
Submitted:
15 November 2025
Posted:
17 November 2025
You are already at the latest version
Abstract
Background: Compassion is a cornerstone of woman-centred maternity care and a critical determinant of women’s experiences of childbirth. When dignity, empathy, and effective communication are upheld, women perceive childbirth as safe, empowering, and affirming. However, evidence from many settings highlights the persistence of disrespect, neglect, and abuse during facility-based intrapartum care, undermining trust in health services and contributing to poor maternal outcomes. Objectives: This scoping review explored and synthesized evidence on women’s experiences and per-ceptions of care, with a focus on how compassionis are experienced and enacted in healthcare settings. Methods: A systematic search was conducted across EBSCOhost databases, ScienceDirect, CINAHL, PubMed, Web of Science, Medline, and PsycINFO. Fifteen studies met the inclusion criteria. Data was charted and thematically analyzed to identify the role of compassion and related interpersonal factors in shaping wom-en’s intrapartum experiences. Results: The review of fifteen studies identified two main themes and 12 sub-themes related to childbirth experiences. Compassionate care, characterized by respect, empathy, effective communication, and support for autono-my, led to positive childbirth outcomes and encouraged future use of health services. Conversely, care encounters lacking relational elements, including neglect, mistreat-ment, discrimination, and unconsented care, resulted in feelings of humiliation and disempowerment, discouraging women from seeking facility-based care in future. Conclusion: Compassion during intrapartum care is both a fundamental human right and an essential component of quality maternal health services. Addressing persistent mistreatment requires systemic reform, provider training in compassionate, rights-based care, stronger accountability, and the active inclusion of women’s voices in shaping maternity services.
Keywords:
childbirth
; compassion
; experiences
; facility births
; intrapartum care
; respectful maternity care
; sub-Saharan Africa
; women
1. Introduction
Compassion is a universal principle and a cornerstone of high-quality healthcare [1]. The World Health Organization [WHO], advocates for facility births with “skilled birth attendants” for optimal maternal and neonatal outcomes [2]. During facility-based births, compassion involves healthcare providers (HCPs) recognizing and responding to women’s physical, emotional, and psychological needs, validating their experiences, contextualizing care, empowering them in decision-making, and performing small acts of kindness [3]. These behaviors foster emotional connection, trust, and satisfaction, and should be regarded as a core component of maternity services rather than an optional add-on. Strauss et al. [4] define compassion as recognizing and understanding suffering, acknowledging shared humanity, forming emotional connections, tolerating challenging emotions, and being motivated to help. Key dimensions include empathy, attentiveness, impartiality, and a genuine commitment to patient well-being [5,6]. Menage et al. [5] further emphasize that compassion encompasses developing a meaningful relationship, genuinely caring for the individual, and treating patients with the same concern one would show family or friends. Cummings and Bennet [6] highlight additional elements care, courage, communication, commitment, and competence underscoring the multifaceted nature of compassionate care, which integrates technical skills with emotional engagement.
When compassion is in maternity care, women may experience mistreatment such as verbal abuse, neglect, or discrimination. These violations erode trust in health systems, discourage future engagement with services, and compromise both maternal and neonatal outcomes [7,8]. In resource-limited settings, such mistreatment deepens existing health disparities, marginalizes vulnerable populations, and obstructs efforts to achieve equitable, rights-based care [7,11,12]. The absence of compassionate interactions not only affects individual experiences but also undermines broader public health goals, making it essential to prioritize dignity, empathy, and ethical conduct in all aspects of maternal healthcare delivery.
In sub-Saharan Africa, studies indicate that 20–80% of women experience some form of mistreatment during childbirth [7,11]. Even a single positive experience of compassionate care can significantly influence future care-seeking behavior and improve adherence to WHO intrapartum care guidelines [13]. Policies and guidelines from the WHO, the White Ribbon Alliance, and national frameworks in countries such as South Africa advocate for the integration of compassionate care throughout the childbirth continuum [14,15]. However, translating these principles into routine practice remains challenging due to systemic constraints, including high workloads, staff burnout, limited training in interpersonal skills, and entrenched institutional cultures [17,18].
Furthermore, environmental care aspects such as cleanliness, privacy, and availability of resources influence the perception of compassionate care. While environmental conditions are not direct expressions of compassion, they influence women’s experiences and interpretations of HCP behavior. For instance, a well-maintained, private, and supportive environment may reinforce women’s sense of being cared for, whereas poor conditions may amplify feelings of neglect or disregard for dignity [19].
Literature emphasizes the importance of both respectful maternity care (RCM), which provides a structural and rights-based framework, and compassionate care, which addresses the emotional and relational aspects, in shaping women's childbirth experiences in sub-Saharan Africa.
1.1. Review Purpose
The emphasis on compassionate care is growing in sub-Saharan Africa to enhance childbirth experiences. While RMC provides a rights-based framework, compassionate care addresses emotional and relational aspects. This scoping review was conducted to explore women's experiences of compassion during facility-based childbirth in the region, as existing research often focuses on disrespect and abuse or RMC, but not directly on compassion. Given the broad and evolving definitions of compassionate and respectful care, a scoping review is more suitable as it allows for the inclusion of diverse, qualitative, and grey literature. The review maps current evidence, clarifies conceptual overlaps, and identifies research gaps, particularly relevant in sub-Saharan contexts shaped by sociocultural and systemic differences. This approach provides a comprehensive foundation for future research, policy development, and targeted interventions to enhance maternal care experiences and outcomes. Since this study focuses on compassionate care, respectful maternity care will be referenced only when drawing distinctions or exploring the relationship between the two concepts.
2. Materials and Methods
The scoping narrative review aimed to deepen understanding of women’s experiences during facility-based intrapartum care by synthesizing qualitative and mixed-methods studies. This approach systematically identified and analyzed primary research to capture women’s perspectives, highlighting behavioral patterns associated with both compassionate and uncompassionate care. Focusing on qualitative and mixed-methods studies was chosen because these designs are best suited to exploring experiences, perceptions, and meanings, which are central to understanding compassionate care during childbirth. A scoping narrative review is useful in the field of compassionate maternity care, where definitions and operationalizations vary, and the literature is heterogeneous, emerging, and context-specific [20,21].
2.1. Review Question
The formulation of the review question was guided by the ECLIPSE framework by Wildridge & Bell [22] (Table 1).
The researchers applied the five steps to gather research evidence from databases according to Arksey and O’Malley [18]. The steps are as follows (I) problem identification, (II) literature search, (III) selecting the data, (IV) documenting the data, and (V) organizing, summarizing, and presenting the findings.
2.1.1. Problem Identification
The literature revealed a persistent prevalence of both mistreatment and lack of compassion toward women during facility-based childbirth across sub-Saharan Africa. Such experiences highlight not only violations of women’s rights but also significant gaps in the consistent provision of compassionate. Despite global commitments to quality, woman-centred care, compassion remains underexplored as a defining element of positive childbirth experiences. This gap underscores the need to better understand how compassion is perceived, expressed, and enacted in maternity settings. Consequently, the researchers formulated the review question:
“What is the available empirical evidence on women's experiences of compassion during facility-based intrapartum care?” This question guided the scoping review to map existing knowledge, identify conceptual and contextual patterns, and highlight areas requiring further research and intervention.
2.1.2. Literature Search
Identifying empirical studies relevant to the review question required an extensive search of scientific databases [23,24,25]. The literature search was conducted from June 2022 to August 2022 and an update (2023-2024) conducted in February 2025. The primary researcher combed through electronic databases and manually searched reference lists of relevant articles for potential studies to identify studies missed during the electronic search. To identify potential studies from databases a combination of search terms was used. The researcher searched the following electronic databases to locate studies: EBSCO host databases, Science Direct, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, Medline, Web of Science and PsychInfo. Search terms helped filter articles from databases by eliminating irrelevant ones. The review process involved on-going co-checking by the two study supervisors.
2.2. The Search Terms
Childbirth OR delivery AND (compassion OR respectful) AND (healthcare facility OR hospital) AND (intrapartum OR labour OR labor) AND (women OR mothers) AND (experiences OR perceptions OR opinions OR views)
Predetermined inclusion and exclusion criteria guided the search process. The criteria eliminated researcher bias while concurrently ensuring accuracy. Only studies that met the predetermined criteria were included.
2.3. Eligibility Criteria
The inclusion criteria were developed to ensure the review captured studies most relevant to women’s lived experiences of compassionate care during childbirth within Sub-Saharan African health facilities. Qualitative studies were included for their ability to provide rich, nuanced insights into perceptions of care, emotional responses, and health system interactions offering depth that quantitative methods alone may overlook. Mixed-methods studies were also considered, as they combine qualitative depth with quantitative breadth, thereby strengthening the comprehensiveness of the findings [26]. The criteria were guided by the review’s aim to synthesise evidence on the emotional, relational, and contextual dimensions of compassionate care rather than clinical outcomes alone. Each inclusion aspect was selected to enhance conceptual alignment with respectful maternity care frameworks and ensure methodological transparency. The criteria also reflect global policy milestones, notably the 2011 introduction of the Respectful Maternity Care Charter, which catalysed research and advocacy on women’s rights and experiences in childbirth [13]. Summaries of the inclusion criteria and rationale for each are provided. (Table 2).
2.4. Selection of Data
This is the fourth step in Arksey and O’Malley [18] once identified from the databases; the data was imported into Covidence a citation manager [27] for screening. Duplicate records were removed in Covidence. Firstly, primary studies meeting the inclusion criteria were screened on title, abstract, and full text before inclusion [15]. The main author conducted the initial screening of titles and abstracts, while two supervisors independently verified inclusion and exclusion decisions to ensure accuracy and consistency. This approach balanced efficiency with methodological rigor and aligns with recommended practices for scoping reviews [24].
2.4.1. Quality Assessment
Formal appraisal is considered optional in scoping reviews and is not a prerequisite for inclusion, as outlined by Arksey and O’Malley [18] and the JBI [24]. The primary aim of a scoping review is to provide a general overview of the existing literature. However, in this study, it was under-taken to assess the quality of evidence but not as a criterion for inclusion or exclusion. The Mixed Methods Appraisal Tool (MMAT), 2018 version [28] was used. The Mixed Methods Appraisal Tool (MMAT, 2018 version) was used to assess study quality. This validated tool evaluates methodological rigor across qualitative, quantitative, and mixed-methods designs using five criteria. In this review, one mixed-methods and fourteen qualitative studies were appraised, and all scored 5 out of 5, demonstrating high methodological quality (Table S1). Furthermore, given the verification process and the exploratory nature of scoping reviews, inter-rater reliability statistics such as Cohen’s kappa were not calculated, consistent with current methodological guidance [24].
2.4.2. Methodological Rigor
The study was conducted under the supervision of two independent researchers who provided ongoing oversight throughout the research process. Each supervisor re-viewed the stages of data collection, analysis, and interpretation separately, offering critical feedback to ensure methodological rigor. The review process included continuous co-checking by both supervisors to maintain consistency and accuracy. Any discrepancies or differing interpretations were discussed and resolved through consensus involving the student and both supervisors.
Although this scoping review was not registered on the Open Science Framework (OSF), transparency was ensured by providing a detailed account of the methodological process, including the review steps, eligibility criteria, and search strategy, to support reproducibility and clarity in the conduct of the study. This review process is illustrated in the PRISMA flow diagram [29] (Figure 1).
2.5. Documenting the Data
The data was organized manually on a predesigned data extraction table. PL the PhD candidate conducted the review while supervisors CSM and WL were co-reviewers of the entire scoping review process. The data extraction table consists of descriptive headings: authors, year, aims and country of focus, methods, population and sample, data collection and analysis, and finally the results applicable to the review. A description of the study findings was summarised under the results (Table S2).
2.6. Organizing, Summarizing, and Presenting the Findings
A thematic analysis of the included studies was undertaken to identify recurring patterns in women’s narratives of intrapartum care across diverse facility-based settings in Sub-Saharan Africa. This process involved familiarization with the data, coding of re-ported experiences, and clustering of codes into broader themes that captured commonalities and variations. The analysis revealed a consistent duality: while many women described elements of compassionate care, negative experiences of neglect, abuse, and lack of autonomy were equally prominent. The findings were organized into two overarching themes, each encompassing six sub-themes (Table 3). A graphical presentation of themes and sub-themes depicting intrapartum care experiences (Figure 2).
3. Results
3.1. Characteristics of Studies Included
Fifteen studies were included in the review. Details of individual studies are included (Table 3). The study designs included one (1) mixed-methods study and fourteen (14) qualitative studies. All the included studies were conducted in sub-Saharan African countries Ethiopia [30,31,32], Kenya [33,34], Malawi [35], Tanzania [36,37], Uganda [38,39] and South Africa [40,41,42,43,44]. The studies reported women’s experiences of facility-based intrapartum care. The birth settings ranged from community health centres, midwife-led units, rural hospitals, and faith-based and private hospitals.
This review incorporated fifteen studies. The methodological composition included one (1) mixed-methods study and fourteen (14) qualitative studies, reflecting a strong emphasis on narrative inquiry and experiential depth. The predominance of qualitative approaches underscores a growing recognition of the value of narrative data in understanding the nuances of maternity care centring women's voices in evaluating maternity care quality and responsiveness particularly in contexts where systemic inequities and cultural dynamics intersect. Details of individual studies are included (Table 4).
Geographically, the studies span six countries Ethiopia [30,31,32], Kenya [33,34], Malawi [35], Tanzania [36,37], Uganda [38,39], and South Africa [40,41,42,43,44] providing a regional lens on maternal health systems shaped by varying cultural, economic, and policy environments. This diversity enhances the transferability of findings while allowing for contextual comparisons.
3.2. Scope of Narratives and Conceptual Framing
The two themes; person-centred encounters and relational deficient care encounters each with six sub-themes are analytically presented below.
3.3. Person-Centred Care Moments
3.3.1. Empathetic and Dignified Care
Women felt dignified and empowered when caregivers showed empathy, respect, and supported their choices.
“They respected my body and allowed me to labour in my own way.” [41]
3.3.2. Empathetic Communication
Clear, compassionate communication improved women's experiences.
“The midwife held my hand and told me I was strong. That made me feel I could do it.” [35]
3.3.3. Informed Consent and Autonomy
Involvement in decision-making fostered trust and satisfaction.
“They asked me before they did anything. I felt like I had control over my birth.” [39]
3.3.4. Privacy and Confidentiality
Women expressed appreciation for facilities and staff who ensured modesty, used curtains, and conducted procedures discreetly.
“They covered me properly and ensured others could not see me.” [35]
3.3.5. Caring Environment
Women valued the presence of supportive companions during labour, which provided comfort, strength, and emotional reassurance.
“They allowed my sister to stay with me I felt strong knowing she was there.” [39]
3.3.6. Caring Attributes
Small gestures a smile, gentle touch, or words of encouragement had profound emotional impact and embodied the essence of compassionate care.
“The midwife held my hand and said, ‘You can do it’; that gave me courage.” [40]
3.4. Relational Deficient Care Encounters
3.4.1. Violation of Bodily Integrity
Incidences of physical mistreatment included slapping, pinching, and hitting.
“… That is very bad because during delivery you push with a lot of pain and you are suffering while been pinched or slapped, it’s not acceptable…” [34]
3.4.2. Authoritarian Care Practices
Women reported procedures conducted without explanation or permission.
“I told the midwifenotto allow [students to enter and observe care], but they were already in the room on practical learning, and the midwife didn’t want to send them out once they were in. In the future, I don’t want that.” [31]
3.4.3. Breach of Confidentiality
“…assessments were done in non-private settings with many students around to observe.” [32]
3.3.4. Verbal Mistreatment and Insensitive Interactions
Women reported shouting, insults, and neglect during labor.
“They say, don’t cry! There is no mum here, eh? Don’t cry. Did your mum make your baby, eh? Or was it your boyfriend?” [43]
3.4.5. Discriminatory and Unequal Treatment
Discrimination based on socioeconomic status, marital status, and ethnicity was reported.
“...theytreatyou depending on your background…If you come wearing nice clothes and accompanied by urban companions, they will give you a priority. For mothers in torn clothes, then things are different.” [30]
3.5. Neglect and Withholding of Care
Women experienced delayed or absent care, sometimes with serious consequences.
“After the baby came, she (the nurse) was about to stitch me and I was afraid because she did not give me anything for pain, so I refused, and she left me in bed with blood all over me for about two to three hours.” [42]
4. Discussion
Mistreatment of women in health facilities remains a pervasive global concern that must be eradicated [45]. However, meaningful progress in maternal health cannot be achieved through structural reforms alone; it requires the intentional integration of compassion into every facet of care. While this review focuses on sub-Saharan African countries, the discussion draws on global literature to contextualize regional findings within broader maternity care discourses. This comparative lens enables a more nuanced understanding of the shared and opposing scope of women’s experiences, particularly in relation to compassionate care, without extending conclusions beyond the scope of the data.
The findings reveal a persistent duality in facility-based childbirth experiences across sub-Saharan Africa wavering between compassionate care and mistreatment. This duality mirrors global patterns observed in South Asia, Latin America, and other low- and middle-income regions, where frameworks promoting safety and dignity often fail to translate into consistent, woman-centred care [7,46].
In the included studies, some women experienced childbirth as a moment of empathy, attentiveness, and emotional support, which nurtured trust in their providers and enhanced person-centred care [31,37,39]. Conversely, others encountered relationally deficient care marked by neglect, mistreatment, and discrimination, leading to psychological trauma and discouraging future use of health facilities [30,32,37,38,41,42]. The nature of care extended beyond clinical skills to encompass relational acts such as attentive listening, encouragement, and comfort practices that reflect WHO’s standards for quality maternal and newborn care [47]. Although the 2016 WHO framework underscores emotional support and individualized attention as essential components of quality maternity care, the included studies reveal inconsistent implementation of these standards. Given this context, communication emerged as a pivotal conduit for compassion.
Women valued providers who offered clear explanations of procedures, engaged empathetically, and provided continuous reassurance throughout labor [31,35,37]. Such communicative practices not only alleviated anxiety but also promoted informed decision-making and reinforced maternal autonomy.These findings echo global evidence that empathetic communication is foundational to positive childbirth experiences [48]. Moreover, achieving gender equity in global health requires an intersectional strategy that addresses compounded disadvantages related to race, class, disability, and geography. The Lancet Commission calls for inclusive governance, measurable progress, and evidence-based tools to guide gender-transformative health policies [49].
Autonomy and participation in decision-making were reinforced through compassionate engagement. Providers who sought consent, invited questions, and involved women in care decisions conveyed recognition of their individuality and agency [30,39]. The landmark study by Bowser and Hill [50] identified lack of compassionate care as a key contributor to disempowerment and birth-related trauma a pattern consistently observed across global contexts.
The physical and institutional environment also shaped the expression of compassion. Clean, calm, and private facilities enabled providers to offer empathetic and responsive care [32,36]. Conversely, overcrowding, inadequate resources, and lack of privacy constrained providers’ ability to deliver compassionate care, reflecting structural limitations common in under-resourced settings [6,51]. Provider attitudes further amplified these dynamics; warmth, attentiveness, and reassurance helped women cope with labor, underscoring that emotional support is as vital as clinical outcomes [52].
Women’s expectations of childbirth encompass both clinical safety and emotional comfort. Many desire a natural labor and birth, supported by competent professionals and birth companions, and appreciate being empowered to make informed decisions even when medical interventions are necessary [53]. The WHO advocates for continuous support and compassionate care as central to positive maternal outcomes.
Negative experiences illuminate systemic and structural barriers to compassion. Reports of physical and verbal mistreatment, non-consented procedures, neglect, and inequitable treatment were widespread [30,32,37,38,41,42]. These practices reflect hierarchical institutional cultures, insufficient staffing, and normalized mistreatment. Structural inadequacies such as lack of privacy intersected with interpersonal failures, eroding trust and discouraging future facility use. Vulnerabilities were exacerbated by socioeconomic disadvantage, adolescent status, and marital circumstances, highlighting the need for an intersectional lens in addressing compassionate care [30,32,42].
The coexistence of compassionate and distressing experiences underscores the unpredictability of facility-based childbirth. While compassionate care can transform childbirth into a safe and affirming experience, systemic neglect and normalized mistreatment undermine trust and deter care-seeking. This review’s findings align with other studies in sub-Saharan Africa that highlight disparities between private and public health facilities. Private facilities often offer more personalized attention, better infrastructure, and higher staff-to-patient ratios, enabling individualized care [54,55]. In contrast, public facilities face challenges such as high patient volumes, staff shortages, and limited resources, which compromise their ability to consistently deliver compassionate care [48].
Prioritizing compassion in maternal care, alongside clinical safety, improves outcomes, builds trust, and promotes equitable, dignified childbirth. Women's satisfaction, linked to compassionate care, influences their perceptions and adherence to medical advice, reflecting the alignment of care with their expectations and needs.
4.1. Strengths and Limitations
This review synthesizes women’s experiences of compassionate care during facility-based childbirth in sub-Saharan Africa, offering rich qualitative insights into the emotional, interpersonal, and gendered dimensions of maternity care. It highlights both compassionate and unsafe practices, illustrating how cultural, structural, and institutional factors shape women’s trust and experiences. A major strength lies in its regional focus and its contribution to conceptualizing compassion within quality maternity care standards.
However, several limitations affect the generalizability and comparability of findings. These include reliance on self-reported data, regional specificity, and variability across studies. The exclusion of provider perspectives further constrains understanding of systemic influences. Additionally, the review is limited by its inclusion of only English-language studies, which may exclude relevant research conducted in other languages and cultural contexts. The lack of quantitative studies also restricts the ability to measure the prevalence and impact of compassionate care practices across settings.
Future research should integrate the perspectives of women, healthcare providers, and policymakers to inform strategies that embed compassion within maternity care systems, while also expanding linguistic and methodological inclusivity to inform strategies that embed compassion in maternity care systems.
4.2. Recommendations
Improving facility-based childbirth experiences requires a multifaceted approach involving education, policy, practice, and research. Training programs should emphasize empathy, communication, and responsiveness, supported by mentorship and reflective supervision. Policies must protect women’s rights through patient charters, audits, and accessible complaint mechanisms. Practical improvements include adequate staffing, infrastructure, and supportive workplace cultures, alongside staff wellness initiatives and recognition for compassionate care and the development of context-sensitive interventions. Research should examine how compassionate care is understood and practiced by both women and providers, with attention to vulnerable groups such as adolescents, cesarean births, and marginalized communities. Together, these strategies promote compassionate, high-quality, and woman-centred maternity care, ensuring childbirth is a safe, dignified, and empowering experience for all women across diverse settings.
5. Conclusion
This review reveals a persistent duality in women’s facility-based childbirth experiences in sub-Saharan Africa, where compassionate care and mistreatment coexist within the same health systems. While some women experienced empathy, emotional support, and empathetic engagement, others reported neglect, abuse, and discrimination shaping their perceptions of care and influencing future health-seeking behavior.
Since the landmark study by Bowser and Hill [50], which brought global attention to the mistreatment of women during childbirth, numerous frameworks have emerged to promote respectful maternity care. However, the findings of this review suggest that progress has been uneven. Mistreatment remains prevalent, indicating that systemic change has been slow and inconsistently implemented across both public and private facilities.
The review contributes a novel perspective by critically examining the blurred boundary between respectful and compassionate care. While respectful care emphasizes procedural fairness and non-abusive treatment, compassionate care encompasses emotional responsiveness, relational attentiveness, and genuine concern for women’s well-being. The review highlights that compassionate care is not consistently recognized or operationalized, despite its central role in shaping positive childbirth experiences and enhancing satisfaction.
Furthermore, the comparative insights into public and private facility dynamics underscore how structural disparities such as staffing levels, infrastructure, and institutional culture affect the delivery of compassionate care. These findings reinforce the need to position compassion not as an optional enhancement, but as a fundamental component of equitable, dignified, and woman-centred maternity care. This aligns with the recommendations, for comprehensive approaches involving education, policy, practice, and research to enhance childbirth experiences.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Combined MMAT Appraisal Table – 15 Studie; Table S2: A description of studies included in the scoping narrative review.
Author Contributions
Conceptualization, P.L; methodology, P.L; software, P.L.; validation, C.S.M and W.L.; formal analysis, P.L.; investigation, resources, P.L., C.S.M and W.L.; data cura-tion, P.L.; writing—original draft preparation, P.L.; writing—review and editing, P.L., C.S.M and W.L.; visualization, P.L.; supervision, C.S.M and W.L; project administration, P.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blomberg K, Griffiths P, Wenstrom Y, May C, Bridges J. Interventions for compassionate nursing care: A systematic review. Int J Nurs Stud. 2016;62:137–155. Epub. [CrossRef]
- World Health Organization (WHO). Definition of skilled health personnel providing care during childbirth: The 2018 joint statement by WHO, UNFPA, UNICEF, ICM, ICN, FIGO and IPA. 2018. https://www.who.int/publications/i/item/definition-of-skilled-health-personnel-providing-care-during-childbirth.
- Vedeler C, Nilsen AB, Downe S, Eri TS. The “doing” of compassionate care in the context of childbirth from a women’s perspective. Qual Health Res. 2025;35(10-11):1177-90. [CrossRef]
- Strauss C, Taylor BE, Gu J, Kuyken W. Baer R, Jones F, Cavanagh J. What is compassion and how can we measure it? A review of definitions and measures. Clin Psychol Rev. [CrossRef]
- Menage D, Bailey E, Lees S, Coad J. Women's lived experience of compassionate midwifery: Human and professional. Mid. 2020;1(85):102662. [CrossRef]
- Cummings J, Bennett V. Compassion in Practice: Nursing, Midwifery and Care Staff - our Vision and Strategy. NHS Commissioning Board. http://www.england.nhs.uk/ wp-content/uploads/2012/12/compassion-in-practice (accessed 1 April 2024).
- Bohren MA, Vogel JP, Hunter EC, Lutsiv O, Makh SK, Souza JP, et al. The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed Method Systematic Review. PLoS Med. 2015;12(6):e1001847. [CrossRef]
- Vusio F, Odentz K, Plunkett C. Experience of compassionate care in mental health and community-based services for children and young people: facilitators of, and barriers to compassionate care–a systematic review. European Child Adolesc Psych. 2025; 4:1-8. [CrossRef]
- Lim SWC, Foo SA, Chan, HG, Mathur M. Int J Reprod Contracept Obstet Gynecol. 2024;13(6):1376-1382. [CrossRef]
- World Health Organization. 2025. HIV and AIDS. https://www.who.int/news-room/fact-sheets/detail/hiv-aids Date accessed 16 August 2025.
- Asefa A, McPake B, Langer A, Bohren MA, Morgan A. Imagining maternity care as a complex adaptive system: understanding health system constraints to the promotion of respectful maternity care. Sex Reprod Health Matters. 2020;28(1):e1854153. [CrossRef]
- Moyer CA, McNally B, Aborigo RA, Williams JEO, Afulani PA. Providing respectful maternity care in northern Ghana: A mixed-methods study with maternity care providers. Midwifery. 2021;94:102904. [CrossRef]
- World Health Organization. The prevention and elimination of disrespect and abuse during facility-based childbirth. http://apps.who.int/iris/bitstream/10665/134588/1/WHO_RHR14.23_eng.pdf (accessed 28 Mar 2024).
- White Ribbon Alliance (WRA). Respectful Maternity Care: The Universal Rights of Childbearing Women. https://content.sph.harvard.edu/wwwhsph/sites/2413/2014/05/Final_RMC_Charter.pdf (accessed 17 Apr 2024).
- National Department of Health. National Integrated Maternal and Perinatal Care Guidelines for South Africa (5th ed.). Government of South Africa. http//www.Department of Health Knowledge Hub: Integrated Maternal and Perinatal Care Guideline_23_10_2024_0.pdf (accessed 20 Aug 2025).
- Thirukumar, M. Short Review on Respectful Maternal Care (RMC). Batticaloa Medic J. 2024;18(2). [CrossRef]
- Mayra K, Catling C, Musa H, Hunter B, Baird K. Compassion for midwives: The missing element in workplace culture for midwives globally. PLOS Glob Public Health. 2023;3(7):e0002034. [CrossRef]
- West M, Bailey S, Williams E. The courage of compassion. Supporting Nurses and Midwives to Deliver High-Quality Care. London: The King’s Fund, London. 2020 Sep.
- Downe S, Finlayson K, Oladapo OT, Bonet M, Gülmezoglu AM. What matters to women during childbirth: A systematic qualitative review. PLOS ONE. 2018;13(4):e0194906. [CrossRef]
- Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Method. 2005;8(1):19-32. [CrossRef]
- Levac D, Colquhoun H, & O'Brien KK. Scoping studies: advancing the methodology. Imp Sci, 201;5(1):69. [CrossRef]
- Wildridge V, Bell L. 2002. How CLIP became ECLIPSE: a mnemonic to assist in searching for health policy/management information. Health Info Libra J. 2002;19(2). [CrossRef]
- Torraco, RJ. Writing Integrative Reviews of the Literature: Methods and Purposes. Int J Adult Vocat Edu Tech. 2016;7(3):62-70. [CrossRef]
- Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z. JBI Manual for Evidence Synthesis. JBI: Adelaide, Australia, 2024. [CrossRef]
- Johanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: Methodology for JBI Scoping Reviews. The Joanna Briggs Institute. 2015 edition Suppl. Accessed September 26, 2024. https://nursing.lsuhsc.edu/JBI/docs/ Reviewers Manuals/ Scoping-.pdf.
- Renjith V, Yesodharan R, Noronha JA, Ladd E, George A. Qualitative methods in health care research. Human Reprod Sci. 2021;14(1), 80–86. [CrossRef]
- Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Edu Info. 2018;34(4), 285–291.
- Covidence. 2025. Covidence Academy. Accessed 21 January https://academy.covidence.org/.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. bmj. 2021;29;372.
- Asrese, K. Quality of intrapartum care at health centers in Jabi Tehinan district, North West Ethiopia: clients’ perspective. BMC Health Serv Res. 2020;20:1-12. [CrossRef]
- Burrowes S, Holcombe SJ, Jara D, Carter D. Smith K. Midwives' and Patients' Perspectives on Disrespect and Abuse During Labor and Delivery Care in Ethiopia: A Qualitative Study. BMC Preg Childbirth. 2017;17:263. [CrossRef]
- Jiru HD, Sendo EG. Promoting compassionate and respectful maternity care during facility-based delivery in Ethiopia: perspectives of clients and midwives. BMJ Open 2021;11:e051220. [CrossRef]
- Afulani PA, Kirumbi L, Lyndon A. What makes or mars the facility-based childbirth experience: thematic analysis of women’s childbirth experiences in western Kenya. Reproductive health. 2017;29;14(1):180.
- Oluoch-Aridi J, Afulani PA, Guzman DB, Makanga C, Miller-Graff L. Exploring women’s childbirth experiences and perceptions of delivery care in peri-urban settings in Nairobi, Kenya. Reprod Health. 2021;18(1):83.
- Kumbani L, Bjune G, Chirwa E, Malata A, Odland JØ. Why some women fail to give birth at health facilities: a qualitative study of women’s perceptions of perinatal care from rural southern Malawi. Reprod Health. 2013;10:9. [CrossRef]
- Metta E, Unkels R, Mselle LT, Hanson C, Alvesson HM, Al-Beity FMA. Exploring women’s experiences of care during hospital childbirth in rural Tanzania: a qualitative study. BMC Preg Childbirth. 2024;24(1):290. [CrossRef]
- Shimpuku Y, Patil CL, Norr KF, Hill PD. Women's perceptions of childbirth experience at a hospital in rural Tanzania. Health Care Women Int. 2013;34(6);461-481.
- Munabi-Babigumira S, Glenton C, Willcox M, Nabudere H. Ugandan health workers’ and mothers’ views and experiences of the quality of maternity care and the use of informal solutions: A qualitative study. PLoS O 2019;14(3):e0213511. [CrossRef]
- Namujju J, Muhindo R, Mselle L T, Waiswa P, Nankumbi J, Muwanguzi P. Childbirth experiences and their derived meaning: A qualitative study among postnatal mothers in Mbale regional referral hospital, Uganda. Reprod Health. 2018;15(1),183. [CrossRef]
- Chadwick RJ, Cooper D, Harries J. Narratives of distress about birth in South African public maternity settings: A qualitative study. Midwifery. 2014;30:862-868. [CrossRef]
- Hastings-Tolsma M, Nolte GW. Temane A. Birth stories from South Africa: Voices unheard. Women Birth. 2018;31(1):e42-e50. [CrossRef]
- Malatji R, Madiba S. Disrespect and Abuse Experienced by Women during Childbirth in Midwife-Led Obstetric Units in Tshwane District, South Africa: A Qualitative Study. Int J Environ Res Pub Health. 2020;17:3667. [CrossRef]
- Wibbelink M, James S, Thomson AM. A qualitative study of women and midwives' reflections on midwifery practice in public maternity units in the Eastern Cape, South Africa. Afri J Mid Women Health. 2022;16(2):1-4. [CrossRef]
- Zitha E, Mokgatle MM. Women’s views of and responses to maternity services rendered during labor and childbirth in maternity units in a semi-rural district in South Africa. Int J Environ Res Pub Health. 2020;17(14):5035. [CrossRef]
- Stanton ME, Gogoi A. Dignity and respect in maternity care. BMJ Global Health 2022;5:e009023. [CrossRef]
- Freedman LP, Kruk ME. Disrespect and abuse of women in childbirth: challenging the global quality and accountability agendas. The Lancet. 2014;384(9948):e42-4. [CrossRef]
- World Health Organization. Standards for improving quality of maternal and newborn care in health facilities. World Health Organization. 2016.
- Bohren MA, Vogel JP, Tunçalp Ö, Fawole B, Titiloye MA, Olutayo AO, Ogunlade M, Oyeniran AA, Osunsan OR, Metiboba L, Idris HA. Mistreatment of women during childbirth in Abuja, Nigeria: a qualitative study on perceptions and experiences of women and healthcare providers. Reprod Health. 2017;14(1):9. [CrossRef]
- Vedam S, Stoll K, Taiwo TK, Rubashkin N, Cheyney M, Strauss N, McLemore M, Cadena M, Nethery E, Rushton E, Schummers L. The Giving Voice to Mothers study: inequity and mistreatment during pregnancy and childbirth in the United States. Reprod Health. 2019;16(1):77. [CrossRef]
- Bowser D, Hill K. Exploring evidence for disrespect and abuse in facility-based childbirth. Boston: USAID-traction project, Harvard school of public health. 2010.
- Hawkes S, Allotey P, Elhadj AS, Clark J, Horton R. The Lancet Commission on gender and global health. The Lancet. 2020 Aug 22;396(10250):521-2.
- Afulani PA, Kelly AM, Buback L, Asunka J, Kirumbi L, Lyndon A. Providers' perceptions of disrespect and abuse during childbirth: a mixed-methods study in Kenya. Health Policy Plan. 2020;35:577-586. [CrossRef]
- WHO recommendations: intrapartum care for a positive childbirth experience. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.
- Chikezie NC, Shomuyiwa DO, Okoli EA, Onah IM, Adekoya OO, Owhor GA, Abdulwahab AA. Addressing the issue of a de-pleting health workforce in sub-Saharan Africa. The Lancet. 2023;401(10389):1649-1650. [CrossRef]
- Okeny PK, Pittalis C, Monaghan CF, Brugha R, Gajewski J. Dimensions of patient-centred care from the perspective of patients and healthcare workers in hospital settings in sub-Saharan Africa: A qualitative evidence synthesis. Plos one. 2024;19(4):e0299627. [CrossRef]
Figure 1.
PRISMA flow chart illustrating the review process.
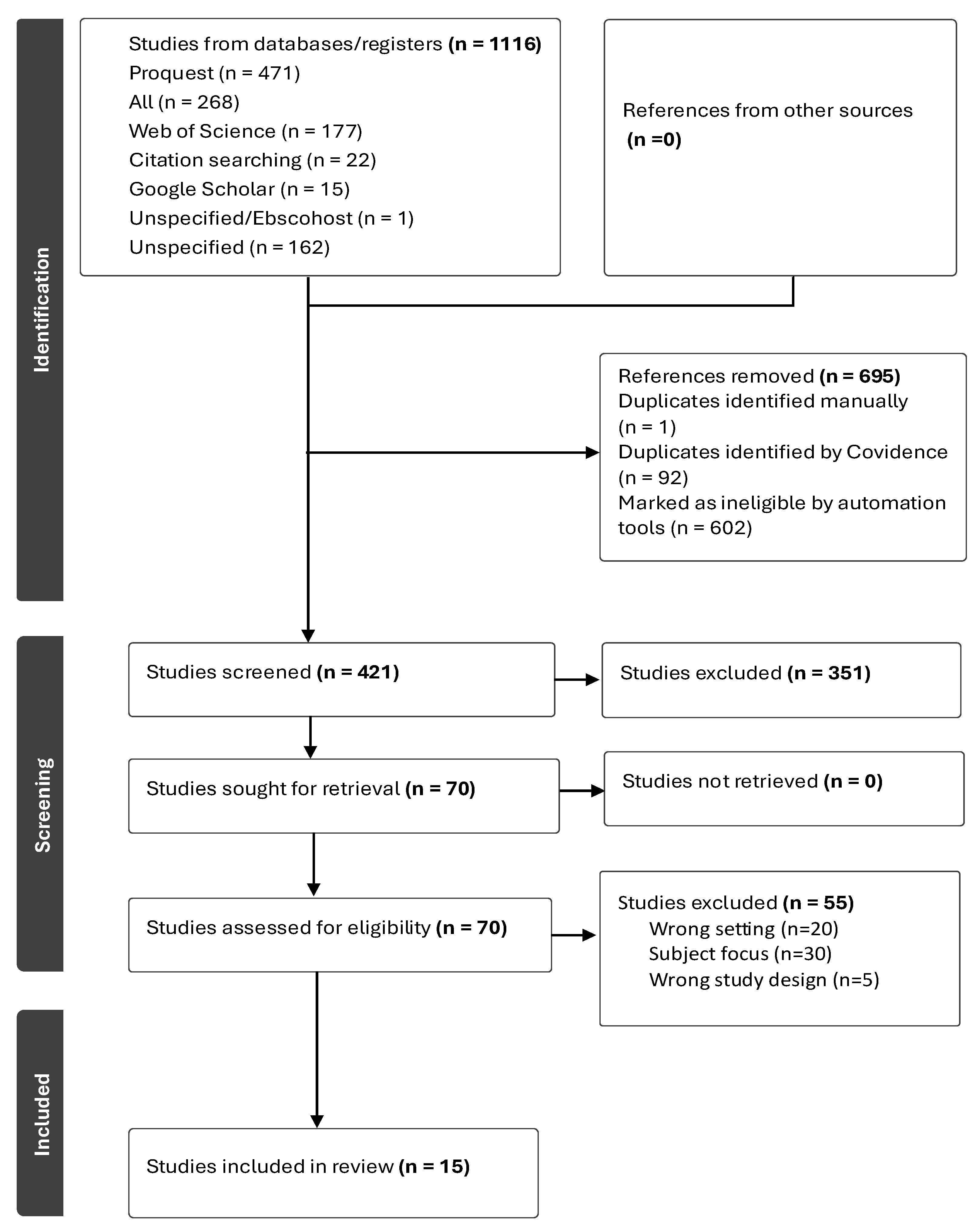
Figure 2.
Themes and sub-themes depicting intrapartum care experiences.
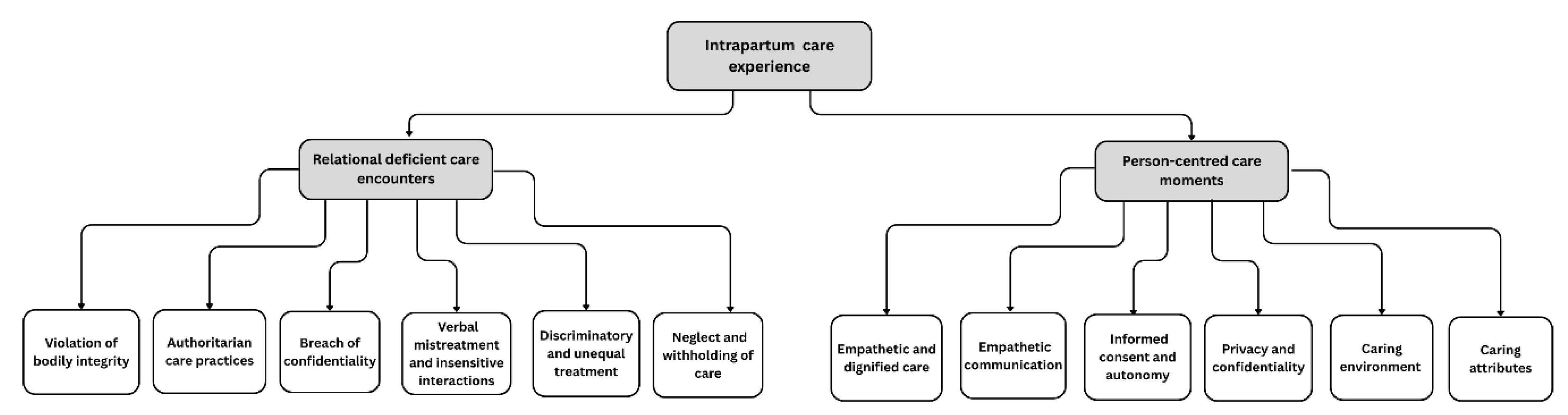

Table 1.
ECLIPSE Framework.
| Expectation | The study aims to provide insight into the experiences of women who gave birth in health facilities. |
|---|---|
| Client group | The focus is specifically on postpartum women who gave birth normally |
| Location | The studies conducted in sub-Saharan Africa |
| Impact | Compassion during intrapartum care |
| Professionals | Midwives/nurses and or doctors are the birth attendants. |
| Service | Refers to intrapartum care rendered to women within health facilities |
Table 2.
Inclusion criteria.
| Description | Rationale |
|---|---|
| Women who gave birth in health facilities across Sub-Saharan Africa | Ensures the review reflects women’s first-hand experiences of care within facility-based childbirth, where health system interactions are most visible and policy interventions are focused. |
| Experiences and perceptions of compassionate, respectful, empathetic, or dignified maternity care during childbirth | Aligns with the review’s aim to explore positive dimensions of care and identify elements that foster respectful, person-centred maternity practices. |
| Qualitative and mixed-methods studies with qualitative components | Captures the richness and depth of women’s narratives, emotional expressions, and interpretations of care that quantitative data alone may overlook. |
| Health facilities such as hospitals, maternity wards, or clinics providing childbirth services | Focuses on institutional contexts where respectful care policies and professional standards are most applicable and measurable. |
| Studies involving women who gave birth within six months prior to data collection | Minimizes recall bias and ensures accounts reflect recent practices, service quality, and prevailing care standards. |
| English language | Facilitates consistent data extraction, synthesis, and interpretation within the linguistic capabilities of the research team. |
| Peer-reviewed, full-text journal articles | Guarantees methodological rigour, transparency, and accessibility of complete findings for quality appraisal. |
| Published between 2012–2024 | Corresponds with the post-2011 period following the introduction of the Respectful Maternity Care Charter, capturing the growing policy and research focus on compassionate and respectful maternity care. |
| Studies conducted in Sub-Saharan African countries | Provides a contextual understanding of women’s experiences within a region marked by shared maternal health challenges, sociocultural contexts, and health system reforms. |
Table 3.
Themes and sub-themes.
| Theme | Theme |
|---|---|
| Person-centred care moments | Relational deficient care encounters |
| Sub-themes | Sub-themes |
| Empathetic and dignified care | Physical mistreatment |
| Empathetic communication | Unconsented care |
| Informed consent and autonomy | Verbal mistreatment and insensitive interactions |
| Privacy and confidentiality | Discriminatory and inequitable care |
| Caring environment | Breach of confidentiality |
| Caring attributes | Neglect and withholding of care |
Table 4.
Details of individual studies are included.
| Authors | Aim / objectives & birth setting | Main results related to the review purpose |
|---|---|---|
| Asrese [30] | To assess the quality of intrapartum care experienced by mothers at health centres and homes in the Jabi Tehinan district, Northwest Ethiopia. | Positive: emotional support, clean environment, privacy, appreciated companions. Negative: unfriendly staff, poor communication, uncaring, verbal abuse, discriminatory care. |
| Burrowes et al. [31] | To examine women’s experiences of care from midwives during labour and delivery including disrespect/abuse in public health centres and homes in Ethiopia. | Positive: facility recommended by friends, oral fluids allowed, appropriate positions. Negative: abuse, unconsented care, lack of privacy, neglect, denial of services/companions, unnecessary procedures, mobility restriction. Resource: inadequate beds. |
| Jiru & Sendo [32] | To explore clients’ and midwives’ perceptions of compassionate and respectful care during facility-based delivery in Bishoftu District (Oromia, Ethiopia). | Positive: caring treatment (“like a friend”). Negative: discriminatory care, verbal abuse, underqualified staff. |
| Afulani et al. [33] | To examine women’s facility–based childbirth experiences in a rural county in Kenya, to identify aspects of care that contribute to a positive or negative birth experience. |
Positive: Warm reception, caring treatment, birth companions allowed, clean linen Negative: abandonment, discriminatory care, verbal abuse. |
| Oluoch-Aridi et al. [34] | To explore women's experiences during childbirth at six health facilities across Embakasi sub-counties (public, private, faith-based) Nairobi, Kenya. | Positive: warm reception, dignified communication, supportive care. Negative: lack of information, discriminatory and non-dignified care, verbal abuse. Companions: often not allowed, women wanted support persons. |
| Kumbani et al. [35] | To describe women’s perceptions of perinatal care among women who delivered at a district hospital in Malawi. | Positive: good reception/respect, breastfeeding advice, positive attitudes, confidentiality. Negative: verbal abuse, neglect, abandonment. |
| Metta et al. [36] | To explore women’s childbirth experiences to inform a co-designed quality improvement intervention in four rural hospitals (including one faith-based) in southern Tanzania. | Positive: good communication, informed procedures, dignified care, midwife support. Negative: lack of information/compassion, verbal abuse. Companions: mixed views. |
| Shimpuku et al. [37] | To explore women's perceptions of childbirth experience at a hospital in rural Tanzania. | Positive: caring/friendly midwives, supportive care, good service, skilled HCPs. Negative: verbal abuse, lack of support/information, abandonment. Companions: relatives appreciated. |
| Munabi-Babigumira et al. [38] | To explore the nature of interactions between mothers and health workers in Mpigi and Rukungiri districts (health facilities and home), Uganda. | Positive: Dignified interactions, staff explained procedures, provider dedication despite constraints. Negative: lack of information, discriminatory care, verbal abuse. Resource: inadequate supplies. Companions: denied due to space. |
| Namujju et al. [39] | To explore childbirth experiences and their meaning among postnatal mothers in a public hospital, Uganda. | Positive: supportive care (comfort, touch, reassurance), empowerment via vaginal birth, cultural meaning in enduring pain. Negative: non-caring, rough handling, limited support. Companions: relatives appreciated and preferred. |
| Chadwick et al. [40] | To explore factors associated with negative maternity settings from women's birth narratives, City of Cape Town, South Africa. | Positive: kindness, reassurance, gentle touch Negative: abuse, neglect, abandonment reported by many. |
| Hastings-Tolsma et al. [41] | To describe experiences of women receiving care during childbirth in private, public, and maternity hospitals, and homes in South Africa. | Positive: shared decision-making in midwife-led care, respect for beliefs/preferences. Negative: neglect, abandonment, lack of autonomy, loneliness without companions. Companions: mixed experiences. |
| Malatji & Madiba [42] | To explore women’s experiences of care during childbirth and examine occurrence of disrespect & abuse (D&A) during childbirth in MOUs, South Africa. | Positive: gentle tone, reassurance, timely clinical care, respect for privacy. Negative: abuse, lack of support, discrimination, poor standards. Companions: mixed as some had, while others did not. |
| Wibbelink et al. [43] | To describe factors affecting clinical practice in public maternity units from women’s perspectives in the Eastern Cape, South Africa. | Positive: caring/friendly midwives, competence in complications, empathetic engagement. Negative: verbal abuse, neglect. |
| Zitha & Mokgatle [44] | To assess views of women about care received during labour and childbirth and interactions with midwives in MOUs and the district hospital in a semi-rural Tshwane district, South Africa. | Positive: empathetic/polite midwives, reassurance, privacy/modesty preserved. Negative: verbal abuse, neglect, lack of informed choice/advice. Companions: mostly denied. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



