
Submitted:
05 November 2025
Posted:
06 November 2025
You are already at the latest version
Abstract
Atrial fibrillation (AF), the most common cardiac arrhythmia, is associated with an increased risk of stroke and heart failure, with both genetic and environmental factors contributing to its pathophysiology. Emerging evidence suggests that KCNH2 gene dysregulation may play a role in arrhythmogenesis, yet data in African populations remain limited. This study investigated KCNH2 gene expression in AF patients and its association with clinical and laboratory parameters. In a matched case–control design at Aminu Kano Teaching Hospital, Nigeria, 25 participants (14 AF patients and 11 age-matched controls) were enrolled. Peripheral blood was collected for RNA extraction and lipid profiling. KCNH2 expression was quantified using reverse transcription real-time PCR, and relative fold changes were calculated via the 2^−ΔΔCt method. Compared with controls, AF patients exhibited significantly higher total cholesterol, LDL cholesterol, and triglyceride levels (p ≤ 0.029). KCNH2 expression was markedly reduced in AF patients, with a 17-fold decrease (median 0.12, IQR 0.04–0.71) versus controls (2.06, IQR 1.30–2.85; p < 0.001). QTc intervals were significantly prolonged in AF patients, and serum triglycerides were negatively correlated with KCNH2 expression (r = –0.472, p = 0.003). These findings suggest that downregulation of KCNH2, in combination with lipid abnormalities and QTc prolongation, may contribute to AF pathogenesis, highlighting the potential utility of molecular and metabolic profiling in risk assessment and precision management of AF.
Keywords:
atrial fibrillation
; KCNH2 gene
; lipid profile
; QTc interval
; cardiovascular risk
1. INTRODUCTION
Atrial fibrillation (AF) is the most prevalent form of sustained cardiac arrhythmia, affecting an estimated 46.3 million individuals worldwide and significantly contributing to stroke, heart failure, and mortality [1,2,3]. In sub-Saharan Africa, AF prevalence is approximately 4.6% [4], with a hospital-based study in Nigeria reporting 3.76% [5]. AF is associated with life-threatening complications, including ventricular tachycardia, sudden cardiac death, coronary artery disease, myocardial infarction, and dementia [6]. Its pathophysiology is complex, involving electrical, structural, and molecular remodeling of atrial tissue [7], with genetic factors—particularly ion channel–encoding genes—playing a significant role [8].
AF can affect individuals across all age groups and often remains undiagnosed due to its asymptomatic and paroxysmal presentation [9]. Limited access to cardiovascular and genetic screening in low-resource settings exacerbates this diagnostic gap [10]. Despite advances in 12-lead electrocardiography, Holter monitoring, echocardiography, and wearable cardiac sensors [11], detection of paroxysmal AF remains suboptimal. Integrating genetic biomarkers could enhance early AF detection, risk stratification, and precision-based management.
KCNH2 encodes the α-subunit of the hERG potassium channel, which mediates the rapid component of the delayed rectifier potassium current (I_Kr), critical for atrial and ventricular repolarization [12]. Mutations or dysregulation of KCNH2 are implicated in arrhythmogenic disorders, including long QT syndrome (LQTS) and AF [13]. However, few studies have evaluated KCNH2 transcription in peripheral blood or atrial tissue, particularly in African populations. Reduced KCNH2 expression has been linked to ventricular arrhythmias and sudden cardiac death [3,4].
Antiarrhythmic medications, especially Class III agents such as amiodarone, act primarily by inhibiting hERG potassium channels, prolonging the cardiac action potential but increasing QT interval (QTc) and torsade de pointes risk [14]. The association between KCNH2 gene expression and AF remains poorly characterized, particularly in resource-limited settings such as Nigeria. This study investigated KCNH2 gene expression in AF patients and explored its relationship with selected cardiovascular parameters. We hypothesized that altered KCNH2 expression is significantly associated with AF and its clinical manifestations, potentially serving as a biomarker for early diagnosis and risk stratification.
2. METHODOLOGY
Study Design and Participants:
This is a hospital-based matched case‒control study conducted on patients with an AF diagnosis between October 2024 and December 2024 at the Department of Internal Medicine, Aminu Kano Teaching Hospital (AKTH), Kano, Nigeria. Patients with AF who received care at the cardiology clinic were recruited. The minimum required sample size for the study was determined via the standard Cochran formula. Age-matched controls were selected from patients visiting the general outpatient department (GOPD) of the same hospital as long as they did not have cardiovascular conditions/complaints, had no relationship with cases and had no family history of AF. Eligible participants included 14 cases and 11 controls.
Inclusion criteria:
Patients aged 18 years and above with a confirmed diagnosis of AF who were stable at the time of the study were enrolled as cases. Patients presenting with GOPD with non-cardiovascular complaints were recruited as controls.
Exclusion criteria:
We excluded patients with decompensated heart failure or any other clinical emergency condition. Patients (both cases and controls) with a known history of cigarette smoking, alcohol consumption, chronic medical conditions (including diabetes and hyperthyroidism) and pregnant women were excluded from the study.
Data collection:
Data were collected via a structured data capture form. Clinical parameters, such as heart rate (HR), blood pressure (BP), and corrected QT interval (QTc) were obtained from hospital records at the time of diagnosis, i.e., when the patients were first diagnosed with AF and recorded again at the time of enrolment in this study, i.e., while they were already on treatment (during the study period). BP and HR were measured via a digital sphygmomanometer with an integrated heart rate monitor. Additionally, comprehensive records of medications prescribed to patients were documented to assess potential therapeutic influences.
Sample collection and processing:
Venous blood samples (5 mL) were collected from each study participant. Two millilitres (2 mL) were transferred into EDTA tubes, and the remaining 3 mL was transferred into plain tubes for serum analysis. The EDTA samples were immediately preserved in RNAlater® solution and transported to the laboratory for RNA extraction and KCNH2 gene expression analysis. The blood in the plain tube was centrifuged at 3,500 rpm for 15 minutes to separate the serum, which was subsequently used for lipid profile assessment.
Lipid profile analysis:
Direct enzymatic methods were used to measure HDL, triglycerides, and total cholesterol. For HDL-cholesterol, the reagent was prepared by mixing R1a with R1b solutions. Test tubes were labelled as blank, standard, and test, and 1,000 µL of reagent was added to each tube. Serum (100 µL) was added to the test tube, 100 µL of lipid calibrator was added to the standard tube, and 100 µL of distilled water was added to the blank. The mixture was incubated at 37 °C for 5 minutes, and the absorbance was measured within 60 minutes. The HDL concentration was calculated by comparing the absorbance of the sample to that of the standard and multiplying it by the known concentration of the standard. For triglycerides and total cholesterol, test tubes were similarly labelled, and 1,000 µL of reagent was added to each tube. Serum, a lipid calibrator, and distilled water (10 µL each) were added to the respective tubes. After incubation at 37 °C for 5 minutes, the absorbance was measured, and the concentrations were determined via the same method as that used for HDL, with the sample’s absorbance being compared with that of the standard.
LDL cholesterol (LDL-C) was estimated via Friedewald’s equation, which calculates LDL levels by subtracting the contribution of HDL cholesterol and a fraction of triglycerides from the total cholesterol value.
RNA Extraction:
Total RNA was extracted from blood samples via the Prime Way Total RNA Extraction Kit (Canada). Briefly, 200 µL of blood was lysed at room temperature with lysis buffer, and the lysate was transferred to a spin column before centrifugation at 12,000 × g for 1 minute. The RNA was bound to the column, washed multiple times to remove contaminants, and treated with DNase to eliminate genomic DNA. Finally, the RNA was eluted in 60 µL of elution buffer and stored at -80 °C before the gene expression assay.
KCNH2 gene Expression Using Two-Steps qRT-PCR:
KCNH2 gene expression was analysed via two-step reverse transcription‒quantitative polymerase chain reaction (qRT‒PCR). First, reverse transcription was conducted via the FIRE Script RT-cDNA Synthesis Kit (Solis Bio Dyne, Estonia) for cDNA synthesis under the following conditions: reverse transcription at 50 °C for 30 minutes, followed by enzyme inactivation at 85 °C for 5 minutes. The cDNA was stored at -80 °C. qPCR was conducted via specific primers and probes for the KCNH2 gene and GAPDH (housekeeping gene). The qPCR protocol included initial activation at 95 °C for 2 minutes, denaturation at 95 °C for 10 seconds, annealing at 60 °C for 20 seconds, and extension at 72 °C for 1 minute.
Primer and probe sequences:
KCNH2 gene-specific primer (NM_000238.1):
Forward primer: 5’-TGAAGGAGACGGAAGAAGG-3’
Reverse primer: 5’-TGGTGCGGAAGTTGATGAG-3’
Kcnh2-gene Probe: TGGCTACGCCTGCCAGCCGC
GAPDH:
Forward primer: 5’-TGACTTCAACAGCGACACC-3’
Reverse primer: 5’-TCTCTCTTCCTCTTGTGCTC-3’
Probe: TGCCCTCAACGACCACTTTGTCAAGCTCATTTCC
The cycle threshold (CT) obtained from the qPCR was used to calculate the relative fold change in KCNH2 gene expression via the ΔΔCt method, with GAPDH serving as the reference gene.
FC = 2(-∆∆Ct)
Were
∆∆Ct = (Cttarget, treated - Ctref, treated) – (Cttarget, control –Ctref, control)
Study variables:
Outcome Variable (also defined as cases): AF
Exposure Variable: The primary exposure of interest was the relative fold change in KCNH2 gene expression.
Explanatory variables: We selected the following variables on the basis of the literature: age (27--70 years), sex (male or female), marital status (single, married, widow/widower, divorced), class of antiarrhythmic drugs (class I--III), family history of atrial fibrillation, heart failure, sudden cardiac death (yes, no), systolic and diastolic blood pressure, heart rate, pulse rate, triglycerides, total cholesterol, HDL cholesterol and LDL cholesterol.
Data Analysis:
All analyses were executed via R statistical software, version 4.4.3, with a type 1 error rate set at 5% (α = 0.05). Descriptive statistics summarized patient demographics and clinical variables. Continuous variables are presented as the means and standard deviations (SDs) or medians and interquartile ranges (IQRs) depending on the normality of the data, which were assessed via the Shapiro‒Wilk test. Categorical variables are presented as frequencies and percentages.
Bivariate associations between case‒control status and categorical independent variables were assessed using the McNemar’s test since cases were matched with controls. For continuous variables, including KCNH2 gene expression, comparisons between cases and controls were performed via paired samples t tests. Additionally, boxplots were used to visually compare KCNH2 gene expression levels between the two groups. The QTc intervals of the AF patients at the time of diagnosis and during the study period were also compared paired sample t-test.
The correlation between KCNH2 relative fold change and the explanatory variables was examined via Pearson’s correlation (for normally distributed variables) or Spearman’s correlation (for non-normally distributed variables). These correlations were graphically illustrated via a correlation matrix plot. Statistically significant correlations were further visualized via scatter plots with regression lines and p values.
Ethical clearance:
Ethical approval for this study was obtained from the Health Research Ethics Committee of Aminu Kano Teaching Hospital (AKTH) (AKTH/MAC/SUB/12A/P-3/V1/3817). Written informed consent was obtained from all participants before enrolment in the study.
3. RESULT
3.1. Participant Characteristics
A total of 25 participants were enrolled in this study, comprising 14 patients with atrial fibrillation (AF) and 11 age-matched controls without AF. The mean age of AF patients was 53.4 ± 16.87 years, compared with 43.8 ± 15.99 years among controls (Table 1; p = 0.082).
The distribution of sex and marital status was similar between the groups. Males constituted 57.14% of the AF group and 54.55% of controls, while married individuals accounted for 71.43% of AF patients and 65.00% of controls.
A significant difference was observed in the family history of AF, which was reported in 42.86% of cases but absent among controls (p = 0.020). Although 28.57% of AF patients reported a family history of heart failure, the difference was not statistically significant (p = 0.112).
Exposure to antiarrhythmic drugs was exclusive to the AF group, with varying combinations of Class II, Class III agents, and digoxin. No significant difference was observed in the family history of sudden cardiac death (p > 0.9).
3.2. Physical Examination and Lipid Profile
All AF patients exhibited irregular pulse rhythms, while all controls demonstrated regular rhythms (p < 0.001). The lipid profile analysis revealed higher levels of total cholesterol, triglycerides, and LDL cholesterol in AF patients compared with controls, with all three showing statistically significant differences (Table 2). HDL cholesterol did not differ significantly (p > 0.9).
3.3. KCNH2 Gene Expression
The real-time PCR amplification plots for KCNH2 and GAPDH are presented in Figure 1 and Figure 2, respectively.
A 17-fold reduction in KCNH2 gene expression (relative fold change) was observed in AF patients (0.12, IQR: 0.04–0.71) compared with controls (2.05, IQR: 1.30–2.85), a difference that was highly significant (p < 0.001) (Figure 3).
3.4. Comparison of Cardiovascular Parameters at Diagnosis and During Study
Among AF patients, QTc intervals were significantly prolonged during the study period (500.00 ± 13.00 ms) compared with baseline diagnosis (346.14 ± 48.37 ms, p < 0.001). The heart rate significantly decreased from 131.43 ± 14.36 bpm at diagnosis to 72.71 ± 14.09 bpm during the study (p < 0.001). No significant differences were observed in systolic and diastolic blood pressures (p > 0.05).

Table 3.
Comparison of cardiovascular parameters at diagnosis and during the study among AF patients.
Table 3.
Comparison of cardiovascular parameters at diagnosis and during the study among AF patients.
| Parameters | At Diagnosis | During study period | P-value |
| SBP (mmHg) | 134.29±43.916 | 111.29±27.585 | 0.131 |
| DBP (mmHg) | 86.57±30.588 | 76.57±19.104 | 0.337 |
| Heart-rate (b/min) | 131.43±14.363 | 72.71±14.092 | 0.000* |
| QTc-Interval (ms) | 346.14±48.368 | 500±13.000 | 0.000* |
| Paired sample T-test |
3.5. Correlation Analysis
Correlation analysis revealed a moderate negative correlation between KCNH2 gene expression and serum triglyceride levels (r = –0.472, p = 0.003), indicating that higher triglyceride levels were associated with reduced KCNH2 expression (Figure 4). No other clinical or laboratory variables demonstrated significant associations.
Table 4.
Correlation of KCNH2 gene expression with cardiovascular and metabolic parameters.
| Clinical Parameter | Correlation with KCNH2 Expression (r) | p-value |
| Heart Rate (HR) | -0.270 | 0.559 |
| Systolic Blood Pressure (SBP) | -0.539 | 0.212 |
| Diastolic Blood Pressure (DBP) | -0.378 | 0.620 |
| LDL Cholesterol | 0.003 | 0.990 |
| HDL Cholesterol | -0.200 | 0.323 |
| Triglycerides | -0.472 | 0.003* |
| Total Cholesterol | -0.066 | 0.755 |
| QTc Interval | -0.470 | 0.912 |
* indicates a significant correlation.
4. Discussion
This study provides insights into the role of KCNH2 gene expression in the pathogenesis of atrial fibrillation (AF) in an African population. We observed significant downregulation of KCNH2 in AF patients compared with matched controls, suggesting a potential molecular mechanism contributing to AF in this population. Our results also highlight the interplay between KCNH2 expression and clinical and laboratory parameters that influence AF outcomes.
The mean age of AF patients in this study was 53.4 years (±16.87), consistent with reports of a younger AF presentation among Africans (~59.8 years) compared with Caucasians (~80 years) [16,17]. This may reflect shorter life expectancy, different genetic backgrounds, or earlier exposure to risk factors in African populations. The male predominance in the AF group aligns with the well-documented higher incidence of AF among men, attributed to social, hormonal, and electrophysiological sex differences, including the cardioprotective effects of estrogen in women [19,20,21,22].
A noteworthy social characteristic in our cohort was the higher proportion of married AF patients. This may suggest a role of psychosocial factors in AF progression, as social support has been linked to better management of chronic diseases [23]. Further studies are needed to explore the influence of marital status on AF outcomes.
A family history of AF was significantly associated with disease status; 42% of AF patients reported a positive history compared with none in the control group. This supports the role of genetic predisposition in AF pathophysiology [1,8]. Similarly, 28.6% of AF patients reported a family history of heart failure, suggesting a shared pathophysiological basis, including atrial remodelling and fibrosis [24]. No significant differences were observed for family history of sudden death, possibly due to the limited sample size.
The significant downregulation of KCNH2 supports its potential role in AF pathogenesis. KCNH2 encodes the hERG potassium channel, crucial for cardiac repolarization. Reduced expression may impair ion channel function, resulting in prolonged QT intervals, early afterdepolarizations, and increased susceptibility to arrhythmias [8]. Assessment of the corrected QT interval (QTc) during follow-up revealed significant prolongation, corroborating the functional impact of reduced KCNH2 expression on ventricular repolarization and potential risk for ventricular tachycardia and sudden cardiac death (SCD). Notably, three AF patients who died during follow-up exhibited the most pronounced downregulation of KCNH2, suggesting a possible dose–response relationship between gene expression and fatal arrhythmic events.
Use of Class III antiarrhythmic drugs, such as amiodarone, may contribute to reduced KCNH2 expression, as these agents are known to suppress transcription [29]. This underscores the importance of routine ECG and QTc monitoring in AF patients receiving potassium channel blockers to mitigate the risk of excessive QT prolongation and arrhythmic complications.
Although there was a trend toward lower KCNH2 expression in female patients, this was not statistically significant. Previous studies have reported sex-based differences in potassium current densities, potentially influenced by estrogen [19,20]. Larger studies are warranted to explore sex-specific patterns of KCNH2 expression in African populations.
Significant elevations in total cholesterol, triglycerides, and LDL-C were observed in AF patients compared with controls. Reduced atrial contraction and impaired perfusion of organs involved in lipid metabolism may contribute to these alterations. Hyperlipidaemia may also promote AF via atherosclerosis, inflammation, oxidative stress, electrophysiological changes, and autonomic imbalance [30]. Importantly, KCNH2 expression correlated negatively with serum triglyceride levels, suggesting a potential metabolic influence on ion channel regulation and AF risk.
LIMITATIONS
While this study provides valuable insights into the association between KCNH2 gene expression and AF, a few limitations should be noted. The sample size, although adequate for initial observations, may limit the generalizability of the findings across a broader population. Additionally, we did not investigate specific KCNH2 gene variants, which could further elucidate the mechanisms influencing gene expression. These considerations highlight the need for larger, variant-inclusive studies to build on our findings.
CONCLUSION
This study revealed significant downregulation of KCNH2 gene expression in patients with AF compared with non-AF controls, suggesting a potential role of the KCNH2 gene in the pathogenesis of AF in the African population. The elevated lipid profile and the strong negative correlation between serum triglyceride levels and KCNH2 expression further support a possible metabolic influence and negative effect of hyperlipidaemia on gene regulation, which may contribute to increased arrhythmogenic risk. Additionally, the prolongation of QTc observed in AF patients on treatment with class III antiarrhythmic drugs confirms the impact of decreased KCNH2 gene expression on cardiac electrophysiology and underscores the importance of regular QTc monitoring in AF patients to prevent and minimize the risk of ventricular arrhythmia and sudden cardiac death. The findings of this study emphasize the potential of this gene as a biomarker for risk stratification and a therapeutic target in AF management.
ACKNOWLEDGEMENTS
The authors sincerely acknowledge the support of the Department of Internal Medicine, Aminu Kano Teaching Hospital, the Kano Independent Research Centre Trust (KIRCT), and the Department of Human Physiology, Bayero University Kano (BUK) for their assistance with participant recruitment, clinical data collection, and laboratory analyses. We acknowledge the Africa Centre of Excellence for Population Health and Policy (ACEPHAP) for funding the gene expression analysis.
Author Contributions
Halima I. Ahmed: Conceptualization, Methodology, Data Collection, Formal Analysis, Writing – Original Draft. Basheer I. Waziri: Study design, Methodology Supervision, Writing – Review & Editing, Corresponding Author. Hassan A. Murtala: Data Curation, Statistical Analysis, Writing – Review & Editing. Nasiru Abdullahi: Review and Editing of Manuscript. Ibrahim Yusuf: Review and Editing of Manuscript. Isah A. Aliyu: Review and Editing of Manuscript. Jameel Ismail: Review and Editing of Manuscript. Shehu A. Kana: Clinical data analysis and Interpretation. Mabruk M. Elkashab: Research concept, Supervision, Manuscript Review. Hamisu M. Salihu: Project Administration, Supervision, Writing – Review & Editing, Approval of Final Manuscript.
Data Availability Statement
All data supporting the findings of this study, including tables and figures, are included within this article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Taizhanova D, Bazarova N, Zholdybayeva E, Kalimbetova A. Association of gene polymorphism at atrial fibrillation: A literature review. J Clin Med Kazakhstan. 2021 Jan 26;18(1):19–22.
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. Circulation. 2019 Mar 5;139(10): e56–528.
- Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014 Feb 25;129(8):837–47.
- Sliwa K, Carrington MJ, Klug E, Opie L, Lee G, Ball J, et al. Predisposing factors and incidence of newly diagnosed atrial fibrillation in an urban African community: insights from the Heart of Soweto Study. Heart Br Card Soc. 2010 Dec;96(23):1878–82.
- Ajayi EA, Adeyeye VO, Adeoti AO. Clinical and Echocardiographic Profile of Patients with Atrial Fibrillation in Nigeria. J Health Sci. 2016;6(3):37–42.
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021 Feb 1;42(5):373–498.
- Nattel S, Heijman J, Zhou L, Dobrev D. Molecular Basis of Atrial Fibrillation Pathophysiology and Therapy: A Translational Perspective. Circ Res. 2020 Jun 19;127(1):51–72.
- Ellinor PT, Lunetta KL, Albert CM, Glazer NL, Ritchie MD, Smith AV, et al. Meta-analysis identifies six new susceptibility loci for atrial fibrillation. Nat Genet. 2012 Apr 29;44(6):670–5.
- Andrade JG, Deyell MW, Verma A, Macle L, Champagne J, Leong-Sit P, et al. Association of Atrial Fibrillation Episode Duration With Arrhythmia Recurrence Following Ablation: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open. 2020 Jul 2;3(7):e208748.
- Berkmen YM, Lande A. Chest roentgenography as a window to the diagnosis of Takayasu’s arteritis. Am J Roentgenol Radium Ther Nucl Med. 1975 Dec;125(4):842–6.
- Jagdesh Kumar, Afshan Nasim, Faraz Farooq Memon, Asad Ali Mahesar, Bilal Ahmad, Ahsan Ali Gaad. 48 hours holter monitoring in detecting occult atrial fibrillation in Adults. Med J South Punjab. 2024 Mar 22;5(01):47–52.
- van den Boogaard M, van Weerd JH, Bawazeer AC, Hooijkaas IB, van de Werken HJG, Tessadori F, et al. Identification and Characterization of a Transcribed Distal Enhancer Involved in Cardiac KCNH2 Regulation. Cell Rep. 2019 Sep 3;28(10):2704-2714.e5.
- Sinner MF, Pfeufer A, Akyol M, Beckmann BM, Hinterseer M, Wacker A, et al. The nonsynonymous coding IKr-channel variant KCNH2 -K897T is associated with atrial fibrillation: results from a systematic candidate gene-based analysis of KCNH2 (HERG). Eur Heart J. 2008 Apr;29(7):907–14.
- Gelman I, Sharma N, Mckeeman O, Lee P, Campagna N, Tomei N, et al. The ion channel basis of pharmacological effects of amiodarone on myocardial electrophysiological properties, a comprehensive review. Biomed Pharmacother. 2024 May 1;174:116513.
- Schnabel RB, Yin X, Gona P, Larson MG, Beiser AS, McManus DD, et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. The Lancet. 2015 Jul 11;386(9989):154–62.
- Akpa MR, Ofori S. Atrial fibrillation: An analysis of etiology and management pattern in a tertiary hospital in Port-harcourt, southern Nigeria. Res J Health Sci. 2015;3(4):303–10.
- Kerr CR, Humphries KH, Talajic M, Klein GJ, Connolly SJ, Green M, et al. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2005 Mar;149(3):489–96.
- Mou L, Norby FL, Chen LY, O’Neal WT, Lewis TT, Loehr LR, et al. Lifetime Risk of Atrial Fibrillation by Race and Socioeconomic Status: ARIC Study (Atherosclerosis Risk in Communities). Circ Arrhythm Electrophysiol. 2018 Jul;11(7):e006350.
- Bai J, Lu Y, Lo A, Zhao J, Zhang H. PITX2 upregulation increases the risk of chronic atrial fibrillation in a dose-dependent manner by modulating IKs and ICaL -insights from human atrial modelling. Ann Transl Med. 2020 Mar;8(5):191.
- Mahmoodzadeh S, Dworatzek E. The Role of 17β-Estradiol and Estrogen Receptors in Regulation of Ca2+ Channels and Mitochondrial Function in Cardiomyocytes. Front Endocrinol. 2019;10:310.
- Malaeb D, Hallit S, Dia N, Cherri S, Maatouk I, Nawas G, et al. Effects of sociodemographic and socioeconomic factors on stroke development in Lebanese patients with atrial fibrillation: a cross-sectional study. F1000Research. 2021;10:793.
- Magnussen C, Niiranen TJ, Ojeda FM, Gianfagna F, Blankenberg S, Njølstad I, et al. Sex Differences and Similarities in Atrial Fibrillation Epidemiology, Risk Factors, and Mortality in Community Cohorts: Results From the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe). Circulation. 2017 Oct 24;136(17):1588–97.
- Valkanova V, Ebmeier KP. Vascular risk factors and depression in later life: a systematic review and meta-analysis. Biol Psychiatry. 2013 Mar 1;73(5):406–13.
- Camm AJ, Lip GYH, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J. 2012 Nov;33(21):2719–47.
- Heijman J, voigt N, Nattel S, Dobrev D. Cellular and Molecular Electrophysiology of Atrial Fibrillation Initiation, Maintenance, and Progression | Circulation Research [Internet]. [cited 2025 Apr 28]. Available from: https://www.ahajournals.org/doi/full/10.1161/CIRCRESAHA.114.302226.
- Varró A, Baczkó I. Cardiac ventricular repolarization reserve: a principle for understanding drug-related proarrhythmic risk. Br J Pharmacol. 2011 Sep;164(1):14–36.
- Zipes, D. P., & Jalife, J. (2017). Cardiac Electrophysiology: From Cell to Bedside (7th ed.). Elsevier. - Google Search [Internet]. [cited 2025 Apr 11]. Available from: https://www.google.com/search?q=Zipes%2C+D.+P.%2C+%26+Jalife%2C+J.+(2017).+Cardiac+Electrophysiology%3A+From+Cell+to+Bedside+(7th+ed.).+Elsevier.&oq=Zipes%2C+D.+P.%2C+%26+Jalife%2C+J.+(2017).+Cardiac+Electrophysiology%3A+From+Cell+to+Bedside+(7th+ed.).+Elsevier.&gs_lcrp=EgZjaHJvbWUyBggAEEUYOTIGCAEQRRhA0gEIMzU0ajBqMTWoAgCwAgA&sourceid=chrome&i.e.,=UTF-8#vhid=zephyr:0&vssid=atritem-https://shop.elsevier.com/books/cardiac-electrophysiology-from-cell-to-bedside/zipes/978-0-323-44733-1.
- Miyasaka Y, Barnes ME, Bailey KR, Cha SS, Gersh BJ, Seward JB, et al. Mortality trends in patients diagnosed with first atrial fibrillation: a 21-year community-based study. J Am Coll Cardiol. 2007 Mar 6;49(9):986–92.
- Sinner MF, Pfeufer A, Akyol M, Beckmann BM, Hinterseer M, Wacker A, et al. The nonsynonymous coding IKr-channel variant KCNH2 -K897T is associated with atrial fibrillation: results from a systematic candidate gene-based analysis of KCNH2 (HERG). Eur Heart J. 2008 Apr;29(7):907–14.
- Li ZZ, Du X, Guo X yuan, Tang R bo, Jiang C, Liu N, et al. Association Between Blood Lipid Profiles and Atrial Fibrillation: A Case‒Control Study. Med Sci Monit Int Med J Exp Clin Res. 2018 Jun 9;24:3903–8.
Figure 1.
Real-time PCR amplification plot of KCNH2 gene.
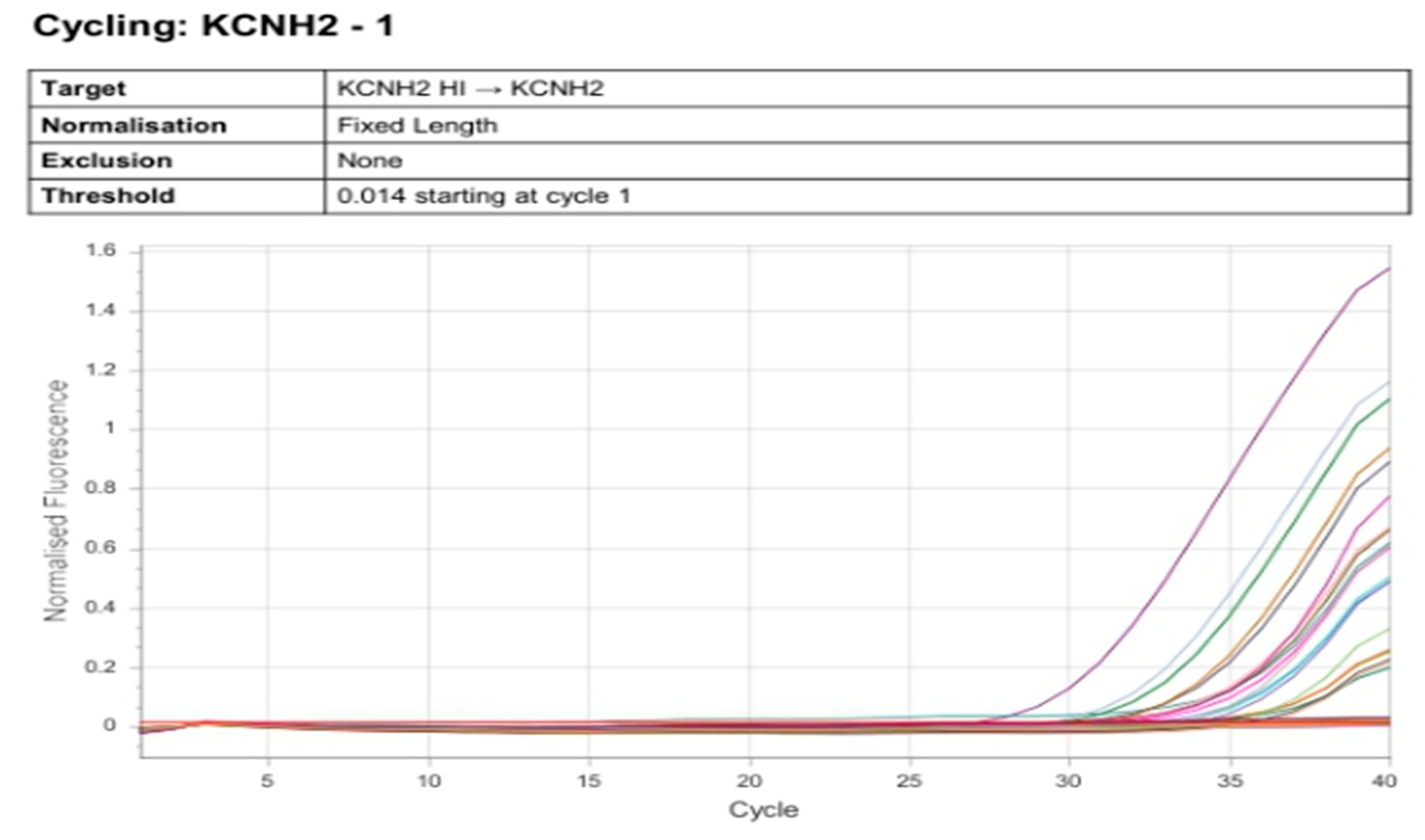
Figure 2.
Real-time PCR amplification plot of GAPDH.
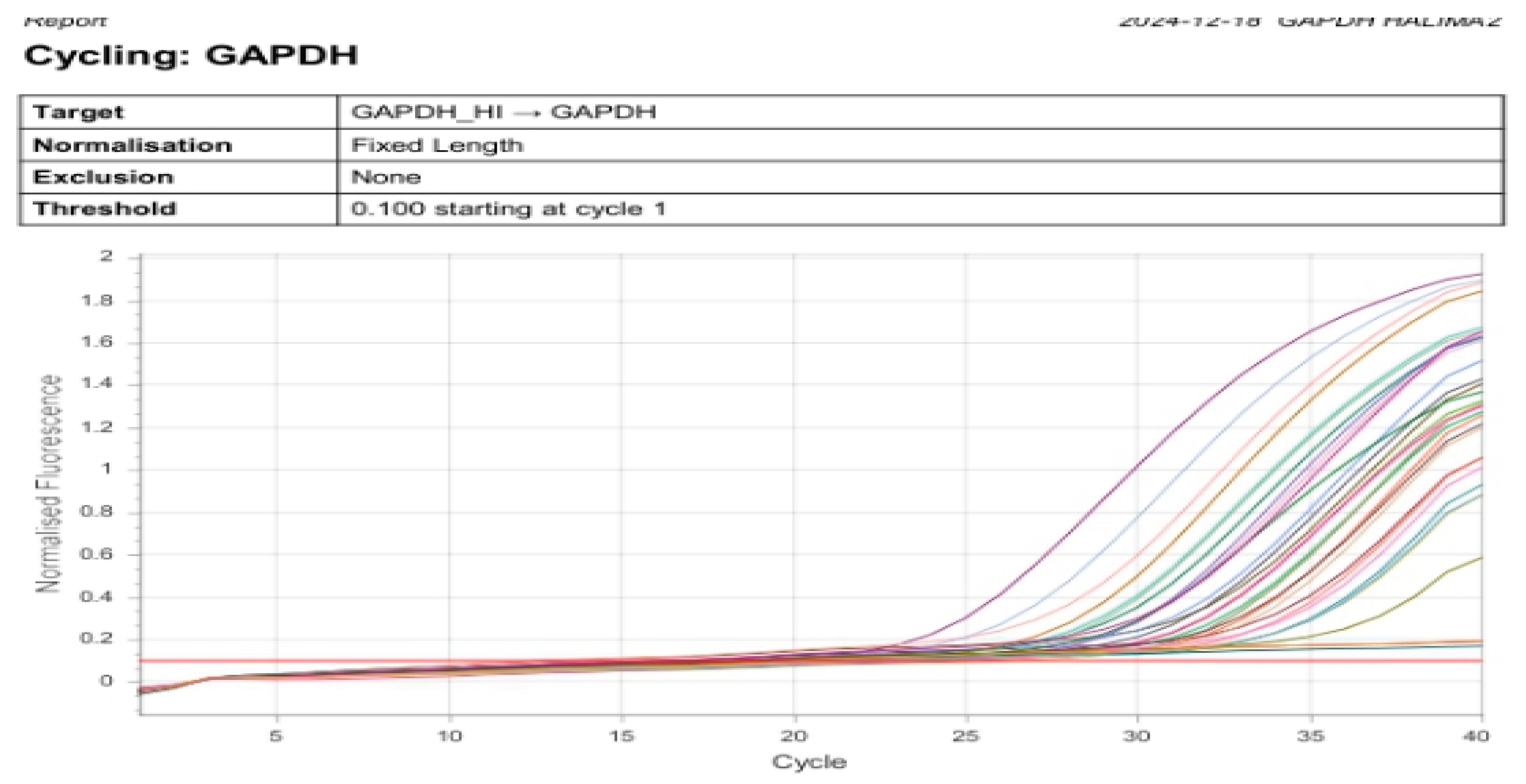
Figure 3.
Comparison of KCNH2 gene expression (relative fold change) between patients AF patients and controls (p < 0.001).
Figure 3.
Comparison of KCNH2 gene expression (relative fold change) between patients AF patients and controls (p < 0.001).
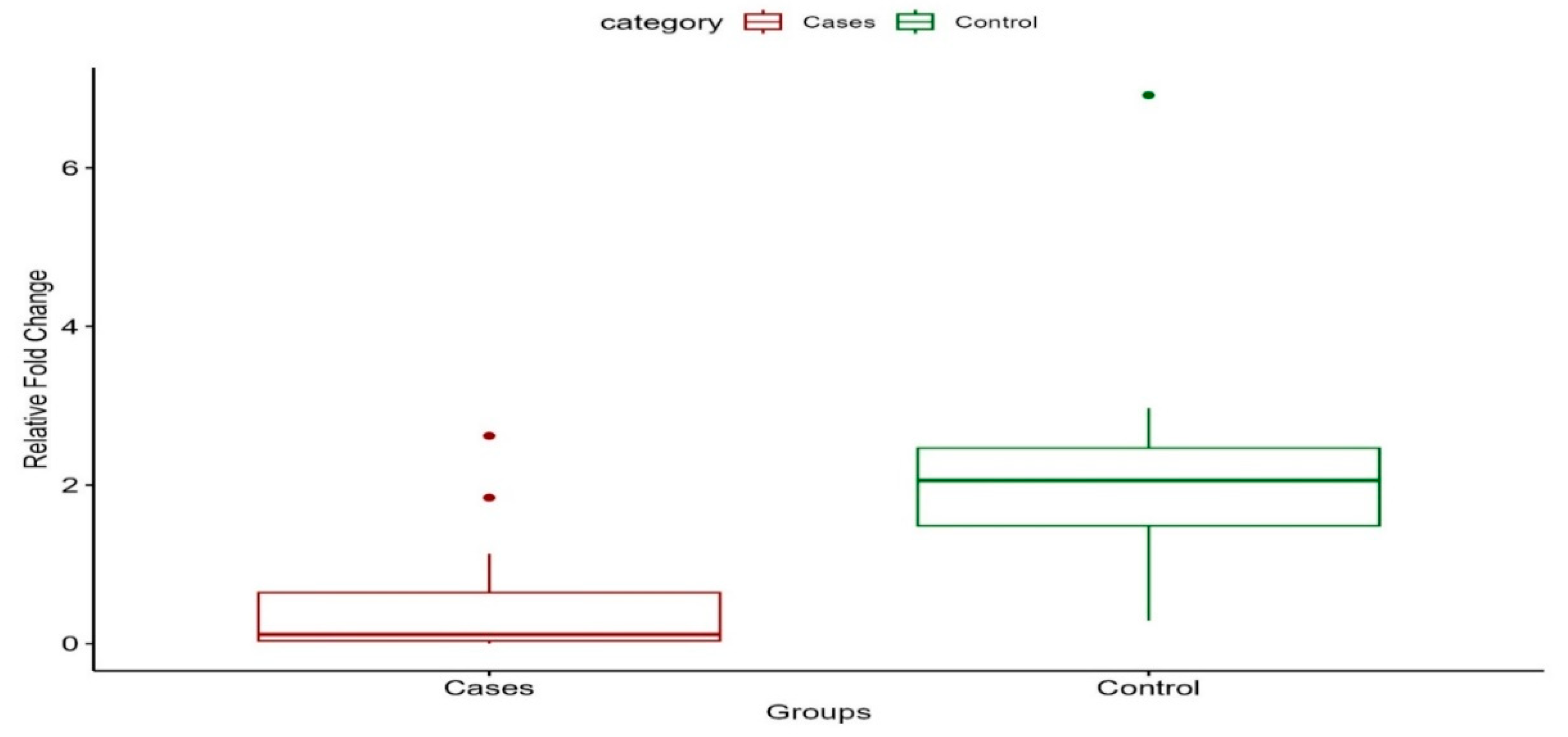
Figure 4.
Correlation between KCNH2 gene expression and serum triglyceride levels (r = –0.472, p = 0.003).
Figure 4.
Correlation between KCNH2 gene expression and serum triglyceride levels (r = –0.472, p = 0.003).
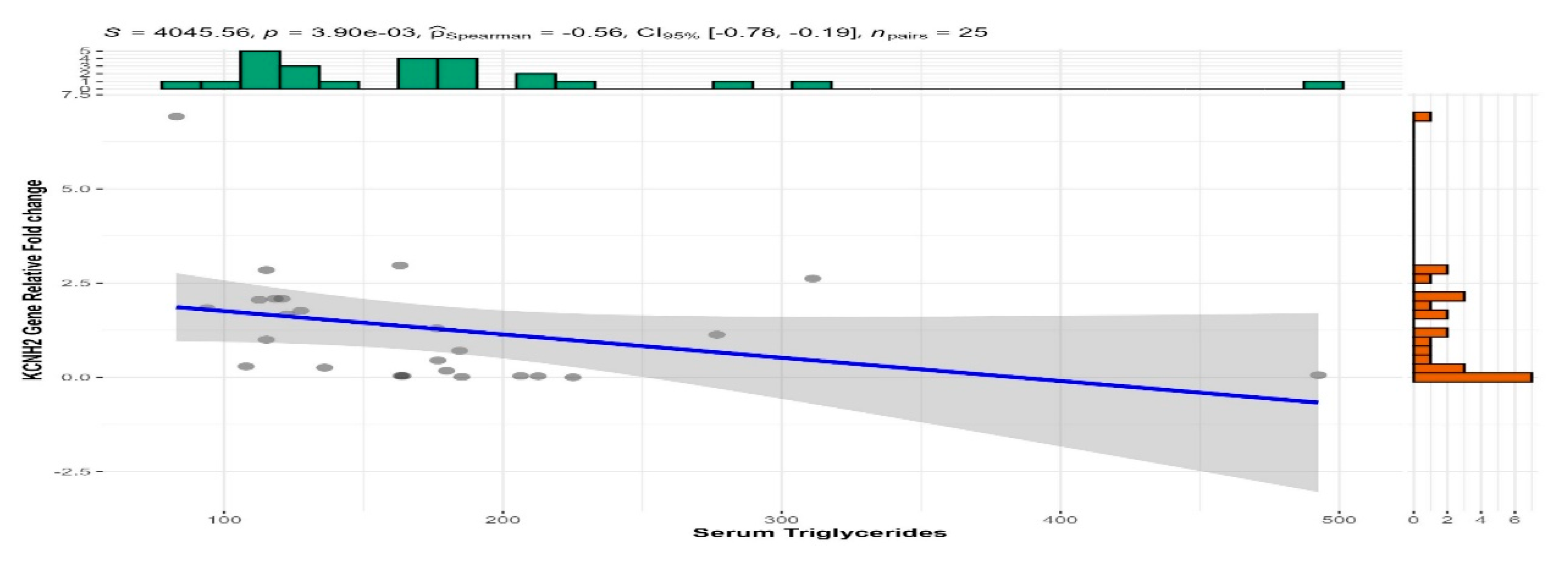
Table 1.
Socio-clinical characteristics of patients with atrial fibrillation and controls.
| Characteristics |
Cases (N = 14) |
Control (N = 11) |
p-value |
| Age, Mean (+SD) | 53.4 (+16.87) | 43.8 (+15.99) | 0.0821 |
| Sex, n (%) | >0.92 | ||
| Male | 8.0 (57.14%) | 6.0 (54.55%) | |
| Female | 6.0 (42.86%) | 5.0 (45.45%) | |
| Marital Status, n (%) | 0.0652 | ||
| Unmarried | 4.0(28.57%) | 3.0 (35.00%) | |
| Married | 10.0(71.43%) | 8.0 (65.00%) | |
| Class of Antiarrhythmic drugs, n (%) | |||
| Class 2 and 3 | 2.0 (28.57%) | 0.0 (0.0%) | |
| Class 2 and 3 + Digoxin | 1.0 (14.29%) | 0.0 (0.0%) | |
| Class 3 | 2.0 (28.57%) | 0.0 (0.0%) | |
| Class 3 + Digoxin | 1.0 (14.29%) | 0.0 (0.0%) | |
| Digoxin | 1.0 (14.29%) | 0.0 (0.0%) | |
| (Missing) | 7 | ||
| Family History of Atrial Fibrillation, n (%) | 0.0202 | ||
| No | 8.0 (57.14%) | 11.0 (100.00%) | |
| Yes | 6.0 (42.86%) | 0.0 (0.00%) | |
| Family History of Heart Failure, n (%) | 0.112 | ||
| No | 10.0 (71.43%) | 11.0 (100.00%) | |
| Yes | 4.0 (28.57%) | 0.0 (0.00%) | |
| Family History of Sudden Death, n (%) | >0.92 | ||
| No | 13.0 (92.86%) | 11.0 (100.00%) | |
| Yes | 1.0 (7.14%) | 0.0 (0.00%) | |
| 1T test; 2McNemar’s Exact Test | |||
Table 2.
Physical examination findings and lipid profile parameters among study participants.
| Characteristic |
Cases (N = 14) |
Control (N = 11) |
p-value |
| Pulse Rhythm, n (%) | <0.001 | ||
| Irregular | 14.00 (100.00%) | 0.00 (0.00%) | |
| Regular | 0.00 (0.00%) | 11.00 (100.00%) | |
| Total Cholesterol, Mean (±SD) | 207.48 (±59.00) | 153.73 (±34.58) | 0.0052 |
| Triglycerides, Median (Q1-Q3) | 184.88 (164.17-225.14) | 118.30 (112.57-127.50) | 0.0081 |
| HDL Cholesterol, Mean (±SD) | 56.20 (±13.48) | 51.50 (±9.07) | >0.92 |
| LDL Cholesterol, Mean (±SD) | 109.88 (±45.65) | 74.91 (±29.19) | 0.0292 |
| 1Wilcoxon signed rank test; 2T test; 3McNemar’s Exact Test | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



