
Submitted:
01 March 2025
Posted:
10 March 2025
You are already at the latest version
Abstract
The aim of this study was to evaluate for the first time the feasibility of implementing LOLA, a speech AI-driven conversational assistant, in monitoring and managing OAT in patients with non-valvular
Methods.
In 2023, we conducted a pilot prospective observational study of patients with AF and TAO. All patients received a first contact call from LOLATAO, and then monthly calls, following a predefined protocol by the hematologists . At the end of the study, a satisfaction questionnaire was carried out.
Results
Fifty patient. The mean age was 75 years with 33% women. One-third of the patients (n=16) were with antivitamin K treatment and two-thirds (33) with DOACs. A total of 579 calls were made with a median follow-up of 278 days. LOLATAO had high rates of acceptability (85%), adherence (90%) and satisfaction (>95%). 42% of the patients reported at least one forgetfulness dose in the last month, 18% ( reported having a scheduled intervention needing bridging therapy. In patients with VKAs , 94% (n=15) reported at least once being unaware of their TRT and, 75% (n=12) of patients reported having a TRT< 65%. Those patients in whom TRT was < 65% were switched to DOACs. LOLA saved a total of 10 hours per month for the hematologists in the follow-up.
Conclusions
The study suggests that LOLATAO seems to be a tool to help in the management of chronic follow-up of patients with AF and OAT that reduces the burden of care with high rates of acceptance and satisfaction by patients.

Keywords:
Virtual Assistant
; Artificial intelligence
; oral anticoagulation
; atrial fibrillation
Introduction
Atrial fibrillation (AF) is the most frequent arrhythmia in adults and its prevalence is expected to double in the next 30 years [1,2,3]. Also, AF increases five-fold the risk of stroke [4]. Oral anticoagulation therapy (OAT) decreases the risk of cardioembolic stroke and all-cause mortality in patients with non-valvular AF [5,6,7,8,9,10]. Thus, OAT is the gold standard for the prophylaxis of AF-related stroke [6,7,8]. Effective OAT implies a lifelong clinical follow-up, including regular assessments of bleeding risk, drug interactions, side effects, dosing adjustments, and control of adherence. Clinical guidelines advocate for a patient-centric and multidisciplinary approach to integrated AF care. This approach emphasises structured follow-up intervals, ranging from every 1 to 6 months, tailored to individual patient factors [6,7,8,11].
The growing healthcare burden associated with AF poses challenges for healthcare centres in implementing this comprehensive care model. Digital health tools facilitate coordination among various specialties (such as cardiologists, haematologists, general practitioners, and nurse-led teams) and enhance patient engagement through home-based services [8,12,13]. Multiple e-health solutions have already been used in AF across all stages of the disease with promising results, from screening and diagnosis through mobile or wearable ECG devices [14,15,16,17,18], to computerised decision-making support systems for antithrombotic therapy optimisation [19,20,21,22] and point-of-care monitoring of anticoagulation for patients using AVKs [23,24,25], to mobile health (mHealth) interventions to increase treatment adherence [26,27], manage cardiovascular modifiable risk factors [22,28,29,30,31] and improve patient’s disease literacy [22,26,27,32].
Conversational agents are a type of mHealth intervention that facilitate automated telephone communication with patients and can therefore enhance health care accessibility and improve the reach of clinical services over face-to-face consultation [33,34,35,36,37]. Due to this heterogeneity, it is very difficult to establish a standardised method for evaluating conversational agents in the health care setting. That is why results from the studies evaluating conversational agents have shown promising but inconsistent effects on their accuracy, user acceptability and effectiveness. Most of the health care conversational agents reported in the literature were predominantly unidirectional and non-AI-driven [33,34,35] and those incorporating AI technologies were mostly text-based even though speech interactions seem to be more natural and comfortable [36,37]. There are few examples of speech AI-driven virtual assistants in medicine. The importance of these systems falls on its understanding of what the user says (speech recognition), the ability to plan an appropriate reaction (natural language processing), and articulating the response (natural language generation). [38,39,40,41].
Nevertheless, voice- assistants like Lola from TUCUVI focus more on customization and adaptation to the specific needs of the user in different clinical contexts. These medical assistants can significantly aid in reducing the workload of healthcare professionals and enhancing patient care efficiency.
Despite this progress, our literature search reveals a critical gap, no AI-driven automated telephone interventions exist for AF patients or monitoring anticoagulation treatment. [30,31,32,33,42,43,44,45]. Our study aims to address this void and evaluate the potential impact of AI-driven conversational agents in these specific contexts.
Given the existing evidence, the aim of this study was to evaluate for the first time the feasibility of implementing LOLA, a speech AI-driven conversational assistant, in monitoring and managing OAT in patients with non-valvular AF.
Material and Methods
Study Design and Population
From 1st January 2023 to 31st December 2023, we conducted an observational prospective study in our Anticoagulation Unit of our Digital unit [46,47] the University Vinalopó Hospital. Approval was obtained from the local ethics committee. (date 22-10-2022, Code ID:LOLA_TAO). Patients were recruited consecutively in our ambulatory facilities. The inclusion criteria included: (1) aged ≥ 18 years, (2) a documented diagnosis of non-valvular AF, (3) receiving OAT, (4) had a mobile phone that was able to receive calls, and (5) were competent in the Spanish language. Participants were excluded from the study if they (1) had a medical illness with anticipated life expectancy of <6 months, (2) were unable to provide written consent, or (3) had a concomitant illness or physical impairment (for example hearing impairment), or mental condition that in the opinion of the study team or the primary physician could interfere with the conduct of the study, including outcome assessment.
The study was based on the use of an AI-based voice virtual assistant (LOLA), a medical device from the company Tucuvi Care SL. It is compliant with European GDPR and certified by ISO 27001 and ENS. It is a voiced-based conversational technology that performs AI-driven automated phone calls. This technology simulates human conversations with proper responses to dialogue. LOLA can analyse verbal speech using VRS and NPL. Then, it uses a speech-to-text algorithm to obtain and codify data in a structured database. (See Figure 1).
The protocol study workflow, chronogram and the different protocols designed by OAT Treatment are represented in Supplemental Figure 1.
First, the medical team established a protocol of questions and possible answers for each type of OAT and defined which answers to interpret as an “alert” by the virtual assistant. (See Supplemental Table 1). Then, regular screening of upcoming patient appointments was conducted by the research team to identify potential participants during a 6-month period (From January to June 2023). These participants were approached (1) face-to-face during their visit to obtain written consent, or (2) over the telephone before they attended their scheduled appointment. If they met the inclusion criteria a research staff member arranged a personal meeting with the prospective participants. All interested participants received an information sheet and a consent form describing the study and providing sufficient information for the participant to decide regarding study participation. Afterward, the consent form was signed by both the participant and the research staff before the participant undertook any study procedure. Eligible individuals who provided informed consent were asked to complete a baseline assessment and demographic data were collected. After baseline data collection, patients were registered in Tucuvi Dashboard, an AI web platform (See Supplemental Figure 2), and were assigned a predefined protocol according to the type of OAT.
Once the patients were included in the web platform, outreaches from LOLA occurred at 24 to 48 hours from the baseline assessment to welcome the patient to the study and inform about the follow-up process (Initial phone call) and then monthly until the end of the 12-month follow-up period (follow-up phone calls). When LOLA detected that an answer fulfilled the definition of alert, a notification was sent to the physician in charge of the patient. Then, the physician reviewed the answer and medical history of the patient and decided whether to perform an intervention or not. At the end of the study, the patients received a phone call with a satisfaction questionnaire (final phone call).
The primary outcome of the study was to assess the acceptability, adherence, and satisfaction of implementing LOLA, an AI-based conversational agent to follow-up AF patients on OAT. The secondary outcomes were to analyse the usability and clinical utility of LOLA. The summary of the parameters evaluated are in Table 2. Acceptability was evaluated measuring the percentage of patients that signed the informed consent of the total of eligible patients. During follow-up, the adherence to the program was evaluated monthly through program engagement metrics (number of answered telephone calls, number of completed telephone calls). Usability of the patients was evaluated by measuring the duration time of each phone call and the usability of the medical doctors by measuring the number of alerts revised and interventions performed. Intervention and alert use metrics were automatically collected through the AI-based conversational agent system and website analytics. Clinical outcomes were evaluated monthly by measuring the number of clinical situations detected, the concordance between the alerts detected and the clinical condition referred by the patient and the number of hours of the medical team saved by the AI-conversational agent. The clinical situations detected were classified as: medication adherence (self-reported), health events (self-reported and medical records) and healthcare service use (self-reported, medical records). The medical team revised the concordance between the alerts detected and the medical records/patient contact to assess if the alerts detected were related to actual clinical events. The number of hours of the medical team saved by LOLA was calculated automatically as a formula based on total calls made to the patients and the time that the doctor would have needed to conduct a follow-up call. To calculate the time spent by a doctor vs. LOLA, it was taken into account that LOLA is 20% more efficient than a human being in terms of follow up visits. On the other hand, the time it would take a person to prepare for the call is also taken into account, (almost 2 minutes). Satisfaction was evaluated at the end of the study by a study-specific questionnaire, Net Promoter Score (NPS) y Customer satisfaction (CSAT) performed also through LOLA. [48,49]
Statistical Methods
We calculated descriptive statistics, including means, medians and ranges. Although the sample size was insufficient for meaningful regression analysis, we also tested for differences across age and gender groups using 2-tailed t tests and chi-square tests. The power for these comparisons was low; therefore, this analysis was an exploratory evaluation that may be important to future study design.
Results
This pilot study enrolled a cohort of 50 patients, from which one was excluded posthumously from the analysis. The mean age was 75±16 years-old and most of them were male (33% women). Regarding OAT, one third of the patients were on AVKs (n=16) and two thirds on DOACs (n=33). (See Table 1).
The workflow during the study is resumed in Figure 2. Oral anticoagulant therapy was administered, with a division of one third on Vitamin K Antagonists (AVKs) and two thirds on Direct Oral Anticoagulants (DOACs). Throughout a median follow-up period of 278 days, a total of 579 telephone calls were conducted, comprising 50 initial, 480 follow-up, and 49 final calls, with an average duration of 3 minutes and 17 seconds per call (range: 3.05 -3.81). The study detected 296 alerts, which led to 55 interventions by the medical team. At the end of the study, the team saved more than 110 hours / year by using LOLATAO.
LOLATAO demonstrated high acceptability at 85% and adherence at 90%, maintaining these rates consistently over the follow-up period. Despite the number of alerts remaining constant, the frequency of interventions decreased, with only 19% of alerts necessitating an intervention. Clinical outcomes revealed that approximately 40% of patients reported missing at least one dose in the previous month, with no significant difference between AVKs and NOACs. The clinical issues identified included bleeding events, the necessity for bridging therapy, renal function impairment, unknown therapeutic range time (TRT), and TRT below 65%, with the latter two showing lower concordance rates of 57% and 65%, respectively. It is noteworthy that over 90% of patients on AVKs were initially unaware of their TRT, but after education, only a quarter of those who reported a TRT below 65% actually had such rates. (See Table 2). Regarding renal impairment, 40% of the patients were already affected before starting the study, yet none required dose adjustments during the follow-up. Bleeding events occurred in 40% of the cohort within the last month, more frequently among those on AVKs, albeit all incidents were minor. About 20% of patients had scheduled surgical interventions within the forthcoming month, with bridging therapy being more prevalent among those on NOACs due to AVK users planning their surgical procedures during INR control visits. In terms of healthcare service utilisation, 36% of patients visited the emergency department, and 6% required hospitalisation, none of which were related to OAT. LOLA shows a high acceptability and adherence were further evidenced by the 85% participation rate among eligible patients, with more than 90% of follow-up calls answered and completed. The stability of alert numbers contrasted with a decline in interventions, where only 19% of detected alerts led to an intervention. (See Supplemental Figure 3)
Initially, the agreement between LOLATAO and the alerts was low, but as a pilot study as time progressed it improved over time as the assistant was trained to better discriminate alerts, and the medical team adjusted the alerts accordingly. By the end of the study, the concordance was high enough that few interventions or unscheduled visits by the haematologist team were required. Adherence data from the 480 follow-up calls indicated that up to 92% responded to the calls, and 91% completed them. The survey showed a high satisfaction measured by NPS and CSAT (see Table 3).
Discussion
To the best of our knowledge, this is the first evaluation of an AI conversational technology to support AF anticoagulation-integrated care , and our findings contribute to the growing body of research on the use of AI in healthcare. Our findings achieve the primary goal of the study, demonstrating the practicality of deploying an AI-Conversational agent for monitoring Oral Anticoagulant Therapy (OAT) in Atrial Fibrillation (AF) patients within the hybrid haematology unit. [46] This aligns with our strategic trajectory of digital transformation, where telemedicine has been successfully integrated into the management of anticoagulated patients in the Anticoagulation (TAO) Unit.[47]. It is noteworthy that LOLATAO enables a more thorough follow-up compared to traditional methods, ensuring higher levels of engagement and adherence. It liberates physicians from the time-intensive follow-up process, allowing prioritisation of care for those in need over stable patients. With only 37% of calls triggering an alert but only 19% needed an intervention, over 60% required no review, enabling us to discern critical alarms and necessitate a telematic visit, thus reducing physician calls by over 60% and, consequently, the healthcare burden.
This investigation is pioneering in presenting data on the viability of a cutting-edge AI-Conversational agent for the standard follow-up of OAT in AF patients. It offers an in-depth assessment of the implementation process, as well as the acceptability, adherence, satisfaction, and clinical value of this digital healthcare intervention. In doing so, it fills a knowledge void regarding the role of AI-Conversational automated monitoring in aiding patients with chronic conditions and, for the first time, establishes a customised follow-up plan tailored to the unique attributes of each patient.
Presently, various virtual assistants exist, each underpinned by distinct machine learning models. For instance, Lola has been documented for tracking COVID-19 patients. A review of clinical trials reveals that merely five studies meet the specified eligibility criteria, yet none resemble the virtual assistant Lola. [39,40,41,42,43,44,45]
The study also addresses critical issues concerning the adherence and educational deficit among OAT patients and concurs with extensive research on this topic [50]. Clinically, LOLATAO has underscored the need for diverse healthcare professionals and clinicians to educate patients about the importance of adherence, even post-development of any safety or efficacy outcomes. In conventional anticoagulation units, the high demand for care makes such comprehensive, monthly patient monitoring challenging [50]. For that reason, the haematologist team has played a crucial role in the implementation of LOLATAO in the OAT Unit. LOLATAO needs to be programmed to obtain the better results, so the investigational team, the haematologists, contributed to the process with the clinical expertise providing the essential medical knowledge required to program and fine-tune LOLATAO. So that, they play crucial roles in the implementation and operation of LOLATAO, ensuring that the system is clinically effective, patient-focused, and continuously improving. Their role encompasses both the technical aspects of programming and adjusting the AI system, as well as the human aspects of patient care and education. After the pilot study, now LOLATAO is ready to be implemented in other anticoagulation Units.
With regards to the significance of the study, it is noteworthy that results underscore the promising role of AI-based virtual assistants in enhancing patient management for FA in TAO, potentially leading to more tailored and efficient healthcare solutions.
This study's limitations include being conducted at a single institution with a small cohort and brief follow-up. It also lacked a control group and had a gender imbalance.
Several Implications of the study are that conversational AI interventions hold the potential to augment clinical care by providing continuous patient support between visits. Future software advancements should aim to integrate such systems with existing electronic medical records in both primary and secondary care settings, representing a significant hurdle for the health information technology industry. Facilitating clinicians’ direct access to data gathered by the system, such as risk assessments and symptom evaluations, would mark a pivotal advancement in the integration of AF care.
Therefore, LOLATAO, as an AI-assistant in anticoagulation management, has proven through our pilot study to enable tighter control, reduce care demand without compromising quality, and provide personalised attention, all while achieving high patient satisfaction among anticoagulated individuals.
Also, the information obtained as secondary objectives of the study, gave us the information related to the practical value or usefulness of an artificial intelligence (AI)-driven assistant based on data collected during a preliminary study. Such studies are essential for assessing the actual clinical performance of AI systems, ensuring safety, evaluating human factors, and paving the way for larger-scale trials.
Artificial Intelligence (AI) can significantly enhance healthcare outcomes for patients with FA through various means such as a personalised care due to that LOLATAO can make a vast amounts of patient phone calls and obtain data and provide personalised interventions, leading to improved patient outcomes, also a better effectivity in treatment due to the ability to automate outreach based on patient journeys, support clinical adherence, and engage patients effectively, and what is also very important of the healthcare workforce support, meanwhile LOLATAO automates this task, healthcare professionals can focus more on meaningful interactions with patients, positively affecting health outcomes.
In summary, AI-driven assistant LOLATAO has the potential to transform the care experience for OAT patients by offering personalised, efficient, and integrated healthcare solutions. The use of LOLATAO in clinical practice may reduce the need for frequent monitoring and interventions, leading to cost savings and improved patient outcomes and saving the patient multiple visits to health services. Further investigations are essential to evaluate the clinical impact of such interventions.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org
Funding
Not applicable.
Conflicts of Interest
No competing interest.
References
- Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: An increasing epidemic and public health challenge. Int J Stroke Off J Int Stroke Soc. 2021 Feb;16(2):217–21.
- Krijthe BP, Kunst A, Benjamin EJ, Lip GYH, Franco OH, Hofman A, et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. 2013 Sep 14;34(35):2746–51.
- Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association [Internet]. [cited 2024 Apr 17]. Available from: https://www.ahajournals.org/doi/epub/10.1161/CIR.0000000000000659.
- Pisters R, Lane DA, Marin F, Camm AJ, Lip GYH. Stroke and Thromboembolism in Atrial Fibrillation: – Systematic Review of Stroke Risk Factors and Risk Stratification Schema –. Circ J. 2012;76(10):2289–304.
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007 Jun 19;146(12):857–67.
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021 Feb 1;42(5):373–498.
- Andrade JG, Aguilar M, Atzema C, Bell A, Cairns JA, Cheung CC, et al. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society Comprehensive Guidelines for the Management of Atrial Fibrillation. Can J Cardiol. 2020 Dec;36(12):1847–948.
- Lip GYH, Freedman B, De Caterina R, Potpara TS. Stroke prevention in atrial fibrillation: Past, present and future: Comparing the guidelines and practical decision-making. Thromb Haemost. 2017;117(07):1230–9.
- Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. The Lancet. 2014 Mar 15;383(9921):955–62.
- Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018 Apr 21;39(16):1330–93.
- Kotecha D, Chua WWL, Fabritz L, Hendriks J, Casadei B, Schotten U, et al. European Society of Cardiology smartphone and tablet applications for patients with atrial fibrillation and their health care providers. Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol. 2018 Feb 1;20(2):225–33.
- Brieger D, Amerena J, Attia J, Bajorek B, Chan KH, Connell C, et al. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Diagnosis and Management of Atrial Fibrillation 2018. Heart Lung Circ. 2018 Oct 1;27(10):1209–66.
- Lowres N, Neubeck L, Salkeld G, Krass I, McLachlan AJ, Redfern J, et al. Feasibility and cost-effectiveness of stroke prevention through community screening for atrial fibrillation using iPhone ECG in pharmacies. The SEARCH-AF study. Thromb Haemost. 2014 Jun;111(6):1167–76.
- Hickey KT, Hauser NR, Valente LE, Riga TC, Frulla AP, Masterson Creber R, et al. A single-center randomised, controlled trial investigating the efficacy of a mHealth ECG technology intervention to improve the detection of atrial fibrillation: the iHEART study protocol. BMC Cardiovasc Disord. 2016 Jul 16;16:152.
- Haberman ZC, Jahn RT, Bose R, Tun H, Shinbane JS, Doshi RN, et al. Wireless Smartphone ECG Enables Large-Scale Screening in Diverse Populations. J Cardiovasc Electrophysiol. 2015 May;26(5):520–6.
- Lowres N, Mulcahy G, Gallagher R, Ben Freedman S, Marshman D, Kirkness A, et al. Self-monitoring for atrial fibrillation recurrence in the discharge period post-cardiac surgery using an iPhone electrocardiogram. Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg. 2016 Jul;50(1):44–51.
- Ricci RP, Morichelli L, Santini M. Remote control of implanted devices through Home Monitoring technology improves detection and clinical management of atrial fibrillation. Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol. 2009 Jan;11(1):54–61.
- Bajorek B, Magin P, Hilmer S, Krass I. A cluster-randomised controlled trial of a computerised antithrombotic risk assessment tool to optimise stroke prevention in general practice: a study protocol. BMC Health Serv Res. 2014 Feb 7;14:55.
- Wang Y, Bajorek B. Safe use of antithrombotics for stroke prevention in atrial fibrillation: consideration of risk assessment tools to support decision-making. Ther Adv Drug Saf. 2014 Feb;5(1):21–37.
- Eckman MH, Wise RE, Naylor K, Arduser L, Lip GYH, Kissela B, et al. Developing an Atrial Fibrillation Guideline Support Tool (AFGuST) for shared decision making. Curr Med Res Opin. 2015 Apr;31(4):603–14.
- Guo Y, Chen Y, Lane DA, Liu L, Wang Y, Lip GYH. Mobile Health Technology for Atrial Fibrillation Management Integrating Decision Support, Education, and Patient Involvement: mAF App Trial. Am J Med. 2017 Dec 1;130(12):1388-1396.e6.
- Bubner TK, Laurence CO, Gialamas A, Yelland LN, Ryan P, Willson KJ, et al. Effectiveness of point-of-care testing for therapeutic control of chronic conditions: results from the PoCT in General Practice Trial. Med J Aust. 2009 Jun 1;190(11):624–6.
- Bereznicki LRE, Jackson SL, Peterson GM. Supervised patient self-testing of warfarin therapy using an online system. J Med Internet Res. 2013 Jul 12;15(7):e138.
- Stafford L, Peterson GM, Bereznicki LR, Jackson SL, Tienen EC van, Angley MT, et al. Clinical Outcomes of a Collaborative, Home-Based Postdischarge Warfarin Management Service. Ann Pharmacother. 2011 Mar 1;45(3):325–34.
- Toscos T, Coupe A, Wagner S, Ahmed R, Roebuck A, Flanagan M, et al. Engaging Patients in Atrial Fibrillation Management via Digital Health Technology: The Impact of Tailored Messaging. J Innov Card Rhythm Manag. 2020 Aug 1;11(8):4209–17.
- Desteghe L, Klutz K, Vijgen J, Koopman P, Dilling-Boer D, Schurmans J, et al. The Health Buddies App as a Novel Tool to Improve Adherence and Knowledge in Atrial Fibrillation Patients: A Pilot Study. JMIR MHealth UHealth. 2017 Jul 19;5(7):e7420.
- Klimis H, Thakkar J, Chow CK. Breaking Barriers: Mobile Health Interventions for Cardiovascular Disease. Can J Cardiol. 2018 Jul 1;34(7):905–13.
- Piette JD, List J, Rana GK, Townsend W, Striplin D, Heisler M. Mobile Health Devices as Tools for Worldwide Cardiovascular Risk Reduction and Disease Management. Circulation. 2015 Nov 24;132(21):2012–27.
- Pfaeffli Dale L, Dobson R, Whittaker R, Maddison R. The effectiveness of mobile-health behaviour change interventions for cardiovascular disease self-management: A systematic review. Eur J Prev Cardiol. 2016 May;23(8):801–17.
- Gandhi S, Chen S, Hong L, Sun K, Gong E, Li C, et al. Effect of Mobile Health Interventions on the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Can J Cardiol. 2017 Feb;33(2):219–31.
- Cevasco KE, Morrison Brown RE, Woldeselassie R, Kaplan S. Patient Engagement with Conversational Agents in Health Applications 2016-2022: A Systematic Review and Meta-Analysis. J Med Syst. 2024 Apr 10;48(1):40. [CrossRef] [PubMed] [PubMed Central]
- Posadzki P, Mastellos N, Ryan R, Gunn LH, Felix LM, Pappas Y, et al. Automated telephone communication systems for preventive healthcare and management of long-term conditions. Cochrane Database Syst Rev. 2016 Dec 14;2016(12):CD009921.
- Kassavou A, Sutton S. Automated telecommunication interventions to promote adherence to cardio-metabolic medications: meta-analysis of effectiveness and meta-regression of behaviour change techniques. Health Psychol Rev. 2018 Jan 2;12(1):25–42.
- Tsoli S, Sutton S, Kassavou A. Interactive voice response interventions targeting behaviour change: a systematic literature review with meta-analysis and meta-regression. BMJ Open. 2018 Feb 1;8(2):e018974.
- Tudor Car L, Dhinagaran D, Kyaw B, Kowatsch T, Joty S, Theng Y, Atun R. Conversational Agents in Health Care: Scoping Review and Conceptual Analysis. J Med Internet Res 2020;22(8):e17158. [CrossRef]
- . Milne-Ives M, de Cock C, Lim E, Shehadeh M, de Pennington N, Mole G, Normando E, Meinert E. The Effectiveness of Artificial Intelligence Conversational Agents in Health Care: Systematic Review. J Med Internet Res 2020;22(10):e20346. [CrossRef]
- de Cock C, Milne-Ives M, van Velthoven MH, Alturkistani A, Lam C, Meinert E. Effectiveness of Conversational Agents (Virtual Assistants) in Health Care: Protocol for a Systematic Review. JMIR Res Protoc. 2020 Mar 9;9(3):e16934. [CrossRef] [PubMed] [PubMed Central]
- McTear, M. F. (2002). Spoken dialogue technology: Enabling the conversational user interface. ACM Computing Surveys, 34(1), 90–169. [CrossRef]
- Lobo, Joana; Ferreira, Liliana; Ferreira, Aníbal JS (2017). CARMIE. International Journal of E-Health and Medical Communications, 8(4), 21–37. [CrossRef]
- A. Cheng, V. Raghavaraju, J. Kanugo, Y. P. Handrianto and Y. Shang, "Development and evaluation of a healthy coping voice interface application using the Google home for elderly patients with type 2 diabetes," 2018 15th IEEE Annual Consumer Communications & Networking Conference (CCNC), Las Vegas, NV, USA, 2018, pp. 1-5. [CrossRef]
- García Bermúdez I, González Manso M, Sánchez Sánchez E, Rodríguez Hita A, Rubio Rubio M, Suárez Fernández C. Utilidad y aceptación del seguimiento telefónico de un asistente virtual a pacientes COVID-19 tras el alta [Usefulness and acceptance of telephone monitoring by a virtual assistant for patients with COVID-19 following discharge]. Rev Clin Esp. 2021 Oct;221(8):464-467. Spanish. Epub 2021 Feb 5. [CrossRef] [PubMed] [PubMed Central]
- Dorado-Díaz PI, Sampedro-Gómez J, Vicente-Palacios V, Sánchez PL. Applications of Artificial Intelligence in Cardiology. The Future is Already Here. Rev Esp Cardiol (Engl Ed). 2019 Dec;72(12):1065-1075. Epub 2019 Oct 12 . [CrossRef] [PubMed]
- Kulkarni P, Mahadevappa M, Chilakamarri S. The Emergence of Artificial Intelligence in Cardiology: Current and Future Applications. Curr Cardiol Rev. 2022;18(3):e191121198124. [CrossRef] [PubMed] [PubMed Central]
- Ledziński Ł, Grześk G. Artificial Intelligence Technologies in Cardiology. J Cardiovasc Dev Dis. 2023 May 6;10(5):202. [CrossRef] [PubMed] [PubMed Central]
- Pegoraro V, Bidoli C, Dal Mas F, et al. Cardiology in a Digital Age: Opportunities and Challenges for e-Health: A Literature Review. J Clin Med. 2023;12(13):4278. Published 2023 Jun 26. [CrossRef]
- Santamaria A, Antón Maldonado C, Sánchez-Quiñones B, Ibarra Vega N, Ayo González M, Gonzalez Cabezas P, Carrasco Moreno R. Implementing Telemedicine in Clinical Practice in the First Digital Hematology Unit: Feasibility Study. JMIR Form Res. 2023 Dec 4;7:e48987. [CrossRef] [PubMed] [PubMed Central]
- Barrios V, Cinza-Sanjurjo S, García-Alegría J, Freixa-Pamias R, Llordachs-Marques F, Molina CA, Santamaría A, Vivas D, Suárez Fernandez C. Role of telemedicine in the management of oral anticoagulation in atrial fibrillation: a practical clinical approach. Future Cardiol. 2022 Sep;18(9):743-754. Epub 2022 Jul 13. [CrossRef] [PubMed]
- aquero A. Net Promoter Score (NPS) and Customer Satisfaction: Relationship and Efficient Management. Sustainability. 2022; 14(4):2011. [CrossRef]
- Rotella P and Chulani, S. "Analysis of customer satisfaction survey data," 2012 9th IEEE Working Conference on Mining Software Repositories (MSR), Zurich, Switzerland, 2012, pp. 88-97. [CrossRef]
- Fatima B, Mohan A, Altaie I, Abughosh S. Predictors of adherence to direct oral anticoagulants after cardiovascular or bleeding events in Medicare Advantage Plan enrollers with atrial fibrillation. J Manag Care Spec Pharm. 2024 May;30(5):408-419. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Lolatao At A Glance.
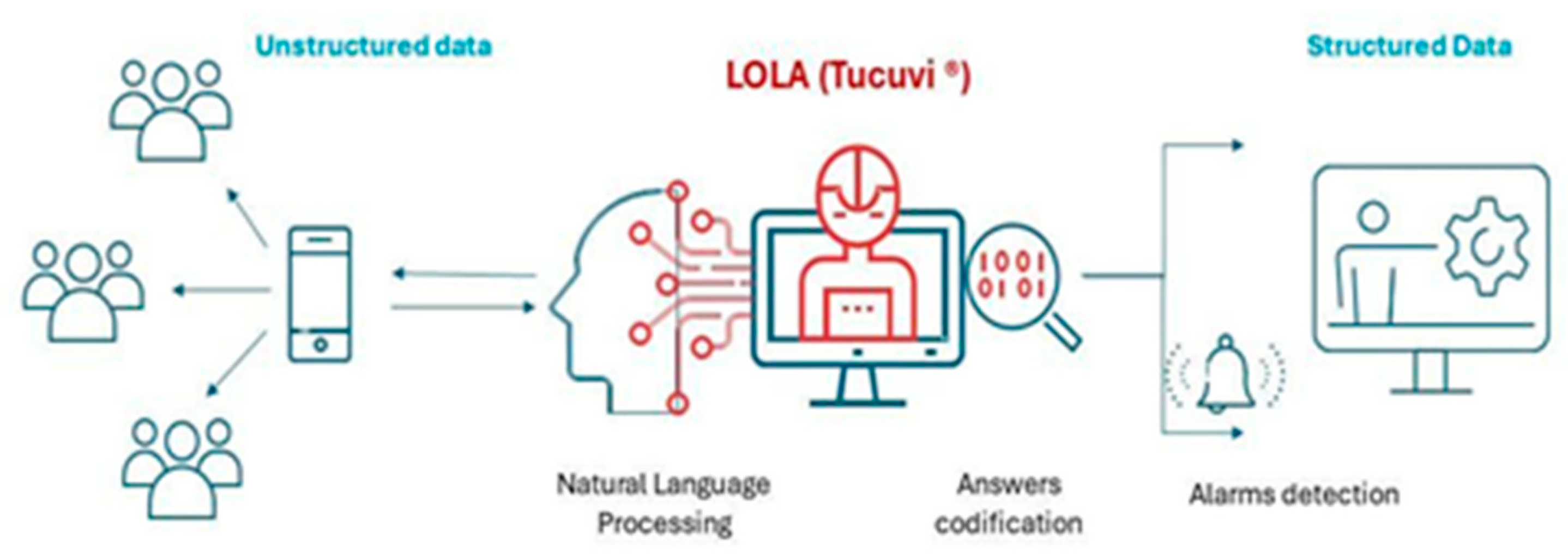
Figure 2.
Study Workflow.
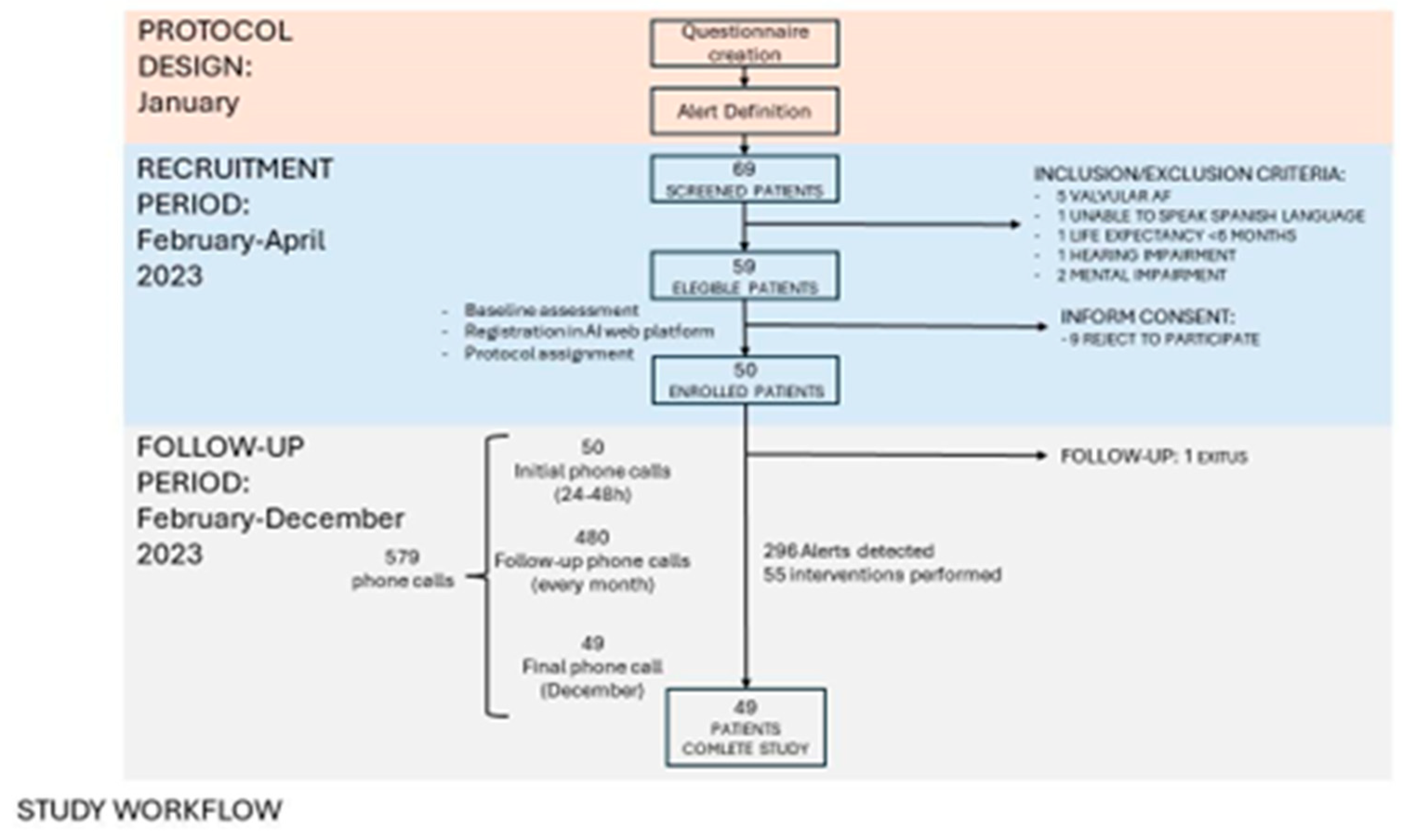

Table 1.
Demographic Characteristics and Type of OAT Treatment.
| Demographics | ||||||
|---|---|---|---|---|---|---|
|
Age (mean, range ) |
AVKs (n=16) | DOACs (n=33) | Total (n=49) | |||
| Male n=12 |
Female n=4 |
Male n=29 |
Female n=11 |
Male n=33 |
Female n=16 |
|
| Type of DOAC (n=33) | ||||||
| Edoxaban (n, %) | 7 (21%) | |||||
| Rivaroxaban (n, %) | 11 (33%) | |||||
| Apixaban (n, %) | 12 (36%) | |||||
| Dabigatran (n, %) | 3 (9%) | |||||
Table 2.
patient and Clinical Outcomes.
| OAT Adherence | ||||
|---|---|---|---|---|
| Medication doses missed | AVKs (n =16) | DOACs (n=33) | Total (n=49) | |
| 0 | 10 (63%) | 18 (55%) | 28 (58%) | |
| 1 | 4 (25%) | 5 (15%) | 9 (18%) | |
| 2 | 1(6%) | 7 (21%) | 8 (16%) | |
| ≥3 | 1(6%) | 3 (9%) | 4 (8%) | |
| Health Events | Concordance (n, %) | |||
| ≥1 Bleeding event | 14 (88%) | 5(15%) | 19(39%) | 19 (100%) |
| Bridging therapy | 1(6%) | 8(24%) | 9(18%) | 9 (100%) |
| Renal function impairment (TFG <60) |
- | 14(42%) | NA | 8 (57%) |
| Unknown TRT | 15(94%) | NA | NA | 15 (100%) |
| TRT <65% | 12(75%) | NA | NA | 9 (75%) |
| Healthcare service use | ||||
| Emergency department | 5(31%) | 12(36%) | 17(35%) | 17 (100%) |
| Hospitalization | 0(0%) | 3(9%) | 3(6%) | 3 (100%) |
Table 3.
Results of Satisfaction Surveys.
| Questionnaire | Result | Explanation |
| CSAT | 4.63/5 | all patients except 1 answered being satisfied or very satisfied with LOLA. 1 patient answered a 3 (neutral) |
| NPS | 44.73% | 38 patients answered this question. Only 5 of them gave a punctuation lower than 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



