
Submitted:
19 November 2025
Posted:
21 November 2025
You are already at the latest version
Abstract
Background: Diagnosing coagulopathy in sepsis remains challenging, as current Conventional scoring systems based on routine coagulation biomarkers are insufficient to predict mortality accurately. Endothelial molecular markers may improve risk stratification. Objectives: To evaluate the prognostic value of thrombin–antithrombin complex (TAT), tissue-type plasminogen activator–inhibitor complex (t-PAIC), and antithrombin (AT) activity, and to develop a unified score augmenting International Society on Thrombosis and Hemostasis (ISTH) overt-DIC criteria. Methods: In this prospective, longitudinal study, adults with Sepsis-3 presenting to the emergency department underwent serial clinical assessment, routine coagulation testing, and measurement of endothelial markers on Days 1, 3, and 7. Receiver operating characteristic (ROC) analyses screened candidate biomarkers, and multivariable logistic regression identified independent predictors of 28-day mortality. A unified score (Unified ISTH+) was constructed by adding optimal molecular markers to ISTH components and compared with ISTH, JAAM, and SIC criteria. In addition, a non-parametric bootstrap procedure was performed to assess the internal stability and empirical power of the predictive models given the modest sample size. Results: Fifty-four patients (mean age 59.6 ± 16.6 years) were included; 28-day mortality was 31.5%. TAT, t-PAIC, and AT activity were independent predictors of mortality. Individual ROC performance was high for t-PAIC (AUC 0.846), TAT (AUC 0.845), and AT (AUC 0.789). The Unified ISTH+ score achieved superior discrimination (AUC 0.856; 95% CI 0.757–0.955) versus ISTH (0.783), JAAM (0.718), and SIC (0.676), and showed the greatest net benefit on DCA across clinically relevant thresholds. Unified ISTH+-positive patients had higher SOFA/APACHE II scores and worse survival (log-rank p < 0.001). Conclusions: t-PAIC, TAT, and AT activity are strong prognostic markers in sepsis-associated coagulopathy. Incorporating them into a unified ISTH+ score improves mortality prediction versus existing criteria and may enable earlier risk stratification and clinical decision-making.
Keywords:
sepsis
; disseminated intravascular coagulation
; endothelial biomarkers
; t-PAIC
; thrombin–antithrombin complex
; antithrombin activity
1. Introduction
Sepsis is a life-threatening syndrome of dysregulated host response to infection that precipitates multiorgan dysfunction and substantial mortality [1]. It is frequently complicated by coagulopathy and endothelial dysfunction, both of which worsen outcomes. Sepsis-induced coagulopathy (SIC) reflects early, systemic activation of coagulation with endothelial perturbation and microvascular thrombosis; progression to overt disseminated intravascular coagulation (DIC) further amplifies the risk of organ failure and death[2,3]. Although coagulation disorders were traditionally viewed as late-stage complications, recent work shows that coagulation abnormalities are present across the entire course of sepsis, influencing both onset and prognosis[3].
Several bedside scoring systems are used to identify coagulopathy in sepsis, each with important limitations. The ISTH overt-DIC criteria include hypofibrinogenemia, which is relatively uncommon in septic DIC and may reduce sensitivity [4] The JAAM DIC score incorporates systemic inflammatory response syndrome (SIRS) elements whose relevance has diminished under Sepsis-3 definitions[5,6]. More recently, the SIC criteria were introduced to enable earlier recognition[7],however, while sensitivity for early mortality is improved, specificity remains limited. Thus, current systems do not consistently capture the dynamic pathophysiology of sepsis-associated coagulopathy or provide robust prognostic discrimination.
An additional limitation is that these criteria largely omit indices of cellular injury, endogenous anticoagulants, and the fibrinolytic–antifibrinolytic balance, despite their recognized roles in sepsis-related coagulopathy[8]. Endothelial biomarkers—such as tissue-type plasminogen activator–inhibitor complex (t-PAIC) and soluble thrombomodulin (sTM)—have been associated with organ failure and death[8,9]. Similarly, hemostatic molecular markers including thrombin–antithrombin (TAT) complex, plasmin–α2-plasmin inhibitor complex (PIC), and the endogenous anticoagulant antithrombin (AT) provide early mechanistic signals of dysregulated coagulation and have demonstrated prognostic relevance[9,10].These markers illuminate the thromboinflammatory processes that conventional scores may overlook[8],
Accordingly, there is growing consensus that DIC should not be viewed as a static, terminal event but rather as a continuum from compensated hypercoagulability (SIC) to decompensated overt DIC[11]. Integrating molecular markers into established frameworks may bridge the gap between pathophysiology and clinical scoring, thereby enhancing early recognition, refining risk stratification, and improving outcome prediction. In this context, the present study evaluates the prognostic value of hemostatic and endothelial markers for 28-day mortality and developed a unified, ISTH-based score that augments conventional criteria with selected molecular markers.
2. Materials and Methods
2.1. Study Design and Setting
The Patients were enrolled from the Emergency department of West China hospital, Sichuan University, from July 2021 to December 2023, as part of a multicenter prospective observational study that evaluated early diagnosis of sepsis using coagulation and cell damage markers. The inclusion criteria were patients who met the Sepsis-3.0 criteria on admission and were >18 years of age. Patients were included only if baseline routine and central laboratory data for DIC determination were available. Exclusion criteria included: history of hematologic disorders; coagulation-related disorders such as heparin-induced thrombocytopenia or thrombotic thrombocytopenic purpura; concomitant malignancies; antiphospholipid syndrome; trauma, intoxication, or pregnancy; cirrhosis Child-Pugh class C; thrombophilia disorders (antithrombin, protein S, or protein C deficiency); prior anticoagulant therapy (warfarin, dabigatran, rivaroxaban, heparin/low-molecular-weight heparin); incomplete data; poor compliance due to psychiatric or other illnesses; and refusal to provide informed consent. All patients received anti-infective treatment and fluid resuscitation according to the 2016 “Surviving Sepsis Campaign (SSC) guidelines[12]. with adjunctive therapies including antithrombin, glucocorticoids, immunoglobulin, and hemoperfusion in severe cases. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University. 2021 Review (No. 800). Informed consent was obtained from all patients or next of kin if patients were unconscious.
2.2. Data Collection and Biomarker Measurements
At enrollment Day 1 and on Days 3 and 7, baseline demographics including age, gender, site of infection, underlying medical history, complete blood count, C-reactive protein (CRP), procalcitonin (PCT), liver function, and kidney function panels were recorded. Coagulation indices including PT, APTT and FIB were assayed using the CS-2100i automatic coagulation analyzer (Sysmex, Japan). For endothelial/hemostatic biomarkers, 2–3 mL of venous blood was drawn into 3.2% sodium-citrate tubes (BD Vacutainer, UK). Samples were centrifuged at 1,500 × g for 10 min at 4 °C; the plasma supernatant was aliquoted in 500 µL portions and stored at −70 °C until batch analysis. On the assay day, frozen aliquots were thawed once in a 37 °C water bath for 5 min and analyzed immediately. Levels of soluble thrombomodulin (sTM), tissue-type plasminogen activator–inhibitor complex (t-PAIC), thrombin–antithrombin (TAT) complex, and plasmin–α2-plasmin inhibitor complex (PIC) were determined by chemiluminescence immunoassay on HISCL automated analyzers (Sysmex, Japan) using the corresponding manufacturer assay kits and instructions. Patients were followed up until hospital discharge or death. The outcome measure was 28-day mortality.
2.3. Definitions and Scoring Systems
We evaluated three established coagulopathy frameworks: the ISTH overt-DIC score as defined by Taylor et al.[4], the JAAM DIC score[6], and the ISTH sepsis-induced coagulopathy (SIC) score[7] .Assessment was based on platelet count, prothrombin time (PT), and fibrinogen levels. D-dimer was used for the fibrin-related marker. No increase, moderate increase and strong increase were defined as D-dimer levels of <0.4 mg/L (the upper limit of normal D-dimer level), 0.4–4 mg/L, and ≥4 mg/L (ten times the upper limit of normal) respectively. The Acute Physiology and Chronic Health Evaluation (APACHE) II score, and the Sequential Organ Failure Assessment (SOFA) score were assessed at the time of enrollment and also during the remaining days of the study. Organ failure was defined as SOFA score ≥ 2[13], and patients with ≥ 2 organ failure were considered to have multiorgan failure (MOF).
2.4. Statistical Analysis
Continuous variables were expressed as mean ± SD or median (IQR) and compared using Student’s t or Mann–Whitney U tests, as appropriate. Categorical variables were presented as counts (%) and compared using chi-square or Fisher’s exact tests as appropriate. Univariable logistic regression screened candidate predictors of 28-day mortality. Variables with P < 0.05 entered a multivariable forward stepwise logistic regression to identify independent factors. Receiver operating characteristic (ROC) curves were constructed for antithrombin activity, TAT, and t-PAIC; areas under the curve (AUCs) with 95% CIs were calculated. Optimal cut-off values were determined using Youden’s index (sensitivity + specificity − 1)[14], and corresponding sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were reported. Cut-points were derived separately for Day-1 data and for an exploratory pooled dataset combining Days 1, 3, and 7; in the pooled analysis, repeated measures from the same patient were treated as independent observations. A unified score (Unified ISTH+) was developed by adding AT, TAT, and t-PAIC (Youden-optimized thresholds) to the ISTH overt-DIC components. Prognostic discrimination of Unified ISTH+ was compared with ISTH, JAAM, and SIC using AUCs (95% CIs); pairwise AUC comparisons were performed by the DeLong method [15]. Decision curve analysis (DCA) evaluated net clinical benefit across wide range of thresholds relevant to clinical decision-making, and calibration curves assessed agreement between predicted and observed risk.
Survival was analyzed using Kaplan–Meier estimates with the log-rank test comparing Unified ISTH+–positive versus –negative groups. Spearman’s rank correlation assessed associations among biomarkers, coagulopathy scores, and severity indices. All tests were two-tailed with P < 0.05 considered statistically significant. Analyses were performed with IBM SPSS Statistics v29.0 (IBM Corp., Armonk, NY, USA) and R v4.4.1 (R Foundation for Statistical Computing).
3. Results
3.1. Patient Characteristics
During the study period, 54 patients fulfilled the inclusion criteria. Among them, 37 patients (68.5%) survived to discharge, whereas 17 patients (31.5%) died within 28 days. Baseline characteristics of the study population are shown in (Table 1)
There were no significant differences in age, gender, origin of sepsis, WBC, CRP and PCT. The primary sources of sepsis were the lung (n=30, 55.6%), urinary tract (n=9, 16.7%), Abdomen (n=8, 5.6%), and others (n=7, 13%). Septic shock occurred more often in non-survivors (58.8%) than in survivors (18.9%, p = 0.004). With respect to severity, both APACHE II (17.5 vs 9.2, p < 0.001) and SOFA scores (10.8 vs 5.0, p < 0.001) were significantly higher in non-survivors. Similarly, coagulopathy scores including ISTH overt DIC and JAAM DIC scores were significantly higher in the nonsurvivors, whereas SIC scores showed a non-significant trend.
To address potential sample-size limitations, a non-parametric bootstrap resampling procedure (B = 1000) was additionally performed. For each bootstrap replicate, the logistic regression model incorporating TAT, t-PAIC, and AT was refitted, and the AUC was recalculated to assess the stability of discriminative performance. Empirical power was defined as the proportion of bootstrap replicates in which the AUC exceeded 0.70, the prespecified threshold for acceptable discrimination, whereas AUC values ≥ 0.80 were interpreted as reflecting good to excellent model performance[16,17].
3.2. Predictors of Mortality Risk in Patients with Sepsis and Septic Shock
We used univariate and multivariate regression to identify clinical parameters significantly related to mortality (Table 2).
Step-wise regression identified antithrombin III, TAT, and tPAIC, as significant predictors of 28-day mortality. ROC analysis of the final stepwise model revealed excellent discrimination ability to predict mortality of the combined model (AUC = 0.882, 95% CI: 0.823–0.941 (Figure 1, Table S1).
Based on a cutoff of 16.04 ng/mL t-PAIC predicted mortality with an AUC of 0.846, sensitivity of 76.5%, and specificity of 89.3% (Table 3). Based on a cutoff of 8.2 ng/mL, TAT predicted mortality with an AUC of 0.845, sensitivity of 78.2%, and specificity of 78.4%. Based on a cutoff of 69.12%, Antithrombin activity levels predicted mortality with an AUC of 0.789, sensitivity of 81.8%, and specificity of 73.9%. Additionally, Longitudinal ROC analyses across days 1, 3, and 7 confirmed the stable performance of TAT, AT and tPAIC.
correlation analysis showed (Table 4). that patients' TAT and tPAIC, were significantly and positively correlated with patients' SOFA scores (P<0.001), whereas AT was significantly and negatively correlated with SOFA scores (p<0.05). while the APACHE II score significantly and positively correlated only with t-PAIC (p>0.05).
3.3. A New Unified DIC Scoring System and Evaluation of Its Predictive Performance.
Owing to the predictive abilities for mortality and their significant correlations with illness severity, TAT (≥ 8.2 = 1 point) or Antithrombin activity (<70% = 1 point) and t-PAIC (≥16= 1 point) components were then added to the ISTH DIC scoring system, and we constructed a new unified scoring system (Table 5).
(Figure 2a). shows the ROC curves of SIC, JAAM, ISTH overt-DIC, and Unified ISTH+ for predicting 28-day mortality. The AUC for Unified ISTH+ was 0.856 (95% CI 0.757–0.955), higher than ISTH (0.783; 95% CI 0.647–0.919), JAAM (0.718; 95% CI 0.568–0.868), and SIC (0.676; 95% CI 0.523–0.830); pairwise DeLong tests versus Unified were p = 0.0865 (ISTH), p = 0.00147 (JAAM), and p = 0.0458 (SIC) (Table 6). The Youden index identified an optimal Unified ISTH+ cutoff of ≥6, yielding 84.1% sensitivity and 73.5% specificity (Table S1) The score maintained strong calibration across mortality as shown (Figure 2b). Furthermore, Decision curve analysis (DCA) demonstrated a greater overall net benefit for Unified ISTH+ than for ISTH, JAAM, or SIC across a wide range of practical threshold probabilities (Figure 2c).
3.4. Comparison of Clinical Characteristics and Outcome Between Groups
Using the Unified ISTH+ criteria, 24 patients (44.4%) were classified as DIC and 30 as non-DIC. Their baseline characteristics are summarized in (Table 7).
Patients in the Unified positive group had significantly higher APACHE II (15.3 vs 9.0, p < 0.001), SOFA (9.0 vs 5.1, p < 0.001), With the increase of the Unified ISTH score, the average APACHE II score and the SOFA score of the patients increased simultaneously (Figure 3). The 28-day mortality was markedly higher in the Positive group (58.3% vs 10.0%, p < 0.001).
3.5. Reflection of Illness Severity Correlation and Survival Analysis by the Unified ISTH+ Score
Correlation analysis (Table S2) revealed the Unified ISTH+ score correlated strongly with ISTH (r = 0.925, p < 0.01), JAAM (r = 0.762, p < 0.01), and SIC (r = 0.688, p < 0.01). Importantly, it correlated more strongly with SOFA (r = 0.649) and APACHE II (r = 0.498) compared with the ISTH and JAAM scores, suggesting improved alignment with overall disease severity. The survival curves derived using the Kaplan-Meier method demonstrated that the survival rate of the DIC-positive patients was significantly lower than that of the DIC-negative patients (log rank test, P < .001) as shown in (Figure 4).
4. Discussion
In sepsis, coagulopathy represents a pivotal driver of morbidity and mortality, yet conventional diagnostic frameworks remain limited in their ability to capture early, dynamic changes in the coagulation system. The ISTH overt-DIC criteria,[4], while widely adopted, primarily identify advanced stages of DIC. and the proposed two-step approach [18] using SIC for screening followed by ISTH confirmation still overlooks endothelial injury, a central mechanism in sepsis-associated coagulopathy. This gap underscores the need to evaluate additional markers that better reflect underlying pathophysiology.
In the present study, multivariable regression analyses demonstrated that endothelial and hemostatic molecular markers, specifically t-PAIC and TAT were the strongest independent predictors of mortality, with AUCs of 0.846 and 0.845, respectively. Antithrombin activity also showed strong prognostic value (AUC 0.789), while conventional coagulation parameters such as platelet count, PT, and fibrinogen were inferior predictors of survival. These findings are consistent with prior evidence that molecular markers of coagulation and endothelial injury change earlier than global coagulation indices and are strongly linked to organ dysfunction [9,19,20,21]. Thus, our results support the view that endothelial injury and impaired anticoagulant activity are not simply downstream effects of sepsis but are critical determinants of outcome in sepsis-induced DIC. The study further revealed that increased TAT and t-PAIC and decreased AT activity could serve as early indicators for the onset of sepsis-induced DIC. Correlation analysis confirmed that TAT and t-PAIC were significantly and positively correlated with SOFA scores, while AT activity was negatively correlated. These findings suggest that all three markers can assist in identifying the occurrence of DIC. Notably, only t-PAIC correlated positively with APACHE II scores, indicating its unique potential to reflect the overall severity of a patient’s condition. Since SOFA reflects the degree of organ dysfunction and APACHE II integrates acute physiology and chronic health, the consistent associations of these molecular markers with severity scores highlight their value in both prognosis and disease monitoring.
To address the gap of current scoring frameworks, we designed a Unified scoring system that incorporates three molecular elements; t-PAIC, TAT, and AT activity into the ISTH overt-DIC criteria. Each of these markers reflects a distinct but complementary domain of coagulopathy. t-PAIC, a complex of tissue plasminogen activator (t-PA) and its inhibitor PAI-1, indicates fibrinolytic shutdown and endothelial dysfunction[22,23]. Elevated levels of t-PAIC have been consistently associated with poor outcomes and microvascular thrombosis[9,24]. Zhong and colleagues reported that serum t-PAIC concentrations ≥17.9 ng/mL were strongly associated with septic shock severity and acted as an independent risk factor for mortality in adults with sepsis[24]. Similarly, Bai et al[25]. and Li et al[26]. demonstrated in pediatric cohorts that t-PAIC and TAT were independent predictors of severe sepsis, and only t-PAIC was consistently elevated in pediatric sepsis-induced coagulopathy, where it correlated with DIC scores, organ dysfunction, and longer ICU stays[25]. In our study, serum t-PAIC levels >16 ng/mL were significantly associated with reduced 28-day survival and correlated with both SOFA and APACHE II scores, confirming its role as a sensitive marker of severity. Although not yet incorporated into diagnostic systems, evidence supports t-PAIC as a sensitive prognostic and diagnostic marker, justifying its inclusion in our unified model.
TAT, a complex of thrombin and antithrombin, reflects net thrombin generation and coagulation activation. Elevated TAT signals ongoing thrombin activity, which fuels microthrombosis, endothelial damage, and organ dysfunction[27]. Antithrombin (AT), conversely, is a natural anticoagulant that regulates thrombin and factor Xa; its depletion in sepsis results from consumption, reduced synthesis, and degradation by neutrophil elastase[28]. Decreased AT activity has been repeatedly shown to predict poor prognosis in septic DIC, and its integration with TAT improves diagnostic accuracy, particularly in early-stage disease[29]. Guo et al. reported that in ICU patients with an ISTH-DIC score <5, the presence of TAT ≥10.8 ng/mL, AT activity ≤58%, or a TAT/AT ratio ≥22.1 predicted progression to overt and irreversible DIC within 7 days [30]. Similarly, modified versions of the JAAM criteria have incorporated AT <70% in place of SIRS to enhance diagnostic precision in sepsis cohorts[31].The Japanese Society on Thrombosis and Hemostasis (JSTH) criteria[32] have previously incorporated markers such as TAT, soluble fibrin, and AT, where validation studies confirmed that their addition improved sensitivity for diagnosing pre-DIC and enhanced prognostic stratification[33,34,35]
In our cohort, patients diagnosed with DIC by the Unified ISTH+ score had significantly higher APACHE II and SOFA scores, higher mortality, and greater rates of septic shock and organ dysfunction compared with non-DIC patients. These findings mirror previous studies showing that patients with DIC have more severe illness than those without [19,21,36]. Importantly, the Unified ISTH+ score not only predicted mortality but also closely reflected disease severity, as shown by its correlations with SOFA and APACHE II. Compared with JAAM, SIC, and ISTH criteria, the Unified ISTH+ score demonstrated superior specificity for mortality prediction. Correlation analyses further confirmed that the Unified ISTH+ score aligned more closely with organ dysfunction scores, underscoring its improved clinical relevance. By integrating t-PAIC, TAT, and AT activity, the Unified ISTH+ system captures endothelial injury, thrombin generation, and anticoagulant depletion within one framework. This comprehensive approach offers earlier and more mechanistically anchored recognition of sepsis-associated DIC compared with conventional systems [20,21]. From a clinical perspective, management of sepsis-associated DIC still relies on treating the underlying infection, with the role of adjunctive anticoagulants remaining controversial[11]. Large randomized trials of anticoagulants have not demonstrated survival benefits, likely due to patient heterogeneity [37,38]. Current consensus suggests anticoagulant therapy may be most beneficial in patients with confirmed sepsis-associated DIC and high severity of illness [39,40]. Although our study did not assess treatment according to the Unified ISTH+ score, its ability to identify patients at highest risk highlights its potential to guide earlier and more targeted therapeutic interventions.
Despite its promise, this study has several limitations. First, the sample size was relatively small, and the single-center design limits generalizability. Second, only internal validation was performed; external validation across diverse cohorts is essential before the score can be widely recommended. Third, the measurement of endothelial and hemostatic molecular markers requires specialized assays not universally available and may be costly, posing barriers to routine clinical adoption. Future work should therefore focus on multicenter prospective validation, cost-effectiveness analyses, and exploration of simplified point-of-care testing strategies.
5. Conclusions
This study highlights that TAT, Antithrombin activity and t-PAIC were predictive of mortality in patients with sepsis and sepsis associated coagulopathy. Moreover, the addition of these molecular markers to the Unified ISTH+ criteria, resulted in greater prognostic value than the ISTH overt DIC alone in patients with sepsis. Larger studies and further clinical investigations are necessary to verify the utility of this new unified scoring system.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S 1. Area Under the ROC Curve (AUC) for Survival Prediction of the combined model and individual markers.; Table S 2. Correlation Between Each Cutoff Point of the Unified ISTH+ Score and Mortality*.Table S 3: Spearman’s rank correlation between different scoring systems and severity of disease.
Author Contributions
Conceptualization, A.A.N.; methodology, A.A.N.; validation, Z.J, YX.Z.; formal analysis, A.A.N. A.J.A; data curation, YX.Z.; writing—original draft preparation, A.A.N.; writing—review and editing, A.A.N, Z.Y.J.; supervision, C.Y., Y.X.Z; . All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University. 2021 Review (No. 800). Informed consent was obtained from all patients or next of kin if patients were unconscious.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following key abbreviations are used throughout this manuscript:
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| AT | Antithrombin activity |
| AUC | Area under the curve |
| APTT | Activated partial thromboplastin time |
| CI | Confidence interval |
| DIC | Disseminated intravascular coagulation |
| FDP | Fibrin/fibrinogen degradation products |
| Fib | Fibrinogen |
| ISTH | International Society on Thrombosis and Haemostasis |
| JAAM | Japanese Association for Acute Medicine |
| MOF | Multiple organ failure |
| NPV | Negative predictive value |
| OR | Odds ratio |
| PCT | Procalcitonin |
| PIC | Plasmin–α₂-plasmin inhibitor complex |
| PLT | Platelet count |
| PPV | Positive predictive value |
| PT | Prothrombin time |
| PT-INR | Prothrombin time–international normalized ratio |
| ROC | Receiver operating characteristic |
| SIC | Sepsis-induced coagulopathy |
| sTM | Soluble thrombomodulin |
| SIRS | Systemic Inflammatory Response Syndrome |
| SOFA | Sequential Organ Failure Assessment |
| TAT | Thrombin–antithrombin complex |
| t-PAIC | Tissue-type plasminogen activator–inhibitor complex |
References
- Chiu C, Legrand M. Epidemiology of sepsis and septic shock. Curr Opin Anesthesiol. 2021 Apr;34(2):71.
- Schmoch T, Möhnle P, Weigand MA, Briegel J, Bauer M, Bloos F, et al. The prevalence of sepsis-induced coagulopathy in patients with sepsis – a secondary analysis of two German multicenter randomized controlled trials. Ann Intensive Care. 2023 Jan 12;13(1):3. [CrossRef]
- Williams B, Zou L, Pittet JF, Chao W. Sepsis-Induced Coagulopathy: A Comprehensive Narrative Review of Pathophysiology, Clinical Presentation, Diagnosis, and Management Strategies. Anesth Analg. 2024 Apr;138(4):696. [CrossRef]
- Taylor FB Jr, Toh CH, Hoots WK, Wada H, Levi M; Scientific Subcommittee on Disseminated Intravascular Coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost. 2001;86(5):1327-1330.
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801–10. [CrossRef]
- Gando S, Wada H, Asakura H, Iba T, Eguchi Y, Okamoto K, et al. Evaluation of new Japanese diagnostic criteria for disseminated intravascular coagulation in critically ill patients. Clin Appl Thromb Off J Int Acad Clin Appl Thromb. 2005 Jan;11(1):71–6. [CrossRef]
- Iba T, Nisio MD, Levy JH, Kitamura N, Thachil J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: a retrospective analysis of a nationwide survey. BMJ Open. 2017 Sept 1;7(9):e017046. [CrossRef]
- Curtiaud A, Iba T, Angles-Cano E, Meziani F, Helms J. Biomarkers of sepsis-induced coagulopathy: diagnostic insights and potential therapeutic implications. Ann Intensive Care. 2025 Jan 17;15(1):12. [CrossRef]
- Li Y, Li H, Wang Y, Guo J, Zhang D. Potential Biomarkers for Early Diagnosis, Evaluation, and Prognosis of Sepsis-Induced Coagulopathy. Clin Appl Thromb. 2023 Jan 1;29:10760296231195089. [CrossRef]
- Iba T, Helms J, Levy JH. Sepsis-induced coagulopathy (SIC) in the management of sepsis. Ann Intensive Care. 2024 Sept 20;14(1):148. [CrossRef]
- Iba T, Helms J, Connors JM, Levy JH. The pathophysiology, diagnosis, and management of sepsis-associated disseminated intravascular coagulation. J Intensive Care. 2023 May 23;11(1):24. [CrossRef]
- Bateman RM, Sharpe MD, Jagger JE, Ellis CG, Solé-Violán J, López-Rodríguez M, et al. 36th International Symposium on Intensive Care and Emergency Medicine : Brussels, Belgium. 15-18 March 2016. Crit Care Lond Engl. 2016 Apr 20;20(Suppl 2):94. [CrossRef]
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996 July 1;22(7):707–10.
- Bewick V, Cheek L, Ball J. Statistics review 13: Receiver operating characteristic curves. Crit Care. 2004 Nov 4;8(6):508. [CrossRef]
- DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988 Sept;44(3):837–45. [CrossRef]
- Kleinman K, Huang SS. Calculating Power by Bootstrap, with an Application to Cluster-Randomized Trials. eGEMs. 2017 Feb 9;4(1):1202. [CrossRef]
- Riesthuis P, Otgaar H, Bücken C. Ready to ROC? A tutorial on simulation-based power analyses for null hypothesis significance, minimum-effect, and equivalence testing for ROC curve analyses. Behav Res Methods. 2025 Mar 18;57(4):120. [CrossRef]
- Iba T, Levy JH, Yamakawa K, Thachil J, Warkentin TE, Levi M, et al. Proposal of a two-step process for the diagnosis of sepsis-induced disseminated intravascular coagulation. J Thromb Haemost JTH. 2019 Aug;17(8):1265–8. [CrossRef]
- Fang X, Fu W, Xu L, Qiu Y. Analysis of the diagnostic value of coagulation markers and coagulation function indices on the occurrence of DIC in sepsis and its prognosis. Allergol Immunopathol (Madr). 2024 Sept 1;52(5):65–72.
- Guo Q, Han F, Peng J, Hou M, Shan T, Xu M. The Proactive Diagnostic Value of Thrombin-Antithrombin Complex and Antithrombin III in Disseminated Intravascular Coagulation. Blood. 2023 Nov 2;142:1268. [CrossRef]
- Mei H, Jiang Y, Luo L, Huang R, Su L, Hou M, et al. Evaluation the combined diagnostic value of TAT, PIC, tPAIC, and sTM in disseminated intravascular coagulation: A multi-center prospective observational study. Thromb Res. 2019 Jan;173:20–6. [CrossRef]
- Zhang J, Xue M, Chen Y, Liu C, Kuang Z, Mu S, et al. Identification of soluble thrombomodulin and tissue plasminogen activator-inhibitor complex as biomarkers for prognosis and early evaluation of septic shock and sepsis-induced disseminated intravascular coagulation. Ann Palliat Med. 2021 Oct;10(10):10170–84. [CrossRef]
- Watanabe R, Wada H, Miura Y, Murata Y, Watanabe Y, Sakakura M, et al. Plasma levels of total plasminogen activator inhibitor-I (PAI-I) and tPA/PAI-1 complex in patients with disseminated intravascular coagulation and thrombotic thrombocytopenic purpura. Clin Appl Thromb Off J Int Acad Clin Appl Thromb. 2001 July;7(3):229–33. [CrossRef]
- Zhong L, Dou J, Lin Q, He L, Zeng Q, Song J. Tissue-Type Plasminogen Activator-Inhibitor Complex as an Early Predictor of Septic Shock: A Retrospective, Single-Center Study. Dis Markers. 2022;2022(1):9364037. [CrossRef]
- Bai H, Shen L, Zhang H, Tang N. Clinical value of TAT, PIC and t-PAIC as predictive markers for severe sepsis in pediatric patients. Front Pediatr. 2024;12:1336583. [CrossRef]
- Li J, Zhou J, Ren H, Teng T, Li B, Wang Y, et al. Clinical Efficacy of Soluble Thrombomodulin, Tissue Plasminogen Activator Inhibitor complex, Thrombin-Antithrombin complex,α2-Plasmininhibitor-Plasmin complex in Pediatric Sepsis. Clin Appl Thromb. 2022 May 22;28:10760296221102929. [CrossRef]
- Song P, Xie J, Li W, Zhang X, Sun Z, You C. Effect of plasma thrombin-antithrombin complex on ischemic stroke: a systematic review and meta-analysis. Syst Rev. 2023 Feb 14;12:17. [CrossRef]
- Zhu L, Dong H, Li L, Liu X. The Mechanisms of Sepsis Induced Coagulation Dysfunction and Its Treatment. J Inflamm Res. 2025 Feb 3;18:1479–95. [CrossRef]
- Curtiaud A, Iba T, Angles-Cano E, Meziani F, Helms J. Biomarkers of sepsis-induced coagulopathy: diagnostic insights and potential therapeutic implications. Ann Intensive Care. 2025 Jan 17;15:12. [CrossRef]
- Guo Q. The Proactive Diagnostic Value of Thrombin-Antithrombin Complex and Antithrombin III in Disseminated Intravascular Coagulation. In ASH; 2023 [cited 2025 Sept 11]. Available from: https://ash.confex.com/ash/2023/webprogram/Paper178993.html. [CrossRef]
- Aota T, Wada H, Yamashita Y, Matsumoto T, Ohishi K, Suzuki K, et al. An Evaluation of the Modified Diagnostic Criteria for DIC Established by the Japanese Society of Thrombosis and Hemostasis. Clin Appl Thromb Off J Int Acad Clin Appl Thromb. 2017 Sept;23(6):579–84. [CrossRef]
- Asakura H, Takahashi H, Uchiyama T, Eguchi Y, Okamoto K, Kawasugi K, et al. Proposal for new diagnostic criteria for DIC from the Japanese Society on Thrombosis and Hemostasis. Thromb J. 2016 Sept 28;14(1):42. [CrossRef]
- Aota T, Wada H, Fujimoto N, Yamashita Y, Matsumoto T, Ohishi K, et al. Evaluation of the Diagnostic Criteria for the Basic Type of DIC Established by the Japanese Society of Thrombosis and Hemostasis. Clin Appl Thromb. 2017 Oct 1;23(7):838–43. [CrossRef]
- Aota T, Wada H, Fujimoto N, Sugimoto K, Yamashita Y, Matsumoto T, et al. The valuable diagnosis of DIC and pre-DIC and prediction of a poor outcome by the evaluation of diagnostic criteria for DIC in patients with hematopoietic injury established by the Japanese Society of Thrombosis and Hemostasis. Thromb Res. 2016 Nov 1;147:80–4. [CrossRef]
- Madoiwa S, Honda G, Kawano N, Uchiyama T, Kawasugi K, Takezako N, et al. An evaluation of the Japanese Society on Thrombosis and Hemostasis criteria for disseminated intravascular coagulation as a predictor of prognosis in patients with infection. Int J Lab Hematol. 2021;43(6):1566–74. [CrossRef]
- Kiya GT, Abebe G, Mekonnen Z, Tadasa E, Milkias G, Asefa ET. A comparison of disseminated intravascular coagulation scoring systems and their performance to predict mortality in sepsis patients: A systematic review and meta-analysis. PLOS ONE. 2025 Jan 16;20(1):e0315797. [CrossRef]
- Seymour CW, Kennedy JN, Wang S, Chang CCH, Elliott CF, Xu Z, et al. Derivation, Validation, and Potential Treatment Implications of Novel Clinical Phenotypes for Sepsis. [cited 2025 Sept 20]; Available from: https://jamanetwork.com/journals/jama/fullarticle/2733996. [CrossRef]
- Omidkhoda N, Abedi F, Ghavami V, Rahimi H, Samadi S, Arasteh O, et al. The Effect of Heparin and Its Preparations on Disseminated Intravascular Coagulation Mortality and Hospitalization: A Systematic Review. Int J Clin Pract. 2022;2022:2226761. [CrossRef]
- Yamakawa K, Gando S, Ogura H, Umemura Y, Kabata D, Shintani A, et al. Identifying Sepsis Populations Benefitting from Anticoagulant Therapy: A Prospective Cohort Study Incorporating a Restricted Cubic Spline Regression Model. Thromb Haemost. 2019 Nov;119(11):1740–51. [CrossRef]
- Umemura Y, Yamakawa K. Optimal patient selection for anticoagulant therapy in sepsis: an evidence-based proposal from Japan. J Thromb Haemost JTH. 2018 Mar;16(3):462–4. [CrossRef]
Figure 1.
OC curves of TAT, t-PAIC and Antithrombin activity for prediction of mortality in patients with sepsis and sepsis shock.
Figure 1.
OC curves of TAT, t-PAIC and Antithrombin activity for prediction of mortality in patients with sepsis and sepsis shock.

Figure 2.
a) Calibration plot of the Unified ISTH+ model for 28-day mortality prediction probability. (b) The ROC curves for each disseminated intravascular coagulation (DIC) scoring system, measuring the ability to predict mortality in sepsis patients (c) Decision curve analysis comparing the clinical net benefit of the Unified ISTH⁺, ISTH overt-DIC, JAAM, and SIC scores for predicting 28-day mortality.
Figure 2.
a) Calibration plot of the Unified ISTH+ model for 28-day mortality prediction probability. (b) The ROC curves for each disseminated intravascular coagulation (DIC) scoring system, measuring the ability to predict mortality in sepsis patients (c) Decision curve analysis comparing the clinical net benefit of the Unified ISTH⁺, ISTH overt-DIC, JAAM, and SIC scores for predicting 28-day mortality.
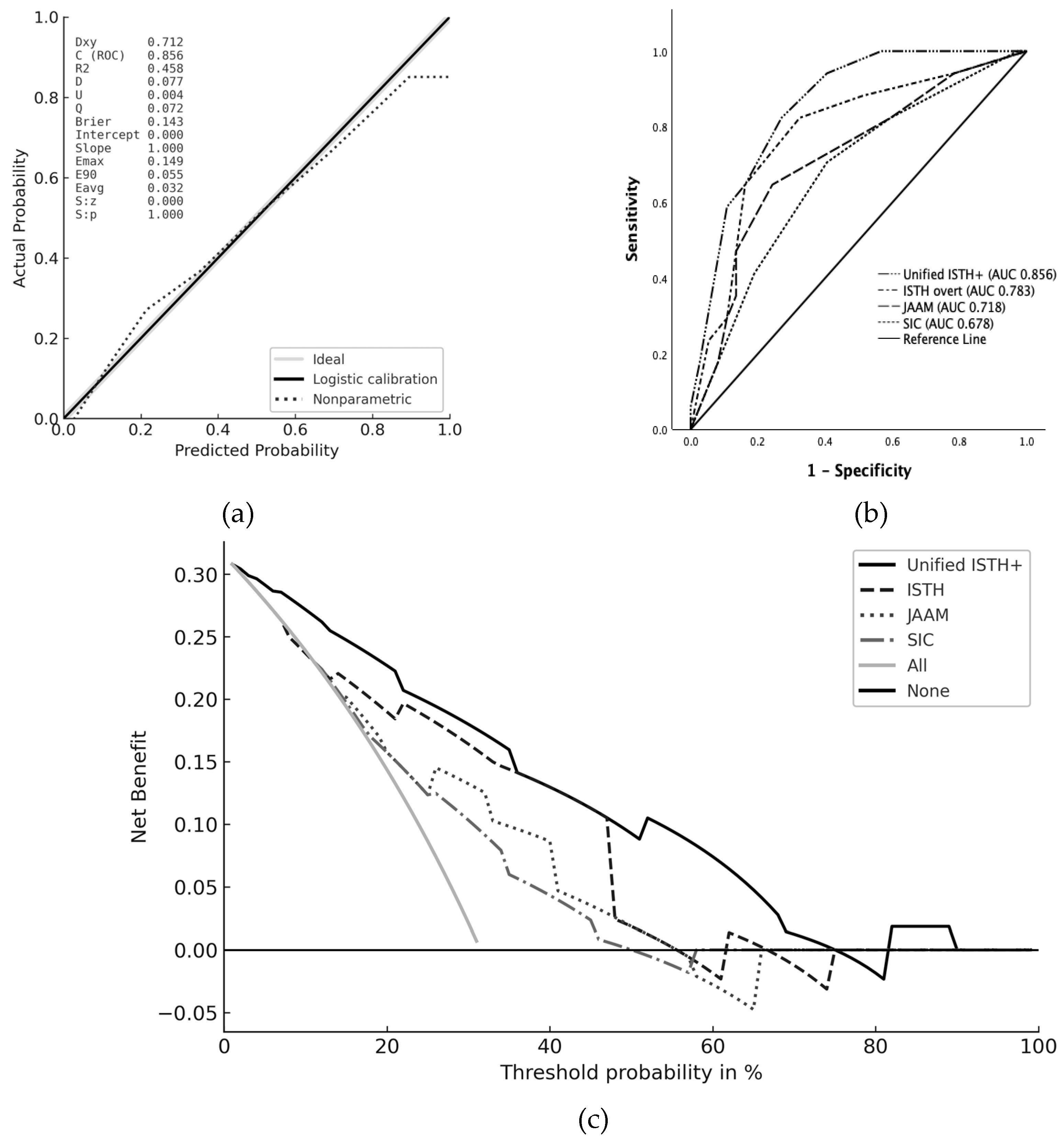
Figure 3.
Correlation between the Unified ISTH score, the average APACHE II score (white bars), the SOFA score (grey bars) and the 28day all Couse mortality (line).
Figure 3.
Correlation between the Unified ISTH score, the average APACHE II score (white bars), the SOFA score (grey bars) and the 28day all Couse mortality (line).
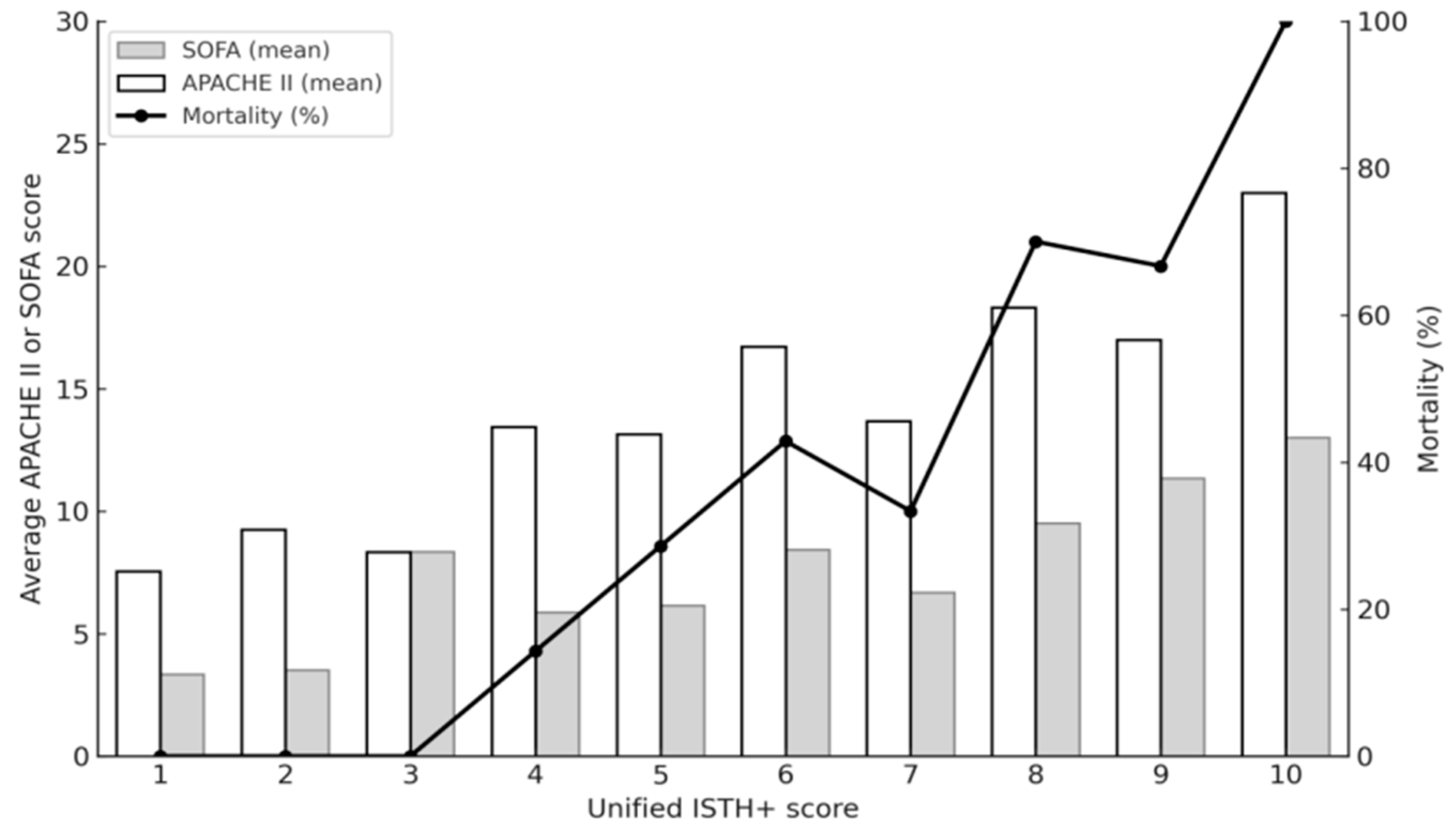
Figure 4.
Kaplan-Meier survival curves of DIC and non-DIC patients using the unified criteria.
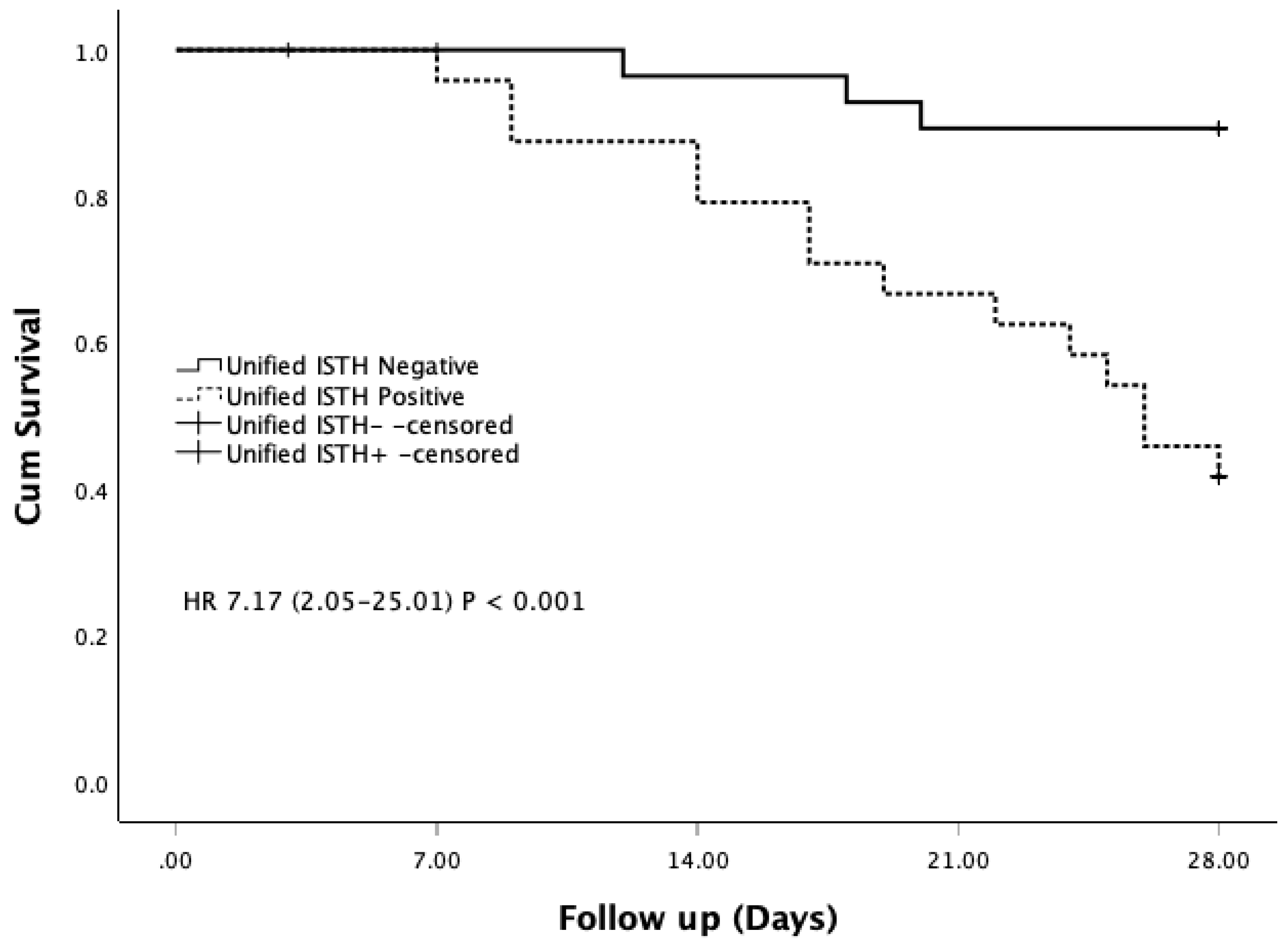

Table 1.
Comparison of baseline clinical characteristics between the study groups.
| Variables | Total (n=54) | Survivors (n=37) | Non-Survivors (n=17) | P value |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 59.61 ± 16.65 | 55.24 ± 15.92 | 64.12 ± 14.41 | 0.052 |
| Male, n (%) | 33 (61.1) | 24 (64.9) | 9 (52.9) | 0.408 |
| Length of hospital stay (days), | 25 (17-33) | 16 (11–29) | 9(7–15) | 0.004 |
| Sepsis Status, n (%) | ||||
| Septic Shock | 19 (31.5) | 7 (18.9) | 12 (58.8) | 0.004 |
| Non-Septic Shock | 35 (64.8) | 29 (81.1) | 6 (41.2) | |
| Severity Scores (IQR) | ||||
| APACHE II score | 14 (11-20) | 13 (9–18) | 19 (15–24) | 0.001 |
| SOFA score | 8 (6-12) | 7 (5–11) | 11 (9–14) | <0.001 |
| SIRS score | 2.53 ± 1.16 | 2.49 ± 1.19 | 2.61 ± 1.12 | 0.329 |
| Comorbidities, n (%) | ||||
| Hypertension | 26 (48.1) | 15 (40.5) | 11 (64.7) | 0.102 |
| Diabetes | 20 (37.0) | 9 (24.3) | 11 (64.7) | 0.075 |
| Heart disease | 10 (18.5) | 5 (13.5) | 5 (29.4) | 0.166 |
| Chronic kidney disease | 15 (27.8) | 6 (16.2) | 9 (52.9) | 0.066 |
| Chronic pulmonary disease | 5 (9.3) | 4 (10.8) | 1 (5.9) | 0.565 |
| Coagulation Scores | ||||
| ISTH overt score | 2.95 ± 1.52 | 3.15 ± 1.72 | 4.82 ± 1.74 | 0.001 |
| JAAM Score | 3.78 ± 1.84 | 4.19 ± 2.04 | 5.82 ± 2.65 | 0.030 |
| SIC score | 2.70 ± 1.79 | 3.30 ± 1.39 | 4.00 ± 1.41 | 0.098 |
| Inflammatory Markers | ||||
| WBC (×10⁹/L) | 15.43 ± 6.97 | 14.28 ± 7.41 | 17.93 ± 5.24 | 0.093 |
| CRP (mg/L) | 127.15 ± 87.68 | 115.75 ± 81.68 | 151.95 ± 97.48 | 0.194 |
| PCT (ng/mL) | 20.30 ± 32.11 | 14.49 ± 26.33 | 32.94 ± 40.09 | 0.057 |
| Source of Infection, n (%) | ||||
| Lung | 30 (55.6) | 22 (59.5) | 8 (47.1) | 0.299 |
| Abdomen | 8 (14.8) | 5 (13.5) | 3 (17.6) | |
| Urinary tract | 9 (16.7) | 8 (21.6) | 1 (5.9) | |
| Others | 7 (13.0) | 2 (5.4) | 5 (29.4) | |
| Treatments, n (%) | ||||
| Immunotherapy | 32 (59.3) | 18 (48.6) | 14 (82.4) | 0.020 |
| Glucocorticoid therapy | 25 (46.3) | 16 (43.2) | 9 (52.9) | 0.511 |
| Anticoagulant | 9 (16.7) | 3 (8.1) | 6 (35.3) | 0.084 |
| Antithrombin therapy | 2 (3.7) | 2 (5.4) | 0 (0.0) | 0.333 |
APACHE II, Acute Physiology and Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment; SIRS, Systemic Inflammatory Response Syndrome; ISTH, International Society on Thrombosis and Haemostasis (overt-DIC score); JAAM, Japanese Association for Acute Medicine (DIC score); SIC, sepsis-induced coagulopathy; WBC, white blood cell count; CRP, C-reactive protein; PCT, procalcitonin;.
Table 2.
Logistic regression analysis of inflammatory, coagulation and endothelial markers to identify predictors of mortality in the study population.
Table 2.
Logistic regression analysis of inflammatory, coagulation and endothelial markers to identify predictors of mortality in the study population.
| Predictor | Univariate |
Multivariate |
||
| OR (95% CI) | p value | aORa (95% CI) | p value | |
| t-PAIC (ng/mL) | 2.086 (1.686 – 2.581) | <0.001* | 0.910 (0.860–0.962) | <0.001 |
| TAT (ng/mL) | 1.518 (1.301 – 1.773) | <0.001* | 0.790 (0.720–0.865) | 0.005 |
| sTM (TU/mL) | 0.910 (0.848–0.976) | 0.009* | ||
| PIC (µg/mL) | 0.967 (0.944–0.996) | 0.035* | ||
| Fib (mg/dL) | 1.644 (1.105–1.444) | 0.101 | ||
| Antithrombin (%) | 1.425 (1.196 – 1.697) | 0.001* | 1.305 (1.003–1.697) | 0.013 |
| PLT (×10⁹/L) | 1.012 (1.002–1.022) | 0.207 | ||
| APTT (s) D1 | 0.844 (0.854–0.945) | 0.033* | ||
| FDP (mg/L) | 0.979 (0.956–1.003) | 0.091 | ||
| D-dimer (mg/L) | 0.956 (0.902–1.012) | 0.124 | ||
| PT (s) | 0.996 (0.961–1.033) | 0.840 | ||
| PCT (ng/mL) | 0.983 (0.966–1.001) | 0.061 | ||
| CRP (mg/L) | 0.995 (0.989–1.002) | 0.172 | ||
| WBC (×10⁹/L) | 0.943 (0.863–1.030) | 0.191 | ||
a Dependent variable coded as survival = 1; OR < 1 indicates lower odds of survival (higher mortality risk); *Variables with p<0.05 in univariate screening were entered into a multivariable model; the aOR column shows the final model after forward stepwise selection (two-sided p<0.05 considered significant); t-PAIC, tissue-type plasminogen activator–inhibitor complex (ng/mL); TAT, thrombin–antithrombin complex (ng/mL); sTM, soluble thrombomodulin (TU/mL); PIC, plasmin–α2-plasmin inhibitor complex (µg/mL); Fib, fibrinogen (mg/dL); AT, antithrombin activity (%); PLT, platelets (×10⁹/L); APTT, activated partial thromboplastin time (s); FDP, fibrin/fibrinogen degradation products (mg/L); PT, prothrombin time (s); PCT, procalcitonin (ng/mL); CRP, C-reactive protein (mg/L); WBC, white blood cells (×10⁹/L); OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval.
Table 3.
Ability of t-PAIC, TAT, or Antithrombin activity to predict mortality, based on Receiver Operating Characteristic curves.
Table 3.
Ability of t-PAIC, TAT, or Antithrombin activity to predict mortality, based on Receiver Operating Characteristic curves.
| Biomarker | AUC (95% CI) | Cut-off value* | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|---|
| tPAIC (ng/mL) | All Daysa | 0.863 (0.764–0.912) | 13.74 | 88.2% | 75.7% | 61.5% | 93.4% |
| Day 1b | 0.846 (0.777–0.969) | 16.04 | 76.5% | 89.2% | 78.9% | 87.5% | |
| TAT (ng/mL) | All Daysa | 0.814 (0.677–0.951) | 7.20 | 82.4% | 67.6% | 52.9% | 89.7% |
| Day 1b | 0.845 (0.764–0.962) | 8.22 | 78.2% | 78.4% | 70.3% | 92.1% | |
| Antithrombin % | All Daysa | 0.760 (0.631-0.888) | 72.15 | 0.850% | 0.726% | 40.5% | 96.1% |
| Day 1b | 0.789 (0.661-0.908) | 69.12 | 0.810% | 0.739% | 58.9% | 92.1% | |
aAll Days indicates a pooled ROC analysis using all available serial measurements (Days 1, 3, and 7) with a single optimized cut-off; bDay 1 uses only the first-day value . *Cut-offs were selected by the Youden index; PPV/NPV are calculated at those cut-offs. Abbreviations: t-PAIC, tissue-type plasminogen activator–inhibitor complex; TAT, thrombin–antithrombin complex; AT, antithrombin activity; ROC, receiver operating characteristic; AUC, area under the ROC curve; CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
Table 4.
Spearman’s rank correlation analysis Between Biomarkers and Disease Severity Scores.
| Indicator | SOFA | APACHE II | ||
|---|---|---|---|---|
| r | p | r | p | |
| Antithrombin | -0.401* | 0.003 | -0.065 | 0.165 |
| TAT | 0.582** | <0.001 | 0.128 | 0.051 |
| tPAIC | 0.521** | <0.001 | 0.265 | 0.041* |
| PIC | 0.420* | 0.002 | 0.052 | 0.913 |
| sTM | 0.308* | 0.023 | 0.097 | 0.309 |
| D-Dimer | 0.312 | 0.005 | 0.099 | 0.312 |
| APTT | 0.421* | 0.002 | 0.189 | 0.070 |
| PT | 0.309 | 0.002 | 0.329 | 0.012 |
| Platelet count | –0.461* | <0.001 | –0.149 | 0.281 |
| Fib | –0.098 | 0.197 | –0.018 | 0.807 |
two-sided p values shown (* p<0.05, **p<0.01). Abbreviations: SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; TAT, thrombin–antithrombin complex; t-PAIC, tissue-type plasminogen activator–inhibitor complex; PIC, plasmin–α2-plasmin inhibitor complex; sTM, soluble thrombomodulin; APTT, activated partial thromboplastin time; PT, prothrombin time; PLT, platelet count; Fib, fibrinogen.
Table 5.
The Unified Criteria Based on the ISTH DIC Criteria, With TAT, AT and t-PAIC Components Added Based on Our Analysis*.
Table 5.
The Unified Criteria Based on the ISTH DIC Criteria, With TAT, AT and t-PAIC Components Added Based on Our Analysis*.
| Parameter | Criterion | Points |
|---|---|---|
| A. Platelet count | 100–50 × 10⁹/L | 1 |
| < 50 × 10⁹/L | 2 | |
| B. PT prolongation (INR) | 3–6 s (1.2–1.4) | 1 |
| > 6 s (> 1.4) | 2 | |
| C. Fibrinogen | < 1.0 g/L | 1 |
| D. FDP (D-dimer) | 0.4 – 4mg/L | 1 |
| ≥ 4 µg/mL | 3 | |
| E. TAT (ng/mL) or AT (%) | TAT ≥ 8.2 ng/mL or AT < 70 % | 1 |
| F. t-PAIC (ng/mL) | ≥ 16 ng/mL | 1 |
| Total Score (A + B + C + D + E + F) | ≥ 6 points Positive | |
| < 6 points Negative | ||
ISTH, International Society on Thrombosis and Haemostasis; DIC, disseminated intravascular coagulation; PT, prothrombin time; INR, international normalized ratio; FDP, fibrin/fibrinogen degradation products; TAT, thrombin–antithrombin complex; AT, antithrombin activity; t-PAIC, tissue-type plasminogen activator–inhibitor complex.
Table 6.
Correlation Between Each Cutoff Point of the Unified ISTH+ Score and Mortality*.
| Scoring System | AUC | 95% CI | Cut-off Score | P* |
| Unified ISTH+ | 0.856 | 0.757–0.955 | ≥ 6 | Reference |
| ISTH | 0.783 | 0.647–0.919 | ≥ 5 | 0.086 |
| JAAM | 0.718 | 0.568–0.868 | ≥4 | 0.001 |
| SIC | 0.676 | 0.523–0.830 | ≥4 | 0.045 |
*DeLong p-values pairwise tests vs Unified ISTH+; AUC area under the ROC curve; CI, confidence interval; DIC, disseminated intravascular coagulation; ISTH, International Society on Thrombosis and Haemostasis; JAAM, Japanese Association for Acute Medicine; SIC, sepsis-induced coagulopathy. “Cut-off Score” is the threshold for each scoring system that maximized the Youden index to classify 28-day mortality in this cohort; Sensitivity/Specificity are reported at that threshold.
Table 7.
Comparison of the Characteristics Between the DIC and Non-DIC Patients Diagnosed with the Unified Criteria*.
Table 7.
Comparison of the Characteristics Between the DIC and Non-DIC Patients Diagnosed with the Unified Criteria*.
| Variables | Unified ISTH+ positive (n=24) | Unified ISTH+ negative (n=30) | P value |
|---|---|---|---|
| Age (years) | 59.88 ± 18.37 | 58.20 ± 14.68 | 0.711 |
| Male, n (%) | 15 (62.5) | 18 (60.0) | 0.853 |
| Septic Shock | 8 (33.3) | 9 (30.0) | 0.795 |
| APACHE II score | 15.29 ± 6.13 | 9.03 ± 5.79 | <0.001 |
| SOFA score | 9.00 ± 3.67 | 5.10 ± 2.67 | <0.001 |
| SIRS score | 2.71 ± 1.08 | 2.27 ± 1.20 | 0.167 |
| ISTH DIC positive | 17 (70.8%) | 2 (6.3%) | <0.001 |
| JAAM DIC positive | 16 (66.7%) | 5 (16.7%) | <0.001 |
| SIC positive | 19 (79.2%) | 8 (26.7%) | <0.001 |
| Immunotherapy | 18 (75.0) | 14 (46.7) | 0.370 |
| Glucocorticoid therapy | 15 (62.5) | 10 (33.3) | 0.340 |
| Anticoagulant | 6 (25.0) | 3 (10.0) | 0.145 |
| Antithrombin therapy | 0 (0.0) | 2 (6.7) | 0.202 |
| 28d Mortality | 14 (58.3) | 3 (10.0) | <0.001 |
| MOF | 6 (25%) | 2 (6%) | 0.046 |
| Acute Respiratory failure | 7 (29.2) | 9 (30.0) | 0.947 |
| Acute kidney injury | 3 (12.5) | 9 (30.0) | 0.128 |
| Acute Liver Failure | 4 (16.7) | 5 (16.7) | 1.000 |
*Data are presented as mean ± standard deviation for continuous variables and frequency (%) for categorical variables. Differences between the DIC-positive and -negative patients were assessed using the student’s t-test or Mann-Whitney U test for continuous variables and the chi-square or Fisher’s exact test for categorical variables, as appropriate. OF; Multi Organ Failure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



