Submitted:
03 November 2025
Posted:
04 November 2025
Read the latest preprint version here
Abstract
Background and Objectives: Periodontitis leads to progressive destruction of periodontal tissues and, despite advances in regenerative approaches, clinical outcomes remain inconsistent. Lasers have been proposed as adjuncts in regenerative periodontology for their antimicrobial, hemostatic, and photobiomodulatory properties, but the available evidence is heterogeneous. This scoping review aim to systematically map clinical and experimental evidence on the role of lasers in periodontal tissue regeneration. Materials and Methods: The review was conducted in accordance with the PRISMA-ScR guidelines. PubMed, Scopus, and Web of Science were searched up to September 2025 without time restrictions. Eligible studies included in vitro, ex vivo, in vivo and clinical research assessing the application of lasers for periodontal tissue regeneration. Reviews, conference abstracts and studies unrelated to regeneration were excluded. Results: The electronic search retrieved 314 records, of which 193 unique articles were screened after duplicates removal. Seventeen full texts were assessed and 15 studies fulfilled the eligibility criteria. Included studies comprised 5 in vitro investigations, 2 ex vivo studies, 1 in vivo animal study, and 7 clinical studies, published between 2015 and 2025. In vitro and ex vivo evidence demonstrated that laser irradiation enhanced cell proliferation, differentiation, growth factor release, and root surface conditioning. The in vivo study confirmed increased angiogenesis and bone formation after Er:YAG photobiomodulation. Clinical studies, including randomized controlled trials and case reports, reported improvements in probing depth reduction, clinical attachment gain, and radiographic bone fill, especially when lasers were used in combination with regenerative techniques or biomaterials. Conclusions: Available evidence suggests that lasers can positively modulate biological processes and enhance the outcomes of regenerative periodontal procedures. However, the limited number of high-quality clinical trials, variability in laser types and parameters, and heterogeneity in protocols limit the strength of current conclusions. Further standardized randomized controlled trials with long-term follow-up are needed to clarify the clinical relevance of lasers in periodontal tissue regeneration.
Keywords:
photobiomodulation
; laser surgery
; periodontal regeneration
; tissue regeneration
; periodontal ligament
; laser regeneration
; oral surgery
; oral pathology
1. Introduction
Periodontitis is one of the leading causes of tooth loss in adults and is characterized by chronic inflammatory processes that progressively destroy the supporting tissues of the teeth, including periodontal ligament, cementum, and alveolar bone [1].
In recent decades, several strategies have been proposed to promote periodontal tissue regeneration, including regenerative surgical approaches, biomaterials, and adjunctive therapies aimed at enhancing wound healing [2]. However, clinical outcomes remain heterogeneous and are influenced by multiple factors, highlighting the need for auxiliary methods that can improve regeneration [3].
Lasers have been introduced in periodontology as tools combining antimicrobial, hemostatic, and biostimulatory effects, with applications in both non-surgical and surgical periodontal therapy [4]. The photothermal and photobiomodulatory actions of lasers extend beyond root surface decontamination and are able to modulate cellular responses, promoting proliferation and differentiation of fibroblasts and periodontal stem cells and stimulating neoangiogenesis [5,6].
Several reviews have assessed the efficacy of different laser types. Erbium lasers (Er:YAG, Er,Cr:YSGG) have proven effective in removing granulation tissue and smear layer, showing promising outcomes in regenerative surgery [7,8]. Nd:YAG lasers demonstrated potential in reducing periodontal pathogens and favoring wound healing [9]. Diode lasers and low-level laser therapy (LLLT)/photobiomodulation (PBM) have been associated with improved cellular responses and enhanced recovery of clinical periodontal parameters [5,10].
Nevertheless, available scientific evidence is not always consistent. Some studies reported significant improvements in probing depth reduction and clinical attachment gain, while others found no relevant differences compared to conventional therapy [1,3]. These discrepancies are mainly attributed to heterogeneity in clinical protocols, irradiation parameters, experimental models, and laser types employed [11,12].
Alongside clinical investigations, basic research has provided insights into the biological mechanisms underlying laser applications in regenerative periodontology. Specific wavelengths have been shown to activate intracellular signaling pathways such as MAPK/ERK and stimulate the expression of osteogenic factors, thus favoring new periodontal tissue formation [5,6].
Despite the increasing interest, there is still a lack of comprehensive syntheses that systematically map the clinical, in vivo, and in vitro evidence on laser applications in periodontal tissue regeneration. Previous reviews have mainly focused on single laser types or specific therapeutic approaches [3,7,9], leaving a gap for an overarching evaluation of the available evidence.
Therefore, the aim of the present scoping review is to provide a comprehensive and up-to-date overview of clinical and experimental evidence on the use of lasers in periodontal tissue regeneration, identifying the laser types studied, irradiation parameters, experimental models, and the major gaps in the current literature.
2. Materials and Methods
2.1. Protocol
This scoping review adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) to comprehensively synthesize existing evidence and identify key concepts regarding the application of lasers in periodontal tissue regeneration (Table S1, Supplementary Materials) [13].
An adapted version of the PICO (Population, Intervention, Comparison, and Outcome) model was employed to formulate a focused question structured around a PEO (Population, Exposure, and Outcome) framework. This approach was utilized to evaluate the relationship between the exposure to laser therapy and the resulting biological and clinical outcomes in periodontal regeneration. It has previously been adopted in qualitative systematic reviews of healthcare interventions, including procedures in oral and periodontal surgery [14,15].
The main question of this scoping review was: “Does the use of laser therapy improve the potential for periodontal tissue regeneration in clinical and in experimental models?”
To address this question, studies reporting outcomes of periodontal regeneration following the application of lasers were analyzed in order to clarify the impact of different wavelengths and protocols on periodontal healing.
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
All sources of evidence had to satisfy specific inclusion criteria to be considered. These encompassed articles written exclusively in English, with no restrictions based on publication date. Eligible study designs included randomized controlled trials (RCTs), prospective and retrospective observational studies, case–control studies, and case reports. In addition, experimental studies conducted in vitro, ex vivo, or in vivo (animal models) were incorporated.
The primary focus of the investigation in these studies had to be the evaluation of periodontal tissue regeneration promoted by laser therapy, with particular emphasis on both clinical and experimental research.
2.2.2. Exclusion Criteria
Any studies that did not meet the specified inclusion criteria were excluded from the review. This included articles written in languages other than English, literature reviews (narrative, systematic, or scoping), conference abstracts, and studies that primarily focused on non-regenerative applications of lasers (such as peri-implantitis management, endodontic procedures, tooth whitening, or soft tissue aesthetics).
2.2.3. Search Strategies and Information Source
To perform this review, the PEO model (Population, Exposure, and Outcome) was adopted for structuring the search strategy across multiple electronic databases, including PubMed, Scopus, and Web of Science.
The PEO model [15] was based on the elements of: Population (no restriction was applied to a specific population, as both human and experimental studies were considered), Exposure (evidence from clinical, in vivo, ex vivo, and in vitro studies related to the use of laser therapy), Outcome (periodontal tissue regeneration).
Specific Medical Subject Headings (MeSH) were employed for PubMed, while free-text keywords were adapted for Scopus and Web of Science, to ensure broad retrieval of pertinent studies in alignment with the PEO framework. Articles were selected based on specific terms including “laser”, “periodontal disease”, and “regeneration”.
2.2.4. Selection of Sources of Evidence
Two independent reviewers (MB and U.R.) carried out the initial screening of titles and abstracts for all retrieved articles. Any duplicate entries across the databases were identified and eliminated using the EndNote Web reference manager software (version 20), by Clarivate Analytics, based in Philadelphia, PA, USA. Full-text articles were then individually assessed for eligibility, and studies that fulfilled the predefined inclusion criteria were selected.
The two reviewers compared their selections, and in the case of discrepancies, these were discussed and resolved by consensus or with the intervention of additional reviewers (A.D.V. and A.B.G.)
2.2.5. Methodological and Reporting Quality Assessment
Since this scoping review aims to map the scientific literature on the role of lasers in periodontal tissue regeneration by synthesizing all available studies to date, including clinical, in vivo, ex vivo, and in vitro research, in accordance with the PRISMA-ScR guidelines, a formal quality assessment of the included studies was not performed.
2.2.6. Analysis of Included Studies
Following the review of the publications, a spreadsheet was generated and sequentially updated during the data extraction process. Separate tables were created for in vitro, ex vivo, in vivo, and clinical studies.
For the in vitro studies, the collected data were organized into tables to provide a structured presentation of information, including: the name of the first author and year of publication, the type of cells investigated (e.g., PDLSCs, gingival fibroblasts), the type of laser and irradiation parameters, the experimental groups investigated, the assays performed (e.g., proliferation, differentiation, migration), and the main results.
For the ex vivo studies, the data were organized into tables including: the first author and year, the type of biological sample (e.g., platelet concentrates, root surfaces), the type of laser and irradiation parameters, the experimental and control groups, the type of analyses performed (e.g., growth factor release, smear layer removal, fibrin adhesion), and the main findings.
For the in vivo study, the extracted information included: the first author and year, the animal model used, the type of study, the type of laser and irradiation parameters, the experimental groups, the follow-up period, histological and molecular analyses (e.g., angiogenesis, VEGF expression, new bone formation), and the outcomes.
For the clinical studies, the data were structured into tables reporting: the first author and year, the study design, the patient/sample size, the type of laser and irradiation parameters, the adjunctive biomaterials or techniques employed, the comparator groups, the follow-up period, the outcomes assessed (e.g., probing depth, clinical attachment level, radiographic bone fill, molecular biomarkers), and the key findings. (Table 1, Table 2, Table 3 and Table 4)
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn. The electronic search retrieved a total of 314 records: 122 from Scopus, 65 from PubMed, and 127 from Web of Science. After removing duplicates, 193 unique articles were screened by title and abstract. Of these, 17 full-texts were evaluated for eligibility. Finally, 15 studies were included in the scoping review, while 2 were excluded on the reason that they addressed esthetic papilla management without evaluating periodontal tissue regeneration [16,17].
A total of 15 studies were included in this scoping review, comprising 5 in vitro investigations [6,18,19,20,21], 2 ex-vivo studies [22,23] 1 in vivo animal study [24], and 7 clinical studies [25,26,27,28,29,30,31]. The publication period ranged from 2015 to 2025.
The search strategy and study selection process are summarized in Figure 1 (PRISMA-ScR flowchart).
Results of Individual Sources of Evidence
The studies included in this scoping review investigated the role of different types of laser devices in periodontal tissue regeneration, using in vitro, ex vivo, in vivo, and clinical designs.
In vitro studies mainly explored the effects of photobiomodulation and laser irradiation on periodontal ligament stem cells, gingival fibroblasts, and osteogenic pathways, consistently demonstrating enhanced cell proliferation, migration, differentiation, and mineralization following irradiation with diode, Nd:YAG, Er:YAG, Er,Cr:YSGG, or LED devices [6,18,19,20,21].
Ex vivo investigations assessed the impact of laser irradiation on platelet concentrates and root surfaces. These studies reported increased release of platelet-derived growth factors from irradiated PRF and A-PRF, and effective removal of smear layer with improved fibrin adhesion on diseased root surfaces, suggesting that lasers may enhance the biological potential of adjunctive regenerative materials [22,23].
The only in vivo study was conducted in a rat model of periodontal defects, confirming that low-level Er:YAG laser irradiation significantly promoted angiogenesis, upregulated VEGF expression, and supported new bone formation, thereby strengthening the translational link between preclinical and clinical applications [24].
Clinical evidence comprised randomized controlled trials and case reports evaluating the adjunctive use of lasers in regenerative periodontal procedures. Most clinical investigations reported improvements in probing depth reduction, clinical attachment gain, and radiographic bone fill, particularly when lasers were applied in combination with regenerative approaches such as guided tissue regeneration, platelet concentrates, or papilla preservation techniques [25,26,27,28,29,30,31]. The detailed characteristics and main findings of the included studies are summarized in Table 1, Table 2, Table 3 and Table 4, which present, respectively, the in vitro investigations, the ex vivo studies, the in vivo animal experiment, and the clinical evidence on the use of lasers in periodontal tissue regeneration.
4. Discussion
This scoping review mapped the available evidence regarding the use of lasers in periodontal tissue regeneration across in vitro, ex vivo, in vivo, and clinical settings. Overall, the findings indicate that laser therapy can exert beneficial biological and clinical effects, although heterogeneity in study designs, laser types, and parameters limits the comparability of results.
In vitro studies consistently demonstrated that laser irradiation promotes key biological processes relevant to periodontal regeneration. Diode lasers at 970 and 980 nm enhanced proliferation and osteogenic differentiation of periodontal ligament stem cells (PDLSCs) and potentiated the effects of stem cell–derived factors [18,19]. Nd:YAG irradiation facilitated PDLSC proliferation and migration via the SDF-1/CXCR4 pathway, supporting the hypothesis that this laser may stimulate endogenous stem cell homing [20]. Red LED light induced ERK1/2 activation, osteogenic marker expression, and mineral deposition [6]. Er:YAG and Er,Cr:YSGG lasers also improved gingival fibroblast proliferation [21]. Collectively, these studies indicate that different wavelengths can modulate cell proliferation, migration, and differentiation, which are essential events for periodontal regeneration.
Ex vivo studies added evidence on the interaction between lasers and biological substrates relevant to regenerative therapy. Diode irradiation increased the release of PDGF-BB from platelet concentrates (PRF and A-PRF), enhancing their growth factor content and regenerative potential [22]. Similarly, Er,Cr:YSGG irradiation effectively removed smear layer and improved fibrin adhesion on periodontally compromised root surfaces, creating more favorable conditions for periodontal attachment and regeneration [23]. These findings suggest that lasers can potentiate the efficacy of adjunctive regenerative materials used in clinical protocols.
The only in vivo study confirmed the translational relevance of these in vitro and ex vivo results. Er:YAG laser irradiation in a rat model of periodontal defects enhanced angiogenesis, increased VEGF expression, and promoted new bone formation compared with sham-irradiated controls [24]. These results support the role of Er:YAG photobiomodulation in accelerating tissue healing and regeneration in vivo.
Clinical evidence, although limited in number and often based on case reports, supports the adjunctive role of lasers in regenerative periodontal surgery. Case reports demonstrated that diode lasers used in combination with bone grafts [25], platelet concentrates [28], or advanced platelet-rich fibrin [31] promoted significant clinical improvements and radiographic bone fill. Laser-assisted curettage using diode devices yielded radiographic regeneration in advanced periodontitis [30]. Randomized controlled trials provided stronger evidence: adjunctive diode irradiation during guided tissue regeneration improved clinical and biochemical outcomes [26]; Nd:YAG-based LANAP combined with LLLT enhanced CAL gain and bone regeneration compared to SRP alone [27]; and LLLT used during papilla preservation flap surgery improved clinical outcomes and upregulated osteogenic markers [29]. Together, these studies suggest that lasers may enhance the effectiveness of regenerative periodontal procedures.
Despite encouraging results, several limitations need to be acknowledged. First, the number of available clinical trials remains small, with most clinical evidence relying on case reports or small-scale studies, limiting the generalizability of findings. Second, significant heterogeneity exists in terms of laser types, irradiation parameters, adjunctive biomaterials, and outcome measures, which prevents direct comparison across studies. Moreover, follow-up periods varied widely, with only a few studies assessing long-term outcomes.
Future research should focus on well-designed randomized controlled trials with standardized protocols, larger sample sizes, and long-term follow-up to determine the clinical relevance of lasers in regenerative periodontal therapy. Moreover, mechanistic studies are needed to better elucidate how specific wavelengths and dosimetry influence cellular pathways, angiogenesis, and tissue remodeling. Finally, integration of laser therapy with advanced biomaterials and biologics represents a promising avenue for optimizing regenerative strategies.
5. Conclusions
This scoping review identified and synthesized evidence from in vitro, ex vivo, in vivo, and clinical studies on the use of lasers for periodontal tissue regeneration. The findings indicate that laser irradiation can positively influence key biological processes, such as cell proliferation, differentiation, angiogenesis, and growth factor release, while clinical studies suggest improved outcomes in probing depth reduction, clinical attachment gain, and radiographic bone fill when lasers are applied as adjuncts to regenerative procedures.
Nevertheless, the current body of evidence is limited by the small number of high-quality clinical trials, heterogeneity in study protocols, and variability in laser parameters and adjunctive therapies. Further well-designed randomized controlled trials with standardized methodologies and long-term follow-up are needed to confirm the clinical relevance of lasers in regenerative periodontal therapy.
Overall, the available evidence supports the potential role of lasers as valuable adjuncts in periodontal regenerative strategies, though stronger clinical validation is required before their widespread adoption in routine practice.
6. Patents
This section is not mandatory but may be added if there are patents resulting from the work reported in this manuscript.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, M.B; methodology, M.B; software, M.B.; validation, U.R. and A.D.V.; formal analysis, M.B.; investigation, M.B.; resources, M.B.; data curation, M.B.; writing—original draft preparation, M.B.; writing—review and editing, M.B., U.B. and A.D.V.; visualization, U.R., A.D.V.; supervision, A.B.G., U.R, A.D.V.; project administration, A.B.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Upon request to the corresponding author, the data are available for use.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| A-PRF | Advanced Platelet-Rich Fibrin |
| A-PRF+ | Advanced Platelet-Rich Fibrin Plus |
| ALP | Alkaline Phosphatase |
| aPDT | Antimicrobial Photodynamic Therapy |
| BMP-2 | Bone Morphogenetic Protein-2 |
| CAL | Clinical Attachment Level |
| CCK-8 | Cell Counting Kit-8 |
| DBM | Demineralized Bone Matrix |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| ERK | Extracellular Signal-Regulated Kinase |
| GMSCs | Gingival Mesenchymal Stem Cells |
| GTR | Guided Tissue Regeneration |
| HLLT | High-Level Laser Therapy |
| LANAP | Laser-Assisted New Attachment Procedure |
| LED | Light-Emitting Diode |
| LLLT | Low-Level Laser Therapy |
| MAPK | Mitogen-Activated Protein Kinase |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5 diphenyltetrazolium bromide assay |
| OCN | Osteocalcin |
| OPN | Osteopontin |
| PBM | Photobiomodulation |
| PD | Probing Depth |
| PDGF-BB | Platelet-Derived Growth Factor-BB |
| PDLSCs | Periodontal Ligament Stem Cells |
| PRF | Platelet-Rich Fibrin |
| RCT | Randomized Controlled Trial |
| RT-PCR | Reverse Transcription Polymerase Chain Reaction |
| RUNX2 | Runt-Related Transcription Factor 2 |
| SEM | Scanning Electron Microscopy |
| SDF-1 | Stromal Cell-Derived Factor-1 |
| SRP | Scaling and Root Planing |
| TGF-β | Transforming Growth Factor-Beta |
| VEGF | Vascular Endothelial Growth Factor |
| Wnt | Wingless/Integrated signaling pathway |
References
- Santonocito S, Polizzi A, Cavalcanti R, Lo Giudice A, Indelicato F, Isola G. Impact of laser therapy on periodontal and peri-implant diseases: A review. Photobiomodul Photomed Laser Surg. 2022;40(7):454-462. [CrossRef]
- Sanz M, Teughels W; Group A of the F. European Workshop on Periodontology. Innovations in non-surgical periodontal therapy: Consensus report of Group A. J Clin Periodontol. 2012;39 Suppl 12:133-138. [CrossRef]
- Behdin S, Monje A, Lin GH, Edwards B, Othman A, Romanos GE. Effectiveness of laser application for periodontal surgical therapy: Systematic review and meta-analysis. J Periodontol. 2015;86(12):1352-1363. [CrossRef]
- Aoki A, Mizutani K, Schwarz F, Sculean A, Yukna RA, Takasaki AA, Romanos GE, Taniguchi Y, Sasaki KM, Zeredo JL, et al. Periodontal and peri-implant wound healing following laser therapy. Periodontol 2000. 2015;68(1):217-269. [CrossRef]
- Dukić W, Bago I. The use of low-level laser therapy in regenerative periodontology. Photomed Laser Surg. 2013;31(2):53-57. [CrossRef]
- Yamauchi T, Yoshida T, Horii K, Yoshino T, Matsuzaka K, Inoue T. The impact of red light-emitting diode irradiation on proliferation and osteogenic differentiation of human periodontal ligament stem cells. J Periodontol. 2017;88(11):1187-1195. [CrossRef]
- Slot DE, Kranendonk AA, Paraskevas S, Van der Weijden GA. The effect of an Er:YAG laser in non-surgical periodontal therapy: A systematic review. J Clin Periodontol. 2011;38(9):736-742. [CrossRef]
- Aoki A, Mizutani K, Takasaki AA, Schwarz F, Sculean A. Current status of Er:YAG laser in periodontal therapy. Jpn Dent Sci Rev. 2024;60:1-14. [CrossRef]
- Slot DE, Kranendonk AA, Bakker EW, Van der Weijden GA. The effect of a pulsed Nd:YAG laser in non-surgical periodontal therapy: A systematic review. J Periodontol. 2014;85(9):1207-1216. [CrossRef]
- Dannan A. The potential applications of laser therapy in periodontics: A review. Dent Res J (Isfahan). 2009;6(3):147-154. PMID: 20379354.
- Sanz-Moliner JD, Arnabat-Dominguez J, Berini-Aytés L, Gay-Escoda C. Lasers in periodontics: A review. Med Oral Patol Oral Cir Bucal. 2009;14(9):E425-E428. PMID: 19680299.
- Sanz-Moliner JD, et al. Lasers in periodontal regeneration: A review. Clin Adv Periodontics. 2012;2(2):96-104. [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [CrossRef]
- Bateson, M. Systematic Reviews to Support Evidence-Based Medicine: How to Review and Apply Findings of Healthcare Research. Postgrad. Med. J. 2004, 80, 123.
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [CrossRef]
- Zanin F, et al. Hemolasertherapy for papilla regeneration: Case report. Photomed Laser Surg. 2018;36(10):541-545. [CrossRef]
- El Mobadder M, et al. Photobiomodulation in esthetic management of black triangles: Case series. Cureus. 2024;16(2):e56789. [CrossRef]
- El-Dahab D, et al. Photobiomodulation with diode laser promotes proliferation and osteogenic differentiation of PDLSCs: An in vitro study. BMC Oral Health. 2024;24:567. [CrossRef]
- Aljabri M, et al. Synergistic effects of LLLT and gingival stem cell conditioned medium on periodontal ligament stem cells. Clin Exp Dent Res. 2025;11:345-356. [CrossRef]
- Wu Y, et al. Nd:YAG low-level laser promotes migration and proliferation of PDLSCs through SDF-1/CXCR4 pathway. BMC Oral Health. 2023;23:987. [CrossRef]
- Talebi-Ardakani MR, et al. Effects of Er:YAG and Er,Cr:YSGG lasers on proliferation of human gingival fibroblasts: An in vitro study. Acta Med Iran. 2015;53(5):310-315. PMID: 26060769.
- Kalaivani K, et al. Effect of diode laser irradiation on growth factor release from PRF and A-PRF+. J Indian Acad Oral Med Radiol. 2025;37(2):123-130. [CrossRef]
- Satish R, et al. Er,Cr:YSGG laser root conditioning enhances fibrin adhesion: An ex vivo study. Contemp Clin Dent. 2023;14(4):211-218. [CrossRef]
- Takemura Y, et al. Er:YAG low-level laser irradiation promotes angiogenesis and bone formation in rat periodontal defects. J Periodontol. 2023;94(8):1021-1032. [CrossRef]
- Bhardwaj A, et al. Low-level laser therapy as adjunct to demineralized bone matrix in treatment of intrabony defect: Case report. J Clin Diagn Res. 2016;10(7):ZD01-ZD03. [CrossRef]
- Cetiner D, et al. Adjunctive aPDT and PBM in regenerative periodontal surgery: RCT. Clin Oral Investig. 2024;28:4567-4578. [CrossRef]
- Dadas M, et al. LANAP and LLLT as adjuncts to SRP in chronic periodontitis: RCT. Lasers Med Sci. 2025;40:1123-1134. [CrossRef]
- Deepthi S, et al. Combined use of diode laser and PRF in molar preservation: Case report. J Indian Soc Periodontol. 2024;28(3):276-280. [CrossRef]
- Prakash PSG, et al. Effect of adjunctive LLLT on outcomes of papilla preservation flap surgery: RCT. Clin Oral Investig. 2025;29:456-467. [CrossRef]
- Puthalath A, et al. Diode laser-assisted curettage in stage IV periodontitis: Case report. Contemp Clin Dent. 2023;14(2):134-138. [CrossRef]
- Tan J, et al. Er:YAG laser combined with A-PRF+ in periodontal bone defects: Case reports with 3-year follow-up. World J Clin Cases. 2022;10(24):8614-8623. [CrossRef]
Figure 1.
Flowchart of the review process.
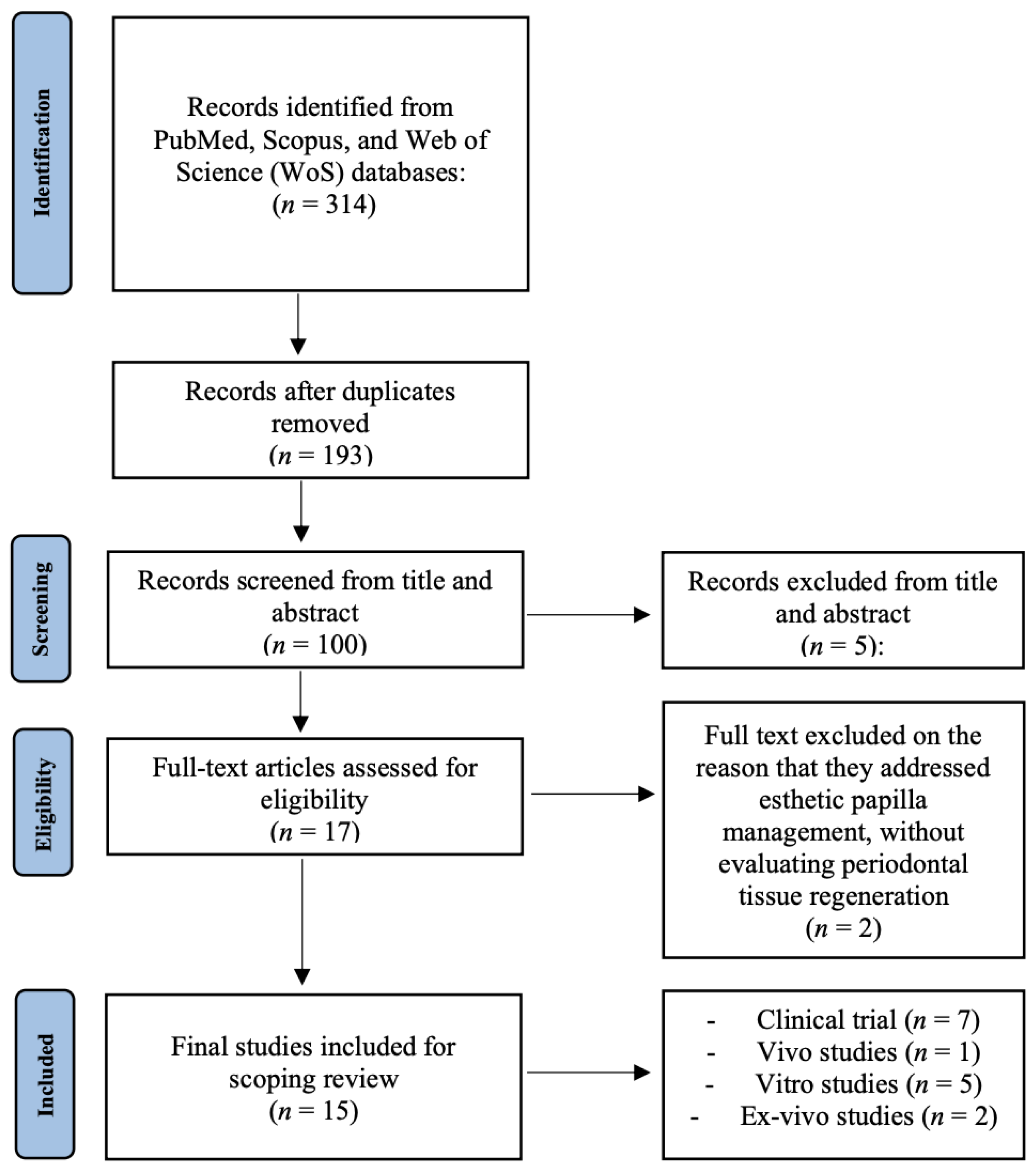

Table 1.
In vitro studies on laser applications for periodontal regeneration.
| Author, Year | Study design & Sample | Intervention | Comparator | Outcomes | Key findings |
| Yamauchi, 2017 Japan [6] |
In vitro study on PDLSCs obtained from human third molars, cultured under osteogenic conditions. | Cells irradiated with a high-power red LED at 650 nm, energy density of 8 J/cm², applied in multiple sessions to simulate photobiomodulation therapy. | Non-irradiated PDLSCs cultured under the same conditions served as controls. | Assessed proliferation rate, ALP activity, calcium deposition, and ERK1/2 signaling pathway activation. | LED irradiation promoted PDLSC proliferation, significantly increased ALP activity and calcium deposition, and upregulated osteogenic marker expression. Activation of ERK1/2 confirmed a molecular mechanism underlying the observed effects. |
| El-Dahab, 2024 Egypt [18] |
In vitro study on human periodontal ligament stem cells (PDLSCs) isolated from extracted teeth and cultured under standard conditions. | Cells were irradiated with a diode laser at 970 nm using parameters consistent with photobiomodulation protocols. Irradiation was performed at multiple time points to assess cumulative effects on proliferation and differentiation. | Non-irradiated PDLSCs cultured in parallel were used as controls. | Cell proliferation assessed by CCK-8 assay; osteogenic differentiation evaluated via ALP activity, mineralized nodule formation, and gene expression of osteogenic markers. | Laser irradiation significantly enhanced PDLSC proliferation and osteogenic differentiation compared with controls, with greater mineralized nodule deposition, supporting the role of diode lasers in periodontal regeneration. |
| Aljabri, 2025 Saudi Arabia [19] |
In vitro study using PDLSCs exposed to gingival mesenchymal stem cell (GMSC)-conditioned medium, designed to mimic paracrine signaling in regeneration. | Diode laser at 980 nm applied under low-level laser therapy (LLLT) parameters. Irradiation was performed in conjunction with GMSC-conditioned medium to test synergistic effects. | PDLSCs without laser and without conditioned medium were used as baseline controls. | Cell viability, osteogenic differentiation markers (RUNX2, OCN, BMP-2), and activation of Wnt/TGF-β signaling were assessed. | The combination of GMSC-conditioned medium and laser irradiation significantly enhanced osteogenesis compared with controls. Upregulation of osteogenic markers and activation of Wnt/TGF-β pathway confirmed synergistic effects. |
| Wu, 2023 China [20] |
In vitro study on PDLSCs derived from extracted human teeth. | Cells irradiated with a Nd:YAG laser at sub-ablative low-energy settings (0.25–1.5 W, 30 s, MSP mode). Different power levels were tested to identify the optimal range for cell stimulation. | Non-irradiated PDLSCs served as controls. | Cell proliferation evaluated by CCK-8 assay, migration tested by Transwell assays, and gene/protein expression of SDF-1/CXCR4 signaling assessed by RT-PCR and Western blot. | Nd:YAG laser irradiation at 1 W significantly enhanced PDLSC proliferation and migration compared to controls. These effects were mediated through SDF-1/CXCR4 signaling, indicating potential for improved stem cell homing in regenerative therapy. |
| Talebi-Ardakani, 2015 Iran [21] |
In vitro study on primary human gingival fibroblasts cultured under standard laboratory conditions. | Fibroblasts were exposed to Er:YAG and Er,Cr:YSGG lasers at sub-ablative energy settings, applied in a controlled in vitro environment. | Non-irradiated fibroblasts were used as controls. | Cell proliferation and viability were assessed by MTT assays. | Both Er:YAG and Er,Cr:YSGG lasers increased fibroblast proliferation compared to controls, suggesting potential for enhanced soft tissue healing in periodontal therapy. |
Abbreviations: ALP (Alkaline Phosphatase), BMP-2 (Bone Morphogenetic Protein-2), CCK-8 (Cell Counting Kit-8), ERK (Extracellular Signal-Regulated Kinase), GMSCs (Gingival Mesenchymal Stem Cells), LLLT (Low-Level Laser Therapy), MTT (3-(4,5-dimethylthiazol-2-yl)-2,5 diphenyltetrazolium bromide assay), OCN (Osteocalcin), PBM (Photobiomodulation), PDLSCs (Periodontal Ligament Stem Cells), RUNX2 (Runt-Related Transcription Factor 2), RT-PCR (Reverse Transcription Polymerase Chain Reaction), SDF-1 (Stromal Cell-Derived Factor-1), Wnt (Wingless/Integrated Signaling Pathway).
Table 2.
Ex vivo studies on laser applications for periodontal regeneration.
| Author, Year | Study design & Sample | Intervention | Comparator | Outcomes | Key findings |
| Kalaivani, 2025 India [22] |
Ex vivo study on platelet concentrates (A-PRF and A-PRF+) prepared from human venous blood samples. | Diode laser irradiation at 630 nm applied in a non-contact mode for 15–20 seconds to stimulate growth factor release. | PRF and A-PRF samples not exposed to laser irradiation served as controls. | Quantification of PDGF-BB release using ELISA assays. | Laser irradiation significantly increased PDGF-BB release compared with non-irradiated controls, indicating that photobiomodulation enhances the regenerative potential of platelet concentrates. |
| Satish, 2023 India [23] |
Ex vivo study on periodontally compromised root surfaces collected from extracted human teeth. | Er,Cr:YSGG laser irradiation applied to root surfaces for smear layer removal and surface conditioning. | Root surfaces treated with EDTA or tetracycline, as well as untreated roots, were used as comparators. | Evaluation of smear layer removal and fibrin adhesion by SEM and histological analysis. | Laser irradiation effectively removed the smear layer and promoted fibrin adhesion, producing root surfaces more favorable for periodontal regeneration compared to conventional chemical conditioning methods. |
Abbreviations: A-PRF (Advanced Platelet-Rich Fibrin), A-PRF+ (Advanced Platelet-Rich Fibrin Plus), ELISA (Enzyme-Linked Immunosorbent Assay), PDGF-BB (Platelet-Derived Growth Factor-BB), PRF (Platelet-Rich Fibrin), SEM (Scanning Electron Microscopy).
Table 3.
In vivo study on laser applications for periodontal regeneration.
| Author, Year | Study design & Model | Intervention | Comparator | Outcomes | Key findings |
| Takemura, 2023 Japan [24] |
Animal study conducted on a rat model with surgically created periodontal defects. | Periodontal defects irradiated with Er:YAG laser in low-level laser therapy (LLLT) mode at sub-ablative parameters, repeated over the healing period. | Sham-irradiated defects served as controls. | Histological assessment of tissue repair, VEGF expression, angiogenesis, and new bone formation. | Er:YAG laser irradiation promoted angiogenesis and VEGF expression, leading to significantly greater new bone formation compared with controls, confirming its regenerative potential in vivo. |
Abbreviations: Er:YAG (Erbium-doped Yttrium Aluminum Garnet), LLLT (Low-Level Laser Therapy), VEGF (Vascular Endothelial Growth Factor).
Table 4.
Clinical studies on laser applications for periodontal regeneration.
| Author, Year | Study design & Sample | Intervention | Comparator | Follow-up | Outcomes | Key findings |
| Bhardwaj, 2016 India [25] |
Case report on a single patient presenting with an intraosseous periodontal defect managed with regenerative surgery. | Treatment consisted of demineralized bone matrix graft combined with adjunctive low-level laser therapy using an 810 nm diode laser in PBM mode, applied post-surgically to stimulate healing. | No direct comparator; results were evaluated against conventional outcomes reported in literature. | 12 months. | Clinical parameters (PD reduction, CAL gain) and radiographic bone fill. | The case showed a marked reduction in PD, significant CAL gain, and radiographic evidence of bone regeneration, supporting LLLT as an adjunct to grafting. |
| Cetiner, 2024 Turkey [26] |
Randomized controlled trial including 40 intrabony defect sites in patients with chronic periodontitis. | Adjunctive diode laser at 970 nm for antimicrobial photodynamic therapy (aPDT) combined with LED photobiomodulation, applied alongside GTR with biomaterials. | Control group received GTR with biomaterials but no laser therapy. | 12 months. | PD, CAL, biochemical markers of bone metabolism. | Adjunctive laser therapy resulted in greater PD and CAL improvements and increased bone marker levels compared with the control group. |
| Dadas, 2025 Turkey [27] |
Randomized controlled trial involving 45 patients with periodontitis undergoing SRP. | LANAP protocol with Nd:YAG laser combined with adjunctive LLLT applied after SRP. | SRP alone served as control. | 12 months. | PD, CAL, radiographic bone regeneration. | LANAP + LLLT produced superior clinical and radiographic outcomes compared with SRP alone, confirming enhanced regenerative effects. |
| Deepthi, 2024 India [28] |
Case report of one patient requiring preservation of a second molar affected by periodontitis. | Combined use of diode laser at 970 nm (HLLT) and PBM with adjunctive platelet-rich fibrin (PRF). | Standard care approaches reported in the literature served as comparison. | 6 months. | PD, CAL, radiographic bone fill. | Laser combined with PRF reduced PD, improved CAL, and demonstrated radiographic regeneration, supporting tooth preservation. |
| Prakash PSG, 2025 India [29] |
Randomized controlled trial including 32 patients with intrabony periodontal defects. | Adjunctive LLLT using a diode laser during simplified papilla preservation flap surgery. | Control group underwent papilla preservation flap surgery without LLLT. | 6 months. | PD, CAL, molecular markers (RUNX2, BMP-2, COL1, OPN). | LLLT enhanced clinical improvements and upregulated osteogenic biomarkers, confirming both clinical and molecular regenerative benefits. |
| Puthalath, 2023 India [30] |
Case report of a patient with stage IV periodontitis requiring regenerative treatment. | Diode 940 nm laser-assisted curettage (LANAP-like protocol). | Conventional curettage outcomes described in literature served as comparator. | 6 months. | PD, CAL, radiographic bone regeneration. | Laser-assisted curettage promoted periodontal healing and radiographic bone regeneration in advanced periodontitis. |
| Tan, 2022 China [31] |
Case report of two patients with periodontal bone defects treated with regenerative surgery. | Er:YAG laser applied in combination with advanced platelet-rich fibrin plus (A-PRF+). | Conventional regenerative approaches in the literature were used as comparators. | 36 months. | PD, CAL, radiographic bone stability. | Laser combined with A-PRF+ provided stable long-term PD reduction, CAL gain, and radiographic bone regeneration over three years. |
Abbreviations: aPDT (Antimicrobial Photodynamic Therapy), A-PRF+ (Advanced Platelet-Rich Fibrin Plus), CAL (Clinical Attachment Level), COL1 (Collagen Type I), DBM (Demineralized Bone Matrix), LANAP (Laser-Assisted New Attachment Procedure), LED (Light-Emitting Diode), LLLT (Low-Level Laser Therapy), OPN (Osteopontin), PBM (Photobiomodulation), PD (Probing Depth), PRF (Platelet-Rich Fibrin), RCT (Randomized Controlled Trial), RUNX2 (Runt-Related Transcription Factor 2), SRP (Scaling and Root Planing).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



