
Submitted:
06 November 2025
Posted:
13 November 2025
You are already at the latest version
Abstract
This study investigates the impact of engagement with online health platforms (OHPs), perceived treatment effectiveness, and country of residence on patient attitudes toward atrial fibrillation (AF) treatments, mediated by threat perception and behavioral evaluation within an adapted Health Belief Model (HBM). A cross-sectional survey conducted in June 2024 included 589 members of two professionally curated OHPs: the AFIP Foundation (Netherlands) and StopAfib.org (United States). Data were analyzed using Structural Equation Modeling (SEM) to examine both direct and indirect relationships among engagement behaviors, perceived treatment effectiveness, country of residence, and patient attitudes toward AF treatments (PAAT). Results indicate that higher engagement (i.e., frequency of OHP visits and time spent on the OHP) positively predicts more favorable PAAT, whereas the number of content types consumed showed no significant mediating effect via threat perception or behavioral evaluation. By increasing awareness of AF and reinforcing the perceived effectiveness of treatments, OHPs can serve as effective tools for patient education and support. From a managerial perspective, these findings provide actionable insights for platform operators and healthcare stakeholders on which engagement factors most effectively enhance patient attitudes toward treatment options.
Keywords:
atrial fibrillation
; patient attitudes towards treatments
; health belief model
; healthcare perception
; sem
; patient engagement
; online health platform
1. Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia in Western countries, with increasing prevalence due to aging populations and lifestyle-related risk factors [1]. Despite advances in treatment, AF recurrence and treatment adherence challenges remain. Non-adherence to treatment plans has become a significant challenge in chronic disease care [2], placing patients with AF at increased risk of disease progression and severe complications such as heart failure, stroke, and even death [3]. According to the American Heart Association [4], failing to adhere to treatment leads to the loss of as many as 125,000 American lives each year. It also imposes a considerable economic burden on the healthcare system, with the annual per-person cost attributable to specific diseases ranging from $949 to $44,190, driven by increased medical appointments, emergency department visits, and hospitalizations [5].
Simultaneously, the emergence of online health platforms (OHPs) has significantly altered patient engagement and health information dissemination [6]. These platforms provide a tool for patients to share and consume information about their experiences ranging from diseases to pharmaceuticals, potentially influencing the attitudes and decisions of others regarding their healthcare.
When considering treatments, patients often face the burden of information asymmetry [7]. While the effectiveness of pharmaceuticals must be assessed by healthcare professionals, OHPs increasingly allow patients to access medical information directly, enhancing their understanding of conditions and treatments [8]. However, exposure to inaccurate or incomplete information can undermine medication adherence, strain patient–clinician relationships, and increase healthcare costs [9]. Patients’ judgments are often shaped by perceptions formed through peers or online content [10]. However, adherence failures also stem from the treatment burden imposed by complex medication regimens and side effects that clinicians may underestimate [11,12]. For in-stance, patients using vitamin K antagonists experienced a higher treatment burden than patients taking non-vitamin K oral anticoagulants, due to frequent INR monitoring and dietary restrictions, which can reduce adherence [12]. OHPs therefore can play a vital role not only in improving understanding of therapies but also in enabling patients, through education, to communicate treatment burden and side effects to their clinicians.
Considering these complexities, the role of OHPs in shaping attitudes toward AF treatment represents a double-edged sword. On one hand, such platforms democratize health information and promote patient autonomy, on the other, seeking health information (which may be of low quality) online without collaboration with a health professional may leave individuals concerned and may distort attitudes and strain patient–clinician relationships [8,9]. For platform providers, this duality presents both a responsibility and an opportunity. By integrating verified medical expertise and ensuring the credibility of shared information, they can foster patient trust and enhance adherence. Strengthening collaboration among healthcare professionals, patient advocacy groups, and platform developers is therefore essential to ensure accuracy and relevance, ultimately improving disease understanding and clinical outcomes while reducing the burden of non-adherence [7].
Despite growing interest in digital health, the specific role of OHPs in attitudes towards treatment management remains underexplored. Previous research has produced mixed results. For instance, smartphone-based health interventions alone did not significantly influence smoking abstinence [13], whereas a mobile-based self-management program combined with traditional care was found to improve medication adherence among patients with coronary heart disease [14] and similar effects were found by peers using apps [15,16]. These inconsistent findings, primarily derived from structured intervention studies, raise an important question regarding how OHPs, which are freely accessible to the general public, affect patients’ attitudes toward medication. Engagement in online health communities is highest among individuals with chronic or life-threatening illnesses and minimal cognitive decline [17]. Given that AF is a chronic condition, it provides a valuable context for examining the influence of OHP use on attitudes toward AF treatment options. Considering the increasing prevalence of AF and the aging demographics of Western societies [18], understanding the impact of OHPs on treatment adherence is both timely and of significant clinical relevance.
The Health Belief Model (HBM) provides a theoretical framework for understanding patients’ health behaviors and treatment attitudes by linking beliefs about health conditions to behavioral intentions. Rooted in expectancy-value theory, the model posits that behavior depends on the perceived value of an outcome and the belief that specific actions will achieve it [19,20]. Research shows that stronger perceptions of disease risk and severity increase adherence to treatment, such as medication use among AF patients [21,22]. For this study, the HBM is adapted to the context of AF by consolidating the original four constructs into two overarching components: threat perception (combining perceived susceptibility and severity of AF) and behavioral evaluation (comprising perceived benefits and barriers of treatment). The current study therefore investigates the following research question: What is the influence of OHP engagement (frequency of platform visit, time spent on the platform, and content type consumed), perceived effectiveness and country of residence of the user on patient attitudes towards treatments for AF, through a mediation of threat perception and behavioral evaluation?
The components of threat perception and behavioral evaluation act as mediating variables in this study’s conceptual model, allowing a focused examination of how patients’ beliefs influence attitudes toward AF treatment and adherence behaviors. To address this, the study employs a cross-sectional survey of AF patients who access information from a Dutch online health platform (AFIP Foundation) and the U.S.-based platform (StopAfib.org), with the data analyzed using Structural Equation Modeling (SEM). The SEM methodology enables complex analysis between different constructs specifically when subjective elements are being measured [23]. This approach allowed for the examination of the direct and indirect relationships among the variables, providing a comprehensive understanding of the pathways through which OHPs and perceived effectiveness influences patients' attitudes.
As OHPs increasingly integrate into patient care, this study reveals whether engagement with these platforms can improve attitudes toward treatment options.
2. Materials and Methods
As previously noted, this study applies the HBM to examine the effects of OHP engagement, perceived treatment effectiveness, and country of residence on patients’ attitudes toward AF treatments. Before detailing the study’s methodology, a review of the relevant literature underlying the theoretical framework is presented.
2.1. Literature Review
The literature review driving theoretical framework begins by an explanation of the HBM as the guiding theory for understanding how patients’ beliefs shape their health behaviors and treatment attitudes. The theoretical framework adapts the HBM to focus on perceived treatment effectiveness and its influence on attitudes toward AF treatments. It then explores how engagement with OHPs relates to these perceptions and attitudes. The section concludes with the introduction of the patient attitudes toward AF treatment construct and a visual model summarizing the study’s conceptual framework and hypotheses.
2.1.1. Patient Attitudes toward AF Treatment
Patient attitudes toward AF treatments are central to understanding treatment perceptions and adherence. Throughout this research, PAAT will be used as an abbreviation for patient attitudes toward AF treatments to facilitate clarity and brevity. Attitudes strongly predict behavior [24,25], shaped by personal beliefs, experiences, and perceived treatment impact on quality of life [26]. Moreover, a study by Lip et al. [27] demonstrated that greater knowledge of AF is associated with improved adherence to medication, which shows the importance of patient education. Yet, measuring medication adherence is inherently complex due to the need for clearly defined parameters and frameworks tailored to individual circumstances [28,29]. The construct of behavior is therefore challenging to capture within the context of AF treatment usage. This complexity arises from the multifaceted nature of health behaviors, which reflect an individual’s physical capacities alongside experiences and opinions shaped by social and psychological contexts [30]. Consequently, this study focuses on attitudes rather than directly on adherence or broader health-related behaviors. Given extensive literature supporting the predictive power of attitudes [24,25], PAAT measured in this study can nonetheless provide meaningful inferences about patients’ likely behavioral actions. The HBM further suggests that patients’ perceptions of disease severity and personal susceptibility critically influence their willingness to adhere to treatment [21]. For instance, if patients perceive their risk as low or consider AF to be non-severe, they may be less motivated to follow prescribed medication regimens. Therefore, enhancing patient awareness of the risks associated with poor adherence is essential. Considering the ability of attitudes to influence behavior, examining PAAT in the context of engagement with professionally curated OHPs provides valuable insights into how patient attitudes can be shaped to promote treatment adherence.
2.1.2 Health Belief Model
The HBM is a well-established psychological framework for predicting and explaining health behaviors, providing a solid basis for analyzing patients’ perceptions and attitudes toward treatments and healthcare-related issues. At its core, the HBM is grounded in expectancy-value theory, which posits that behavior is determined by 1) the subjective value placed on a health outcome and 2) the expectation that a given action will achieve that outcome [19,20]. Empirical evidence indicates that patients’ beliefs about the severity of their condition and their susceptibility to complications strongly influence adherence to prescribed medical regimens [21,31]. In the context of atrial fibrillation (AF), these perceptions can shape the urgency with which patients approach treatment and their engagement with interventions such as medication schedules [21,22]. In its original form, the HBM comprises four primary constructs, namely: perceived susceptibility, perceived severity, perceived benefits, and perceived barriers, with self-efficacy and health motivation subsequently added [21,32]. For the purposes of this study, the model has been adapted to the AF context by consolidating perceived susceptibility and perceived severity into a single component, threat perception, reflecting the degree to which an individual perceives both personal vulnerability and the seriousness of potential adverse outcomes. The constructs of perceived benefits and barriers are combined into a second component, behavioral evaluation, capturing the individual’s assessment of the potential effectiveness of actions to reduce the threat relative to the effort or obstacles involved [33]. The health motivation construct is excluded from this study due to its abstract nature and relative difficulty of direct measurement [34]. This streamlined adaptation aligns with prior research demonstrating that the HBM can be successfully modified to accommodate diverse cultural and topical contexts [35]. The two resulting components (i.e., threat perception and behavioral evaluation) serve as mediators in the proposed conceptual model (Figure 1), providing a focused framework to examine how patients’ beliefs shape their attitudes toward AF treatment and adherence behaviors.
2.1.3. Treat Perception: Perceived Susceptibility
Perceived susceptibility, as part of threat perception, refers to an individual’s assessment of their likelihood of developing a disease. People are more likely to engage in preventive or treatment-related behaviors when they believe they are at risk, that recommended actions can reduce this risk, and that the benefits outweigh the barriers [22]. Factors shaping perceived susceptibility include personal or vicarious experience with illness [36], knowledge about the condition [37], and demographic characteristics such as age, gender, and socioeconomic status [38]. Building on these insights, the inclusion of country of residence as a contextual variable may capture cross-national differences in perceived susceptibility, which in turn could lead to variations in PAAT across countries.
2.1.4. Threat perception: perceived severity
Perceived severity, the second component of threat perception, reflects an individual’s assessment of the seriousness of a disease and is influenced by personal experience, observation of others, and health knowledge [36]. Psychological factors, such as anxiety and stress, as well as public exposure to health threats, further shape perceived severity [8,38]. Higher perceived severity, combined with perceived susceptibility, is expected to increase patients’ positive PAAT (H1). OHPs may enhance threat perception by providing educational resources, thereby promoting preventive behaviors, adherence to medical advice, and ultimately reducing health risks associated with AF.
2.1.5. Behavioral evaluation: perceived benefits
Perceived benefits, as part of behavioral evaluation, refer to an individual’s evaluation of the advantages of engaging in health-related behaviors. Personal experience, such as previous successful health actions, strengthens the belief in these benefits [39]. Health knowledge also plays a key role, as understanding how preventive measures can avert serious illness increases perceived benefits [40,41]. Moreover, psychological factors, including optimism and self-efficacy, further enhance the perception of benefits, as do media coverage and public health campaigns that highlight successful health outcomes [42,43].
2.1.6. Behavioral Evaluation: Perceived Barriers
Another component of behavioral evaluation is the perceived barriers, which refers to the obstacles individuals identify when engaging in health-related behaviors [39]. These barriers often arise from social influences, such as discouragement from peers, and environmental constraints, including limited healthcare access or financial challenges [44,45]. Additionally, factors like discomfort or emotional strain can heighten perceived barriers [46]. Since perceived benefits and barriers operate in opposition, behavioral change tends to occur when benefits outweigh perceived obstacles. Consequently, this study hypothesizes (in H2) that a higher perceived behavioral evaluation will result in a more positive PAAT.
2.1.7. Engagement with OHPs
Engagement with OHPs plays a vital role in shaping patients’ attitudes toward treatments and healthcare. As digital health adoption rises [47], understanding engagement behaviors is important. However, although patient engagement has become a widely used term, the exact definition varies in the literature. According to Higgins et al. [48], patient engagement can be regarded as the desire and capability to actively participate in care in way uniquely appropriate to the individual, in cooperation with an institution, to maximize positive outcomes. Therefore, the authors state that patient engagement refers to an individual’s willingness and ability to actively participate in their care. On the other hand, user engagement on OHPs extends to information seeking, video viewing, and social interaction [49]. Research highlights that trust, platform design, and especially content quality and relevance strongly influence engagement [50]. Moreover, platforms that foster social support and provide credible, personalized information achieve higher user retention and positive attitudes [49]. Accordingly, hypotheses 3-5 state that frequent, prolonged platform use, as well as increased content consumption, positively influence PAAT.
2.1.8. Perceived effectiveness
The construct of perceived effectiveness and benefits of is being regarded as a critical determinant of health behavior [32]. It’s defined as an individual’s belief in the efficacy of an action to mitigate or prevent a health threat [51]. Rajpura and Nayak [52] reported that positive beliefs regarding the effectiveness of medication, predicted adherence to medication among elders with hypertension. At the same time, patient satisfaction with treatment has been associated with better adherence and compliance [53]. Furthermore, Horne and Weinman (1999) found that patients who believed that their prescribed medication was necessary for maintaining health also reported higher compliance. A finding that can explicitly relate to threat perception of the HBM, delineating a connection between one’s perceived effectiveness of medication and the underlying experience of threat for their own’s medical condition. The conceptual model of this study (Figure 1) depicts the expected impact of the country of residence, engagement on the OHP, and perceived effectiveness on PAAT through mediation by the HBM.

Table 1.
Overview of the six hypotheses of this study.
| H1: |
|
| H2: |
|
| H3: |
|
| H4: |
|
| H5: |
|
| H6: |
|
2.2. Method
To examine the impact of country of residence, engagement with OHPs, and perceived effectiveness on PAAT, mediated by the constructs of the HBM, a cross-sectional survey was conducted in June 2024 among members of the Dutch AFIP Foundation and the American AF organization StopAfib.org. These two organizations were selected because they represent leading sources of information and support for individuals with AF in their respective countries, namely the Netherlands and the United States. Both platforms provide professionally curated and evidence-based content which ensures reliable and medically accurate information. Therefore, these organizations offer an appropriate context for assessing the influence of OHP engagement on patient attitudes, as well as for comparing potential differences between the two countries. All members of the two platforms were approached by emails (sent by the organizations), asking for participation in a short questionnaire. Members who were willing to participate were redirected to the University of Amsterdam affiliated Qualtrics environment to complete the survey.
2.2.1. Sample size
A solid sample size is essential for a robust data analysis and in turn reflects a better external validity [54]. To estimate the preferred size of total respondents, the Cochran formula [55] has been used.
For this study, a 95% confidence level was desired, which corresponds to a Z-score of 1.96. The estimated proportion of the population () was set at 0.5 to ensure maximum variability, and the margin of error () was set at 0.05. These values were plugged into the above Cochran's formula to give the required sample size of 385 respondents.
2.2.2. Data collection
The final questionnaire consisted of two sections comprising a total of 31 items, with the first part of the survey consisting of dichotomous or multiple-choice questions, answering questions about country of origin, current treatment usage and diagnosis date. Then the second part was structured around statements regarding the perception and usage of OHPs. The statements were derived from existing literature concerning the HBM and its application on OHPs [21,31,36]. For this part of the questionnaire, a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree) was used to test perceptions and attitudes of the participants. The 7-point scale provides more reliability by improving internal consistenct for measuring attitudes and perceptions than the 5-point scale [56], and therefore served as the preferred option for this study. See Supplementary section 3 for the complete overview of the scales used in this study.
Statements regarding Threat Perception were stated as (but not limited to): (1) I believe AF could significantly affect my health if not managed properly. (2) I am concerned about the possible impact of AF on my daily life. These statements were mostly focused on how users of OHPs perceive the threat of AF and how it affects there sense of own health.
Statements regarding Behavioral Evaluation were stated as (but not limited to): (1) I believe that it is beneficial to adhere to prescribed treatments for AF. (2) I am having a hard time following my treatment plan due to cost, side effects or other reasons. Most statements in the survey were focused around the concept of adherence to treatments and how users evaluate their own adherence. The statements also touched upon how users view the possible obstacles or limitations of AF treatments and how it affects their behavior regarding for example their medication regimen (3): I am having a hard time following my treatment plan due to cost, side effects or other reasons.
Simultaneously, PAAT was measured using statements as (but not limited to): (1) I often read or participate in discussions about the benefits of treatment on the platforms or (2) My platforms have helped me gain more confidence in managing my AF.
The first version was developed Dutch in coordination with representatives from the AFIP, but after completion it was translated to English in coherence with the representative from StopAfib.org. The transcripts of both surveys are included in the appendix section of this research (Supplementary section 3 and 4).
2.2.3. Analysis
This study aimed to answer the research question by using SEM. This approach allowed for the examination of the direct and indirect relationships among the variables, providing a comprehensive understanding of the pathways through which OHPs and perceived effectiveness influences patients' attitudes. Raw data was loaded into SPSS version 29 and manually checked for overall quality and consistency. The textual data from the first section was recoded to numerical values to be usable for data transformation and analysis purposes. Question 1 (country of residence) was recoded into dummy variables, stating The Netherlands as reference group (0) and the US as group (1). Items that demonstrated a different country of origin were excluded from the final dataset.
Additionally, the variable content on OHP was composed of six questions. These questions were aggregated to form a single variable, representing the total number of different activities a person engages in on the platform. Also, time spent on OHP was recoded to be in line with the variable OHP visits per month, so that they both measure the same construct. Lastly the variable PAAT was created based on 12 scale items, retained from statements in the second section of the survey to measure the construct proposed in theoretical framework.
In SPSS, descriptives and frequency tables were loaded to check for outliers and errors. Then, a one-way ANOVA was used to test the mean difference between quantitative groups on significance level as well as Pearson’s correlation to test correlation between variables. Consequently, the multiple mediation has been performed on the collected data by using Hayes Process model 4 and 7. The confidence interval was set on 95% and used 5000 bootstrap samples to compute bias-corrected and accelerated confidence intervals. This mediation analysis was used to perform a pre-test and to be visually scanned for possible errors.
The final data set was then loaded into the R statistical software environment for a thorough SEM analysis using the lavaan package. Output was summarized and transformed into R workbench tables and used for inferential analysis. Results and syntax from both R and SPSS are included in appendix 2 & 3.
2.2.4. Variables
For this research, PAAT serves as the outcome variable (Y). The predictor variables (X) are identified as Engagement on OHP (X1,2,3) consisting of content types consumed on OHP (X1), frequency of OHP visits (X2) and time spent on OHP (X3). And the other predictor variables perceived effectiveness (X4) and country of residence (X5). The variables mediating the relationships are threat perception (M1) and behavioral evaluation (M2).
For the predictor variable (X1), the content was quantified by the total number of content types used. This variable ranges from 1, indicating the use of one type of content on the OHP to 6, indicating the use of six different types of content on the platform. The options available to respondents included, but were not limited to, activities such as reading articles and participating in forums or discussion groups.
Then after identification, the formation of a multistep mathematical approach was applied to deduct possible assumptions between variables. The core of the model is structured around the two mediator variables resulting in the following equations.
Where represents the path coefficients from the predictors (Xi) to the mediator (Mi) variables and are the error terms. These equations can subsequently be substituted into the effect of mediator on dependent variable formula.
And thereafter together with the direct effect equation,
substituting the two models into one combined model, used for actual data analysis purposes.
In these equations, represents paths from mediator (Mi) variables to the dependent variable (Y), the represents the direct pathways from the predictor (Xi) variables to the dependent (Y), where lastly describes the paths from both predictor and mediator variables to the outcome (Y) variable in a combined model with representing the residual terms.
3. Results
3.1. Data descriptives
A total of 927 responses were recorded of which 664 (69.5%) fully completed the survey. The participants were distributed by country as follows: United States (44.4%), The Netherlands (44.3%), Canada (4.4%), United Kingdom (3.2%) and other (see appendix 2d). During the data analysis, only the ‘base’ country of respectively AFIP Foundation (The Netherlands) and StopAfib.org (United States) were included which corresponds to a cumulative percentage of 88.7% (N = 589).
3.2. Assumptions
Essential for further analysis, is the adherence to analytic assumptions. During the preparation, linearity of the data was tested through a normal P-P plot and displayed normality as well as linearity (Supplementary section 2a). Additionally, homoscedasticity was verified using a scatterplot, which confirmed that this assumption was met (Supplementary section 2a). Moreover, no multicollinearity issues were detected.
3.3. Coefficients and Correlations
Table 2 shows the correlations between de variables of interest and the Cronbach’s alpha of individual constructs. Notably, the dependent variable PAAT demonstrated excellent reliability solidifying the overall validity of the construct. The highest correlation was observed between PAAT and visits on OHP In this study, multiple regression analysis demonstrated that the second strongest predictor on PAAT is the content on OHP and subsequent the country of residence and lasty time spent on OHP and perceived effectiveness as the gatekeepers and .
3.4. Structural Model
In this phase, the procedure of constructing the altered HBM to measure the results of the structural model was evaluated. The proposed hypotheses of the study were tested using SEM. The findings of the study are presented in Table 3 and 4.
Overall consistency of the model was tested using several fit indices. Chi-square test statistic was found to be significant . Conversely the Comparative Fit Index (CFI) and Tucker-Lewis Index (TLI) suggested a good and acceptable fit, being respectively (.987 and .624). In addition, the Standardized Root Mean Square Residual (SRMS) was found to be .07, indicating a good fit.
Direct effects
The direct effects of the predictor variables on the mediators and outcome variable were examined (Table 3). Country or residence demonstrated the strongest effect with both mediators (path 1: ; path 2:, as well with PAAT (path 3: implicating that US respondents (1) hold more positive overall attitudes towards AF treatments compared to reference group The Netherlands (0).
Simultaneously, hypotheses 1 and 2 proposed that both mediators significantly and positively affect PAAT. The results indicate that both mediators indeed influence PAAT; however, behavioral evaluation demonstrated a negative relationship with PAAT (β=-.153,p<.003). Thus, the results refute H2, as a one-unit increase in behavioral evaluation results in a decrease in PAAT through a direct path. Conversely, H1 is accepted, suggesting that a higher perception of threat by an individual increases PAAT (β=.254,p<.000).
A primary component in this study is the measured engagement on OHPs and the proposed impact on PAAT. Based on the performed direct analysis, content types consumed on OHP only demonstrate a significant direct effect on PAAT and not through mediators . Also visits on OHP demonstrated the same non significance for both mediators, respectively and , while being significant with PAAT . Indicating that both content types consumed on OHP and frequency of visits on OHPs only affect PAAT and not one of the mediators. Time spent on OHPs showed different results and demonstrated significance with threat perception and PAAT , but not with behavioral evaluation . Indicating that more time spent on platforms, does increase an individual’s threat perception, and besides directly increase their attitudes towards AF treatments.
Lastly, perceived effectiveness demonstrated a significant positive effect on PAAT and behavioral evaluation . However, contrary to the drawn-up hypothesis 6, it did not show a significant effect with threat perception whatsoever . Yet, as H6 included the mediation effect with PAAT through primarily threat perception, indirect effects will be considered in the next section.
Mediation effects
Besides, direct relation between predictor and outcome variables, this study also examined the possible indirect effects that could be inferred from multiple regression analysis (table 4). The pathway from perceived effectiveness to PAAT through both mediators was found to be non-significant . Despite the non-significant positive relationship through threat perception , the non-significant negative coefficient through behavioral evaluation resulted in a net negative indirect effect. Indicating that perceived effectiveness only directly influences patient attitudes but not via both mediators, thereby rejecting H6.
Hypotheses 3, 4 and 5 propose that more engagement on OHPs, significantly and positively impacts PAAT through a mediation of M1 and M2. Combining the effects from the performed analysis, both time spent on OHP and visits on OHP do positively and significantly correlate with PAAT through M1 and M2 . Noteworthy that only time spent on OHP has a significant indirect path through M1. while visits on OHP displays no significance through the separate mediators. Yet, as previously discussed visits on OHP does report a significant relation with PAAT, possibly due to aggregated effects of mediators accepting H3 and 4 in turn. Conversely, the amount of content types consumed on OHPs does not significantly correlate with PAAT through M1,2 therefore rejecting H5. These findings suggest that increased time spent and more frequent visits to online health platforms (OHPs) enhance PAAT, with the effect of time spent on OHPs being mediated by an increase in threat perception. Conversely, the results indicate that the content types consumed on OHPs does not significantly enhance PAAT through either mediator.
Table 4.
Mediator (indirect effects) X1,2,3,4,5 → M1 → M2 → Y (N =589)
| Indirect through threat perception | Indirect through behavioral evaluation | Total indirect effect on patient attitudes towards AF treatments | ||||||||
| SD | SD | SD | Sig. | |||||||
| Content types consumed | .00864 | .010 | .377 | -.003823 | .006 | .160 | .004815 | .010 | .466 | No |
| Perceived Effectiveness | .00813 | .006 | .166 | -.029070 | .021 | .120 | -.020942 | .023 | .372 | No |
| Country of Residence | .17663 | .032 | <.001 | -.082527 | .030 | .006 | .094103 | .037 | .010 | Yes |
| Visits on OHP | .01778 | .009 | .055 | .011016 | .008 | .184 | .028796 | .010 | .006 | Yes |
| Time spent on OHP | .04191 | .015 | .005 | .011016 | .018 | .117 | .052926 | .018 | .004 | Yes |
| Total through M1 | .253 | .047 | <.000 | Yes | ||||||
| Total through M2 | -.093* | .029 | .001 | Yes | ||||||
| Total indirect effect on Y | .160* | .051 | .002 | Yes | ||||||
|
*. Correlation is significant at 0.05 level (two-tailed)123456 **. Correlation is significant at 0.01 level (two-tailed)123456 a. p > 0.05 | ||||||||||
Lastly, country of residence has been found to be significantly influence PAAT through both mediators , where both mediators separately also demonstrate significance through the pathways. The results show that US respondents hold more positive attitudes towards PAAT overall compared to Dutch respondents.
Table 5.
Overview hypotheses outcomes.
| HYPOTHESES | RESULTS | |
| 1 | Higher perceived threat perception will result in a more positive PAAT. | Accepted |
| 2 | Higher perceived behavioral evaluation will result in a more positive PAAT. | Rejected |
| 3 | More frequent visits on the OHP will positively increase PAAT through both mediators perceived threat and perceived behavioral evaluation. | Accepted |
| 4 | Longer sessions on the OHP will positively increase PAAT through both mediators perceived threat perception and perceived behavioral evaluation. | Accepted |
| 5 | More content types consumed on the OHP will positively increase PAAT through both mediators perceived threat perception and perceived behavioral evaluation. | Rejected |
| 6 | Hhigher perceived effectiveness will positively increase PAAT through primarily perceived threat perception. | Rejected |
4. Discussion
This study aimed to examine how engagement with OHPs, perceived treatment effectiveness, and country of residence influence patient attitudes toward AF treatments, through the mediating effects of threat perception and behavioral evaluation as outlined in the HBM. Building upon the premise that patients’ beliefs and engagement behaviors significantly shape their treatment attitudes and adherence, this research contributes to the growing body of evidence on the influence of OHP participation on attitudes towards treatment options. By comparing two professionally curated OHPs (i.e., the AFIP Foundation (Netherlands) and StopAfib.org (United States)) this study provides valuable insights into how these platforms may affect patients’ treatment attitudes through the mediation of threat perception and behavioral evaluation.
The results demonstrate a significant relationship between engagement on OHPs and patient attitudes towards AF treatments. Specifically, higher engagement characterized by frequent visits and longer time spent on OHPs positively influences PAAT, being in line with existing literature [57,58]. Within the context of the HBM, this involvement may increase the perceived threat of AF or the benefits of treatments, possibly leading to better health behavior. However, the results indicated that the number of content types consumed on OHPs did not significantly affect behavioral evaluation and threat perception and only showed positive direct effects on patient attitudes. A possible explanation for this could be that too much information on a platform could lead to an overload, reducing the ability of patients to process the information [59]. Besides, Taibanguay et al. [60] showed in their clinical trial that educating patients led to significant improvements in medication adherence, with no notable differences observed between single-component and multicomponent educational approaches.
Moreover, higher engagement on OHPs positively influenced PAAT through the mediating effects of threat perception and behavioral evaluation, indicating that patients perceive AF-related threats as more severe with increased platform involvement. Boulos & Hassan [36] already reported that expanded health knowledge increases perceived severity and subsequently threat perception. Similarly, Cho and Cho [40] demonstrated that perceived benefits, representing a positive behavioral evaluation as part of health belief, were among the major factors influencing young adults’ intentions to undergo health check-ups. These findings align with previous research indicating that active engagement with health-related digital platforms can enhance patients' perceived understanding and management of their health conditions [6,7].
Furthermore, this study regarded perceived effectiveness being an important actor within the HBM and the foundation of how patients may perceive their treatments. Although perceived effectiveness had a significant positive effect on behavioral evaluation, behavioral evaluation did not mediate the relationship between perceived effectiveness and PAAT. The results show only a direct effect, suggesting that patients who perceive their treatments as effective are more likely to hold favorable attitudes toward adherence. This finding aligns with existing literature that emphasizes the crucial role of perceived effectiveness in shaping health behaviors and adherence [61,62,63,64]. Since the mediation analysis of perceived effectiveness on PAAT through threat perception did not show a significant effect, there may be an interplay of other factors in how patient perceive AF-related threats and corresponding treatment attitude. Personal experiences could distort the perception of treatments resulting in a biased image of certain medications. Welton-Mitchell et al. [65] found out that mental health and emotional states significantly impact risk perception and behaviors. Specifically, anxiety and depression were shown to heighten perceived risks, leading to greater hesitancy in accepting treatment options possibly relating to how treatments overall are being perceived.
Simultaneously, Yin and Lui [66] emphasize that the source of information significantly influences individual risk perception, possibly being a factor in-between perceived effectiveness and PAAT. Namely, platforms that have high credibility and are widely trusted have potential to spark more engagement thus possibly leading to more understanding of the threat [67]. Consequently, the trustworthiness of the information source enhances patients' confidence in the effectiveness of their treatment options, leading to more positive health outcomes.
Notably, country of residence also played a significant role, with patients in the Netherlands displaying more negative attitudes towards AF treatments compared to their counterparts in the United States. This difference may be attributed to varying healthcare systems and cultural attitudes towards healthcare and treatment adherence. In the US, the healthcare system is often characterized by advanced medical technology and a high level of specialized care, which can contribute to a more positive perception of treatment efficacy [68]. Moreover, the U.S. healthcare system emphasizes patient autonomy and choice, particularly among White Caucasian Americans, enabling patients to actively participate in treatment decisions and thereby enhancing their confidence in the care they receive [69]. Furthermore, the competitive nature of the US healthcare market often drives innovation and improvements in treatment options, which can lead to higher patient satisfaction and better perceived effectiveness of treatments [70].
Overall, these findings highlight the significant impact of engagement on online health platforms on patient attitudes towards AF treatments. The study confirms that frequent visits and extended time spent on these platforms positively influence patient attitudes. However, it also reveals that the quantity of content types consumed does not impact behavioral evaluation and threat perception, suggesting potential information overload issues. Additionally, the role of perceived effectiveness in shaping patient attitudes underscores the need for trustworthy and credible health information sources.
Encouraging frequent engagement on platforms could provide significant benefits for overall attitudes towards AF treatments. Operators of OHPs could employ newsletters or nudges through notifications to actively incentivize patients to engage on the platform. Also, prolonging the time individuals spent on the platform through patient tailored content, would also positively affect attitudes patients may hold regarding AF treatments. Previous research has demonstrated that incorporating positive emotions, particularly in combination with the topics of kinship care and affiliation, within platform communication significantly enhances engagement in online health communities, as evidenced by increased average time spent on the platform and higher community subscription rates [71]. Simultaneously, considering the negative effect of behavioral evaluation on attitudes towards AF treatments, healthcare providers could analyze more deeply how evaluated barriers may diminish attitudes people hold towards AF treatments.
Despite its contributions, this study has several limitations that are important to mention. First, although the study provided first insights into the comparison of two professionally curated OHPs across the Netherlands (AFIP Foundation) and the United States (StopAfib.org), the generalizability of the findings to other countries may be limited. Expanding the study to a more diverse set of countries could provide a broader understanding of how cultural and healthcare system differences influence patient engagement and attitudes toward AF treatments. Additionally, the respondents were already familiar with the OHPs used in this study, indicating that the sample may have been relatively well-informed about AF, which could have contributed to generally more positive attitudes toward treatments. To account for differences in awareness and engagement, the study included variables such as perceived effectiveness, frequency of platform visits, and the diversity of content types consumed. These measures allowed for an assessment of how exposure and information consumption influence patients’ attitudes toward AF treatments. Nonetheless, future research could extend these findings by comparing OHP users with non-users to determine whether the observed relationships hold across broader or less-informed populations. Moreover, although AF is a chronic condition and patients with chronic conditions share similar needs [72], cultural background and ethnicity influence health motivations [73] and autonomy [69]. This leaves room for further investigation to validate these findings in more diverse contexts with the inclusion of more extensive ethnic and sociodemographic components. Finally, while this study conceptualized engagement as an independent variable in a mediation model, future research could examine its role as a moderator in a moderated-mediation framework to explore how engagement interacts with threat perception and behavioral evaluation.
5. Conclusions
In conclusion, this study highlights the significant influence of engagement with OHPs on patient attitudes toward atrial fibrillation treatments through the lens of an adapted Health Belief Model. The findings underscore the critical role of professionally curated online resources in shaping patients’ perceptions and fostering more positive attitudes toward treatment adherence. While AF management remains a complex, multifaceted challenge that cannot be addressed solely through digital platforms, the demonstrated positive impact of OHP engagement offers a valuable opportunity for stakeholders to leverage and enhance these platforms. Such efforts may not only improve AF treatment strategies but also contribute to a more health-literate patient population overall.
Author Contributions
Conceptualization, M.K. and J.S.; Methodology, J.S. and M.K.; Survey development, M.K., J.S., M.H., and B.B.; Participant acquisition, M.H., B.B., and M.K.; Analysis, J.S., M.K., and U.K.; Writing—original draft preparation, J.S. and M.K.; Writing—review and editing, M.K.; Visualization, J.S.; Supervision, M.K. and U.K.; Project administration, M.K.; Funding acquisition, M.K. and B.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Nederlandse Organisatie voor Wetenschappelijk Onderzoek (NWO) through the CIRCULAR project (NWA.1389.20.157) and Take-off I Commit2Data (NWO 22057).
Institutional Review Board Statement
The study was approved by the Ethics Committee of Amsterdam UMC (2024-0345) on 17-04-2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. See Supplementary section 3 and 4.
Data Availability Statement
Data supporting the findings of this study are owned by the participating OHPs and are therefore not publicly accessible. Requests for access can be directed to the corresponding author and will be considered on a reasonable basis.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT (GPT-5) to assist in the curation and refinement of some sentences. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AF | Atrial fibrillation |
| HBM | Health Belief Model |
| PAAT | Patient attitudes toward AF treatments |
| SEM | Structural Equation Modeling |
References
- Brundel, B.J.J.M.; Ai, X.; Hills, M.T.; Kuipers, M.F.; Lip, G.Y.H.; de Groot, N.M.S. Atrial Fibrillation. Nat Rev Dis Primers 2022, 8, 1–23. [Google Scholar] [CrossRef]
- Cheen, M.H.H.; Tan, Y.Z.; Oh, L.F.; Wee, H.L.; Thumboo, J. Prevalence of and Factors Associated with Primary Medication Non-Adherence in Chronic Disease: A Systematic Review and Meta-Analysis. Int J Clin Pract 2019, 73, e13350. [Google Scholar] [CrossRef]
- Zhao, S.; Zhao, H.; Wang, X.; Gao, C.; Qin, Y.; Cai, H.; Chen, B.; Cao, J. Factors Influencing Medication Knowledge and Beliefs on Warfarin Adherence among Patients with Atrial Fibrillation in China. Patient Preference and Adherence 2017, 11, 213–220. [Google Scholar] [CrossRef]
- American Heart Association Medication Adherence: Taking Your Meds as Directed Available online:. Available online: https://www.heart.org/en/health-topics/consumer-healthcare/medication-information/medication-adherence-taking-your-meds-as-directed (accessed on 21 October 2025).
- Cutler, D.M. The Good and Bad News of Health Care Employment. JAMA 2018, 319, 758–759. [Google Scholar] [CrossRef]
- Willis, E. Applying the Health Belief Model to Medication Adherence: The Role of Online Health Communities and Peer Reviews. Journal of Health Communication 2018, 23, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Osborn, C.Y.; Mayberry, L.S.; Wallston, K.A.; Johnson, K.B.; Elasy, T.A. Understanding Patient Portal Use: Implications for Medication Management. Journal of Medical Internet Research 2013, 15, e2589. [Google Scholar] [CrossRef] [PubMed]
- Luo, A.; Qin, L.; Yuan, Y.; Yang, Z.; Liu, F.; Huang, P.; Xie, W. The Effect of Online Health Information Seeking on Physician-Patient Relationships: Systematic Review. Journal of Medical Internet Research 2022, 24, e23354. [Google Scholar] [CrossRef]
- Aref-Adib, G.; O’Hanlon, P.; Fullarton, K.; Morant, N.; Sommerlad, A.; Johnson, S.; Osborn, D. A Qualitative Study of Online Mental Health Information Seeking Behaviour by Those with Psychosis. BMC Psychiatry 2016, 16, 232. [Google Scholar] [CrossRef]
- Alanzi, T.M. Public Perceptions Towards Online Health Information: A Mixed-Method Study in Eastern Province of Saudi Arabia. J Healthc Leadersh 2023, 15, 259–272. [Google Scholar] [CrossRef]
- Potpara, T.S.; Mihajlovic, M.; Zec, N.; Marinkovic, M.; Kovacevic, V.; Simic, J.; Kocijancic, A.; Vajagic, L.; Jotic, A.; Mujovic, N.; et al. Self-Reported Treatment Burden in Patients with Atrial Fibrillation: Quantification, Major Determinants, and Implications for Integrated Holistic Management of the Arrhythmia. Europace 2020, 22, 1788–1797. [Google Scholar] [CrossRef]
- Mihajlovic, M.; Simic, J.; Marinkovic, M.; Kovacevic, V.; Kocijancic, A.; Mujovic, N.; Potpara, T.S. Sex-Related Differences in Self-Reported Treatment Burden in Patients with Atrial Fibrillation. Front. Cardiovasc. Med. 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.-Q.; Chen, Y.; Dabbs, A.D.; Wu, Y. The Effectiveness of Smartphone App–Based Interventions for Assisting Smoking Cessation: Systematic Review and Meta-Analysis. Journal of Medical Internet Research 2023, 25, e43242. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Gong, Y.; Zheng, B.; Fan, F.; Yi, T.; Zheng, Y.; He, P.; Fang, J.; Jia, J.; Zhu, Q.; et al. Effects on Adherence to a Mobile App-Based Self-Management Digital Therapeutics Among Patients With Coronary Heart Disease: Pilot Randomized Controlled Trial. JMIR Mhealth Uhealth 2022, 10, e32251. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.; Kwan, Y.H.; Yap, W.L.; Lim, Z.Y.; Phang, J.K.; Loo, Y.X.; Aw, J.; Low, L.L. Factors Influencing Medication Adherence in Multi-Ethnic Asian Patients with Chronic Diseases in Singapore: A Qualitative Study. Front. Pharmacol. 2023, 14. [Google Scholar] [CrossRef]
- Hermans, A.N.L.; Gawalko, M.; Dohmen, L.; van der Velden, R.M.J.; Betz, K.; Duncker, D.; Verhaert, D.V.M.; Heidbuchel, H.; Svennberg, E.; Neubeck, L.; et al. Mobile Health Solutions for Atrial Fibrillation Detection and Management: A Systematic Review. Clin Res Cardiol 2022, 111, 479–491. [Google Scholar] [CrossRef]
- Hodgkin, P.; Horsley, L.; Metz, B. The Emerging World of Online Health Communities (SSIR) Available online:. Available online: https://ssir.org/articles/entry/the_emerging_world_of_online_health_communities (accessed on 23 January 2024).
- Tonko, J.B.; Wright, M.J. Review of the 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation—What Has Changed and How Does This Affect Daily Practice. Journal of Clinical Medicine 2021, 10, 3922. [Google Scholar] [CrossRef]
- Acosta, R.W.; Wolfe, M.S. Chapter 5 - Structure and Organization of the Pre-Travel Consultation and General Advice for Travelers. In Travel Medicine (Second Edition); Keystone, J.S., Kozarsky, P.E., Freedman, D.O., Nothdurft, H.D., Connor, B.A., Eds.; Mosby: Edinburgh, 2008; ISBN 978-0-323-03453-1. [Google Scholar]
- Glanz, K. CHAPTER 6 - Current Theoretical Bases for Nutrition Intervention and Their Uses. In Nutrition in the Prevention and Treatment of Disease; Coulston, A.M., Rock, C.L., Monsen, E.R., Eds.; Academic Press: San Diego, 2001; ISBN 978-0-12-193155-1. [Google Scholar]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Education Monographs 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Education Quarterly 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Suhr, D. The Basics of Structural Equation Modeling.
- Frymier, A.B.; Nadler, M.K. Persuasion : Integrating Theory, Research, and Practice; 4th ed. 2017. [Google Scholar]
- Haddock, G.; Thorne, S.; Wolf, L.J. Attitudes and Behavior. In Oxford Research Encyclopedia of Psychology; 2020 ISBN 978-0-19-023655-7.
- Zolnoori, M.; Fung, K.W.; Fontelo, P.; Kharrazi, H.; Faiola, A.; Wu, Y.S.S.; Stoffel, V.; Patrick, T. Identifying the Underlying Factors Associated With Patients’ Attitudes Toward Antidepressants: Qualitative and Quantitative Analysis of Patient Drug Reviews. JMIR Mental Health 2018, 5, e10726. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Keshishian, A.; Li, X.; Hamilton, M.; Masseria, C.; Gupta, K.; Luo, X.; Mardekian, J.; Friend, K.; Nadkarni, A.; et al. Effectiveness and Safety of Oral Anticoagulants Among Nonvalvular Atrial Fibrillation Patients. Stroke 2018, 49, 2933–2944. [Google Scholar] [CrossRef]
- Lam, W.Y.; Fresco, P. Medication Adherence Measures: An Overview. BioMed Research International 2015, 2015, 217047. [Google Scholar] [CrossRef]
- Vitolins, M.Z.; Rand, C.S.; Rapp, S.R.; Ribisl, P.M.; Sevick, M.A. Measuring Adherence to Behavioral and Medical Interventions. Controlled Clinical Trials 2000, 21, S188–S194. [Google Scholar] [CrossRef] [PubMed]
- Short, S.E.; Mollborn, S. Social Determinants and Health Behaviors: Conceptual Frames and Empirical Advances. Current Opinion in Psychology 2015, 5, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, C.J. A Meta-Analysis of the Effectiveness of Health Belief Model Variables in Predicting Behavior. Health Communication 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Karl, J.A.; Fischer, R.; Druică, E.; Musso, F.; Stan, A. Testing the Effectiveness of the Health Belief Model in Predicting Preventive Behavior During the COVID-19 Pandemic: The Case of Romania and Italy. Front. Psychol. 2022, 12. [Google Scholar] [CrossRef]
- Faculty of Business and Management, UCSI University Sarawak Campus, Malaysia; Hiew, L. -C.; Lee, A.H.; Faculty of Hospitality and Tourism Management, UCSI University Sarawak Campus, Malaysia; Leong, C.-M.; UCSI Graduate Business School, UCSI University, Kuala Lumpur Campus, Malaysia; Liew, C.-Y.; Faculty of Business and Management, UCSI University, Kuala Lumpur Campus, Malaysia; Soe, M.-H.; Malaysian Medical Association (MMA), Kuala Lumpur, Malaysia Do They Really Intend to Adopt E-Wallet? Prevalence Estimates for Government Support and Perceived Susceptibility. AJBR 2022, 12. [Google Scholar] [CrossRef]
- Ullah, F.; Ragazzoni, L.; Hubloue, I.; Barone-Adesi, F.; Valente, M. The Use of the Health Belief Model in the Context of Heatwaves Research: A Rapid Review. Disaster Medicine and Public Health Preparedness 2024, 18, e34. [Google Scholar] [CrossRef]
- Scarinci, I.C.; Bandura, L.; Hidalgo, B.; Cherrington, A. Development of a Theory-Based (PEN-3 and Health Belief Model), Culturally Relevant Intervention on Cervical Cancer Prevention Among Latina Immigrants Using Intervention Mapping. Health Promotion Practice 2012, 13, 29–40. [Google Scholar] [CrossRef]
- Boulos, D.N.K.; Hassan, A.M. Using the Health Belief Model to Assess COVID-19 Perceptions and Behaviours among a Group of Egyptian Adults: A Cross-Sectional Study. BMC Public Health 2023, 23, 1624. [Google Scholar] [CrossRef]
- Yang, X.; Wei, L.; Liu, Z. Promoting COVID-19 Vaccination Using the Health Belief Model: Does Information Acquisition from Divergent Sources Make a Difference? International Journal of Environmental Research and Public Health 2022, 19, 3887. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K. How Well the Constructs of Health Belief Model Predict Vaccination Intention: A Systematic Review on COVID-19 Primary Series and Booster Vaccines. Vaccines 2023, 11, 816. [Google Scholar] [CrossRef] [PubMed]
- LaMorte, W.W. Online MPH and Teaching Public Health | SPH Available online:. Available online: https://www.bu.edu/sph/online-mph-and-teaching-public-health/ (accessed on 21 October 2025).
- Cho, M.-K.; Cho, Y.-H. Role of Perception, Health Beliefs, and Health Knowledge in Intentions to Receive Health Checkups among Young Adults in Korea. International Journal of Environmental Research and Public Health 2022, 19, 13820. [Google Scholar] [CrossRef] [PubMed]
- Ghorbani-Dehbalaei, M.; Loripoor, M.; Nasirzadeh, M. The Role of Health Beliefs and Health Literacy in Women’s Health Promoting Behaviours Based on the Health Belief Model: A Descriptive Study. BMC Women’s Health 2021, 21, 421. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Wu, Y.; Huang, Z.; Sun, X. Associations between Media Use, Self-Efficacy, and Health Literacy among Chinese Rural and Urban Elderly: A Moderated Mediation Model. Front. Public Health 2023, 11. [Google Scholar] [CrossRef]
- Good, A.; Abraham, C. Can the Effectiveness of Health Promotion Campaigns Be Improved Using Self-Efficacy and Self-Affirmation Interventions? An Analysis of Sun Protection Messages. Psychol Health 2011, 26, 799–818. [Google Scholar] [CrossRef]
- Ware, L.J.; Prioreschi, A.; Bosire, E.; Cohen, E.; Draper, C.E.; Lye, S.J.; Norris, S.A. Environmental, Social, and Structural Constraints for Health Behavior: Perceptions of Young Urban Black Women During the Preconception Period-A Healthy Life Trajectories Initiative. J Nutr Educ Behav 2019, 51, 946–957. [Google Scholar] [CrossRef]
- Andajani-Sutjahjo, S.; Ball, K.; Warren, N.; Inglis, V.; Crawford, D. Perceived Personal, Social and Environmental Barriers to Weight Maintenance among Young Women: A Community Survey. International Journal of Behavioral Nutrition and Physical Activity 2004, 1, 15. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S. Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic. International Journal of Environmental Research and Public Health 2020, 17, 8666. [Google Scholar] [CrossRef]
- Moorman, C.; van Heerde, H.J.; Moreau, C.P.; Palmatier, R.W. Marketing in the Health Care Sector: Disrupted Exchanges and New Research Directions. Journal of Marketing 2024, 88, 1–14. [Google Scholar] [CrossRef]
- Higgins, T.; Larson, E.; Schnall, R. Unraveling the Meaning of Patient Engagement: A Concept Analysis. Patient Education and Counseling 2017, 100, 30–36. [Google Scholar] [CrossRef]
- Korda, H.; Itani, Z. Harnessing Social Media for Health Promotion and Behavior Change. Health Promotion Practice 2013, 14, 15–23. [Google Scholar] [CrossRef]
- Wu, J.; Fan, S.; Zhao, J.L. Community Engagement and Online Word of Mouth: An Empirical Investigation. Information & Management 2018, 55, 258–270. [Google Scholar] [CrossRef]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education : Theory, Research, and Practice; 4th ed.; Jossey-Bass/Wiley, 2008; ISBN 978-0-7879-9614-7.
- Rajpura, J.; Nayak, R. Medication Adherence in a Sample of Elderly Suffering from Hypertension: Evaluating the Influence of Illness Perceptions, Treatment Beliefs, and Illness Burden. JMCP 2014, 20, 58–65. [Google Scholar] [CrossRef]
- Chrystyn, H.; Small, M.; Milligan, G.; Higgins, V.; Gil, E.G.; Estruch, J. Impact of Patients’ Satisfaction with Their Inhalers on Treatment Compliance and Health Status in COPD. Respiratory Medicine 2014, 108, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Faber, J.; Fonseca, L.M. How Sample Size Influences Research Outcomes. Dental Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. Sampling Techniques; Wiley series in probability and mathematical statistics; 3. ed. Wiley: New York, NY, 1977; ISBN 978-0-471-16240-7. [Google Scholar]
- Russo, G.M.; Tomei, P.A.; Serra, B.; Mello, S. Differences in the Use of 5- or 7-Point Likert Scale: An Application in Food Safety Culture. Organizational Cultures: An International Journal 2021, 21, 1–17. [Google Scholar] [CrossRef]
- Wang, J.; Yao, T.; Wang, Y. Patient Engagement as Contributors in Online Health Communities: The Mediation of Peer Involvement and Moderation of Community Status. Behavioral Sciences 2023, 13, 152. [Google Scholar] [CrossRef]
- Meng, F.; Zhang, X.; Liu, L.; Ren, C. Converting Readers to Patients? From Free to Paid Knowledge-Sharing in Online Health Communities. Information Processing & Management 2021, 58, 102490. [Google Scholar] [CrossRef]
- Hong, H.; Kim, H.J. Antecedents and Consequences of Information Overload in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health 2020, 17, 9305. [Google Scholar] [CrossRef]
- Taibanguay, N.; Chaiamnuay, S.; Asavatanabodee, P.; Narongroeknawin, P. Effect of Patient Education on Medication Adherence of Patients with Rheumatoid Arthritis: A Randomized Controlled Trial. PPA 2019, 13, 119–129. [Google Scholar] [CrossRef]
- Chan, A.H.Y.; Horne, R.; Hankins, M.; Chisari, C. The Medication Adherence Report Scale: A Measurement Tool for Eliciting Patients’ Reports of Nonadherence. Br J Clin Pharmacol 2020, 86, 1281–1288. [Google Scholar] [CrossRef]
- Shitu, K.; Adugna, A.; Kassie, A.; Handebo, S. Application of Health Belief Model for the Assessment of COVID-19 Preventive Behavior and Its Determinants among Students: A Structural Equation Modeling Analysis. PLOS ONE 2022, 17, e0263568. [Google Scholar] [CrossRef]
- Jebarajakirthy, C.; Das, M.; Rundle-Thiele, S.; Ahmadi, H. Communication Strategies: Encouraging Healthy Diets for on-the-Go Consumption. Journal of Consumer Marketing 2022, 40, 27–43. [Google Scholar] [CrossRef]
- Zhou, T. Understanding Online Health Community Users’ Information Adoption Intention: An Elaboration Likelihood Model Perspective. Online Information Review 2021, 46, 134–146. [Google Scholar] [CrossRef]
- Welton-Mitchell, C.; Dally, M.; Dickinson, K.L.; Morris-Neuberger, L.; Roberts, J.D.; Blanch-Hartigan, D. Influence of Mental Health on Information Seeking, Risk Perception and Mask Wearing Self-Efficacy during the Early Months of the COVID-19 Pandemic: A Longitudinal Panel Study across 6 U.S. States. BMC Psychology 2023, 11, 203. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.D.-C.; Lui, J.N.-M. Factors Influencing Risk Perception during Public Health Emergencies of International Concern (PHEIC): A Scoping Review. BMC Public Health 2024, 24, 1372. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Yin, J.; Song, Y. An Exploration of Rumor Combating Behavior on Social Media in the Context of Social Crises. Computers in Human Behavior 2016, 58, 25–36. [Google Scholar] [CrossRef]
- Davis, K.; Schoen, C.; Schoenbaum, S.C.; Doty, M.M.; Holmgren, A.L.; Kriss, J.L.; Shea, K.K. MIRROR, MIRROR ON THE WALL: AN INTERNATIONAL UPDATE ON THE COMPARATIVE PERFORMANCE OF AMERICAN HEALTH CARE.
- Thompson, G.A.; Segura, J.; Cruz, D.; Arnita, C.; Whiffen, L.H. Cultural Differences in Patients’ Preferences for Paternalism: Comparing Mexican and American Patients’ Preferences for and Experiences with Physician Paternalism and Patient Autonomy. International Journal of Environmental Research and Public Health 2022, 19, 10663. [Google Scholar] [CrossRef]
- Cutler, D.M.; Scott Morton, F. Hospitals, Market Share, and Consolidation. JAMA 2013, 310, 1964–1970. [Google Scholar] [CrossRef]
- Kuipers, M.F.; Konus, U.; Brundel, B.J.J.M.; İlker Birbil, Ş. Communication Strategies Driving Online Health Community Patient Awareness and Engagement Investigated within Atrial Fibrillation Context. npj Digit. Med. 2025, 8, 446. [Google Scholar] [CrossRef]
- Fayn, M.-G.; des Garets, V.; Rivière, A. Collective Empowerment of an Online Patient Community: Conceptualizing Process Dynamics Using a Multi-Method Qualitative Approach. BMC Health Services Research 2021, 21, 958. [Google Scholar] [CrossRef]
- Pick, C.M. OPEN Fundamental Social Motives Data Descriptor Measured across Forty-Two Cultures in Two Waves. Scientific Data.
Figure 1.
Depiction of the conceptual model, showing the expected relationship between the predictor variables (country of residence, engagement on the OHP, and perceived effectiveness), the mediators (threat perception and behavioral evaluation), and the outcome variable (patients’ attitudes towards AF treatment).
Figure 1.
Depiction of the conceptual model, showing the expected relationship between the predictor variables (country of residence, engagement on the OHP, and perceived effectiveness), the mediators (threat perception and behavioral evaluation), and the outcome variable (patients’ attitudes towards AF treatment).
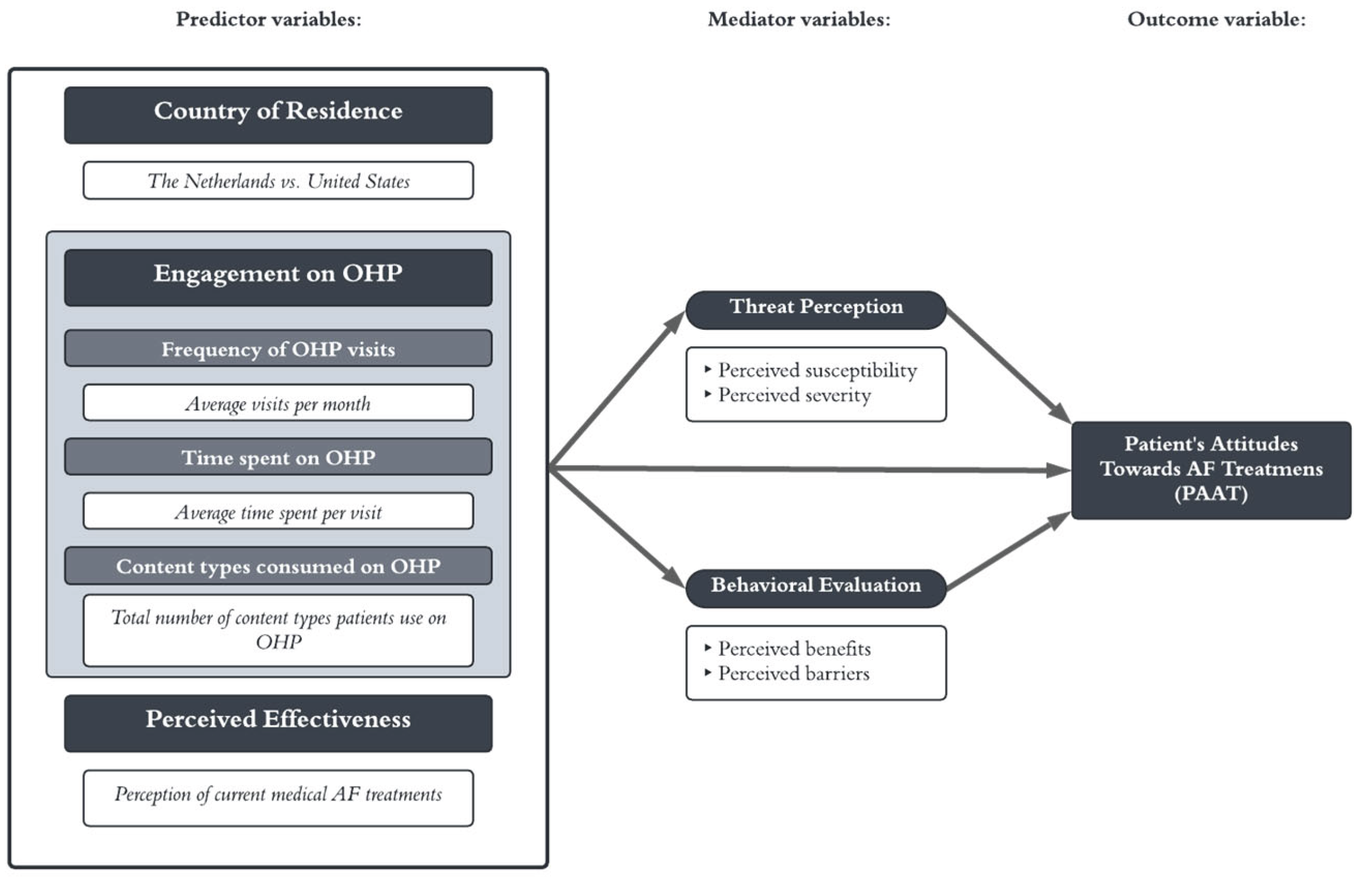
Table 2.
Means, standard deviations and Pearson correlation matrix for ordinal variables (N = 589)
| M | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | |
| Threat Perception | 5.6797 | .9711 | (.709) | |||||||
| Behavioral Evaluation | 5.4174 | 1.065 | .242** | (.764) | ||||||
| Country of Residence | .5008 | .50042 | .407** | .304** | − | |||||
| Content types consumed (count) | 1.8509 | 1.0144 | .162** | -.001a | .114** | − | ||||
| Visits of OHP | 1.8183 | 1.1078 | .210** | .006a | .278** | .394** | − | |||
| Time spent on OHP | 1.64 | .732 | .182** | -.025a | .098* | .409** | .146** | − | ||
| Perceived Effectiveness | 5.38 | 1.841 | .129** | .377** | .213** | .028a | .022a | .001** | − | |
| Patients’ Attitudes | 4.3693 | 1.0470 | .390** | .009a | .344** | .390** | .438** | .284** | .165** | (.925) |
| Cronbach’s alphas are shown in the diagonals.123456 *. Correlation is significant at 0.05 level (two-tailed)123456 **. Correlation is significant at 0.01 level (two-tailed)123456 a. p > 0.05 | ||||||||||
Table 3.
Analysis of direct pathways X1,2,3,4,5 → M1,2 and X1,2,3,4,5 → Y and M1,2 → Y (N = 589)
| Path 1 (a1) | Path 2 (a2) | Path 3 (b1b2c’) | ||||||||
| Threat perception | Behavioral Evaluation | PAAT | ||||||||
| (SD) | (SD) | (SD) | ||||||||
| Constant | 4.664* | 31.775 | <.000 | 4.326* | 27.775 | <.000 | 2.070* | 7.449 | <.000 | |
| (.147) | − | − | (.156) | − | − | (.278) | − | − | ||
| Content on OHP | .034a | .802 | .442 | .025a | .555 | .579 | .197* | 4.955 | <.000 | |
| (.042) | − | − | (.045) | − | − | (.040) | − | − | ||
| Perceived Effectiveness | .0320a | 1.597 | .110 | .190* | 8.926 | <.000 | .083* | 4.124 | <.000 | |
| (.02) | − | − | (.021) | − | − | (.020) | − | − | ||
| Country of Residence | .695* | 8.972 | <.000 | .539* | 6.563 | <.000 | .340* | 4.234 | <.000 | |
| (.077) | − | − | (.082) | − | − | (.080) | − | − | ||
| Visits on OHP | .070a | 1.910 | .056 | -.072a | -1.834 | .067 | .239* | 6.839 | <.000 | |
| (.037) | − | − | (.039) | − | − | (.035) | − | − | ||
| Time spent on OHP | .165* | 3.025 | .002 | -.072a | -1.243 | .214 | .154* | 2.976 | <.000 | |
| (.054) | − | − | (.058) | − | − | (.052) | − | − | ||
| Threat Perception (M1) | .254* | 6.525 | <.000 | |||||||
| (.039) | − | − | ||||||||
| Behavioral Evaluation (M2) | -.153* | -4.159 | <.003 | |||||||
| (.037) | − | − | ||||||||
|
*. p < .05 a. p > .05 |
||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



