
Submitted:
30 November 2025
Posted:
02 December 2025
You are already at the latest version
Abstract
Boron Neutron Capture Therapy (BNCT) is a radiotherapeutic modality which couples selective pharmacological delivery of 10B with irradiation by low-energy neutrons to achieve highly localized tumor cell killing. The BNCT therapeutic approach is undergoing rapid evolution driven primarily by advances in compact accelerator-driven neutron-source and associated facility-level nuclear infrastructure. This review examines the key physical and radiobiological principles of BNCT, with emphasis on the current engineering and operational aspects, such as neutron production and moderation, spectral shaping, beam optimization and dosimetric quantification, that critically influence clinical translation. Recent progress in 10B production and enrichment, as well as in strategies for efficient 10B delivery, is also briefly addressed. By tracing the pathway from neutron source to clinical target, the review defines the state of the art in BNCT technology , identifies the main physical and infrastructural challenges and delineates the multidisciplinary advances needed to support widespread clinical implementation of next-generation BNCT systems.
Keywords:
BNCT
; accelerator-based neutron sources
; neutron beam management
; dosimetry
; radiobiology
; neutron-tissue interaction
; 10B delivery
; 10B production
Introduction
Boron Neutron Capture Therapy (BNCT) is a radiotherapeutic approach that exploits the nuclear reaction between 10B isotope and low-energy neutrons. This interaction results in the release of densely ionising α particles and recoiling 7Li nuclei . The high linear energy transfer (LET) of α-particles and of 7Li nuclei , both in the 150-200 keV·µm⁻¹ range, combined with their path lengths of 4–10 μm, comparable to the diameter of a mammalian cell, enables highly localized energy deposition capable of destroying tumor cells at the cellular level [1].
In BNCT, 10B is selectively transported to the tumor tissues by specific pharmacological carriers , consequently the cytotoxic effects are confined to 10B-loaded cells and damages to surrounding healthy tissues are minimized [2]. A schematic representation of the BNCT concept is shown in Figure 1.
The BNCT concept was originally proposed by G. L. Locher in 1936, who suggested the use of neutron capture reactions for selective tumor irradiation [4], whereas first clinical trials were conducted in the early 1950s at the Brookhaven National Laboratory and Massachusetts General Hospital by Sweet and Javid [5].These pioneering attempts used 10B compounds (sodium borate and boric acid) lacking tumor specificity, and reactor-based thermal neutron beams, which resulted in limited therapeutic success due to poor tumor selectivity and considerable irradiation damage to surrounding healthy tissues. In the 1960s the technique has been refined by adopting sodium borocaptate (BSH) as a 10B-carrier and developing intraoperative irradiation methods for enhanced tumor dose localization [6]. Further progress during the 1980s and 1990s included the development of p-boronophenylalanine (BPA) and the application of more energetic neutron beams, which improved tissue penetration and dose distribution [7].
However, it was only during the past two decades that BNCT has experienced a significant resurgence .This renewed interest in a nuclear therapy originally conceived in the mid-20th century has been driven by major advances in 10B production and enrichment, the development of more effective Boron delivery agents and , above all, by the emergence of reliable neutron sources, in primis medical accelerator-based BNCT systems [8,9] It should be noted that the term “accelerator-based BNCT “(AB-BNCT) generally refers to any system that accelerates protons or deuterons onto a target to generate therapeutic neutron beams. This category includes low-energy electrostatic machines and higher-energy linacs, synchrotrons and cyclotrons, these latter being the most widely used neutron sources for BNCT. In the literature, the terms cyclotron-based and accelerator-based BNCT are often used interchangeably, although cyclotron-based systems represent a specific and predominant subset of accelerator-based neutron sources .
The efficacy of BNCT against various tumor types has now been validated through in vitro studies and clinical trials [10,11], demonstrating significant therapeutic outcomes and confirming its potential as an effective treatment modality [3,12,13,14]. Taken together, these recent technological and biological developments, further supported by progress in nanomaterial engineering and image-guided treatments, have now established the scientific and technological basis necessary to transform BNCT from an experimental concept into an applicable therapeutic option in modern oncology [15].
The key scientific and technological aspects of BNCT introduced above are examined in detail in the following sections, where both the physical and biological rationales are outlined. While the biological basis is presented to provide the necessary radiobiological context, this review primarily focuses on the physical aspects, with particular emphasis on the state of the art and the current challenges in nuclear infrastructure and beam management. These factors, together with the critical issue of ensuring a reliable supply of enriched ¹⁰B, play a pivotal role in determining both the feasibility of BNCT clinical translation and its practical implementation.
Physical and Biological Foundation of BNCT
The therapeutic concept of BNCT relies on the selective uptake of 10B-containing compounds by malignant cells , followed by neutron capture reactions that emit short-range, high-LET particles . This results in a highly targeted form of tumor radiotherapy in which energy deposition is confined to 10B-loaded cells. The therapeutic effectiveness of BNCT therefore arises from the combination of physical selectivity , stemming from localized energy release, and biological selectivity, resulting from the Boron preferential accumulation in tumor cells. This dual selectivity constitutes the distinctive physical–biological rationale of BNCT, setting it apart from any other external-beam radiotherapy modalities [2].
The Physical Rationale
Neutron-Tissue Interactions
The therapeutic outcome of BNCT depends primarily on how neutrons interact with 10B and with the various constituents of biological tissues, as these interactions determine the radiobiological impact of the treatment.
The interactions of neutrons with biological tissues strongly depend on their energy. Neutrons are commonly classified as thermal (<0.5 eV), epithermal (~ 0.5 eV–10 keV) and fast (>10 keV), with each energy range exhibiting specific penetration depths and biological effects .
Thermal neutrons traverse biological tissues without significant absorption until they are captured by stable light nuclei such as Hydrogen (1H), Boron (10B) ,Carbon (12C) and Nitrogen (14N). It should be noted that the thermal neutron capture cross section of 1H at a neutron velocity of 2200 m/s is 0.329 barns [16], while that of 14N is approximately 1.7 barns [17]. In addition, neutron capture by 12C can also occur, although with an even lower probability .The thermal neutron capture cross section of 12C at a neutron velocity of 2200 m/s is approximately 0.0034 barns [17], making it negligible compared to that of 1H, 14N, and particularly 10B, which exhibits a thermal neutron capture cross section of about 3837 barns [18].
When a thermal neutron is captured by 10B, an excited 11B* is initially formed :
10B + n 11B* .
The highly unstable 11B* rapidly decays into a 7Li nucleus and an α- particle :
11B* α + 7Li
This last decay proceeds through two channels. In approximately 6% of reactions, 7Li is produced directly in its ground state without accompanying γ-emission. In the remaining 94% of cases, 7Li is generated in an excited state at 0.478 MeV, and subsequently de-excites by emitting a 0.478 MeV γ-ray. Figure 2 illustrates the energy-level scheme of the decay channels associated with the reaction sequence 10B + n 11B* α + 7Li , conventionally expressed in the compact nuclear-reaction notation as 10B (n,α)7Li
The kinetic energies of the reaction products depend on the decay channel. In the predominant channel (94%), the α-particle carries ~1.47 MeV and 7Li ~0.84 MeV. This reaction channel has a Q-value of 2.31 MeV. In the minor channel (6%), the α-particle carries ~1.78 MeV and 7L ~1.01 MeV, resulting in a Q-value of 2.79 MeV. The track lengths of these α and 7Li high-LET particles are approximately 4–5 µm and 9–10 µm , respectively. Such highly localized energy deposition, resulting in dense ionization tracks within the cell and particularly around the nucleus, is primarily responsible for the cytotoxic effect of BNCT.
However, the therapeutic effectiveness of BNCT is governed not only by the microdistribution of 10B within the tumor and the surrounding tissues, but also by the energy spectrum of the incident neutron flux .In effect , from a radiological perspective, neutron–induced effects involve far more than just the 10B (n,α) 7Li reaction .
Thermal neutrons penetrating biological tissues interact with a variety of constituent elements , giving rise to a complex pattern of energy deposition at both microscopic and macroscopic levels. Whereas the 10B (n,α) 7Li reaction contribute significantly to the localized absorbed dose, other nuclear reactions and scattering processes also play a role in the overall radiobiological effect [19]. Among these processes, thermal neutrons primarily undergo elastic scattering with the nuclei of tissue constituents, particularly light elements. During these interactions, neutrons transfer part of their kinetic energy to the target nuclei, moderating their energy and further shaping the spatial distribution of energy deposition until neutron capture becomes probable. This process is particularly effective for 1H , owing to the comparable masses of the neutron and the proton. The resulting recoil protons acquire energies determined by the neutron energy spectrum and the scattering angle, and their relatively high LET contributes significantly to the biological effectiveness of neutron irradiation.
In addition to recoil protons produced by elastic scattering with 1H, neutron interactions with 14N nuclei, mainly through the 14N(n,p)14C reaction, yield additional energetic protons that induce localized ionization events .These emitted protons contribute to the absorbed dose similarly to recoil protons, although with a energy spectrum determined by the reaction kinematics. Nitrogen constitutes roughly 2.5% of air and of biological tissues , so the 14N(n,p)14C channel contributes appreciably to the overall proton dose, particularly in thermalized neutron fields.
Additionally, thermal neutron capture by 1H, following the 1H(n,γ)2H reaction, generates typical 2.223 MeV γ-rays . Even if the capture cross-section of 1H for thermal neutrons is relatively small, in Hydrogen-rich tissues the resulting γ-dose can become relevant and contribute to a low-LET photon dose component across the irradiated volume.
As a result, neutron capture, elastic scattering and charged-particle emission are concurrent processes that give rise to the complex mixed radiation field associated with neutron irradiation of tissue, in which high- and low-LET components coexist and jointly contribute to the overall biological effectiveness. The relative contributions of each interaction process to the secondary radiation dose are mainly dependent on tissue composition , in terms of Hydrogen, Carbon, Oxygen and Nitrogen contents, as well as on geometry of the irradiated region and, most importantly , on the energy spectrum of the incident neutron beam. These factors determine not only the localization and magnitude of the absorbed dose but also the relative biological effectiveness of neutron irradiation.
To ensure therapeutic efficacy and maximize the tumor-to-normal tissue dose, it is necessary not only to optimize 10B distribution, but also to employ strategies related to neutron beam shaping . These include beam collimation to reduce undesired non-boron reactions, beam filtering to enhance the fraction of neutrons within the desidered energy range , and γ-ray control to minimize off-target irradiation. Therefore, precise knowledge and modulation of the neutron energy spectrum are essential to optimize radiation quality and related therapeutic efficacy. This aspect is intrinsically linked to the characteristics of the neutron sources employed in clinical settings.
Neutron Sources and Beam Characteristics
Several types of neutron sources, including reactor- and accelerator-based systems, have been developed to produce neutrons with fluxes, energy spectra (thermal, epithermal, fast) and beam characteristics suitable for practical implementation of BNCT [20].
Until the last decade, BNCT relied primarily on thermal neutrons generated by nuclear research reactors [21]. Regarding the current status of reactor-based neutron sources, it is to be noted that, while many reactors historically used for BNCT have been decommissioned or repurposed, the few facilities still in operation continue to play a key role in both clinical treatments and medical research, focusing on the optimization of beam characteristics, dosimetry, and 10B delivery.
However, the low energy of the thermal neutrons (E < 0.5 eV) limits tissue penetration depth, restricting the therapeutic effectiveness mainly to superficial tumors, such as melanoma. To overcome this limitation and increase the penetration depth , the use of epithermal neutrons has been proposed. Epithermal neutrons can penetrate several centimeters into biological tissue , gradually losing energy through successive scattering processes and slowing down to the thermal range where neutron capture becomes effective. This moderation process results in a more deep and uniform distribution of neutrons within the target region.
The enhanced treatment depth and therapeutic efficacy achievable using epithermal neutrons have therefore established them as the preferred option in BNCT . Accordingly, efforts are presently directed towards the development of advanced cyclotron- or accelerator-based epithermal neutron sources (C-BENS), optimized to effectively target previously untreatable deep-seated tumors [22,23].
To accurately assess the characteristics of an accelerator-based neutron source for BNCT and to predict its therapeutic effects, beyond experimental studies also Monte Carlo (MC) simulations are being employed . In particular particle and heavy ion transport MC codes enable to model a wide range of particle-induced nuclear reactions [24].
Based on these studies , a further promising step toward the broader clinical implementation of BNCT is provided by the emergence of compact , hospital-compatible systems capable of delivering epithermal neutron fluxes and energy distributions appropriate for triggering the ¹⁰B(n,α)⁷Li reaction [25,26] . The clinical adoption of epithermal neutron sources suitable for installation within hospital environments reduces dependence on large research reactors and, by enhancing BNCT accessibility for a broader patient population, represents a critical step toward establishing BNCT as a practical therapeutic modality. Compared with large reactors, the compact accelerator-based sources offer additional advantages, including a smaller footprint, lower costs, and reduced regulatory constraints [15].
These cyclotrons or accelerators (radio-frequency quadrupole , drift tube linac, tandem and single-ended systems) produce neutrons through proton-induced nuclear reactions, typically 9Be(p,n)9B or 7Li(p,n)7Be [20]. A distinctive approach to neutron production is provided by low-energy electrostatic quadrupole accelerators, such as the one developed in Argentina, where neutrons are generated via the 9Be(d,n)10B or the 13C(d,n)14N reaction [27].
In all these infrastructures, the resulting neutron spectrum is subsequently moderated, filtered, and collimated by a proper Beam Shaping Assembly (BSA) to achieve an epithermal energy range while reducing unwanted fast-neutron and γ-ray components [28,29]. The general scheme of a typical accelerator-based BNCT system is shown in Figure 3.
According to the International Atomic Energy Agency (IAEA) , in 2023 the 11 Member States hosted 20 accelerator-based BNCT facilities at various stages of planning or routine operation [15]. Presently, about 26 accelerator-based BNCT projects have been reported, of which 15 focus on clinical applications and 11 on research. These initiatives are primarily concentrated in Asia (Japan, South Korea, China) and Europe, with Argentina hosting the first facility in the Americas [27].
Regarding Europe, Neutron Therapeutics and Helsinki University Hospital announced on 16 May 2025 that they have successfully treated the first cancer patients in a European hospital with accelerator-based BNCT [30]. Meanwhile , the Italian Government has approved the ANTHEM project, funded within the Next Generation EU initiatives, for the realization in Italy of an innovative continuous-wave RFQ accelerator capable of producing a 30 mA, 5 MeV proton beam impinging on a 7Be-target. The resulting epithermal neutrons, with a flux of 109 n/cm2 s, will have characteristics suitable for the treatment of deep tumors [31].
It should be noted that , in addition to neutron sources specifically developed for BNCT, several facilities originally designed for other purposes, from industrial applications to nuclear cross-section measurements, offer promising capabilities also for BNCT . A notable example is the vacuum-insulated tandem accelerator (VITA) at the Budker Institute (Russia), where proton or deuteron beams impinging on a 7Li target produce neutron intensities typically unattainable in conventional BNCT setups [32].
Neutron Moderation and Energy Spectrum
The efficient and safe clinical application of BNCT requires careful optimization of the BSA, a key component of any accelerator-based system. The BSA , positioned between the neutron source and the irradiation field, not only shapes, filters, and collimates the neutron beam but also provides essential shielding. It should be noted that the neutron energies and their classification are measured at the BSA outlet. Beyond the production of a neutron spectrum suitable for clinical applications, the adoption of adequate safety measures is indeed required to ensure protection of both patients and healthcare staff . Additional critical considerations are the thermal load and cooling of neutron targets. In cyclotron- or other accelerator-based BNCT systems, high-power proton beams deposit substantial energy in the target, potentially leading to overheating, material damage, and reduced neutron production yield. Efficient target cooling is therefore crucial to maintain a stable neutron flux and prevent thermal stresses during BNCT treatments. Figure 4 depicts a MC–modeled prototype BSA, highlighting the various components of the beam shaping assembly and the additional shielding.
Efforts to maximize epithermal neutron intensity while reducing thermal and fast neutron contamination started with Bleuel et al. [34], who investigated the ⁷Li(p,n)⁷Be reaction, compared moderator materials for shaping an epithermal spectrum, and modeled neutron transport and dose distributions using Monte Carlo MCNP code MCNP. Since then, MC simulations have become indispensable tools for designing BSA and for predicting and optimizing neutron spectra, target configurations, dose distributions and shielding requirements essential for the development and validation of clinical accelerator-based BNCT systems.
The 2003 study by Yonai et al. has been a key reference for the development of cyclotron-based epithermal neutron sources based on the ⁹Be(p,n)⁹B reaction and paved the way for the design and realization of the C-BENS (Cyclotron-Based Epithermal Neutron Source) project [35].
Following these pioneering study, subsequent investigations have progressively focused on optimizing dose distributions and clinical applicability [36].
In 2021 systematic studies were conducted to evaluate the impact of the maximum epithermal neutron energy on 10B capture rates and the resulting dose distribution in head phantoms [37]. MC simulations highlighted a significant influence of the upper energy limit of the epithermal spectrum on 10B capture rates and dose composition at different depths, demonstrating the critical importance of spectral optimization for improving therapeutic efficacy .
Detailed neutronics analyses performed at the accelerator-based BNCT source of Nagoya University showed that introducing a double-layer collimator for a 30 MeV cyclotron BNCT neutron source provided significant advantages in beam shaping [33]. The resulting epithermal neutron flux reached ~1.2 × 10⁹ n/cm²·s. MC simulations indicated a very low thermal-to-epithermal ratio, with the thermal neutron flux negligible compared to the epithermal flux,and a γ-dose per epithermal neutron flux of approximately 1.5 × 10⁻¹³ Gy·cm²/n [33]. The quantitative beam parameters reported in this study have become key benchmarks for comparing different systems and for driving the clinical implementation of accelerator-based BNCT.
During the same years, in vitro studies carried out at the Kyoto University experimentally validated the clinical applicability of the epithermal neutrons spectra “free in air” at the BSA exit of the C-BENS reactor, demonstrating the positive biological effectiveness of this neutron beam [38] .
The progressive advancements in beam shaping strategies over the years have provided a solid baseline for the design of innovative facilities from which different types of neutron can be extracted . A recent example is reported in [39], where a proper configuration of both the target and the moderator enabled to obtain a thermal neutron port and an epithermal neutron port (fluxes up to ~9×10⁹ n/cm²·s ) from a single compact accelerator-driven neutron source. The characteristics of the in-air beam at both ports meet the IAEA specifications for both epithermal and thermal BNCT radiation fields. By providing thermal fluxes that reach their maximum at the surface and epithermal fluxes that reach their maximum at a depth of about 3 cm in a head phantom, such configuration makes it possible to treat tumors located at different tissue depths.
A similar conceptual approach has been adopted by Schmidt et al.[40], who used the MC code PHITS to simulate a series of target–moderator–reflector (TMR) configurations for epithermal and fast neutron extraction channels within the High Brilliance Neutron Source (HBS) project. A total of 450 combinations of pre-moderator and moderator materials with various thicknesses have been analyzed. For the 96 Hz station with a 167 µs proton pulse width, the average neutron fluxes achieved were approximately ~9×10⁹ n/cm²·s for the epithermal and ~2×10¹⁰ n/cm²·s for the fast neutron channels. These studies demonstrate that epithermal neutrons can be effectively generated even in systems primarily designed for alternative purposes, such as the HBS. By optimizing the TMR configurations and implementing distinct extraction channels, the HBS facility can deliver neutron beams with tailored energy spectra, encompassing in this case both epithermal and fast neutron ranges.
Dosimetry in the BNCT radiation field
Another key aspect, closely related to the neutron energy spectra and to the complex BNCT radiation field , is the evaluation of dose distribution.
In radiation protection and dosimetry the quantitative assessment of the total equivalent dose requires determining either the Radiation Quality factor (Q) or, according to the International Commission on Radiological Protection (ICRP) recommendations, the standardized Radiation Weighting factor (WR) that replaces Q, together with the Relative Biological Effectiveness (RBE) [41,42]. The RBE factor is an experimentally derived ratio between the dose of a given radiation to that of photon radiation required to produce the same biological effect [43] .
Due to its dependence on both the biological systems and radiation characteristics , the RBE factor exhibits a marked variability. Even within the thermal neutron range, studies on cell survival/ proliferation have demonstrated a pronounced dependence of RBE on tissue or cell line as well as on neutron energy spectrum [44].
In BNCT, the situation is further complicated because the absorbed dose results not only from the high-LET α-particles and 7Li nuclei produced by the primary 10B neutron capture, but also from the complex radiation field, consisting of thermal/epithermal/fast neutrons, of recoil protons and of γ-rays, that collectively contribute to the secondary radiation dose [19,45].
Since the radiobiological effects of the secondary radiations differ substantially from the therapeutic impact of the 10B capture reaction, accurately assessing the biologically effective dose in the complex BNCT radiation field requires correcting the physically measured doses not only by the RBE factor but , more significantly, by the Compound Biological Effectiveness (CBE) factor. The CBE factor accounts for the contributions of all radiation components, each weighted by an appropriate RBE. Overall, it reflects the combined influence of the specific ¹⁰B carrier, its resulting intracellular distribution, the tissue’s biological response, and the localized energy deposition from the ¹⁰B(n,α)⁷Li reaction. Representative measured and modeled values of RBE and CBE for various tissues and ¹⁰B compounds can be found in [46,47] . Recently, a microdosimetric study based on Monte Carlo track-structure simulations updated the ionization cross-sections for Li and subsequently verified the ranges and stopping powers of 7Li, α-particles, and protons in BNCT [48].
To express BNCT mixed-field doses in terms of an equivalent photon dose, in the past has been proposed the “photon isoeffective dose” formalism, based on experimental dose–response relationships in human and animal models [49]. Subsequent studies have simplified this formalism by introducing dose-independent weighting factors, which facilitate biological dose evaluation and practical application in treatment planning [44]. This groundwork allowed the isoeffective approach to be further refined and biologically validated [50]. More recently, Postuma et al. applied the isoeffective dose formalism to compare BNCT with carbon-ion therapy within a unified dosimetric framework , highlighting its utility for predicting clinical outcomes [51].
In parallel with these modelling approaches, experimental investigations have also advanced toward a deeper understanding of the microscopic dose deposition in BNCT . A dosimetry study on accelerator-based BNCT has introduced experimental frameworks that decompose the total absorbed dose into its individual components and emphasize the essential role of the weighting factors in estimating the biologically effective dose [19]. A subsequent approach has involved detailed microdosimetric measurements at different Boron concentrations using tissue-equivalent proportional counters [52]. By developing a specific procedure to isolate the contribution of 10B neutron capture from the mixed-field radiation , this work made it possible to realistically determine the proportional relationship between microdosimetric dose enhancement and 10B content.
Since accurate dosimetry represents a key requiremen in BNCT, Monte Carlo–based computational modeling has become an essential tool to estimate spatial dose distributions and optimize neutron beam parameters. MC transport codes such as MCNP and GEANT4 are typically used to simulate the complex interactions of neutrons and secondary radiation within tissue-equivalent phantoms or patient geometries. These simulations account for all relevant interaction channels, including elastic and inelastic scattering leading to recoil protons, neutron capture reactions accompanied by γ- emission (e.g.,1H(n,γ)2H and other capture events ), and the production of secondary charged-particle from (n,x) reactions, such as 14N(n,p)14C, occurring in the presence of specific elements .The contributions of all these interactions to the resulting dose distributions in tissues can thus be accurately determined, and the biologically effective dose evaluated from the simulated physical dose by applying the appropriate RBE and CBE correction factors. Following this approach, the biologically weighted dose distribution obtained through MC–based dosimetry provides a highly realistic estimation of the dose deposited in patient tissues [53].
It should be noted that MC modelling, particularly when integrated with patient-specific imaging modalities such as Positron Emission Tomography (PET), Single Photon Emission Computed Tomography (SPECT) and Magnetic Resonance Imaging (MRI), offers advanced capabilities for quantitative dose assessment. This combined approach enables a more realistic evaluation of dose distributions than conventional methods, while image-guided BNCT planning facilitates dose optimization and delivery verification, enhancing tumor targeting and radiological safety.
The Biological Rationale
Mechanisms of DNA Damage and Cell Killing
Following neutron capture by 10B nuclei via the ¹⁰B(n,α)⁷Li reaction, the emitted high-LET α-particles (~ 150 keV·µm⁻¹ ) and 7Li nuclei (~ 175 keV·µm⁻¹) traverse the intracellular environment with path lengths of 4–10 μm , comparable to the diameter of a single cell.
The densely ionizing reaction fragments produce highly localized energy deposition, causing double-strand breaks (DSBs), single-strand breaks (SSBs), base damage and DNA–protein crosslinks in close spatial proximity, collectively resulting in complex/clustered DNA damage (CDD), defined as two or more lesions occurring within one or two helical turns of the DNA [54].
Depending on the extent and spatial distribution of such DNA damage, cells may undergo apoptosis or necrosis , whereas the high-LET energy can also compromise other critical cellular structures, such as membranes and mitochondria [3]. Additionally, the mixed high-LET/low-LET radiation field to which cells are exposed and the associated BNCT secondary radiation, induce further damage. This enhanced cytotoxicity , not observed with low-LET X-rays or γ-rays [55], triggers cell death pathways and is at the basis of the biological effectiveness of BNCT [56], even if the unevenly distributed secondary radiation is at least partly responsible for unwanted effects, such as necrosis of the surrounding normal tissue [57].
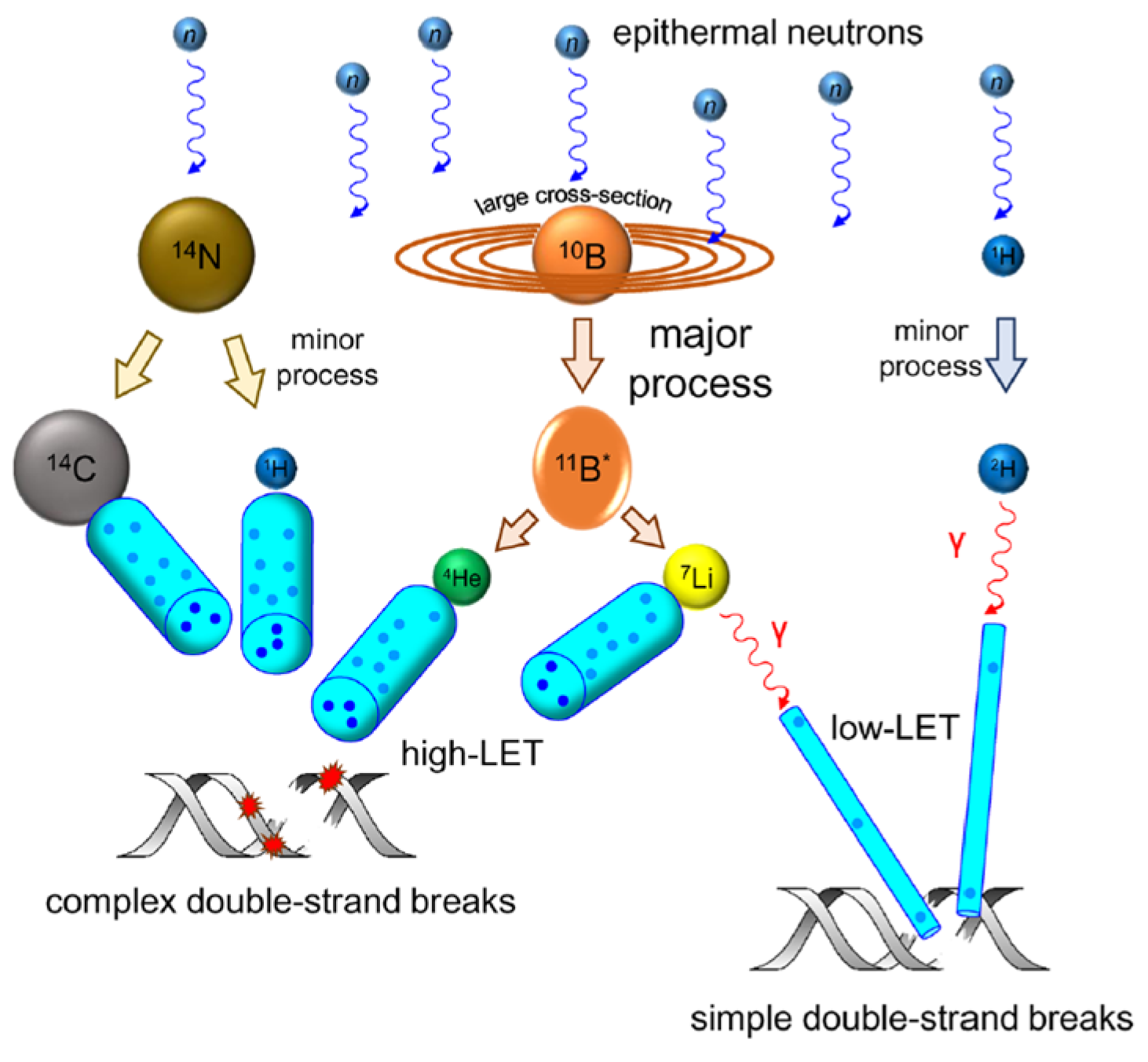
Figure 5 illustrates the nuclear reactions, ionization processes and the subsequent DNA damage occurring during BNCT, highlighting the progression of interactions from radiation deposition to cellular effects.
Overall, to fully exploit the BNCT therapeutic potential, 10B must be delivered with high spatial precision at both the cellular and subcellular levels, since the microscopic dose distribution critically determines the extent of cell kill. This requirement highlights the importance of strategies that specifically target Boron to tumor cells and their subcellular compartments. Ultimately, efficient boron delivery defines the radiobiological impact and therapeutic outcome of BNCT.
Boron Delivering strategies
While the physical efficacy of BNCT is determined by neutron interactions with 10B and tissue constituents , from a biological point of view the effectiveness in destroying tumor cells while largely sparing healthy cells depends on achieving an adequate accumulation of 10B within the tumor . In this view clinically effective treatments require the administration of boronated compounds that exhibit both spatial selectivity (high tumor-to-normal tissue uptake ratio) and temporal selectivity (long retention in tumor tissue and rapid clearance from normal tissue) [1].
The conversion of Boron into chemical forms suitable as delivery agents, along with the control of impurities that may influence toxicity or pharmacokinetics, represent a critical task . The two established Boron-carriers currently used in clinical trials, namely boronophenylalanine (BPA) and sodium borocaptate (BSH), exhibit significant limitations in terms of tumor selectivity and pharmacokinetic behavior [58]. Biopharmaceutical research is now focusing on next-generation delivery systems that, although still experimental, show considerable promise.
In particular, recent advances in nanomaterial engineering have expanded the range of strategies available for boron delivery in BNCT [59]. Various nanosized systems, such as boron carbide (B₄C) nanoparticles [60,61], liposomes [62], dendrimers [63] and polymeric nanocarriers [64] have been investigate to enhance Boron delivery efficiency, tumor selectivity and biocompatibility.
Surface functionalization with antibodies [59], peptides [65,66] or aptamers [67], has been shown to enable selective tumor targeting, to prolong circulation times within tumor tissues, and to allow a tunable Boron release [68] . Moreover, multifunctional delivery agents [69] have opened the way for theranostic applications by combining BNCT with imaging modalities such as PET, SPECT, or MRI. As demonstrated in recent studies , these advanced platforms enable real-time treatment monitoring [70,71].
Standardized protocols for the in vitro and in vivo evaluation of boron agents, such as those proposed by Hattori et al. [72] provide now a robust framework for comparing the performance of different delivery systems and optimizing their design for clinical application. However, despite encouraging preclinical results, significant challenges remain regarding long-term biodistribution, clearance mechanisms and potential systemic toxicity [73].
Production and Processing of Enriched ¹⁰B
In addition to neutron field characterization and dosimetry, the availability of enriched ¹⁰B is another critical factor in BNCT . This section outlines its production and processing, which provide the foundation for preparing the 10B isotope in forms suitable for therapeutic delivery, and bridge the physical rationale with subsequent biological applications.
Since natural Boron contains only about 19 at% ¹⁰B, the production of isotopically enriched ¹⁰B is a prerequisite for achieving the purity required for predictable and reliable neutron capture reactions, as demanded by BNCT and other neutron-based scientific and industrial applications. However, ¹⁰B enrichment is highly energy-intensive and technologically complex, so its supply is often limited by industrial capacity and geopolitical factors. Furthermore, also high chemical purity is necessary to ensure spatial homogeneity, dose predictability and compliance with regulatory standards in clinical use of Boron .
Historically , industrial ¹⁰B enrichment has relied on chemical exchange and low-temperature distillation of boron trifluoride (BFT) . Such processes are based on small equilibrium isotope effects between gaseous and liquid donor compounds to progressively concentrate ¹⁰B through multistage separation, as exemplified by the dimethyl-ether·BF₃ exchange/distillation cascade [74]. This methodology, offering a practical combination of acceptable separation factors and scalability, provided the foundation for large-scale industrial production. A comprehensive review of the methods for ¹⁰B separation was published in 2010, summarizing both the historical development of chemical-exchange processes and the introduction of new donor compounds with improved separation factors [75].
Subsequent developments have further refined operational parameters, column configurations and material choices , leading to an enhancement of enrichment efficiency and of long-term process stability . Building upon the conventional BF₃-based exchange–distillation systems, Li [76] experimented 10B separation via a chemical exchange reaction in a benzene–ether–boron trifluoride system, whereas recent research has focused on process intensification through a microchannel distillation technology. Tang et al. [77] designed a microchannel apparatus for exchange-chemical-distillation and demonstrated that micro-structured contactors can significantly increase mass transfer efficiency, enabling a more energy-efficient isotopic separation process. This approach can be particularly advantageous in applications where gas handling must be minimized or where seamless integration with downstream chemical processes is needed . Alternative liquid–liquid chemical-exchange approaches that avoid the use of toxic BF3 have been described in [78] and further developed by Ivanov et al. [79]. In this latter study, the systematic experimental modeling of the isotopic exchange kinetics demonstrated an enhanced 10B enrichment through optimized phase composition and reaction conditions, thus providing a safer and potentially scalable alternative to traditional BF₃-based processes.
The ion-exchange chromatography, a different, more industrially sustainable route to 10B isotope separation, had been early demonstrated using weakly basic anion-exchange resins [80]. Subsequent developments have further improved the chromatographic process through the use of specialized resins, confirming it as a less energy-intensive and promising method for large-scale industrial application [81]. A novel method of isotope separation based on liquid solution-centrifugation has also been proposed [82]. Although still under experimental investigation, liquid solution-centrifugation represents an interesting and less conventional approach, offering potential applicability to a wide range of elements and yielding large separation factors.
Much more selective are the historical electromagnetic and photochemical isotopic separation techniques, which demonstrated the feasibility of achieving high isotopic purity on a limited, small-scale basis. Electromagnetic separation based on mass-dependent ion trajectories in magnetic fields was early employed by the Manhattan Project for Uranium enrichment .In the 1980s was demonstrated the potential of photochemical methods for isotope separation through wavelength-specific excitation of molecular species via laser-induced reactions [83]. In those years , laser-assisted isotope separation and other photochemical methods have been developed to exploit isotope-specific optical transitions in vapor-phase Boron halides [84,85].
A recently published paper provides the most comprehensive and up-to-date review of laser isotope separation (LIS) for Boron [86]. This outstanding paper analyzes the underlying physicochemical mechanisms, summarizes key experimental achievements and critically assesses the technological feasibility and limitations of LIS approaches for Boron isotopes production. The review outlines that, despite their intrinsically high isotopic selectivity, laser-based separation techniques remain largely confined to research laboratories or pilot-scale demonstrations. Their broader deployment is still hindered by significant technical complexity, substantial energy constraits and challenges associated with scaling-up the processes.
While laser-based isotope separation techniques do not appear promising in terms of industrial scalability, recent institutional and media reports from China , even if not yet substantiated by peer-reviewed scientific publications , have described alternative routes for 10B enrichment. In particular, the China Institute of Atomic Energy (CIAE), under the China National Nuclear Corporation (CNNC), has reported an innovative “low-temperature distillation process” that enables the stable and continuous production of high-purity ¹⁰B compounds, achieving enrichment levels up to approximately 70%. The research effort, led by Prof. Hu Shilin (Chinese Academy of Engineering), has been presented as a significant step toward the realization of large-scale 10B production [87,88].
The strong international interest and worlwide ongoing efforts to enhance the production of high-purity 10B stem from the fact that, beyond its radiological importance, the wider availability of this critical isotope is also of substantial engineering significance. While enriched 10B is indispensable for BNCT , it is equally essential for nuclear reactor safety systems, where 10B-containing compounds are employed for neutron absorption, reactivity control, and emergency shutdown. In nuclear power plants, the use of 10B-enriched boric acid has been shown to improve overall reactor safety margins and operational efficiency [89].
Closing Remarks
The extraordinary biological effectiveness of BNCT, derived from the synergistic interplay between selective 10B accumulation and the microdosimetric signature of the 10B(n,α)7Li reaction, provides a key therapeutic advantage. However, despite substantial progress, BNCT still remains at a transitional stage between experimental innovation and large-scale clinical adoption.
From a biological perspective, the emergence of novel 10B carriers , such as engineered nanomaterials, is enabling the development of highly selective Boron delivery systems with favorable pharmacokinetics. Moreover, the design of innovative multifunctional agents is paving the way for platforms supporting image-guided, real-time–monitored treatments. Recent results indicate that the enhanced therapeutic precision and the resulting meaningful local tumor control, achieved with a tolerable toxicity level , are establishing a solid radiobiological foundation for translating BNCT from a promising modality into clinically impactful applications.
Nevertheless, treatment reproducibility continues to be constrained by uncertainties in 10B biodistribution at the cellular and subcellular scales, which directly affect dose accuracy. Owing to the complex mixed radiation field produced during neutron irradiation, BNCT dosimetry is inherently more challenging than conventional physical dose calculations. This underscores the need for standardized experimental protocols and advanced computational models capable of accurately assessing the relative biological effectiveness (RBE) and the compound biological effectiveness (CBE), radiobiological parameters essential for improving dosimetric precision and reducing uncertainty in dose–effect relationships.
Although biological advances significantly contribute to treatment optimization, the most transformative innovations for broader BNCT implementation and for its transition toward routine clinical practice, will stem from the widespread adoption of compact, hospital-compatible accelerator-based neutron sources.
The primary technological challenge is to engineer nuclear infrastructures capable of delivering clinically relevant neutron fluxes with tunable spectral characteristics, thereby optimizing dose distributions while minimizing beam contamination. Additional technological requirements include the ability to generate, using the same facility, different neutron spectra - thermal, epithermal, and fast - thus providing a multifunctional platform for both medical and industrial applications. The achievement of neutron beams with well-defined spectral shapes and the evolution toward such multifunctional platforms will require major advancements in beam-shaping assembly (BSA) design as well as precise operational strategies for moderating, filtering, and collimating neutrons emitted from primary sources. These developments needs the strong support of computational tools, particularly Monte Carlo simulations, which, beyond their essential role in dose distribution analysis, dosimetry, and treatment planning, are also critical for facility design, neutron spectrum modeling and shielding optimization.
Beyond radiobiological and technological challenges, additional considerations must be taken into account when envisioning BNCT within routine clinical workflows. Among the numerous operational, logistical, and socio-economic factors, encompassing radiation safety, equipment costs, infrastructure maintenance and regulatory approvals, one of the most critical is the establishment of reliable supply chains and robust purification procedures for producing medical-grade enriched 10B.
Ultimately, the successful integration of BNCT into standard clinical practice will depend on the combination of multiple interrelated scientific and technological advancements, spanning pharmacology, neutron-source engineering, 10B production, and nanomaterial design. Only through coordinated progress across these domains can BNCT fully realize its therapeutic potential and evolve into a mature, widely accessible treatment modality.
Although these challenges may seem to pose formidable barriers to large-scale implementation, the presence of several BNCT facilities, either operational and already treating patients or under development in multiple countries, demonstrates that this therapeutic option is far more than a purely conceptual goal and that its translation into routine clinical practice is indeed feasible.
As recent examples have shown, realizing the full therapeutic impact of BNCT in modern oncology requires overcoming not only scientific and technological hurdles but also economic and regulatory constraints. From this perspective, the future progress of BNCT, a therapeutic strategy intrinsically grounded in nuclear physics, radiobiology, chemistry, and personalized nanomedicine, will critically depend on fostering and effectively sustaining interdisciplinary and international collaborations, as well as on training highly skilled multidisciplinary teams capable of integrating these diverse fields into coherent clinical programs.
References
- H. He, J. Li, P. Jiang, S. Tian, H. Wang, R. Fan, J. Liu, Y. Yang, Z. Liu, J. Wang. The basis and advances in clinical application of boron neutron capture therapy. Radiat. Oncol. 16, 216 (2021). [CrossRef]
- A. Monti Hughes, N. Hu. Optimizing boron neutron capture therapy (BNCT) to treat cancer: an updated review on the latest developments on boron compounds and strategies. Cancers 15, 4091 (2023). [CrossRef]
- L.D. Punshon, M.R. Fabbrizi, B. Phoenix, S. Green, J.L. Parsons. Current insights into the radiobiology of boron neutron capture therapy and the potential for further improving biological effectiveness. Cells 13, 2065 (2024). [CrossRef]
- G.L. Locher. Biological effects and therapeutic possibilities of neutrons. Am. J. Roentgenol. Radium Ther. Nucl. Med. 36, 1–13 (1936).
- W.H. Sweet, M. Javid. The possible use of neutron-capturing isotopes such as boron 10 in the treatment of neoplasms. I. Intracranial tumors. J. Neurosurg. 9, 200–209 (1952). [CrossRef]
- H. Hatanaka, K. Sano. A revised boron-neutron capture therapy for malignant brain tumours. I. Experience on terminally ill patients after Co-60 radiotherapy. Z. Neurol. 204, 309–332 (1973). [CrossRef]
- R.G. Fairchild, D. Gabel, B.H. Laster, D. Greenberg, W. Kiszenick, P.L. Micca. Microanalytical techniques for boron analysis using the 10B(n,α)7Li reaction. Med. Phys. 13, 50–56 (1986). [CrossRef]
- Kato, Y. Fujita, A. Maruhashi, H. Kumada, M. Ohmae, M. Kirihata, Y. Imahori, M. Suzuki, Y. Sakrai, T. Sumi, S. Iwai, M. Nakazawa, I. Murata, H. Miyamaru, K. Ono. Effectiveness of boron neutron capture therapy for recurrent head and neck malignancies. Appl. Radiat. Isot. 67, S37–S42 (2009). [CrossRef]
- R.F. Barth, M.G.H. Vicente, O.K. Harling, W.S. Kiger, et al. Current status of boron neutron capture therapy of high grade gliomas and recurrent head and neck cancer. Radiat. Oncol. 7, 146 (2012).
- T.D. Malouff, D.S. Seneviratne, D.K. Ebner, W.C. Stross, M.R. Waddle, D.M. Trifiletti, S. Krishnan. Boron neutron capture therapy: a review of clinical applications. Front. Oncol. 11, 601820 (2021). [CrossRef]
- ClinicalTrials.gov. Boron neutron capture therapy using CICS-1 and SPM-011 for malignant melanoma and angiosarcoma. Identifier: NCT04293289. Updated 2023-02-08. Accessed 2025-10-15.
- T. Zhou, K. Igawa, T. Kasai, T. Sadahira, W. Wang, T. Watanabe, P. Huang, et al. The current status and novel advances of boron neutron capture therapy clinical trials. Am. J. Cancer Res. 14, 429–447 (2024).
- P. Karihtala. The current status and future perspectives of clinical boron neutron capture therapy trials. Health Technol. 14, 1001–1005 (2024). [CrossRef]
- N. Farha, D. Dima, F. Ullah, S. Kamath. Precision oncology targets in biliary tract cancer. Cancers 15, 2105 (2023). [CrossRef]
- International Atomic Energy Agency. Advances in Boron Neutron Capture Therapy. Vienna: IAEA (2023). ISBN 978-92-0-132723-9.
- B. Hamermesh, G.R. Ringo, S. Wexler. The thermal neutron capture cross section of hydrogen. Phys. Rev. 90, 603–606 (1953). [CrossRef]
- S.F. Mughabghab. Atlas of Neutron Resonances: Resonance Parameters and Thermal Cross Sections Z = 1–100, 6th ed.; Elsevier: Amsterdam, 2018. ISBN 978-0-444-63744-2.
- M.B. Chadwick, et al. ENDF/B-VII.1 nuclear data files for neutron-induced reactions and advanced applications. Nucl. Data Sheets 112, 2887–2996 (2011).
- M. Bikchurina, T. Bykov, I. Ibrahim, et al. Dosimetry for boron neutron capture therapy developed and verified at the accelerator based neutron source VITA. Front. Nucl. Eng. 2, 1266562 (2023). [CrossRef]
- H. Kumada, T. Sakae, H. Sakurai. Current development status of accelerator based neutron source for boron neutron capture therapy. EPJ Techn. Instrum. 10, 18 (2023). [CrossRef]
- S. Altieri, N. Protti. A brief review on reactor based neutron sources for boron neutron capture therapy. Ther. Radiol. Oncol. 2, 1–6 (2018). [CrossRef]
- K. Hirose, A. Konno, J. Hiratsuka, et al. Boron neutron capture therapy using cyclotron-based epithermal neutron source and borofalan (10B) for recurrent or locally advanced head and neck cancer (JHN002): an open-label phase II trial. Radiother. Oncol. 155, 182–187 (2021). [CrossRef]
- A.A. Ivanov, A.N. Smirnov, S.Yu. Taskaev, et al. Accelerator-based neutron source for boron neutron capture therapy. Uspekhi Fiz. Nauk 192, 893–912 (2022).
- Y. Matsuya, T. Kai, T. Sato, et al. Track-structure modes in particle and heavy ion transport code system (PHITS): application to radiobiological research. Int. J. Radiat. Biol. 98, 148–157 (2022). [CrossRef]
- S. Jing, H. Guo, Y. Qi, G. Yang, Y. Huang. A portable fast neutron irradiation system for tumor therapy. Appl. Radiat. Isot. 160, 109138 (2020). [CrossRef]
- H. Kumada, K. Takada, S. Tanaka, et al. Evaluation of the characteristics of the neutron beam of a linac-based neutron source for boron neutron capture therapy. Appl. Radiat. Isot. 165, 109246 (2020). [CrossRef]
- M.E. Capoulat, D. Cartelli, M. Baldo, et al. Accelerator based-BNCT facilities worldwide and an update of the Buenos Aires project. Appl. Radiat. Isot. 219, 111723 (2025). [CrossRef]
- G. Li, W. Jiang, L. Zhang, W. Chen, Q. Li. Design of beam shaping assemblies for accelerator-based BNCT with multi-terminals. Front. Public Health 9, 642561 (2021). [CrossRef]
- N. Hu, H. Tanaka, K. Akita, et al. Accelerator based epithermal neutron source for clinical boron neutron capture therapy. J. Neutron Res. 24, 359–366 (2022). [CrossRef]
- PR Newswire. Neutron Therapeutics and Helsinki University Hospital treat first patients in the United States in phase 1 trial of boron neutron capture therapy. PR Newswire, May 16, 2025. https://go.gale.com/ps/i.do?id=GALE%7CA839961052.
- A. Pisent, F. Grespan, C. Baltador, et al. ANTHEM Project, construction of a RFQ driven BNCT neutron source. In Proceedings of the 32nd Linear Accelerator Conference (LINAC 2024), Chicago, IL, USA, 25–30 August 2024. [CrossRef]
- M. Bikchurina, T. Bykov, E. Byambatseren, et al. VITA high flux neutron source for various applications. J. Neutron Res. 24, 273–279 (2022).
- T. Nishitani, S. Yoshihashi, Y. Tanagami, et al. Neutronics analyses of the radiation field at the accelerator-based neutron source of Nagoya University for the BNCT study. J. Nucl. Eng. 3, 222–232 (2022). [CrossRef]
- D.L. Bleuel, R.J. Donahue, B.A. Ludewigt, J. Vujic. Designing accelerator-based epithermal neutron beams for boron neutron capture therapy. Med. Phys. 25, 1725–1734 (1998).
- S. Yonai, T. Aoki, Y. Tahara, M. Manabe, H. Hatanaka, K. Nakagawa. Feasibility study on epithermal neutron field for cyclotron-based boron neutron capture therapy. Med. Phys. 30, 2021–2030 (2003). [CrossRef]
- H. Tanaka, Y. Sakurai, M. Suzuki, et al. Improvement of dose distribution in phantom by using epithermal neutron source based on the Be(p,n) reaction using a 30 MeV proton cyclotron accelerator. Appl. Radiat. Isot. 67, S258–S261 (2009). [CrossRef]
- M. Hervé, N. Sauzet, D. Santos. On the epithermal neutron energy limit for accelerator-based BNCT: study and impact of new energy limits. Phys. Med. 88, 148–157 (2021). [CrossRef]
- N. Hu, M. Suzuki, S. Masunaga, et al. Experimentally determined relative biological effectiveness of cyclotron-based epithermal neutrons designed for clinical BNCT: in vitro study. J. Radiat. Res. 64, 811–815 (2023). [CrossRef]
- H. Shuai, E. Dian, F. Mezei, P. Sipos, S. Czifrus. An accelerator-based neutron source design with a thermal neutron port and an epithermal neutron port for boron neutron capture therapy. Appl. Radiat. Isot. 217, 111647 (2025). [CrossRef]
- N.S. Schmidt, D. Shabani, J. Li, P. Zakalek, E. Mauerhofer, J. Dawidowski, T. Gutberlet. Development of an epithermal and fast neutron target station for the High Brilliance Neutron Source. Eur. Phys. J. Plus 140, 171 (2025).
- International Commission on Radiological Protection (ICRP). Relative biological effectiveness (RBE), quality factor (Q), and radiation weighting factor (wₙ). Ann. ICRP 33, 2003.
- International Commission on Radiological Protection (ICRP). The 2007 recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 37, 2–4 (2007).
- J. Choi, J.O. Kang. Basics of particle therapy II: relative biological effectiveness. Radiat. Oncol. J. 30, 1–13 (2012). [CrossRef]
- M. Pedrosa-Rivera, J. Praena, I. Porras, M.P. Sabariego, U. Köster, M. Haertlein, V.T. Forsyth, J.C. Ramírez, C. Jover, D. Jimena, et al. Thermal neutron relative biological effectiveness factors for boron neutron capture therapy from in vitro irradiations. Cells 9, 2144 (2020). [CrossRef]
- J. Rassow, W. Sauerwein, A. Wittig, E. Bourhis-Martin, K. Hideghéty, R. Moss. Advantage and limitations of weighting factors and weighted dose quantities and their units in boron neutron capture therapy. Med. Phys. 31, 1128–1134 (2004). [CrossRef]
- T. Sato, S.I. Masunaga, H. Kumada, N. Hamada. Microdosimetric modeling of biological effectiveness for boron neutron capture therapy considering intra- and intercellular heterogeneity in 10B distribution. Sci. Rep. 8, 988 (2018). [CrossRef]
- H. Fukuda. Response of normal tissues to boron neutron capture therapy (BNCT) with 10B-BSH and 10B-BPA. Cells 10, 2883 (2021). [CrossRef]
- Y. Han, C. Geng, J.N.D. Kondo, M. Li, J. Ramos Méndez, S. Altieri, Y. Liu, X. Tang. Microdosimetric analysis for boron neutron capture therapy via Monte Carlo track structure simulation with modified lithium cross sections. Radiat. Phys. Chem. 209, 110956 (2023). [CrossRef]
- S.J. González, E.C.C. Pozzi, A.M. Hughes, L. Provenzano, H. Koivunoro, D.G. Carando, S.I. Thorp, M.R. Casal, S. Bortolussi, V.A. Trivillin, et al. Photon iso-effective dose for cancer treatment with mixed field radiation based on dose-response assessment from human and an animal model: clinical application to BNCT for head and neck cancer. Phys. Med. Biol. 62, 7938–7958 (2017).
- G.F. Perotti Bernardini, S. Bortolussi, H. Koivunoro, L. Provenzano, C. Ferrari, L. Cansolino, I. Postuma, D.G. Carando, L. Kankaanranta, H. Joensuu, S.J. González. Comparison of photon isoeffective dose models based on in vitro and in vivo radiobiological experiments for head and neck cancer treated with BNCT. Radiat. Res. 198, 134–144 (2022). [CrossRef]
- Postuma, C. Magni, B. Marcaccio, et al. Using the photon isoeffective dose formalism to compare and combine BNCT and CIRT in a head and neck tumour. Sci. Rep. 14, 418 (2024). [CrossRef]
- V. Conte, A. Bianchi, A. Selva. Boron neutron capture therapy: microdosimetry at different boron concentrations. Appl. Sci. 14, 216 (2024). [CrossRef]
- A. Tedjani, R. Abdi, D. Boumala, A. Belafrites, J.-E. Groetz. Boron neutron capture therapy: dosimetric evaluation of a brain tumor and surrounding healthy tissues using Monte Carlo simulation. Nucl. Instrum. Methods Phys. Res., Sect. A 1040, 167240 (2022). [CrossRef]
- M.R. Fabbrizi, C.M. Nickson, J.R. Hughes, E.A. Robinson, K. Vaidya, C.P. Rubbi, A. Kacperek, H.E. Bryant, T. Helleday, J.L. Parsons. Targeting OGG1 and PARG radiosensitises head and neck cancer cells to high-LET protons through complex DNA damage persistence. Cell Death Dis. 15, 150 (2024). [CrossRef]
- E. Melia, J.L. Parsons. DNA damage and repair dependencies of ionising radiation modalities. Biosci. Rep. 43, BSR20222586 (2023). [CrossRef]
- G.V. Mechetin, D.O. Zharkov. DNA damage response and repair in boron neutron capture therapy. Genes 14, 127 (2023). [CrossRef]
- K. Maliszewska-Olejniczak, D. Kaniowski, M.T. Araszkiewicz, K. Tyminska, A. Korgul. Molecular mechanisms of specific cellular DNA damage response and repair induced by the mixed radiation field during boron neutron capture therapy. Front. Oncol. 11, 676575 (2021). [CrossRef]
- W.H. Jin, C. Seldon, M. Butkus, W. Sauerwein, H.B. Giap. A review of boron neutron capture therapy: its history and current challenges. Int. J. Part. Ther. 9, 71–82 (2022). [CrossRef]
- X. Li, P. He, Y. Wei, C. Qu, F. Tang, Y. Li. Application and perspectives of nanomaterials in boron neutron capture therapy of tumors. Cancer Nano 16, 25 (2025). [CrossRef]
- Y. Zhang, H.G. Kang, H.-Z. Xu, H. Luo, M. Suzuki, Q. Lan, X. Chen, N. Komatsu, L. Zhao. Tumor eradication by boron neutron capture therapy with 10B-enriched hexagonal boron nitride nanoparticles grafted with poly(glycerol). Adv. Mater. 35, e2301479 (2023). [CrossRef]
- S. Xu, Y. Yu, B. Zhang, K. Zhu, Y. Cheng, T. Zhang. Boron carbide nanoparticles for boron neutron capture therapy. RSC Adv. 15, 10717–10730 (2025). [CrossRef]
- M.J. Luderer, B. Muz, K. Alhallak, J. Sun, K. Wasden, N. Guenthner, P. de la Puente, C. Federico, A.K. Azab. Thermal sensitive liposomes improve delivery of boronated agents for boron neutron capture therapy. Pharm. Res. 36, 144 (2019).
- A.-M. Caminade, F. Rodríguez, R. Gramage-Doria. Dendritic structures functionalized with boron clusters, in view of BNCT. Pharmaceutics 15, 2117 (2023).
- W.-Y. Fu, Y.-L. Chiu, S.-C. Huang, W.-Y. Huang, F.-T. Hsu, H.-Y. Lee, T.-W. Wang, P.-Y. Keng. Boron neutron capture therapy enhanced by boronate ester polymer micelles: synthesis, stability, and tumor inhibition studies. Biomacromolecules 25, 4215–4232 (2024). [CrossRef]
- J. Xiang, L. Ma, J. Tong, N. Zuo, W. Hu, Y. Luo, J. Liu, T. Liang, Q. Liu. Boron-peptide conjugates with angiopep-2 for boron neutron capture therapy. Front. Med. 10, 1199881 (2023). [CrossRef]
- V.G.S.S. Jyothi, N. Kommineni. Peptide conjugated boron neutron capture therapy for enhanced tumor targeting. Nanotheranostics 8, 458–472 (2024). [CrossRef]
- M.A. Vorobyeva, M.A. Dymova, D.S. Novopashina, E.V. Kuligina, V.V. Timoshenko, I.A. Kolesnikov, S.Y. Taskaev, V.A. Richter, A.G. Venyaminova. Tumor cell-specific 2’-fluoro RNA aptamer conjugated with closo-dodecaborate as a potential agent for boron neutron capture therapy. Int. J. Mol. Sci. 22, 7326 (2021). [CrossRef]
- A. Rudawska, B. Szermer-Olearnik, A. Szczygieł, J. Mierzejewska, K. Węgierek-Ciura, P. Żeliszewska, D. Kozień, M. Chaszczewska-Markowska, Z. Adamczyk, P. Rusiniak, K. Wątor, A. Rapak, Z. Pędzich, E. Pajtasz-Piasecka. Functionalized boron carbide nanoparticles as active boron delivery agents dedicated to boron neutron capture therapy. Int. J. Nanomed. 20, 6637–6657 (2025). [CrossRef]
- S.O. Oloo, K.M. Smith, M.D.G.H. Vicente. Multi-functional boron-delivery agents for boron neutron capture therapy of cancers. Cancers 15, 3277 (2023). [CrossRef]
- A. Lanfranco, D. Alberti, S. Parisotto, P. Renzi, V. Lecomte, S. Geninatti Crich, A. Deagostino. Biotinylation of a MRI/Gd BNCT theranostic agent to access a novel tumour-targeted delivery system. Org. Biomol. Chem. 20, 5342–5354 (2022).
- A. Vitali, M.P. Demichelis, G. Di Martino, I. Postuma, S. Bortolussi, A. Falqui, C. Milanese, C. Ferrara, P. Sommi, U. Anselmi-Tamburini. Synthesis and characterization of Gd-functionalized B₄C nanoparticles for BNCT applications. Life 3, 429 (2023).
- Y. Hattori, T. Andoh, S. Kawabata, N. Hu, H. Michiue, H. Nakamura, T. Nomoto, M. Suzuki, T. Takata, H. Tanaka, T. Watanabe, K. Ono. Proposal of recommended experimental protocols for in vitro and in vivo evaluation methods of boron agents for neutron capture therapy. J. Radiat. Res. 64, 859–869 (2023). [CrossRef]
- Y.-T. Zhou, et al. Recent progress of nano-drugs in neutron capture therapy. Theranostics 14, 3193–3212 (2024). [CrossRef]
- F.P. McCandless, R.S. Herbst. Separation of the isotopes of boron by chemical exchange reactions. U.S. Patent 5,419,887 (1995).
- S. Song, Y. Mu, X. Li, P. Bai. Advances in boron-10 isotope separation by chemical exchange distillation. Ann. Nucl. Energy 37, 1–4 (2010). [CrossRef]
- J.-P. Li. Studies on separation process and production technology of boron isotope. J. Isotopes 27, 87–92 (2014).
- Y. Tang, Y. Zheng, J. Tian, J. Sun. Process intensification of chemical exchange method for boron isotope separation using micro-channel distillation technology. Micromachines 12, 1222 (2021). [CrossRef]
- A.V. Khoroshilov. Separation of boron isotopes by chemical exchange in liquid–liquid systems. J. Phys.: Conf. Ser. 1099, 012006 (2018).
- P.I. Ivanov, A.V. Khoroshilov, N.S. Panyukova. Experimental modeling of boron-10 isotope enrichment during chemical exchange in a liquid–liquid system. Russ. J. Phys. Chem. A 98, 2891–2896 (2024). [CrossRef]
- Y. Sakuma, M. Aida, M. Okamoto, H. Kakihana. Boron isotope separation by ion exchange chromatography using weakly basic anion exchange resin. Bull. Chem. Soc. Jpn. 53, 1860–1863 (1980).
- H. Zhao, R. Gao, P. Bai. Advances in boron isotope separation by ion exchange chromatography. Asian J. Chem. 26, 2187–2190 (2014).
- J.F. Wild, H. Chen, K. Liang, J. Liu, S.E. Cox, A.N. Halliday, Y. Yang. Liquid solution centrifugation for safe, scalable, and efficient isotope separation. Sci. Adv. 9, eadg8993 (2023). [CrossRef]
- V.S. Letokhov. Laser-induced separation of isotopes. At. Energy 62, 297–311 (1987). [CrossRef]
- F. Tang, et al. Studies of irradiation products of laser boron isotope separation by infrared absorption spectroscopy. Chin. Phys. 2, 2 (1982).
- U.S. Patent 4,447,303 (1984), University of California / U.S. Department of Energy.
- G.N. Makarov. Laser separation of boron isotopes: research results and options for technological implementation. Phys.-Uspekhi 68, 452–489 (2025). [CrossRef]
- Global Times. China achieves breakthrough in low-temperature distillation of boron-10 isotopes to support nuclear safety. October 10 (2024). Available at: https://www.ecns.cn/news/sci-tech/2024-10-10/detail-ihehxcae7641285.shtml.
- China Nuclear Energy Association (CNEA). China’s breakthrough in boron-10 isotope separation technology. 2024. Available at: https://en.china-nea.cn/site/content/47860.
- W. Zhang, T. Liu, J. Xu. Preparation and characterization of 10B boric acid with high purity for nuclear industry. SpringerPlus 5, 1202 (2016).
Figure 1.
Schematic illustration of the BNCT principle, showing selective ¹⁰B uptake in tumor cells and the subsequent ¹⁰B(n,α)⁷Li reactions that generate high-LET particles responsible for localized cellular damage (from Ref.[3]).
Figure 1.
Schematic illustration of the BNCT principle, showing selective ¹⁰B uptake in tumor cells and the subsequent ¹⁰B(n,α)⁷Li reactions that generate high-LET particles responsible for localized cellular damage (from Ref.[3]).
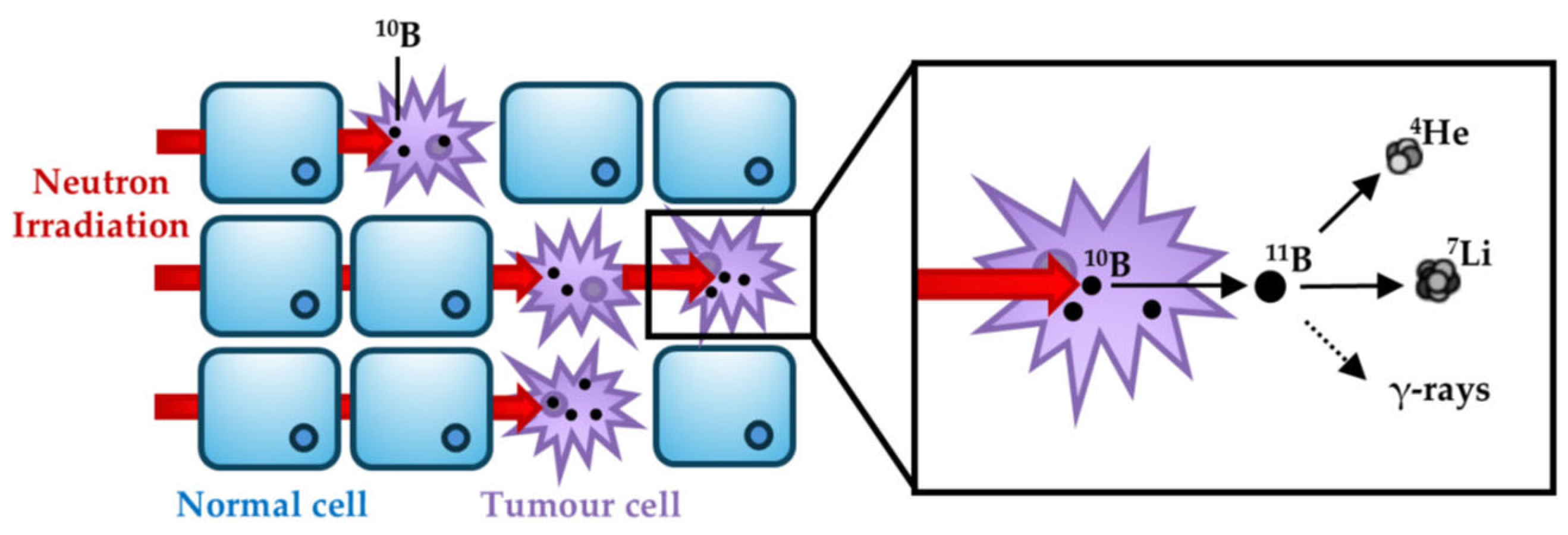
Figure 2.
- Energy-level scheme of the two decay channels associated with the reaction sequence ¹⁰B + n → ¹¹B* → α + ⁷Li, illustrating the excited-state formation and subsequent particle emission pathways.
Figure 2.
- Energy-level scheme of the two decay channels associated with the reaction sequence ¹⁰B + n → ¹¹B* → α + ⁷Li, illustrating the excited-state formation and subsequent particle emission pathways.
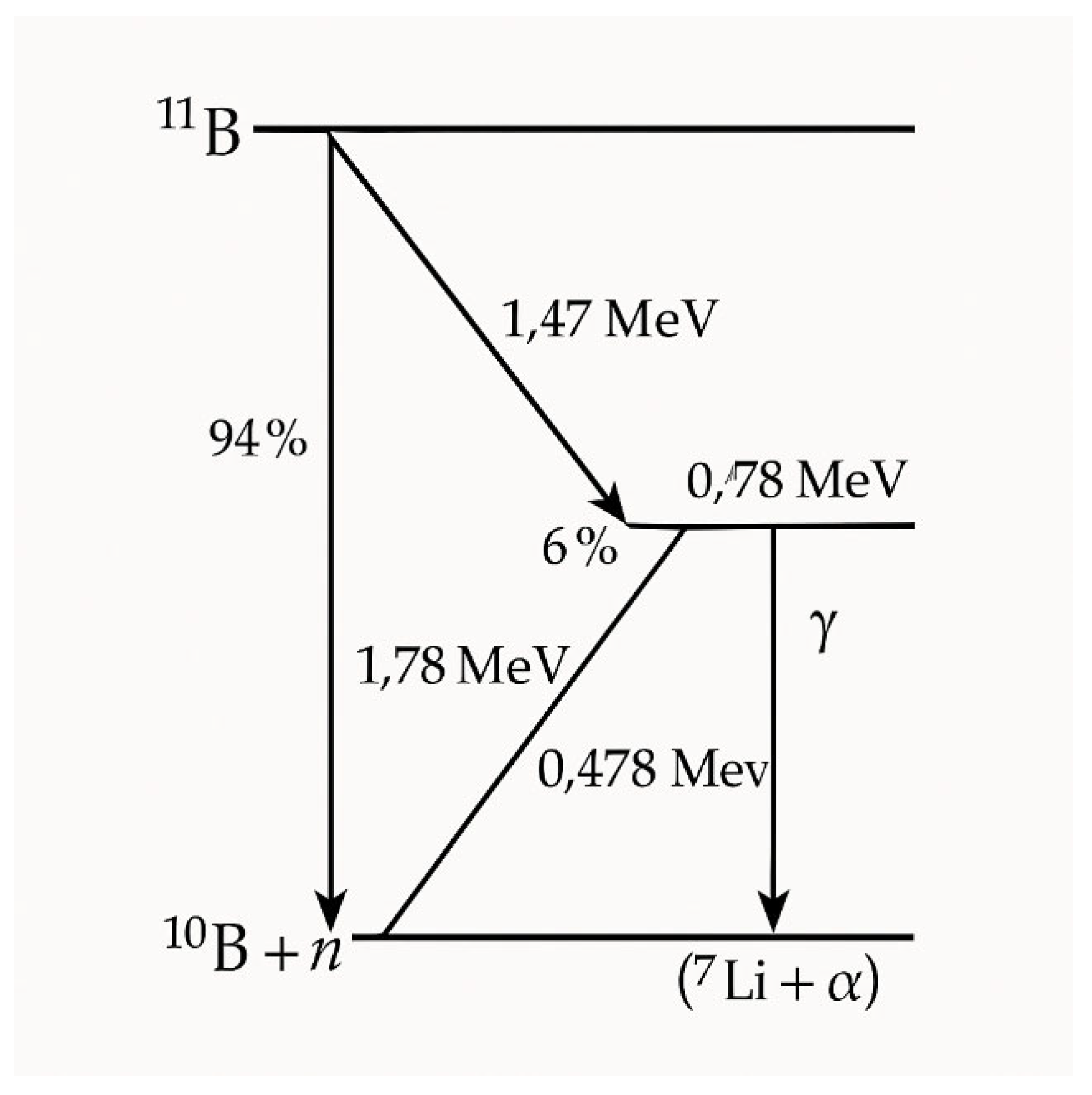
Figure 3.
Schematic layout of an accelerator-based neutron source for BNCT, showing the main system components (accelerator, proton–target interaction region, beam-shaping assembly) together with typical proton energies at the target and resulting neutron energy ranges after the moderation path (from Ref.[20]).
Figure 3.
Schematic layout of an accelerator-based neutron source for BNCT, showing the main system components (accelerator, proton–target interaction region, beam-shaping assembly) together with typical proton energies at the target and resulting neutron energy ranges after the moderation path (from Ref.[20]).
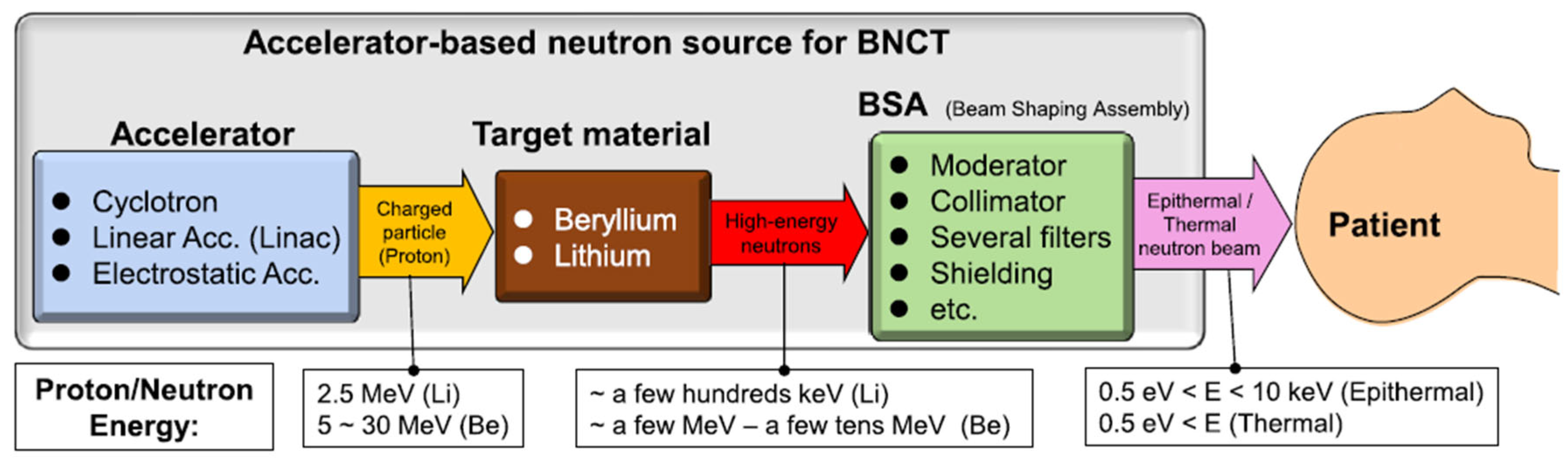
Figure 4.
Schematic view of a BSA modeled by Monte Carlo, showing the different components of the beam shaping assembly and the surrounding shielding (from Ref.[33]).
Figure 4.
Schematic view of a BSA modeled by Monte Carlo, showing the different components of the beam shaping assembly and the surrounding shielding (from Ref.[33]).
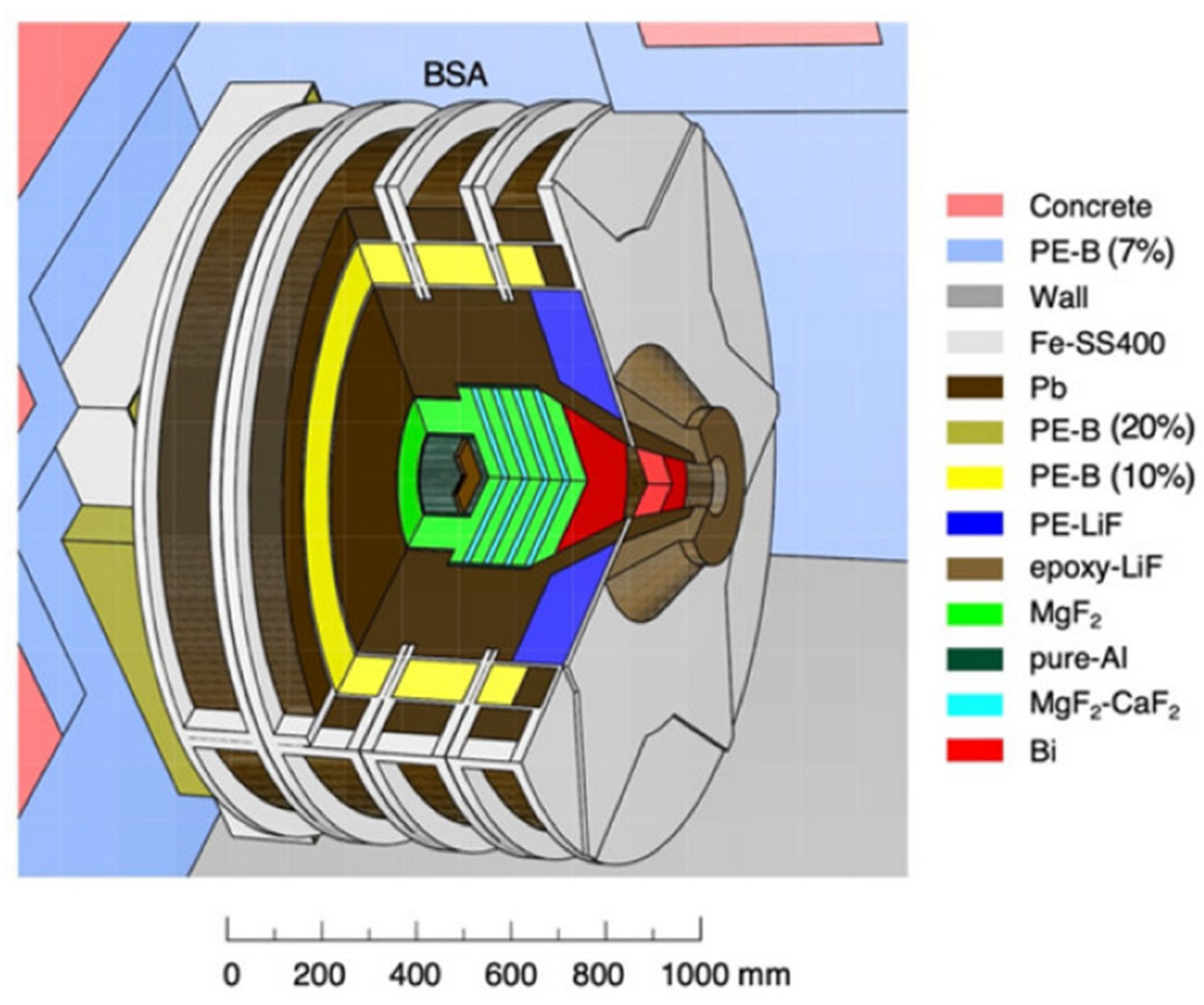
Figure 5.
Schematic illustration of the nuclear reactions, ionization processes, and resulting DNA damage occurring during BNCT (from Ref.[56]).
Figure 5.
Schematic illustration of the nuclear reactions, ionization processes, and resulting DNA damage occurring during BNCT (from Ref.[56]).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



