
Submitted:
06 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
Background/Objectives: The standard and effective therapy for treating periodontal disease is scaling and root planing (SRP). However, the adjunctive use of antimicrobial photodynamic therapy (aPDT) has been investigated as a promising approach to enhance periodontal health. This therapy involves the activation of a photosensitizer (PS) through laser, leading to the transfer of energy or electrons to the surrounding environment, ultimately generating reactive oxygen species (ROS). These ROS interact with various intracellular targets, exerting antimicrobial effects. Methylene blue is the most commonly used PS due to its favorable characteristics, including a neutral pH and an absorption peak at 660 nm. The objective of this study was to conduct a literature review to highlight the benefits of methylene blue-mediated aPDT as an adjunct to periodontal treatment. The inclusion criteria were randomized clinical trials that used methylene blue as the PS, published between 2009 and 2024, with a minimum follow-up of three months. Studies included patients with periodontitis treated with SRP alone or in combination with aPDT. Out of 237 initially identified studies with potential for inclusion, 23 met the eligibility criteria and were included in this review. The selected studies were assessed for risk of bias using the Cochrane criteria for randomized trials, in addition to data tabulation and detailed analysis. Although the included studies presented heterogeneous clinical outcomes, an overall improvement in periodontal clinical parameters was observed. The variability in clinical protocols among the studies limited the ability to perform a more homogeneous analysis. Despite these findings supporting the potential role of aPDT as an adjunctive therapy in periodontal treatment, further long-term randomized clinical trials are needed, especially to evaluate its effects across different patient profiles.
Keywords:
Periodontal Disease
; Photodynamic Therapy
; Periodontitis
; Methylene Blue
1. Introduction
The use of light-based therapies in periodontics has gained prominence as a favorable therapeutic approach, particularly through the application of low-level laser therapies [1]. The treatment of choice for periodontal disease (PD) remains oral hygiene instruction combined with scaling and root planing (SRP), aimed at the removal of biofilm, calculus, and contaminated cementum. The primary clinical goal is to achieve a probing depth (PD) of ≤4 mm without bleeding on probing (BOP) [2]. To enhance the clinical outcomes of SRP, various adjunctive therapies have been proposed [3]. In this context, aPDT may also be employed as an adjunct to SRP, contributing to the reduction of bacterial load and inflammation in periodontal tissues, while additionally promoting biostimulatory effects [4].
Currently, the scientific literature has increasingly highlighted the benefits of aPDT in both Periodontics and Implantology [1], demonstrating that this approach is effective and safe for a variety of clinical conditions. aPDT acts on multidrug-resistant microorganisms and, apparently, does not induce bacterial resistance [5].
In aPDT, the type of photosensitizer (PS) can significantly influence therapeutic outcomes. Among the available PSs, synthetic dyes such as methylene blue and toluidine blue are among the most used in clinical protocols [6]. Methylene blue is particularly prominent due to several advantageous characteristics, including its low cost, market availability, and favorable clinical performance [7]. Furthermore, methylene blue possesses a neutral pH, a peak absorption at 660 nm, and is hydrophilic in nature [8].
Despite promising results, the literature still presents conflicting findings regarding the efficacy of aPDT as an adjunct to conventional periodontal therapy. Considering that methylene blue is the most widely used PS and that its absorption peak (660 nm) corresponds to the emission wavelength of many commercially available lasers, the objective of this literature review is to investigate current evidence related to this therapy and to clarify the controversial results reported in the literature.
2. Materials and Methods
The present literature review was structured to answer the following question: “Does adjuvant antimicrobial photodynamic therapy using methylene blue as a photosensitizer promotes additional benefits in periodontal treatment?”
2.1. Study Design
This review analyzed randomized clinical trials that investigated the effects of antimicrobial photodynamic therapy (aPDT), mediated by methylene blue, in patients diagnosed with periodontitis (Stage 1 to 4). The objective was to demonstrate the potential clinical benefits of this therapy in individuals without systemic conditions, those with diagnosed systemic disorders, or those presenting deleterious habits that negatively impact periodontal health. Accordingly, the following primary clinical parameters were evaluated: Probing Depth (PD), Bleeding on Probing (BOP), Clinical Attachment Level (CAL), Plaque Index (PI), Gingival Index (GI), Gingival Recession (GR) or Gingival Level (GL). Secondary outcomes included microbiological and/or immunological analyses.
2.2. Eligibity Criteria
2.2.1. Inclusion Criteria
Randomized clinical trials; Studies that applied methylene blue as photosensitizer; Studies involving patients with periodontitis (stage 1 to 4), treated by adjuvant aPDT and accompanied for at least 3 months; Studies that included smokers; Studies involving patients with furcation lesions and residual periodontal pockets; Studies that evaluated periodontal clinical parameters and/or microbiological and/or immunological analysis; Studies involving patients with periodontitis and systemic diseases; Studies in English language.
2.2.2. Exclusion Criteria
Studies that used other photosensitizer than methylene blue; Animal or in-vitro studies; Studies that exclusively evaluated gingivitis; Studies that evaluated peri-implantitis or periimplant mucositis; Case-series; Studies presenting insufficient or unclear information that hindered data extraction; absence of response from authors after e-mail requesting additional information.
2.3. Search Strategy
The research was conducted in the MEDLINE (PubMed) database using keywords combined with Boolean operators (OR, AND). All articles published between 2009 and August 2024 were included, with a restriction to publications in English. The search strategy involved the terms "periodontal disease and antimicrobial photodynamic therapy" and "periodontitis and antimicrobial photodynamic therapy," with the selection of "clinical trial" as the article type. In addition to the electronic search, manual searches were also performed to complement the results obtained.
2.4. Study Selection
For the selection of studies, the titles and abstracts were initially evaluated, followed by a full-text assessment. The studies that met the criteria outlined in this review were then subjected to data acquisition and risk of bias analysis.
2.5. Data Collection Process
In the data collection process, two investigators (HHCO and RF) were responsible for the data collection and review. When necessary, the authors of the selected articles were contacted to clarify any doubts.
2.6. Risk of Bias
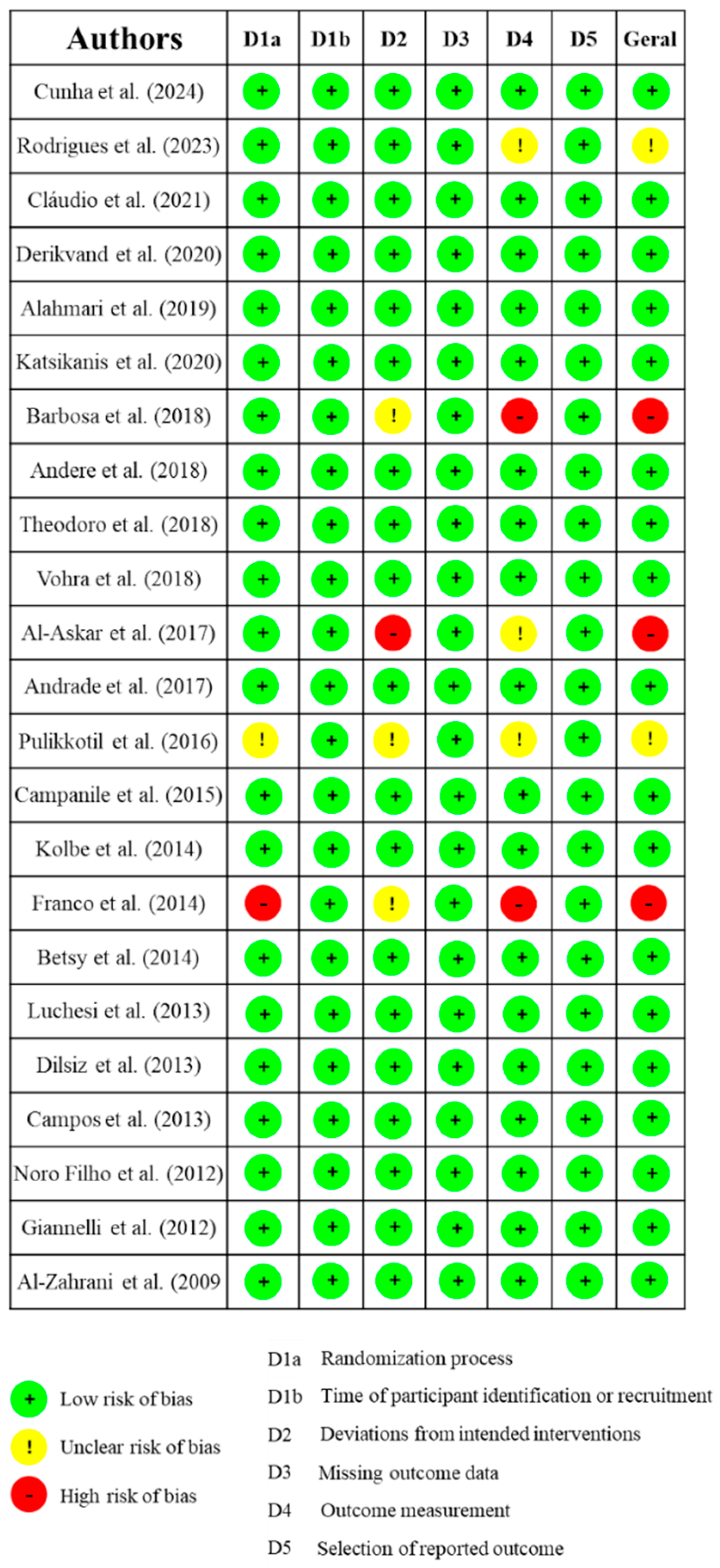
All the studies selected for this review underwent a risk of bias assessment. This assessment was conducted using the Cochrane Risk of Bias tool for randomized trials (RoB 2.0), which considers five domains: (D1) Randomization process and timing of participant identification or recruitment; (D2) Deviations from intended interventions; (D3) Missing outcome data; (D4) Outcome measurement; (D5) Selection of reported outcomes. Based on the analysis of these studies, they were classified as having high risk of bias (+), low risk of bias (-), or unclear risk of bias (!).
2.7. Data Analysis
For the data synthesis, the following information was collected from the selected articles: authors and year of publication, clinical parameters assessed, microbiological parameters assessed, study design type, number of patients involved in the research, the underlying disease of the patients involved, data related to the laser used, its dosimetry, the light source, whether local anesthesia was used for the procedure, whether pre-irradiation irrigation was performed, the concentration of the dye, the pre-irradiation time of the PS, the frequency of aPDT sessions, and the main results found.
3. Results
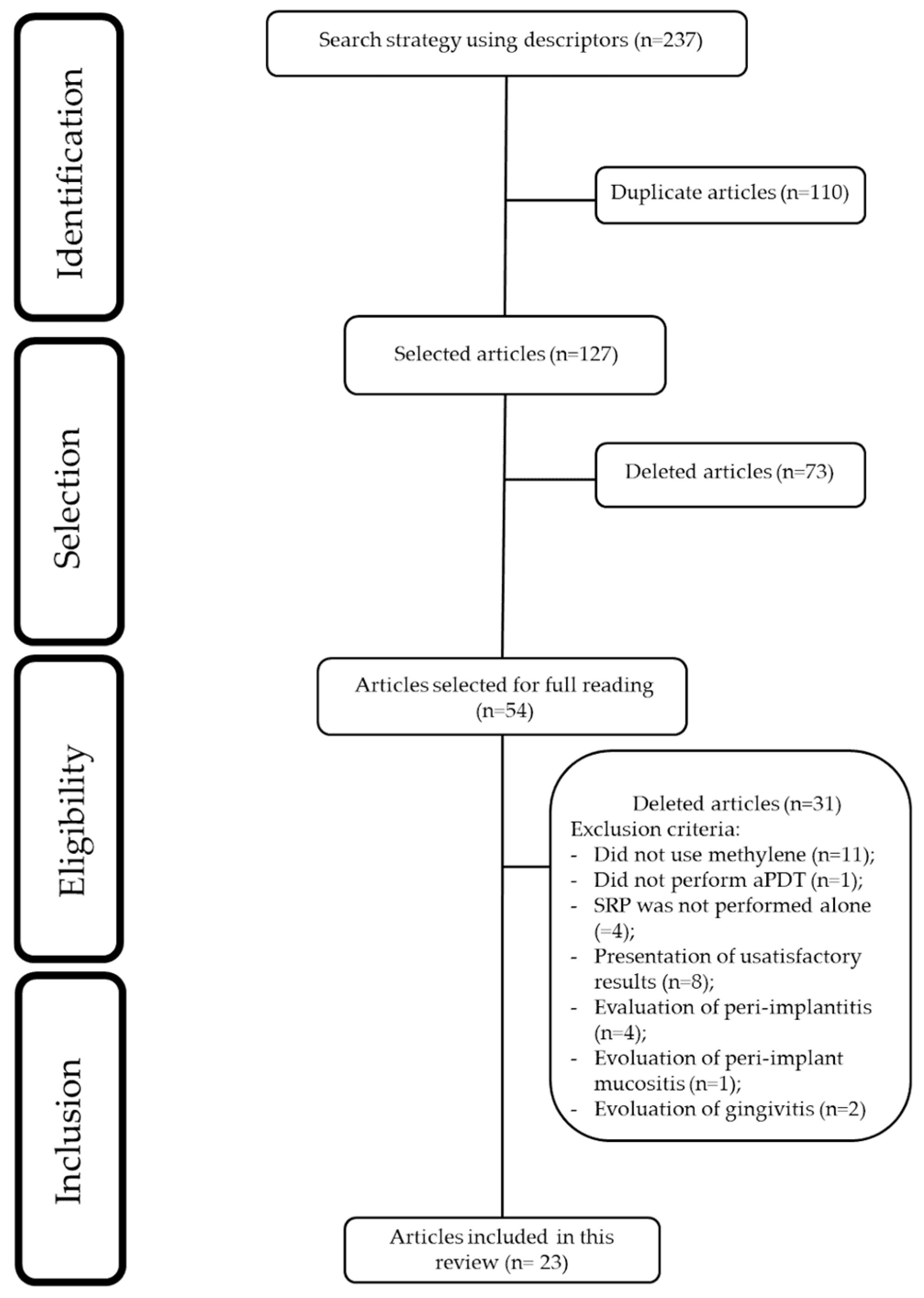
A total of 237 potentially relevant articles for this review were found. Using the descriptor “periodontal disease and antimicrobial photodynamic therapy,” 123 articles were selected, and with the descriptor “periodontitis and antimicrobial photodynamic therapy,” 114 articles were selected. Using the “Rayyan” platform, duplicate articles were excluded. After reading the titles and abstracts, 73 articles were excluded. Following a full-text review of the selected articles, 30 articles were excluded. Ultimately, 23 articles were included in this review.
Figure 1.
Flowchart of study selection.
3.1. Clinical Studies Included sin This Review
The clinical trials selected for this integrative review addressed different patient profiles. Table 1 shows the quantitative distribution of these studies.
Table 2 provides a summary of the studies selected for this review. Table 3 presents the follow-up periods of the clinical trials. Table 5 displays the data on statistically significant differences between the test and control groups for each variable.
The studies included in this review employed either a split-mouth design (n=9) [16,18,22,23,25,26,28,29,31] or a parallel-group design (n=14) [9,10,11,12,13,14,15,17,19,20,21,24,27,30].
Additionally, only (n=6) [10,14,17,27,28,31] studies evaluated microbiological parameters. One study assessed levels of P. gingivalis (Pg) and P. intermedia (Pi) [10], while another analyzed levels of P. gingivalis (Pg), P. micra (Pm), and P. intermedia (Pi) [17]. Levels of P. gingivalis (Pg), A. actinomycetemcomitans (Aa), T. forsythia (Tf), T. denticola (Td), P. intermedia (Pi), and P. micra (Pm) were evaluated in [27]. Other studies examined levels of A. actinomycetemcomitans (Aa), P. gingivalis (Pg), and T. forsythia (Tf) [14,28,31].
Local anesthesia was used in 11 studies [10,14,16,17,18,20,23,25,28,29,30]. In contrast, 6 studies did not use local anesthesia [11,15,19,21,22,26]. Its use was not reported in 5 studies [9,12,24,27,31], and in 1 study it was administered only if necessary [13].
Local irrigation after photosensitization was performed in 9 studies [11,14,18,20,21,24,25,28,29], whereas in 11 studies it was not performed [9,10,13,15,16,17,19,22,26,27,30]. In 3 studies, this information was not reported [12,23,31].
Regarding the pre-irradiation time, the studies were quite heterogeneous, with durations ranging from 10 seconds [13,15,30], 1 minute [9,10,14,17,20,22,27,28,29], 2 minutes [16], 3 minutes [24,25], to 5 minutes [11,18,19,21,23,26,31]. Only one study did not report the pre-irradiation time used [12].
3.2. Risk of Bias Assessment
The risk of bias assessment identified 19 clinical trials as having a low risk of bias [9,10,13,14,15,16,17,19,20,21,24,25,26,27,28,29,30,31]. In contrast, three studies were classified as having an unclear risk of bias [18];[22], and three were considered to have a high risk of bias [11,12,23].
The studies deemed to have a high risk of bias received this classification primarily due to the absence of methodological details regarding randomization, which made it unclear whether adequate blinding of researchers was implemented [11,12,23]. In one of the studies categorized as having an unclear risk of bias, baseline characteristics of the participants were not sufficiently reported to determine potential differences between groups, and homogeneity among groups was not addressed [18]. Additionally, the randomization process was inadequately described in one of the included studies [22].
Figure 2.
Risk of bias.
4. Discussion
This integrative literature review aimed to examine the efficacy of antimicrobial photodynamic therapy (aPDT), mediated by the methylene blue photosensitizer, as an adjuvant in the treatment of periodontitis. Upon analyzing the selected articles, it was observed that most clinical studies demonstrated favorable outcomes for aPDT as an adjunct to scaling and root planing (SRP) in the non-surgical management of periodontal disease (PD), albeit often limited to a single assessed periodontal parameter [11,18,19,20,22,23,24,25,26,27,29,31]. However, several clinical trials reported no statistically significant differences between aPDT and the control group (SRP) for any of the evaluated clinical parameters [10,12,13,14,17,21,28].
Most articles in this review focused on the application of aPDT in chronic periodontitis treatment [10,11,12,13,14,15,16,17,18,19,20,21,23,30,31] or in residual pockets [27,28,29], among patients undergoing periodontal maintenance therapy. Notably, methylene blue (MB) was consistently used as the photosensitizer (PS) in combination with 660–670 nm laser light, which corresponds to the optimal absorption spectrum of this PS.
It is crucial to emphasize that all included articles underwent rigorous risk of bias assessment, even within the context of an integrative literature review. The evaluation of risk of bias in randomized clinical trials is paramount to ensure the reliability of reported findings. Studies with a high risk of bias may yield skewed conclusions, thereby compromising the integrity of the results and subsequent clinical decision-making. Furthermore, poor randomization and lack of masking may result in an overestimation of the intervention effects in randomized clinical trials [42].
The distribution of experimental designs among the reviewed studies was relatively homogeneous. The split-mouth model was employed in 9 studies [16,18,22,23,25,26,28,29,31] whereas the parallel-group design was utilized in 14 studies [9,10,11,12,13,14,15,17,19,20,21,24,27,30]. Split-mouth studies enrolled as few as 12 or 13 patients [29,31] or up to 26 patients [26]. In contrast, the largest parallel-group trials recruited 83 and 88 patients, respectively [15,24].
Regarding probing depth (PD) outcomes, several included studies reported PD reduction in patients treated with scaling and root planing (SRP) combined with aPDT (n=9) [18,19,20,24,25,26,27,29,31]. Notably, only one clinical trial demonstrated PD reduction favoring the SRP-alone group [9], though this involved patients with diabetes, a population with distinct clinical considerations. Despite these promising findings for aPDT as an adjuvant therapy in PD reduction, it is critical to acknowledge that numerous other studies (n=13) reported no statistically significant superior outcomes for aPDT [10,11,12,13,14,15,16,17,21,22,23,28,30].
Thus, while the data suggest potential benefits of aPDT, it is imperative to exercise caution in interpreting these results as conclusive evidence for its widespread clinical validation. Significant heterogeneity exists across studies, particularly regarding patient profiles (e.g., systemic conditions like diabetes), PS concentration, number of aPDT applications, and light dosimetry parameters. These methodological discrepancies underscore the need for standardized protocols and further high-quality randomized controlled trials to establish definitive conclusions.
Improvement in bleeding on probing (BOP) in patients who received aPDT as an adjunctive treatment was observed in several studies (n=7) [11,22,23,24,26,29,31]. A common feature among most of these studies was the use of a split-mouth design (n=5) [22,23,26,29,31]. Moreover, the majority of studies used a fiber-optic tip for intrapocket light delivery [23,24,26,29,31]; which may favor the photodegradation reaction of the photosensitizer. However, there was considerable heterogeneity regarding photosensitizer concentration, pre-irradiation time, and number of applications, which introduces bias when evaluating the actual efficacy of this clinical parameter.
Furthermore, four studies reported a statistically significant improvement in clinical attachment level (CAL), with better outcomes observed in patients who received adjunctive aPDT [24,25,26,29]. These findings suggest that aPDT may contribute to additional improvements in CAL when compared to conventional treatment alone. However, this interpretation should be approached with caution due to variability in the aPDT application protocols and differences in patient characteristics across the studies. Such heterogeneity reflects inconsistencies in the outcomes, underscoring the need for further in-depth analysis.
This analysis also extends to other clinical parameters, such as plaque index (PI) and gingival recession (GR). Regarding PI, only a few studies (n=2) reported improvement in this clinical parameter among patients treated with aPDT [11,23]. In contrast, other studies found lower plaque levels in patients treated with scaling and root planing (SRP) alone [15,16,30]. Similarly, studies assessing gingival recession (GR) were limited. Most of those that did analyze GR reported no statistically significant differences between groups [9,18,20,27,31].
In recent years, the potential of aPDT to secondarily promote periodontal healing has been widely discussed, particularly when low-level laser is used as the light source. In animal studies, this effect has been reported by some authors [39,40]. Although certain clinical studies did not demonstrate significant improvements in clinical parameters, they showed favorable outcomes regarding inflammatory markers, such as a reduction in MMP-8 [41]. Additionally, one study reported a decrease in TNF-α levels in patients treated with aPDT [9]. There is also the possibility of using low-level laser therapy independently, either immediately after SRP or in alternating sessions with aPDT, to promote tissue repair. However, it is important to emphasize that this approach does not fall within the standard aPDT protocol.
In relation to repetition of applications, a study which applied between 4 and 10 sessions of aPDT, suggests that increasing the number of aPDT applications may enhance clinical outcomes [26]. The highest number of aPDT sessions among all those included in this review, resulted in improvements across all evaluated clinical parameters (probing depth [PD], bleeding on probing [BOP], and clinical attachment level [CAL]). It also employed a longer pre-irradiation time (5 minutes), compared to other studies. This methodology remains underexplored, particularly in studies assessing the effectiveness of methylene blue as a photosensitizer. A pioneering study highlighted the benefits of aPDT using the HELBO® system in patients undergoing periodontal maintenance [43]. Five sessions of aPDT over a two-week period led to clinical improvements that persisted for up to six months post-treatment. However, even a single application of aPDT yielded positive results in clinical parameters (PD, BOP, CAL, and PI), despite a shorter pre-irradiation time of 3 minutes [24]. Therefore, the assumption that increasing the number of aPDT sessions will necessarily lead to better periodontal outcomes remains inconclusive and warrants further investigation through well-designed clinical trials.
Antimicrobial photodynamic therapy (aPDT) was applied twice a week for the treatment of residual pockets, resulting in a reduction in probing depth and C-reactive protein levels. These benefits were sustained for up to three months [27]. Additionally, the treatment resulted in the absence of residual pockets at the end of the study. All three articles included in this review that assessed residual pockets included patients diagnosed with periodontitis who had previously undergone supportive periodontal therapy prior to the experimental intervention [27,28,29]. Only two studies [27,29] demonstrated improvement in probing depth for patients who received aPDT. Improvements in bleeding on probing (BOP) and clinical attachment level (CAL) were also reported [29].
The use of aPDT in the treatment of furcation lesions did not demonstrate improvements in periodontal clinical parameters. A study [14] that focused on class II furcation lesions did not find specific clinical differences between the groups. Besides that, the researchers observed a reduction in Porphyromonas gingivalis (Pg.) and Tannerella forsythia (Tf.) bacteria during the 6-month follow-up. This was the only study included in this review that addressed furcation lesion treatment, and it is important to note that no biomaterial was used in the treatment.
In addition to surgical approaches, other alternatives have been proposed. A combination of high-intensity laser was used to remove all epithelium from the periodontal pocket before aPDT [26]. This technique resulted in improvements in clinical parameters, with long-lasting effects observed up to one year after treatment.
There are still few publications on the use of aPDT in patients with compromised systemic conditions. In the case of patients with diabetes, aPDT was compared or combined with antibiotics, such as doxycycline. This combination did not result in improvements in periodontal clinical parameters, although a reduction in glycated hemoglobin was noted in the group that received antibiotics alone [13]. These results suggest that, while aPDT has potential, it may not be as effective when used alone in patients with diabetes, highlighting the need for further investigation in this area. In a study analyzing patients with type 1 diabetes, a significant reduction in TNF-α levels in crevicular fluid in the group treated with aPDT was observed [9]. Additionally, plaque index varied between patients with and without diabetes, with diabetes group showing a higher plaque index. There were no statistically significant differences in probing depth between the diabetes and non-diabetes groups that only underwent scaling, nor were there differences in the groups treated with aPDT. On the other hand, in a study of patients with HIV [31], there was a beneficial effect of aPDT, with improvements in clinical parameters, and the beneficial effects persisted for up to six months. However, no significant differences in microbial composition were found when compared to the group that received conventional treatment (SRP). More recently, a study has demonstrated promising results in patients with Down syndrome [49]. Therefore, future research may include a broader range of patients with other special needs or specific conditions, such as those in intensive care units.
The variability of results is also evident in studies involving smoking patients. aPDT may contribute to improvements in clinical parameters, but none of the studies showed statistically promising results for therapy in the smoking group [15,16,17]. Worse clinical outcomes, for the smoking group compared to non-smokers, as higher probing depth (PD) and clinical attachment level (CAL) values were observed in smokers at the 3-month follow-up [15]. This indicates uncertainty regarding the effectiveness of the therapy in this patient profile.
A systematic review reported noteworthy findings. The authors observed that in studies with parallel and split-mouth designs, there were no significant differences in clinical outcomes between the approaches. They also highlighted that an application time of 60 seconds was more effective in reducing probing depth and improving clinical attachment gain. However, due to the wide variety of protocols used in the studies, it was not possible to conduct a consistent analysis regarding the type of photosensitizer or laser parameters. What could be observed, however, is that all studies employed wavelengths between 660 and 680 nm, which coincide with the absorption peaks of common photosensitizers such as phenothiazine chloride (HELBO®) and methylene blue (Periowave® or other preparations) [36]. This suggests that the positive effects of aPDT may be linked to these specific evaluation conditions, although further research is needed. A degree of positive results can be noted when analyzing the findings of systematic reviews [44]. On the other hand, another review indicated that despite aPDT being extensively investigated, evidence of its superior clinical benefits compared to SRP alone remains uncertain. The analyzed data did not show consistent improvements in parameters such as probing depth (PD), bleeding on probing (BOP), and clinical attachment level (CAL) six months after treatment [32]. It is also important to note that all these systematic reviews did not focus exclusively on methylene blue but included various types of photosensitizers, which is the primary focus of this review.
Unfortunately, some studies employ an inappropriate combination of photosensitizer (PS) and laser wavelength, mismatched with the PS absorption spectrum [25,45,46,47]. The main principle in aPDT is the absorption peak of FS must be in the same range of laser wavelength to create a photodynamic reaction (The Grotthuss–Draper law - Principle of Photochemical Activation). That is why blue FS (toluidine and methylene blue) are used with red lasers. It is of utmost importance that the combination of the photosensitizer and laser wavelength is appropriately applied in clinical trials, and this information should be critically evaluated and reported by journal reviewers [48].
Some of the studies addressed in this review presented satisfactory clinical outcomes in the group of patients who received aPDT, with these benefits typically being short-term, showing improvement within 1 month of follow-up [11]. However, the 6-month follow-up did not show a statistically significant difference between the patients who received aPDT and those who only received scaling and root planing (SRP). This is further compounded by the fact that these studies involved single-session aPDT. Studies demonstrate that increasing the pre-irradiation time and performing multiple sessions of aPDT appear to benefit both clinical and immunological outcomes [23,26].
The lack of consensus on protocols, along with the variability of clinical outcomes among patients with different systemic conditions and habits, such as smoking, may limit the universal applicability of the technique. Future investigations should prioritize controlled and randomized clinical trials that adopt a more rigorous methodological approach, aiming to conduct long-term follow-ups and therapy applications to assess the maintenance of aPDT benefits over time and its true effectiveness in specific patient subgroups.
5. Conclusions
Antibacterial photodynamic therapy associated with methylene blue seems to contribute to the clinical improvement of periodontal parameters, particularly probing depth (PD), bleeding on probing (BOP), clinical attachment level (CAL), and plaque index (PI). However, the heterogeneity of clinical trials creates a duality regarding the role this therapy may play for patients with periodontitis. In the reviewed studies, there is a general trend of absence of statistically significant between groups over the evaluation periods. However, when differences are found, the group that received aPDT tends to show more satisfactory results, highlighting its true additional clinical benefits in periodontal health.
6. Future Directions
Based on the findings of this review, aPDT using methylene blue presents promising but still inconclusive implications for the future of periodontics. While several studies report short-term clinical improvements, the variability in patient profiles, application protocols, and follow-up periods raises concerns about reproducibility and generalizability. Future directions in periodontal therapy should focus on standardizing aPDT protocols, including photosensitizer concentration (with an appropriate light source), irradiation time, and frequency of application (multiple sessions). Moreover, further randomized controlled trials with robust design and long-term molecular and clinical follow-up are essential to establish aPDT as a reliable adjunctive treatment. If such consistency and efficacy can be demonstrated, aPDT may become a valuable tool in the personalized management of periodontal disease, particularly for patients with disabilities, systemic conditions, and users of alternative forms of tobacco consumption (waterpipe or electronic smoking device users) or treatment-resistant profiles.
Author Contributions
Conceptualization, CAD.; methodology, HHCO.; validation, RF; formal analysis, HHCO; investigation, RF; resources, CAD.; data curation, RF.; writing—original draft preparation, RF.; writing—review and editing, GMCT, CAD; visualization, RF.; supervision, RF; project administration, CAD. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Material will be available upon request to interested researchers.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Passanezi, E.; Damante, C. A.; de Rezende, M. L.; Greghi, S. L. Lasers in periodontal therapy. Periodontol. 2000 2015, 67, 268–291. [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M. S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 Suppl 22(Suppl 22), 4–60. [CrossRef]
- Figuero, E.; Roldán, S.; Serrano, J.; Escribano, M.; Martín, C.; Preshaw, P. M. Efficacy of adjunctive therapies in patients with gingival inflammation: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 Suppl 22, 125–143. [CrossRef]
- Salvi, G. E.; Stähli, A.; Schmidt, J. C.; Ramseier, C. A.; Sculean, A.; Walter, C. Adjunctive laser or antimicrobial photodynamic therapy to non-surgical mechanical instrumentation in patients with untreated periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 Suppl 22, 176–198. [CrossRef]
- Gois, M. M.; Kurachi, C.; Santana, E. J.; Mima, E. G.; Spolidório, D. M.; Pelino, J. E.; Salvador Bagnato, V. Susceptibility of Staphylococcus aureus to porphyrin-mediated photodynamic antimicrobial chemotherapy: An in vitro study. Lasers Med. Sci. 2010, 25, 391–395. [CrossRef]
- Ghorbani, J.; Rahban, D.; Aghamiri, S.; Teymouri, A.; Bahador, A. Photosensitizers in antibacterial photodynamic therapy: an overview. Laser therapy. 2018, 827(4), 293–302. [CrossRef]
- Figueiredo-Godoi, L.M.A.; Garcia, M.T.; Pinto, J.G.; Ferreira-Strixino, J.; Faustino, E.G.; Pedroso, L.L.C.; Junqueira, J.C. Antimicrobial Photodynamic Therapy Mediated by Fotenticine and Methylene Blue on Planktonic Growth, Biofilms, and Burn Infections of Acinetobacter baumannii. Antibiotics. 2022, 11, 619. [CrossRef]
- Usacheva M. N; Teichert M. C.; Sievert C. E.; Biel M. A. Effect of Cat on the photobactericidal efficacy of methylene blue and toluidine blue against gram-negative bacteria and the dye affinity for lipopolysaccharides. Lasers Surg Med. 2006; 38(10):946-54.
- Cunha, P. O.; Gonsales, I. R.; Greghi, S. L. A.; Sant'ana, A. C. P.; Honório, H. M.; Negrato, C. A.; Zangrando, M. S. R.; Damante, C. A. Adjuvant antimicrobial photodynamic therapy improves periodontal health and reduces inflammatory cytokines in patients with type 1 diabetes mellitus. J. Appl. Oral Sci. 2024, 32, e20240258. [CrossRef]
- Cláudio, M. M.; Nuernberg, M. A. A.; Rodrigues, J. V. S.; Belizário, L. C. G.; Batista, J. A.; Duque, C.; Garcia, V. G.; Theodoro, L. H. Effects of multiple sessions of antimicrobial photodynamic therapy (aPDT) in the treatment of periodontitis in patients with uncompensated type 2 diabetes: A randomized controlled clinical study. Photodiagnosis Photodyn. Ther. 2021, 35, 102451. [CrossRef]
- Barbosa, F. I.; Araújo, P. V.; Machado, L. J. C.; Magalhães, C. S.; Guimarães, M. M. M.; Moreira, A. N. Effect of photodynamic therapy as an adjuvant to non-surgical periodontal therapy: Periodontal and metabolic evaluation in patients with type 2 diabetes mellitus. Photodiagnosis Photodyn. Ther. 2018, 22, 245–250. [CrossRef]
- Al-Askar, M.; Al-Kheraif, A. A.; Ahmed, H. B.; Kellesarian, S. V.; Malmstrom, H.; Javed, F. Effectiveness of mechanical debridement with and without adjunct antimicrobial photodynamic therapy in the treatment of periodontal inflammation among patients with prediabetes. Photodiagnosis Photodyn. Ther. 2017, 20, 91–94. [CrossRef]
- Al-Zahrani, M. S.; Bamshmous, S. O.; Alhassani, A. A.; Al-Sherbini, M. M. Short-term effects of photodynamic therapy on periodontal status and glycemic control of patients with diabetes. J. Periodontol. 2009, 80, 1568–1573. [CrossRef]
- Luchesi, V. H.; Pimentel, S. P.; Kolbe, M. F.; Ribeiro, F. V.; Casarin, R. C.; Nociti, F. H., Jr.; Sallum, E. A.; Casati, M. Z. Photodynamic therapy in the treatment of class II furcation: A randomized controlled clinical trial. J. Clin. Periodontol. 2013, 40, 781–788. [CrossRef]
- AlAhmari, F.; Ahmed, H. B.; Al-Kheraif, A. A.; Javed, F.; Akram, Z. Effectiveness of scaling and root planning with and without adjunct antimicrobial photodynamic therapy in the treatment of chronic periodontitis among cigarette-smokers and never-smokers: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2019, 25, 247–252. [CrossRef]
- Katsikanis, F.; Strakas, D.; Vouros, I. The application of antimicrobial photodynamic therapy (aPDT, 670 nm) and diode laser (940 nm) as adjunctive approach in the conventional cause-related treatment of chronic periodontal disease: A randomized controlled split-mouth clinical trial. Clin. Oral Investig. 2020, 24, 1821–1827. [CrossRef]
- Theodoro, L. H.; Assem, N. Z.; Longo, M.; Alves, M. L. F.; Duque, C.; Stipp, R. N.; Vizoto, N. L.; Garcia, V. G. Treatment of periodontitis in smokers with multiple sessions of antimicrobial photodynamic therapy or systemic antibiotics: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2018, 22, 217–222. [CrossRef]
- Rodrigues, R. D.; Araujo, N. S.; Filho, J. M. P.; Vieira, C. L. Z.; Ribeiro, D. A.; Dos Santos, J. N.; Cury, P. R. Photodynamic therapy as adjunctive treatment of single-rooted teeth in patients with grade C periodontitis: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2023, 44, 103776. [CrossRef]
- Derikvand, N.; Ghasemi, S. S.; Safiaghdam, H.; Piriaei, H.; Chiniforush, N. Antimicrobial Photodynamic Therapy with Diode laser and Methylene blue as an adjunct to scaling and root planning: A clinical trial. Photodiagnosis Photodyn. Ther. 2020, 31, 101818. [CrossRef]
- Andere, N. M. R. B.; Dos Santos, N. C. C.; Araujo, C. F.; Mathias, I. F.; Rossato, A.; de Marco, A. C.; Santamaria, M., Jr.; Jardini, M. A. N.; Santamaria, M. P. Evaluation of the local effect of nonsurgical periodontal treatment with and without systemic antibiotic and photodynamic therapy in generalized aggressive periodontitis. A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2018, 24, 115–120. [CrossRef]
- Andrade, P. V.C.; Euzebio Alves, V. T.; de Carvalho, V. F.; De Franco Rodrigues, M.; Pannuti, C. M.; Holzhausen, M.; De Micheli, G.; Conde, M. C. Photodynamic therapy decrease immune-inflammatory mediators levels during periodontal maintenance. Lasers Med. Sci. 2017, 32, 9–17. [CrossRef]
- Pulikkotil, S. J.; Toh, C. G.; Mohandas, K.; Leong, K. Effect of photodynamic therapy adjunct to scaling and root planing in periodontitis patients: A randomized clinical trial. Aust. Dent. J. 2016, 61, 440–445. [CrossRef]
- Franco, E. J.; Pogue, R. E.; Sakamoto, L. H.; Cavalcante, L. L.; Carvalho, D. R.; de Andrade, R. V. Increased expression of genes after periodontal treatment with photodynamic therapy. Photodiagnosis Photodyn. Ther. 2014, 11, 41–47. [CrossRef]
- Betsy, J.; Prasanth, C. S.; Baiju, K. V.; Prasanthila, J.; Subhash, N. Efficacy of antimicrobial photodynamic therapy in the management of chronic periodontitis: A randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 573–581. [CrossRef]
- Dilsiz, A.; Canakci, V.; Aydin, T. Clinical effects of potassium-titanyl-phosphate laser and photodynamic therapy on outcomes of treatment of chronic periodontitis: A randomized controlled clinical trial. J. Periodontol. 2013, 84, 278–286. [CrossRef]
- Giannelli, M.; Formigli, L.; Lorenzini, L.; Bani, D. Combined photoablative and photodynamic diode laser therapy as an adjunct to non-surgical periodontal treatment: A randomized split-mouth clinical trial. J. Clin. Periodontol. 2012, 39, 962–970. [CrossRef]
- Campanile, V. S. M.; Giannopoulou, C.; Campanile, G.; Cancela, J. A.; Mombelli, A. Single or repeated antimicrobial photodynamic therapy as adjunct to ultrasonic debridement in residual periodontal pockets: Clinical, microbiological, and local biological effects. Lasers Med. Sci. 2015, 30, 27–34. [CrossRef]
- Kolbe, M. F.; Ribeiro, F. V.; Luchesi, V. H.; Casarin, R. C.; Sallum, E. A.; Nociti, F. H., Jr.; Ambrosano, G. M.; Cirano, F. R.; Pimentel, S. P.; Casati, M. Z. Photodynamic therapy during supportive periodontal care: clinical, microbiologic, immunoinflammatory, and patient-centered performance in a split-mouth randomized clinical trial. J. Periodontol. 2014, 85, e277–e286. [CrossRef]
- Campos, G. N.; Pimentel, S. P.; Ribeiro, F. V.; Casarin, R. C.; Cirano, F. R.; Saraceni, C. H.; Casati, M. Z. The adjunctive effect of photodynamic therapy for residual pockets in single-rooted teeth: A randomized controlled clinical trial. Lasers Med. Sci. 2013, 28, 317–324. [CrossRef]
- Vohra, F.; Akram, Z.; Bukhari, I. A.; Sheikh, S. A.; Javed, F. Short-term effects of adjunctive antimicrobial photodynamic therapy in obese patients with chronic periodontitis: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2018, 21, 10–15. [CrossRef]
- Noro Filho, G. A.; Casarin, R. C.; Casati, M. Z.; Giovani, E. M. PDT in non-surgical treatment of periodontitis in HIV patients: A split-mouth, randomized clinical trial. Lasers Surg. Med. 2012, 44, 296–302. [CrossRef]
- Jervøe-Storm, P. M.; Bunke, J.; Worthington, H. V.; Needleman, I.; Cosgarea, R.; MacDonald, L.; Walsh, T.; Lewis, S. R.; Jepsen, S. Adjunctive antimicrobial photodynamic therapy for treating periodontal and peri-implant diseases. Cochrane Database Syst. Rev. 2024, 7, CD011778. [CrossRef]
- Vohra, F.; Akram, Z.; Safii, S. H.; Vaithilingam, R. D.; Ghanem, A.; Sergis, K.; Javed, F. Role of antimicrobial photodynamic therapy in the treatment of aggressive periodontitis: A systematic review. Photodiagnosis Photodyn. Ther. 2016, 13, 139–147. [CrossRef]
- Javed, F.; Qadri, T.; Ahmed, H. B.; Al-Hezaimi, K.; Corbet, F. E.; Romanos, G. E. Is photodynamic therapy with adjunctive non-surgical periodontal therapy effective in the treatment of periodontal disease under immunocompromised conditions? J. Coll. Physicians Surg. Pakistan 2013, 23, 731–736. [CrossRef]
- Sgolastra, F.; Petrucci, A.; Gatto, R.; Marzo, G.; Monaco, A. Photodynamic therapy in the treatment of chronic periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2013, 28, 669–682. [CrossRef]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Graziani, F.; Gatto, R.; Monaco, A. Adjunctive photodynamic therapy to non-surgical treatment of chronic periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2013, 40, 514–526. [CrossRef]
- Atieh, M. A. Photodynamic therapy as an adjunctive treatment for chronic periodontitis: A meta-analysis. Lasers Med. Sci. 2010, 25, 605–613. [CrossRef]
- Azarpazhooh, A.; Shah, P. S.; Tenenbaum, H. C.; Goldberg, M. B. The effect of photodynamic therapy for periodontitis: A systematic review and meta-analysis. J. Periodontol. 2010, 81, 4–14. [CrossRef]
- de Almeida, J. M.; Theodoro, L. H.; Bosco, A. F.; Nagata, M. J.; Bonfante, S.; Garcia, V. G. Treatment of experimental periodontal disease by photodynamic therapy in rats with diabetes. J. Periodontol. 2008, 79, 2156–2165. [CrossRef]
- Prates, R. A.; Yamada, A. M.; Suzuki, L. C.; França, C. M.; Cai, S.; Mayer, M. P.; Ribeiro, A. C.; Ribeiro, M. S. Histomorphometric and microbiological assessment of photodynamic therapy as an adjuvant treatment for periodontitis: A short-term evaluation of inflammatory periodontal conditions and bacterial reduction in a rat model. Photomed. Laser Surg. 2011, 29, 835–844. [CrossRef]
- Queiroz, A. C.; Suaid, F. A.; de Andrade, P. F.; Oliveira, F. S.; Novaes, A. B., Jr.; Taba, M., Jr.; Palioto, D. B.; Grisi, M. F.; Souza, S. L. Adjunctive effect of antimicrobial photodynamic therapy to nonsurgical periodontal treatment in smokers: A randomized clinical trial. Lasers Med. Sci. 2015, 30, 617–625. [CrossRef]
- Savović, J.; Turner, R. M.; Mawdsley, D.; Jones, H. E.; Beynon, R.; Higgins, J. P. T.; Sterne, J. A. C. Association Between Risk-of-Bias Assessments and Results of Randomized Trials in Cochrane Reviews: The ROBES Meta-Epidemiologic Study, American Journal of Epidemiology, Volume 187, Issue 5, May 2018, Pages 1113–1122. doi: 10.1093/aje/kwx344.
- Lulic, M.; Leiggener Görög, I.; Salvi, G. E.; Ramseier, C. A.; Mattheos, N.; Lang, N. P. One-year outcomes of repeated adjunctive photodynamic therapy during periodontal maintenance: A proof-of-principle randomized-controlled clinical trial. J. Clin. Periodontol. 2009, 36, 661–666. [CrossRef]
- Moro, M. G.; de Carvalho, V. F.; Godoy-Miranda, B. A.; Kassa, C. T.; Horliana, A. C. R. T.; Prates, R. A. Efficacy of antimicrobial photodynamic therapy (aPDT) for nonsurgical treatment of periodontal disease: A systematic review. Lasers Med. Sci. 2021, 36, 1573–1590. [CrossRef]
- Malgikar, S.; Harinath, R.; Vidya, S.; Satyanarayana.; Vikram, R.; Julieta, J. Clinical effects of photodynamic and low-level laser therapies as an adjunct to scaling and root planing of chronic periodontitis: A split-mouth randomized controlled clinical trial. Indian Journal of Dental Research, Mar–Apr 2016, 27, 121-126. |. [CrossRef]
- Annaji, S., Sarkar, I., Rajan, P., Pai, J., Malagi, S., Bharmappa, R., Kamath, V. Efficacy of Photodynamic Therapy and Lasers as an Adjunct to Scaling and Root Planing in the Treatment of Aggressive Periodontitis - A Clinical and Microbiologic Short Term Study. Journal of clinical and diagnostic research. JCDR. 2016, 10, ZC08–ZC12. doi: 10.7860/JCDR/2016/13844.7165.
- Lui, J.; Corbet, E. F.; Jin, L. Combined photodynamic and low-level laser therapies as an adjunct to nonsurgical treatment of chronic periodontitis. J. Periodontal Res. 2011, 46, 89–96. [CrossRef]
- Damante CA. Laser parameters in systematic reviews. J Clin Periodontol. 2021 48, 550-552. Epub 2021 Jan 31. PMID: 33522004. [CrossRef]
- Ferreira, R.; Greghi, S. L. A.; Sant'Ana, A. C. P.; Zangrando, M. S. R.; Damante, C. A. Multiple Sessions of Antimicrobial Photodynamic Therapy Improve Periodontal Outcomes in Patients with Down Syndrome: A 12-Month Randomized Clinical Trial. Dentistry journal, 2025, 13, 33. [CrossRef]

Table 1.
Relationship between the number of selected studies and the addressed patient profile.
| Patient profile | Number of articles (n) | Reference |
| Diabetes | 5 | [9,10,11,12,13] |
| Furcation lesion | 1 | [14] |
| Smokers | 3 | [15,16,17] |
| Periodontitis | 9 | [18,19,20,21,22,23,24,25,26] |
| Residual periodontal pockets | 3 | [27,28,29] |
| Different patient profiles (Obesity and HIV) | 2 | [30] (Obesity); [31] (HIV) |
Table 2.
Clinical trials that evaluated the use of photodynamic therapy as an adjunct to scaling and root planing in periodontal treatment using MB as the photosensitizer (PS).
Table 2.
Clinical trials that evaluated the use of photodynamic therapy as an adjunct to scaling and root planing in periodontal treatment using MB as the photosensitizer (PS).
| Authors, year and participant (n) | wavelength | Laser parameters | Optic fiber | Concentration of dye | Repetition | Main results |
| Cunha et al. (2024) (n=38) [9] | 650 | 100mW/80s | Optic fiber (d=600μm) | 10 mg/ml | 3 sessions | SRP group presented greater values of PD (p<0.05). There was a significant reduction of TNF-α in crevicular fluid of patients treated by aPDT (p<0.05) |
| Rodrigues et al. (2023) (n=14) [18] | 660 | 100mW/0.25 mW/cm² / 14.94 J/cm² /10s | NR | 1% | 2 sessions | aPDT promoted better results of PD after 3 months. There was 18% less probability of presenting a final PD > 4 mm compared to SRP. |
| Cláudio et al. (2021) ** (n=34) [10] | 660 | 157 J/ cm²/100 mW/50s | Optic fiber (d=0.03 cm²) | 10 mg/ml | 3 sessions | aPDT presented a reduction of NRP after 3 and 6 months (p<0.05). |
| Derikvand et al. (2020) (n=50) [19] | 660 | 150 mW/ 60s | NR | 100 μg/mL | Single | Reduction in PD at aPDT group after 3 and 6 months, in comparison to SRP group (p<0.01) |
| Katsikanis et al. (2020) ** (n=21) [16] |
670 | 350 mW/ 0.445 W/ cm²/ 120s | Diameter - 1 cm | 1% | 3 sessions | Only PI presented statistically significant differences at baseline (p=0.038) in SRP group. |
| Alahmari et al. (2019) (n=83) [15] | 660 | 150 mW/75 mW/cm²/60 s | Optic fiber (d=600μm) | 0.005% | Single | Only PI in SRP group presented statistically significant differences (p< 0.05) after 1 month. PD and CAL were greater in S group When compared to NS group. |
| Barbosa et al. (2018) (n=12) [11] | 660 | 40mW/120s/4.8J | - | 10 mg/ml | Single | There was no difference between groups for PD and CAL (p >0.05). aPDT group presented better results for PI after 1 month and BOP after 6 months. |
| Andere et al. (2018) (n=36) [20] | 660 | 60 mW / 129 J/cm² / 60s | Optic fiber | 10 mg/ml | Single | Group UPD+CLM+aPDT presented greater CAL values when compared to UPD and UPD+aPDT (p < 0.05). |
| Theodoro et al. (2018) (n=51) [17] | 660 | 100mW/160 J/cm2/48s | Optic fiber (d= 0.03 cm2) | 10 mg/ml | 3 sessions | After 6 months, group MTZ + AMX and aPDT presented lower PD, greater CAL and less BOP, but without statistical significant differences between SRP and aPDT. |
| Vohra et al. (2018) ** (n=52) [30] | 670 | 150mW/60 s | Optic fiber (d=0.6 mm) | 0.005% | Single | PI was better for SRP group after 1.5 and 3 months (p<0.05). |
| Al-Askar et al. (2017) * (n=70) [12] | 670 | 150 mW/60 s | NR | 0.005% | Single | There was no difference between groups and periods. There was no difference in CBL in all groups at 3 and 6 months. |
| Andrade et al. (2017) (n=28) [21] | 660 | 40mW/90s/90J/cm² | Optic Fiber (d=200μm) | 0.01% | Single | There were no differences between groups. There was a reduction in IL-8 in aPDT group after 3 months (p=0.04). |
| Pulikkotil et al. (2016) (n=20) [22] |
Red LED (628Hz) | 628 Hz/ 20s | NR | NR | Single | There was a significant reduction in BOP after 3 months in aPDT group. (p<0.01). There was no differences in A.a. quantification. |
| Campanile et al. (2015) (n=28) [27] | 670 | 280 mW, ±0.2 dB | Optic fiber | NR | Twice a week | aPDT group presented reduction in PD after 3 and 6 months. There was a reduction in C reactive protein. There were no microbiological differences. |
| Kolbe et al. (2014) (n=22) [28] | 660 | 0.06W, 129J/cm², 60s | Optic fiber (d=600μm) | 10mg/ml | Single | There were no statistically significant differences in clinical parameters. Reduction in Pg., Aa., and inflammatory cytokines. |
| Franco et al. (2014) ** (n=15) [23] | 660 | 0.06W/cm², 90s, 5.4Jcm² | Optic fiber (d=0.4mm) | 0.01% | Once a week - total of 4 sessions | Reduction in BOP in aPDT group (p<0.05). Increase in RANK/OPG and FGF-2 levels. |
| Betsy et al. (2014) (n=88) [24] | 655 | 1W, 0.06W/cm²,60s | Optic fiber (d=0.5mm) | 10mg/ml | Single | Significant reductions in PD, CAL, BOP, PI and GI for aPDT group (p<0.05). |
| Luchesi et al. (2013) (n=37) [14] | 660 | 0.06W, 129J/cm², 60s | Optic fiber (d=600μm) | 10mg/ml | Single | There were no statistically significant differences in clinical parameters. Reduction in Pg., Aa., and inflammatory cytokines up to 6 months. |
| Dilsiz et al. (2013) (n=24) [25] | 808 | 0.1W, 6J, 60s | Optic fiber (d=300μm) | 1% | Single | aPDT group presented reduction in PD and CAL after 6 months. (p<0.05). |
| Campos et al. (2013) (n=13) [29] | 660 | 0.06W, 129J/cm², 60s | Optic fiber (d=600μm) | 10mg/ml | Single | aPDT group presented reduction in PD, CAL, and BOP after 6 months. |
| Noro Filho et al. (2012) (n=12) [31] |
660 | 0.03W, 0.428W/cm², 57.14J/cm², 133s | Optic fiber (a= 0.07 cm²) | 0.01% | Single | aPDT presented reduction in PD after 6 months, BOP after 3 and 6 months. There were no differences in microbiological parameters. |
| Giannelli et al. (2012) (n=26) [26] | 635 | 0.1W, 120s (60s inside + 60s outside) d= 0.6mm | Optic fiber (d=0.6mm) | 0.3% | 4 to 10 sessions | aPDT presented reduction in PD, CAL, BOP and spirochetes after 12 months. |
| Al-Zahrani et al. (2009) (n=45) [13] | 670 | 60s | NR | 0.01% | Single | There were no significant differences. |
They allied pre-diabetics; ** = In this article, averages were calculated from the ranges presented, therefore, they are estimated values; aPDT = antimicrobial photodynamic therapy; a= area; AMX = amoxicillin; CBL = Crestal bone loss; CLM = clarithromycin; d= diameter; DMT1 = Type 1 diabetes mellitus; UPD = ultrasonic periodontal debridement; S = Smokers; HbA1c = glycated hemoglobin index; PI = plaque index; GI = gingival index; m= months; MTZ = metronidazole; CAL= Clinical Attachment Level; nº = number; NRP = number residual pockets; NS= Non-smokers; NR = Not related; PD = Probing depth;; Aa.= Aggregatibacter Actinomicetemcomitans; Pg.= Porphyromonas gingivalis; Pi. = Prevotella intermedia; Pm = Parvimonas micra; Td = Treponema denticola; Tf = Tannerella forsythia; GR = gingival recession ;BOP = bleeding on probing; s = seconds; SRP= scaling and root planing.
Table 3.
Study evaluation time.
| Evaluation time (months) | Number of articles (n) | Reference |
| 0, 1, 3 e 6 | 3 | [9,11,24] |
| 0 e 3 | 4 | [13,18,23,29] |
| 0, 3 e 6 | 8 | [10,12,14,16,17,20,27,28] |
| 0, 1,5 3 e 6 | 2 | [19,31] |
| 0, 1 e 3 | 2 | [15,22] |
| 0, 1,5 e 3 | 1 | [30] |
| 0, 3 e 12 | 1 | [21] |
| 0 e 6 | 1 | [25] |
| 0 e 12 | 1 | [26] |
Table 4.
Randomness of the distribution of study groups.
| Randomization process | ||
| Method used | Number of articles (n) |
Reference |
| Coin toss | 3 | [15,22,30] |
| Computer-generated list | 8 | [13,14,20,25,27,28,29,31] |
| Computer-generated numbers | 1 | [9] |
| Random numbers | 1 | [24] |
| Online randomizer | 3 | [10,17] |
| Deck of cards | 1 | [18] |
| Lottery draw | 1 | [19] |
| Randomization chart | 1 | [16] |
| Computer software | 2 | [11,21] |
| Drawing lots from an opaque bag | 1 | [12] |
| Sealed opaque envelopes | 1 | [26] |
| Not reported | 1 | [23] |
Table 5.
Presentation of statistically significant differences according to each variable.
| Authors | Patient profile | PD | BOP (%) | CAL | PI (%) | GI | GR |
| Cunha et al. (2024) [9] | Periodontitis/Type 1 Diabetes Mellitus | SRP (p<0.05) |
NHE | NHE | NHE | - | - |
| Rodrigues et al. (2023) [18] | Periodontitis | aPDT (p=0.02 at 3 months |
- | NHE | - | - | NHE |
| Cláudio et al. (2021) [10] | Diabetes Mellitus | NHE | NHE | NHE | NHE | - | NHE |
| Derikvand et al. (2020) [19] | Periodontitis | aPDT (p<0.01) at 3 and 6 months | - | - | NHE | NHE | - |
| Alahmari et al. (2019) [15] | Smokers | NHE | NHE | NHE | SRP (p<0.01) at 1 month | - | - |
| Katsikanis et al. (2020) [16] | Moderate smoker | NHE | NHE | NHE | SRP (p=0.038) at baseline | - | - |
| Barbosa et al. (2018) [11] | Periodontitis / Diabetes Mellitus | NHE | aPDT (p=0.05) at 6 months | NHE | aPDT (p=0.02) only at 1-month follow-up | - | - |
| Andere et al. (2018) [20] | Periodontitis | aPDT (p<0.05) at 3 months | NHE | NHE | - | - | NHE |
| Theodoro et al. (2018) [17] | Smokers | NHE | NHE | NHE | - | - | - |
| Vohra et al. (2018) [30] | Obesity/Periodontitis | NHE | NHE | NHE | SRP (p<0.01) at 1.5 months and 3 months | - | - |
| Al-Askar et al. (2017) [12] | Pre-diabetes | NHE | NHE | - | NHE | - | - |
| Andrade et al. (2017) [21] | Periodontitis | NHE | NHE | NHE | NHE | - | - |
| Pulikkotil et al. (2016) [22] | Periodontitis | NHE | aPDT (p<0.01) at 3 months | NHE | NHE | - | - |
| Campanile et al. (2015) [27] | Residual pockets | aPDT (p=0.04) at 3 months | NHE | NHE | NHE | NHE | - |
| Kolbe et al. (2014) [28] | Residual pockets | NHE | NHE | NHE | - | - | - |
| Franco et al. (2014) [23] | Periodontitis | NHE | aPDT (p<0.05) | NHE | NHE | - | - |
| Betsy et al. (2014) [24] | Periodontitis | aPDT (p<0.05) at 3 and 6 months | aPDT (p<0.05) at 1 and 3 months | aPDT (p<0.05) at 3 and 6 months | aPDT (p<0.05) at 2 weeks | aPDT (p<0.05) at 1 and 3 months | NHE |
| Luchesi et al. (2013) [14] | Furcation Class III | NHE | NHE | NHE | NHE | - | - |
| Dilsiz et al. (2013) [25] | Periodontitis | aPDT (p<0.05) at 6 months | NHE | aPDT (p<0.05) at 6 months | NHE | NHE | - |
| Campos et al. (2013) [29] | Residual pockets | aPDT (p<0.05) at 3 months | aPDT (p<0.05) at 3 months | aPDT (p<0.05) at 3 months | - | - | - |
| Noro Filho et al. (2012) [31] | HIV | aPDT (p<0.05) at 6 months | aPDT (p<0.05) at 3 and 6 months | NHE | NHE | - | NHE |
| Giannelli et al. (2012) [26] | Periodontitis | aPDT (p<0.001) at 12 months | aPDT (p<0.001) at 12 months | aPDT (p<0.001) at 12 months | |||
| Al-Zahrani et al. (2009) [13] | Diabetes Mellitus | NHE | NHE | NHE | NHE | - | - |
- = not reported by the study; PD = Probing depth; BOP = bleeding on probing; CAL = Clinical Attachment Level; PI = plaque index; GI = gingival index; GR = gingival recession; aPDT = SRP + antimicrobial photodynamic therapy group; SRP = Group that received only scaling and root planning; NHE = No statistically significant difference was found between the groups; m = months; P<0.05 = Statistically significant difference between the groups.
Table 6.
Presentation of scientific evidence from systematic reviews.
| Authors and year | Selected articles and study participants (n) | Conclusion |
| Jervøe-Storm et al. (2024) [32] | 50 selected articles (n=1407) | The available evidence is quite limited, making it difficult to draw definitive conclusions about the superior clinical benefits of aPDT as an adjunctive therapy in the active treatment or maintenance of periodontitis. Furthermore, the data suggest that the observed improvements may be too small to hold clinical relevance. To enhance the reliability of these findings, it is essential to conduct large, well-designed, and rigorously evaluated randomized controlled trials (RCTs), taking into account the variability of outcomes over time. |
| Salvi et al. (2020) [4] | 17 selected articles (n=370) | The available evidence on adjunctive therapy with lasers and aPDT is limited to a small number of controlled studies, with notable variability in study designs. |
| Vohra et al. (2016) [33] | 7 selected articles (n=218) |
In the use of aPDT for the treatment of aggressive periodontitis, the authors concluded that this therapeutic approach may be effective as an adjunct to SRP. However, further randomized clinical trials are needed to confirm these findings. |
| Javed et al. (2013) [34] | 6 selected articles (n= 615 and 270*) | aPDT was analyzed as an adjunct to non-surgical periodontal therapy in immunocompromised patients. After review, only six articles were found, of which only one was a randomized clinical trial; the others were laboratory studies conducted in rats. Various factors, such as smoking and poor oral hygiene, may interfere with the outcomes, making it difficult to assess the effectiveness of this therapy. In conclusion, further studies are needed. |
| Sgolastra et al. (2013) [35] | 7 selected articles (n=261) |
After evaluating seven articles, the clinical outcomes were found to be modest, indicating a lack of scientific evidence and the need for further studies to assess the efficacy of aPDT as an adjunct to SRP. |
| Sgolastra et al. (2013) [36] | 14 selected articles (n=389) |
A more rigorous systematic review was recently published, including 14 studies, but without promising results. aPDT may have short-term effects, as the evidence does not indicate significant differences after six months. Therefore, the authors recommend conducting additional clinical trials with long-term follow-up. |
| Atieh, 2010 [37] | 4 selected articles (n= 161) |
The analysis included only four articles, with a post-therapy follow-up of three weeks. The results showed a clinical gain of 0.29 mm in attachment level and a reduction of 0.11 mm in probing depth. The authors concluded that the use of aPDT may be beneficial, but they cautioned about the limitation of the small number of studies included. |
| Azarpazhooh et al. (2010) [38] |
5 selected articles (n=74 and 62**) |
The review included five studies, three of which were similar to Atieh, 2010, without distinguishing the types of periodontitis between them, considering studies with follow-up at 3 and 6 months. The results showed a minimal gain in clinical attachment (0.34 mm) and a reduction in probing depth (0.25 mm). The authors concluded that aPDT was not shown to be more effective. |
*= animal studies; ** = sites.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



