Submitted:
11 November 2025
Posted:
13 November 2025
You are already at the latest version
Abstract
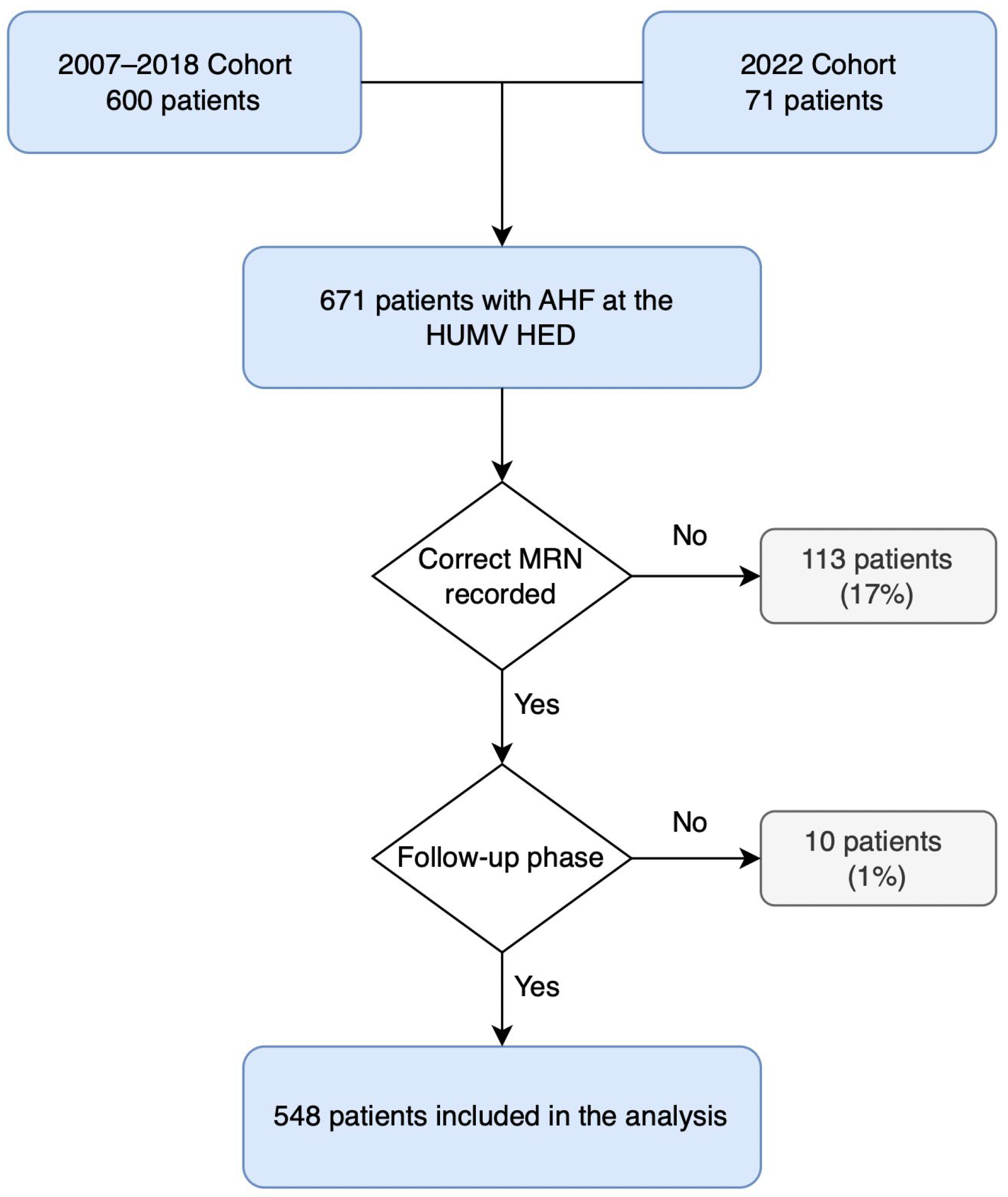
Background/Objectives: Acute heart failure (AHF) is a common cause of hospitalization in older adults, associated with high morbidity and mortality. In this population, frailty, comorbidity, and functional variability significantly influence prognosis. This study evaluated short-term (30-day) and long-term (1-year) mortality predictors in elderly patients with AHF treated in the emergency department (HED), considering clinical variables, comorbidities, and precipitating factors (PFs). Materials and Methods: An observational cohort study was conducted based on a secondary analysis of older patients with AHF included in the Epidemiology of Acute Heart Failure in Emergency Departments (EAHFE) registry, treated at Hospital Universitario Marqués de Valdecilla (HUMV) between 2007 and 2022. Clinical, laboratory, and PF-related variables were collected. The primary outcome was all-cause mortality at 30 days and 1 year. Univariate and multivariate logistic regression analyses were performed. Results: A total of 548 patients were included (mean age: 80.7 years), of whom 78.6% required hospitalization, mainly in the Internal Medicine department. Mortality was 11.1% at 30 days and 29.9% at 1 year. Age, valvular heart disease, dementia, and elevated creatinine levels were independently associated with higher mortality. Hypoxemia and low-output symptoms were linked to short-term mortality, while NYHA class III and anemia were associated with long-term mortality. Among PFs, acute coronary syndrome (ACS) was related to worse short-term outcomes, whereas rapid atrial fibrillation (AF) was inversely associated with long-term mortality. Conclusions: The prognostic relevance of risk factors differs between short- and long-term outcomes in older patients with AHF. Incorporating clinical characteristics and PFs into risk stratification models may support individualized management and guide follow-up strategies tailored to the geriatric profile. This multidimensional approach is essential to improve clinical decision-making and outcomes in a highly vulnerable population.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Study Variables
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Clinical Profile of the Cohort
3.2. In-Hospital Course and Mortality
3.3. Prognostic Factors for Mortality
3.3.1. Univariate Analysis of 30-Day Mortality
3.3.2. Univariate Analysis of 12-Month Mortality
3.4. Multivariable Analysis of Prognostic Factors
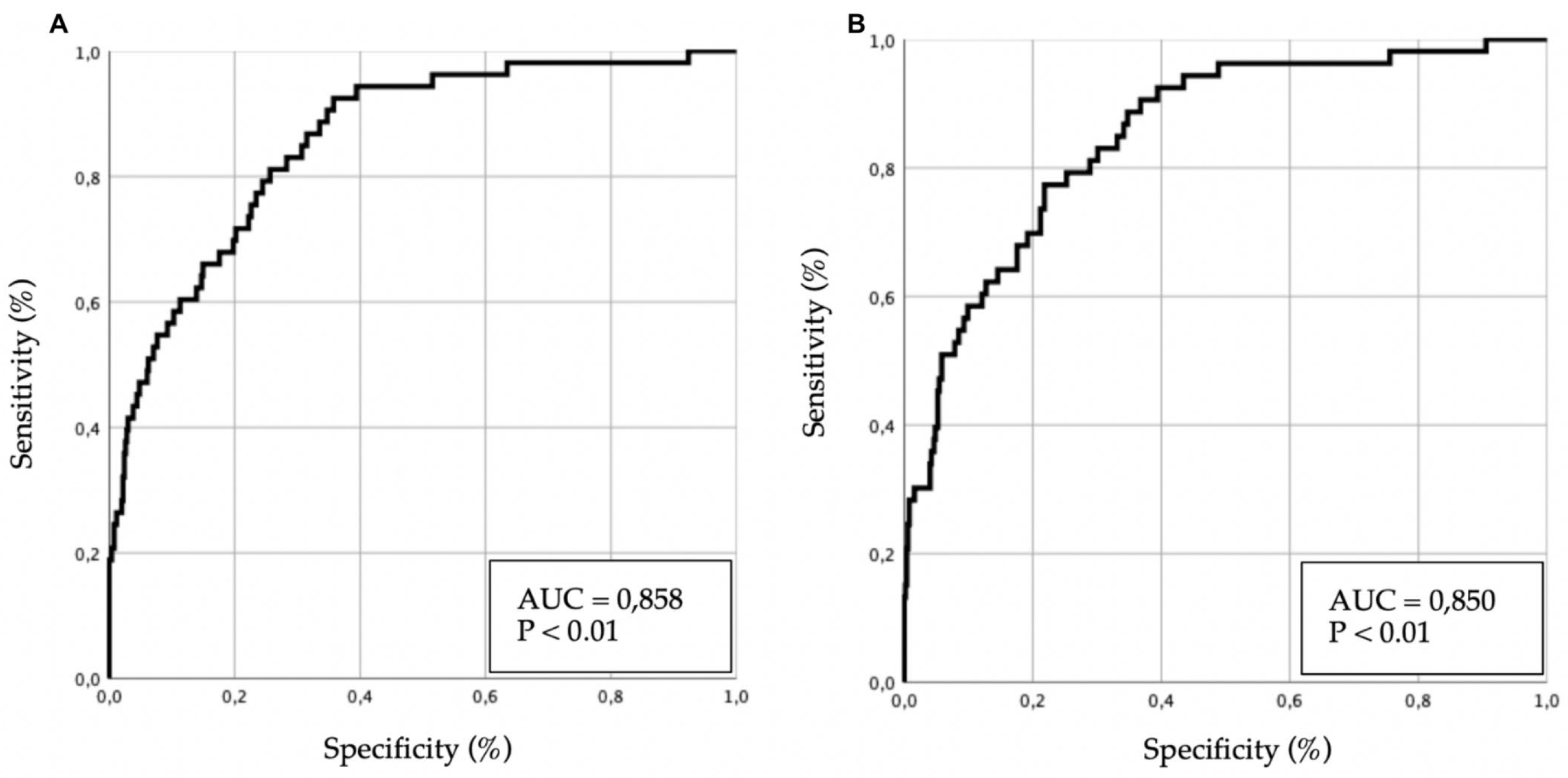
3.4.1. Multivariate Analysis of 30-Day Mortality
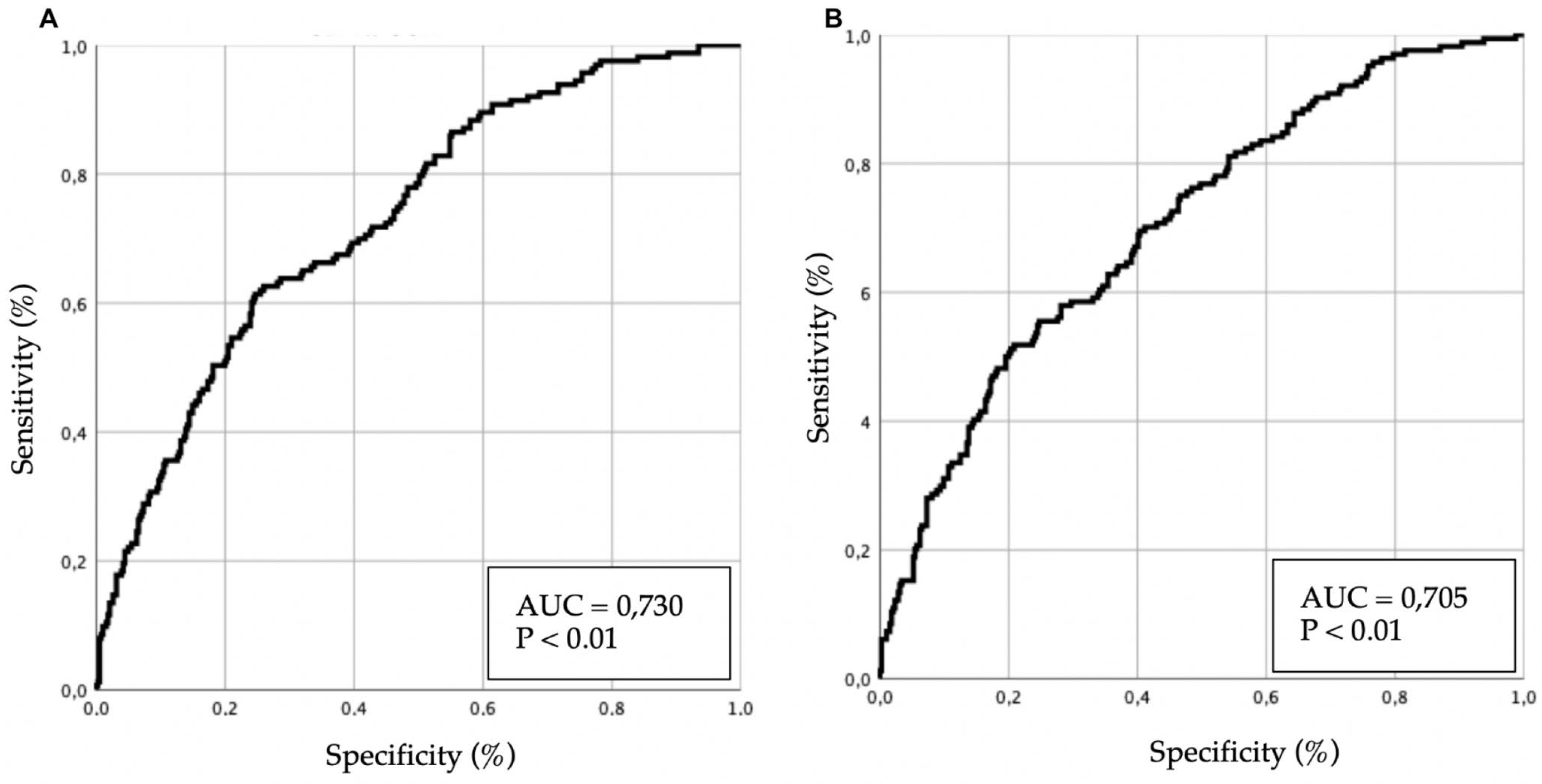
3.4.2. Multivariate Analysis of 12-Month Mortality
4. Discussion
4.1. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACS | Acute Coronary Syndrome |
| AF | Atrial Fibrillation |
| AHF | Acute Heart Failure |
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| COPD | Chronic Obstructive Pulmonary Disease |
| DM | Diabetes Mellitus |
| EAHFE | Epidemiology of Acute Heart Failure in Emergency Departments |
| ECG | Electrocardiogram |
| HF | Heart Failure |
| HED | Hospital Emergency Department |
| HUMV | Marqués de Valdecilla University Hospital |
| IQR | Interquartile Range |
| MRN | Medical Record Number |
| NYHA | New York Heart Association |
| NTproBNP | N-terminal pro-B-type Natriuretic Peptide |
| OR | Odds Ratio |
| PF(s) | Precipitating Factor(s) |
| RICA | National Heart Failure Registry (Registro Nacional de Insuficiencia Cardiaca) |
| ROC | Receiver Operating Characteristic |
| SPSS | Statistical Package for the Social Sciences |
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Sicras-Mainar, A.; Sicras-Navarro, A.; Palacios, B.; Varela, L.; Delgado, J.F. Epidemiology and treatment of heart failure in Spain: The HF-PATHWAYS study. Rev. Esp. Cardiol. 2022, 75, 31–38. [Google Scholar] [CrossRef]
- Ho, K.K.; Pinsky, J.L.; Kannel, W.B.; Levy, D. The epidemiology of heart failure: The Framingham Study. J. Am. Coll. Cardiol. 1993, 22, 6A–13A. [Google Scholar] [CrossRef] [PubMed]
- Díez-Villanueva, P.; Alfonso, F. Heart failure in the elderly. J. Geriatr. Cardiol. 2016, 13, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; et al. Heart disease and stroke statistics—2021 update: A report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Ortman, J.; Velkoff, V.; Hogan, H. An Aging Nation: The Older Population in the United States; Population Estimates and Projections; U.S. Census Bureau: Washington, DC, USA, 2014; Volume P25. [Google Scholar]
- Gaur, A.; Carr, F.; Warriner, D. Cardiogeriatrics: The current state of the art. Heart 2024, 110, 933–939. [Google Scholar] [CrossRef]
- He, W.; Goodkind, D.; Kowal, P. An Aging World: 2015; U.S. Census Bureau: Suitland, MD, USA, 2016; Volume P95. [Google Scholar]
- West, L.; Cole, S.; Goodkind, D.; He, W. 65+ in the United States: 2010; U.S. Census Bureau: Washington, DC, USA, 2014; Volume P23. [Google Scholar]
- Escobar, C.; Palacios, B.; Gonzalez, V.; Gutiérrez, M.; Duong, M.; Chen, H.; et al. Evolution of Economic Burden of Heart Failure by Ejection Fraction in Newly Diagnosed Patients in Spain. BMC Health Serv. Res. 2023, 23, 1340. [Google Scholar] [CrossRef]
- Stein, G.Y.; Kremer, A.; Shochat, T.; Bental, T.; Korenfeld, R.; Abramson, E.; et al. The diversity of heart failure in a hospitalized population: The role of age. J. Card. Fail. 2012, 18, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Comorbidities in heart failure: A key issue. Eur. J. Heart Fail. Suppl. 2009, 8 (Suppl. 1). [CrossRef]
- Ozierański, K.; Kapłon-Cieślicka, A.; Peller, M.; Tymińska, A.; Balsam, P.; Galas, M.; et al. Clinical characteristics and predictors of one-year outcome of heart failure patients with atrial fibrillation compared to heart failure patients in sinus rhythm. Kardiol. Pol. 2016, 74, 251–261. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Givertz, M.M.; Aguilar, D.; Allen, L.A.; Chan, M.; Desai, A.S.; et al. Type 2 diabetes mellitus and heart failure: A scientific statement from the American Heart Association and the Heart Failure Society of America. Circulation 2019, 140, e294–e324. [Google Scholar] [CrossRef]
- Díez-Villanueva, P.; Jiménez-Méndez, C.; Pérez-Rivera, Á.; Barge Caballero, E.; López, J.; Ortiz, C.; et al. Different impact of chronic kidney disease in older patients with heart failure according to frailty. Eur. J. Intern. Med. 2025, 132, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Gorodeski, E.Z.; Goyal, P.; Hummel, S.L.; Krishnaswami, A.; Goodlin, S.J.; Hart, L.L.; et al. Domain management approach to heart failure in the geriatric patient: Present and future. J. Am. Coll. Cardiol. 2018, 71, 1921–1936. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Lampert, B.C. Heart failure in older adults: Medical management and advanced therapies. Geriatrics 2022, 7, 36. [Google Scholar] [CrossRef] [PubMed]
- Nadziakiewicz, P.; Szczurek-Wasilewicz, W.; Szyguła-Jurkiewicz, B. Heart failure in elderly patients: Medical management, therapies and biomarkers. Pharmaceuticals 2024, 18, 32. [Google Scholar] [CrossRef]
- López Díez, M.P.; Llorens, P.; Martín-Sánchez, F.J.; Gil, V.; Jacob, J.; Herrero, P.; et al. Emergency Department Observation of Patients with Acute Heart Failure Prior to Hospital Admission: Impact on Short-Term Prognosis. Emergencias 2022, 34, 345–351. [Google Scholar] [CrossRef]
- Miró, Ò.; García Sarasola, A.; Fuenzalida, C.; Calderón, S.; Jacob, J.; Aguirre, A.; et al. Departments Involved during the First Episode of Acute Heart Failure and Subsequent Emergency Department Revisits and Rehospitalisations: An Outlook through the NOVICA Cohort. Eur. J. Heart Fail. 2019, 21, 1231–1244. [Google Scholar] [CrossRef]
- Martínez, F.; Martínez-Ibañez, L.; Pichler, G.; Ruiz, A.; Redon, J. Multimorbidity and Acute Heart Failure in Internal Medicine. Int. J. Cardiol. 2017, 232, 208–215. [Google Scholar] [CrossRef]
- Guisado-Espartero, M.E.; Salamanca-Bautista, P.; Aramburu-Bodas, Ó.; Conde-Martel, A.; Arias-Jiménez, J.L.; Llàcer-Iborra, P.; et al. Heart Failure with Mid-Range Ejection Fraction in Patients Admitted to Internal Medicine Departments: Findings from the RICA Registry. Int. J. Cardiol. 2018, 255, 124–128. [Google Scholar] [CrossRef]
- Ruigómez, A.; Michel, A.; Martín-Pérez, M.; García Rodríguez, L.A. Heart Failure Hospitalization: An Important Prognostic Factor for Heart Failure Re-Admission and Mortality. Int. J. Cardiol. 2016, 220, 855–861. [Google Scholar] [CrossRef]
- Guisado-Espartero, M.E.; Salamanca-Bautista, P.; Aramburu-Bodas, Ó.; Manzano, L.; Quesada Simón, M.A.; Ormaechea, G.; et al. Causas de Muerte en Pacientes Hospitalizados en Servicios de Medicina Interna por Insuficiencia Cardíaca Según la Fracción de Eyección. Registro RICA. Med. Clin. (Barc) 2022, 158, 13–19. [Google Scholar] [CrossRef]
- Masip, J.; Formiga, F.; Comín-Colet, J.; Corbella, X. Short Term Prognosis of Heart Failure after First Hospital Admission. Med. Clin. (Barc) 2020, 154, 37–44. [Google Scholar] [CrossRef]
- Ichihara, Y.K.; Shiraishi, Y.; Kohsaka, S.; Nakano, S.; Nagatomo, Y.; Ono, T.; et al. Association of Pre-Hospital Precipitating Factors with Short- and Long-Term Outcomes of Acute Heart Failure Patients: A Report from the WET-HF2 Registry. Int. J. Cardiol. 2023, 389, 131161. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Voors, A.A.; Girerd, N.; Billotte, M.; Anker, S.D.; Cleland, J.G.; et al. Heart Failure Etiologies and Clinical Factors Precipitating for Worsening Heart Failure: Findings from BIOSTAT-CHF. Eur. J. Intern. Med. 2020, 71, 62–69. [Google Scholar] [CrossRef]
- Sánchez-Marcos, C.; Jacob, J.; Llorens, P.; Rodríguez, B.; Martín-Sánchez, F.J.; Herrera, S.; et al. Análisis de la efectividad y seguridad de las unidades de estancia corta en la hospitalización de pacientes con insuficiencia cardíaca aguda. Propensity Score UCE-EAHFE. Rev. Clin. Esp. 2022, 222, 443–457. [Google Scholar] [CrossRef]
- Espinosa, B.; Llorens, P.; Gil, V.; Rossello, X.; Jacob, J.; Herrero, P.; et al. Prognosis of acute heart failure based on clinical data of congestion. Rev. Clin. Esp. 2022, 222, 321–331. [Google Scholar] [CrossRef]
- Sánchez-Marcos, C.; Espinosa, B.; Coloma, E.; San Inocencio, D.; Pilarcikova, S.; Guzmán-Martínez, S.; et al. Safety and efficiency of discharge to home hospitalization directly after emergency department care of patients with acute heart failure. Emergencias 2023, 35, 176–184. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; Chapter 4, Model-Building Strategies and Methods for Logistic Regression; Wiley: New York, NY, USA, 2013; pp. 89–151. [Google Scholar]
- Hilbe, J.M. Logistic Regression Models; Chapter 5, Model Development; Chapman & Hall/CRC Press: Boca Raton, FL, USA, 2009; pp. 73–187. [Google Scholar]
- Ostolaza-Tazón, I.; Alonso-Valle, H.; Muñoz-Cacho, P. Identificación y prevalencia de factores precipitantes en la insuficiencia cardiaca aguda en un servicio de urgencias español y su pronóstico a corto y largo plazo. Rev. Esp. Urg. Emerg. 2025, 4, 34–40. [Google Scholar] [CrossRef]
- Hamana, T.; Fujimoto, W.; Konishi, A.; Takemoto, M.; Kuroda, K.; Yamashita, S.; et al. Differences in Prognostic Factors among Patients Hospitalized for Heart Failure According to the Age Category: From the KUNIUMI Registry Acute Cohort. Intern. Med. 2022, 61, 3171–3180. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.; Parenica, J.; Park, J.J.; Ishihara, S.; AlHabib, K.F.; Laribi, S.; et al. Clinical Presentation and Outcome by Age Categories in Acute Heart Failure: Results from an International Observational Cohort. Eur. J. Heart Fail. 2015, 17, 1114–1123. [Google Scholar] [CrossRef]
- Metra, M.; Mentz, R.J.; Chiswell, K.; Bloomfield, D.M.; Cleland, J.G.; Cotter, G.; et al. Acute Heart Failure in Elderly Patients: Worse Outcomes and Differential Utility of Standard Prognostic Variables. Insights from the PROTECT Trial. Eur. J. Heart Fail. 2015, 17, 109–118. [Google Scholar] [CrossRef]
- Tromp, J.; Shen, L.; Jhund, P.S.; Anand, I.S.; Carson, P.E.; Desai, A.S.; et al. Age-Related Characteristics and Outcomes of Patients with Heart Failure with Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2019, 74, 601–612. [Google Scholar] [CrossRef]
- Gimeno-Miguel, A.; Gracia Gutiérrez, A.; Poblador-Plou, B.; Coscollar-Santaliestra, C.; Pérez-Calvo, J.I.; Divo, M.J.; et al. Multimorbidity Patterns in Patients with Heart Failure: An Observational Spanish Study Based on Electronic Health Records. BMJ Open 2019, 9, e033174. [Google Scholar] [CrossRef]
- Hamana, T.; Fujimoto, W.; Konishi, A.; Takemoto, M.; Kuroda, K.; Yamashita, S.; et al. Differences in Prognostic Factors among Patients Hospitalized for Heart Failure According to the Age Category: From the KUNIUMI Registry Acute Cohort. Intern. Med. 2022, 61, 3171–3180. [Google Scholar] [CrossRef]
- Machida, K.; Minamisawa, M.; Motoki, H.; Teramoto, K.; Okuma, Y.; Kanai, M.; et al. Clinical Profile and Prognosis of Dementia in Patients with Acute Decompensated Heart Failure: From the CURE-HF Registry. Circ. J. 2023, 88, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, S.M.; Warner Stevenson, L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; et al. 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized with Heart Failure: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2019, 74, 1966–2011. [Google Scholar] [CrossRef] [PubMed]
- Miró, Ò.; Conde-Martel, A.; Llorens, P.; Salamanca-Bautista, P.; Gil, V.; González-Franco, Á.; et al. The Influence of Comorbidities on the Prognosis after an Acute Heart Failure Decompensation and Differences According to Ejection Fraction: Results from the EAHFE and RICA Registries. Eur. J. Intern. Med. 2023, 111, 97–104. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Heywood, J.T.; Heidenreich, P.A.; Lopatin, M.; Yancy, C.W.; ADHERE Scientific Advisory Committee and Investigators. Temporal Trends in Clinical Characteristics, Treatments, and Outcomes for Heart Failure Hospitalizations, 2002 to 2004: Findings from the Acute Decompensated Heart Failure National Registry (ADHERE). Am. Heart J. 2007, 153, 1021–1028. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Abraham, W.T.; Albert, N.M.; Gattis, W.A.; Gheorghiade, M.; Greenberg, B.; O’Connor, C.M.; Yancy, C.W.; Young, J. Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF): Rationale and Design. Am. Heart J. 2004, 148, 43–51. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Delgado Jimenez, J.F.; Metra, M.; et al.; Heart Failure Association (HFA) of the European Society of Cardiology (ESC) European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-Year Follow-Up Outcomes and Differences across Regions. Eur. J. Heart Fail. 2016, 18, 613–625. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Bueno, H.; Gil, V.; Jacob, J.; Martín-Sánchez, F.J.; Llorens, P.; et al. Synergistic Impact of Systolic Blood Pressure and Perfusion Status on Mortality in Acute Heart Failure. Circ. Heart Fail. 2021, 14, e007347. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.P.; Sideris, K.; Taleb, I.; Maneta, E.; Hamouche, R.; Tseliou, E.; et al. Clinical Characteristics and Outcomes of Patients Suffering Acute Decompensated Heart Failure Complicated by Cardiogenic Shock. Circ. Heart Fail. 2024, 17, e011358. [Google Scholar] [CrossRef]
- Cooper, L.B.; Lippmann, S.J.; DiBello, J.R.; Gorsh, B.; Curtis, L.H.; Sikirica, V.; et al. The Burden of Congestion in Patients Hospitalized with Acute Decompensated Heart Failure. Am. J. Cardiol. 2019, 124, 545–553. [Google Scholar] [CrossRef]
- Franco, J.; Formiga, F.; Corbella, X.; Conde-Martel, A.; Llácer, P.; Álvarez Rocha, P.; et al. De Novo Acute Heart Failure: Clinical Features and One-Year Mortality in the Spanish Nationwide Registry of Acute Heart Failure. Med. Clin. (Barc) 2019, 152, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Zafrir, B.; Lund, L.H.; Laroche, C.; Ruschitzka, F.; Crespo-Leiro, M.G.; Coats, A.J.S.; et al. Prognostic Implications of Atrial Fibrillation in Heart Failure with Reduced, Mid-Range, and Preserved Ejection Fraction: A Report from 14,964 Patients in the European Society of Cardiology Heart Failure Long-Term Registry. Eur. Heart J. 2018, 39, 4277–4284. [Google Scholar] [CrossRef] [PubMed]
- Son, M.K.; Park, J.J.; Lim, N.K.; Kim, W.H.; Choi, D.J. Impact of Atrial Fibrillation in Patients with Heart Failure and Reduced, Mid-Range or Preserved Ejection Fraction. Heart 2020, 106, 1160–1168. [Google Scholar] [CrossRef] [PubMed]
- Rewiuk, K.; Wizner, B.; Fedyk-Łukasik, M.; Zdrojewski, T.; Opolski, G.; Dubiel, J.; et al. Epidemiology and management of coexisting heart failure and atrial fibrillation in an outpatient setting. Pol. Arch. Med. Wewn. 2011, 121, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, N.P.; Clare, R.M.; Harrington, J.L.; Badjatiya, A.; Wojdyla, D.M.; Udell, J.A.; et al. Morbidity and Mortality Associated with Heart Failure in Acute Coronary Syndrome: A Pooled Analysis of 4 Clinical Trials. J. Card. Fail. 2023, 29, 1603–1614. [Google Scholar] [CrossRef]
- Miró, Ò.; Rossello, X.; Gil, V.; Martín-Sánchez, F.J.; Llorens, P.; Herrero-Puente, P.; et al. Predicting 30-Day Mortality for Patients with Acute Heart Failure in the Emergency Department: A Cohort Study. Ann. Intern. Med. 2017, 167, 698–705. [Google Scholar] [CrossRef]
- Jacob, J.; Martín-Sanchez, F.J.; Herrero, P.; Miró, Ò.; Llorens, P. Valor Pronóstico de la Troponina en Pacientes con Insuficiencia Cardiaca Aguda Atendidos en los Servicios de Urgencias Hospitalarios Españoles: Estudio TROPICA (TROPonina en Insuficiencia Cardiaca Aguda). Med. Clin. (Barc) 2013, 140, 145–151. [Google Scholar] [CrossRef]
- Arrigo, M.; Gayat, E.; Parenica, J.; Ishihara, S.; Zhang, J.; Choi, D.J.; et al. Precipitating Factors and 90-Day Outcome of Acute Heart Failure: A Report from the Intercontinental GREAT Registry. Eur. J. Heart Fail. 2017, 19, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Lee, C.H.; Lin, H.W.; Lin, S.H.; Li, Y.H. Impact of Infection-Related Admission in Patients with Heart Failure: A 10 Years National Cohort Study. Sci. Rep. 2023, 13, 6941. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.W.; Ashok, T.; Patni, N.; Fatima, M.; Lamis, A.; Anne, K.K. Anemia and Heart Failure: A Narrative Review. Cureus 2022, 14, e27167. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Johnson, J.; Patel, V.; Pekmezaris, R.; Seepersaud, H.; Kumar, P.; et al. Understanding Social Risk Factors in Patients Presenting to the Emergency Department for Acute Heart Failure: A Pilot Study. Am. J. Emerg. Med. 2024, 84, 7–14. [Google Scholar] [CrossRef]
- de Los Ángeles Fernández-Rodríguez, M.; Prieto-García, B.; Vázquez-Álvarez, J.; Jacob, J.; Gil, V.; Miró, O.; et al. Prognostic Implications of Anemia in Patients with Acute Heart Failure in Emergency Departments: ANEM-AHF Study. Int. J. Clin. Pract. 2021, 75, e13712. [Google Scholar] [CrossRef]
- van den Berge, J.C.; Constantinescu, A.A.; van Domburg, R.T.; Brankovic, M.; Deckers, J.W.; Akkerhuis, K.M. Renal Function and Anemia in Relation to Short- and Long-Term Prognosis of Patients with Acute Heart Failure in the Period 1985–2008: A Clinical Cohort Study. PLoS ONE 2018, 13, e0201714. [Google Scholar] [CrossRef]
- Collins, S.P.; Jenkins, C.A.; Harrell, F.E.; Liu, D.; Miller, K.F.; Lindsell, C.J.; et al. Identification of Emergency Department Patients with Acute Heart Failure at Low Risk for 30-Day Adverse Events. JACC Heart Fail. 2015, 3, 737–747. [Google Scholar] [CrossRef]
- Stiell, I.G.; Clement, C.M.; Brison, R.J.; Rowe, B.H.; Borgundvaag, B.; Aaron, S.D.; et al. A Risk Scoring System to Identify Emergency Department Patients with Heart Failure at High Risk for Serious Adverse Events. Acad. Emerg. Med. 2013, 20, 17–26. [Google Scholar] [CrossRef]
- American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Acute Heart Failure Syndromes. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department with Acute Heart Failure Syndromes: Approved by ACEP Board of Directors, June 23, 2022. Ann. Emerg. Med. 2022, 80, e31–e59. [Google Scholar] [CrossRef]

| Patients (n=548) | |
|---|---|
| Epidemiological data | |
| Age (years) | 80.7 ± 9.9 |
| Female sex | 272 (49.6%) |
| Cardiovascular history | |
| Atrial fibrillation | 196 (35.8%) |
| Ischemic heart disease | 130 (23.7%) |
| Valvular heart disease | 108 (19.7%) |
| Heart failure history | |
| Previous episodes of AHF | 343 (62.6%) |
| NYHA Functional Class | |
| Class I-II | 371 (67.7%) |
| Class III-IV | 177 (32.3%) |
| Non-cardiovascular comorbidities | |
| COPD | 70 (12.8%) |
| Dementia | 31 (5.7%) |
| Patients (n=548) | |
|---|---|
| Clinical status of the patient | |
| Respiratory rate > 25 breaths/min | 37 (6.8%) |
| Oxygen saturation (%) | 93.6 ± 6.7 |
| Congestive signs | 428 (78.1%) |
| Low-output symptoms | 14 (2.6%) |
| Acute heart failure profile | |
| Hemodynamic profile | |
| Warm and wet | 474 (86.5%) |
| Cold and wet | 64 (11.7%) |
| Cold and dry | 5 (0.9%) |
| Warm and dry | 5 (0.9%) |
| Precipitating factor | |
| Infection | 190 (34.7%) |
| Rapid atrial fibrillation | 95 (17.3%) |
| Acute coronary syndrome | 31 (5.7%) |
| Laboratory test results | |
| Hemoglobin (g/dL) | 12.4 ± 5.3 |
| Creatinine (mg/dL) | 1.4 ± 1.1 |
| Potassium (mEq/L) | 4.5 ± 1.7 |
| Emergency department management | |
| Hospital admission | 421 (76.8%) |
| OR | 95% IC | p | AUC (%) | |
|---|---|---|---|---|
| Model 1 | 85.8% | |||
| Age | 1.12 | 1.07 – 1.17 | < 0.01 | |
| Ischemic heart disease | 3.07 | 1.49 – 6.31 | < 0.01 | |
| Valvular heart disease | 2.16 | 1.01 – 4.61 | 0.05 | |
| Previus HF | 1.42 | 0.64 – 3.14 | 0.39 | |
| AHF Types | ||||
| Hypertensive (reference) | - | - | < 0.01 | |
| Normotensive | 4.52 | 1.02 – 20.06 | 0.05 | |
| Hypotensive without shock | 8.28 | 1.75 – 39.24 | < 0.01 | |
| Hypotensive with cardiogenic shock | 22.73 | 1.13 – 457.66 | 0.04 | |
| AHF associated with ACS | 231.65 | 27.52 – 1949.61 | < 0.01 | |
| NYHA functional class | ||||
| Class I (referencia) | - | - | < 0.01 | |
| Class II | 0.68 | 0.24 – 1.94 | 0.47 | |
| Class III | 2.21 | 0.83 – 5.87 | 0.11 | |
| Class IV | 16.40 | 3.52 – 76.36 | < 0.01 | |
| Creatinine | 1.61 | 1.27 – 2.04 | < 0.01 | |
| Model 2 | 85.0% | |||
| Age | 1.12 | 1.07 – 1.17 | < 0.01 | |
| Ischemic heart disease | 2.93 | 1.44 – 5.98 | < 0.01 | |
| Acute Heart Failure Types | 4.53 | 1.02 – 20.17 | 0.05 | |
| Hypertensive (reference) | - | - | < 0.01 | |
| Normotensive | 3.80 | 0.89 – 16.16 | 0.07 | |
| Hypotensive without shock | 7.81 | 1.71 – 35.71 | < 0.01 | |
| Hypotensive with cardiogenic shock | 15.99 | 0.83 – 307.04 | 0.07 | |
| AHF associated with ACS | 187.05 | 23.66 – 1478.48 | < 0.01 | |
| NYHA functional class | ||||
| Class I (referencia) | - | - | < 0.01 | |
| Class II | 0.79 | 0.29 – 2.16 | 0.65 | |
| Class III | 2.25 | 0.86 – 5.88 | 0.10 | |
| Class IV | 17.59 | 3.97 – 77.89 | < 0.01 | |
| Creatinine | 1.60 | 1.27 – 2.03 | < 0.01 |
| OR | 95% IC | p | AUC (%) | |
|---|---|---|---|---|
| Model 1 | 73.0% | |||
| Age | 1.05 | 1.02 – 1.07 | < 0.01 | |
| Valvular heart disease | 1.48 | 0.91 – 2.41 | 0.11 | |
| Previus HF | 1.71 | 1.08 – 2.73 | 0.02 | |
| NYHA functional class | ||||
| Class I (referencia) | - | - | < 0.01 | |
| Class II | 1.29 | 0.71 – 2.33 | 0.40 | |
| Class III | 2.32 | 1.28 – 4.21 | < 0.01 | |
| Class IV | 4.03 | 1.19 – 13.68 | 0.02 | |
| AF as PF | 0.77 | 0.43 – 1.37 | 0.37 | |
| ACS as PF | 2.44 | 1.06 – 5.64 | 0.04 | |
| Creatinine | 1.25 | 1.04 – 1.50 | 0.02 | |
| Hemoglobin | 0.88 | 0.79 – 0.98 | 0.02 | |
| Potassium | 1.26 | 0.96 – 1.65 | 0.09 | |
| Hospital admission | 2.00 | 1.19 – 3.36 | < 0.01 | |
| Model 2 | 70.5% | |||
| Age | 1.04 | 1.02 – 1.07 | < 0.01 | |
| Previus HF | 1.81 | 1.16 – 2.82 | < 0.01 | |
| NYHA functional class | ||||
| Class I (referencia) | - | - | < 0.01 | |
| Class II | 1.34 | 0.75 – 2.39 | 0.32 | |
| Class III | 2.35 | 1.31 – 4.19 | < 0.01 | |
| Class IV | 4.55 | 1.36 – 15.14 | 0.01 | |
| Creatinine | 1.34 | 1.12 – 1.60 | < 0.01 | |
| Hospital admission | 1.97 | 1.18 – 3.28 | < 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



