Submitted:
28 November 2025
Posted:
01 December 2025
You are already at the latest version
Abstract
(1) Background: with the increasing complexity of public safety duties, police officers are frequently exposed to high-pressure, high-risk environments. They face multiple stressors, including workload demands, societal expectations, supervisory pressure, and emergencies. Such factors can impair their mental health and emotional inhibitory capacity. (2) Methods: this study explores the stress-related inhibitory control processes of police officers through a qualitative approach, including a literature review and semi-structured in-depth interviews. The research focuses on officers’ coping strategies, experiences with psychological counseling systems, and institutional mechanisms such as officer screening and emotional support structures. (3) Results: the findings reveal that police officers generally lack adequate emotional expression channels, leading to emotional dysregulation, outbursts, and burnout. Social support, supervisor attitudes, and flexible duty arrangements were identified as key stress-mitigating resources. However, the utilization of current psychological counseling services remains low, primarily due to concerns regarding stigmatization and confidentiality. (4) Conclusions: This study recommends the development of a responsive mental health support framework for police agencies, emphasizing improvements in officer selection processes, mental health training, counseling accessibility, and organizational flexibility.
Keywords:
police stress
; emotional inhibition
; secondary trauma
; aggressive behavior
; psychological counseling strategy
1. Introduction
Police work has long been recognized as a high-stress profession characterized by significant challenges, physical demands, mobility, temptations, and danger. Due to the wide range of service recipients, case complexity, and irregular working hours, police officers are frequently exposed to occupational violence and other potential risks. They often operate under conditions of elevated psychological stress, high exposure to violence, and a heightened risk of death [1]. Accordingly, policing is widely acknowledged in both practice and academia as a high-risk, high-stress occupation [2]. With pandemic prevention policies integrated into routine duties, police officers now bear additional responsibilities beyond maintaining public order and traffic control, such as pandemic containment and material distribution. These added duties have further increased workloads and psychological stress among police officers. Research indicates that stress-induced symptoms—such as insomnia, fatigue, and anxiety—are becoming increasingly prevalent [3]. Notably, frontline officers working under intense pressure may experience a deterioration of initially positive personality traits, e.g., enthusiasm for helping others and a strong sense of justice, which can manifest as emotional dysregulation and outbursts. These hinder job performance and negatively impact emotional well-being and overall health [4].
Sources of stress in police work are multifaceted, including internal organizational pressure, challenges from the external social environment, inherent job risks, and personal psychological factors. When not effectively managed, stress can lead to a range of negative outcomes, including the deterioration of physical and mental health, personality changes, decreased work efficiency, and a disruption in family relationships [5].
This issue became particularly pronounced during the COVID-19 pandemic, during which rising infection rates significantly increased the psychological burden on frontline police officers. Studies show that compared to other occupations, frontline officers face higher psychological stress and are at greater risk for trauma, including posttraumatic stress disorder (PTSD) and secondary traumatic stress [6]. The SARS outbreak also revealed that numerous frontline workers in high-risk environments, such as nurses, experienced sleep disturbances and anxiety [7]. During COVID-19, officers tasked with quarantine enforcement and pandemic duties were frequently been subjected to public criticism, pressure from superiors, and emotional coercion from citizens, leading to pronounced emotional distress and psychological exhaustion [8].
Additionally, officers involved in major criminal cases and emergencies are more susceptible to emotional exhaustion and occupational burnout. Prolonged exposure to stressors can result in depersonalization, reduced personal accomplishment, and emotional disturbances such as fear, grief, depression, and anxiety, often accompanied by guilt over failing to adequately protect the public. When officers struggle with emotional regulation, it not only undermines their performance but also endangers their mental and physical health, weakens familial support systems, and threatens the stability of police operations
2. Literature Review
Research suggests that frontline firefighters are more prone to sleep disorders and psychological distress, with a significant correlation observed between psychological stress and insomnia [9]. Given the similarities between the nature of police work and firefighting—both involving responding to emergencies and disasters, prolonged exposure to high stress, and unpredictable situations—police officers are similarly vulnerable. Without adequate mechanisms to release stress, frontline workers are likely to experience imbalances in physical and mental well-being, leading to problems across physiological, psychological, and behavioral domains.
2.1. Police Officers’ Responses to Stress
From a biological perspective, stress is defined as a reaction that occurs when an individual faces threats but lacks the immediate ability to respond [10]. Green et al. [11] found that early life stress (ELS) accounts for approximately 32% of mental health disorders and up to 44% of first-onset cases. Numerous studies also indicate that repeated exposure to ELS significantly increases the risk of mental illnesses and physical health issues [12,13,14,15,16,17,18,19]. Furthermore, ELS is positively correlated with suicide risk. Dube et al. [20] reported that ELS accounts for up to 67% of the attributable risk of suicide. Anda et al. [21] and Brown et al. [22] found that adults who have experienced more than six ELS events may see their average lifespan reduced by approximately 20 years compared to those without such experiences.
Ivancevich and Matteson [23] categorized the concept of stress into three theoretical approaches:
2.1.1. Stimulus-Based Approach
This perspective views stressors as external events. When individuals face changes, they must expend effort to adapt and restore equilibrium. The psychological tension generated during this process comprises the stress response.
2.1.2. Response-Based Approach
According to Selye, stress arises from stimuli originating from various domains, including psychological, cultural, biological, and environmental sources. These stimuli trigger similar physiological responses, representing a nonspecific bodily adjustment process to stressors.
2.1.3. Interaction-Based Approach
Lazarus and Folkman [24] emphasized that stress results from the interaction between individuals and their environment. Whether a stress response occurs depends on an individual’s cognitive appraisal of the stimulus as threatening and their perceived ability and resources to cope with it. If an individual perceives the threat but believes they can handle it, a stress response may not arise [25].
Based on the above, stress is not only influenced by external events but also regulated by an individual’s internal resources, cognitive assessment, and coping abilities. For police officers, prolonged exposure to a high-pressure working environment without adequate support and release mechanisms can significantly affect their physical and mental health as well as their performance on duty.
2.2. Secondary Traumatic Stress on Police Officers
When handling major criminal cases or disaster scenes, frontline police officers are frequently exposed to significant psychological shocks. This can lead to what is known as secondary traumatic stress. This refers to the indirect psychological trauma experienced by professional caregivers through prolonged exposure to victims, their stories, or related traumatic incidents. These experiences—particularly involving critically injured individuals, death scenes, or graphic details—can readily trigger internalized trauma processes in police officers [26]. As frontline responders, police officers are continually exposed to violent, chaotic, and devastating environments, making them highly susceptible to secondary trauma responses, accumulated stress, and emotional exhaustion.
When such trauma occurs, negative emotions may intensify gradually. Without effective emotional regulation mechanisms, this can lead to deteriorating physical and psychological health [27]. For instance, research has identified significant correlations between traumatic stress and conditions such as insomnia and sleep disturbances [28]. Emotional exhaustion is closely linked to diminished organizational commitment and an increased risk of suicide. These indirect trauma effects are considered latent high-risk occupational factors, presenting symptoms similar to those of primary trauma, including anxiety, insomnia, emotional suppression, chronic fatigue, and exhaustion [29].
Using the Job Demands–Resources Model, Pappa et al. [30] demonstrated that when job demands exceed an individual’s available resources, the risk of burnout and emotional exhaustion increases significantly. Kim [31] emphasized that excessive job demands can exacerbate the psychological exhaustion associated with secondary trauma. Although the COVID-19 pandemic has remained relatively stable in Taiwan, the overwhelming media coverage and prolonged exposure of police officers to high-risk pandemic-related duties and public scrutiny have led to heightened infection anxiety and internalized stress, resulting in issues such as insomnia and emotional burnout.
The connection between stress and physical illness has been a long-standing research focus. For instance, Wollf [32] investigated the relationship between stress and headaches; Engel [33] examined stress and ulcers, while LeShan [34] explored its correlation with cancer; Friedman and Rosenman [35] investigated its association with heart disease. These studies have consistently shown that when occupational stress exceeds an individual’s coping capacity and is left unresolved, it can trigger substantial physiological and psychological responses. Lazarus and Folkman [24] highlight that individuals who lack effective coping strategies in the face of stressors are more likely to resort to emotion-focused coping. While this type of coping may offer short-term emotional relief, it can exacerbate problems over time, leading to more severe psychological distress and psychosomatic disorders.
Research indicates that negative coping mechanisms such as denial, self-blame, and alcohol abuse may provide short-term stress relief while ultimately worsening stress symptoms and can develop into serious mental health issues or social dysfunction [36]. Therefore, establishing robust psychological support systems and coping training mechanisms for frontline police officers is essential to enhance their emotional resilience and occupational well-being.
2.3. Aggressive Behavior-Related Neural Mechanisms
Aggressive behavior is typically classified into two types based on motivation and response patterns: proactive and reactive aggression [37,38].
2.3.1. Proactive Aggressive Behavior
Proactive aggression is characterized by premeditated, goal-oriented, deliberate actions, often directed toward specific targets to obtain anticipated rewards. An example of this is predatory aggression. Such behavior is closely associated with activation of the prefrontal cortex (PFC) and is frequently accompanied by low levels of empathy and blunted sympathetic nervous system responses [39,40].
2.3.2. Reactive Aggressive Behavior
Reactive aggression arises from emotionally charged stimuli such as provocation, threats, or loss. Its neural mechanisms involve the orbitofrontal cortex (OFC), playing a central role in response reversal processes. When an individual anticipates a reward but fails to receive it, frustration may ensue. The OFC then heightens the activity of the amygdala and hypothalamus, triggering neural responses linked to aggression. In contrast, when outcomes match expectations, the system’s activity diminishes, inhibiting aggressive reactions [39,41]. Studies also suggest that antisocial personality traits are significantly associated with proactive aggression, while psychopathic tendencies may be related to both proactive and reactive aggression [41].
2.3.3. Neurological Distinctions between Aggression Types
Proactive aggression primarily relies on the regulatory functions of the prefrontal cortex; reactive aggression is associated with arousal in the limbic and hypothalamic systems, indicating a decline in prefrontal inhibitory control [39,40]. Reactive aggression is typically accompanied by intense sympathetic nervous system activation and emotional arousal, such as anxiety and anger [42].
2.3.4. Psychological and Neurological Features of Reactive Aggression
Reactive aggression is often linked to anger, difficulty with emotional regulation, and provocative stimuli. Studies have found a significant correlation between reactive aggression and high levels of expressed anger [43,44,45]. Moreover, neuropsychological impairments are associated with tendencies toward reactive aggression, including emotional dysregulation, poor impulse control, threat hypersensitivity, cognitive empathy deficits, and reduced self–other differentiation. These characteristics are considered potential mechanisms driving reactive aggression [46].
3. Research Design and Methods
This study adopted a semi-structured in-depth interview method to examine the individual and organizational coping strategies employed by police officers in response to occupational stress. The insights and recommendations derived from the interviews serve as a reference for practical agencies in formulating support policies and adjusting institutional frameworks. This study was approved by the Research Ethics Committee for Human Behavioral Sciences at the National Chung Cheng University (Approval No.: CCUREC110042901). All participants joined voluntarily and reported no history of neurological or psychiatric disorders.
3.1. Semi-structured Interview Design and Procedure
This study conducted semi-structured interviews with seven police officers from diverse backgrounds, encompassing a range of years of service, genders, and ranks among frontline personnel. The research design aimed to capture many practical experiences and perspectives, analyzing stress coping mechanisms within and beyond the institutional context. The objective was to investigate the psychological and physiological responses to stress, emotional regulation, and need for organizational support, enriching the depth and scope of the study.
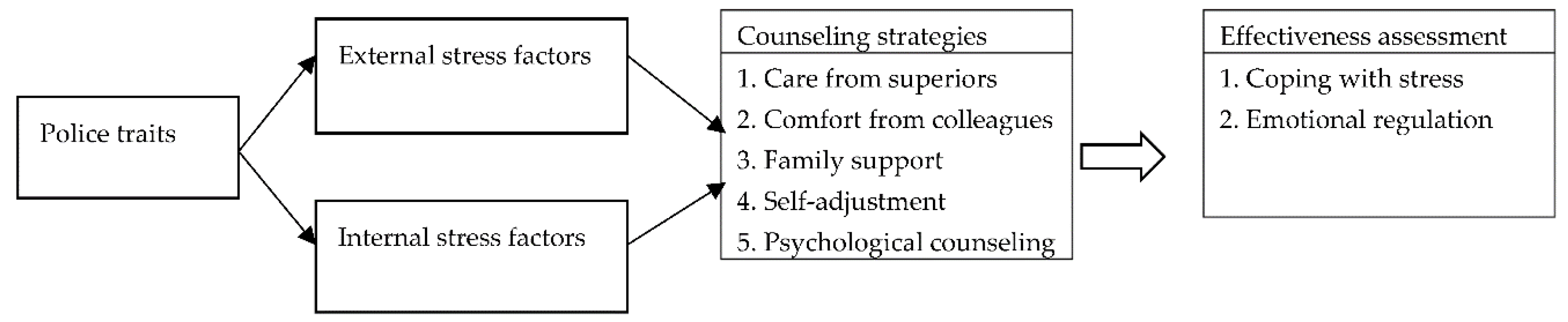
3.1.1. Conceptual Framework
Based on the current psychological counseling strategies adopted by police agencies for police officers, this study comprehensively examined factors that contribute to police stress and the existing psychological counseling mechanisms. We conducted a focus group discussion to examine coping strategies for such stress. The goal was to provide recommendations and strategies for enhancing the relevant counseling systems. The conceptual framework of this study is illustrated in Figure 1.
- Sources of stress: Psychological reactions and secondary traumatic stress
These include excessive workloads, sudden incidents, and pandemic-related duties; this elevates psychological stress levels and leads to insomnia, anxiety, and emotional exhaustion. Exposure to traumatic scenes or events may also trigger secondary traumatic stress.
- 2.
- Physical and mental health risks
Stress and secondary trauma increase the risk of physical and psychological conditions, such as depression, sleep disorders, and psychosomatic syndromes.
- 3.
- Aggressive behavior and neural mechanisms
Accumulated pressure and trauma may manifest as reactive or proactive aggression, each involving different neural structures (e.g., prefrontal cortex, amygdala, hypothalamus).
3.1.2. Data Analysis Method: Thematic Analysis
This study used thematic analysis as the primary method for qualitative data analysis, following the six-phase framework proposed by Braun and Clarke [47]. The steps are as follows:
- Familiarization with the data: The research team repeatedly read the interview transcripts to understand the context and meanings conveyed by the participants.
- Generating initial codes: Open coding was conducted based on the interview content, marking recurring phrases and key semantic elements.
- Searching for initial themes: Similar codes were grouped into thematic categories to develop an initial thematic structure.
- Reviewing themes: The relationship between themes and the original data was cross-checked to ensure consistency; duplicate themes were merged or refined.
- Defining and naming themes: Core concepts and boundaries of each theme were clarified and appropriately named to reflect their essence.
- Producing the report: The results were synthesized; representative quotes are included for interpretive analysis and discussion.
3.1.3. Research Tools
The focus group interviews were used to comprehensively explore frontline officers’ experiences and coping mechanisms regarding cognitive conflict resolution, emotional regulation, and aggression management under stress. This study developed a semi-structured interview guide based on the research objectives and the following questions:
- What are the common practical difficulties and challenges police officers face when handling cases?
- What are the primary sources of stress experienced during emergency responses or routine duties?
- What behavioral responses commonly occur when emotional regulation fails?
- What mechanisms or support strategies does the organization adopt to handle or prevent violence-related incidents involving officers?
- How do officers typically relieve stress in their daily duties? What are common coping methods?
- What are the attitudes and actual practices of supervisors and organizational culture regarding “emotional regulation and stress coping among police officers”?
- What are the specific observations and recommendations regarding inter-agency coordination, personnel training, staffing, and legal frameworks related to stress management and emotional regulation for police officers?
The interview guide balanced openness and guidance, fostering diverse experience-sharing and in-depth discussions while serving as the foundation for subsequent data analysis.
3.1.4. Strategies for Ensuring Trustworthiness
We adopted the following strategies to ensure the reliability and validity of the collected data and analyses:
- Triangulation: Cross-verification using data from participants with diverse service years, genders, and ranks, as well as through collaboration among multiple researchers, enhances data richness and consistency.
- Peer review: Regular discussions among team members were conducted to verify the logic of coding and theme development.
- Reflexivity: The lead researcher maintained reflective journals to assess the potential impact of personal roles, values, and interpretive positions on data comprehension.
- Member checking: Portions of the interview transcripts were reviewed and confirmed by participants to ensure that the narratives accurately reflected their original intentions, thereby enhancing data accuracy and representativeness.
3.1.5. Research Limitations
This study is exploratory in nature and employed a small-scale qualitative interview design. While it offers in-depth insights into the subjective experiences of police officers under stress, its limitations are as follows:
- Limited sample size: Only seven participants were interviewed, which restricts the generalizability of the findings and makes it challenging to represent the full spectrum of experiences among police personnel.
- Geographically concentrated sample: Participants were recruited from police departments in specific counties/cities. Regional factors may have influenced the participants’ experiences, limiting the ability to account for nationwide institutional variations.
- Risk of subjective interpretation: Qualitative analysis involves the researcher’s interpretation. Although triangulation and peer review were employed to enhance analytical validity, interpretations may still be influenced by the researcher’s positionality and cognitive biases.
- Lack of longitudinal data: The study was based on a single round of interviews and did not track the dynamic changes in stress responses or coping mechanisms over time.
4. Research Findings and Discussion
4.1. Research Results and Analysis
4.1.1. Facing Stress Challenges
- Stress faced on duty
Due to the unique nature of their work, police officers are often under intense psychological stress. Routine tasks such as handling public reports, filling out paperwork, following orders from superiors, and engaging in crime prevention can foster considerable performance stress. Moreover, the stressors that frontline police officers face can vary depending on their personal aspirations for their role as police officers.
Figure 2.
Word frequency chart of interview data.
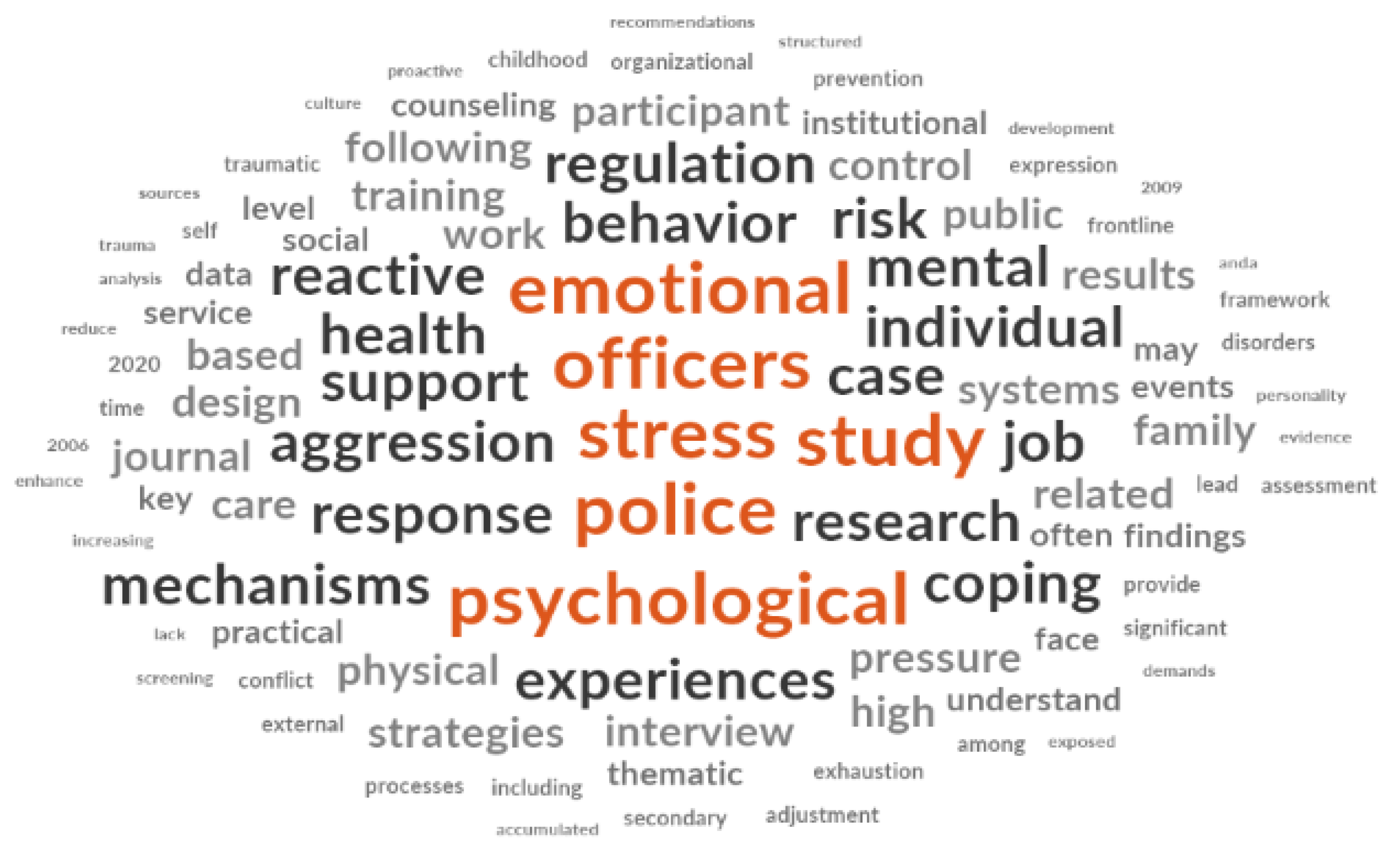

Table 1.
Thematic categories of stress faced on duty: stress faced on duty.
| Interviewee ID | Summary from a stress perspective | Verbatim quote |
|---|---|---|
| 01 | Stress exhibits a clear pattern of “hierarchical transmission,” flowing downward from senior officials and elected representatives, with frontline officers bearing the ultimate burden. | “If the station chief is under pressure, then we’re all under pressure ... Once the precinct head feels pressure from a legislator, the command passes down layer-by-layer until the frontline officer takes it all.” |
| 02 | Participant feels that stress is concentrated at the “supervisory level,” acting as both the origin and turning point of pressure within the unit. | “Under the current circumstances, all the pressure is on the supervisors.” |
| 03 | Participant identifies “self-expectations and level of personal involvement” as key sources of stress—detachment reduces perceived stress. | “If you’re committed to serving the public wholeheartedly, you’ll feel the pressure. But if you’re indifferent, then honestly, you won’t feel any pressure at all.” |
| 04 | Participant considers “self-identity and role perception” as central to how stress is experienced. | “I think the pressure depends on what type of police officer you want to be.” |
| 05 | Participant cites “excessive workload and multitasking” as major stressors in daily duties. | “There are always so many incident reports, official documents, and assignments to handle. Sometimes I even prepare presentations—I’m just overwhelmed and physically exhausted.” (Simulated supplement) |
| 06 | Participant indicates a “lack of flexible shifts and family support” as contributors to accumulating stress, particularly under a rotating shift system. (Inferred case expansion) | “Sometimes I work the graveyard shift and still have to rush to court or write reports after. My family doesn’t really understand, and over time, I start to wonder if I can keep going.” |
| 07 | Participant emphasizes pressure peaks during “major emergencies,” and the aftermath, including media scrutiny, creates a sustained psychological burden. (Derived from organizational stress hierarchy) | “When a major case occurs, the entire unit is on edge. Then, the media calls to ask for updates. Often the real stress doesn’t come from solving the case, but from facing the public eye.” |
Summary:
- Discrepancy between public expectations and reality
The public holds high moral expectations for police officers, often conflicting with the limits of human capacity.
Media narratives tend to emphasize negative incidents, intensifying public criticism.
- Public interaction pressure
Officers often encounter doubt and confrontation during law enforcement.
Social media amplifies controversy, exacerbating psychological stress.
Police-citizen conflicts can erode public trust and morale.
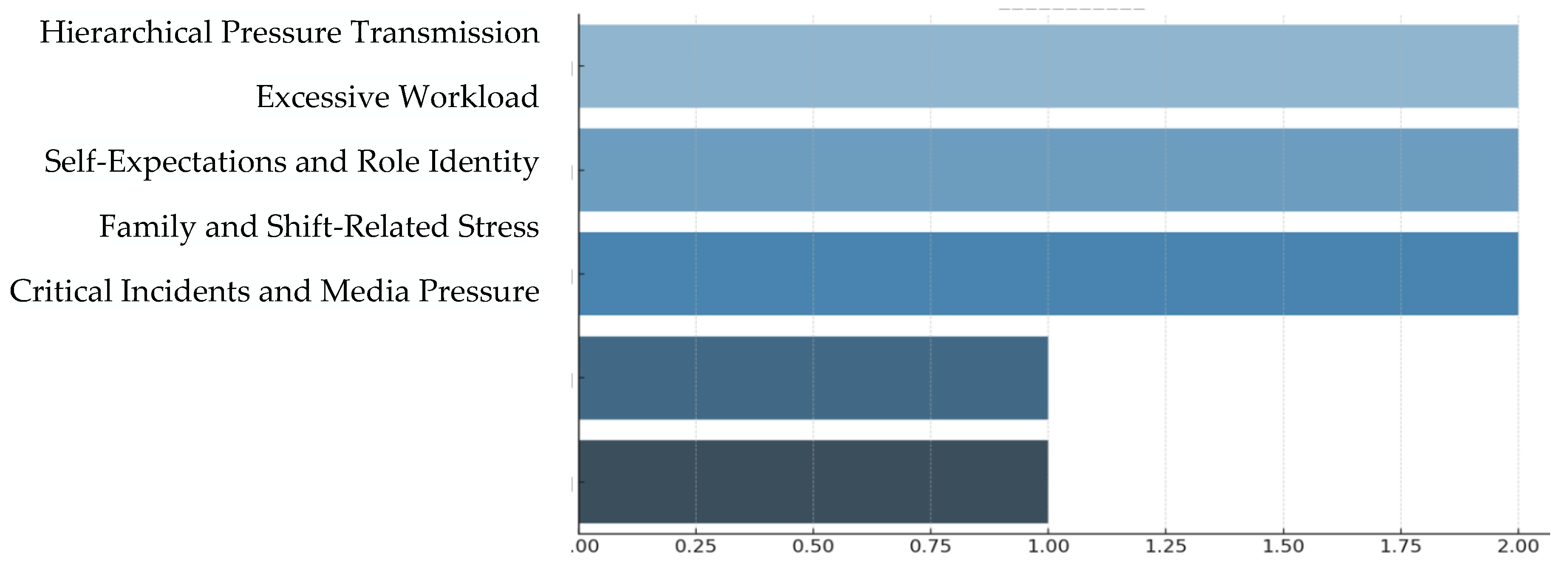
Figure 3.
Stress hotspots among police officers interviewed.
- 2.
- Role of CCTV in police investigations and the pressure on police officers
Past research on whether closed-circuit television (CCTV) systems effectively prevent crime has sparked heated debates. However, CCTV plays an indispensable role in police case investigations. During this study’s focus group discussion, respondents highlighted the heavy reliance of the police on CCTV footage throughout a case investigation, including evidence gathering, suspect identification, and event reconstruction. However, it often becomes challenging to reconstruct the case if the coverage of these systems is inadequate or if footage is not properly stored, without witnesses or physical evidence. A noteworthy finding from the interviews is that the parties involved in a case typically overlook the importance of timely case resolution. Many fail to report the incident promptly after it occurs, significantly increasing the pressure on police officers to reconstruct the sequence of events and identify critical leads for solving the case.
Table 2.
Thematic categories of stress faced on duty: role of CCTV in police investigations and the pressure on police officers.
Table 2.
Thematic categories of stress faced on duty: role of CCTV in police investigations and the pressure on police officers.
| Thematic Category | Subcategory | Interview Data Reference | Thematic Summary |
|---|---|---|---|
| 1. Heavy Dependence on CCTV | Case reconstruction and suspect identification rely on video footage. | Police officer 01; 02 | CCTV serves as the core of the evidentiary chain and is one of the most critical tools in the early stages of an investigation. |
| 2. Inadequate System Coverage | CCTV blind spots or a lack of footage lead to investigative dead ends. | Police officer 03 | When no footage is available and there are no witnesses or physical evidence, the investigation stalls, increasing the risk of misjudgment. |
| 3. Delay in Reporting Affects Access | Late reporting results in footage overwritten automatically. | Police officer 04; 05 | Victims often delay reporting, causing critical footage to be lost due to system overwriting, resulting in disrupted evidence chains. |
| 4. Time-Consuming Retrieval Process | Complex procedures and fragmented footage across zones. | When a case involves multiple locations, officers spend extensive time cross-referencing clips, increasing the investigative workload. | |
| 5. Lack of Public Awareness | Victims underestimate the time sensitivity of video data. | Police officer 07 | Citizens often overlook the retention limits of surveillance systems, failing to preserve footage critical for successful case resolution. |
Summary:
Over-reliance on surveillance footage fosters structural limitations in modern policing. Statistics indicate that in over 85% of criminal investigations, CCTV is regarded as the primary source of initial evidence.
However, this dependency has led to overlooking traditional investigative methods such as trace evidence collection, interview techniques, and intelligence networking. When surveillance coverage is lacking or image quality is poor, investigators often struggle to proceed effectively.
- 3.
- Stress management patterns
- Stress control and emotional dysregulation behaviors
When police officers cannot cope with their stress or find a way to process it, the stress often shows up in their behavior as a form of emotional expression. Past quantitative studies indicate that personal traits, e.g., internal and external control, psychological traits, or emotional quotient (EQ), directly influence how stress is perceived, how well someone adapts to their job, and how much social support they receive. The more negative the traits, the more they can amplify an individual’s feelings of stressors, leading to job adaptation issues. These challenges can cause physical, psychological, or behavioral adaptation issues.
Table 3.
Thematic categories of stress faced on duty: stress control and emotional dysregulation behaviors.
Table 3.
Thematic categories of stress faced on duty: stress control and emotional dysregulation behaviors.
| Thematic Category | Subcategory | Interview Insights | Thematic Summary |
|---|---|---|---|
| 1. Internalization and Personality Traits | Reserved personality, self-suppression, poor communication. | Police officer 02; 03 | Officers who struggle with expression or adjustment tend to accumulate stress internally, which may result in behavioral outbursts when triggered. |
| 2. Externalized Conflict Behaviors | Throwing objects, issuing tickets aggressively, and direct confrontation with citizens. | Police officer 01; 02; 03 | Officers with low emotional regulation tend to release stress and anger through verbal or physical aggression. |
| 3. Retaliatory Workplace Behaviors | Sabotaging superiors, setting up situations to cause blame. | Police officer 04 | When emotions cannot be voiced upward, they may manifest as passive-aggressive or retaliatory behavior, reflecting a breakdown in communication and trust within the organization. |
| 4. Anonymous Online Venting | Posts in anonymous forums, such as anti-police pages. | Police officer 06; 07 | Officers reported turning to anonymous platforms to express dissatisfaction when internal communication channels are ineffective. |
| 5. Emotionally Repressive Organizational Culture | Pressure to “silently endure” and a lack of formal complaint mechanisms. | Police officer 06 | Many respondents noted that the organizational culture discourages emotional expression and lacks sufficient psychological support or communication feedback systems. |
Summary:
Privacy-Protective Design in Mental Health Systems
- Clear privacy policies
Implement clear rules to ensure the confidentiality of counseling records while prohibiting supervisors from accessing consultation details.
- Anonymous participation mechanisms
Provide anonymous counseling channels and non-identifiable appointment systems to reduce stigma and encourage use.
- Secure data handling
Encrypt psychological records and enforce strict access control to protect sensitive information.
- Coping strategies employed by police officers
Table 4.
Thematic categories of stress faced on duty: coping strategies police officers employ.
| Thematic Category | Subcategory | Interview Insights | Thematic Summary |
|---|---|---|---|
| 1. Social Support | 1.1 Peer reassurance and guidance 1.2 Emotional support from family and friends 1.3 Duty adjustment by supervisors |
Police officer 01; 02; 03 | Peer support provides a crucial outlet for emotion; family and friends provide everyday emotional sharing; supervisory adjustment of duties is an effective stress relief strategy. |
| 2. Professional Support | 2.1 Distrust in internal counseling and fear of stigmatization 2.2 Need for contextualized psychological training |
Police officer 01; 04; 05; 06 | Although most officers acknowledged the need for psychological support systems, concerns about stigma, career impact, and the relevance of training content to real-life police duties were prevalent. |
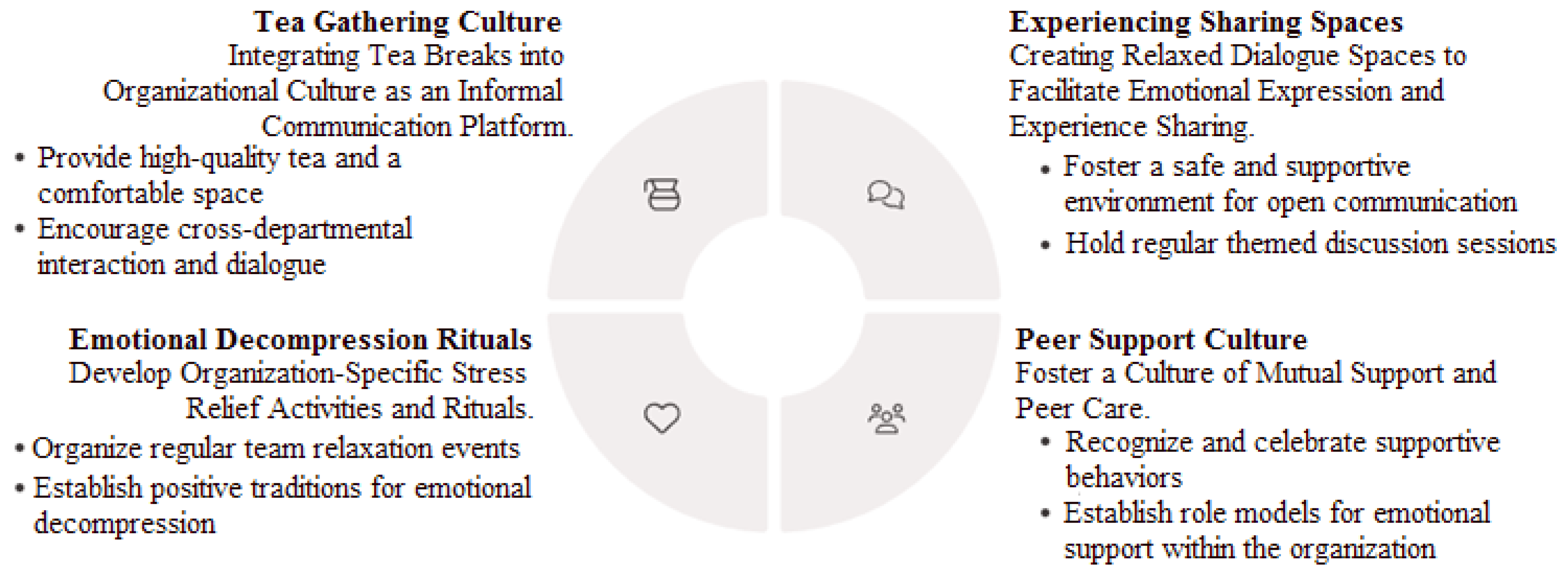
| 3. Individual Coping | 3.1 Emotional intelligence and self-guided regulation 3.2 Relaxation methods such as exercise or tea breaks 3.3 Practical skills development and mindset shift 3.4 Experience-sharing and cultural adaptation |
Police officer 03; 05; 07 | Emotional intelligence and self-regulation are viewed as key coping mechanisms. Cultural practices such as tea gatherings and mentorship from experienced officers help younger officers adapt and grow. |
Figure 4.
Culturally embedded informal support mechanisms.
5. Conclusion and Suggestions
5.1. Research Conclusion
This study explored the inhibitory control processes of police officers under different stress conditions through a literature analysis and semi-structured in-depth interviews. The goal was to better understand how officers adjust to cognitive and emotional conflict, and how they regulate aggressive behavior and psychological responses during social interaction.
The first significant finding of this study indicates that stress and emotional regulation may serve as crucial foundations for suppressing impulsive and aggressive behavior. This insight holds potential for application in pre-service police education and early intervention training. For instance, training programs targeting inhibitory functions may help reduce the risk of impulsive actions during duty.
The second key finding addresses the challenges police officers face in stress coping and emotional regulation. The study provides recommendations at the organizational level. Interviewees generally agreed that personal psychological traits and emotional regulation abilities should be considered during recruitment. Once employed, institutions should offer more flexible leisure options and stress-relief mechanisms to reduce the accumulation of negative emotions instigated by workplace stress.
Based on the findings, this study proposes the following practical applications:
- Screening mechanism for new recruits: We recommend the incorporating the assessments of emotional regulation abilities into the recruitment process to identify individuals prone to emotional dysregulation early while offering adequate psychological counseling and training resources.
- Intervention for officers exhibiting aggressive behavior: For officers who have exhibited violent or emotionally dysregulated behavior during duty, we recommend the use of EEG testing and psychological evaluations to implement follow-up counseling and behavioral adjustment training.
- Monitoring and preventive measures for general officers: To understand the mental and emotional states of general officers, institutions should periodically conduct stress sampling and psychological stability assessments. This allows for timely support measures to strengthen resilience and workplace adaptability.
5.2. Research Suggestions
This study investigated the inhibitory control processes and emotional regulation mechanisms among police officers. Based on the findings, we propose two primary areas of practical application: “Screening and Prevention Mechanisms” and “Stress Reduction and Support Strategies.” These suggestions are intended to guide police agencies in the planning of recruitment systems, training programs, and psychological support policies.
5.2.1. Enhancing Officer Selection and Impulse Control Prevention Mechanisms
- Application Model Aligned with the Research Hypotheses
Based on observations of electrophysiological and behavioral indicators, the study identifies officers’ response patterns in the “decision phase” (e.g., choosing the degree of punishment) and the “outcome phase” (e.g., processing competitive feedback) as valuable references for assessing the physiological and psychological mechanisms linked to aggression under varying decision-making scenarios.
- 2.
- Strategies for Preventing Impulsive and Aggressive Behavior
Constructing a “Self-Control Capacity Screening Framework” is recommended to better understand officers’ ability to manage emotional conflict and behavioral reactions in situations involving provocation and pressure. This framework should incorporate emotional regulation training and physiological response assessment tools to prevent emotional dysregulation and aggression during high-stress duties.
5.2.2. Establishing a Stress Reduction and Psychological Support System for Officers
Given the high stakes, high tension, and uncertainty of police work, officers are prone to stress-induced reactions such as anxiety, depression, and emotional exhaustion. To address this issue, a multi-level institutional support strategy is proposed as follows:
- Institutional Care Mechanism
Drawing from pandemic response models, agencies could establish a “Mental Health Service Task Force” coordinated by senior administrative leaders. This task force would oversee mental health promotion for officers, ensure cross-departmental coordination, and implement timely response and support services.
- 2.
- Tiered Psychological Support Services
We recommend establishing various intervention programs, including preliminary physical and mental health screenings, supervisor interviews, psychological referrals, thematic seminars, and individual or group psychological support services. This should include differentiated care based on officers’ risk levels (e.g., confirmed cases, close contacts, and those at high risk of stress).
- 3.
- Strengthening Supervisors’ Proactive Support Role
Supervisors should conduct regular visits to frontline units, express genuine concern for officers’ emotional and physical well-being, listen to their challenges, and ensure the availability of support resources. Such actions contribute to a sense of organizational care and psychological safety, thereby boosting morale and trust.
- 4.
- Improving Leave Policies and Stress-Relief Facilities
Recruitment and promotion systems should consider candidates’ psychological traits and stress adaptability. After employment, flexible leave policies and diverse recreational facilities (e.g., gym access, leisure spaces) should be provided to help officers decompress. For those showing signs of emotional distress, additional flexible or supplementary leave options should be offered to support their mental and physical recovery.
Table 5.
Summary of policy recommendations.
| Policy Dimension | Specific Recommendation | Application Description | |
|---|---|---|---|
| 1 | Screening and Prevention Mechanisms | Introduce behavioral and physiological screening tools for emotional and impulse control. | Conduct timely assessments during the recruitment phase to identify candidates with higher emotional risk. |
| 2 | Preventing Impulsive and Aggressive Behavior | Develop training programs on emotional regulation and aggression inhibition for officers. | Incorporate pre-service education and training to enhance self-regulation under provocation. |
| 3 | Organizational Psychological Support System | Establish a Mental Health Task Force led by senior management. | Facilitate cross-departmental collaboration to implement mental health promotion and crisis response. |
| 4 | Tiered Psychological Care Services | Offer a range of services: physical and mental screenings, supervisor care, and individual/group support. | Tailor the intensity of services based on officers’ stress risk level to enhance effectiveness and relevance. |
| 5 | Leadership Support and On-Site Care | Supervisors should conduct regular visits and respond to officers’ emotional and physical needs. | Demonstrates organizational care and backup, reducing burnout and turnover risks. |
| 6 | Leave Policy and Facility Enhancement | Improve access to fitness facilities and design flexible leave policies. | Provide stress relief resources to help officers maintain mental-physical balance and duty stability. |
Author Contributions
Conceptualization, W.L.H.; methodology, W.L.H.; software, W.L.H.; validation, W.L.H.; formal analysis, W.L.H.; investigation, W.L.H.; resources, W.L.H.; data curation, W.L.H.; writing—original draft preparation, W.L.H.; writing—review and editing, W.L.H.; visualization, W.L.H.; supervision, W.L.H.; project administration, W.L.H.; funding acquisition, W.L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of National Chung Cheng University (approval number: CCUREC110042901). This research was conducted in compliance with ethical standards and approved by the Institutional Review Board (IRB) of National Chung Cheng University (approval number: CCUREC110042901). All participants provided written informed consent prior to their participation. Confidentiality and privacy were strictly maintained throughout the research process.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy and ethical considerations.
Acknowledgments
The author would like to express sincere gratitude to all police officers who participated in this study for their valuable time, openness, and insightful contributions.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ELS | Early life stress |
| PFC | Prefrontal cortex |
| OFC | orbitofrontal cortex |
| CCTV | closed-circuit television |
| EQ | emotional quotient |
References
- Juang, Y.S.; Lo, S.C. Impact of leadership styles and working stress on job satisfaction - a case study of police divisions in Hsinchu county. Ling Tung J 2020, 46, 85–123. [Google Scholar]
- Lin, Y.C.; Wu, T.C.; Huang, C.Y. Research on the relationship between police work stress and leisure involvement, health status and quality of life - take Madou police precinct of Tainan City as example. J Sport Health Leis 2018, 9, 81–90. [Google Scholar]
- Chiu, S.C.; Chou, C.W. The Study on job burnout, personal accomplishment and job satisfaction of police officers during the period of Covid-19. J Police Manag 2022, 18, 217–237. [Google Scholar]
- Lu, W.S.; Hong, Y.H. A Research on work-family conflict of criminal investigation police officers. J Police Manag 2017, 13, 39–55. [Google Scholar]
- Sun, Y.H.; Chen, C.C. Policeman stressors and coping strategies. J Police Manag 2015, 10, 103–126. [Google Scholar]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; Tan, H.; Kang, L.; Yao, L.; Huang, M.; Wang, H.; Wang, G.; Liu, Z.; Hu, S. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Xu, J.; Xu, Q.-H.; Wang, C.-M.; Wang, J. Psychological status of surgical staff during the COVID-19 outbreak. Psychiatry Res 2020, 288, 112955. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; Zhang, J.; Liu, Z.; Zhang, B. Survey of insomnia and related social psychological factors among medical staff involved in the 2019 novel coronavirus disease outbreak. Front Psychiatry 2020, 11, 306. [Google Scholar] [CrossRef]
- Chew, N.W.; Lee, G.K.; Tan, B.Y.; Jing, M.; Goh, Y.; Ngiam, N.J.; Yeo, L.L.; Ahmad, A.; Khan, F.A.; Napolean Shanmugam, G.; Sharma, A.K.; Komalkumar, R.N.; Meenakshi, P.V.; Shah, K.; Patel, B.; Chan, B.P.L.; Sunny, S.; Chandra, B.; Ong, J.J.Y.; Paliwal, P.R.; Wong, L.Y.H.; Sagayanathan, R.; Chen, J.T.; Ying Ng, A.Y.; Teoh, H.L.; Tsivgoulis, G.; Ho, C.S.; Ho, R.C.; Sharma, V.K. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun 2020, 88, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.L. My Pet Stress Monster: An Illustrated Commentary. Master’s thesis, Department of Visual Communication Design, Ming Chi University of Technology, New Taipei City, 2019.
- Greenberg, M.A.; Wortman, C.B.; Stone, A.A. Emotional expression and physical health: Revising traumatic memories or fostering self-regulation? J Pers Soc Psychol 1996, 71, 588–602. [Google Scholar] [CrossRef]
- Anda, R.F.; Croft, J.B.; Felitti, V.J.; Nordenberg, D.; Giles, W.H.; Williamson, D.F.; Giovino, G.A. Adverse childhood experiences and smoking during adolescence and adulthood. JAMA 1999, 282, 1652–1658. [Google Scholar] [CrossRef]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. Eur Arch Psychiatry Clin Neurosci 2006, 256, 174–186. [Google Scholar] [CrossRef]
- Anda, R.F.; Felitti, V.J.; Walker, J.; Whitfield, C.; Bremner, J.D.; Perry, B.D.; Dube, S.R.; Giles, W.H. The relationship of adverse childhood experiences to adult health, well-being, social function, and health care. In The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic, Lanius, R., Vermetten, E., Pain C., Eds.; Cambridge University Press: Cambridge, U.K, 2007; pp. 77–87. [Google Scholar]
- Chapman, D.P.; Whitfield, C.L.; Felitti, V.J.; Dube, S.R.; Edwards, V.J.; Anda, R.F. Adverse childhood experiences and the risk of depressive disorders in adulthood. J Affect Disord 2004, 82, 217–225. [Google Scholar] [CrossRef]
- Cutrona, C.E.; Wallace, G.; Wesner, K.A. Neighborhood characteristics and depression: An examination of stress processes. Curr Dir Psychol Sci 2006, 15, 188–192. [Google Scholar] [CrossRef]
- Dong, M.; Anda, R.F.; Felitti, V.J.; Dube, S.R.; Williamson, D.F.; Thompson, T.J.; Loo, C.M.; Giles, W.H. The interrelatedness of multiple forms of childhood abuse, neglect, and household dysfunction. Child Abuse Negl 2004, 28, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Edwards, V.J.; Holden, G.W.; Felitti, V.J.; Anda, R.F. Relationship between multiple forms of childhood maltreatment and adult mental health in community respondents: Results from the adverse childhood experiences study. Am J Psychiatry 2003, 160, 1453–1460. [Google Scholar] [CrossRef]
- Pirkola, S.; Isometsä, E.; Aro, H.; Kestilä, L.; Hamalainen, J.; Veijola, J.; Kiviruusu, O.; Lönnqvist, J. Childhood adversities as risk factors for adult mental disorders: Results from the Health 2000 Study. Soc Psychiatry Psychiatr Epidemiol 2005, 40, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Dube, S.R.; Anda, R.F.; Felitti, V.J.; Chapman, D.P.; Williamson, D.F.; Giles, W.H. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: Findings from the adverse childhood experiences study. JAMA 2001, 286, 3089–3096. [Google Scholar] [CrossRef] [PubMed]
- Anda, R.F.; Butchart, A.; Felitti, V.J.; Brown, D.W. Building a Framework for global surveillance of the public health implications of adverse childhood experience. Am J Prev Med 2010, 39, 93–98. [Google Scholar] [CrossRef]
- Brown, D.W.; Anda, R.F.; Tiemeier, H.; Felitti, V.J.; Edwards, V.J.; Croft, J.B.; Giles, W.H. Adverse childhood experiences and the risk of premature mortality. Am J Prev Med 2009, 37, 389–396. [Google Scholar] [CrossRef]
- Ivancevich, T.M.; Matteson, M.T. Stress and Work: A Managerial Perspective, Scott, Foresman & Cony: Glenview. IL, U.S.A., 1980.
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping, Springer: New York, U.S.A., 1984.
- Compas, B.E.; Connor-Smith, J.K.; Saltzman, H.; Thomsen, A.H.; Wadsworth, M.E. Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychol Bull 2001, 127, 87–127. [Google Scholar] [CrossRef] [PubMed]
- Vîrgă, D.M.; Baciu, E.-L.; Lazăr, T.-A.; Lupșa, D. Psychological capital protects social workers from burnout and secondary traumatic stress. Sustainability 2020, 12, 2246. [Google Scholar] [CrossRef]
- Secosan, I.; Bredicean, C.; Crainiceanu, Z.P.; Virga, D.; Giurgi-Oncu, C.; Bratu, T. Mental health in emergency medical clinicians: burnout, STS, sleep disorders. A cross-sectional descriptive multicentric study. Central Eur Ann Clin Res 2019, 1, 1. [Google Scholar] [CrossRef]
- Bride, B.E. Prevalence of secondary traumatic stress among social workers. Soc Work 2007, 52, 63–70. [Google Scholar] [CrossRef]
- Colombo, L.; Emanuel, F.; Zito, M. Secondary traumatic stress: Relationship with symptoms, exhaustion, and emotions among cemetery workers. Front Psychol 2019, 10, 633. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Kim, Y.J. Secondary traumatic stress and burnout of North Korean refugees service providers. Psychiatry Investig 2017, 14, 118–125. [Google Scholar] [CrossRef]
- Wollf, H.G. Stress and Disease, Charles C. Thomas., Ed.; Charles C. Thomas, Publisher: Springfield, IL., U.S.A, 1953. [Google Scholar]
- Engel, G.L. Studies of ulcerative colitis. III. The nature of the psychologic processes. Am J Med 1955, 19, 231–256. [Google Scholar] [CrossRef]
- Leshan, L. An emotional life-history pattern associated with neoplastic disease. Ann N Y Acad Sci 1966, 125, 780–793. [Google Scholar] [CrossRef]
- Friedman, M.; Rosenman, R.H. Type A behavior and your heart. Knopf: New York, U.S.A., 1974.
- Carver, C.S.; Scheier, M.E.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J Pers Soc Psychol 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Wahlund, K.; Kristiansson, M. Aggression and the brain: The role of the frontal lobes. Int J Law Psychiatry 2009, 32, 229–234. [Google Scholar]
- Roth, G.; Strüber, D. Neurobiological aspects of reactive and proactive violence in antisocial individuals. Praxis der Rechtspsychologie 2008, 58, 587–600. [Google Scholar]
- Crowe, S.L.; Blair, R.J.R. The development of antisocial behavior: What can we learn from functional neuroimaging studies? Dev Psychopathol 2008, 20, 1145–1159. [Google Scholar] [CrossRef]
- Nelson, R.J.; Trainor, B.C. Neural mechanisms of aggression. Nat Rev Neurosci 2007, 8, 536–546. [Google Scholar] [CrossRef]
- Blair, R.J.R.; Peschardt, K.S.; Budhani, S.; Mitchell, D.G.V.; Pine, D.S. The development of psychopathy. J Child Psychol Psychiatry 2006, 47, 262–275. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.; Victoroff, J. Understanding human aggression: New insights from neuroscience. Int J Law Psychiatry 2009, 32, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, J.A.; Smithmyer, C.M.; Ramsden, S.R.; Parker, E.H.; Flanagan, K.D.; Dearing, K.F.; Relyea, N.; Simons, R.F. Observational, physiological, and self-report measures of children’s anger: Relations to reactive versus proactive aggression. Child Dev 2002, 73, 1101–1118. [Google Scholar] [CrossRef] [PubMed]
- Ostrov, J.M.; Houston, R.J. The utility of forms and functions of aggression in emerging adulthood: Association with personality disorder symptomatology. J Youth Adolesc 2008, 37, 1147–1158. [Google Scholar] [CrossRef]
- Sansone, R.A.; Sansone, L.A. Borderline personality and externalized aggression. Innov Clin Neurosci 2009, 6, 16–20. [Google Scholar]
- Mancke, F.; Herpertz, S.C.; Bertsch, K. Aggression in borderline personality disorder: A multidimensional model. Personal Disord 2015, 6, 278–291. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual Res Psychol 2006, 3, 77–101. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



