
Submitted:
05 November 2025
Posted:
06 November 2025
You are already at the latest version
Abstract
Background: Hepatocellular carcinoma (HCC) remains a major cause of cancer-related mortality, with many patients initially unsuitable for curative resection or transplantation. Transarterial radioembolization (TARE) has emerged as a locoregional therapy to downstage tumors and expand surgical eligibility. Methods: This retrospective study included 25 patients with HCC who underwent TARE as a bridging treatment. The primary outcomes assessed were the efficacy of TARE in facilitating curative surgery and long-term oncological outcomes, specifically overall survival (OS) and disease-free survival (DFS). Results: Seventeen patients subsequently underwent surgical resection and eight underwent living donor liver transplantation (LDLT). At a median follow-up of 33.4 months, the median DFS was 11.2 months, with patients experiencing recurrence showing significantly shorter DFS (3.65 months) than those without recurrence (27.1 months). Median OS for the cohort was 33.4 months, with 76% of patients alive and disease-free at last follow-up. Kaplan–Meier analysis demonstrated sustained OS in the LDLT group, while resection patients gradually declined within the first two years. Conclusion: TARE is an effective bridging strategy that enables curative-intent surgery in selected patients with HCC and supports favorable long-term oncological outcomes. Careful patient selection and multidisciplinary management remain essential to optimize survival benefits.
Keywords:
hepatocellular carcinoma (HCC)
; living donor liver transplant (LDLT)
; surgical resection
; transarterial radioembolization (TARE)
Introduction
Patients suffering from hepatocellular carcinoma (HCC) are often diagnosed in an advanced stage of the disease, which makes them ineligible for immediate life-saving therapies like surgical removal of the tumor or liver transplantation [1,2]. Transarterial radioembolization (TARE) using Yttrium-90 (Y-90) is now one of the most aggressive local therapies for controlling tumors and facilitating contralateral lobe hypertrophy of the liver. Thus, it links to curative surgery in formerly unresectable patients [3]. Initially, TARE was used only for palliative purposes, but increasing evidence supports its use for downstaging and bridging purposes before transplantation or resection [4]. As with portal vein embolization, TARE also causes selective radiation-induced atrophy of the treated liver lobe and atrophy and hypertrophy of the contralateral future liver remnant (FLR), but with additional tumoricidal effects [5].
In a landmark review of Korean experience, Kim et al. (2017) described the safety and efficacy of TARE in unresectable HCC patients, reporting longer time to progression, better tumor downsizing, less post-embolization syndrome, and shorter hospitalization compared with conventional transarterial chemoembolization (TACE) [6]. Similarly, Shehta and colleagues evaluated a small series of patients undergoing major hepatectomy after Y-90 TARE as a bridging strategy: in 5 patients, tumor shrinkage of ~24.5% was observed and the expected remnant liver volume improved significantly (from ~354.6 mL to 500.8 mL), enabling resection in all, with no serious radiation-related complications and favorable short-term outcomes (all alive at mean 15 months, no recurrence) [7]. These studies support the dual action of TARE in controlling tumor progression and inducing contralateral hypertrophy, making it an attractive option for patients at risk of insufficient liver remnant or waiting for transplantation.
Beyond those, additional series provide further evidence of the downstaging and conversion potential of TARE. For example, Tabone et al. (2019) reported that in a cohort of 24 patients with unresectable HCC (many with portal vein involvement), ~20% were successfully downstaged to resection following Y-90 resin microsphere radioembolization; higher tumor-absorbed radiation doses and lower baseline AFP levels correlated with successful downstaging, suggesting a dose–response and biomarker interplay in patient selection [8]. Moreover, a multidisciplinary working group recently provided recommendations on converting previously unresectable HCC to resection status after radioembolization, emphasizing optimal patient selection, timing, and imaging follow-up strategies to maximize safety and efficacy during the bridging window [9]. Despite the promising data, significant gaps remain. Many series are retrospective and limited in sample size, especially for resection-conversion settings; the optimal radiation dose thresholds or biomarkers predictive of response are not clearly defined; comparative prospective trials between TARE and other loco-regional strategies (TACE, ablation) in bridging or downstaging contexts are scarce; and long-term oncological outcomes (beyond short- or mid-term follow-up) in the resection or transplant-context remain underexplored. Therefore, this study aims to evaluate the efficacy and safety of TARE in patients with HCC.
Methodology
Patients
This retrospective observational study included patients with hepatocellular carcinoma (HCC) who underwent TARE within a defined study period at a tertiary liver cancer center. Eligible patients were those diagnosed with HCC based on imaging criteria and considered initially unresectable due to large tumor size, multifocal disease, vascular invasion, or inadequate future liver remnant (FLR) volume. Patients with extrahepatic spread, advanced hepatic decompensation (Child–Pugh C), uncontrolled comorbidities, or other locoregional therapies (e.g., TACE or RFA alone) were excluded. Patients lacking adequate pre- or post-TARE imaging or clinical follow-up data were also excluded.
Data Collection
Clinical and oncological data were extracted from medical records. Baseline parameters included patient demographics, liver function tests, tumor burden, and imaging findings. TARE treatment details were collected, such as microsphere dose, dosimetry, and distribution. HCC patients were reassessed for surgical eligibility using imaging, tumor markers including alpha-fetoprotein (AFP) and protein induced by vitamin K absence or antagonist-II (PIVKA-II), and liver function after TARE. Surgical outcomes included type of surgery (resection and LDLT), operative parameters (margin status, blood loss, complications), and recovery (hospitalization and liver function recovery). Oncological outcomes assessed recurrence-free survival (RFS) and overall survival (OS).
TARE Procedure
All patients underwent hepatic angiography and mapping before Y-90 administration to assess vascular anatomy and minimize non-target embolization. The dose was individualized according to tumor size, liver volume, and lung shunt fraction. Following treatment, patients underwent regular clinical and radiological follow-up to evaluate tumor response, hypertrophy of the future liver remnant, and liver function. Conversion surgery was considered if adequate FLR was achieved and extrahepatic disease remained absent. Resection was performed in patients with preserved hepatic reserve, while LDLT was chosen for those with cirrhosis or insufficient FLR.
Statistical Analysis
All analyses were performed using SPSS Inc., based in Chicago, IL, USA, developed the SPSS software (version 29.0) for the statistical analyses.Continuous variables were expressed as median (range) and compared using Mann-Whitney U tests. Categorical variables were compared using Chi-square or Fisher’s exact tests as appropriate. Survival outcomes (RFS and OS) were estimated using Kaplan–Meier methods, and differences between groups were analyzed with the log-rank test. A p-value <0.05 was considered statistically significant.
The study followed institutional ethical guidelines and received approval from the hospital’s Institutional Review Board Samsung Medical center (SMC-2025-10-110). We omitted the requirement for informed consent due to the retrospective nature of this analysis of de-identified data.
Result
Baseline Characteristics
A total of 25 patients diagnosed with hepatocellular carcinoma (HCC) were included in this study, comprising 17 males (68%) and 8 females (32%), indicating a male predominance. The mean age was 57.76 years for males and 58.63 years for females. The mean body mass index (BMI) for the cohort was 24.36 kg/m², ranging from 16.11 to 32.10 kg/m², with male patients averaging 24.10 kg/m² and female patients 24.98 kg/m²; notably, one patient was classified as obese with a BMI ≥30 kg/m². Table 1 gives a detailed demographic overview. Fifteen patients (60%) had HCC, while 10 patients (40%) presented with hepatocellular carcinoma or necrotic nodules, with no significant gender differences in diagnosis. Baseline laboratory parameters revealed comparable hematological profiles between patients undergoing surgical resection and living donor liver transplantation (LDLT). However, the LDLT group exhibited higher bilirubin levels and prolonged INR, reflecting more advanced liver dysfunction. Baseline tumor markers, including AFP and PIVKA-II, were elevated in the surgical resection group, whereas inflammatory markers such as CRP showed no significant differences. Liver stiffness assessments indicated that 50% of LDLT patients had advanced fibrosis (F4, ≥11 kPa), 25% had moderate fibrosis (F3, 8.1–10.9 kPa), and 25% had mild fibrosis (F2, <8 kPa). CAP values ranged from 166 to 301 dB/m, and increased spleen stiffness corresponded with higher fibrosis stages, highlighting a predominance of moderate-to-advanced liver damage within the cohort. Table 1 presents baseline demographic, clinical, and pathological characteristics of patients.
Pre-Operative Factors
Of the 25 patients, 17 underwent surgical resection and 8 underwent LDLT. The most common surgical intervention was right hemihepatectomy (9 cases, 37.5%), followed by LDLT (8 cases, 32%), laparoscopic extended right hemihepatectomy (3 cases, 12.5%), and segmentectomy (2 cases, 8.3%). Less frequently performed procedures included caudate lobectomy, laparoscopic S2/S3 wedge resection, laparoscopic extended left hemihepatectomy, and laparoscopic central hepatectomy involving segments 4, 5, and 8. Secondary procedures were occasionally required, with cholecystectomy being most common (2 cases, 8.3%), and single instances of open cholecystectomy, abdominal adhesiolysis, and en bloc diaphragm resection. LDLT procedures were associated with significantly longer operation times (p<0.001) and higher estimated blood loss (p=0.011) compared to surgical resection, reflecting increased procedural complexity. ASA classification showed a higher proportion of ASA 3 patients in the LDLT group, indicating greater preoperative risk. Age distribution revealed that older patients predominantly underwent major hepatic resections such as right or left hemihepatectomies, while LDLT was often performed in younger candidates with preserved hepatic function.
Pathology
Pathological analysis included 18 HCC cases and 7 post-treatment necrotic nodules. Tumor sizes varied widely, ranging from 1.2 cm to 12.5 cm, and one patient exhibited more than 30 tumors across multiple hepatic segments (S2, S4, S7, S8), demonstrating extensive intrahepatic spread. The most frequently involved segments were S5, S6, S7, and S8, with multinodular cases such as five in S8 and 14 in S7. Cirrhosis or incomplete cirrhosis was present in approximately half of the cohort. Microvascular invasion was observed in several cases, although portal vein invasion was absent. Surgical margins were negative in all patients, ranging from 0.1 to 4 cm. Solitary tumors were more common in the surgical resection group. In contrast, LDLT patients exhibited higher rates of microvascular invasion (p=0.028) and intrahepatic metastasis (p=0.010). Necrotic nodules consistently demonstrated 100% necrosis, while HCC cases displayed variable necrosis ranging from 1% to 99.5%, reflecting the heterogeneity of treatment response (Table 2).
TARE
Transarterial radioembolization (TARE) and transarterial chemoembolization (TACE) were widely used as preoperative interventions. Multiple HCC was the primary indication, observed in 4 surgical resection patients (23.5%) and all 8 LDLT patients (100%). Other indications, including portal vein tumor thrombosis with satellite nodules (2 cases, 11.8%) and small remnant liver volume (3 cases, 17.6%), were exclusive to the surgical resection group. Table 3 categorizes tumors based on the degree of necrosis observed post-TARE, alongside the corresponding tumor-to-normal liver (T/N) ratios, radiation doses delivered, and procedure-related complications.TARE outcomes were variable; while some patients achieved complete devascularization, others experienced persistent or recurrent lesions. Adverse events included renal dysfunction with myalgia, liver function test elevation with fever, nausea, vomiting, generalized abdominal discomfort, and radiation pneumonia. Complications were more common in patients with cirrhosis, whereas incomplete cirrhosis or septal fibrosis was associated with a broader range of side effects. TACE alone often resulted in tumor progression, whereas combination therapies (TACE + TARE) helped stabilize disease, particularly in multifocal HCC, but rarely achieved complete eradication. The interval between TARE and surgery ranged from 5.6 to 34 months, with a median of 9.1 months, reflecting individualized clinical decision-making. Key procedural outcomes across all cases were evaluated to analyse the efficacy and safety of transarterial radioembolization (TARE) in hepatocellular carcinoma. The detailed clinical, laboratory, imaging, and treatment characteristics of patients undergoing transarterial radioembolization (TARE) are presented in Table 4.
Outcomes
During follow-up, 6 patients (24%) experienced disease recurrence, and 2 patients (8%) died, both following recurrences. Median disease-free survival (DFS) for the cohort was 11.2 months, with recurrent cases showing significantly shorter DFS (3.65 months) compared to non-recurrent patients (27.1 months). Median overall survival (OS) was 33.4 months overall; paradoxically, patients with recurrence had higher median OS (45.45 months) than those without recurrence (27.1 months), likely due to follow-up timing differences, shown in Figure 1. Surgical resection patients had significantly longer follow-up (p=0.030), suggesting better long-term outcomes, whereas LDLT patients with more advanced disease had more complex surgeries and higher intraoperative risk. Multimodal treatment strategies combining TARE, TACE, RFA, chemotherapy, and radiotherapy were integral in optimizing tumor control, downstaging disease, and improving resectability. Liver stiffness and CAP assessments highlighted that the majority of patients had moderate-to-advanced fibrosis, influencing both treatment tolerance and post-procedural recovery. Postoperative care emphasized monitoring for radiation-induced liver injury, portal vein thrombosis, and hepatic dysfunction to ensure optimal recovery. Kaplan-Meier survival analysis demonstrated a gradual decline in survival in the surgical resection group during the first two years. In contrast, LDLT patients maintained nearly 100% survival throughout the observed period, illustrating the complexity of patient outcomes and the impact of individualized treatment strategies.
Discussion
Postoperative complications and the requirement for intensive care unit (ICU) support reinforce the need for comprehensive post-surgical management. The presence of radiation-induced liver injury, portal vein thrombosis, and treatment-related hepatic dysfunction in some patients underscores the complexity of post-treatment recovery. Close monitoring of hepatic function, management of post-surgical infections, and timely intervention for complications are critical for optimizing recovery.
This study provides meaningful insights into the surgical management of hepatocellular carcinoma (HCC), highlighting key patterns in treatment approaches, surgical outcomes, and postoperative complications. Among the procedures analyzed, right hemihepatectomy emerged as the most frequently performed intervention, reaffirming its status as a cornerstone surgical option for liver malignancies [10,11]. Consistent with earlier research, our findings demonstrate that resection continues to be widely adopted where donor availability is limited, despite the associated risks [12,13]. Importantly, living donor liver transplantation (LDLT) was associated with fewer postoperative complications compared with resection, aligning with previous studies that underscore the protective role of transplantation in patients with cirrhosis and compromised hepatic reserve [10,11,14,15,16,17]. These findings reinforce LDLT as a compelling alternative, particularly in well-selected younger patients with preserved functional capacity and access to suitable donors.
Preoperative interventions played a decisive role in shaping surgical feasibility. In particular, transarterial radioembolization (TARE) was instrumental in tumor downstaging and improving resectability [2,18]. The presence of necrotic nodules in post-treatment pathological evaluations further validates the therapeutic potential of locoregional therapies [19]. Multiple studies have demonstrated the feasibility of resection following TARE. Studies reported that 27.7% of patients with single large HCC (≥5 cm) treated with TARE could undergo subsequent resection, achieving comparable overall survival and postoperative outcomes to upfront surgical candidates, especially when higher radiation doses were administered (mean ⁹⁰Y dose 211.89 Gy vs. 128.7 Gy, p < 0.001) [20,21]. Similarly, another study demonstrated that radiation lobectomy using TARE significantly increased FLR volume over 9 months and correlated with reduced gadolinium-EOB uptake on MRI, marking functional parenchymal changes predictive of resectability [3,22]. Consensus guidelines and expert working groups have now recommended using TARE for conversion to resection in carefully selected patients, emphasizing its dual role in achieving hypertrophy and oncologic control [22].
In addition to favorable clinical outcomes, TARE has shown advantages in cost-effectiveness and bridging success. Wu et al. found TARE more cost-effective than TACE for downstaging in liver transplant candidates, yielding higher quality-adjusted life years (QALYs) with only marginally higher costs [23]. A pooled analysis study affirmed that TARE produces higher downstaging rates than TACE and supports its application in patients beyond the Milan criteria. However, indications for its use in transplant settings remain variable [4]. Furthermore, Korean institutional experiences have highlighted the utility of TARE in inducing tumor necrosis and vascular remodeling while maintaining acceptable safety profiles, particularly in the context of radiation lobectomy protocols [3].
However, this benefit must be weighed against the risk of adverse events, including hepatic function derangements and renal impairment, which were observed in our cohort. These complications mirror those reported in larger series, where the tolerability of TARE was closely linked to baseline liver function and degree of fibrosis [24,25]. Careful patient selection and vigilant post-procedural monitoring remain critical to balance efficacy with safety.
When stratified by age, younger patients were more likely to undergo LDLT, whereas older patients tended to receive resection. This pattern reflects surgical eligibility, donor availability, and liver reserve, consistent with prior reports [15,26]. Our findings also highlight that advanced fibrosis and cirrhosis influence treatment allocation and postoperative outcomes, with such patients experiencing more TARE-related adverse effects and surgical complications, in line with previous studies [11,24].
The study also sheds light on the prognostic role of recurrence. Early recurrence, particularly within the first-year post-surgery, was strongly associated with significantly worse overall survival (OS). This finding parallel reports from other series emphasizing the aggressive biology of early-relapsing HCC and its detrimental impact on long-term outcomes [27,28]. Yet, observing that some patients with recurrence achieved durable survival highlights the importance of post-recurrence management strategies, such as repeat resection, salvage transplantation, or locoregional therapies. When tailored to the individual, these options can substantially modify the survival trajectory, as noted in recent comparative studies [29,30]. Interestingly, our cohort's variable interval between TARE and surgery did not independently predict survival outcomes. This suggests that timing alone is not the decisive prognostic factor but a constellation of clinical, pathological, and technical variables that interact to shape prognosis.
Comparison with prior literature underscores several converging and diverging trends. While our study observed higher rates of complications following surgical resection, including nausea, vomiting, liver enzyme derangements, and radiation pneumonia, these are in line with existing evidence that major hepatic resections carry increased perioperative risks [31]. However, margin negativity was more commonly achieved in resection cases than in LDLT. This suggests that although transplantation may be protective against complications and recurrence in cirrhotic patients, aggressive resection still plays an irreplaceable role in curative intent, particularly when anatomical considerations favor clear margin achievement [32]. Another important observation was the association between microvascular invasion, multicentric disease, and recurrence. This reiterates findings from prior studies that microscopic tumor spread remains a key challenge in achieving durable cures. As suggested in previous reports, strategies such as intraoperative ultrasound, frozen section analysis, and expanded resection margins may help mitigate these risks and improve long-term disease control [33].
These findings emphasize that no single modality offers a universal solution. LDLT, resection, and locoregional therapies all contribute distinct benefits and risks, and optimal outcomes depend on integrating them into an individualized, multidisciplinary treatment framework. For patients with preserved hepatic function and favorable anatomy, resection offers curative potential with the advantage of immediate availability. For those with cirrhosis or advanced fibrosis, LDLT provides a safer postoperative profile and improved long-term outcomes, but is constrained by donor limitations. Meanwhile, when judiciously applied, TARE represents a valuable adjunct in multimodal planning, enhancing resectability and tumor control.
Despite its contributions, this study has important limitations. The relatively small sample size (n=25) restricts statistical power and limits generalizability. Larger multicenter cohorts are needed to confirm these trends. The retrospective design also introduces potential biases in reporting complications and outcomes, and patient-reported measures were not systematically captured. Another limitation is the lack of extended follow-up data to fully evaluate long-term survival and recurrence patterns, both of which are crucial indicators of treatment efficacy. Additionally, the variability in preoperative treatments, particularly in the type and timing of locoregional therapies, complicates efforts to isolate the independent effect of each intervention.
Conclusion
This study emphasizes the evolving landscape of liver cancer treatment, where multimodal strategies, including preoperative locoregional therapies and surgical interventions, are essential for optimizing patient outcomes. LDLT demonstrated a lower complication rate than surgical resection, highlighting its value in selected patient populations. The effectiveness of TARE in tumor downstaging was evident, though individual responses varied, reinforcing the need for patient-specific treatment planning. Importantly, patients were observed for approximately six months after TARE, allowing for a meaningful assessment of treatment response and its impact on surgical resectability and postoperative outcomes.
Author Contributions
Conceptualization, A.A., D.H., J.K.; methodology, A.A.; software, A.A.; validation, A.A., D.H. and J.K..; formal analysis, A.A., D.H., J.K..; investigation, A.A.; resources, A.A., D.H., J.K.; data curation, A.A., writing original draft preparation, A.A.; writing—review and editing, A.A., S.C., N.O., G.C., J.R., D.H., J.K..; visualization, A.A.; supervision, D.H., J.K.; project administration, D.H., J.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The study was conducted according to institutional ethical guidelines and approved by the Institutional Review Board (IRB) of Samsung Medical center (SMC-2025-10-110).
Informed Consent Statement
We omitted the requirement for informed consent due to the retrospective nature of this analysis of de-identified data.
Data Availability Statement
The data supporting this study's findings are available from the corresponding author upon reasonable request. Due to patient privacy concerns, the data are not publicly shared.
Conflicts of Interest
The authors declare no conflicts of interest related to this study.
Abbreviations:
| HCC | Hepatocellular Carcinoma |
| TARE | Transarterial Radioembolization |
| LDLT | Living Donor Liver Transplantation |
| TACE | Transarterial Chemoembolization |
| RFA | Radiofrequency Ablation |
| FLR | Future Liver Remnant |
| ASA | American Society of Anesthesiologists |
| AFP | Alpha-Fetoprotein |
| PIVKA-II | Protein Induced by Vitamin K Absence-II |
| CRP | C-Reactive Protein |
| LFT | Liver Function Test |
| OS | Overall Survival |
| DFS | Disease-Free Survival |
| CAP | Controlled Attenuation Parameter |
| HBV | Hepatitis B Virus |
| HCV | Hepatitis C Viru |
| EBL | Estimated Blood Loss |
| TTS | TIME TO SURGERY |
| TTR | TIME TO RECURRANCE |
References
- D. Y. Kim and K. H. Han: Epidemiology and surveillance of hepatocellular carcinoma. Liver Cancer. 2012, 1:2-14.
- J. M. Kim, C. H. Kwon, J. W. Joh et al.: Effectiveness of locoregional therapy before living donor liver transplantation in patients with hepatocellular carcinoma who meet the Milan criteria. Transplant Proc. 2012, 44:403-8.
- Y. Bekki, A. Mahamid, S. Lewis et al.: Radiological and pathological assessment with EOB-MRI after Y90 radiation lobectomy prior to liver resection for hepatocellular carcinoma. HPB (Oxford). 2022, 24:2185-2192. [CrossRef]
- V. Lopez-Lopez, K. Miura, C. Kuemmerli et al.: Selecting the Appropriate Downstaging and Bridging Therapies for Hepatocellular Carcinoma: What Is the Role of Transarterial Radioembolization? A Pooled Analysis. Cancers (Basel). 2023, 15. [CrossRef]
- H. Nebelung, T. Wolf, S. Bund et al.: Radioembolization versus portal vein embolization for contralateral liver lobe hypertrophy: effect of cirrhosis. Abdominal Radiology. 2021, 46:4046-4055. [CrossRef]
- H. C. Kim: Radioembolization for the treatment of hepatocellular carcinoma. Clin Mol Hepatol. 2017, 23:109-114. [CrossRef]
- A. Shehta, J. M. Lee, K. S. Suh et al.: Bridging and downstaging role of trans-arterial radio-embolization for expected small remnant volume before liver resection for hepatocellular carcinoma. Ann Hepatobiliary Pancreat Surg. 2020, 24:421-430. [CrossRef]
- M. Tabone, A. Calvo, N. Russolillo et al.: Downstaging unresectable hepatocellular carcinoma by radioembolization using 90-yttrium resin microspheres: a single center experience. Journal of Gastrointestinal Oncology. 2019, 11:84-90. [Online]. Available: https://jgo.amegroups.org/article/view/29381.
- T. Baker, P. Tabrizian, I. Zendejas et al.: Conversion to resection post radioembolization in patients with HCC: recommendations from a multidisciplinary working group. HPB. 2022, 24:1007-1018. [CrossRef]
- L. Crocetti, E. Bozzi, P. Scalise et al.: Locoregional Treatments for Bridging and Downstaging HCC to Liver Transplantation. Cancers (Basel). 2021, 13. [CrossRef]
- F. Y. Yao, L. Ferrell, N. M. Bass et al.: Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001, 33:1394-403. [CrossRef]
- M. Reig, A. Forner, J. Rimola et al.: BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022, 76:681-693. [CrossRef]
- J. Lindemann, J. Yu, and M. M. B. Doyle: New horizons in liver transplantation for hepatocellular carcinoma. S Afr J Surg. 2024, 62:8-12.
- V. Mazzaferro, E. Regalia, R. Doci et al.: Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996, 334:693-9. [CrossRef]
- W. H. She and T. T. Cheung: Bridging and downstaging therapy in patients suffering from hepatocellular carcinoma waiting on the list of liver transplantation. Translational Gastroenterology and Hepatology. 2016, 1. [Online]. Available: https://tgh.amegroups.org/article/view/3569.
- K. K. Lee, D. G. Kim, I. S. Moon et al.: Liver transplantation versus liver resection for the treatment of hepatocellular carcinoma. J Surg Oncol. 2010, 101:47-53. [CrossRef]
- S. Tamura, Y. Sugawara, and N. Kokudo: Living donor liver transplantation for hepatocellular carcinoma: the Japanese experience. Oncology. 2011, 81 Suppl 1:111-5. [CrossRef]
- E. Tsochatzis, E. Fatourou, rsquo et al.: Transarterial chemoembolization and bland embolization for hepatocellular carcinoma. World Journal of Gastroenterology. 2014, 20:3069-3077. [CrossRef]
- M. Ravaioli, G. L. Grazi, G. Ercolani et al.: Partial necrosis on hepatocellular carcinoma nodules facilitates tumor recurrence after liver transplantation. Transplantation. 2004, 78:1780-6. [CrossRef]
- K. Sasaki, L. I. Ruffolo, M. H. Kim et al.: The Current State of Liver Transplantation for Colorectal Liver Metastases in the United States: A Call for Standardized Reporting. Ann Surg Oncol. 2023, 30:2769-2777. [CrossRef]
- S. Tzedakis, A. Sebai, H. Jeddou et al.: Resection Postradioembolization in Patients With Single Large Hepatocellular Carcinoma. Ann Surg. 2023, 278:756-762. [CrossRef]
- T. Baker, P. Tabrizian, I. Zendejas et al.: Conversion to resection post radioembolization in patients with HCC: recommendations from a multidisciplinary working group. HPB (Oxford). 2022, 24:1007-1018. [CrossRef]
- X. Wu, A. Kwong, M. Heller et al.: Cost-effectiveness analysis of interventional liver-directed therapies for downstaging of HCC before liver transplant. Liver Transpl. 2024, 30:151-159. [CrossRef]
- H. Bismuth, P. E. Majno, and R. Adam: Liver transplantation for hepatocellular carcinoma. Semin Liver Dis. 1999, 19:311-22. [CrossRef]
- T. Shimamura, N. Akamatsu, M. Fujiyoshi et al.: Expanded living-donor liver transplantation criteria for patients with hepatocellular carcinoma based on the Japanese nationwide survey: the 5-5-500 rule - a retrospective study. Transpl Int. 2019, 32:356-368. [CrossRef]
- A. Bharat, D. B. Brown, J. S. Crippin et al.: Pre-liver transplantation locoregional adjuvant therapy for hepatocellular carcinoma as a strategy to improve longterm survival. J Am Coll Surg. 2006, 203:411-20. [CrossRef]
- Y. X. Gao, Q. Q. Ning, P. X. Yang et al.: Recent advances in recurrent hepatocellular carcinoma therapy. World J Hepatol. 2023, 15:460-476. [CrossRef]
- W. Abdelhamed and M. El-Kassas: Hepatocellular carcinoma recurrence: Predictors and management. Liver Research. 2023, 7:321-332. [CrossRef]
- Y. Takahashi, Y. Nishimoto, T. Matsuura et al.: Surgical complications after living donor liver transplantation in patients with biliary atresia: a relatively high incidence of portal vein complications. Pediatr Surg Int. 2009, 25:745-51. [CrossRef]
- U. Cillo and L. Carlis, Liver Transplantation and Hepatobiliary Surgery Interplay of Technical and Theoretical Aspects: Interplay of Technical and Theoretical Aspects. 2020.
- E. Giustiniano, F. Nisi, L. Rocchi et al.: Perioperative Management of Complex Hepatectomy for Colorectal Liver Metastases: The Alliance between the Surgeon and the Anesthetist. Cancers (Basel). 2021, 13. [CrossRef]
- J. Figueras, E. Jaurrieta, C. Valls et al.: Resection or transplantation for hepatocellular carcinoma in cirrhotic patients: outcomes based on indicated treatment strategy. J Am Coll Surg. 2000, 190:580-7. [CrossRef]
- Y. Jiang, X. Dong, Y. Zhang et al.: Navigating the complexities: challenges and opportunities in conversion therapy for advanced hepatocellular carcinoma. Clinical and Experimental Medicine. 2025, 25:169. [CrossRef]
Figure 1.
Kaplan-Meier survival curves comparing liver resection and living donor liver transplantation (LDLT).
Figure 1.
Kaplan-Meier survival curves comparing liver resection and living donor liver transplantation (LDLT).
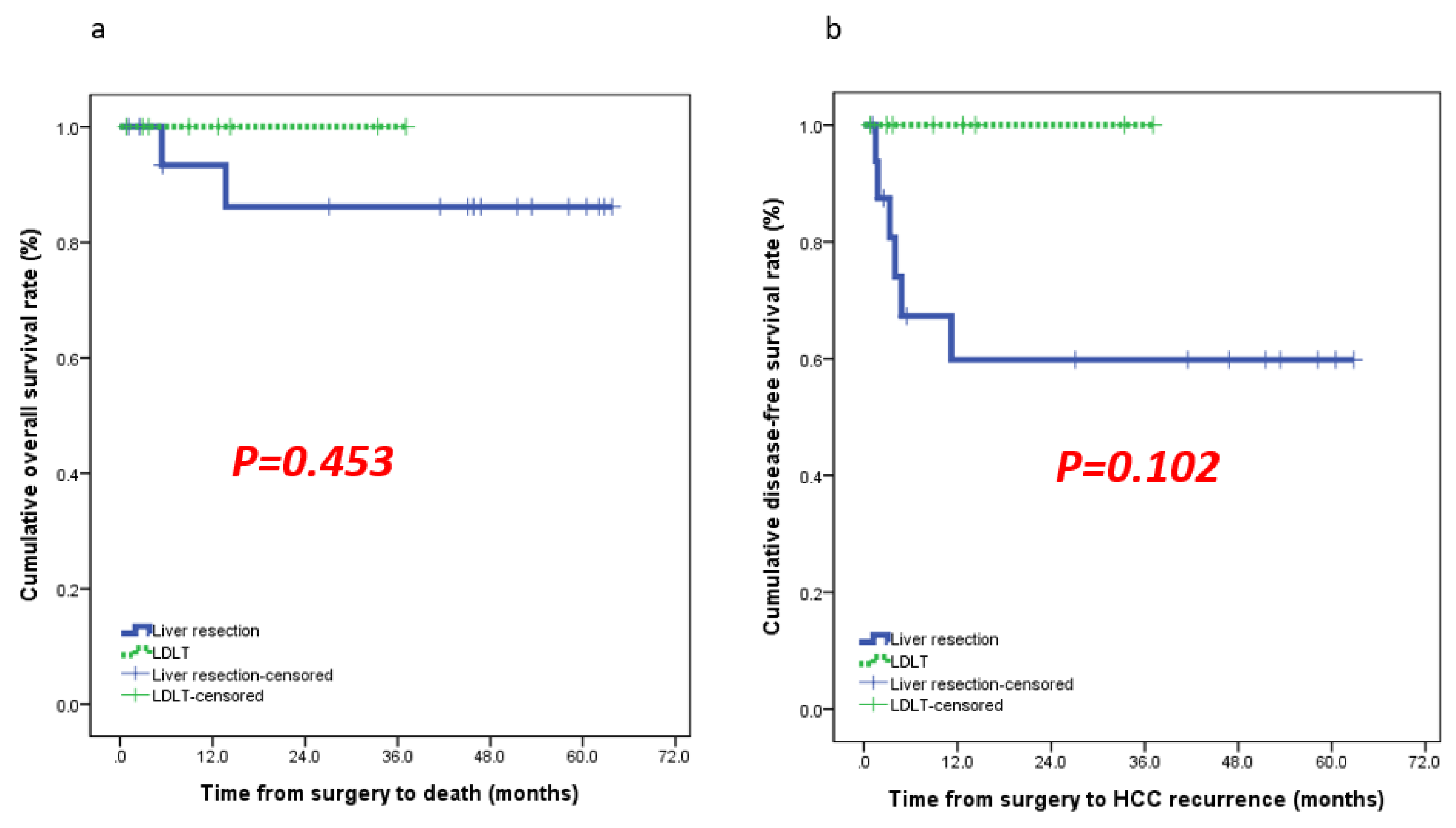

Table 1.
Baseline Demographic Data.
| Parameters | Surgical Resection | LDLT | p-Value |
|---|---|---|---|
| (n=17) | (n=8) | ||
| Sex (Male) | 16 (94.1%) | 6 (75.0%) | 0.231 |
| Age (Years) | 61 (37-78) | 57 (41-71) | 0.673 |
| BMI (kg/m²) | 25.3 (19.5-32.1) | 22.3 (16.1-29.8) | 0.673 |
| WBC (×10⁹/L) | 5,020 (1,930-13,100) | 5,045 (1,710-13,010) | 1.000 |
| NLR | 0.40 (0.09-1.01) | 0.31 (0.06-0.59) | 0.673 |
| Hemoglobin (g/dL) | 13.5 (9.7-15.9) | 12.1 (6.5-17.0) | 1.000 |
| Total bilirubin (mg/dL) | 0.6 (0.2-1.4) | 2.9 (0.3-20.8) | 0.081 |
| AST (U/L) | 27 (15-62) | 33 (18-300) | 0.389 |
| ALT (U/L) | 20 (9-69) | 26 (12-140) | 0.411 |
| INR | 1.01 (0.89-1.12) | 1.16 (0.96-1.45) | 0.010 |
| Creatinine (mg/dL) | 0.78 (0.61-1.68) | 0.74 (0.50-2.37) | 0.673 |
| CRP (mg/L) | 0.47 (0.09-6.85) | 0.19 (0.03-6.76) | 0.637 |
| Time from TARE to surgery (months) | 8.9 (5.6–34.0) | 10.7 (5.8–29.2) | 0.411 |
| Radiation lobectomy | 5 (29.4%) | 0 (0%) | 0.140 |
| Scheduled surgery | 8 (47.1%) | 2 (25.0%) | 0.402 |
| Initial AFP (ng/mL) | 7.8 (1.3–2,751) | 3.6 (2.4–21.0) | 0.042 |
| Initial PIVKA-II (mAU/mL) | 941 (19–49,984) | 15 (9–189) | 0.002 |
| Preoperative AFP (ng/mL) | 4.3 (2.4–149.3) | 3.7 (1.6–145.0) | 0.234 |
| Preoperative PIVKA-II (mAU/mL) | 40 (14–486) | 50 (18–28,293) | 1.000 |
| ASA 1 2 3 |
0 17(100%) 0 |
1(12.5%) 2(25%) 5(62.5%) |
Table 2.
Tumour & Pathology Features.
| Tumour & Pathology Features | |||
|---|---|---|---|
| Parameters | Surgical resection | LDLT | p-value |
| (n=17) | (n=8) | ||
| Maximum tumor size (cm) | 4.2 (1.5–12.5) | 4.5 (1.0–16.2) | 1.000 |
| Tumor number (solitary) | 14 (82.4%) | 2 (25.0%) | 0.012 |
| Tumor grade III | 1 (9.1%) | 0 (0%) | 0.539 |
| Microvascular invasion | 4 (23.5%) | 6 (75.0%) | 0.028 |
| Serosal involvement | 1 (5.9%) | 2 (25.0%) | 0.231 |
| Intrahepatic metastasis | 3 (17.6%) | 6 (75.0%) | 0.010 |
| Tumor necrosis | |||
| Total | 9 (52.9%) | 5 (62.5%) | |
| 5 0–99% | 7 (41.2%) | 1 (12.5%) | 0.171 |
| <50% | 1 (5.9%) | 2 (25.0%) | |
| Follow-up duration(months) | 45.8 (1.1–63.8) | 10.8 (0.8–37.1) | 0.030 |
Table 3.
Tumor Necrosis (T/N) Summary of Transarterial Radioembolization.
| Tumor Necrosis (T/N) | Number of Cases (n) | Mean T/N Ratio | Radiation Dose (Gy) | Complications Observed |
|---|---|---|---|---|
| Near-complete / Complete | 14 | 7.8 | 462 ± 150 | None reported; mild LFT elevation in a few cases, Radiation pneumonia |
| Partial | 8 | 4.9 | 270 ± 120 | Mild abdominal pain in 2 cases, otherwise none |
| Minimal / Poor | 3 | 2.5 | 122 ± 50 | None reported |
Table 4.
Clinical characteristics, treatment details, and outcomes of patients who underwent transarterial radioembolization (TARE).
Table 4.
Clinical characteristics, treatment details, and outcomes of patients who underwent transarterial radioembolization (TARE).
| Pt. No | TARE Reason | TARE Side Effects | Procedure | Initial | Pre-op | Y-90 Dose (GBq) | Tumour Radiation Dose (Gy) | TTS | TTR | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AFP | PIVKA-II | AFP | PIVKA-II | ||||||||
| 1 | AAA | Renal dysfunction, myalgia | TARE | 1.3 | 13235 | 8.1 | 394 | Multiple infusions | N/A | 7.1 | 10.3 |
| 2 | Satellite nodules | none | TARE | 17.3 | 193 | 149.3 | 25 | N/A | N/A | 10.8 | 12.2 |
| 3 | Satellite nodules, small remnant liver volume | LFT elevation, Fever | TARE | 5.5 | 30324 | 4.3 | 20 | Resin-type | N/A | 6.1 | 68.8 |
| 4 | Satellite nodule | none | TACE + TARE | 50.4 | 49984 | 2.6 | 113 | 3.7 | 170 | 8 | 12 |
| 5 | small remnant volume | nausea, vomiting, poor oral intake | Selective TARE | 1.3 | 105 | 2.4 | 32 | 36 | N/A | 6.3 | 66.7 |
| 6 | Satellite nodules, small remnant liver volume, stomach cancer | nausea, vomiting, pain | TARE | 2751 | 941 | 3.8 | 33 | 2.8 | 413.69 | 10.0 | 68.1 |
| 7 | small remnant volume | Generalized abdominal discomfort | TARE + cTACE | 5.5 | 1242 | 6 | 40 | Resin-type | N/A | 5.6 | 58.9 |
| 8 | PVTT, irregular mass, satellite nodules | none | TARE Segmentectomy | 3 | 1357 | 3 | 184 | Glass-type | N/A | 6.7 | 8.5 |
| 9 | Two HCC | none | Selective TARE | 8.6 | 1460 | 6.9 | 31 | 4.62 | 344 _ 120 | 11.5 | 62.9 |
| 10 | Satellite nodule | none | Right Lobar TARE | 16.3 | 709 | 6.8 | 56 | 4.42 | 120 _ 240 | 7.1 | 53.8 |
| 11 | Infiltrative HCC with PVTT | none | TARE | 16.9 | 7231 | 2.5 | 63 | 3 + 10 | 120 _ 240 | 34.0 | 38.8 |
| 12 | Large HCC, satellite nodules | Radiation pneumonia | TARE | 32 | 1141 | 4.1 | 17 | 3.9 | 122 _ 211.9 | 7.4 | 18.6 |
| 13 | small remnant volume | none | Right Lobar TARE | 1121 | 297 | 10.7 | 44 | 2.5 | 269.7 | 8.9 | 50.4 |
| 14 | PCI unstable angina., DM, advanced LC (Plt 69,000) | none | TARE | 6.3 | 706 | 5.3 | 14 | 5 | 216 – 233 | 18.3 | 45.4 |
| 15 | Multiple HCC, irregular margin | none | Right Lobar TARE | 21 | 11 | 145 | 38 | 4 | 354.4 | 10.8 | 23.5 |
| 16 | Multiple HCC | none | TARE Segmentectomy | 3.2 | 12 | 3.6 | 61 | 22 | 250 _ 240 | 29.2 | 66.2 |
| 17 | Multiple HCC | none | TARE Segmentectomy | 2.4 | 12 | 1.9 | 18 | 2.01 | 120 _ 240 | 25.3 | 58.6 |
| 18 | Multiple HCC | none | TARE + cTACE | 5.1 | 18 | 4 | 37 | 5.23 | 420 | 6.0 | 20.2 |
| 19 | Multiple HCC | none | Right Lobar TARE | 2.5 | 162 | 3.8 | 1271 | 5.8 | 164.03 | 15.3 | 18.2 |
| 20 | Multiple HCC | none | Segmental TARE | 7.8 | 69 | 17.9 | 486 | 3.98 | 625 | 14.3 | 16.8 |
| 21 | Multiple HCC | none | Segmental TARE | 3.5 | 19 | 4.1 | 19 | 4.18 | 907 _ 403 | 15.5 | 16.6 |
| 22 | Multiple HCC | none | Right Lobar TARE | 5.1 | 17 | 12.6 | 68 | 5.01 | 462 | 5.8 | 14.7 |
| 23 | Multiple HCC | none | TARE Segmentectomy | 2.2 | 26 | 4.1 | 44 | 3.98 | 603 | 9.0 | 14.5 |
| 24 | Multiple HCC | none | TARE Segmentectomy | 3.9 | 9 | 1.6 | 24 | 7.95 | 618 | 10.6 | 14.3 |
| 25 | Multiple HCC | none | TARE | 3.2 | 189 | 1.6 | 28293 | N/A | N/A | 9.1 | 9.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



