-integrated information literacy instruction; study resources and spaces; research support for scholarly projects; clinical resources during rotations | Students graduate without required information literacy competencies; educational quality declines; accreditation jeopardized | HIGH |
| Research Mission (Basic-Level) | Faculty at primarily teaching institutions | Literature searching and retrieval; interlibrary loan; basic reference consultation; citation management support | Faculty conduct literature reviews less efficiently; publication productivity constrained | MODERATE |
| Research Mission (Research-Intensive) | Faculty at institutions with >$50M research expenditures | Systematic review services with librarian co-authorship; bioinformatics consultation; research data management; scholarly communication expertise; bibliometrics | Research quality compromised; researchers cannot compete for funding; compliance with funder mandates fails | HIGH |
| Clinical Care Mission | Attending physicians, residents, fellows, advanced practice providers | Clinical decision support tools at point of care; embedded clinical librarian services; support for practice guideline development | Clinicians make decisions without current evidence; clinical quality suffers; patient safety compromised | HIGH |
| Community Service Mission | Public, patients, community partners | Consumer health information; health literacy resources; training for professionals in patient education | Community engagement opportunities missed; population health impact limited | MODERATE |
Stage 3: Service Characteristics Analysis explores the unique features of each critical service that influence its delivery methods within the organization [35].
Table 3.
Service Delivery Characteristics Analysis Framework.
| Characteristic Dimension | High/Critical Level | Moderate/Preferential Level | Low/Independent Level | Organizational Implication |
| Specialization Level | Systematic reviews requiring methodological sophistication; bioinformatics requiring computational expertise | Research consultation requiring professional librarian knowledge; information literacy instruction | Circulation services; basic access support; routine interlibrary loan | High specialization favors hub concentration |
| Geographic Dependence | Clinical embedding requiring physical presence at care sites; student services requiring campus proximity | Reference consultation benefiting from face-to-face but functional via video | Systematic reviews fully location-independent; electronic resource management | Geographic dependence requires spoke presence |
| Time Sensitivity | Clinical questions requiring evidence within hours; urgent grant deadlines | Literature support for manuscripts needed within days | Systematic review projects unfolding over months | High time sensitivity demands local presence |
| Volume and Frequency | Information literacy instruction in hundreds of sessions annually; daily clinical consultations | Systematic review requests averaging 30-50 annually | Specialized methodology consultation occurring occasionally | High volume justifies dedicated positions |
Stage 4: Structure Evaluation marks the final step in the translation process, in which service requirements identified from the mission analysis are aligned with organizational capabilities. At this stage, the key question is: considering the services this library needs to provide for institutional mission success, and the characteristics of those services that influence how they are delivered, which organizational structures best support effective service delivery?
2.1.2. Mission Primacy: Why Mission Alignment Must Be the Primary Principle
A central and deliberate aspect of this conceptual framework is highlighting that mission-driven analysis serves as the foundational and vital principle of organizational design, rather than merely one element to balance with others [37]. This focus on its priority is essential to ensuring the framework's logical consistency and real-world applicability.
Imagine mission alignment as just one of many equally important factors. In such cases, organizations might focus on secondary issues like cost savings, ease of implementation, or popular management theories, which can lead to sacrificing mission support—either intentionally or unintentionally [38]. For instance, budget cuts meant to save costs by reducing essential services often harm mission effectiveness, even if they lower expenses [39]. By prioritizing mission alignment as the core principle and explicitly ranking other factors below it, the decision-making process gains a clear hierarchy [40].
2.2. Organizational Theories as Analytical Tools
The conceptual framework clearly positions organizational theories—such as stakeholder theory, resource dependency theory, institutional theory, and service delivery models—as analytical tools for understanding organizational behavior, rather than as prescriptive templates to be applied universally [41,42].
Organizational theories provide valuable insights into why specific structures thrive or fail in particular contexts [43]. Stakeholder theory explains which interests are emphasized by different organizational structures and which might be neglected [44]. Resource dependency theory illustrates how structures are influenced by reliance on vital resource providers [45]. Institutional theory demonstrates how organizations modify their structures to meet external legitimacy and professional standards [46].
2.3. Literature Review: Findings and Implications
The literature review revealed notable gaps in understanding library organizational models within academic health systems. Most existing research is descriptive rather than analytical, emphasizing organizational structures without examining the reasons for their choices or their impact on outcomes. Publication bias often favors success stories, and the predominance of studies conducted in North America limits insights into their applicability elsewhere. There is little comparative analysis among different models, and economic evaluations are rare. While hub-spoke models are mentioned in practical contexts, few studies explicitly analyze them using this framework. Moreover, fragmentation across the educational continuum is widely acknowledged, yet effective, systematic solutions are still lacking.
2.4. Accreditation Requirements: Establishing Minimum Standards
Accreditation bodies for medical education and residency training set minimum standards for library resources and services that organizational structures must support [51].
Table 4.
Accreditation Standards and Organizational Implications.
| Accrediting Body | Applicable Standard | Key Requirements | Organizational Implications |
| LCME | Standard 6.1: Library Resources and Staff | Sufficient resources and staff at all sites; adequate personnel with expertise; training in literature searching | Distribution requirement: challenges campus-only models. Expertise requirement: cannot rely solely on non-professional staff. |
| LCME | Standard 7.5: Self-Directed and Lifelong Learning | Prepare students for lifelong learning; information literacy as core competency | Curriculum integration imperative: library must be educational partner. |
| ACGME | Common Program Requirement II.B.1 | Residents have access to adequate resources at all training sites | Multi-site access requirement: creates challenge for traditional campus libraries. |
| ACGME | Common Program Requirement IV.C | Adequate resources for scholarly activities | GME-specific support requirement: services that school-based libraries may not provide. |
3. Research Methods
This section describes the systematic approach used to develop the mission-driven organizational framework. [11]
3.1. Research Approach
This study adopts a qualitative research approach that integrates systematic literature synthesis, application of organizational theory, thematic analysis, and an iterative process for framework development [52,53]. The research is conducted within a pragmatic paradigm that emphasizes practical usefulness while ensuring analytical rigor [54]. The search strategy includes databases such as PubMed, LISTA, Web of Science, ERIC, and Scopus from 2000 to 2025, along with gray literature from professional organizations [55]. Thematic analysis was performed using Braun and Clarke's method, incorporating both deductive and inductive coding. [56] The framework was developed iteratively through several refinement cycles to meet quality criteria, including comprehensiveness, coherence, utility, transferability, and clarity [57]. Economic analysis was triangulated using salary surveys, institutional reports, and consultations with practitioners. [8]
4. Organizational Models and Mission Alignment Analysis
This section provides a detailed analysis of three main organizational models: independent school-based libraries, integrated university library systems, and hub-spoke distributed models [3,4].
4.0. Comparative Overview: Three Primary Models
Table 5.
Organizational Models: Comparative Summary.
| Dimension | Independent (School-Based) | Integrated (University Library) | Hub-Spoke (Distributed) |
| Governance | Reports to Dean of Medical School | Reports through university library administration | Unified governance across distributed locations |
| Budget Structure | School educational budget | University library allocation with health sciences share | Multiple funding sources pooled |
| Typical Staffing | 6-10 FTE | 6-12 FTE health sciences specialists plus shared services | 12-18 FTE (6 hub + 7-12 spokes) |
| Geographic Reach | Single campus concentration | Single campus or limited distribution | System-wide distributed presence |
| 136 refereUME Support | Excellent | Good to Strong | Excellent |
| GME Support | Weak to Minimal | Weak to Moderate | Excellent |
| Research Support (Generalist) | Good | Strong | Excellent |
| Research Support (Specialized) | Limited | Strong to Excellent | Excellent |
| Clinical Care Support | Weak | Weak to Moderate | Excellent |
| Implementation Complexity | Low | Moderate | High |
| Optimal Context | Education-focused, geographically centralized, 300-600 students | Research-intensive universities, multiple health sciences programs, cost efficiency priority | Large geographically distributed AHS, 3+ clinical sites, >1,500 residents/clinicians |
| Primary Strength | Deep educational integration | Cost efficiency through economies of scale | Comprehensive mission support across distributed geography |
| Primary Limitation | Cannot sustain specialized services; limited GME/clinical reach | Risk of health sciences focus dilution | Highest organizational investment and coordination complexity |
4.1. Independent School-Based Library Model
The independent school-based library model reflects the traditional setup in academic medicine, in which the library operates as a separate administrative unit within the medical school, with the library director reporting directly to the dean. Usually, this model has a director overseeing six to ten full-time professional librarians and support staff, serving a focused community of about 400-600 medical students and 150-200 faculty members, mainly located on a single campus.
From a mission alignment perspective, the independent school-based model strongly supports undergraduate medical education through various interconnected mechanisms [51,59]. Being positioned directly within medical school administrative structures provides natural routes for library involvement in curriculum committees, educational governance, and assessment initiatives [60]. This structural integration fosters proper curriculum integration, enabling information literacy instruction to develop progressively across the four to six years of medical education [61].
The independent model excels at supporting educational missions but has notable limitations in achieving other institutional goals. Research support is generally at a broad level because school budgets usually cannot fund specialized library roles. Support for the clinical mission is even more challenged, as these libraries often have little to no organizational ties to hospital operations. Additionally, geographic distribution remains a significant obstacle for modern academic health systems, primarily as they increasingly function across multiple clinical locations.
Analysis of the cost structure for a typical independent school-based implementation shows moderate overall costs but relatively high per-person expenses. Personnel costs are approximately $663,000 to $917,000 per year for eight full-time staff. Non-personnel expenses range from $640,000 to $1,050,000. The total yearly operating costs range from $1.3 million to $2.0 million [8].
4.2. Integrated University Library System Model
The integrated university library system model incorporates health sciences library services into overall university library systems rather than treating them as separate school units [4]. Leadership usually involves an Associate University Librarian for Health Sciences, who reports to the university library administration rather than directly to health sciences deans [66].
From a mission alignment standpoint, integrated university library models offer notable benefits for research-oriented missions that need specialized services, which smaller independent libraries are unable to sustain [67]. These university library systems, serving thousands of faculty and students across multiple programs, can financially support specialized roles such as systematic review librarians, data specialists, and scholarly communication experts [68]. Additionally, cost efficiency gained through economies of scale is a significant advantage [69].
However, integrated models encounter notable challenges [70]. The primary issue is the potential dilution of focus on health sciences as library resources are spread across different university groups [71]. Additionally, organizational disconnect from health sciences leadership presents another hurdle [72]. Establishing links to the clinical mission is particularly challenging, as universities often lack direct connections to hospital operations [64].
The integrated model works best when research demands specialized services, cost efficiency is a key strategic focus, multiple health sciences programs are available, and university library systems are firmly committed to health sciences [4]. Its cost structure shows moderate total spending with the lowest per-capita costs. Annual costs range between $1.4 million and $2.2 million [8].
4.3. Hub-Spoke Distributed Model
The hub-and-spoke distributed model describes an organizational structure that balances centralized expertise with local access [12,13]. This model includes a central hub where specialized librarians are based, linked to multiple spoke locations where librarians offer local presence [73].
Figure 2 illustrates this architecture, highlighting how the central hub of specialized expertise (such as systematic reviews, informatics, and scholarly communication) connects to various spokes that differ in size and function. The size of each spoke indicates the level of service provided—large spokes at teaching hospitals include embedded librarians, while smaller spokes at outpatient clinics mainly receive virtual support. Bidirectional arrows demonstrate the flow of expertise from the hub to the spokes and the inward flow of complex referrals from spokes back to the hub.
From a mission-alignment perspective, hub-and-spoke models provide comprehensive support across the full range of AHS missions [74]. The hub concentrates rare, expensive expertise, including systematic review specialists, informatics experts, and scholarly communication specialists [75]. Simultaneously, distributed spoke librarians positioned at major clinical sites provide a local, accessible presence [76].
Clinical embedding is possible when librarians are physically present at hospitals [77,78]. Supporting graduate medical education is feasible when librarians at training hospitals establish connections with residency programs [79]. The educational continuum is especially beneficial, as a distributed presence enables monitoring learners across various training stages [14].
However, hub-spoke models present notable challenges. [80] Their implementation requires recruiting multiple spoke librarians, establishing workspaces across various locations, and developing the necessary technology infrastructure. [81] Cost is a key consideration—these models require the highest overall investment due to distributed staffing, typically 12-18 full-time equivalents (FTE). [8] The initial setup costs range from $325,000 to $575,000, while annual operating expenses range from $2.0 to $2.9 million. By comparison, maintaining separate libraries at each location would cost $2.8 to $4.2 million annually, so hub-spoke models can achieve savings of approximately 30-40%. [82] ROI analysis shows that these models yield an ROI of 1.84-2.14. [83]
5. Service Delivery Across the Educational Continuum
Challenges along the educational continuum demand targeted analysis as developing health professionals become more critical, yet library structures often fragment at phase transitions.
5.1. The Continuum Challenge
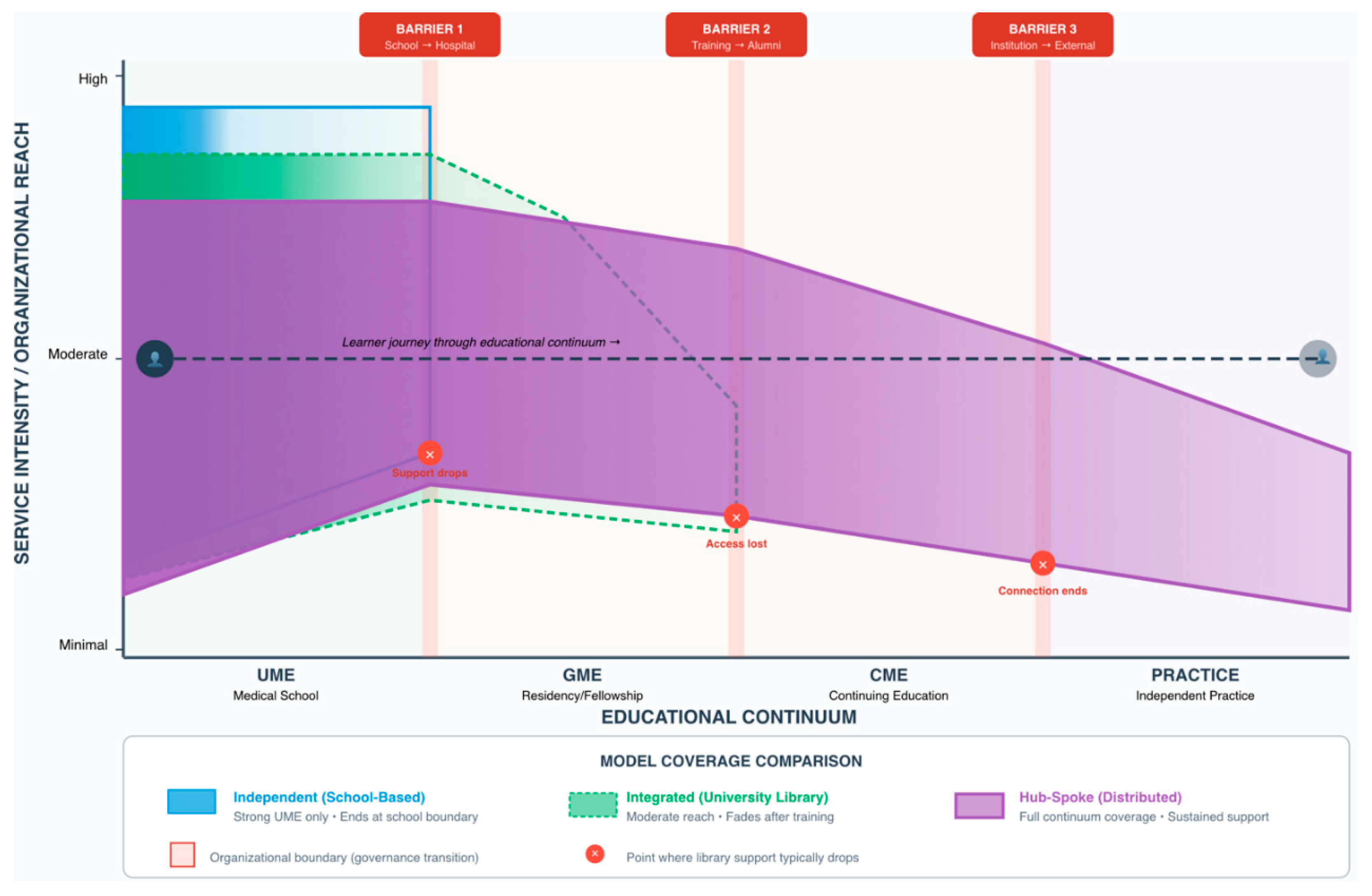
Medical education increasingly focuses on a continuous development path from undergraduate medical education (UME) through graduate medical education (GME) to continuing medical education (CME) and lifelong learning. [30] Competency-based education frameworks aim for gradual skill improvement that builds over time. [84] The competencies in evidence-based practice learned during medical school should be further refined during residency and maintained throughout a physician's career. [85] However, library support often breaks apart at transition points, creating gaps where ongoing support is most needed and where continuity is crucial. [14]
Figure 3 depicts this fragmentation using a coverage map that overlays three organizational models along the same continuum, illustrating their distinct outreach levels: independent models (blue) sharply end at the school-hospital governance boundary; integrated models (green) extend further but lessen after training ceases; only hub-spoke models (purple) maintain substantial coverage across the entire continuum. Vertical barriers show where organizational boundaries, not educational principles, lead to support decline.
5.2. Phase-Specific Characteristics and Support Requirements
Undergraduate medical training occurs within organized curricular frameworks that include clear learning objectives, regular assessments, close faculty supervision, and designated study time [30,86]. Medical students primarily need to gain core knowledge, understand disease mechanisms, and learn to consult evidence regularly [87]. The library's educational role can be formally structured, with librarians providing instructional sessions that are integrated into the curriculum [51,60].
Graduate medical education occurs in fundamentally different contexts. [88,89] Residents take on direct patient care responsibilities under supervision, gradually gaining more autonomy. [90] The schedules are intense, providing little protected time. [91] With training across multiple sites, residents only have brief rotations at the main campus. [92] Their information needs to focus more on immediate clinical concerns. [93]
Continuing medical education and independent practice are even more demanding contexts. [94,95]. Physicians face intense time constraints. [96] They need immediate, specific information. [97] There is a lack of institutional infrastructure that offers protected learning time. [98] Despite this, the need for evidence-based practice remains equally, if not more, critical. [85]
5.3. Organizational Models and Continuum Support
Independent school-based libraries excel at supporting UME but face significant gaps in GME and CME support due to organizational boundaries. [3,62] While integrated university library models can provide a broader range of resources, they encounter similar challenges. [4] Hub-spoke models offer the greatest potential for continuous support, with distributed spoke presence and coordinated hubs ensuring ongoing skill development. [13,74] Nonetheless, establishing continuum support demands planning rather than developing spontaneously. [99]
6. Implementation Framework
Implementation quality frequently has a greater impact than choosing a specific organizational model. [16,100] Here, we offer systematic guidance to support effective organizational transformations. [101]
6.1. Pre-Implementation Assessment
Successful implementation starts with an honest assessment of organizational readiness. [102,103] Leadership capacity and commitment must be evaluated. [104] Stakeholder alignment involves identifying who needs to cooperate. [44] The resource adequacy assessment should determine if funding is available. [105] Cultural readiness examines whether the organizational culture is open to change. [106]
6.2. Phased Implementation Approach
Implementation occurs through deliberate phases that support learning and adaptation. [16,109] Phase 1, which lasts 3-6 months, involves detailed organizational planning and design. [110] Phase 2, spanning 2-4 months, focuses on recruiting staff and establishing infrastructure. [111] Phase 3, lasting 6-12 months, starts with pilot testing at 1-2 sites. [112] Phase 4, taking 12-24 months, involves expanding and refining efforts to the remaining sites. [113] Finally, Phase 5, also 12-24 months, aims to stabilize and integrate the project into ongoing, sustainable operations. [114]
6.3. Stakeholder Engagement
Stakeholder engagement involves systematically identifying and mapping stakeholders. [44,115] It also requires developing engagement strategies tailored to their levels of power and interest. [116] Implementing various communication channels is essential. [117] To manage resistance effectively, understanding its origins and fostering supportive coalitions is crucial. [118]
6.4. Monitoring and Adaptation
Implementation monitoring involves tracking both process and outcome measures. [119] Feedback loops should be designed for quick responses to critical feedback. [120] When making adaptations, it is important to balance staying true to core principles with making necessary peripheral adjustments. [121]
7. Discussion
7.1. Key Findings
This research establishes five central findings. [122] First, mission-driven organizational design is a foundational principle, positioning organizational structure as a dependent variable determined by mission requirements. [22] Second, context-dependent appropriateness characterizes model selection with no universal optimal model. [27] Third, educational continuum fragmentation persists systematically at transitions. [14] Fourth, economic analysis demonstrates that mission-aligned structures generate favorable ROI. [83] Fifth, implementation quality determines outcomes as much as model selection. [16]
7.2. Theoretical and Practical Implications
This framework offers multiple contributions. [123] Theoretically, it positions mission-driven analysis as a core principle, [23] combines organizational theory with implementation science, [11] and illustrates how to systematically translate hub-spoke principles. [12] Practically, it equips library directors with structured frameworks, [7] helps AHS leadership view organizational structure as a strategic choice, [124] and provides educators and researchers with tools for professional development. [125]
7.3. Limitations
The evidence primarily comprises descriptive accounts rather than controlled comparison studies. [6] Publication bias tends to favor success stories. [48] Geographic concentration creates uncertainty about international applicability. [49] Limited economic data necessitate estimation. [8] Nonetheless, systematic synthesis is a notable advancement despite these limitations. [126]
8. Conclusion
8.1. Central Conclusions
Five central conclusions emerge. [127] Mission-driven design must be established as the foundational principle. [22] Context-dependent appropriateness characterizes optimal model selection. [27] Persistent continuum gaps fragment support at educational transitions. [14] Economic analysis reveals that value considerations should drive decisions. [83] Implementation quality often matters more than model selection. [16]
8.2. Recommendations by Stakeholder Group
Library directors should perform mission-oriented organizational analysis using the provided framework. This approach helps position libraries as essential infrastructure aligned with their mission. They should also focus on designing services that support the entire educational continuum, develop implementation capacity before large-scale changes, and seek collaborative solutions when resources are constrained. [7,128]
Academic health system leadership should view the library's organizational structure as a strategic decision that impacts mission success. They should base resource allocation on value creation rather than just minimizing costs, facilitate ongoing support through cross-boundary coordination, allocate sufficient resources for implementation, and assess effectiveness using outcome metrics aligned with institutional priorities. [124,129]
Educators and researchers ought to integrate organizational analysis frameworks into professional training, perform empirical validation studies, create economic valuation techniques, consider international transferability, and support wider organizational scholarship. [125,130]
Professional associations ought to strengthen accreditation standards that promote continuous development, develop resource repositories, lobby for funding policies, broaden workforce development programs, and support international knowledge exchange. [131]
8.3. Call to Action and Final Reflections
Frameworks by themselves do not generate change. Successful implementation demands institutional resolve to strive for organizational excellence with dedication and rigor. An organization's structure reflects its core values. Libraries positioned as strategic assets demonstrate a genuine commitment to evidence-based excellence. Academic health systems dedicated to excellence need to acknowledge libraries as vital institutional resources and allocate appropriate investments [132,133,134,135,136].
References
- Cooper ID, Crum JA. New activities and changing roles of health sciences librarians: a systematic review, 1990-2012. J Med Libr Assoc. 2013;101(4):268-77. [CrossRef]
- Rankin JA, Grefsheim SF, Canto CC. The emerging informationist specialty: a systematic review of the literature. J Med Libr Assoc. 2008;96(3):194-206. [CrossRef]
- Lessick S, Perryman C, Billman BL, Alpi KM, De Groote SL, Babin TD. Academic health sciences libraries and affiliated hospitals: a study of collaboration models. J Med Libr Assoc. 2020;108(2):269-78.
- Sathe NA, Jerome RN, Giuse NB. Librarian-perceived barriers to the implementation of the informationist/information specialist in context role. J Med Libr Assoc. 2007;95(3):270-4. [CrossRef]
- Gore SA, Nordberg JM, Palmer LA, Piorun ME. Trends and gaps in awareness of systematic review methodology: a pilot survey of medical librarians in the northeastern United States. J Med Libr Assoc. 2018;106(4):541-6.
- Gore SA, Epstein BA, Grayson K, Kramer JS, Layton R, Palmer LA, et al. Health sciences librarian research and instruction services in pandemic information environments. J Med Libr Assoc. 2022;110(2):198-209.
- Tooey MJ. Information and Innovation: A Natural Combination for Health Sciences Libraries. J Med Libr Assoc. 2018;106(4):423-9.
- Breathnach R, O'Connor Á. Key Performance Indicators in Irish Hospital Libraries: Developing Outcome-Based Metrics to Support Advocacy and Service Delivery. Evid Based Libr Inf Pract. 2017;12(4):27-44.
- Hamdy H, Anderson MB. The Arabian Gulf University College of Medicine and Medical Sciences: a successful model of a multinational medical school. Acad Med. 2006;81(12):1085-90. [CrossRef]
- Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581-629. [CrossRef]
- Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10:53. [CrossRef]
- Elrod JK, Fortenberry JL Jr. The hub-and-spoke organization design: an avenue for serving patients well. BMC Health Serv Res. 2017;17(Suppl 1):457. [CrossRef]
- Katz SS, Linderman AR, Akers AK, Campion TR Jr. Health Sciences Libraries Advancing Collaborative Clinical Research. J Med Libr Assoc. 2018;106(3):308-16.
- Maggio LA, Tannery NH, Chen HC, ten Cate O, O'Brien B. Evidence-based medicine training in undergraduate medical education: a review and critique of the literature published 2006-2011. Acad Med. 2013;88(7):1022-8.
- Holmboe ES, Sherbino J, Long DM, Swing SR, Frank JR. The role of assessment in competency-based medical education. Med Teach. 2010;32(8):676-82.
- Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care. 1998;7(3):149-58. [CrossRef]
- Wartman SA. Toward a virtuous cycle: the changing face of academic health centers. Acad Med. 2008;83(9):797-9. [CrossRef]
- Eldredge JD, Morley SK, Hendrix IC, Carr MP, Bengtson JD. Library services in the curricula of U.S. nurse practitioner programs. Bull Med Libr Assoc. 2001;89(1):26-33.
- Lappa E. Undertaking an information-needs analysis of the emergency-care physician to inform the development of a digital library at the point of care. Health Info Libr J. 2005;22(2):124-32.
- Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65-76. [CrossRef]
- Michener JL, Yaggy S, Lyn M, Warburton S, Champagne M, Black M, et al. Improving the health of the community: Duke's experience with community engagement. Acad Med. 2008;83(4):408-13. [CrossRef]
- Detlefsen EG. The information behaviors and reflective learning of pre-clinical medical students. J Med Libr Assoc. 2013;101(1):20-30.
- Urquhart C, Yeoman A. Reflective practice and continuing professional development in health library and information services. Health Info Libr J. 2010;27(4):255-64.
- Jabareen Y. Building a conceptual framework: philosophy, definitions, and procedure. Int J Qual Methods. 2009;8(4):49-62. [CrossRef]
- Harvey G, Kitson A. PARIHS revisited: from heuristic to integrated framework for the successful implementation of knowledge into practice. Implement Sci. 2016;11:33. [CrossRef]
- Pfeffer J, Salancik GR. The external control of organizations: a resource dependence perspective. Am Sociol Rev. 1978;23(2):123-33.
- Greenhalgh T, Papoutsi C. Studying complexity in health services research: desperately seeking an overdue paradigm shift. BMC Med. 2018;16(1):95. [CrossRef]
- Sen BA. Defining and measuring effectiveness and productivity in the academic library. Libr Manag. 2014;35(3):200-5.
- Cooke M, Irby DM, O'Brien BC. Educating physicians: a call for reform of medical school and residency. N Engl J Med. 2010;362(14):1339-40.
- Frank JR, Snell LS, Cate OT, Holmboe ES, Carraccio C, Swing SR, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638-45.
- Moses H 3rd, Matheson DH, Cairns-Smith S, George BP, Palisch C, Dorsey ER. The anatomy of medical research: US and international comparisons. JAMA. 2015;313(2):174-89.
- Donabedian A. The quality of care. How can it be assessed? JAMA. 1988;260(12):1743-8.
- Darnell JS, Cahn S, Turnock B, Becker C, Franzel J. Factors associated with state health department engagement in community health improvement. J Public Health Manag Pract. 2013;19(5):432-41.
- Lyon JA, Giuse NB, Williams A, Koonce T, Walden R. A model for training the new bioinformationist. J Med Libr Assoc. 2004;92(2):188-95.
- Koufogiannakis D, Buckingham J, Alibhai A, Rayber D. Impact of librarians in first-year medical and dental student problem-based learning (PBL) groups: a controlled study. Health Info Libr J. 2005;22(3):189-95. [CrossRef]
- Eldredge JD. Evidence-based librarianship: an overview. Bull Med Libr Assoc. 2000;88(4):289-302.
- McGowan J, Hogg W, Campbell C, Rowan M. Just-in-time information improved decision-making in primary care: a randomized controlled trial. PLoS One. 2008;3(11):e3785. [CrossRef]
- Lappa E. Teaching information literacy for evidence-based practice at the medical school of the University of Patras. Health Info Libr J. 2009;26(1):64-8.
- Shaneyfelt T, Baum KD, Bell D, Feldstein D, Houston TK, Kaatz S, et al. Instruments for evaluating education in evidence-based practice: a systematic review. JAMA. 2006;296(9):1116-27.
- Dee C, Blazek R. Information needs of the rural physician: a descriptive study. Bull Med Libr Assoc. 1993;81(3):259-64.
- Tenopir C, King DW, Edwards S, Wu L. Electronic journals and changes in scholarly article seeking and reading patterns. Aslib Proc. 2009;61(1):5-32. [CrossRef]
- Rethlefsen ML, Murad MH, Livingston EH. Engaging medical librarians to improve the quality of review articles. JAMA. 2014;312(10):999-1000. [CrossRef]
- Swinkels JA, Albarqouni L, de Boer A, Borra R, Burger H, Cunningham M, et al. Large-scale systematic review support for guideline developers by health science librarians: a mixed-methods study. J Med Libr Assoc. 2024;112(3):304-14.
- Frooman J. Stakeholder influence strategies. Acad Manage Rev. 1999;24(2):191-205.
- Hillman AJ, Withers MC, Collins BJ. Resource dependence theory: a review. J Manage. 2009;35(6):1404-27. [CrossRef]
- Zucker LG. Institutional theories of organization. Annu Rev Sociol. 1987;13:443-64.
- Federer LM, Lu YL, Joubert DJ. Data literacy training needs of biomedical researchers. J Med Libr Assoc. 2016;104(1):52-7. [CrossRef]
- Rothstein HR, Sutton AJ, Borenstein M. Publication bias in meta-analysis. J Am Stat Assoc. 2006;101(473):318-20.
- Dorsey ER, de Roulet J, Thompson JP, Reminick JI, Thai A, White-Stellato Z, et al. Funding of US biomedical research, 2003-2008. JAMA. 2010;303(2):137-43. [CrossRef]
- Tenopir C, Sandusky RJ, Allard S, Birch B. Research data management services in academic research libraries and perceptions of librarians. Libr Inf Sci Res. 2014;36(2):84-90. [CrossRef]
- Topper LA, Boyce KM, Maggio LA. Leveraging accreditation to integrate sustainable information literacy instruction into the medical school curriculum. J Med Libr Assoc. 2018;106(3):355-63.
- Eisenhardt KM, Graebner ME. Theory building from cases: opportunities and challenges. Acad Manage J. 2007;50(1):25-32. [CrossRef]
- Yin RK. Case study research and applications: design and methods. 6th ed. Thousand Oaks: SAGE; 2018.
- Morgan DL. Pragmatism as a paradigm for social research. Qual Inq. 2014;20(8):1045-53. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. [CrossRef]
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77-101.
- May CR, Johnson M, Finch T. Implementation, context and complexity. Implement Sci. 2016;11:141.
- Davidoff F, Florance V. The informationist: a new health profession? Ann Intern Med. 2000;132(12):996-8. [CrossRef]
- Perry GJ, Kronenfeld MR. Evidence-based practice: a new paradigm brings new opportunities for health sciences librarians. Med Ref Serv Q. 2005;24(4):1-16.
- Swanberg SM, Dennison CC, Farrell A, Machel V, Marton C, O'Brien KK, et al. Integrating Information Literacy and Evidence-based Medicine Content within a New School of Medicine Curriculum. J Med Libr Assoc. 2016;104(2):134-42.
- Williams L, Zipperer L. Improving access to information: librarians and nurses team up for patient safety. Nurs Econ. 2003;21(5):199-201.
- Giuse DA, Williams AM, Giuse NB. Integrating best evidence into patient care: a process facilitated by a seamless integration with information technology. J Med Libr Assoc. 2010;98(3):220-2. [CrossRef]
- Crespo J. Training the health information seeker: quality issues in health information websites. Libr Trends. 2004;53(2):360-74.
- Marshall JG, Morgan JC, Klem ML, Thompson CA, Wells AL. The value of library and information services in patient care: results of a multisite study. J Med Libr Assoc. 2013;101(1):38-46. [CrossRef]
- Carlson J, Kneale R. Embedded librarianship in the research context: navigating new waters. Coll Res Libr News. 2011;72(3):167-70. [CrossRef]
- Kronenfeld MR, Stephenson PL, Nail-Chiwetalu B, Tweed EM, Sauers EL, McLeod TCV, et al. Review for librarians of evidence-based practice in nursing and the allied health professions in the United States. J Med Libr Assoc. 2007;95(4):394-407. [CrossRef]
- Beyer FR, Wright K. Can we prioritise which databases to search? A case study using a systematic review of frozen shoulder management. Health Info Libr J. 2013;30(1):49-58. [CrossRef]
- Ma J, Stahl L, Knotts E. Emerging roles of health information professionals for library and knowledge services in the face of automation. Med Ref Serv Q. 2018;37(3):288-99.
- Banks MA, Cogdill KW, Selden CR, Cahn MA. Complementary competencies: public health and health sciences librarianship. J Med Libr Assoc. 2005;93(4):452-8.
- Williams L, Zipperer L, Muñoz M. Clinical librarian participation in interprofessional education and practice. J Interprof Care. 2019;33(4):430-2.
- Huber JT, Snyder M. Facilitating access to consumer health information: a collaborative approach addressing information overload. J Med Libr Assoc. 2007;95(3):284-92.
- Maggio LA, Leroux TC, Meyer HS, Artino AR Jr. #MedEd: exploring the relationship between altmetrics and traditional measures of dissemination in health professions education. Perspect Med Educ. 2018;7(4):239-47. [CrossRef]
- Giuse NB, Williams AM, Giuse DA. Evolving to meet user needs: case studies of library spaces that support redefined roles of academic health sciences libraries. J Med Libr Assoc. 2013;101(3):171-7.
- Shumaker D, Talley M. Models of embedded librarianship: a research summary. Inf Outlook. 2010;14(1):26-8.
- Morris M, Boruff J, Gore GC. Scoping reviews: establishing the role of the librarian. J Med Libr Assoc. 2016;104(4):346-54.
- Dee C, Stanley EE. Information-seeking behavior of nursing students and clinical nurses: implications for health sciences librarians. J Med Libr Assoc. 2005;93(2):213-22.
- Wagner KC, Briere L, Corrêa JA, Marcotte S, Bouffard AS. Integrating Medical Librarians Into Infectious Disease Consultations: Enhancing Evidence-Based Practice. J Med Libr Assoc. 2024;112(2):223-32.
- Perrier L, Farrell A, Ayala AP, Lightfoot D, Kenny T, Aaronson E, et al. Effects of librarian-provided services in healthcare settings: a systematic review. J Am Med Inform Assoc. 2014;21(6):1118-24. [CrossRef]
- Weightman AL, Williamson J; Library and Information Research Group. The value and impact of information provided through library services for patient care: a systematic review. Health Info Libr J. 2005;22(1):4-25. [CrossRef]
- Fixsen DL, Blase KA, Naoom SF, Wallace F. Core implementation components. Res Soc Work Pract. 2009;19(5):531-40. [CrossRef]
- Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients' care. Lancet. 2003;362(9391):1225-30.
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for implementation research. Implement Sci. 2009;4:50. [CrossRef]
- Berwick DM. Disseminating innovations in health care. JAMA. 2003;289(15):1969-75.
- Ilic D, Maloney S. Methods of teaching medical trainees evidence-based medicine: a systematic review. Med Educ. 2014;48(2):124-35. [CrossRef]
- Guyatt GH, Meade MO, Jaeschke RZ, Cook DJ, Haynes RB. Practitioners of evidence based care. Not all clinicians need to appraise evidence from scratch but all need some skills. BMJ. 2000;320(7240):954-5.
- Straus SE, Richardson WS, Glasziou P, Haynes RB. Evidence-based medicine: how to practice and teach it. 4th ed. Edinburgh: Churchill Livingstone; 2010.
- Burnham E, Peterson EB. Health information literacy: a library case study. Health Info Libr J. 2005;22(2):97-105.
- Dyrbye LN, Thomas MR, Shanafelt TD. Medical student distress: causes, consequences, and proposed solutions. Mayo Clin Proc. 2005;80(12):1613-22. [CrossRef]
- Chen FM, Bauchner H, Burstin H. A call for outcomes research in medical education. Acad Med. 2004;79(10):955-60.
- Kennedy TJ, Regehr G, Baker GR, Lingard LA. Progressive independence in clinical training: a tradition worth defending? Acad Med. 2005;80(10 Suppl):S106-11. [CrossRef]
- Philibert I, Friedmann P, Williams WT; ACGME Work Group on Resident Duty Hours. New requirements for resident duty hours. JAMA. 2002;288(9):1112-4.
- Norcini JJ. Current perspectives in assessment: the assessment of performance at work. Med Educ. 2005;39(9):880-9. [CrossRef]
- Prideaux D. Curriculum design. BMJ. 2003;326(7383):268-70.
- Hunt DP, Haidet P, Coverdale JH, Richards B. The effect of using team learning in an evidence-based medicine course for medical students. Teach Learn Med. 2003;15(2):131-9. [CrossRef]
- Schuers M, Griffon N, Kerdelhué G, Foubert A, Mercier A, Darmoni SJ. Behavior and attitudes of residents and general practitioners in searching for health information. Int J Med Inform. 2016;89:9-14. [CrossRef]
- Murphy SA, Boden C. Benchmarking participation in Canadian health sciences journal clubs. J Med Libr Assoc. 2015;103(1):38-46.
- Davies K. Formulating the evidence based practice question: a review of the frameworks. Evid Based Libr Inf Pract. 2011;6(2):75-80.
- Crumley E, Koufogiannakis D. Developing evidence-based librarianship: practical steps for implementation. Health Info Libr J. 2002;19(2):61-70. [CrossRef]
- Blake L, Ballance D. Teaching evidence-based practice in the hospital and the library: two different groups, one course. Med Ref Serv Q. 2013;32(1):100-10. [CrossRef]
- Rycroft-Malone J, Seers K, Chandler J, Hawkes CA, Crichton N, Allen C, et al. The role of evidence, context, and facilitation in an implementation trial. Implement Sci. 2013;8:28. [CrossRef]
- Concannon TW, Meissner P, Grunbaum JA, McElwee N, Guise JM, Santa J, et al. A new taxonomy for stakeholder engagement in patient-centered outcomes research. J Gen Intern Med. 2012;27(8):985-91. [CrossRef]
- Greenhalgh T, Wieringa S. Is it time to drop the 'knowledge translation' metaphor? A critical literature review. J R Soc Med. 2011;104(12):501-9. [CrossRef]
- Rapport F, Clay-Williams R, Churruca K, Shih P, Hogden A, Braithwaite J. The struggle of translating science into action: foundational concepts of implementation science. J Eval Clin Pract. 2018;24(1):117-26. [CrossRef]
- Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction to implementation science for the non-specialist. BMC Psychol. 2015;3:32. [CrossRef]
- Boaz A, Hanney S, Borst R, O'Shea A, Kok M. How to engage stakeholders in research: design principles to support improvement. Health Res Policy Syst. 2018;16(1):60. [CrossRef]
- Brownson RC, Eyler AA, Harris JK, Moore JB, Tabak RG. Getting the word out: new approaches for disseminating public health science. J Public Health Manag Pract. 2018;24(2):102-11. [CrossRef]
- Nilsen P, Bernhardsson S. Context matters in implementation science: a scoping review of determinant frameworks. BMC Health Serv Res. 2019;19(1):189. [CrossRef]
- Lewis CC, Fischer S, Weiner BJ, Stanick C, Kim M, Martinez RG. Outcomes for implementation science: an enhanced systematic review of instruments. Implement Sci. 2015;10:155. [CrossRef]
- Brehaut JC, Eva KW. Building theories of knowledge translation interventions: use the entire menu of constructs. Implement Sci. 2012;7:114. [CrossRef]
- Stirman SW, Miller CJ, Toder K, Calloway A. Development of a framework and coding system for modifications and adaptations of evidence-based interventions. Implement Sci. 2013;8:65. [CrossRef]
- Ferlie EB, Shortell SM. Improving the quality of health care in the United Kingdom and the United States: a framework for change. Milbank Q. 2001;79(2):281-315. [CrossRef]
- Mendel P, Meredith LS, Schoenbaum M, Sherbourne CD, Wells KB. Interventions in organizational and community context: a framework for building evidence. Adm Policy Ment Health. 2008;35(1-2):21-37. [CrossRef]
- Olswang LB, Prelock PA. Bridging the gap between research and practice: implementation science. J Speech Lang Hear Res. 2015;58(6):S1818-26. [CrossRef]
- Lehoux P, Grimard D, Hivon M, Williams-Jones B. The practice of health technology assessment: what might implementation science bring? Healthc Policy. 2014;9(4):10-4.
- Eccles MP, Mittman BS. Welcome to Implementation Science. Implement Sci. 2006;1:1.
- Wensing M, Grol R. Knowledge translation in health: how implementation science could contribute more. BMC Med. 2019;17(1):88. [CrossRef]
- Sales A, Smith J, Curran G, Kochevar L. Models, strategies, and tools: theory in implementing evidence-based findings into health care practice. J Gen Intern Med. 2006;21(Suppl 2):S43-9.
- Brehaut JC, Colquhoun HL, Eva KW, Carroll K, Sales A, Michie S, et al. Practice feedback interventions: 15 suggestions for optimizing effectiveness. Ann Intern Med. 2016;164(6):435-41.
- Crabtree BF, Nutting PA, Miller WL, Stange KC, Stewart EE, Jaén CR. Summary of the National Demonstration Project and recommendations for the patient-centered medical home. Ann Fam Med. 2010;8(Suppl 1):S80-90. [CrossRef]
- Lewis CC, Klasnja P, Powell BJ, Lyon AR, Tuzzio L, Jones S, et al. From classification to causality: advancing understanding of mechanisms of change in implementation science. Front Public Health. 2018;6:136. [CrossRef]
- Koczwara B, Stover AM, Davies L, Davis MM, Fleisher L, Raber M, et al. Harnessing the synergy between improvement science and implementation science in cancer: a call to action. J Oncol Pract. 2018;14(6):335-40. [CrossRef]
- Schneider KA, Houk KM, Humphreys BL, Cooper ID. Realizing the vision: a 10-year follow-up survey of US academic libraries. J Med Libr Assoc. 2022;110(3):331-45.
- Giuse NB, Huber JT, Giuse DA, Brown RL, Bankowitz RA, Hunt S. Information needs of health care professionals in an AIDS outpatient clinic as determined by chart review. J Am Med Inform Assoc. 1994;1(5):395-403. [CrossRef]
- Shearer BS, Seymour A, Capitani C. Bringing the best of medical librarianship to the patient team. J Med Libr Assoc. 2002;90(1):22-6.
- Tenopir C, Dalton ED, Allard S, Frame M, Pjesivac I, Birch B, et al. Changes in data sharing and data reuse practices and perceptions among scientists worldwide. PLoS One. 2015;10(8):e0134826. [CrossRef]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane handbook for systematic reviews of interventions. 2nd ed. Chichester: John Wiley & Sons; 2019.
- Johnson RB, Onwuegbuzie AJ. Mixed methods research: a research paradigm whose time has come. Educ Res. 2004;33(7):14-26. [CrossRef]
- Trotter RT 2nd. Qualitative research sample design and sample size: resolving and unresolved issues and inferential imperatives. Prev Med. 2012;55(5):398-400. [CrossRef]
- Anderson KM. Organizational complexity and leadership. J Nurs Adm. 2012;42(12):575-9.
- Poll R, Payne P. Impact measures for libraries and information services. Libr Hi Tech. 2006;24(4):547-62. [CrossRef]
- Petticrew M, Roberts H. Systematic reviews in the social sciences: a practical guide. Malden: Blackwell; 2006.
- Schonfeld RC, Long MP. Ithaka S+R US Library Survey 2013. New York: Ithaka S+R; 2014.
- Eskola EL. University students' information seeking behaviour in a changing learning environment. Inf Res. 2005;10(2):paper 215.
- Hallam G, Hiskens A. Challenges to library and information science education in Australia. IFLA J. 2008;34(4):343-51.
- Davidoff F, Haynes B, Sackett D, Smith R. Evidence based medicine: a new journal to help doctors identify the information they need. BMJ. 1995;310(6987):1085-6.
- Grol R, Wensing M, Eccles M, Davis D, editors. Improving patient care: the implementation of change in health care. 2nd ed. Chichester: Wiley-Blackwell; 2013.
Figure 1.
Mission to Structure Translation Framework.
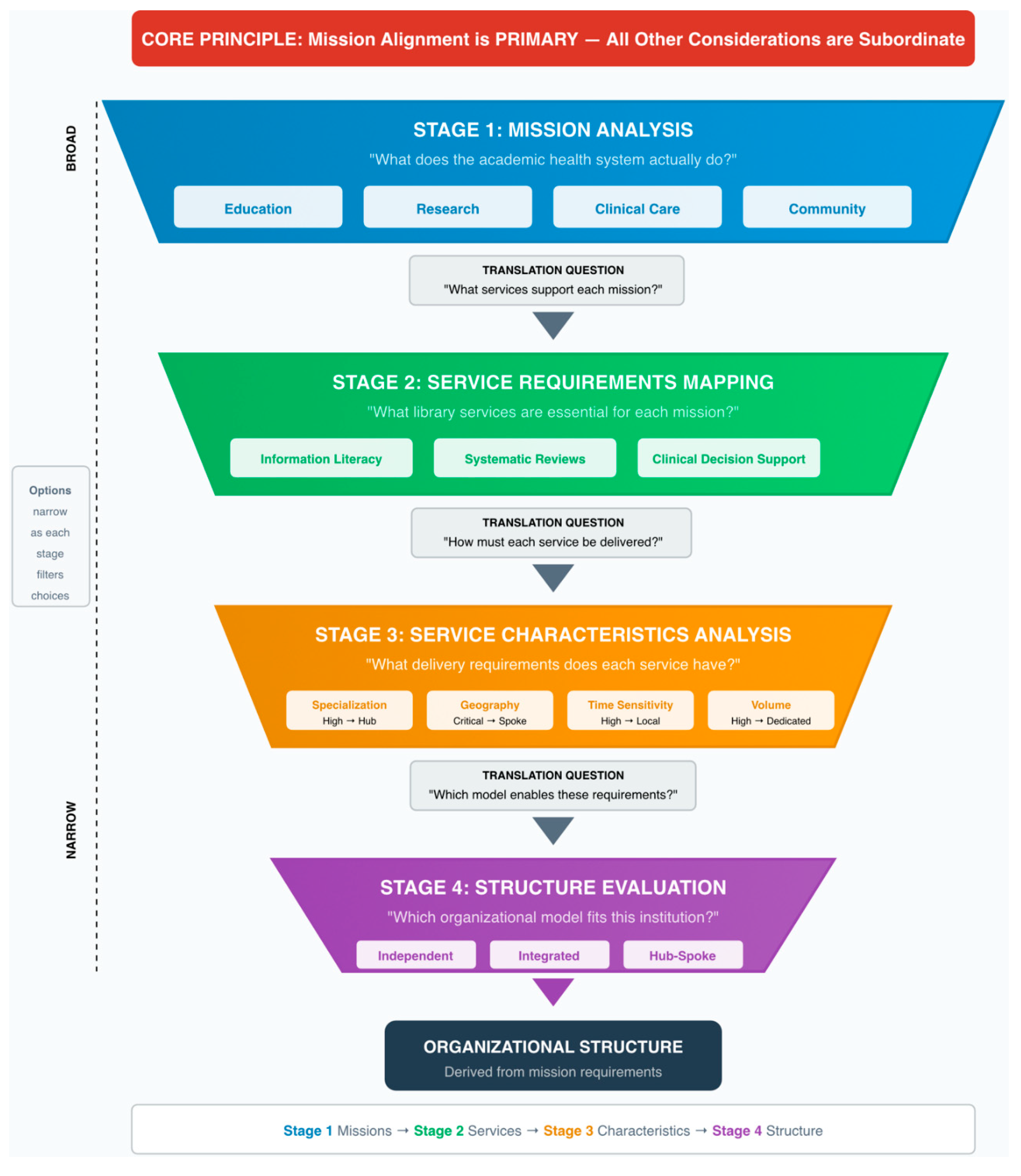
Figure 2.
Hub-Spoke Library Organization – Structure and Flow.
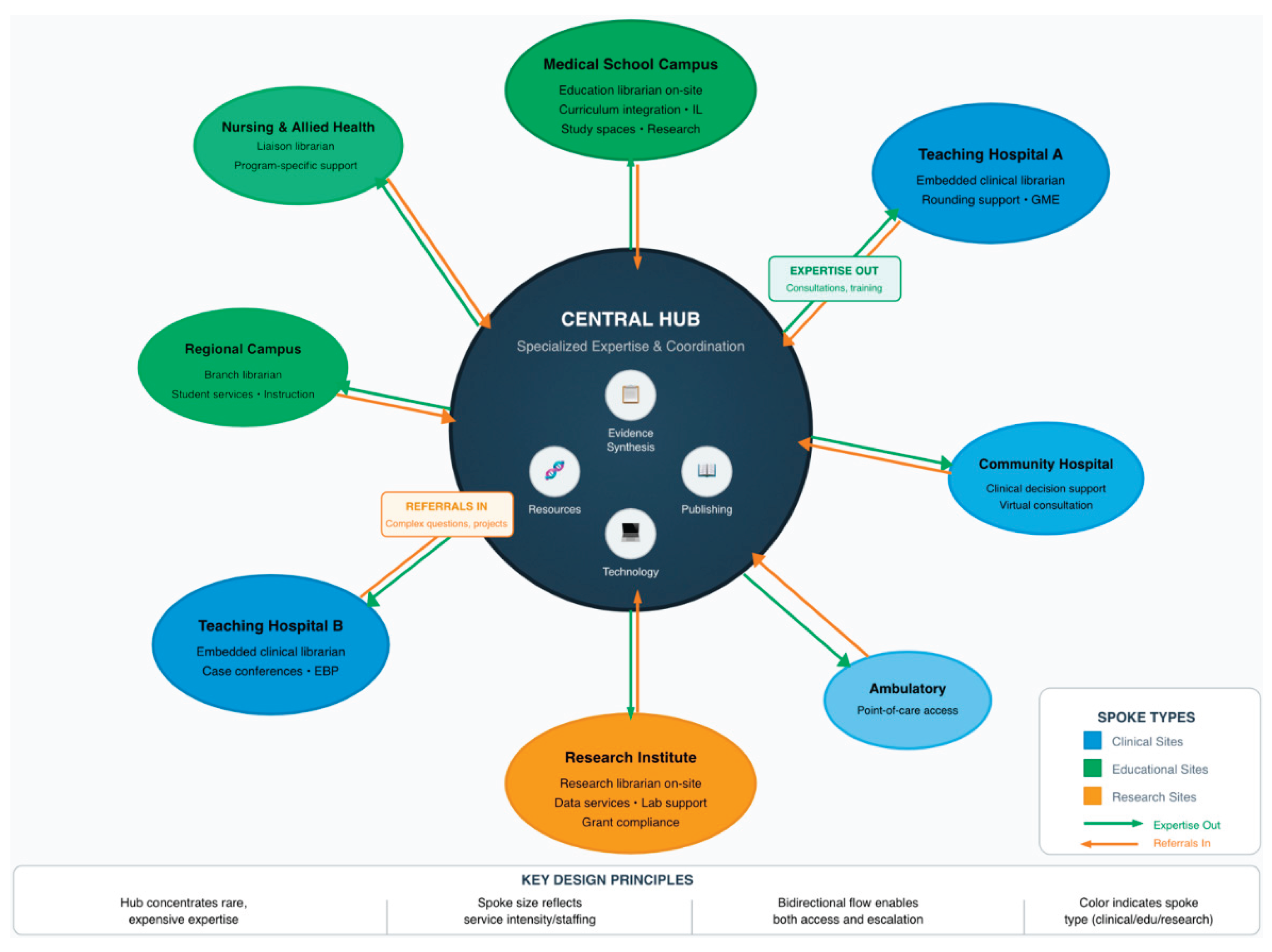
Figure 3.
Educational Continuum Coverage by Organizational Model.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



