
Submitted:
18 August 2025
Posted:
19 August 2025
You are already at the latest version
Abstract
Dementia and mild cognitive impairment (MCI) are growing health concerns in Canada’s aging population. Over 700,000 Canadians currently live with dementia, and this number is expected to rise. As the older adult population increases, coupled with an already strained healthcare system, there is a pressing need for innovative tools that support aging in place. This study explored the feasibility and acceptability of using a Digital Human (DH) conversational agent, combined with AI-driven speech analysis, to monitor cognitive function, anxiety, and depression in adults aged 65 and older with and without MCI. Sixty older adults participated in up to three in-person sessions over six months, interacting with the DH through journaling and picture description tasks. Afterward, 51 of the participants completed structured interviews about their experiences and perceptions of the DH and AI more generally. Findings showed that 84% enjoyed interacting with the DH, and 96% expressed interest in learning more about AI in healthcare. While participants were open and curious about AI, 55% expressed concerns about AI replacing human healthcare providers. Most found the DH friendly, though reactions to its appearance varied. Overall, participants viewed AI as a promising tool, provided it complements, rather than replaces, human interactions.
Keywords:
Digital human
; mild cognitive impairment
; dementia
; healthcare
; older adults
; AI literacy
; remote health monitoring
1. Introduction
Dementia is a chronic condition affecting over 700,000 Canadians [1], and more than 50 million people globally [2]. By 2030, it is projected that approximately 1 million Canadians will be living with dementia, with this number increasing by 65% to an estimated 1.7 million by 2050 [1]. Although less severe than dementia, mild cognitive impairment (MCI) also afflicts a significant portion of the population. However, due to factors such as diagnostic testing used to define MCI, age of assessment and follow-up, published prevalence rates of MCI among Canadians are unavailable [3]. In the United States, the prevalence of MCI among adults aged 70 or older ranges from 9.9% to 35.2% [3]. Canadians are also living longer, with the life expectancy reaching 81.5 years of age as of 2022 [4]. As the older adult population grows, the prevalence of MCI and dementia is expected to rise, increasing the demand for healthcare services and supports [5]. Canada’s population is projected to grow 36% over the next 20 years [6], with older adults comprising approximately a quarter of the total population [7]. The most significant growth is anticipated within the 65-84 and 85+ age groups, driven by the aging Baby Boomer cohort [6,8].
These demographic trends are expected to present significant challenges for the healthcare system. By 2040, over half of individuals aged 65 and older are projected to live with a major illness [6]. Currently, the Canadian healthcare system is under strain, grappling with overcrowded emergency rooms, a shortage of family doctors, and overburdened healthcare workers [9]. Healthcare spending is highest among the older adult population, with expenditures on this demographic increasing by 2.2% over the last decade [10]. The aging population coupled with the challenges faced by the healthcare system underscore the urgent need for innovative health-related tools and technologies that enable timely care and support aging in place. The Government of Canada has committed close to $200 billion CAD over 10 years to improve health services, with a focus on modernizing healthcare through digital tools [9].
AI is increasingly integrating into daily life, including for use in healthcare monitoring. Increased accessibility to smartphones, coupled with Wi-Fi and artificial intelligence (AI), more generally, has transformed the way that individuals monitor their health [11,12]. Remote patient monitoring (RPM) technologies, such as wearable devices, utilize AI to monitor and record physiological data and daily activities, for example [13]. These tools enable healthcare workers to collect real-time, non-urgent medical data, and monitor changes in health over time [13,14,15,16], while also empowering patients to manage their health from the comfort of their own home [17]. The benefits of RPM technologies are multifaceted, including, but not limited to offering patients some autonomy over their health, reducing transportation barriers, side-stepping long-wait times at hospitals and clinics, offering cost-saving benefits for the end-user, and alleviating some pressure on the healthcare system [17,18,19,20,21]. Despite the growing promise of RPM technologies, their full potential remains unrealized due to limited real-world studies and insufficient co-creation with end users. Without meaningful engagement and feedback from those who would use these technologies, their effectiveness in practical settings is not fully understood.
Given the aging population, the projected increases in MCI and dementia, and inefficiencies and challenges within the healthcare system, the demand for effective technologies to maintain and support cognitive health in older adults will continue to grow. Specifically, there is a growing need for innovative tools and technologies that facilitate timely healthcare delivery to older adults, and support aging in place.
The present mixed-methods observational study aimed to address this need through two primary objectives: (1) to investigate the feasibility, acceptability and performance of a Digital Human (DH) conversation agent combined with an AI-driven speech analysis algorithm for monitoring cognitive function, anxiety, and depression in older adults with and without an MCI diagnosis, and (2) to collect qualitative data on participants’ experiences with the DH and their AI-literacy.
2. Materials and Methods
2.1. Participants
Seventy-two community-dwelling older adults (CDOA) were recruited from the research database maintained by the Centre for Elder Research (CER) at Sheridan College in Ontario, Canada, and recruitment notices distributed by community organizations. Twelve participants withdrew or dropped-out prior to the initial in-person visit due to various reasons, including time commitment (n=1), discomfort with audio/video recording (n=1), transportation or distance challenges (n=1), lack of response to follow-up communications (n=7), or undisclosed reasons (n=2). As a result, 60 older adults were enrolled for the baseline in-person assessment. Participant demographics are summarized in Table 1. Eligibility criteria included: 1) being aged 65 or older; 2) feeling comfortable maintaining a conversation in English; and 3) being able to reasonably commit to multiple in-person visits to CER, spaced approximately three months apart over the course of six months. All participants provided written or electronic informed consent using REDCap and were compensated for their participation in the study. The study was approved by Sheridan’s Research Ethics Board (SREB No. 2002-06-005-007).
2.2. In-Person Assessments
Participants visited CER up to three times, approximately every three months over the course of six months. Each visit was approximately 30 minutes. Within two weeks of each in-person visit, participants completed the Patient Health Questionnaire-8 (PHQ-8) and the Generalized Anxiety Disorder questionnaire-7 (GAD-7). PHQ-8 and GAD-7 data is summarized in Table 2. During the in-person visit, the Mini Mental State Exam (MMSE) was administered by the Research Coordinator. Following the MMSE, participants were seated in front of a computer where they interacted with the Digital Human (DH), which guided them through a series of vocal tasks. During each visit, participants completed a journaling task administered by the DH, which is an open-ended prompting question asking participants to describe what they did the day before for up to two minutes. They also answered a one-item general mental health question, rating their current mental health on a scale from “poor” to “excellent”. At baseline and the six-month visit, the DH also asked participants to complete two picture description tasks. Participants were presented with two black-and-white drawings depicting a scenario (ie. living room scene, kitchen scene, restaurant scene), and were asked to describe everything that they saw in the picture for up to two minutes. Audio and video data were collected passively during the entire interaction with the DH.
2.3. Final Interview
Approximately six weeks after completing their final in-person visit, participants were invited to take part in a one-hour structured interview conducted via video or phone call. These interviews collected qualitative data on participants’ experiences and feedback regarding the DH, their familiarity with AI, their level of AI literacy, and their concerns about the use of AI, specifically within healthcare.
3. Results
3.1. In-Person Assessments
Sixty CDOA completed the initial in-person assessment. Following this, three participants withdrew from the study without providing a reason. Of the remaining participants, 54 completed the second assessment, and 13 completed the third assessment. The decline in participation rates, specifically between visit two and three was primarily due to the early termination of the study due to factors outside the control of the researchers. After the initial interaction with the DH, approximately 70% of participants responded positively to the DH (ie. “DH was pleasant and had kind eyes”), 13% had a neutral reaction (ie. “DH was fine”), and 17% had a negative reaction (Ie. “DH was creepy and disconcerting”).
3.2. Final Interview
Fifty-one participants completed the final phone interview about their experience with and opinions of the DH and AI technology, more generally. Participants were asked to rate their answers on a scale from 1 to 5, with 1 meaning the least and 5 meaning the most. Approximately 84% at least somewhat enjoyed interacting with the DH, the entire cohort (100%) felt at least somewhat comfortable interacting with the DH, almost all (96%) found the DH to be at least a little likeable, almost all (90%) are interested in learning to use new technologies, almost all (98%) felt at least a little confident with learning to use new technologies, all (100%) are at least a little interested in AI-related technologies and their applications, while almost all (96%) are interested in learning more about the uses of AI, specifically in healthcare.
When asked to give more detailed answers about their opinions of AI in healthcare, more than half of the cohort (55%) stated they felt a mix of excitement and concern about the increasing use of AI in daily life, while 23% felt more excited than concerned, and 22% felt more concerned than excited. More than half (53%) stated that they would feel uncomfortable if their healthcare provider relied on AI for their medical care, while 27% said they would feel comfortable, and 20% would feel a mix of both. 67% of the cohort thinks that AI in healthcare would lead to better outcomes for patients, 10% thinks it would lead to worse outcomes, 10% think it would not make much of a difference, while 13% felt unsure about the outcomes. A third (35%) of the cohort thinks that AI in healthcare would worsen the personal connection between a patient and their healthcare provider, while 18% believe that personal connection would get better. However, 47% said the connection would either stay the same, or the quality of the connection would depend more on the healthcare provider than on AI. 92% stated that they were interested in learning to use new technologies, with 8% failing to provide a definitive answer. Almost all (96%) stated they were interested in learning more about the uses of AI in fields like healthcare, with 4% failing to provide a definitive answer. These results are summarized in Figure 1, Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6 .
4. Discussion
Canada’s population demographics are shifting, with individuals aged 65 and older outpacing those 20 and younger [22]. This aging population is driving an evolving demand for healthcare services, especially with the projected rise in chronic conditions such as MCI and dementia. This demographic shift underscores the increasing need for targeted healthcare solutions that are non-invasive, engaging and user-friendly to monitor mental health and cognition in older adults. Involving older adults in the design and development of these tools and technologies will help to ensure that they are trustworthy, widely accepted, and tailored to their unique needs. Public knowledge and acceptance of AI in healthcare is evolving. However, older adults exhibit mixed levels of trust in these technologies, and there is limited research on AI literacy among this demographic. Kaur and Chen addressed this gap and found significant variability in AI literacy [23]. Not unlike ethical concerns identified by previous studies [23,24], two-thirds (67%) of our cohort voiced concerns about AI replacing human interaction in healthcare potentially diminishing empathy and increasing social isolation and feelings of loneliness [23]. Roughly 35% of participants believed that AI would worsen the personal connection between patients and doctors, citing distrust in AI, concerns about over-reliance on technology, and the importance of empathy in healthcare interactions. Trust emerged as a central theme influencing perceptions of remote health monitoring (RHM) technologies [25]. As noted by Feldberg [25], concerns around privacy, security, and misuse of personal data were prevalent, with participants noting fears about third-party access, data breaches, and the misuse of. Similarly, the 2022 Pew Research Center survey found that 37% of American adults believe AI in healthcare could worsen the security of patient information [26]. These findings highlight that trust plays a significant emotional role in the acceptance and perceptions of RHM and AI-related technology, like our DH [27]. This suggests that developers of these technologies should prioritize transparency of functions and security of data to build consumer confidence and trust in novel technologies. Despite these reservations, optimism regarding AI’s potential in healthcare persists. Two-thirds (67%) in our cohort believed that AI in healthcare could lead to better patient outcomes, by alleviating some of the burden on healthcare workers, increasing efficiency, and enhancing diagnostic accuracy. This optimism exceeds the 34% of American adults aged 65 and older who shared similar views in the Pew survey [26]. On the other hand, 10% of our cohort thinks AI in healthcare would worsen outcomes, citing concerns about AI’s inability to interpret human nuances in body language and facial expressions, and a preference for human judgement over technology.
Both our study and the Pew survey identified fears that increased reliance on AI might reduce the face-to-face interactions, leadings to feelings of disconnection and depersonalized care. These concerns align with those expressed by users of RHM for chronic conditions, who worry about being “lost in data” and losing personalized healthcare [28]. Some participants in our study expressed strong opposition to interacting with a DH when it relates to their healthcare. For example, when asked about one's thoughts about interacting with a DH for the purpose of remote health monitoring, Participant 025 shared, “I am getting close to 70 years old, and I am dealing with health issues. I want to talk to a real human. I want personal care. I am not interested in AI healthcare. Maybe I would feel differently if I was 20 or 30.” To improve acceptance and perceived usefulness of DH platforms, public education and awareness of AI in healthcare must be enhanced, especially if they are to be adopted into daily life or home use.
The differences in attitudes toward AI in healthcare between our study and the Pew survey may speak to the differences in healthcare systems and access to healthcare between Canada and the United States (US). While Canadian healthcare is publicly funded [29], access to timely care remains a significant challenge. In 2023, only 26% of Canadians reported securing same- or next-day appointments with their healthcare provider, and approximately one in five lack a regular primary healthcare provider [30,31]. Wait-times are especially problematic for those 65 and older compared to other Commonwealth countries [32]. Canadians also reported the longest wait times for specialist care among Commonwealth countries, with 62% waiting one month or more to see a specialist [31,33]. Comparatively, the US healthcare system is predominantly privately funded, with the National Medicare program providing coverage for people 65 and older [34]. In 2023, 38% of Americans reported securing a same- or next-day appointment with their healthcare provider [30]. Only 31% reported waiting a month or more for a specialist appointment, about half the rate reported by Canadians [33]. These differences in healthcare access may influence attitudes towards AI-based technologies in healthcare. Canadians, facing longer wait-times and limited access to primary care, may be more receptive to screening tools, like the DH platform, which could provide more immediate healthcare services and alleviate wait-times. By addressing barriers to healthcare access, AI-related tools could enhance the overall healthcare experience for Canadians. Additionally, Feldberg [25] observed a disconnect between older adult’s recognition of the general benefits of RHM technologies and the personal benefits. Perception biases play a role in the adoption of RHM technologies where potential users may fail to see a potential need for the technology. Health status was a key factor in recognizing the personal value of RHM [25,35]. Therefore, the perceived benefit of a DH as a screening tool for mental health and cognitive decline may l increase acceptance and adoption of the technology in populations with strained access to healthcare, as it addresses immediate healthcare needs.
Kaur and Chen found that many older adults expressed interest in learning more about AI to make informed decisions about AI-enabled products and services [23]. Our findings reflect this trend, with 92% of participants expressing interest in learning to use new technologies, and 96% wanting to explore AI applications in healthcare. Motivations included staying current with technological advancements, maintaining autonomy over their own healthcare, recognizing AI’s benefits for aging populations, and general curiosity about AI developments. Contrary to assumptions that older adults’ technological concerns would hinder the adoption of home telemedicine services and RHM technologies, our findings suggest otherwise [25,28,36]. Our findings are congruent with those of Feldberg [25], where participants expressed high levels of confidence and trust in learning to use new technologies like the DH platform. Despite the physical and cognitive barriers to technology adoption, such as mobility challenges, unclear instructions, limited customer support, short-term memory changes, and poor interface design, participants maintained a strong interest in adopting new technologies. However, the Dunning-Kruger effect should be considered, as older adults may overestimate their ability to handle novel technologies [37]. Future research should test the DH platform in real-world, uncontrolled environments to better assess the feasibility, usability and acceptance. This approach will help identify unforeseen challenges that may not be captured in a lab setting and provide more accurate insights into users’ experiences and potential barriers in everyday use.
AI in healthcare holds significant potential for supporting independent living, enhancing autonomy over health, and improving well-being and quality of life for older adults. However, realizing these benefits requires a concerted effort to increase AI literacy within this population. Tailored AI literacy programs, educational initiatives, and supportive resources can bridge this gap. Furthermore, designing user-friendly interfaces can enhance the usability and acceptance of AI-enabled technologies, apps, and services ensuring they meet the specific needs of older adults.
Digital tools, like the DH paired with the speech analysis technology, could support aging in place. Although many participants expressed concerns about AI diminishing human interaction with healthcare providers, there already exist numerous health-related tools, technologies and apps to support aging in place. For example, smartphones and mobile health apps, which utilize AI, play an important role in RHM for older adults [38]. A study of CDOA found mixed acceptance of the usefulness of technologies that support aging in place [39]. They preferred technologies that improve mobility and safety, or reduce cognitive decline, whereas others did not perceive such technologies as useful tools to help them remain at home [39]. Three-quarters of our participants indicated they would prefer accessing the DH from home rather than visiting a community testing site already part of their routine, citing privacy, convenience and accessibility. These findings highlight how perceptions of usefulness across groups varies depending on the type of technology and the specific concerns it addresses.
Integrating the DH into RHM could address barriers such as limited access to healthcare professionals, long wait times, and mobility or transportation challenges. A 2015 study on remote patient monitoring systems for older adults living in rural areas, found that perceived usefulness, ease of use and behavioural intention remained stable and high, with acceptance increasing over time [40]. That is, as users became more familiar with the technology, they believed others in their lives would also benefit from it, highlighting the importance of social factors in technology adoption [40]. This finding was mirrored in our study, where many participants reported that they had never interacted with a DH. Nonetheless, approximately 84% at least somewhat enjoyed interacting with the DH, the entire cohort felt at least somewhat comfortable with the interaction, and 96% found the DH at least a little likeable. These findings suggest that acceptability may increase with repeated exposure. For example, during a phone interview, Participant 002 reflected on how her perception of the DH evolved over time, stating, “either [Sam] changed, or I adapted to Sam. I became more comfortable over the course of the visits [to the Centre].” This highlights the importance of habituation when understanding how older adults accept and adopt new technologies.
Participants also provided feedback on the appearance of the DH, emphasizing a preference for a DH that closely resembles them in terms of age, gender, and most notably, ethnicity. In particular, Participant 058 highlighted the importance of ethnic concordance, especially when the DH is intended for use within marginalized communities, such as Indigenous populations. This aligns with existing research that has found that when given the choice, patients often prefer healthcare providers who share their racial or ethnic background [48,49,50]. A growing body of research also supports the race concordance hypothesis with mental health care, whereby racially minoritized patients who are matched with mental health providers of a similar racial or ethnic background report greater satisfaction, perceive higher quality of care, and overall experience better health outcomes [51,52,53,54,55]. These findings suggest that a racially concordant DH may yield similar positive effects. Race concordance, especially among racially minoritized patients, has been associated with improved communication, enhanced perceptions of care, better health outcomes, and increased trust in providers [49,56,57]. Additionally, participant feedback regarding the customizability of the DH is valuable and aligns with prior research indicating that patients find it easier to build a close relationship with racially concordant mental health providers, which fosters greater trust, mutual respect, positive affect, and overall greater satisfaction [49,55,56,57]. Taken together, these insights underscore the importance of incorporating user preferences into the design of a DH to enhance its acceptability. Enabling patients to select or customize their DH may foster greater trust and higher adoption rates, particularly among older adults and racially minoritized groups.
A key limitation of our study was the inclusion of primarily cognitively healthy older adults, which constrained our ability to validate the speech analysis technology as a tool for detecting cognitive decline over time. Nearly all participants scored 26 or higher on the MMSE across all visits indicating no cognitive impairments within the cohort. During the eligibility screening, two participants self-reported an MCI diagnosis. However, both scored within the normal range on the MMSE. Conversely, one participant, who scored 22 on the MMSE during their initial assessment did not self-report an MCI diagnosis during screening. These discrepancies underscore the limitations of the MMSE. While widely used as a screening tool [41], the MSSE primarily assesses only basic memory, attention, language and visuospatial function [42]. It has limited sensitivity to detecting early-stage dementia, especially MCI, or the breadth of cognitive decline experienced by those living with milder forms of cognitive impairments [41,42]. Although the MMSE is the most common screening tool for dementia, and is quick and easy to administer, future studies could explore the use of more robust screening tools for MCI and dementia, such as The Addenbrooke’s Cognitive Examination (ACE-III) [43,44], or The Montreal Cognitive Assessment (MoCA). The MOCA is a validated tool, and evaluates eight areas of cognition, including executive function, which the MMSE does not address [45]. It is reliable and has demonstrated higher sensitivity for detecting MCI and AD and is recommended by the Alzheimer’s society for clinical use [46,47]. For example, the MoCA was found to be better than the MMSE in the detection of MCI among those 60 and older [45], and it has higher specificity in identifying 87% of healthy controls [45]. While our study was not conducted in a clinical setting, using more sensitive screening tools could better support the validation of the speech analysis program as a non-invasive tool for detecting cognitive decline and impairment in older adults.
The relatively high cognitive functioning of our cohort also limits the generalizability of our findings to the broader older adult population, especially those living with MCI or dementia. For example, upwards of three-quarters of our cohort responded positively to their first interaction with the DH, with 88% reporting that they at least somewhat enjoyed the experience, and the entire cohort feeling at least somewhat comfortable interacting with the DH. However, these results cannot be extended to individuals living with cognitive impairments. Notably, some participants descried the DH as disconcerting, lacking empathy, or “looking through” them, which may elicit stronger negative reactions in those living with cognitive impairments. Therefore, future studies should consider including participants with MCI as an eligibility requirement to assess the acceptance and usability of this technology within this population. This approach would provide more nuanced insights into the potential for the DH and speech analysis program to support individuals living with cognitive impairments and facilitate their integration into everyday care practices.
5. Conclusions
As chronic conditions like dementia become more prevalent, developing non-invasive, home-based technologies are essential for improving healthcare access, and enabling early interventions. RHM technologies, like the DH platform, offer practical solutions for early detection and intervention to improve patient outcomes, support aging in place, and alleviate pressures on healthcare systems. Designing healthcare technologies that meet the unique needs of older adults, and incorporating end-user feedback is essential in creating tools that are not only effective, but also widely accepted by the population they are designed to serve.
Author Contributions
Conceptualization, E.C., C.S. and L.T.; formal analysis, I.P.; funding acquisition, C.S. and L.T.; investigation, I.P.; Methodology, E.C., C.S. and L.T.; project administration, I.P. and L.T.; resources, I.P. and L.T.; supervision, L.T.; visualization, I.P.; writing – original draft, I.P.; writing – review and editing, I.P., C.S. and L.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded in part by the Ontario Brain Institute.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Sheridan Research Ethics Board (SREB), Sheridan College, SREB No 2022-06-005-007, dated April 13, 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request. Due to the multi-phase nature of the study and the involvement of community partners, the dataset requires contextual understanding to ensure accurate interpretation. As such, we ask that interested researchers contact the authors to discuss the study protocol and data structure prior to data sharing.
Conflicts of Interest
The funders contributed to the co-development of the study design and protocol. The funders had no role in the collection of data, analysis or interpretation of data, and they did not engage with the participants in any way. The funders reviewed the manuscript.
References
- Dementia numbers in Canada. Available online: https://alzheimer.ca/en/about-dementia/what-dementia/dementia-numbers-canada (accessed on 5 November 2024).
- Global Dementia Observatory (GDO). Available online: https://www.who.int/data/gho/data/themes/global-dementia-observatory-gdo (accessed on 30 October 2024).
- Cognitive Impairment—Clinician Summary. Available online: https://canadiantaskforce.ca/cognitive-impairment-clinician-summary/ (accessed on 29 October 2024).
- Life expectancy and other elements of the complete life table, three-year estimates, Canada, all provinces except Prince Edward Island. [CrossRef]
- Dementia: Overview. Available online: https://www.canada.ca/en/public-health/services/diseases/dementia.html (accessed on 23 October 2024).
- Projected patterns of illness in Ontario. In Dalla Lana School of Public Health. Available online: https://pophealthanalytics.com/wp-content/uploads/2024/10/Study-Projected-Patterns-of-Illness-in-Ontario-Released-October-16-Final.pdf (accessed on 7 November 2024).
- Aging and chronic diseases: A profile of Canadian seniors. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/aging-chronic-diseases-profile-canadian-seniors-report.html (accessed on 26 February 2024).
- Population projections for Canada (2021 to 2068), provinces and territories (2021 to 2043). Available online: https://www150.statcan.gc.ca/n1/pub/91-520-x/91-520-x2022001-eng.htm (accessed on 20 October 2024).
- Strengthening the Health Care System in Canada. Available online: https://www.canada.ca/en/health-canada/news/2024/07/strengthening-the-health-care-system-in-canada.html (accessed on 30 October 2024).
- National health expenditure trends, 2024—Infographics. Available online: https://www.cihi.ca/en/national-health-expenditure-trends-2024-infographics#has (accessed on 4 December 2024).
- Rathbone, A.L.; Prescott, J. The use of mobile apps and SMS messaging as physical and mental health interventions: Systematic review. J. Med. Internet Res. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.L.; Mack, E.; Namanya, J. Mobile phones and mental well-being: Initial evidence suggesting the importance of staying connected to family in rural, remote communities in Uganda. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Serrano, L.P.; Maita, K.C.; Avila, F.R.; Torres-Guzman, R.A.; Garcia, J.P.; Eldaly, A.S.; Haider, C.R.; Felton, C.L.; Paulson, M.R.; Maniaci, M.J.; et al. Benefits and challenges of remote patient monitoring as perceived by health care practitioners: A systematic review. Permanente J. 2023, 27, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Lakkireddy, D.R.; Chung, M.K.; Deering, T.F.; Gopinathannair, R.; Albert, C.M.; Epstein, L.M.; Harding, C.V.; Hurwitz, J.L.; Jeffery, C.C.; Krahn, A.D.; et al. Guidance for rebooting electrophysiology through the COVID-19 pandemic. Heart Rhythm 2020, 17, e242–e254. [Google Scholar] [CrossRef]
- Wootton, R. Twenty years of telemedicine in chronic disease management – An evidence synthesis. J. Telemed. Telecare 2012, 18, 211–220. [Google Scholar] [CrossRef]
- Majumder, S.; Mondal, T.; Deen, M. Wearable sensors for remote health monitoring. Sensors 2017, 17. [Google Scholar] [CrossRef]
- Deen, M.J. Information and communications technologies for elderly ubiquitous healthcare in a smart home. Pers. Ubiquitous Comput. 2015, 19, 573–599. [Google Scholar] [CrossRef]
- Becker, S.; Miron-Shatz, T.; Schumacher, N.; Krocza, J.; Diamantidis, C.; Albrecht, U. MHealth 2.0: Experiences, possibilities, and perspectives. JMIR Mhealth Uhealth 2014, 2. [Google Scholar] [CrossRef]
- Martín, J.A.C.; Martínez-Pérez, B.; De La Torre-Díez, I.; López-Coronado, M. Economic impact assessment from the use of a mobile app for the self-management of heart diseases by patients with heart failure in a Spanish region. J. Med. Syst. 2014, 38. [Google Scholar] [CrossRef]
- Luxton, D.D.; Hansen, R.N.; Stanfill, K. Mobile app self-care versus in-office care for stress reduction: A cost minimization analysis. J. Telemed. Telecare 2014, 20, 431–435. [Google Scholar] [CrossRef]
- Nghiem, N.; Leung, W.; Cleghorn, C.; Blakely, T.; Wilson, N. Mass media promotion of a smartphone smoking cessation app: Modelled health and cost-saving impacts. BMC Public Health 2019, 19. [Google Scholar] [CrossRef] [PubMed]
- An Aging World: 2015. Available online: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf (accessed on 24 April 2024).
- Kaur, A.; Chen, W. Exploring AI literacy among older adults. Stud. Health Technol. Inform. 2023. [Google Scholar] [CrossRef]
- Chan, A.; Cohen, R.; Robinson, K.; Bhardwaj, D.; Gregson, G.; Jutai, J.W.; Millar, J.; Rincón, A.R.; Fekr, A.R. Evidence and user considerations of home health monitoring for older adults: Scoping review. JMIR Aging 2022, 5. [Google Scholar] [CrossRef]
- Feldberg, R. Understanding older adults’ perceptions towards use of remote health monitoring through smart health devices. Master’s Thesis, University of Twente, Enschede, The Netherlands, 2022. [Google Scholar]
- 60% of Americans would be uncomfortable with provider relying on AI in their own health care. Available online: https://www.pewresearch.org/science/2023/02/22/60-of-americans-would-be-uncomfortable-with-provider-relying-on-ai-in-their-own-health-care/ (accessed on 1 December 2024).
- Yang, H.; Lee, H.; Zo, H. User acceptance of smart home services: An extension of the theory of planned behavior. Ind. Manag. Data Syst. 2017, 117, 68–89. [Google Scholar] [CrossRef]
- Walker, R.C.; Tong, A.; Howard, K.; Palmer, S.C. Patient expectations and experiences of remote monitoring for chronic diseases: Systematic review and thematic synthesis of qualitative studies. Int. J. Med. Inform. 2019, 124, 78–85. [Google Scholar] [CrossRef]
- Health Canada Act. Available online: https://www.canada.ca/en/health-canada/services/health-care-system/canada-health-care-system-medicare/canada-health-act.html (accessed on 7 December 2024).
- International survey shows Canada lags behind peer countries in access to primary health care. Available online: https://www.cihi.ca/en/international-survey-shows-canada-lags-behind-peer-countries-in-access-to-primary-health-care (accessed on 7 December 2024).
- Duong, D.; Vogel, L. National survey highlights worsening primary care access. CMAJ 2023, 195, E592–E593. [Google Scholar] [CrossRef]
- Doty, M.M.; Shah, A.; Fields, K.; FitzGerald, M.; Williams, R.D., II. Comparing Nations on Timeliness and Coordination of Health Care; Commonwealth Fund: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Canadian Institute for Health Information. How Canada Compares: Results from the Commonwealth Fund’s 2020 International Health Policy Survey of the General Population in 11 Countries; CIHI: Ottawa, ON, Canada, 2021. [Google Scholar]
- Ross University School of Medicine. US vs. Canadian Healthcare: What is the Difference? Available online: https://medical.rossu.edu/about/blog/us-vs-canadian-healthcare (accessed on 7 December 2024).
- Ghorayeb, A.; Comber, R.; Gooberman-Hill, R. Older adults’ perspectives of smart home technology: Are we developing the technology that older people want? Int. J. Hum.-Comput. Stud. 2020, 147, 102571. [Google Scholar] [CrossRef]
- Cimperman, M.; Brenčič, M.M.; Trkman, P.; De Leonni Stanonik, M. Older adults’ perceptions of home telehealth services. Telemed. J. E-Health 2013, 19, 786–790. [Google Scholar] [CrossRef]
- Kruger, J.; Dunning, D. Unskilled and unaware of it: How difficulties in recognizing one’s own incompetence lead to inflated self-assessments. J. Pers. Soc. Psychol. 1999, 77, 1121–1134. [Google Scholar] [CrossRef]
- Dupuis, K.; Tsotsos, L.E. Technology for remote health monitoring in an older population: A role for mobile devices. Multimodal Technol. Interact. 2018, 2. [Google Scholar] [CrossRef]
- Verloo, H.; Kampel, T.; Vidal, N.; Pereira, F. Perceptions about technologies that help community-dwelling older adults remain at home: Qualitative study. J. Med. Internet Res. 2020, 22. [Google Scholar] [CrossRef]
- Giger, J.T.; Pope, N.D.; Vogt, H.B.; Gutierrez, C.; Newland, L.A.; Lemke, J.; Lawler, M.J. Remote patient monitoring acceptance trends among older adults residing in a frontier state. Comput. Hum. Behav. 2014, 44, 174–182. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state. ” J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Devenney, E.; Hodges, J.R. The Mini-Mental State Examination: Pitfalls and limitations. Pract. Neurol. 2016, 17, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.; Schubert, S.; Hoon, C.; Mioshi, E.; Hodges, J.R. Validation of the Addenbrooke’s Cognitive Examination III in frontotemporal dementia and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2013, 36, 242–250. [Google Scholar] [CrossRef]
- Mathuranath, P.; Nestor, P.; Berrios, G.; Rakowicz, W.; Hodges, J. A brief cognitive test battery to differentiate Alzheimer’s disease and frontotemporal dementia. Neurology 2000, 55, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Dautzenberg, G.; Lijmer, J.; Beekman, A. Diagnostic accuracy of the Montreal Cognitive Assessment (MoCA) for cognitive screening in old age psychiatry. Int. J. Geriatr. Psychiatry 2019, 35, 261–269. [Google Scholar] [CrossRef]
- Ciesielska, N.; Sokołowski, R.; Mazur, E.; Podhorecka, M.; Polak-Szabela, A.; Kędziora-Kornatowska, K. Is the MoCA test better suited than the MMSE in MCI detection among people aged over 60? Psychiatr. Pol. 2016, 50, 1039–1052. [Google Scholar] [CrossRef]
- Cooper-Patrick, L. Race, gender, and partnership in the patient-physician relationship. JAMA 1999, 282. [Google Scholar] [CrossRef]
- Gray, B.; Stoddard, J.J. Patient-physician pairing: Does racial and ethnic congruity influence selection of a regular physician? J. Community Health 1997, 22, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Taggart, S.H.; Komaromy, M.; Bindman, A.B. Do patients choose physicians of their own race? Health Aff. 2000, 19, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.H.; Hampton, C.; Brandon, W.P. Physicians, physician extenders and health outcomes: Race, gender and patient-health provider concordance. J. Health Care Poor Underserved 2018, 29, 530–555. [Google Scholar] [CrossRef] [PubMed]
- Meyer, O.L.; Zane, N. The influence of race and ethnicity in clients’ experiences of mental health treatment. J. Community Psychol. 2013, 41, 884–901. [Google Scholar] [CrossRef]
- Alizadeh, S.; Chavan, M. Cultural competence dimensions and outcomes: A systematic review of the literature. Health Soc. Care Community 2015, 24, e117–e130. [Google Scholar] [CrossRef]
- Alegría, M.; Roter, D.L.; Valentine, A.; Chen, C.; Li, X.; Lin, J.; Rosen, D.; Lapatin, S.; Normand, S.-L.; Larson, S.; et al. Patient–clinician ethnic concordance and communication in mental health intake visits. Patient Educ. Couns. 2013, 93, 188–196. [Google Scholar] [CrossRef]
- Nazione, S.; Perrault, E.K.; Keating, D.M. Finding common ground: Can provider-patient race concordance and self-disclosure bolster patient trust? J. Racial Ethn. Health Disparities 2019, 6, 962–972. [Google Scholar] [CrossRef]
- Moore, C.; Coates, E.; Watson, A.; de Heer, R.; McLeod, A.; Prudhomme, A. Correction to: “It’s important to work with people that look like me.” J. Racial Ethn. Health Disparities 2022. [CrossRef]
- van Ryn, M. Research on the provider contribution to race/ethnicity disparities in medical care. Med. Care 2002, 40 (Suppl), I–140–I–151. [Google Scholar] [CrossRef]
Figure 1.
Pie chart illustrating participant responses to the question: “Would you say you are more excited than concerned about the increasing use of AI in daily life, more concerned than excited, or a mix of both? Why do you feel that way?”.
Figure 1.
Pie chart illustrating participant responses to the question: “Would you say you are more excited than concerned about the increasing use of AI in daily life, more concerned than excited, or a mix of both? Why do you feel that way?”.
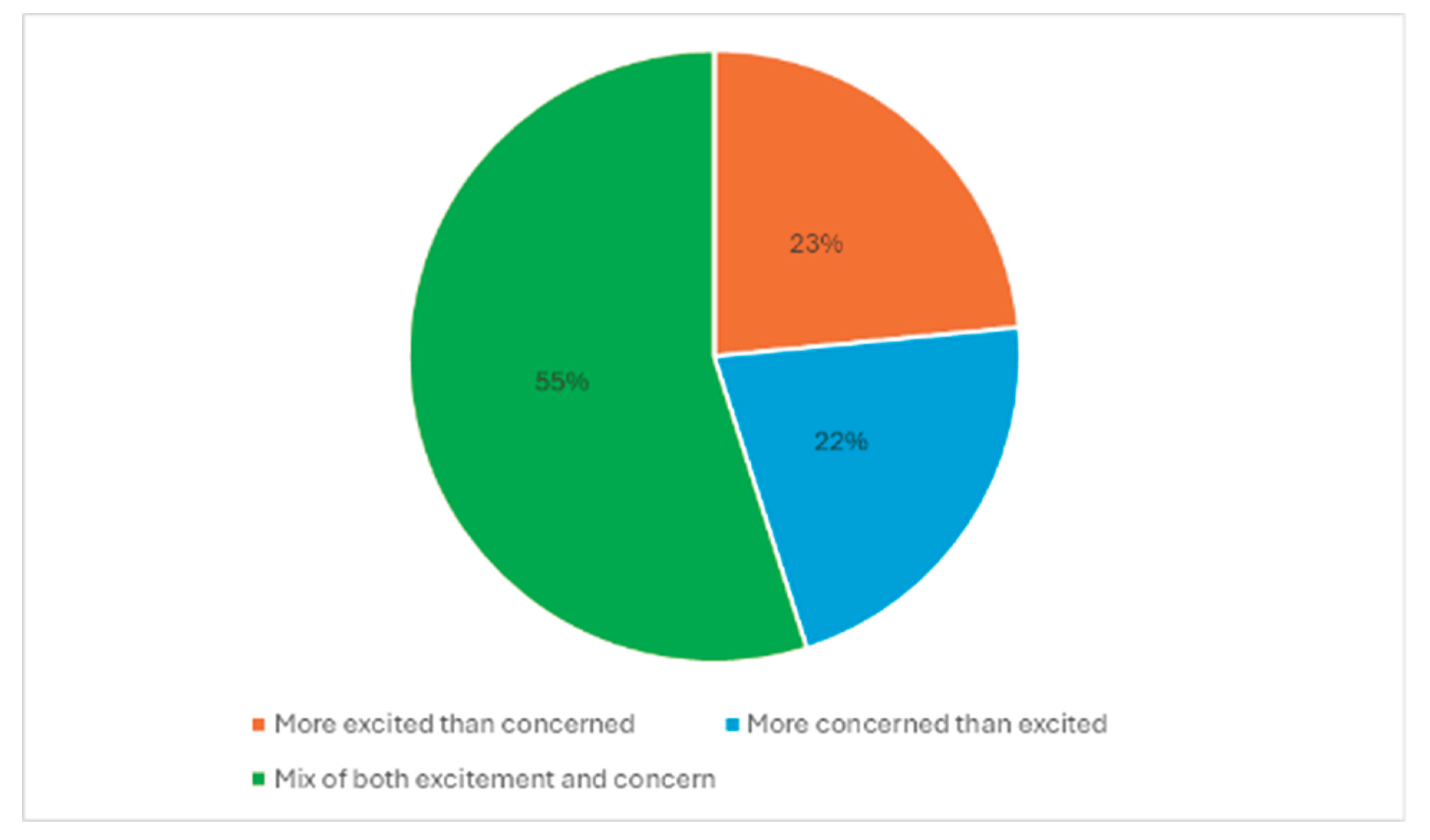
Figure 2.
Pie chart illustrating participant responses to the question: “Would you feel comfortable if your healthcare provider relied on AI for your medical care, or would you say you would be uncomfortable? Why do you feel that way?”.
Figure 2.
Pie chart illustrating participant responses to the question: “Would you feel comfortable if your healthcare provider relied on AI for your medical care, or would you say you would be uncomfortable? Why do you feel that way?”.
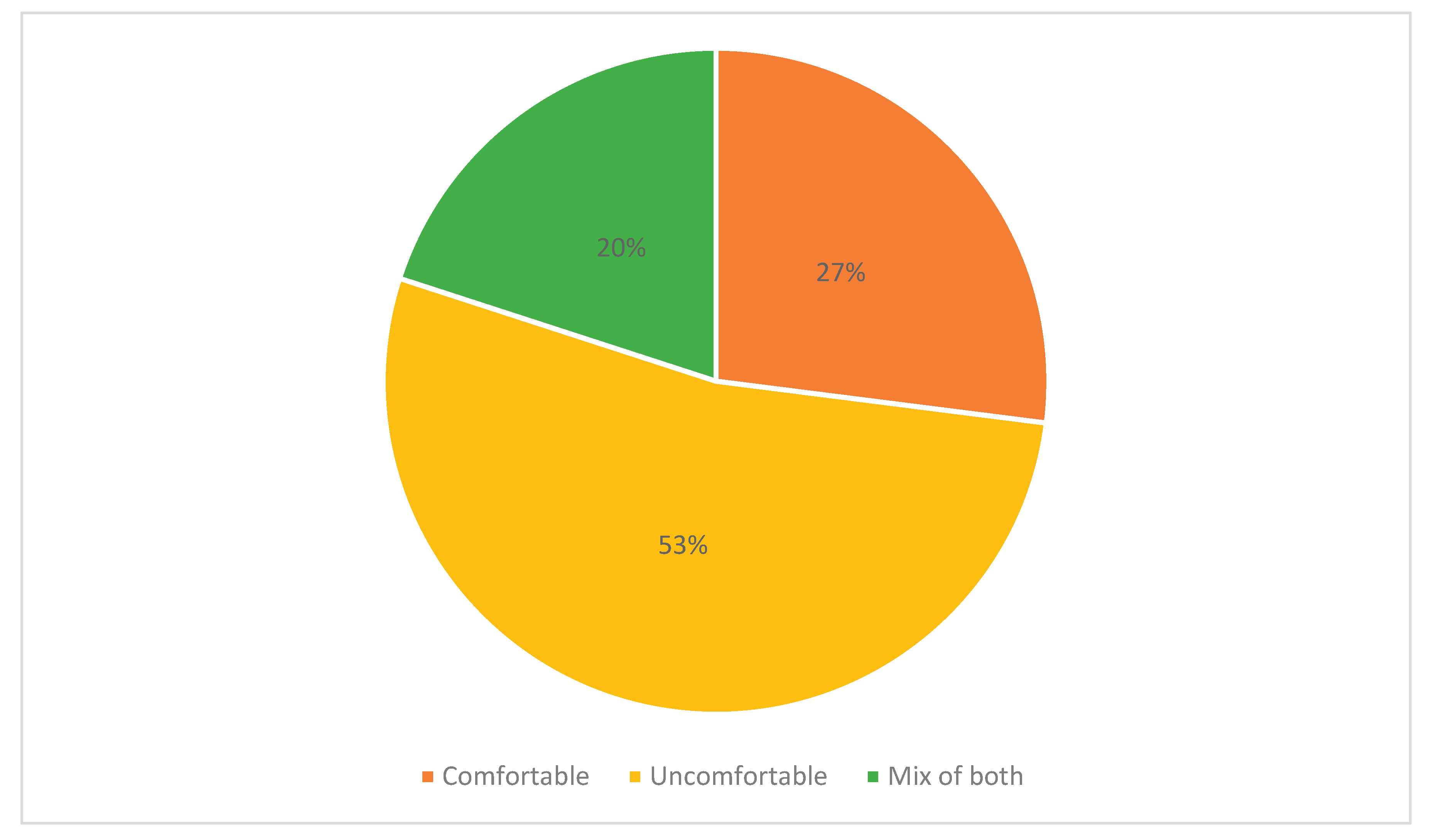
Figure 3.
Pie chart illustrating participant responses to the question: “Do you think AI in health care would lead to better outcomes for patients, worse outcomes, or it wouldn’t make much difference? Why do you feel that way?”.
Figure 3.
Pie chart illustrating participant responses to the question: “Do you think AI in health care would lead to better outcomes for patients, worse outcomes, or it wouldn’t make much difference? Why do you feel that way?”.
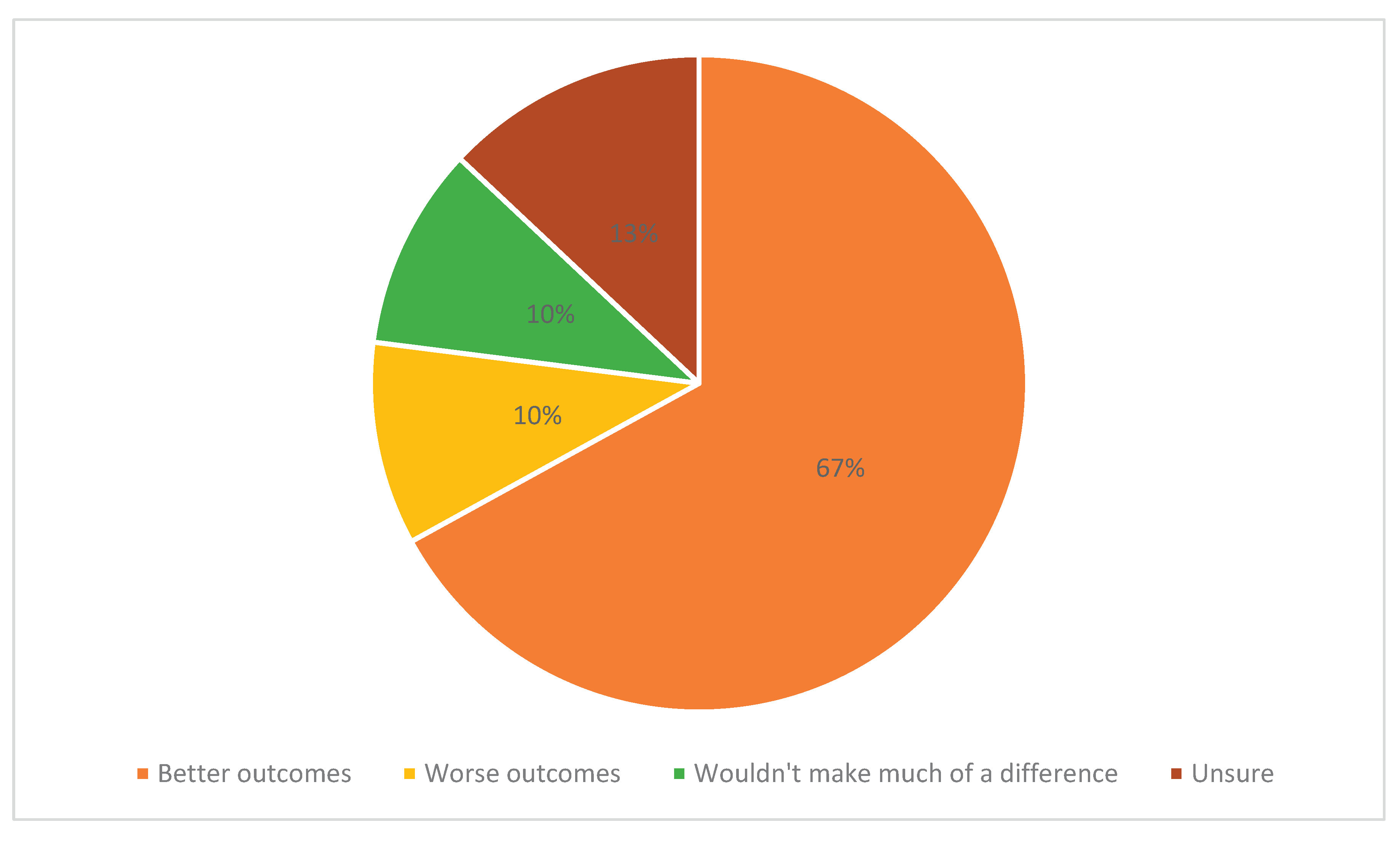
Figure 4.
Pie chart illustrating participant responses to the question: “How do you think AI would impact the personal connection between a patient and their healthcare provider? Would it get worse, get better or stay the same? Why do you feel that way?”.
Figure 4.
Pie chart illustrating participant responses to the question: “How do you think AI would impact the personal connection between a patient and their healthcare provider? Would it get worse, get better or stay the same? Why do you feel that way?”.
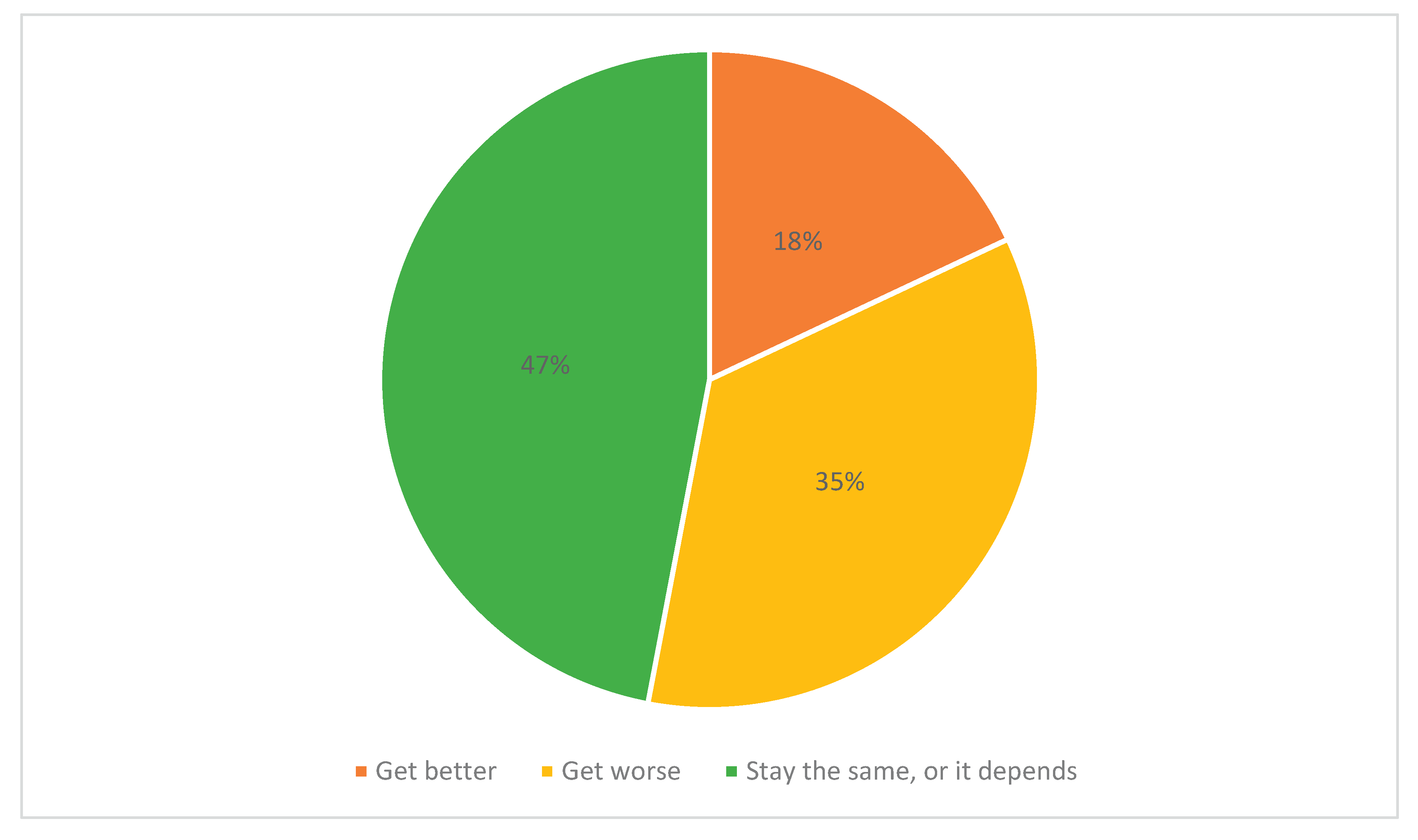
Figure 5.
Pie chart illustrating participant responses to the question: “Are you interested in learning to use new technologies?”.
Figure 5.
Pie chart illustrating participant responses to the question: “Are you interested in learning to use new technologies?”.

Figure 6.
Pie chart illustrating participant responses to the question: “Are you interested in learning more about the uses of AI in fields like healthcare?”.
Figure 6.
Pie chart illustrating participant responses to the question: “Are you interested in learning more about the uses of AI in fields like healthcare?”.

Table 1.
Participant demographics.
| In-person assessments (n=60) | Follow-up phone interview (n=54) | |
|---|---|---|
| Age (years) | 75.0 ± 6.2 | 74.8 ± 6.4 |
|
Gender (%) Male Female |
30 70 |
28 72 |
|
Ethnicity (%) Arabic (Middle East, North Africa) Black (e.g., African, American, Caribbean, etc.) Latin American (e.g., Mexican, Chilean, Costa Rican, etc.) South Asian (e.g., East Indian, Pakistani, Sri Lankan, Bangladeshi, etc.) White I would like to specify an identity not listed |
2.0 1.7 1.7 3.3 86.7 5.0 |
1.9 1.9 1.9 3.7 85.2 5.6 |
|
Education (%) High school College diploma University degree Post graduate degree Other |
6.7 31.7 35.0 20.0 6.7 |
7.4 27.8 38.9 18.5 7.4 |
Table 2.
PHQ-8 and GAD-7 Summary Data.
| Patient Health Questionnaire (PHQ-8) Total Score |
Generalized Anxiety Disorder Questionnaire (GAD-7) Total Score |
||
|---|---|---|---|
| Visit 1 | Minimum | 0 | 0 |
| Maximum | 16 | 21 | |
| Mean | 3.25 | 2.79 | |
| Standard Deviation | 3.26 | 3.94 | |
| Visit 2 | Minimum | 0 | 0 |
| Maximum | 16 | 18 | |
| Mean | 3.11 | 2.60 | |
| Standard Deviation | 3.11 | 3.31 | |
| Visit 3 | Minimum | 0 | 0 |
| Maximum | 7 | 6 | |
| Mean | 2.67 | 1.53 | |
| Standard Deviation | 2.26 | 1.92 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



