
Submitted:
28 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
Background: Young adults with mood and anxiety disorders often remain hamstrung by "brain-fog," headaches, and other bodily complaints even after standard antidepressants or sedatives take the edge off their mood. An inexpensive OTC oral augmentation stack proposed by Cheung (2025)—dextromethorphan for NMDA blockade, low-dose fluoxetine to slow its metabolism, and piracetam to boost AMPA signalling—may reproduce ketamine's rapid neuroplastic effects without an infusion suite.Case: A 25-year-old law student arrived with severe depression (PHQ-9 = 23), generalized anxiety (GAD-7 = 15), daily tension headaches, cramping abdominal pain, episodic breathlessness, and crippling cognitive fog that had already cost her an exam. A sedative‐heavy regimen (risperidone 0.5 mg, alprazolam 0.25 mg prn, lemborexant 1.25 mg, flupentixol/melitracen 1 tablet) eased the physical distress and improved sleep, yet panic and mental slowdown roared back when the new term began.Intervention: In early September the medication plan pivoted to the Cheung Glutamatergic Regimen: fluoxetine 10 mg each morning plus dextromethorphan 30 mg and piracetam 600 mg once daily. Somatic and anxiety symptoms calmed within days, but heavy fatigue and poor concentration lingered until the DXM–piracetam pair was given twice daily.Outcome: Within a week of the dosing change the patient reported a sudden "lights-on" clarity, sustained focus, and return to full study hours. By late November her scores had fallen to PHQ-9 = 15, GAD-7 = 8; headaches and abdominal pain were rare and alprazolam use had nearly stopped.Conclusion: This report suggests that pairing oral NMDA antagonism with AMPA potentiation—especially in a morning-and-evening schedule—can quickly lift refractory cognitive and somatic symptoms where serotonergic and sedative strategies fall short. The approach merits systematic study.
Keywords:
depression
; generalized anxiety
; brain‐fog
; somatic symptoms
; dextromethorphan
; fluoxetine
; piracetam
; CYP2D6 inhibition
; NMDA antagonist
; AMPA potentiator
; ketamine‐class therapy
; oral glutamatergic regimen
; neuroplasticity
; rapid‐acting antidepressant
; treatmentresistant
; young adult case report
; Cheung Glutamatergic Regimen
1. Introduction
In everyday clinical practice, depression and generalized anxiety seldom appear in isolation. They tend to drag along a procession of bodily complaints—headaches, gut pain, breathlessness—and a particularly troublesome companion often called “brain-fog.” Among university students the price is steep: missed classes, failed exams, and the gut-level fear that a hard-won career is slipping away (1). Unfortunately, the agents we still reach for first—the selective serotonin re-uptake inhibitors (SSRIs) and benzodiazepines—have a mixed record in this subgroup; they calm emotional reactivity but leave many patients shackled by pain and cognitive slowdown (2).
Basic science has begun to explain why. Excess drive through N-methyl-D-aspartate (NMDA) receptors seems to lock the brain in an internal alarm state, while weak α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid (AMPA) signalling starves circuits of the plasticity required for clear thinking (3). Intravenous ketamine can flip this balance within hours, yet its cost, monitoring needs, and dissociative side-effects keep it out of reach for most patients. Cheung (4) recently outlined a pocket-sized alternative, a.k.a. “Cheung Glutamatergic Regimen”: combine dextromethorphan (DXM) for the NMDA block, a potent CYP2D6 inhibitor such as fluoxetine to hold DXM in the blood, and the AMPA positive modulator piracetam to propel the downstream glutamate burst.
We describe a 25-year-old law student whose anxiety, depression, and intense somatic pain initially responded only to heavy sedation. When classes resumed, she again collapsed—this time under a blanket of panic attack and cognitive deficits. Switching to the Cheung’s Regimen, and later adding a simple extra morning dose of DXM plus piracetam, not only silenced the bodily alarm but also cleared the mental haze that had threatened her degree.
2. Methods
This single-case report was conducted in a private psychiatry practice (Cheung Ngo Medical) in Tsim Sha Tsui, Hong Kong. From July to November 2025 the patient was seen exclusively by the author-clinician, who carried out all assessments, prescriptions, and follow-up visits.
The patient was seen at our clinic about once a month. At each appointment she completed fresh PHQ-9 and GAD-7 questionnaires; the scores were then discussed in a semi-structured interview that also covered physical symptoms, any compulsive behaviours, school attendance, and day-to-day functioning. No new psychotherapy or additional treatments were introduced during this monitoring period.
Written informed consent for anonymous publication of de-identified information was obtained from the patient’s mother, and the patient herself signed an assent form. All details that could reveal identity have been removed in line with ethical standards for single-case reports.
3. Case Presentation
A 25-year-old female postgraduate law student was first evaluated on 25 July 2025 for disabling anxiety and depression accompanied by tension headaches, episodic breathlessness and cramping abdominal pain that flared each time she stepped onto campus. Motivation had evaporated, insomnia was chronic, and she had already missed an examination, convinced this failure would derail her professional diploma. Psychometric testing confirmed a PHQ-9 of 23 and a GAD-7 of 15. A sedation-centred regimen was started: lemborexant 2.5 mg at half-tablet strength (1.25 mg) each night to restore sleep, alprazolam 0.25 mg once daily for daytime panic, risperidone 0.5 mg nightly to quiet ruminations and a morning tablet of flupentixol/melitracen for mood and somatic tension. Two weeks later she described feeling “quieter inside,” the abdominal pain had eased and the longer stretches of sleep felt restorative, though irritability persisted.
The improvement collapsed when term resumed in early September. A brief campus-triggered panic spell with dizziness was followed by a dense “brain fog” that made it impossible to revise; her GAD-7 returned to 15. On 5 September the strategy shifted to the Cheung glutamatergic combination: fluoxetine 10 mg each morning together with dextromethorphan 30 mg (two 15 mg tablets) and piracetam 600 mg (half of a 1 200 mg tablet) once daily, while the original medications were left in place and alprazolam 0.25 mg kept for breakthroughs. The new cocktail eased anxiety, yet hypersomnia and low drive lingered; she missed two weeks of classes late in October even as headaches and abdominal discomfort stayed muted.
Because cognitive inertia persisted, the glutamatergic agents were titrated at the end of October to twice-daily dosing—dextromethorphan 30 mg and piracetam 600 mg now taken both morning and night. At her follow-up on 28 November she reported that the additional morning dose “switches the lights on,” giving several hours of clear, sustained concentration and finally lifting the mood-related cognitive fog. At that visit she remained on fluoxetine 10 mg each morning, dextromethorphan 30 mg twice daily, piracetam 600 mg twice daily, risperidone 0.5 mg nightly, flupentixol/melitracen one tablet every morning, and a reduced supportive schedule of lemborexant 1.25 mg nocte and alprazolam 0.125 mg only as needed. Scores had settled to a PHQ-9 of 15 and a GAD-7 of 8, somatic complaints were largely subdued, and she had resumed effective study for her forthcoming examinations.
4. Conclusions
The patient’s course draws a clear line between quelling autonomic arousal and restoring neuroplastic capacity. Sedatives—lemborexant, alprazolam, low-dose risperidone—and the older antidepressant blend flupentixol/melitracen quickly helped her sleep and took the edge off her visceral pain. Yet the underlying glutamatergic imbalance remained untouched, so the first spike of academic stress reignited panic and shut down executive function.
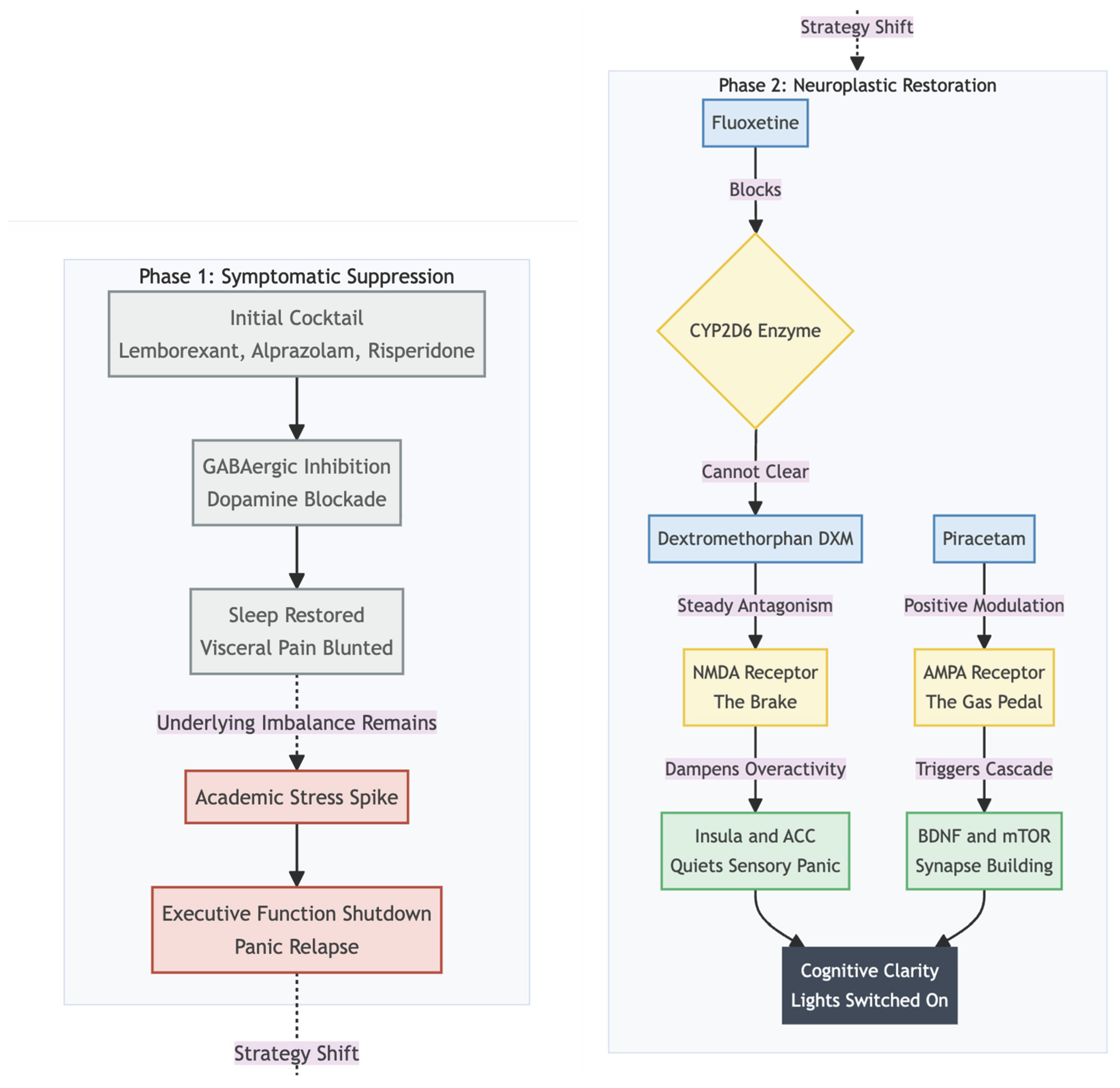
During the second stage of therapy we finally tackled what the sedatives had missed. Because fluoxetine blocks CYP2D6, each dose of dextromethorphan (DXM) lingered longer in the bloodstream, giving a steady NMDA-receptor block that works much like a gentle, oral version of ketamine. That constant dampening of NMDA activity probably quieted the over-reactive insula and anterior cingulate—the brain hubs that can turn ordinary body sensations into pain or panic—so the headaches and stomach cramps eased off for good (5). Yet the fog in her head didn’t truly lift until we added piracetam to her morning pills. Piracetam nudges AMPA receptors into higher gear, boosting the glutamate burst that follows NMDA blockade and setting off a cascade of BDNF release and mTOR-driven synapse building (6). With DXM and piracetam taken twice a day, she finally had both a “brake” on runaway excitation and a “gas pedal” for fresh neural connections—a mix she described as the instant the lights switched back on.
In practical terms, this case lends real-world support to Cheung’s (4) proposal that an inexpensive oral stack can reproduce much of ketamine’s rapid relief without intravenous logistics. It also offers a simple clinical pearl: for patients whose main barrier is cognitive—rather than purely emotional—an extra morning dose of DXM and piracetam may be the key to unlocking productivity. Controlled studies should now test optimal timing, watch for serotonin-syndrome risk, and explore whether adding dietary l-glutamine, as Cheung suggests, further stabilises presynaptic glutamate stores.
Funding
None declared.
Conflicts of Interest
None declared.
References
- McIntyre, R.S.; Cha, D.S.; Soczynska, J.K.; Woldeyohannes, H.O.; Gallaugher, L.A.; Kudlow, P.; Alsuwaidan, M.; Baskaran, A. Cognitive deficits and functional outcomes in major depressive disorder: determinants, substrates, and treatment interventions. Depression Anxiety 2013, 30, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, P. Management of somatic symptom disorder. Dialogues in Clinical Neuroscience 2018, 20, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Aghajanian, G.K. Synaptic dysfunction in depression: potential therapeutic targets. Science 2012, 338, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N. DXM, CYP2D6-Inhibiting Antidepressants, Piracetam, and Glutamine: Proposing a Ketamine-Class Antidepressant Regimen with Existing Drugs. Preprints 2025. [Google Scholar] [CrossRef]
- Bègue, I.; Adams, C.; Stone, J.; Perez, D.L. Structural alterations in functional neurological disorder and related conditions: a software and hardware problem? NeuroImage Clin. 2019, 22, 101798. [Google Scholar] [CrossRef] [PubMed]
- Koike, H.; Iijima, M.; Chaki, S. Involvement of AMPA receptor in both the rapid and sustained antidepressant-like effects of ketamine in animal models of depression. Behav. Brain Res. 2011, 224, 107–111. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



