Submitted:
12 November 2025
Posted:
13 November 2025
You are already at the latest version
Abstract
The intratumoral microbiota, comprising bacteria, fungi, and viruses within the tumor microenvironment, actively influences carcinogenesis. Key mechanisms include the induction of host DNA damage, modulation of critical oncogenic signaling pathways such as WNT-β-catenin, NF-κB, and PI3K, and the orchestration of inflammatory processes. The microbiome's interaction with the host immune system is complex and bidirectional. On one hand, specific microbes can foster a pro-tumorigenic niche by suppressing the activity of cytotoxic T cells and natural killer (NK) cells or by promoting the accumulation of immunosuppressive cell types like tumor-associated macrophages (TAMs). On the other hand, microbial components can serve as neoantigens for T cell recognition or produce metabolites that reprogram the immune landscape to enhance anti-tumor responses. The composition of this microbiome is emerging as a crucial factor influencing the outcomes of immunotherapies. Future research should focus on mechanistic studies using multi-omics approaches, well-designed clinical trials to validate microbial biomarkers, and the rational development of microbiome-targeted interventions.
Keywords:
intratumoral microbiome
; tumor microenvironment
; immune response
; cell therapy
; gut-tumor axis
; antitumor immunity
; CAR-T cells
1. Introduction
Immunotherapy represents a rapidly advancing field that has demonstrated significant progress in recent years with regard to the treatment of oncological diseases. The findings of research conducted to date indicate that this therapeutic method is effective in the suppression of tumor growth and the improvement of clinical outcomes. The treatment approach has been demonstrated to stimulate the host’s immune system, thereby restoring immunological functions and eliminating tumor cells over an extended period of time [1]. The employment of immunotherapy can be considered as a standalone treatment strategy or in combination with traditional methods, thereby demonstrating the potential for a synergistic effect [2]. Cellular immunotherapy can be defined as the administration of living immune cells to patients for therapeutic purposes. It may be active, as in dendritic cell vaccines that stimulate an antitumor immune response, or passive, as in adoptive cell transfer (ACT), where autologous or allogeneic lymphocytes with intrinsic antitumor activity are administered, either in their natural form or after modification [3]. Non-specific OCI encompasses a variety of cell types, including dendritic cells (DCs), natural killer cells (NKCs), cytokine-induced killer cells (CIKs), tumor-infiltrating lymphocytes (TILs), lymphocyte-activated killer cells (LAKs), and killer-induced macrophages (MAKs), among others. In specific OCI, immune cell activation is mediated by tumor antigens and specific stimulating factors. These methods include TIL-based therapy, T-cell receptor-transfer (TCR-T) technologies, and chimeric antigen receptor-positive T-cell (CAR-T) immunotherapy [4,5,6,7,8,9,10]. The U.S. Food and Drug Administration (FDA) has granted regulatory approval to several cell-based therapies. In the domain of immune cell therapies, a number of CAR-T products have received approval for the treatment of hematologic malignancies, including certain forms of leukemia, lymphoma, and multiple myeloma. Examples include tisagenlecleucel (Kymriah), axicabtagene ciloleucel (Yescarta), and idecabtagene vicleucel (Abecma) [11]. Furthermore, the TIL drug lifileucel (Amtagvi) has been approved for the treatment of adult patients with unresectable or metastatic melanoma [12]. However, immunotherapy still faces many challenges. These include relatively low efficacy in solid tumors, in part due to heterogeneity and the difficulty of targeting specific antigens. Other challenges include tumor microenvironment immunosuppression and complications in cellular drug delivery [13]. Furthermore, there are also safety concerns [14,15]. Immunotherapy has been shown to be associated with a risk of adverse effects, including unfavorable outcomes [16,17]. Nevertheless, the development of next-generation drugs and additional approaches aimed at increasing the effectiveness and safety of cell therapy is ongoing [18].
The human microbiome both positively and negatively contributes to carcinogenesis by influencing signaling pathways involved in inflammation, DNA repair, and stability [19]. Moreover, the gut microbiome is widely recognized as a factor that significantly influences the regulation of local and systemic immune responses in mouse models and human studies [20]. It has been demonstrated that the composition of the microbiota, particularly the levels of abundance of individual bacterial taxa, exerts a substantial influence on the efficacy of the host’s immune response [21]. The relationship between the microbiome and immune cells used in immunotherapy is a relatively new and understudied area of research [22]. A substantial body of research has evidenced the correlation between specific taxa of microbiota and the manifestation of a response to immunotherapy. However, the comparability of these findings is constrained by the paucity of shared species among studies. Clinical data underscores the deleterious effect of antibiotics administered prior to treatment outcomes and survival. Broad-spectrum antibiotics reduce microbial diversity, disrupt the balance between beneficial and unfavorable taxa, promote the growth of immunosuppressive fungi, and alter the intestinal mucosa, which disrupts host-microbiome interactions and modulate the immune response [23].
The long-standing hypothesis that microorganisms may inhabit tumor tissues of organs outside the gastrointestinal tract has only recently gained support through advanced technological methodologies, revealing that organs and tissues traditionally considered sterile can in fact harbor diverse microbial communities [24]. A range of molecular biology techniques are employed in the study of the intratumoral microbiome, including next-generation sequencing (NGS) methods such as the sequencing of the 16S rRNA gene and whole-genome shotgun sequencing (WGS). To validate NGS results and confirm the presence, localization, and metabolic activity of bacteria directly within the tumor, methods such as fluorescence in situ hybridization (FISH) and fluorescently labeled D-alanine incorporation technologies are used [25]. The handling of tumor tissues presents significant challenges due to the low concentration of bacterial DNA, rendering samples highly susceptible to contamination from reagents, the laboratory environment, and adjacent tissues [26]. Moreover, the analysis of bioinformatics data presents a considerable challenge, given the possibility of false-positive results in the identification of bacterial reads [27]. A substantial body of evidence suggests a close association between a number of malignant neoplasms and infection by microorganisms, including bacteria, viruses, and fungi. Intratumoral microbiota is regarded as an important element in the development of cancer, exhibiting both stimulatory and inhibitory effects on tumor progression [28,29].
The aim of this review is to summarize data on the role of the intratumoral microbiome in the development and progression of cancer, as well as the interaction of microorganisms in tumor tissue with immune cells, especially in the context of cellular immunotherapy.
2. Origin of the Intratumoral Microbiota and Relationships with Other Human Microbiomes
The human body contains a multitude of ecological niches that are populated by microorganisms. Furthermore, these distinct microbiomes have the capacity to influence each other [30]. For instance, the oral cavity is in direct connection with the gut, and members of the oral microbiome can enter the gut via the enteral route [31]. While the oral-intestinal barrier is generally considered to be effective in preventing the translocation of most microorganisms, there are instances in which these first lines of defense are compromised, allowing for oral-intestinal transfer. Low gastric acidity, particularly due to the use of proton pump inhibitors, has been demonstrated to shift the composition of the gut microbiota toward oral profiles [32]. A recent study showed that F. nucleatum resists gastric acid due to the presence of erucic acid in the cell membrane [33]. In addition, intestinal bacteria themselves may be a potential barrier to the growth of oral microorganisms in the intestine, providing colonization resistance [34]. However, some studies have not found significant colonization of the gut microbiome by oral bacteria in either healthy individuals or patients taking long-term antibiotics [35,36]. The hematogenous route of bacterial transmission from the oral cavity to the intestine involves oral bacteria, particularly pathobionts entering the bloodstream during transient bacteremia induced by daily activities such as toothbrushing or chewing, as well as by dental procedures that disrupt periodontal barriers [37]. These microbes survive in circulation by resisting immune clearance and interacting with endothelial cells, then translocate to intestinal vascular beds, where inflammation enhances adhesion and mucosal seeding, contributing to diseases like colorectal cancer and inflammatory bowel disease [38]. Other microbiomes, such as the skin or genital microbiome, can interact with the gut and oral microbiomes primarily through various metabolites [39,40]. Gut-derived metabolites, such as short-chain fatty acids (SCFAs), secondary bile acids, and tryptophan catabolites, reach the skin via the circulatory system. There, they modulate cutaneous barrier function, local immune responses, and the composition and activity of resident microbial communities. This shapes susceptibility to inflammatory dermatoses and ageing-related dysbiosis [41]. A meta-analysis found that, compared with low fiber intake, high fiber intake was consistently associated with an improved therapeutic response to cancer immunotherapy (pooled odds ratio: 5.79). In experimental models, restricting methionine and cysteine, as well as reducing leucine and glutamine intake, slowed tumour progression. Meanwhile, a combination of checkpoint inhibitors with intermittent fasting or a fasting-mimicking diet significantly reduced tumour volume in mice bearing melanoma. In patients, higher concentrations of short-chain fatty acids and lactic acid-producing bacteria (Faecalibacterium prausnitzii and Akkermansia muciniphila) correlated with increased objective response rates [42]. In an in vivo study, it has been demonstrated that skin damage can result in alterations to the intestinal microbiome, particularly through the increased expression of Reg3 and Muc2 in intestinal epithelial cells [43]. Through the gut–lung axis, the same classes of metabolites influence pulmonary immunity (for example by altering alveolar macrophage and regulatory T-cell function), which in turn modifies the ecological niche in the respiratory tract and can drive shifts in lung microbial composition and infection susceptibility [44].
The origins of intratumoral microbiota remain a subject of investigation. However, it has been demonstrated that microorganisms capable of penetrating the intestinal mucosal barrier and entering the bloodstream can disseminate to other organs within the gastrointestinal tract, thereby contributing to tumor development [45]. Therefore, bacteria that have migrated from the intestine to the liver have been demonstrated to play a role in the development of hepatocellular carcinoma [46]. Furthermore, the presence of intestinal bacteria has been shown to promote the dissemination of colorectal cancer metastases to the liver by enhancing the formation of a premetastatic niche and attracting metastatic cells [47]. The study showed that Fusobacterium is preferentially associated with cancer cells in metastases, and treatment with metronidazole reduces bacterial load, cell proliferation and tumor growth [48]. Another study demonstrated that in patients with colon cancer, compared with the control groups and patients with adenomatous polyps, there was an enrichment of oral biofilm bacteria (Fusobacterium, Gemella, Parvimonas, Granulicatella, Leptotrichia, Peptostreptococcus, Campylobacter, Selenomonas, Porphyromonas, Prevotella) and a number of intestinal taxa (Phascolarctobacterium, Bacteroides, Tyzzerella, Desulfovibrio, Eubacterium, Lachnospiraceae), with the species F. nucleatum dominating [49]. It was shown that alpha diversity in tumor samples was lower than in healthy tissue, in addition to a decrease in the representation of Bacteroides, Lachnospiraceae, Clostridiales and Clostridium and an increase in Enterococcus, Streptococcus in tumors [50]. The Bacilli class showed a bidirectional positive association with malignant melanoma. The Betaproteobacteria and Gammaproteobacteria classes demonstrated a causal relationship with an increased risk of developing malignant melanoma and basal cell carcinoma, respectively. In a reverse Mendelian analysis, malignant melanoma was associated with reduced abundance of members of the Bacteroidetes (Bacteroidota) phylum [51]. Veillonella parvula was identified as the most common taxon driving this association. In the lung cancer model, V. parvula-induced lower respiratory tract dysbiosis resulted in decreased survival, increased tumor burden, and the development of an inflammatory phenotype mediated by the cytokine IL-17 [52]. Experimental data have shown that intestinal bacteria, including Enterococcus faecalis and Escherichia coli, are able to migrate to the pancreas, forming an intrapancreatic microbiome primarily represented by the phyla Proteobacteria (Pseudomonadota), Bacteroidetes (Bacteroidota), and Firmicutes (Bacillota). Mice with oncogenic pancreatic mutations showed a progressive enrichment of Bifidobacterium pseudolongum and Actinobacteria, indicating the involvement of intestinal dysbiosis in the development and progression of pancreatic adenocarcinoma [53].
3. The Role of the Intratumoral Microbiome in Cancer Progression
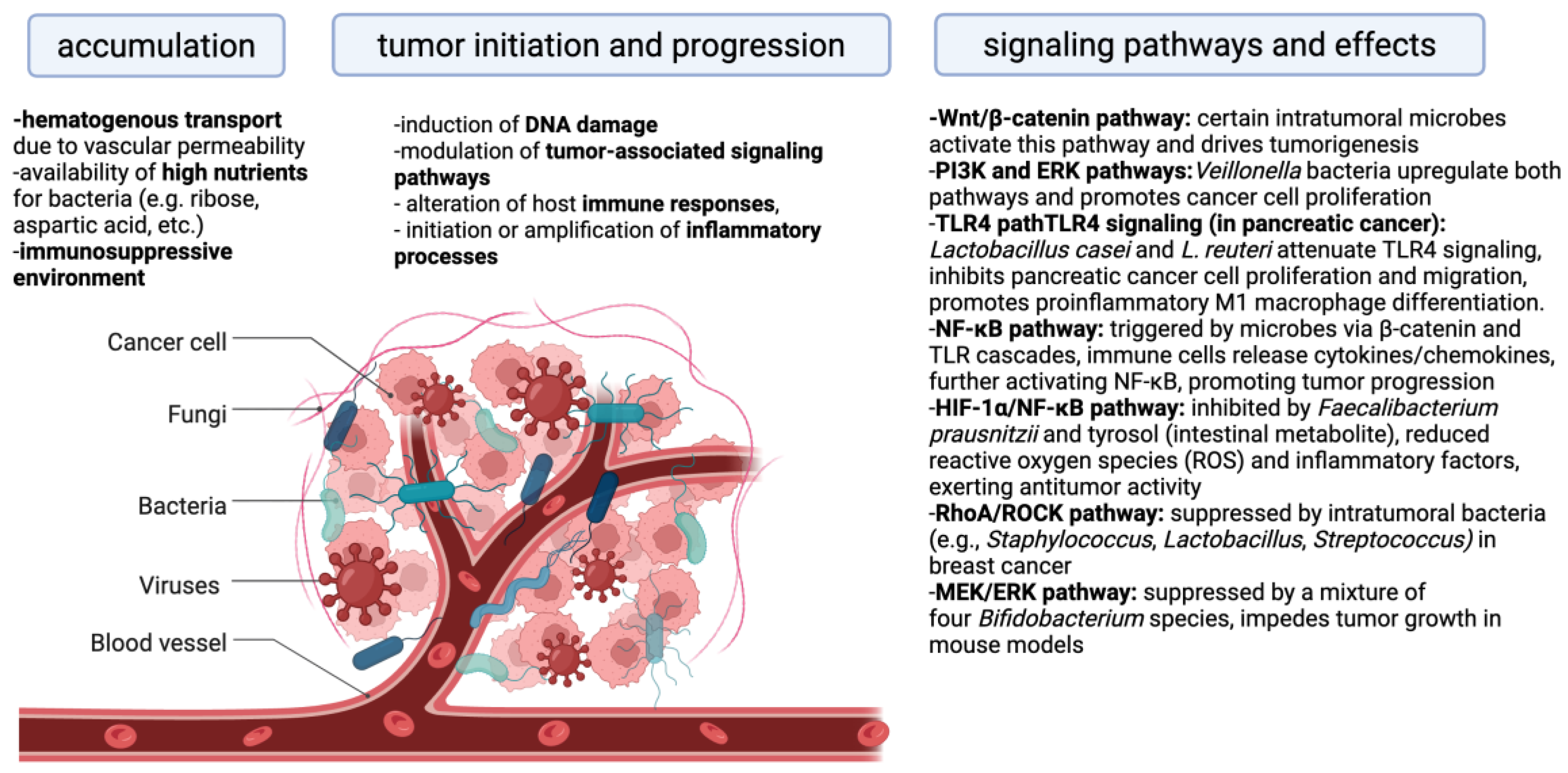
The intratumoral microbiome is constituted by a consortium of microorganisms, comprising bacteria, fungi, and viruses, that inhabit tumor tissue [54]. The potential mechanisms of microbes’ entry into the tumor include damaged mucosal membranes, direct migration from adjacent normal tissue, and hematogenous dissemination [55]. It is noteworthy that bacteria are predominantly localized inside cells [56]. The accumulation of microorganisms in tumor tissue is multifactorial. Immune evasion by cancer cells creates an immunosuppressive environment within the tumor, thereby allowing the tumor to evade immune clearance [57]. The process of hematogenous transport is facilitated by increased vascularization and vascular permeability of tumor tissue. Tumor tissue is characterized by a high nutrient content and the presence of specific metabolites (e.g., ribose, aspartic acid, etc.), which attract bacteria [58].
The tumor microbiome demonstrates low biomass. However, this parameter is influenced by various factors, including cancer type, microenvironmental conditions, and the implementation of antibiotic treatment [59,60]. The bacterial composition of tumors in various organs has been demonstrated to have distinct characteristics. The study revealed that the predominant taxa at the phylum level in esophageal carcinoma were Bacteroidetes, Firmicutes, Proteobacteria, Fusobacteria, and Actinobacteria. A substantial increase in the abundance of Firmicutes was observed, accompanied by a concurrent decrease in Proteobacteria [61]. The composition of the taxa Alistipes, Blautia, Pasteurellales, and Porphyromonas was correlated with the clinical characteristics of patients with gastrointestinal cancer, particularly colorectal cancer [62]. Studies have demonstrated that the composition of the lung microbiota undergoes significant alterations in lung cancer. An increased abundance of Thermus has been observed in patients with advanced-stage tumors, whereas Legionella is more prevalent in those with metastatic disease [63]. Moreover, metabolic pathways linked to smoking are enriched in the lung microbiota of cancer patients, with specific taxa such as Acidovorax showing notable associations with these changes [64]. Increased abundance of intratumoral Neisseriaceae has been demonstrated to promote accelerated lymph node metastasis in squamous cell carcinoma of the oropharyngeal tonsils [65]. Furthermore, the presence of certain tumor microorganisms, such as Brevundimonas and Staphylococcus, has been identified as a contributing factor to the development of distant metastases in breast cancer cases [66]. F. nucleatum, a bacterium detected in both primary tumors and metastatic lesions across various cancer types, is of particular interest, as it substantiates its potential role in the maintenance and spread of tumorigenesis [60].
The intratumoral microbiome exerts multifaceted effects on the processes of carcinogenesis. Extensive research has explored the mechanisms through which microbial communities contribute to tumor initiation and progression. To date, four principal mechanisms have been identified: induction of DNA damage with a consequent increase in mutation rates, modulation of tumor-associated signaling pathways, alteration of host immune responses, and the initiation or amplification of inflammatory processes [67]. The process of DNA mutation induction serves as a key mechanism in the context of microbial carcinogenicity. Some bacteria have been shown to cause DNA damage and mutations. E. coli that expresses the genotoxin colibactin (PKS locus) has been shown to induce double-strand DNA breaks and promote the development of colorectal cancer. It has been demonstrated that other pathogenic E. coli strains are capable of injecting the genotoxin UshA via the type III secretion system, thereby inducing DNA damage in intestinal epithelial cells [68]. Bacteroides fragilis-produced toxin (Bft) has been reported to increase levels of reactive oxygen species (ROS) in intestinal epithelial cells, leading to oxidation and DNA damage to host tissues and, consequently, malignant transformation of cells [69]. The signaling pathways that facilitate cell movement, growth, survival, and metabolism are critical to the fundamental functioning of normal and tumor tissues. The intratumoral microbiome may play a role in tumor-associated signaling cascades. The modulation of various signaling pathways by microbes is a critical factor in the development and progression of cancer [70]. Representatives of the intratumoral microbiome have been shown to modulate cascades of signaling pathways such as WNT/β-catenin, NF-κB, Toll-like receptors (TLR), ERK, PI3K, and RhoAROCK in tumor cells, thereby influencing carcinogenesis [67].
The Wnt/β-catenin signaling pathway is a conserved signaling pathway that regulates embryonic development and tissue homeostasis. β-catenin has been observed to bind to the TCF transcription complex and translocate to the nucleus, where it has been shown to stimulate transcription of downstream target genes such as c-Myc, cyclin D1, MMP, or survivin. This process contributes to the development of various types of cancer. [71]. It has been demonstrated that several intratumoral microorganisms possess the capacity to activate the Wnt/β-catenin signaling pathway. Annexin A1, a regulatory protein that has been recently implicated in this pathway, has been shown to enhance the expression of FadA, a secreted protein produced by F. nucleatum in colorectal tumours, via E-cadherin. [72]. The study demonstrated that bacteria belonging to the genus Veillonella upregulate the ERK and PI3K signaling pathways in lung cancer. Activation of the PI3K pathway promotes cancer cell proliferation and is considered an early event in lung tumorigenesis [73]. Moreover, stimulation of Toll-like receptor 4 (TLR4) by bacterial lipopolysaccharides induces the expression of proinflammatory genes, contributing to the progression of tumor-promoting inflammation across various cancer types [74]. The NF-κB signaling pathway plays a pivotal role in the development of chronic microbial-induced inflammation. It has been demonstrated that microorganisms can trigger the NF-κB pathway by activating the β-catenin and TLR signaling cascades. This activation results in the release of proinflammatory mediators and the development of a persistent inflammatory state. This process is bidirectional: immune cells recruited to the site of inflammation release cytokines and chemokines, which in turn increase NF-κB activation, creating a positive feedback loop that promotes tumor development and progression [75]. A recent study demonstrated that Faecalibacterium prausnitzii and the intestinal metabolite tyrosol exert antitumor effects by inhibiting the activation of the HIF-1α/NF-κB signaling pathway, resulting in reduced levels of reactive oxygen species and inflammatory factors [76]. The presence of bacteria within tumor cells has been shown to suppress the RhoA/ROCK signaling pathway, thereby facilitating the adaptation of circulating tumor cells to fluid shear stress through cytoskeletal remodeling and enhancing their potential for distant colonization [77]. Elevated concentrations of Staphylococcus, Lactobacillus, and Streptococcus have been detected within breast cancer cells, where these bacteria inhibit the RhoA/ROCK pathway, a key regulator of cytoskeletal organization. This inhibition enables tumor cells to withstand mechanical stress encountered in the circulatory system, reducing cellular damage and promoting metastatic dissemination [78].
However, it has been demonstrated that certain microorganisms can exert a beneficial influence by impeding the progression of cancer. Bacterial peptides are presented on tumor and antigen-presenting cell HLA molecules, creating neo-like targets that can be recognized by T cells and potentially broaden antitumor repertoires. Intracellular tumor bacteria and their microbe-associated molecular patterns can activate pattern-recognition pathways, interfacing with innate sensing hubs that shape T cell priming in the tumor microenvironment [79]. Microbial-derived metabolites (e.g. short-chain fatty acids (SCFAs) can reprogram local immunity and myeloid states; colorectal models show that leveraging microbiota metabolism can increase intratumoral SCFAs and augment chemotherapy and immune activation [80]. Therefore, Lactobacillus casei and Lactobacillus reuteri have been documented to impede the proliferation and migration of pancreatic cancer cells by attenuating TLR4 signaling. Furthermore, these bacterial species counteract the induction of the M2 macrophage phenotype by pancreatic cancer cells and promote the differentiation toward the pro-inflammatory M1 macrophage subtype [81]. Besides, a study employing a mouse glioma model demonstrated that a mixture of four Bifidobacterium species impeded tumor growth by suppressing the MEK/ERK signaling pathway [82].
Figure 1.
The key mechanisms and signaling pathways that explain the influence of the intratumoral microbiome on cancer development.
Figure 1.
The key mechanisms and signaling pathways that explain the influence of the intratumoral microbiome on cancer development.
4. The Relationship Between Immune Cells and Intratumoral Microbiota in the Context of Treatment Outcomes
The intratumoral microbiota exerts a multifaceted influence on immune cells, shaping the unique immune microenvironment of tumors. Early in their interactions, microorganisms are recognized by the innate immune system through highly conserved pathogen-associated molecular patterns (PAMPs), including lipopolysaccharides (LPS), unmethylated double-stranded DNA, lipoproteins, single-stranded RNA, and flagellin [83]. These patterns are detected by pattern recognition receptors (PRRs), such as Toll-like receptors (TLRs) and Nod-like receptors (NLRs), initiating signaling cascades that regulate inflammation, activation of antigen-presenting cells, and subsequent immune response [84]. Transcriptional and immune profiles of tumor tissues demonstrate that a high load of intratumoral microbiota can significantly alter the composition of immune infiltration. Specifically, in nasopharyngeal carcinoma, an increased bacterial load is associated with decreased CD8⁺ T-cell infiltration, leading to a pronounced immunosuppressive effect and reduced antitumor activity of cytotoxic lymphocytes [85]. These effects are related to the fact that microbes are capable of not only causing inflammation, but also selectively suppressing key components of the adaptive immune system. Some bacteria use specific molecular mechanisms to evade immune surveillance. For example, Helicobacter pylori produce vacuolating cytotoxin A (VacA), which enhances cancer cell colonization while simultaneously suppressing T-cell proliferation. VacA disrupts antigen presentation by B cells, alters macrophage signaling pathways, and thereby weakens the immune system’s ability to destroy infected cells [86]. Similar immunosuppressive properties have been identified in F. nucleatum. This microorganism can interact with inhibitory receptors, including TIGIT (T cell immunoreceptor with Ig and ITIM domains) and CEACAM1 (carcinoembryonic antigen-related cell adhesion molecule 1), blocking natural killer (NK) cell cytotoxicity and T cell activity. This creates a microenvironment conducive to colorectal cancer progression [87]. Furthermore, in oral squamous cell carcinoma (OSCC), F. nucleatum activates the GalNAc-autophagy-TBC1D5 signaling pathway, which causes membrane GLUT1 accumulation, increases lactate production, and stimulates the formation of tumor-associated macrophages (TAMs). These macrophages enhance inflammatory metabolism and accelerate tumor growth [88].
Microbial metabolites also play a key role in regulating immune cells. In the tumor microenvironment, short-chain fatty acids, nucleosides, bile acid derivatives, and tryptophan catabolites influence dendritic cell maturation, T-cell polarization, and NK cell activity through receptor and epigenetic mechanisms [89]. These metabolites can both enhance the immune response and maintain immunosuppression depending on their concentration, local bioavailability, and interaction with immune cell receptors. In addition to their metabolic effects, bacteria can directly integrate into antigen-presentation mechanisms. Tumor cells are capable of presenting intracellular bacterial peptides on HLA class I and II molecules, creating additional antigenic targets for T cells [90]. This additional layer of antigenicity alters the specificity of T-cell receptors and their priming dynamics, complementing the action of tumor neoantigens [91]. Certain members of the oral microbiota, such as Porphyromonas gingivalis, possess pronounced immunomodulatory properties. Within tumor tissue, P. gingivalis can activate the NLRP3 inflammasome, inducing neutrophils to release elastase and promoting the formation of an inflammatory and immunosuppressive microenvironment [92]. Furthermore, stimulation of macrophages with P. gingivalis or its lipopolysaccharides is accompanied by a significant increase in the secretion of IL-1α, CCL3, and CCL5 [93]. Different bacterial strains induce different cytokine responses, indicating strain-specific immunomodulation. Single-nucleus RNA-sequencing (scRNA-seq) data reveal significant B cell heterogeneity in tumors and indicate that the intratumoral microbiome regulates their differentiation through the activation of genes including MMEL1 and CITED4 [94]. Actinomyces co-localizes with colorectal cancer-associated fibroblasts and reduces CD8+ T-lymphocyte infiltration into the tumor microenvironment by activating the TLR2/NF-κB pathway, thereby promoting tumor progression [95].
The study demonstrated that intratumoral microbiota shape tumor–immune interactions across multiple cancer types. In MMTV-PyMT mice, imaging revealed spatial segregation between microbes and CD4⁺/CD8⁺ T cells, indicating exclusion of activated T cells from bacterially colonized regions [96]. In the mice PDAC model, fungal components drove IL-33 upregulation and TH2/ILC2 recruitment, while IL-33 ablation or antifungal therapy reversed tumor growth [97]. In early-stage triple-negative breast cancer, higher microbial diversity and load correlated with increased CD4⁺CXCL13⁺ T cells, reduced tumor-associated macrophages, and better chemo-immunotherapy response [98]. In prostate cancer, Cutibacterium acnes was linked to Treg infiltration and macrophage PD-L1, CCL17, and CCL18 upregulation, supporting an immunosuppressive microenvironment that may promote tumor progression [99].
These results suggest the benefits of microbial interventions in the context of immunotherapy; however, further studies are needed in patients with different types of cancer.

Table 1.
Examples of studies aimed at studying the influence of intratumoral microorganisms and the immune response.
Table 1.
Examples of studies aimed at studying the influence of intratumoral microorganisms and the immune response.
| Year | Disease/Model | Population | Brief Results | References |
|---|---|---|---|---|
| 2024 | Colorectal cancer | Data from The Cancer Genome Atlas (TCGA) database | Network analysis revealed significant interactions between microbial abundance and genes involved in CTL evasion. Among these, suppressor of cytokine signaling 1 (SOCS1) exhibited the highest number of negative correlations, particularly with the genera Phascolarctobacterium, Sneathia, and Intestinimonas. Additionally, the genus Oscillibacter was negatively associated with exon skipping in the CD74 gene, indicating that the tumor-associated microbiota may influence the regulation of antigen presentation and thereby modulate the antitumor immune response. | Liu et al. [100] |
| 2024 | Breast cancer | Female MMTV-PyMT transgenic mice | Both three-dimensional imaging and X-Y optical sections revealed spatial segregation between the intratumor microbiome and CD4⁺ and/or CD8⁺ T cell clusters, indicating the exclusion of activated T cells from bacterially colonized tumor regions. These data are consistent with the observed isolation of TLS and NK cells from microbe-enriched areas, highlighting the spatial compartmentalization of immune and microbial niches within tumor tissue. | Wang et al. [96] |
| 2022 | Lung cancer | 12 patients with early-stage lung cancer |
The bacterial load was significantly higher in tumor cells compared to T cells, macrophages, other immune cells, and stromal components, forming a gradient that increased from normal lung tissue and tertiary lymphoid structures to tumor cells and the airways. This pattern suggests potential penetration of intratumoral bacteria through the respiratory tract. Moreover, bacterial load levels showed a positive correlation with the expression of oncogenic β-catenin, tumor histological type, and environmental exposures. | Wong-Rolle et al. [101] |
| 2024 | Colorectal cancer | C57BL/6 (B6) and Balb/c mice | The immunogenic chemotherapeutic agent oxaliplatin synergizes with E. coli, activating the innate and adaptive immune response in the colorectal tumor microenvironment, leading to complete remission and the formation of stable antitumor immunological memory in mice. The combined action of oxaliplatin and bacteria significantly enhances the expression of costimulatory and antigen-presenting molecules on antigen-presenting cells, facilitating the effective activation of cytotoxic T lymphocytes against tumor cells. | Lim et al. [102] |
| 2022 | Colorectal cancer | C57BL/6 (B6) Thy 1.1 mice | The live attenuated Brucella melitensis strain (BmΔvjbR) was found to selectively colonize tumor tissue and remodel the tumor microenvironment by inducing proinflammatory polarization of M1 macrophages and enhancing both the number and activity of CD8⁺ cytotoxic T cells. In a colorectal adenocarcinoma model, treatment combining BmΔvjbR with adoptive transfer of tumor-specific CD8⁺ T cells almost completely suppressed tumor growth and achieved 100% animal survival. These findings highlight the potential of live attenuated bacteria to overcome tumor resistance to CAR-T therapy by remodeling the tumor microenvironment and activating macrophage-T-cell antitumor immunity. | Guo et al. [103] |
| 2023 | Leukemia | Non-obese diabetic scid gamma mice | A probiotic-targeted CAR-T cell (ProCAR) platform was developed in which tumor-colonizing probiotics secrete synthetic targets that mark tumor tissue for local lysis by CAR-T cells. Using the Escherichia coli Nissle 1917 strain with a synchronized lysis system (SLIC) enabled the release of synthetic targets directly into the tumor microenvironment, inducing safe and effective CAR-T cell activation in various cancer models. Additionally, an engineered strain co-expressing the chemokine mutant CXCL16K42A enhanced ProCAR-T cell recruitment and antitumor activity, resulting in increased hCD45⁺CD3⁺ T cell infiltration and significant tumor growth inhibition without toxic effects. | Vincent et al. [104][ |
| 2021 | Melanoma | C57BL/6NTac germ-free, BALB/cAnNCrl, B6-Ly5.1/Cr, B6-Ifnar1 (Ifnar1 KO) and C57BL/6J-Tmem173/J (STING KO) mice, 6 patients with melanoma | The microbiota regulates the immune compartment of the tumor microenvironment, reprogramming mononuclear phagocytes into immune-stimulatory monocytes and dendritic cells. The absence of microbiota shifts the balance of the tumor microbiome toward pro-tumorigenic macrophages, while microbial STING agonists induce type I interferon production, regulating macrophage polarization and NK cell–dendritic cell interactions. Modulation of the microbiota with a high-fiber diet activated the IFN-I–NK–DC axis and enhanced the efficacy of immune checkpoint blockade therapy, as confirmed in both experimental models and patients with melanoma. | Lam et al. [105] |
| 2022 | Pancreatic cancer | C57BL/6 mice | Oncogenic KrasG12D was shown to induce IL-33 expression in pancreatic ductal adenocarcinoma cells, which promotes the recruitment and activation of TH2 and ILC2 cells, which stimulate tumor growth. Ablation of IL-33 in tumor cells or antifungal therapy reduced TH2 and ILC2 cell infiltration, induced tumor regression, and increased survival. Thus, the intratumor mycobiome regulates IL-33 secretion and promotes the formation of a protumorigenic environment, opening up opportunities for targeted therapy for PDAC. | Alam et al. [97] |
| 2025 | Breast cancer | 89 female patients | In patients with early-stage TNBC treated with neoadjuvant chemo-immunotherapy, the pCR group exhibited higher intratumoral microbiota diversity and load compared to the non-pCR group. Single-cell RNA sequencing revealed enhanced T cell infiltration and reduced tumor-associated macrophages in the pCR group. Microbiota load positively correlated with CD4⁺CXCL13⁺ T cells and negatively with CD68⁺SPP1⁺ macrophages. Combined 16S and scRNA-seq analyses confirmed bacterial presence in both cancer and immune cells. A predictive model integrating microbial and clinicopathological data accurately forecasted pCR outcomes. | Chen et al. [98] |
| 2022 | Cutaneous melanoma | Data from The Cancer Genome Atlas (TCGA) database |
Low CD8⁺ T cell counts were associated with worse patient survival (OR = 1.57; 95% CI: 1.17–2.10; p = 0.002). The Lachnoclostridium genus showed the highest positive correlation with CD8⁺ T cell infiltration and expression of chemokines CXCL9, CXCL10, and CCL5, and its high level was associated with a reduced risk of mortality (p = 0.0003). | Zhu et al. [106] |
| 2021 | Prostate cancer | 137 men | Macrophages stimulated with Cutibacterium acnes in vitro were shown to increase the expression of PD-L1, CCL17, and CCL18 (p < 0.05), and the presence of C. acnes in prostate cancer patients was positively correlated with Tregs infiltration in the tumor stroma and epithelium (p = 0.0004 and p = 0.046). These data suggest that C. acnes contribute to the formation of an immunosuppressive tumor microenvironment that promotes prostate cancer progression. | Davidsson et al. [99] |
| 2018 | Pancreatic cancer | KC, C57BL/6 (H-2Kb) mice, | Pancreatic tumor tissue in mice and humans contains a significantly more abundant microbiome compared to normal tissue, with certain bacterial taxa selectively enriched compared to the intestine. Microbiome ablation prevented the development of pancreatic ductal adenocarcinoma and induced immune reprogramming of the microenvironment with increased M1 macrophage polarization and activation of CD4⁺ Th1 and CD8⁺ T cells. Furthermore, microbiome ablation enhanced the efficacy of immunotherapy by upregulating PD-1 expression, while the PDA microbiome induced a tolerogenic phenotype through activation of specific Toll-like receptors. | Pushalkar et al. [53] |
| 2019 | Pancreatic cancer | 68 patients | Long-term survivor patients with pancreatic ductal adenocarcinoma exhibited higher alpha diversity of the tumor microbiome and a characteristic microbial signature (Pseudoxanthomonas–Streptomyces–Saccharopolyspora–Bacillus clausii) predicting a favorable prognosis. Transplantation of microbiota from long-term survivor donors into mice slowed tumor growth and enhanced immune infiltration. Immunohistochemistry analysis revealed that long-term survivor patients had significantly higher densities of CD3⁺, CD8⁺, and GzmB⁺ T cells (p = 0.0273; p < 0.0001; p = 0.04), which positively correlated with both overall survival and microbiome diversity, suggesting a link between microbial diversity, CD8⁺ T cell activation, and the antitumor immune response. | Riquelme et al. [13] |
5. Current limitation and Future Direction
Despite mounting evidence that the intratumoral microbiome plays a pivotal role in cancer progression and therapeutic response, several critical limitations impede the translation of these findings into clinical practice. A significant deficit in the extant literature pertains to the paucity of research addressing the influence of immune-cell therapies, including adoptive T-cell transfer, CAR-T or TIL therapies, on outcomes across diverse cancer types within the context of intratumoral microbial communities. To date, the majority of studies have been of an observational nature, having been limited to particular tumor types or immune checkpoint inhibitors, as opposed to cell therapies. For example, while the intratumoral microbiome has been implicated in shaping responses to immunotherapy, data specific to immune cell therapy remains scarce [108].
Mechanistically, the pathways by which intratumoral microbes modulate immune responses are only beginning to be elucidated. The complexity of microbial-immune-tumor cross-talk remains under-characterized, particularly in the setting of treated tumors, immune cell infusion, or following therapy-induced modifications of the tumor microenvironment. Although studies report involvement of pathways such as STING, TLR/NF-κB, β-catenin, and ROS signaling in microbe-driven immune modulation [109]. Furthermore, the relationship between extratumoral microbiomes (gut, oral cavity, and respiratory tract) and the intratumoral microbiome remains to be elucidated. The sources of the tumor-resident microbiome—whether via translocation, circulation, lymphatic spread, or local colonization—vary across tumor types and clinical contexts. In addition, the impact of these sources on intratumoral immune modulation is remains unclear [80].
These limitations indicate several key avenues for future research. In order to elucidate the manner in which specific microbial taxa or their metabolites modulate the behavior of transplanted immune cells, including their persistence, exhaustion, phenotype, trafficking, and interactions with the host immune microenvironment, mechanistic studies employing advanced experimental systems are required. Examples of such systems include tumour organoids, humanized mouse models, spatial transcriptomics, and multi-omics approaches. [110]. Prospective clinical trials incorporating longitudinal microbiome sampling (tumor-intrinsic, gut, and oral) in patients receiving immune cell therapy are essential to delineate associations between microbial community states and therapeutic outcomes (response, persistence, and toxicity) and to evaluate the efficacy of microbiome-modulating interventions [111]. Comprehensive mapping of the interrelationships among systemic microbiomes (gut, oral, and skin), the intratumoral microbiome, and the immune landscape is necessary to identify upstream microbial drivers and causal pathways underlying immune modulation. The validation of microbial signatures as biomarkers or companion diagnostics for immune-based therapies, including immune cell therapies, should be prioritized, with an emphasis on assessing their additive predictive value beyond existing genomic, immunological and clinical parameters [112]. Therapeutic innovation should focus on the rational development of microbiome-targeted adjuncts to immune cell therapy, such as engineered bacterial strains, bacteriophage-based strategies, or microbial metabolite modulators, while ensuring rigorous evaluation of their safety, off-target effects, and regulatory compliance. Translational progress in this field will depend on the standardization of microbiome sampling and sequencing protocols, stringent contamination control, and the establishment of open data-sharing frameworks to enhance reproducibility and accelerate biomarker discovery [113].
6. Conclusions
The intratumoral microbiome is a critical and functionally active component of the tumor microenvironment that significantly impacts cancer development, progression, and response to therapy. Microorganisms can either promote tumorigenesis through mechanisms like inducing genomic instability and fostering an immunosuppressive state or inhibit it by enhancing anti-tumor immunity. Future research should focus on mechanistic studies using multi-omics approaches, well-designed clinical trials to validate microbial biomarkers, and the rational development of microbiome-targeted interventions. Harnessing the therapeutic potential of the intratumoral microbiome could lead to innovative strategies to overcome treatment resistance and improve patient outcomes.
Author Contributions
Design and the main concept of the paper, G.L., D.S., A.S. and D.G.; writing—original draft, G.L. and D.S.; visual material preparation, D.S., G.L.; funding acquisition, D.S.; writing—review and editing, G.L., D.S., A.S., O.M. and D.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ministry of Education and Science, grant number КBК: 075 0110 47 2 U8 70440 621. Scientific topic code: FSSF-2025-0004.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
The authors acknowledge the BioRender team for providing the artwork creation online service (https://www.BioRender.com, accessed on 25 October 2025).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CAR-T | Chimeric Antigen Receptor-Positive T-cell |
| NK | Natural Killer (cells) |
| NF-κB | NF-kappa B (Signaling Pathway) |
| PI3K | PI3K (Signaling Pathway) |
| TAMs | Tumor-Associated Macrophages |
| ACT | Adoptive Cell Transfer |
| OCI | Oncology Cellular Immunotherapy |
| DCs | Dendritic Cells |
| NKCs | Natural Killer Cells |
| CIKs | Cytokine-Induced Killer Cells |
| TILs | Tumor-Infiltrating Lymphocytes |
| LAKs | Lymphocyte-Activated Killer Cells |
| MAKs | Killer-Induced Macrophages |
| TCR-T | T-cell Receptor-Transfer |
| FDA | U.S. Food and Drug Administration |
| NGS | Next-Generation Sequencing |
| rRNA | Ribosomal RNA |
| WGS | Whole-Genome Shotgun sequencing |
| FISH | Fluorescence In Situ Hybridization |
| SCFAs | Short-Chain Fatty Acids |
| ROS | Reactive Oxygen Species |
| TLR | Toll-like receptors |
| ERK | ERK (Signaling Pathway) |
| RhoA/ROCK | RhoA/ROCK signaling pathway |
| TLR4 | Toll-like Receptor 4 |
| HIF-1α | Hypoxia-Inducible Factor 1 Alpha |
| HLA | Human Leukocyte Antigen |
| PAMPs | Pathogen-Associated Molecular Patterns |
| LPS | Lipopolysaccharides |
| PRRs | Pattern Recognition Receptors |
| TLRs | Toll-like Receptors |
| NLRs | Nod-like Receptors |
| VacA | Vacuolating cytotoxin A |
| TIGIT | T cell Immunoreceptor with Ig and ITIM domains |
| CEACAM1 | Carcinoembryonic antigen-related cell adhesion molecule 1 |
| OSCC | Oral Squamous Cell Carcinoma |
| GLUT1 | Glucose Transporter 1 |
| PDAC | Pancreatic Ductal Adenocarcinoma |
| ILC2 | Innate Lymphoid Cell 2 |
| PD-L1 | Programmed Death-Ligand 1 |
| TCGA | The Cancer Genome Atlas |
| CTL | Cytotoxic T Lymphocyte |
| TLS | Tertiary Lymphoid Structures |
| SLIC | Synchronized Lysis System |
| IFN-I | Type I Interferon |
| STING | Stimulator of Interferon Genes |
References
- Mukherjee, A.G.; Wanjari, U.R.; Namachivayam, A.; Murali, R.; Prabakaran, D.S.; Ganesan, R.; Renu, K.; Dey, A.; Vellingiri, B.; Ramanathan, G.; et al. Role of Immune Cells and Receptors in Cancer Treatment: An Immunotherapeutic Approach. Vaccines 2022, 10, 1493, doi:10.3390/vaccines10091493. [CrossRef]
- Zhang, Y.; Zhang, Z. The History and Advances in Cancer Immunotherapy: Understanding the Characteristics of Tumor-Infiltrating Immune Cells and Their Therapeutic Implications. Cell. Mol. Immunol. 2020, 17, 807–821, doi:10.1038/s41423-020-0488-6. [CrossRef]
- Hayes, C. Cellular Immunotherapies for Cancer. Ir. J. Med. Sci. 2021, 190, 41–57, doi:10.1007/s11845-020-02264-w. [CrossRef]
- Zhao, Y.; Deng, J.; Rao, S.; Guo, S.; Shen, J.; Du, F.; Wu, X.; Chen, Y.; Li, M.; Chen, M.; et al. Tumor Infiltrating Lymphocyte (TIL) Therapy for Solid Tumor Treatment: Progressions and Challenges. Cancers 2022, 14, 4160, doi:10.3390/cancers14174160. [CrossRef]
- Sharma, A.; Ren, X.; Rosato, A.; Sangiolo, D.; Wang, Z.; Tettamanti, S.; Zhang, Y.; Rettinger, E.; Fenix, K.A.; Sommaggio, R.; et al. Cytokine-Induced Killer (CIK) Cells, Successes and Challenges: Report on the First International Conference Dedicated to the Clinical Translation of This Unique Adoptive Cell Immunotherapy. Cancer Immunol. Immunother. CII 2024, 73, 21, doi:10.1007/s00262-023-03605-1. [CrossRef]
- Chu, J.; Gao, F.; Yan, M.; Zhao, S.; Yan, Z.; Shi, B.; Liu, Y. Natural Killer Cells: A Promising Immunotherapy for Cancer. J. Transl. Med. 2022, 20, 240, doi:10.1186/s12967-022-03437-0. [CrossRef]
- Wculek, S.K.; Cueto, F.J.; Mujal, A.M.; Melero, I.; Krummel, M.F.; Sancho, D. Dendritic Cells in Cancer Immunology and Immunotherapy. Nat. Rev. Immunol. 2020, 20, 7–24, doi:10.1038/s41577-019-0210-z. [CrossRef]
- Chen, P.; Chen, Y.; Wang, Y.; Sharma, A.; Veronika, L.-K.; Weiher, H.; Maria, A.G.-C.; Schmidt-Wolf, I.G.H. Macrophage-Derived pro-Inflammatory Cytokines Augment the Cytotoxicity of Cytokine-Induced Killer Cells by Strengthening the NKG2D Pathway in Multiple Myeloma. Sci. Rep. 2025, 15, 16739, doi:10.1038/s41598-025-99289-x. [CrossRef]
- Tan, S.; Li, D.; Zhu, X. Cancer Immunotherapy: Pros, Cons and Beyond. Biomed. Pharmacother. Biomedecine Pharmacother. 2020, 124, 109821, doi:10.1016/j.biopha.2020.109821. [CrossRef]
- Jogalekar, M.P.; Rajendran, R.L.; Khan, F.; Dmello, C.; Gangadaran, P.; Ahn, B.-C. CAR T-Cell-Based Gene Therapy for Cancers: New Perspectives, Challenges, and Clinical Developments. Front. Immunol. 2022, 13, 925985, doi:10.3389/fimmu.2022.925985. [CrossRef]
- Khan, A.N.; Asija, S.; Pendhari, J.; Purwar, R. CAR-T Cell Therapy in Hematological Malignancies: Where Are We Now and Where Are We Heading For? Eur. J. Haematol. 2024, 112, 6–18, doi:10.1111/ejh.14076. [CrossRef]
- Hu, L.; Fan, C.; Bross, P.; Das, A.; Cho, E.S.; Knudson, K.M.; Tegenge, M.; Gao, Q.; Brewer, J.R.; Theoret, M.R.; et al. FDA Approval Summary: Lifileucel for Unresectable or Metastatic Melanoma Previously Treated with an Anti–PD-1–Based Immunotherapy. Clin. Cancer Res. 2025, 31, 4004–4009, doi:10.1158/1078-0432.CCR-25-0880. [CrossRef]
- Zhao, T.; You, J.; Wang, C.; Li, B.; Liu, Y.; Shao, M.; Zhao, W.; Zhou, C. Cell-Based Immunotherapies for Solid Tumors: Advances, Challenges, and Future Directions. Front. Oncol. 2025, 15, 1551583, doi:10.3389/fonc.2025.1551583. [CrossRef]
- Bates, S.M.; Evans, K.V.; Delsing, L.; Wong, R.; Cornish, G.; Bahjat, M. Immune Safety Challenges Facing the Preclinical Assessment and Clinical Progression of Cell Therapies. Drug Discov. Today 2024, 29, 104239, doi:10.1016/j.drudis.2024.104239. [CrossRef]
- Leonov, G.E.; Grinchevskaya, L.R.; Makhnach, O.V.; Samburova, M.V.; Goldshtein, D.V.; Salikhova, D.I. Safety Assessment of Stem Cell-Based Therapies: Current Standards and Advancing Frameworks. Cells 2025, 14, 1660, doi:10.3390/cells14211660. [CrossRef]
- Jayathilaka, B.; Mian, F.; Franchini, F.; Au-Yeung, G.; IJzerman, M. Cancer and Treatment Specific Incidence Rates of Immune-Related Adverse Events Induced by Immune Checkpoint Inhibitors: A Systematic Review. Br. J. Cancer 2025, 132, 51–57, doi:10.1038/s41416-024-02887-1. [CrossRef]
- Mw, H.; Sy, J.; Ch, S.; H, P.; Jp, G.; Ry, H.; Kw, K.; Dh, Y. Incidence of Immune Effector Cell-Associated Neurotoxicity among Patients Treated with CAR T-Cell Therapy for Hematologic Malignancies: Systematic Review and Meta-Analysis. Front. Neurol. 2024, 15, doi:10.3389/fneur.2024.1392831. [CrossRef]
- Garg, P.; Pareek, S.; Kulkarni, P.; Horne, D.; Salgia, R.; Singhal, S.S. Next-Generation Immunotherapy: Advancing Clinical Applications in Cancer Treatment. J. Clin. Med. 2024, 13, 6537, doi:10.3390/jcm13216537. [CrossRef]
- Ahmad, A.; Mahmood, N.; Raza, M.A.; Mushtaq, Z.; Saeed, F.; Afzaal, M.; Hussain, M.; Amjad, H.W.; Al-Awadi, H.M. Gut Microbiota and Their Derivatives in the Progression of Colorectal Cancer: Mechanisms of Action, Genome and Epigenome Contributions. Heliyon 2024, 10, e29495, doi:10.1016/j.heliyon.2024.e29495. [CrossRef]
- Rahman, M.M.; Islam, M.R.; Shohag, S.; Ahasan, M.T.; Sarkar, N.; Khan, H.; Hasan, A.M.; Cavalu, S.; Rauf, A. Microbiome in Cancer: Role in Carcinogenesis and Impact in Therapeutic Strategies. Biomed. Pharmacother. Biomedecine Pharmacother. 2022, 149, 112898, doi:10.1016/j.biopha.2022.112898. [CrossRef]
- Hou, K.; Wu, Z.-X.; Chen, X.-Y.; Wang, J.-Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in Health and Diseases. Signal Transduct. Target. Ther. 2022, 7, 135, doi:10.1038/s41392-022-00974-4. [CrossRef]
- Zhang, M.; Liu, J.; Xia, Q. Role of Gut Microbiome in Cancer Immunotherapy: From Predictive Biomarker to Therapeutic Target. Exp. Hematol. Oncol. 2023, 12, 84, doi:10.1186/s40164-023-00442-x. [CrossRef]
- Clavijo-Salomon, M.A.; Trinchieri, G. Unlocking the Power of the Microbiome for Successful Cancer Immunotherapy. J. Immunother. Cancer 2025, 13, doi:10.1136/jitc-2024-011281. [CrossRef]
- Nejman, D.; Livyatan, I.; Fuks, G.; Gavert, N.; Zwang, Y.; Geller, L.T.; Rotter-Maskowitz, A.; Weiser, R.; Mallel, G.; Gigi, E.; et al. The Human Tumor Microbiome Is Composed of Tumor Type–Specific Intracellular Bacteria. Science 2020, doi:10.1126/science.aay9189. [CrossRef]
- Xue, C.; Chu, Q.; Zheng, Q.; Yuan, X.; Su, Y.; Bao, Z.; Lu, J.; Li, L. Current Understanding of the Intratumoral Microbiome in Various Tumors. Cell Rep. Med. 2023, 4, 100884, doi:10.1016/j.xcrm.2022.100884. [CrossRef]
- Eisenhofer, R.; Minich, J.J.; Marotz, C.; Cooper, A.; Knight, R.; Weyrich, L.S. Contamination in Low Microbial Biomass Microbiome Studies: Issues and Recommendations. Trends Microbiol. 2019, 27, 105–117, doi:10.1016/j.tim.2018.11.003. [CrossRef]
- Gihawi, A.; Ge, Y.; Lu, J.; Puiu, D.; Xu, A.; Cooper, C.S.; Brewer, D.S.; Pertea, M.; Salzberg, S.L. Major Data Analysis Errors Invalidate Cancer Microbiome Findings. mBio 2023, 14, e01607-23, doi:10.1128/mbio.01607-23. [CrossRef]
- Triner, D.; Devenport, S.N.; Ramakrishnan, S.K.; Ma, X.; Frieler, R.A.; Greenson, J.K.; Inohara, N.; Nunez, G.; Colacino, J.A.; Mortensen, R.M.; et al. Neutrophils Restrict Tumor-Associated Microbiota to Reduce Growth and Invasion of Colon Tumors in Mice. Gastroenterology 2019, 156, 1467–1482, doi:10.1053/j.gastro.2018.12.003. [CrossRef]
- Singh, R.P.; Kumari, N.; Gupta, S.; Jaiswal, R.; Mehrotra, D.; Singh, S.; Mukherjee, S.; Kumar, R. Intratumoral Microbiota Changes with Tumor Stage and Influences the Immune Signature of Oral Squamous Cell Carcinoma. Microbiol. Spectr. 2023, doi:10.1128/spectrum.04596-22. [CrossRef]
- Reynoso-García, J.; Miranda-Santiago, A.E.; Meléndez-Vázquez, N.M.; Acosta-Pagán, K.; Sánchez-Rosado, M.; Díaz-Rivera, J.; Rosado-Quiñones, A.M.; Acevedo-Márquez, L.; Cruz-Roldán, L.; Tosado-Rodríguez, E.L.; et al. A Complete Guide to Human Microbiomes: Body Niches, Transmission, Development, Dysbiosis, and Restoration. Front. Syst. Biol. 2022, 2, doi:10.3389/fsysb.2022.951403. [CrossRef]
- Kitamoto, S.; Nagao-Kitamoto, H.; Hein, R.; Schmidt, T.M.; Kamada, N. The Bacterial Connection between the Oral Cavity and the Gut Diseases. J. Dent. Res. 2020, 99, 1021–1029, doi:10.1177/0022034520924633. [CrossRef]
- Minalyan, A.; Gabrielyan, L.; Scott, D.; Jacobs, J.; Pisegna, J.R. The Gastric and Intestinal Microbiome: Role of Proton Pump Inhibitors. Curr. Gastroenterol. Rep. 2017, 19, 42, doi:10.1007/s11894-017-0577-6. [CrossRef]
- Li, X.; Zhang, S.; Sheng, H.; Zhen, Y.; Wu, B.; Li, Z.; Chen, D.; Zhou, H. Oral Fusobacterium Nucleatum Resists the Acidic pH of the Stomach Due to Membrane Erucic Acid Synthesized via Enoyl-CoA Hydratase-Related Protein FnFabM. J. Oral Microbiol. 2025, 17, 2453964, doi:10.1080/20002297.2025.2453964. [CrossRef]
- Woelfel, S.; Silva, M.S.; Stecher, B. Intestinal Colonization Resistance in the Context of Environmental, Host, and Microbial Determinants. Cell Host Microbe 2024, 32, 820–836, doi:10.1016/j.chom.2024.05.002. [CrossRef]
- Rashidi, A.; Ebadi, M.; Weisdorf, D.J.; Costalonga, M.; Staley, C. No Evidence for Colonization of Oral Bacteria in the Distal Gut in Healthy Adults. Proc. Natl. Acad. Sci. 2021, 118, e2114152118, doi:10.1073/pnas.2114152118. [CrossRef]
- Rashidi, A.; Koyama, M.; Dey, N.; McLean, J.S.; Hill, G.R. Colonization Resistance Is Dispensable for Segregation of Oral and Gut Microbiota. BMC Med. Genomics 2023, 16, 31, doi:10.1186/s12920-023-01449-3. [CrossRef]
- Kunath, B.J.; De Rudder, C.; Laczny, C.C.; Letellier, E.; Wilmes, P. The Oral–Gut Microbiome Axis in Health and Disease. Nat. Rev. Microbiol. 2024, 22, 791–805, doi:10.1038/s41579-024-01075-5. [CrossRef]
- Tortora, S.C.; Agurto, M.G.; Martello, L.A. The Oral-Gut-Circulatory Axis: From Homeostasis to Colon Cancer. Front. Cell. Infect. Microbiol. 2023, 13, doi:10.3389/fcimb.2023.1289452. [CrossRef]
- De Pessemier, B.; Grine, L.; Debaere, M.; Maes, A.; Paetzold, B.; Callewaert, C. Gut–Skin Axis: Current Knowledge of the Interrelationship between Microbial Dysbiosis and Skin Conditions. Microorganisms 2021, 9, 353, doi:10.3390/microorganisms9020353. [CrossRef]
- Elkafas, H.; Walls, M.; Al-Hendy, A.; Ismail, N. Gut and Genital Tract Microbiomes: Dysbiosis and Link to Gynecological Disorders. Front. Cell. Infect. Microbiol. 2022, 12, 1059825, doi:10.3389/fcimb.2022.1059825. [CrossRef]
- Mahmud, Md.R.; Akter, S.; Tamanna, S.K.; Mazumder, L.; Esti, I.Z.; Banerjee, S.; Akter, S.; Hasan, Md.R.; Acharjee, M.; Hossain, Md.S.; et al. Impact of Gut Microbiome on Skin Health: Gut-Skin Axis Observed through the Lenses of Therapeutics and Skin Diseases. Gut Microbes 14, 2096995, doi:10.1080/19490976.2022.2096995. [CrossRef]
- Somodi, C.; Dora, D.; Horváth, M.; Szegvari, G.; Lohinai, Z. Gut Microbiome Changes and Cancer Immunotherapy Outcomes Associated with Dietary Interventions: A Systematic Review of Preclinical and Clinical Evidence. J. Transl. Med. 2025, 23, 756, doi:10.1186/s12967-025-06586-0. [CrossRef]
- Dokoshi, T.; Chen, Y.; Cavagnero, K.J.; Rahman, G.; Hakim, D.; Brinton, S.; Schwarz, H.; Brown, E.A.; O’Neill, A.; Nakamura, Y.; et al. Dermal Injury Drives a Skin to Gut Axis That Disrupts the Intestinal Microbiome and Intestinal Immune Homeostasis in Mice. Nat. Commun. 2024, 15, 3009, doi:10.1038/s41467-024-47072-3. [CrossRef]
- Dang, A.T.; Marsland, B.J. Microbes, Metabolites, and the Gut–Lung Axis. Mucosal Immunol. 2019, 12, 843–850, doi:10.1038/s41385-019-0160-6. [CrossRef]
- Ivleva, E.A.; Grivennikov, S.I. Microbiota-Driven Mechanisms at Different Stages of Cancer Development. Neoplasia N. Y. N 2022, 32, 100829, doi:10.1016/j.neo.2022.100829. [CrossRef]
- Dapito, D.H.; Mencin, A.; Gwak, G.-Y.; Pradere, J.-P.; Jang, M.-K.; Mederacke, I.; Caviglia, J.M.; Khiabanian, H.; Adeyemi, A.; Bataller, R.; et al. Promotion of Hepatocellular Carcinoma by the Intestinal Microbiota and TLR4. Cancer Cell 2012, 21, 504–516, doi:10.1016/j.ccr.2012.02.007. [CrossRef]
- Bertocchi, A.; Carloni, S.; Ravenda, P.S.; Bertalot, G.; Spadoni, I.; Lo Cascio, A.; Gandini, S.; Lizier, M.; Braga, D.; Asnicar, F.; et al. Gut Vascular Barrier Impairment Leads to Intestinal Bacteria Dissemination and Colorectal Cancer Metastasis to Liver. Cancer Cell 2021, 39, 708-724.e11, doi:10.1016/j.ccell.2021.03.004. [CrossRef]
- Bullman, S.; Pedamallu, C.S.; Sicinska, E.; Clancy, T.E.; Zhang, X.; Cai, D.; Neuberg, D.; Huang, K.; Guevara, F.; Nelson, T.; et al. Analysis of Fusobacterium Persistence and Antibiotic Response in Colorectal Cancer. Science 2017, 358, 1443–1448, doi:10.1126/science.aal5240. [CrossRef]
- Senthakumaran, T.; Moen, A.E.F.; Tannæs, T.M.; Endres, A.; Brackmann, S.A.; Rounge, T.B.; Bemanian, V.; Tunsjø, H.S. Microbial Dynamics with CRC Progression: A Study of the Mucosal Microbiota at Multiple Sites in Cancers, Adenomatous Polyps, and Healthy Controls. Eur. J. Clin. Microbiol. Infect. Dis. 2023, 42, 305–322, doi:10.1007/s10096-023-04551-7. [CrossRef]
- Menéndez, G.G.; Sichel, L.; López, M. del C.; Hernández, Y.; Arteaga, E.; Rodríguez, M.; Fleites, V.; Fernández, L.T.; Cano, R.D.J. From Colon Wall to Tumor Niche: Unraveling the Microbiome’s Role in Colorectal Cancer Progression. PLOS ONE 2024, 19, e0311233, doi:10.1371/journal.pone.0311233. [CrossRef]
- Zhu, Y.; Liu, W.; Wang, M.; Wang, X.; Wang, S. Causal Roles of Skin Microbiota in Skin Cancers Suggested by Genetic Study. Front. Microbiol. 2024, 15, doi:10.3389/fmicb.2024.1426807. [CrossRef]
- Tsay, J.-C.J.; Wu, B.G.; Sulaiman, I.; Gershner, K.; Schluger, R.; Li, Y.; Yie, T.-A.; Meyn, P.; Olsen, E.; Perez, L.; et al. Lower Airway Dysbiosis Affects Lung Cancer Progression. Cancer Discov. 2021, 11, 293–307, doi:10.1158/2159-8290.CD-20-0263. [CrossRef]
- Pushalkar, S.; Hundeyin, M.; Daley, D.; Zambirinis, C.P.; Kurz, E.; Mishra, A.; Mohan, N.; Aykut, B.; Usyk, M.; Torres, L.E.; et al. The Pancreatic Cancer Microbiome Promotes Oncogenesis by Induction of Innate and Adaptive Immune Suppression. Cancer Discov. 2018, 8, 403–416, doi:10.1158/2159-8290.CD-17-1134. [CrossRef]
- Meng, Y.-F.; Fan, Z.-Y.; Zhou, B.; Zhan, H.-X. Role of the Intratumoral Microbiome in Tumor Progression and Therapeutics Implications. Biochim. Biophys. Acta Rev. Cancer 2023, 1878, 189014, doi:10.1016/j.bbcan.2023.189014. [CrossRef]
- Xie, Z.; Wu, Z.; Liu, Y.; Gu, Y.; Niu, J.; Lv, K. Intratumoral Microbiota: Implications for Cancer Progression and Treatment. Front. Microbiol. 2025, 16, 1551515, doi:10.3389/fmicb.2025.1551515. [CrossRef]
- Narunsky-Haziza, L.; Sepich-Poore, G.D.; Livyatan, I.; Asraf, O.; Martino, C.; Nejman, D.; Gavert, N.; Stajich, J.E.; Amit, G.; González, A.; et al. Pan-Cancer Analyses Reveal Cancer-Type-Specific Fungal Ecologies and Bacteriome Interactions. Cell 2022, 185, 3789-3806.e17, doi:10.1016/j.cell.2022.09.005. [CrossRef]
- Zhou, Z.; Lv, Y.; Zuo, A.; Zhu, X.; Xu, Y.; Zuo, L.; Xu, H.; Liu, S.; Zhang, Y.; Weng, S.; et al. Interactions between Microbiota and Innate Immunity in Tumor Microenvironment: Novel Insights into Cancer Progression and Immunotherapy. hLife 2025, 3, 462–493, doi:10.1016/j.hlife.2025.05.008. [CrossRef]
- Chen, Y.; Wu, F.-H.; Wu, P.-Q.; Xing, H.-Y.; Ma, T. The Role of The Tumor Microbiome in Tumor Development and Its Treatment. Front. Immunol. 2022, 13, 935846, doi:10.3389/fimmu.2022.935846. [CrossRef]
- Dohlman, A.B.; Mendoza, D.A.; Ding, S.; Gao, M.; Dressman, H.; Iliev, I.D.; Lipkin, S.M.; Shen, X. The Cancer Microbiome Atlas: A Pan-Cancer Comparative Analysis to Distinguish Tissue-Resident Microbiota from Contaminants. Cell Host Microbe 2021, 29, 281-298.e5, doi:10.1016/j.chom.2020.12.001. [CrossRef]
- Li, L.; Chandra, V.; McAllister, F. Tumor-Resident Microbes: The New Kids on the Microenvironment Block. Trends Cancer 2024, 10, 347–355, doi:10.1016/j.trecan.2023.12.002. [CrossRef]
- Wang, Y.; Guo, H.; Gao, X.; Wang, J. The Intratumor Microbiota Signatures Associate With Subtype, Tumor Stage, and Survival Status of Esophageal Carcinoma. Front. Oncol. 2021, 11, doi:10.3389/fonc.2021.754788. [CrossRef]
- Wang, J.; Wang, Y.; Li, Z.; Gao, X.; Huang, D. Global Analysis of Microbiota Signatures in Four Major Types of Gastrointestinal Cancer. Front. Oncol. 2021, 11, 685641, doi:10.3389/fonc.2021.685641. [CrossRef]
- Yu, G.; Gail, M.H.; Consonni, D.; Carugno, M.; Humphrys, M.; Pesatori, A.C.; Caporaso, N.E.; Goedert, J.J.; Ravel, J.; Landi, M.T. Characterizing Human Lung Tissue Microbiota and Its Relationship to Epidemiological and Clinical Features. Genome Biol. 2016, 17, 163, doi:10.1186/s13059-016-1021-1. [CrossRef]
- Xie, Y.; Xie, F.; Zhou, X.; Zhang, L.; Yang, B.; Huang, J.; Wang, F.; Yan, H.; Zeng, L.; Zhang, L.; et al. Microbiota in Tumors: From Understanding to Application. Adv. Sci. 2022, 9, 2200470, doi:10.1002/advs.202200470. [CrossRef]
- Rajasekaran, K.; Carey, R.M.; Lin, X.; Seckar, T.D.; Wei, Z.; Chorath, K.; Newman, J.G.; O’Malley, B.W.; Weinstein, G.S.; Feldman, M.D.; et al. The Microbiome of HPV-Positive Tonsil Squamous Cell Carcinoma and Neck Metastasis. Oral Oncol. 2021, 117, 105305, doi:10.1016/j.oraloncology.2021.105305. [CrossRef]
- Chiba, A.; Bawaneh, A.; Velazquez, C.; Clear, K.Y.J.; Wilson, A.S.; Howard-McNatt, M.; Levine, E.A.; Levi-Polyachenko, N.; Yates-Alston, S.A.; Diggle, S.P.; et al. Neoadjuvant Chemotherapy Shifts Breast Tumor Microbiota Populations to Regulate Drug Responsiveness and the Development of Metastasis. Mol. Cancer Res. MCR 2020, 18, 130–139, doi:10.1158/1541-7786.MCR-19-0451. [CrossRef]
- Zhang, W.; Xiang, Y.; Ren, H.; Liu, Y.; Wang, Q.; Ran, M.; Zhou, W.; Tian, L.; Zheng, X.; Qiao, C.; et al. The Tumor Microbiome in Cancer Progression: Mechanisms and Therapeutic Potential. Mol. Cancer 2025, 24, 195, doi:10.1186/s12943-025-02403-w. [CrossRef]
- Yang, L.; Li, A.; Wang, Y.; Zhang, Y. Intratumoral Microbiota: Roles in Cancer Initiation, Development and Therapeutic Efficacy. Signal Transduct. Target. Ther. 2023, 8, 35, doi:10.1038/s41392-022-01304-4. [CrossRef]
- Goodwin, A.C.; Shields, C.E.D.; Wu, S.; Huso, D.L.; Wu, X.; Murray-Stewart, T.R.; Hacker-Prietz, A.; Rabizadeh, S.; Woster, P.M.; Sears, C.L.; et al. Polyamine Catabolism Contributes to Enterotoxigenic Bacteroides Fragilis-Induced Colon Tumorigenesis. Proc. Natl. Acad. Sci. 2011, 108, 15354–15359, doi:10.1073/pnas.1010203108. [CrossRef]
- Sevcikova, A.; Mladosievicova, B.; Mego, M.; Ciernikova, S. Exploring the Role of the Gut and Intratumoral Microbiomes in Tumor Progression and Metastasis. Int. J. Mol. Sci. 2023, 24, 17199, doi:10.3390/ijms242417199. [CrossRef]
- Ji, Y.; Lv, J.; Sun, D.; Huang, Y. Therapeutic Strategies Targeting Wnt/Β catenin Signaling for Colorectal Cancer (Review). Int. J. Mol. Med. 2022, 49, 1–17, doi:10.3892/ijmm.2021.5056. [CrossRef]
- Yu, R.; Wang, S.; Han, L. Relevance of Harmful Intratumoral Microbiota in Cancer Progression and Its Clinical Application. Biomed. Pharmacother. 2024, 178, 117238, doi:10.1016/j.biopha.2024.117238. [CrossRef]
- Tsay, J.-C.J.; Wu, B.G.; Badri, M.H.; Clemente, J.C.; Shen, N.; Meyn, P.; Li, Y.; Yie, T.-A.; Lhakhang, T.; Olsen, E.; et al. Airway Microbiota Is Associated with Upregulation of the PI3K Pathway in Lung Cancer. Am. J. Respir. Crit. Care Med. 2018, 198, 1188–1198, doi:10.1164/rccm.201710-2118OC. [CrossRef]
- Pandya, G.; Kirtonia, A.; Singh, A.; Goel, A.; Mohan, C.D.; Rangappa, K.S.; Pandey, A.K.; Kapoor, S.; Tandon, S.; Sethi, G.; et al. A Comprehensive Review of the Multifaceted Role of the Microbiota in Human Pancreatic Carcinoma. Semin. Cancer Biol. 2022, 86, 682–692, doi:10.1016/j.semcancer.2021.05.027. [CrossRef]
- Guo, Q.; Jin, Y.; Chen, X.; Ye, X.; Shen, X.; Lin, M.; Zeng, C.; Zhou, T.; Zhang, J. NF-κB in Biology and Targeted Therapy: New Insights and Translational Implications. Signal Transduct. Target. Ther. 2024, 9, 53, doi:10.1038/s41392-024-01757-9. [CrossRef]
- Guo, J.; Meng, F.; Hu, R.; Chen, L.; Chang, J.; Zhao, K.; Ren, H.; Liu, Z.; Hu, P.; Wang, G.; et al. Inhibition of the NF-κB/HIF-1α Signaling Pathway in Colorectal Cancer by Tyrosol: A Gut Microbiota-Derived Metabolite. J. Immunother. Cancer 2024, 12, e008831, doi:10.1136/jitc-2024-008831. [CrossRef]
- Zhang, S.; Huang, J.; Jiang, Z.; Tong, H.; Ma, X.; Liu, Y. Tumor Microbiome: Roles in Tumor Initiation, Progression, and Therapy. Mol. Biomed. 2025, 6, 9, doi:10.1186/s43556-025-00248-9. [CrossRef]
- Fu, A.; Yao, B.; Dong, T.; Chen, Y.; Yao, J.; Liu, Y.; Li, H.; Bai, H.; Liu, X.; Zhang, Y.; et al. Tumor-Resident Intracellular Microbiota Promotes Metastatic Colonization in Breast Cancer. Cell 2022, 185, 1356-1372.e26, doi:10.1016/j.cell.2022.02.027. [CrossRef]
- Naghavian, R.; Faigle, W.; Oldrati, P.; Wang, J.; Toussaint, N.C.; Qiu, Y.; Medici, G.; Wacker, M.; Freudenmann, L.K.; Bonté, P.-E.; et al. Microbial Peptides Activate Tumour-Infiltrating Lymphocytes in Glioblastoma. Nature 2023, 617, 807–817, doi:10.1038/s41586-023-06081-w. [CrossRef]
- Zhang, H.; Fu, L.; Leiliang, X.; Qu, C.; Wu, W.; Wen, R.; Huang, N.; He, Q.; Cheng, Q.; Liu, G.; et al. Beyond the Gut: The Intratumoral Microbiome’s Influence on Tumorigenesis and Treatment Response. Cancer Commun. 2024, 44, 1130–1167, doi:10.1002/cac2.12597. [CrossRef]
- Lin, L.; Zhang, D. Unveiling the Microbial Influence: Bacteria’s Dual Role in Tumor Metastasis. Front. Oncol. 2025, 15, 1524887, doi:10.3389/fonc.2025.1524887. [CrossRef]
- Fan, H.; Wang, Y.; Han, M.; Wang, L.; Li, X.; Kuang, X.; Du, J.; Peng, F. Multi-Omics-Based Investigation of Bifidobacterium’s Inhibitory Effect on Glioma: Regulation of Tumor and Gut Microbiota, and MEK/ERK Cascade. Front. Microbiol. 2024, 15, doi:10.3389/fmicb.2024.1344284. [CrossRef]
- Mogensen, T.H. Pathogen Recognition and Inflammatory Signaling in Innate Immune Defenses. Clin. Microbiol. Rev. 2009, 22, 240–273, doi:10.1128/CMR.00046-08. [CrossRef]
- Zhang, J.; You, Z.; Li, X.; Hu, J.; Li, J.; Jing, Z. Harnessing Intratumoral Microbiota: New Horizons in Immune Microenvironment and Immunotherapy. J. Transl. Med. 2025, 23, 897, doi:10.1186/s12967-025-06916-2. [CrossRef]
- Qiao, H.; Tan, X.-R.; Li, H.; Li, J.-Y.; Chen, X.-Z.; Li, Y.-Q.; Li, W.-F.; Tang, L.-L.; Zhou, G.-Q.; Zhang, Y.; et al. Association of Intratumoral Microbiota With Prognosis in Patients With Nasopharyngeal Carcinoma From 2 Hospitals in China. JAMA Oncol. 2022, 8, 1301–1309, doi:10.1001/jamaoncol.2022.2810. [CrossRef]
- Xu, S.; Wu, X.; Zhang, X.; Chen, C.; Chen, H.; She, F. CagA Orchestrates eEF1A1 and PKCδ to Induce Interleukin-6 Expression in Helicobacter Pylori-Infected Gastric Epithelial Cells. Gut Pathog. 2020, 12, 31, doi:10.1186/s13099-020-00368-3. [CrossRef]
- Gur, C.; Ibrahim, Y.; Isaacson, B.; Yamin, R.; Abed, J.; Gamliel, M.; Enk, J.; Bar-On, Y.; Stanietsky-Kaynan, N.; Coppenhagen-Glazer, S.; et al. Binding of the Fap2 Protein of Fusobacterium Nucleatum to Human Inhibitory Receptor TIGIT Protects Tumors from Immune Cell Attack. Immunity 2015, 42, 344, doi:10.1016/j.immuni.2015.01.010. [CrossRef]
- Sun, J.; Tang, Q.; Yu, S.; Xie, M.; Zheng, W.; Chen, G.; Yin, Y.; Huang, X.; Wo, K.; Lei, H.; et al. F. Nucleatum Facilitates Oral Squamous Cell Carcinoma Progression via GLUT1-Driven Lactate Production. eBioMedicine 2023, 88, 104444, doi:10.1016/j.ebiom.2023.104444. [CrossRef]
- Schöpf, F.; Marongiu, G.L.; Milaj, K.; Sprink, T.; Kikhney, J.; Moter, A.; Roderer, D. Structural Basis of Fusobacterium Nucleatum Adhesin Fap2 Interaction with Receptors on Cancer and Immune Cells. Nat. Commun. 2025, 16, 8104, doi:10.1038/s41467-025-63451-w. [CrossRef]
- Wang, M.; Yu, F.; Li, P. Intratumor Microbiota in Cancer Pathogenesis and Immunity: From Mechanisms of Action to Therapeutic Opportunities. Front. Immunol. 2023, 14, 1269054, doi:10.3389/fimmu.2023.1269054. [CrossRef]
- Nagler, A.; Kalaora, S.; Rosenberg, D.G.; Alon, M.; Barnea, E.; Levy, R.; Vervier, K.; Trabish, S.; Dadosh, T.; Zaidman, S.; et al. 672 Identification of Microbial-Derived HLA-Bound Peptides in Melanoma. J. Immunother. Cancer 2020, 8, doi:10.1136/jitc-2020-SITC2020.0672. [CrossRef]
- Wang, X.; Jia, Y.; Wen, L.; Mu, W.; Wu, X.; Liu, T.; Liu, X.; Fang, J.; Luan, Y.; Chen, P.; et al. Porphyromonas Gingivalis Promotes Colorectal Carcinoma by Activating the Hematopoietic NLRP3 Inflammasome. Cancer Res. 2021, 81, 2745–2759, doi:10.1158/0008-5472.CAN-20-3827. [CrossRef]
- Liu, S.; Zhou, X.; Peng, X.; Li, M.; Ren, B.; Cheng, G.; Cheng, L. Porphyromonas Gingivalis Promotes Immunoevasion of Oral Cancer by Protecting Cancer from Macrophage Attack. J. Immunol. 2020, 205, 282–289, doi:10.4049/jimmunol.1901138. [CrossRef]
- Yijia, Z.; Li, X.; Ma, L.; Wang, S.; Du, H.; Wu, Y.; Yu, J.; Xiang, Y.; Xiong, D.; Shan, H.; et al. Identification of Intratumoral Microbiome-Driven Immune Modulation and Therapeutic Implications in Diffuse Large B-Cell Lymphoma. Cancer Immunol. Immunother. 2025, 74, 131, doi:10.1007/s00262-025-03972-x. [CrossRef]
- Xu, Z.; Lv, Z.; Chen, F.; Zhang, Y.; Xu, Z.; Huo, J.; Liu, W.; Yu, S.; Tuersun, A.; Zhao, J.; et al. Dysbiosis of Human Tumor Microbiome and Aberrant Residence of Actinomyces in Tumor-Associated Fibroblasts in Young-Onset Colorectal Cancer. Front. Immunol. 2022, 13, 1008975, doi:10.3389/fimmu.2022.1008975. [CrossRef]
- Wang, Y.; Jiang, Z.; Zhang, K.; Tang, H.; Wang, G.; Gao, J.; He, G.; Liang, B.; Li, L.; Yang, C.; et al. Whole-Tumor Clearing and Imaging of Intratumor Microbiota in Three Dimensions with miCDaL Strategy. Adv. Sci. 2024, 11, 2400694, doi:10.1002/advs.202400694. [CrossRef]
- Alam, A.; Levanduski, E.; Denz, P.; Villavicencio, H.S.; Bhatta, M.; Alhorebi, L.; Zhang, Y.; Gomez, E.C.; Morreale, B.; Senchanthisai, S.; et al. Fungal Mycobiome Drives IL-33 Secretion and Type 2 Immunity in Pancreatic Cancer. Cancer Cell 2022, 40, 153-167.e11, doi:10.1016/j.ccell.2022.01.003. [CrossRef]
- Chen, Y.; Yang, L.; Huang, Y.; Zhu, T.; Zhang, L.; Cheng, M.; Wu, C.; Li, P.; Liang, M.; Zhang, X.; et al. Intratumoral Microbiota Predicts the Response to Neoadjuvant Chemoimmunotherapy in Triple-Negative Breast Cancer. J. Immunother. Cancer 2025, 13, e010365, doi:10.1136/jitc-2024-010365. [CrossRef]
- Davidsson, S.; Carlsson, J.; Greenberg, L.; Wijkander, J.; Söderquist, B.; Erlandsson, A. Cutibacterium Acnes Induces the Expression of Immunosuppressive Genes in Macrophages and Is Associated with an Increase of Regulatory T-Cells in Prostate Cancer. Microbiol. Spectr. 9, e01497-21, doi:10.1128/spectrum.01497-21. [CrossRef]
- Liu, Z.; Zhang, X.; Zhang, H.; Zhang, H.; Yi, Z.; Zhang, Q.; Liu, Q.; Liu, X. Multi-Omics Analysis Reveals Intratumor Microbes as Immunomodulators in Colorectal Cancer. Microbiol. Spectr. 2023, 11, e05038-22, doi:10.1128/spectrum.05038-22. [CrossRef]
- Wong-Rolle, A.; Dong, Q.; Zhu, Y.; Divakar, P.; Hor, J.L.; Kedei, N.; Wong, M.; Tillo, D.; Conner, E.A.; Rajan, A.; et al. Spatial Meta-Transcriptomics Reveal Associations of Intratumor Bacteria Burden with Lung Cancer Cells Showing a Distinct Oncogenic Signature. J. Immunother. Cancer 2022, 10, e004698, doi:10.1136/jitc-2022-004698. [CrossRef]
- Lim, S.-K.; Lin, W.-C.; Huang, S.-W.; Pan, Y.-C.; Hu, C.-W.; Mou, C.-Y.; Hu, C.-M.J.; Mou, K.Y. Bacteria Colonization in Tumor Microenvironment Creates a Favorable Niche for Immunogenic Chemotherapy. EMBO Mol. Med. 2024, 16, 416–428, doi:10.1038/s44321-023-00022-w. [CrossRef]
- Guo, F.; Das, J.K.; Kobayashi, K.S.; Qin, Q.-M.; A Ficht, T.; Alaniz, R.C.; Song, J.; Figueiredo, P.D. Live Attenuated Bacterium Limits Cancer Resistance to CAR-T Therapy by Remodeling the Tumor Microenvironment. J. Immunother. Cancer 2022, 10, e003760, doi:10.1136/jitc-2021-003760. [CrossRef]
- Vincent, R.L.; Gurbatri, C.R.; Li, F.; Vardoshvili, A.; Coker, C.; Im, J.; Ballister, E.R.; Rouanne, M.; Savage, T.; de los Santos-Alexis, K.; et al. Probiotic-Guided CAR-T Cells for Solid Tumor Targeting. Science 2023, 382, 211–218, doi:10.1126/science.add7034. [CrossRef]
- Lam, K.C.; Araya, R.E.; Huang, A.; Chen, Q.; Modica, M.D.; Rodrigues, R.R.; Lopès, A.; Johnson, S.B.; Schwarz, B.; Bohrnsen, E.; et al. Microbiota Triggers STING-Type I IFN-Dependent Monocyte Reprogramming of the Tumor Microenvironment. Cell 2021, 184, 5338-5356.e21, doi:10.1016/j.cell.2021.09.019. [CrossRef]
- Zhu, G.; Su, H.; Johnson, C.H.; Khan, S.A.; Kluger, H.; Lu, L. Intratumour Microbiome Associated with the Infiltration of Cytotoxic CD8+ T Cells and Patient Survival in Cutaneous Melanoma. Eur. J. Cancer Oxf. Engl. 1990 2021, 151, 25–34, doi:10.1016/j.ejca.2021.03.053. [CrossRef]
- Riquelme, E.; Zhang, Y.; Zhang, L.; Montiel, M.; Zoltan, M.; Dong, W.; Quesada, P.; Sahin, I.; Chandra, V.; Lucas, A.S.; et al. Tumor Microbiome Diversity and Composition Influence Pancreatic Cancer Outcomes. Cell 2019, 178, 795-806.e12, doi:10.1016/j.cell.2019.07.008. [CrossRef]
- Sfanos, K.S. Intratumoral Bacteria as Mediators of Cancer Immunotherapy Response. Cancer Res. 2023, 83, 2985–2986, doi:10.1158/0008-5472.CAN-23-1857. [CrossRef]
- Zheng, J.; Chen, H. Effects of Intratumoral Microbiota on Tumorigenesis, Anti-Tumor Immunity, and Microbe-Based Cancer Therapy. Front. Oncol. 2024, 14, 1429722, doi:10.3389/fonc.2024.1429722. [CrossRef]
- Zheng, S.; Su, Y.; Cai, F.; Xu, D.; Xu, Y. From Mechanisms to Precision Medicine: The Role of Organoids in Studying the Gut Microbiota-Tumor Microenvironment Axis. Front. Microbiol. 2025, 16, 1669482, doi:10.3389/fmicb.2025.1669482. [CrossRef]
- Sun, Y.; Zhang, X.; Jin, C.; Yue, K.; Sheng, D.; Zhang, T.; Dou, X.; Liu, J.; Jing, H.; Zhang, L.; et al. Prospective, Longitudinal Analysis of the Gut Microbiome in Patients with Locally Advanced Rectal Cancer Predicts Response to Neoadjuvant Concurrent Chemoradiotherapy. J. Transl. Med. 2023, 21, 221, doi:10.1186/s12967-023-04054-1. [CrossRef]
- Harmak, Z.; Kone, A.-S.; Ghouzlani, A.; Ghazi, B.; Badou, A. Beyond Tumor Borders: Intratumoral Microbiome Effects on Tumor Behavior and Therapeutic Responses. Immune Netw. 2024, 24, e40, doi:10.4110/in.2024.24.e40. [CrossRef]
- Wang, N.; Wu, S.; Huang, L.; Hu, Y.; He, X.; He, J.; Hu, B.; Xu, Y.; Rong, Y.; Yuan, C.; et al. Intratumoral Microbiome: Implications for Immune Modulation and Innovative Therapeutic Strategies in Cancer. J. Biomed. Sci. 2025, 32, 23, doi:10.1186/s12929-025-01117-x. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



