Submitted:
27 November 2025
Posted:
27 November 2025
You are already at the latest version
Abstract
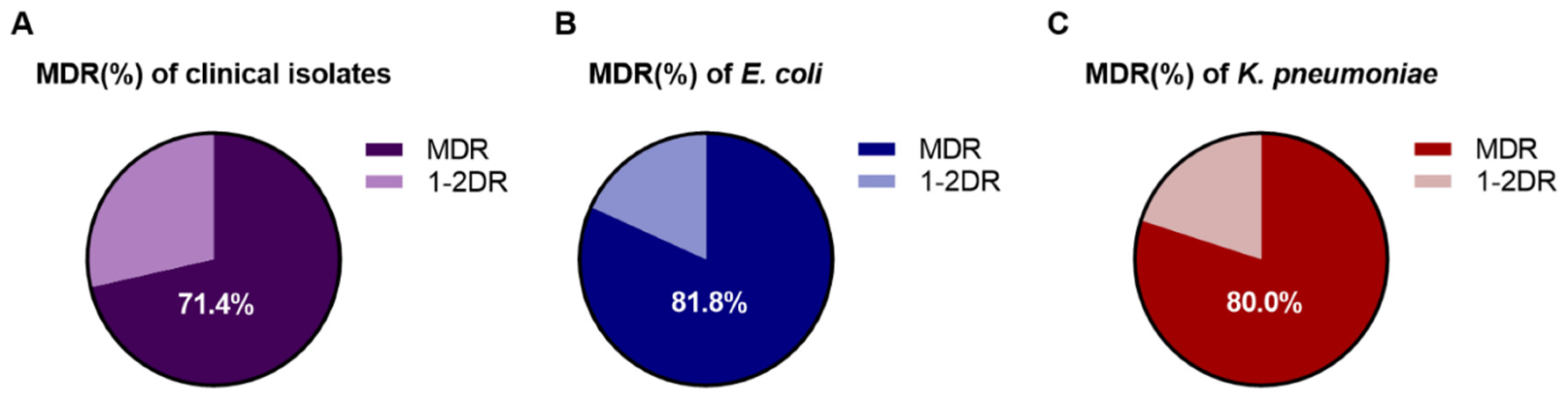
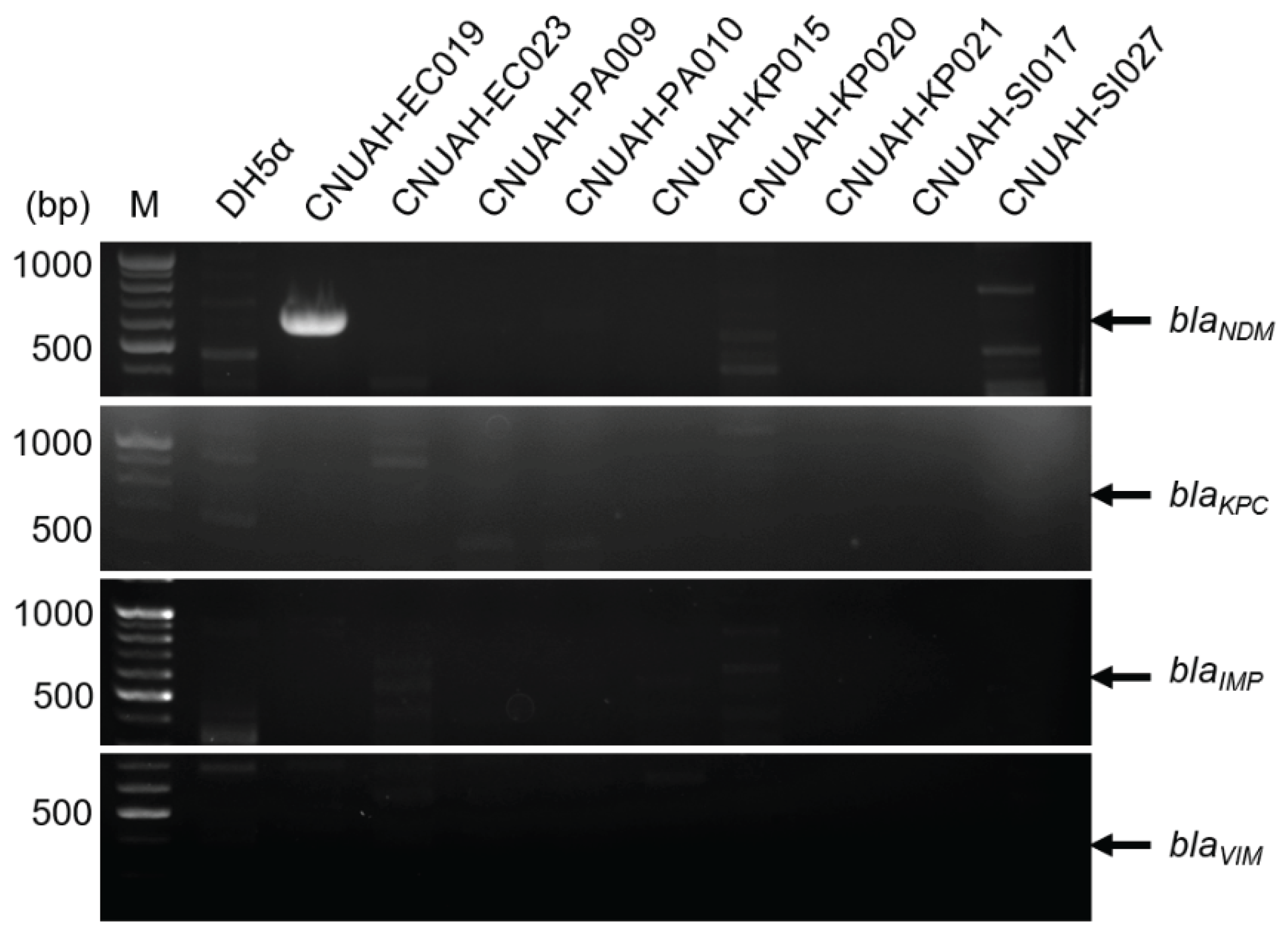
Emerging antimicrobial resistance (AMR) in companion animals represents a global health concern as they serve as potential reservoirs for multidrug-resistant (MDR) bacteria, which can be transmitted to humans. Herein, we provide comprehensive surveillance data on resistance patterns in veterinary hospital settings, focusing on urinary tract infection. A total of 23 bacterial strains were isolated from urine specimens of hospitalized companion animals suspected of UTI between 2022 and 2024. 16S rRNA sequencing analysis revealed that Escherichia coli (47.8%), Klebsiella pneumoniae (21.7%), and Pseudomonas aeruginosa (8.7%) were predominant uropathogens. Minimum inhibitory concentration and minimum bactericidal concentration tests were employed to analyze AMR patterns across different classes of antibiotics. Moreover, antimicrobial susceptibility test exhibited 73.91% MDR according to the standard definition given by the Clinical and Laboratory Standards Institute (CLSI) M100 guidelines. Most Gram-negative bacteria have been shown to be resistant to beta-lactam antibiotics, especially carbapenems. Notably, an E. coli strain was confirmed to possess the blaNDM-1 gene encoding the carbapenemase New Delhi metallo-β-lactamase. These findings support the implementation of targeted infection control measures and evidence-based treatment protocols to preserve antimicrobial efficacy in companion animal medicine to minimize potential public health risks through the One Health approach.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Antibiotic Discs
2.2. Sample Collection and Clinical Information
2.3. Identification of Bacterial Strains
2.4. Antimicrobial Susceptibility Test
2.5. Minimum Inhibitory Concentration (MIC) and Minimum Bactericidal Concentration (MBC)
2.6. Polymerase Chain Reaction
3. Results
3.1. Isolation of Bacterial Strains in Urine Specimens
3.2. Characterization of the Antibiotic Resistance Profile of the Gram-Negative Strains
3.3. Carbapenemase Gene-Harboring Isolates
3.4. MIC and MBC of All Bacterial Strains
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AMR | Antimicrobial resistance |
| CLSI | Clinical and laboratory standards institute |
| CRE | Carbapenem-resistant Enterobacterales |
| ESBL | Extended-spectrum beta-lactamase |
| HGT | Horizontal gene transfer |
| MBC | Minimum bactericidal concentration |
| MIC | Minimum inhibitory concentration |
| MDR | Multidrug-resistant |
| MHA MHB |
Mueller-Hinton agar Mueller-Hinton broth |
| 3GCRE | Third-generation cephalosporin-resistant |
| UTIs | Urinary tract infections |
| UPEC | Uropathogenic E. coli |
| WHO XDR |
World Health Organization Extensive drug-resistance |
References
- Collaborators, G. 2.A.R. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet 2024, 404, 1199–1226. [Google Scholar] [CrossRef]
- WHO Bacterial Priority Pathogens List 2024: Bacterial Pathogens of Public Health Importance, to Guide Research, Development, and Strategies to Prevent and Control Antimicrobial Resistance. 1st ed. Geneva: World Health Organization; 2024.
- Marques, C.; Belas, A.; Aboim, C.; Cavaco-Silva, P.; Trigueiro, G.; Gama, L.T.; Pomba, C. Evidence of Sharing of Klebsiella pneumoniae Strains between Healthy Companion Animals and Cohabiting Humans. J. Clin. Microbiol. 2019, 57. [Google Scholar] [CrossRef] [PubMed]
- Hernando, E.; Vila, A.; D'IPpolito, P.; Rico, A.; Rodon, J.; Roura, X. Prevalence and Characterization of Urinary Tract Infection in Owned Dogs and Cats From Spain. Top. Companion Anim. Med. 2021, 43, 100512. [Google Scholar] [CrossRef]
- Caddey, B.; Fisher, S.; Barkema, H.W.; Nobrega, D.B. Companions in antimicrobial resistance: examining transmission of common antimicrobial-resistant organisms between people and their dogs, cats, and horses. Clin. Microbiol. Rev. 2025, 38, e0014622. [Google Scholar] [CrossRef]
- Monteiro, H.I.G.; Silva, V.; de Sousa, T.; Calouro, R.; Saraiva, S.; Igrejas, G.; Poeta, P. Antimicrobial Resistance in European Companion Animals Practice: A One Health Approach. Animals 2025, 15, 1708. [Google Scholar] [CrossRef]
- Castillo-Ramírez, S.; Aguilar-Vera, A.; Kumar, A.; Evans, B. Acinetobacter baumannii : much more than a human pathogen. Antimicrob. Agents Chemother. 2025, 69, e0080125. [Google Scholar] [CrossRef]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef]
- Rantala, M.; Huovinen, P.; Hölsö, K.; Lilas, A.; Kaartinen, L. Survey of condition-based prescribing of antimicrobial drugs for dogs at a veterinary teaching hospital. Veter- Rec. 2004, 155, 259–262. [Google Scholar] [CrossRef]
- De Briyne, N.; Atkinson, J.; Borriello, S.P.; Pokludová, L. Antibiotics used most commonly to treat animals in Europe. Vet. Rec. 2014, 175, 325. [Google Scholar] [CrossRef]
- Weese, J.S.; Blondeau, J.; Boothe, D.; Guardabassi, L.G.; Gumley, N.; Papich, M.; Jessen, L.R.; Lappin, M.; Rankin, S.; Westropp, J.L.; et al. International Society for Companion Animal Infectious Diseases (ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Veter- J. 2019, 247, 8–25. [Google Scholar] [CrossRef]
- Mazzariol, A.; Bazaj, A.; Cornaglia, G. Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: a review. J. Chemother. 2017, 29, 2–9. [Google Scholar] [CrossRef]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Kranz, J.; Bartoletti, R.; Bruyère, F.; Cai, T.; Geerlings, S.; Köves, B.; Schubert, S.; Pilatz, A.; Veeratterapillay, R.; E Wagenlehner, F.M.; et al. European Association of Urology Guidelines on Urological Infections: Summary of the 2024 Guidelines. Eur. Urol. 2024, 86, 27–41. [Google Scholar] [CrossRef]
- Hawkey, J.; Wyres, K.L.; Judd, L.M.; Harshegyi, T.; Blakeway, L.; Wick, R.R.; Jenney, A.W.J.; Holt, K.E. ESBL plasmids in Klebsiella pneumoniae: diversity, transmission and contribution to infection burden in the hospital setting. Genome Med. 2022, 14, 1–13. [Google Scholar] [CrossRef]
- Seo, Y.-R.; Choi, S.-Y.; Kim, S.; Kang, K.-S.; Ro, C.-S.; Hyeon, J.-Y. Antimicrobial resistance profiles of Staphylococcus spp. and Escherichia coli isolated from dogs and cats in Seoul, South Korea during 2021–2023. Front. Veter- Sci. 2025, 12, 1563780. [Google Scholar] [CrossRef] [PubMed]
- Wei, A.Y.; Thompson, M.F.; Worthing, K.A.; Venturini, C.; Brookes, V.J.; Norris, J.M. Frequency and antimicrobial susceptibility profiles of bacterial species isolated from canine and feline urine samples in Sydney, Australia, 2012–2021. Veter- Microbiol. 2025, 306, 110541. [Google Scholar] [CrossRef]
- Feuer, L.; Frenzer, S.K.; Merle, R.; Bäumer, W.; Lübke-Becker, A.; Klein, B.; Bartel, A. Comparative Analysis of Methicillin-Resistant Staphylococcus pseudintermedius Prevalence and Resistance Patterns in Canine and Feline Clinical Samples: Insights from a Three-Year Study in Germany. Antibiotics 2024, 13, 660. [Google Scholar] [CrossRef]
- da Silva, J.M.; Menezes, J.; Marques, C.; Pomba, C.F. Companion Animals—An Overlooked and Misdiagnosed Reservoir of Carbapenem Resistance. Antibiotics 2022, 11, 533. [Google Scholar] [CrossRef]
- Sellera, F.P.; Fernandes, M.R.; Ruiz, R.; Falleiros, A.C.M.; Rodrigues, F.P.; Cerdeira, L.; Lincopan, N. Identification of KPC-2-producing Escherichia coli in a companion animal: a new challenge for veterinary clinicians. J. Antimicrob. Chemother. 2018, 73, 2259–2261. [Google Scholar] [CrossRef]
- Kyung, S.M.; Choi, S.-W.; Lim, J.; Shim, S.; Kim, S.; Bin Im, Y.; Lee, N.-E.; Hwang, C.-Y.; Kim, D.; Yoo, H.S. Comparative genomic analysis of plasmids encoding metallo-β-lactamase NDM-5 in Enterobacterales Korean isolates from companion dogs. Sci. Rep. 2022, 12, 1–9. [Google Scholar] [CrossRef]
- Park, C.; Kim, S.B.; Choi, S.H.; Kim, S. Comparison of 16S rRNA Gene Based Microbial Profiling Using Five Next-Generation Sequencers and Various Primers. Front Microbiol. 2021, 12, 715500. [Google Scholar] [CrossRef] [PubMed]
- Doyle, D.; Peirano, G.; Lascols, C.; Lloyd, T.; Church, D.L.; Pitout, J.D.D. Laboratory Detection of Enterobacteriaceae That Produce Carbapenemases. J. Clin. Microbiol. 2012, 50, 3877–3880. [Google Scholar] [CrossRef] [PubMed]
- Saputra, S.; Jordan, D.; Mitchell, T.; Wong, H.S.; Abraham, R.J.; Kidsley, A.; Turnidge, J.; Trott, D.J.; Abraham, S. Antimicrobial resistance in clinical Escherichia coli isolated from companion animals in Australia. Veter- Microbiol. 2017, 211, 43–50. [Google Scholar] [CrossRef]
- Leite-Martins, L.R.; Mahú, M.I.; Costa, A.L.; Mendes, Â.; Lopes, E.; Mendonça, D.M.; Niza-Ribeiro, J.J.; de Matos, A.J.; da Costa, P.M. Prevalence of antimicrobial resistance in enteric Escherichia coli from domestic pets and assessment of associated risk markers using a generalized linear mixed model. Prev. Veter- Med. 2014, 117, 28–39. [Google Scholar] [CrossRef]
- Hernandez, J.; Bota, D.; Farbos, M.; Bernardin, F.; Ragetly, G.; Médaille, C. Risk factors for urinary tract infection with multiple drug-resistant Escherichia coli in cats. J. Feline Med. Surg. 2013, 16, 75–81. [Google Scholar] [CrossRef]
- Marques, C.; Gama, L.T.; Belas, A.; Bergström, K.; Beurlet, S.; Briend-Marchal, A.; Broens, E.M.; Costa, M.; Criel, D.; Damborg, P.; et al. European multicenter study on antimicrobial resistance in bacteria isolated from companion animal urinary tract infections. BMC Veter- Res. 2016, 12, 1–17. [Google Scholar] [CrossRef]
- Rampacci, E.; Bottinelli, M.; Stefanetti, V.; Hyatt, D.R.; Sgariglia, E.; Coletti, M.; Passamonti, F. Antimicrobial susceptibility survey on bacterial agents of canine and feline urinary tract infections: Weight of the empirical treatment. J. Glob. Antimicrob. Resist. 2018, 13, 192–196. [Google Scholar] [CrossRef]
- Fonseca, J.D.; Mavrides, D.E.; Graham, P.A.; McHugh, T.D. Results of urinary bacterial cultures and antibiotic susceptibility testing of dogs and cats in the UK. 2021. [Google Scholar] [CrossRef]

| Strains | Species | Specimen | Breeds | Age | Sex |
|---|---|---|---|---|---|
| CNUAH-EC002 | Escherichia coli | Urine | Maltese | 16y | SF |
| CNUAH-EC003 | Escherichia coli | Urine | Jindo | 9y | SF |
| CNUAH-EC004 | Escherichia coli | Urine | Mixed | 9y | SF |
| CNUAH-EC005 | Escherichia coli | Urine | Labrador retriever | 11y | SF |
| CNUAH-EC019 | Escherichia coli | Urine | Jindo | 12y | SF |
| CNUAH-EC023 | Escherichia coli | Urine | Mixed | 7y | SF |
| CNUAH-EC025 | Escherichia coli | Urine | Yorkshire terrier | 12y | SF |
| CNUAH-EC026 | Escherichia coli | Urine | Shiba Inu | 6y | SF |
| CNUAH-EC029 | Escherichia coli | Urine | Welsh Corgi | 8y | CM |
| CNUAH-EC030 | Escherichia coli | Urine | Spitz | 7y | CM |
| CNUAH-EC031 | Escherichia coli | Urine | Maltese | 15y | SF |
| CNUAH-KP014 | Klebsiella pneumoniae | Urine | Mixed | 12y | M |
| CNUAH-KP015 | Klebsiella pneumoniae | Urine | Mixed | 12y | M |
| CNUAH-KP020 | Klebsiella pneumoniae | Urine | Mixed | 5y | SF |
| CNUAH-KP021 | Klebsiella pneumoniae | Urine | Mixed | 14y | SF |
| CNUAH-KP022 | Klebsiella pneumoniae | Urine | Mixed | 14y | SF |
| CNUAH-PA009 | Pseudomonas aeruginosa | Urine | Mixed | 13y | SF |
| CNUAH-PA010 | Pseudomonas aeruginosa | Urine | Mixed | 13y | CM |
| CNUAH-PM028 | Proteus mirabilis | Urine | Maltese | 13y | SF |
| CNUAH-SF024 | Shigella flexneri | Urine | Beagle | 7y | SF |
| CNUAH-EH032 | Enterobacter hormaechei | Urine | Yorkshire terrier | 8y | M |
| CNUAH-SI017 | Staphylococcus pseudintermedius | Urine | Jindo | 12y | SF |
| CNUAH-SI027 | Staphylococcus pseudintermedius | Urine | Maltese | 13y | SF |
| Antibiotics | Resistance (%) | |||
|---|---|---|---|---|
| Total (n = 21) |
E. coli (n = 11) |
K. pneumoniae (n = 5) |
P. aeruginosa (n = 2) |
|
| Amikacin | 0.0 | 0.0 | 0.0 | 0.0 |
| Gentamicin | 9.5 | 18.2 | 0.0 | 0.0 |
| Kanamycin | 23.8 | 27.3 | 0.0 | 100 |
| Streptomycin | 47.6 | 36.4 | 60 | 100 |
| Tobramycin | 4.7 | 9.1 | 0.0 | 0.0 |
| Ampicillin | 90.4 | 90.9 | 100 | 100 |
| Amoxicillin/Clavulanic Acid | 90.4 | 90.9 | 100 | 100 |
| Ampicillin/Sulbactam | 80.9 | 81.8 | 100 | 100 |
| Cefazolin | 76.2 | 81.8 | 60 | 100 |
| Cefaclor | 76.2 | 81.8 | 60 | 100 |
| Cefoxitin | 47.6 | 36.4 | 60 | 100 |
| Cefuroxime | 52.3 | 63.6 | 40 | 100 |
| Cefixime | 71.4 | 81.8 | 60 | 100 |
| Cefotaxime | 47.6 | 63.6 | 20 | 100 |
| Ceftazidime | 19.0 | 36.4 | 0.0 | 0.0 |
| Ceftriaxone | 28.5 | 54.5 | 0.0 | 0.0 |
| Cefepime | 9.5 | 18.2 | 0.0 | 0.0 |
| Ertapenem | 19.0 | 18.2 | 0.0 | 100 |
| Imipenem | 4.7 | 9.1 | 0.0 | 0.0 |
| Meropenem | 23.8 | 9.1 | 60 | 0.0 |
| Aztreonam | 4.7 | 9.1 | 0.0 | 0.0 |
| Chloramphenicol | 28.5 | 9.1 | 60 | 100 |
| Ciprofloxacin | 42.8 | 45.5 | 60 | 0 |
| Colistin | 0.0 | 0.0 | 0.0 | 0.0 |
| Doxycycline | 61.9 | 45.5 | 100 | 100 |
| Tetracycline | 57.1 | 36.4 | 100 | 100 |
| Tigecycline | 9.5 | 0.0 | 0.0 | 100 |
| Nalidixic Acid | 61.9 | 45.5 | 60 | 100 |
| Azithromycin | 19.0 | 18.2 | 0.0 | 50 |
| Antibiotics | EC002 | EC003 | EC004 | EC005 | EC019 | EC023 | EC025 | EC026 | EC029 | EC030 | EC031 | KP014 | KP014 | KP020 | KP021 | KP022 | PA009 | PA010 | PM028 | SF024 | EH032 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC (μg/mL) | ||||||||||||||||||||||||||||||||||||||
| AMI | <4 | <4 | <4 | <4 | 8 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | |||||||||||||||||
| AUG2 | >8/4 | >8/4 | 8/4 | 8/4 | >8/4 | >8/4 | 2/1 | >8/4 | >8/4 | >8/4 | 2/1 | 8/4 | 4/2 | >8/4 | >8/4 | >8/4 | >8/4 | >8/4 | 1/0.5 | 2/1 | >8/4 | |||||||||||||||||
| AMP | >8 | >8 | >8 | >8 | >8 | >8 | 2 | >8 | >8 | >8 | 2 | >8 | >8 | >8 | >8 | >8 | >8 | >8 | >8 | 2 | >8 | |||||||||||||||||
| FAZ | >32 | >32 | >32 | >32 | 32 | >32 | 2 | >32 | >32 | >32 | 2 | 4 | 4 | >32 | >32 | >32 | >32 | >8 | 2 | 2 | >32 | |||||||||||||||||
| FOV | >8 | >8 | >8 | >8 | >8 | >8 | <0.25 | 8 | >8 | >8 | <0.25 | >8 | <0.25 | >8 | 8 | >8 | >8 | >8 | >8 | <0.25 | 2 | |||||||||||||||||
| POD | >8 | >8 | >8 | >8 | >8 | >8 | <1 | >8 | >8 | >8 | <1 | >8 | <1 | >8 | >8 | >8 | >8 | >8 | >8 | <1 | 4 | |||||||||||||||||
| TAZ | >16 | >16 | <4 | <4 | >16 | 16 | <4 | <4 | >16 | 16 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | >16 | >16 | >16 | |||||||||||||||||
| LEX | <0.25 | <0.25 | >2 | 2 | >2 | <0.25 | <0.25 | >16 | >16 | >16 | 8 | >2 | 8 | >16 | >16 | >16 | <0.25 | >16 | 8 | 8 | >16 | |||||||||||||||||
| CHL | 4 | <2 | 4 | <2 | 8 | 4 | 4 | <2 | 32 | 4 | 4 | 4 | 4 | >32 | >32 | >32 | 16 | 32 | 32 | <2 | 4 | |||||||||||||||||
| DOX | 1 | 1 | >8 | 8 | >8 | 1 | 0.5 | 0.5 | 8 | 1 | 1 | >8 | >8 | >8 | 8 | 8 | 1 | 8 | >8 | 0.5 | >8 | |||||||||||||||||
| ENRO | 0.25 | <0.12 | >4 | >4 | >4 | <0.12 | <0.12 | 0.25 | >4 | 0.25 | <0.12 | <0.12 | <0.12 | <0.12 | >4 | >4 | 0.25 | 0.25 | >4 | >4 | 4 | |||||||||||||||||
| GEN | 1 | 1 | >8 | >8 | >8 | 2 | 1 | 4 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | <0.25 | <0.25 | 4 | 1 | 0.5 | |||||||||||||||||
| IMI | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | |||||||||||||||||
| MAR | 0.25 | 0.25 | >4 | >4 | >4 | 0.25 | <0.12 | 0.5 | >4 | 0.25 | <0.12 | <0.12 | <0.25 | 4 | 4 | 4 | <0.25 | <0.12 | >4 | <0.25 | 2 | |||||||||||||||||
| ORB | <1 | <1 | >8 | >8 | >8 | <1 | <1 | 2 | >8 | <1 | <1 | <1 | <1 | >8 | >8 | >8 | <1 | <1 | >8 | >8 | 8 | |||||||||||||||||
| P/T4 | <8/4 | <8/4 | <8/4 | <8/4 | >64/4 | <8/4 | <8/4 | <8/4 | 16/4 | <8/4 | <8/4 | <8/4 | <8/4 | <8/4 | <8/4 | 16/4 | <8/4 | <8/4 | <8/4 | <8/4 | <8/4 | |||||||||||||||||
| PRA | <0.25 | <0.25 | >2 | 2 | >2 | >2 | <0.25 | <0.25 | >2 | >2 | <0.25 | <0.25 | <0.25 | 2 | 2 | 2 | <0.25 | <0.25 | 2 | 2 | 1 | |||||||||||||||||
| TET | <4 | <4 | >16 | >16 | >16 | <4 | <4 | <4 | >16 | <4 | <4 | >16 | >16 | >16 | >16 | >16 | <4 | 8 | >16 | <4 | >16 | |||||||||||||||||
| SXT | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | 2/38 | >4/76 | >4/76 | >4/76 | >4/76 | |||||||||||||||||
| Antibiotics | EC002 | EC003 | EC004 | EC005 | EC019 | EC023 | EC025 | EC026 | EC029 | EC030 | EC031 | KP014 | KP014 | KP020 | KP021 | KP022 | PA009 | PA010 | PM028 | SF024 | EH032 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MBC (μg/mL) | |||||||||||||||||||||
| AMI | <4 | <4 | <4 | <4 | 8 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 |
| AUG2 | >8/4 | >8/4 | >8/4 | >8/4 | >8/4 | >8/4 | 2/1 | >8/4 | >8/4 | >8/4 | 2/1 | 8/4 | 8/4 | >8/4 | >8/4 | >8/4 | >8/4 | >8/4 | 1/0.5 | 2/1 | >8/4 |
| AMP | >8 | >8 | >8 | >8 | >8 | >8 | 2 | >8 | >8 | >8 | 2 | >8 | >8 | >8 | >8 | >8 | >8 | >8 | >8 | 2 | >8 |
| FAZ | >32 | >32 | >32 | >32 | 32 | >32 | 2 | >32 | >32 | >32 | 2 | 4 | 4 | >32 | >32 | >32 | >32 | <1 | 4 | 2 | >32 |
| FOV | >8 | >8 | >8 | >8 | >8 | >8 | <0.25 | 8 | >8 | >8 | <0.25 | 0.5 | <0.25 | >8 | >8 | >8 | >8 | >8 | >8 | <0.25 | 2 |
| POD | >8 | >8 | >8 | >8 | >8 | >8 | <1 | >8 | >8 | >8 | <1 | <1 | <1 | >8 | >8 | >8 | >8 | >8 | >8 | <1 | 4 |
| TAZ | >16 | >16 | <4 | <4 | >16 | 16 | <4 | <4 | >16 | 16 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | <4 | >16 | >16 | >16 |
| LEX | <0.25 | <0.25 | >2 | 2 | >16 | <0.25 | <0.25 | >16 | >16 | >16 | 8 | 8 | 8 | >16 | >16 | >16 | >16 | >16 | 16 | 8 | >16 |
| CHL | 8 | <2 | >8 | <2 | 8 | 4 | >8 | <2 | 32 | 4 | 4 | >8 | >8 | >32 | >32 | >32 | 16 | 32 | >32 | <2 | 8 |
| DOX | 2 | 1 | >8 | 8 | >8 | 1 | >1 | 0.5 | 8 | 1 | 1 | >8 | >8 | >8 | >8 | >8 | 1 | 8 | >8 | >1 | >8 |
| ENRO | 0.5 | <0.12 | >4 | >4 | >4 | <0.12 | <0.12 | 0.25 | >4 | 0.25 | <0.12 | <0.12 | <0.12 | <0.12 | >4 | >4 | 0.25 | 0.25 | >4 | >4 | 4 |
| GEN | 2 | 1 | >8 | >8 | >8 | 2 | 1 | 4 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | <0.25 | <0.25 | 4 | 1 | 0.5 |
| IMI | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 | <1 |
| MAR | 0.25 | 0.25 | >4 | >4 | >4 | 0.25 | <0.12 | 0.5 | >4 | 0.25 | <0.12 | <0.12 | <0.12 | 4 | 4 | 4 | <0.12 | <0.12 | >4 | <0.12 | 2 |
| ORB | <1 | <1 | >8 | >8 | >8 | <1 | <1 | 2 | >8 | <1 | <1 | <1 | <1 | >8 | >8 | >8 | <1 | <1 | >8 | >8 | 8 |
| P/T4 | <8/4 | <8/4 | <8/4 | <8/4 | >64/4 | <8/4 | <8/4 | <8/4 | 32/4 | <8/4 | <8/4 | <8/4 | <8/4 | <8/4 | <8/4 | 4/16 | <8/4 | <8/4 | <8/4 | <8/4 | <8/4 |
| PRA | <0.25 | <0.25 | >2 | 2 | >2 | >2 | <0.25 | <0.25 | >2 | >2 | <0.25 | <0.25 | <0.25 | 2 | 2 | >2 | <0.25 | <0.25 | >2 | 2 | 2 |
| TET | <4 | <4 | >16 | >16 | >16 | <4 | <4 | <4 | >16 | <4 | <4 | >16 | >16 | >16 | >16 | >16 | <4 | 8 | >16 | <4 | >16 |
| SXT | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 | >4/76 |
| Antibiotics | MIC (μg/mL) | MBC (μg/mL) | ||
|---|---|---|---|---|
| SI017 | SI027 | SI017 | SI027 | |
| AMI | <16 | <16 | <16 | <16 |
| AUG2 | <0.25/0.12 | <0.25/0.12 | <0.25/0.12 | <0.25/0.12 |
| AMP | <0.25 | <0.25 | <0.25 | <0.25 |
| FAZ | <2 | <2 | <2 | <2 |
| FOV | 0.12 | 0.12 | 0.24 | 0.24 |
| POD | <2 | <2 | <2 | <2 |
| CEP | <2 | <2 | <2 | <2 |
| CHL | 16 | 16 | >32 | >32 |
| CLI | >4 | >4 | >4 | >4 |
| DOX | >0.5 | >0.5 | >0.5 | >0.5 |
| ENRO | 0.5 | 0.5 | 0.5 | 1 |
| ERY | >4 | >4 | >4 | >4 |
| GEN | <4 | <4 | <4 | <4 |
| IMI | <1 | <1 | <1 | <1 |
| MAR | <1 | <1 | <1 | <1 |
| MIN | 2 | >2 | >2 | >2 |
| NIT | <16 | 64 | <16 | 64 |
| OXA+ | <0.25 | >2 | <0.25 | >2 |
| PEN | <0.06 | 1 | <0.06 | 1 |
| PRA | <0.25 | <0.25 | <0.25 | <0.25 |
| RIF | <1 | <1 | <1 | <1 |
| TET | >1 | >1 | >1 | >1 |
| SXT | >4/76 | <2/38 | >4/76 | <2/38 |
| VAN | <1 | >16 | <1 | >16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



