
Submitted:
02 November 2025
Posted:
04 November 2025
You are already at the latest version
Abstract
Pain catastrophizing (PC) and hopelessness are increasingly recognized as central de-terminants of pain severity, disability, and treatment response in individuals with rheumatic and immune-mediated diseases. Traditionally conceptualized as secondary emotional reactions to pain, these cognitive-affective constructs instead represent active mechanisms that shape symptom perception, behavioral responses, and long-term outcomes. In this review, we synthesize evidence across neurobiological, psychological, and clinical domains to elucidate the pathways linking PC and hopelessness to mala-daptive coping, kinesiophobia, and functional decline. Early life stress, trauma, and maladaptive cognitive schemas emerge as upstream vulnerability factors that prime heightened emotional reactivity and reduced prefrontal regulatory control, facilitating amplified pain signaling and fear-based avoidance behaviors. Avoidance and inactivity foster physical deconditioning, fatigue, and higher perceived disability, creating a self-reinforcing cycle that sustains distress and poor quality of life. Moreover, inactivi-ty-related metabolic dysfunction and weight gain may contribute to low-grade in-flammation, particularly in conditions such as psoriatic arthritis, thereby intersecting with biological disease pathways. Importantly, these psychological processes identify a distinct patient subgroup for whom further escalation of immunosuppressive therapy provides limited benefit. Instead, integrated psychological approaches - including cog-nitive-behavioral therapy, acceptance and commitment therapy, and coping-skills training - demonstrate meaningful effects on catastrophizing, agency, and functional recovery. We emphasize the need for routine screening to detect patients with mala-daptive cognitive-emotional profiles and propose a stratified care model prioritizing targeted psychological interventions alongside standard rheumatologic therapy. Future research should refine phenotyping strategies, clarify neuroimmune links, and develop scalable intervention models to break the avoidance cycle and improve patient-centered outcomes.
Keywords:
pain catastrophizing
; hopelessness
; autoimmunity
; quality of life
; cognitive-behavioral-treatment
; pain
; fibromyalgia
; psychotherapy
1. Introduction
The experience of pain in rheumatic disease is not simply a matter of peripheral inflammation or joint damage. Central neural systems, cognitive-emotional processes and behavioral responses all interact to shape individual variance in pain intensity, physical disability and thus treatment outcomes [1,2,3]. Within this context, pain catastrophizing (PC) and hopelessness have consistently emerged as key determinants of pain experience and patient outcomes in these conditions.
PC in rheumatic disease has been defined as a persistent tendency to magnify the threat of pain, ruminate on pain sensations, and feel helpless in the fact of pain [4]. In its entirety, it is not simply a reaction to severe pain but it is independently associated with higher pain intensity, disability, poorer physical function and reduced treatment response, even when inflammatory markers are controlled for [5,6]. Closely linked to catastrophizing is the psychological construct of hopelessness, which reflects a broader sense of negative future expectancy, and the belief that improvement or control over pain is unlikely.
Crucially, both constructs are modifiable. Psychological interventions that are tailored to rheumatic disease, such as pain coping skills training, Cognitive Behavioral Therapy, Acceptance and Commitment Therapy, and Behavioral Activation, have been shown to reduce catastrophizing and improve patient outcomes by restoring a sense of agency and adaptive engagement [12,13]. These therapies likely work in part by strengthening prefrontal regulation networks, thus restoring positive expectancy pathways. This will then counteract the neurobiological patterns associated with pain distress.
2. Neurobiological Connection Between Pain Catastrophizing and Hopelessness
Neurobiologically, PC has been linked to heightened responsivity in the salience network, particularly the insula and anterior cingulate cortex (ACC), which function to assign emotional significance to sensory input [7]. Increased activation in these regions reflects greater pain-related threat appraisal, and sustained hypervigilance. Alongside, catastrophizing is associated with reduced engagement of prefrontal regulatory regions, including the dorsolateral and ventromedial prefrontal cortex (PFC) which ordinarily dampen emotional distress and support cognitive reappraisal (Figure 1) [8]. This pattern of strong emotional amplification with weakened cognitive regulation offers a biological pathway explaining why patients with rheumatic disease may report severe pain even during periods of minimal inflammatory activity.
On the other hand, hopelessness has been associated with reduced activity in reward and motivational circuits, including the subgenual ACC, ventromedial PFC, and ventral striatum, which are central to the generation of positive expectancy and goal directed engagement (Figure 1) [9,10]. When these circuits are underactive, patients may struggle to maintain motivation or belief in the possibility of improvement. This reinforces withdrawal, inactivity and reduced coping, all of which are patterns frequently observed in chronic rheumatic disease [1].
It is likely that PC and hopelessness interact in a dynamic cycle. Heightened distress and perceived lack of control in the fact of pain catastrophizing can, over time, lead to loss of hope when the pain then persists despite treatment efforts. In turn, hopelessness reduces motivation to engage in adaptive strategies, which may worsen pain, increase disability, and reinforce catastrophizing. Currado et al., demonstrated this interaction in Psoriatic Arthritis (PsA) and Axial Spondylarthritis (axSpA), showing that higher catastrophizing was associated with higher disease activity and disability, alongside lower levels of psychological flexibility and hope [5].
This cycle has direct implications for clinical outcomes. Patients with high levels of catastrophizing and hopelessness tend to report greater pain and fatigue even during controlled inflammation [4,6], experience reduced function and quality of life [5], respond less effectively to pharmacological therapy alone [1], require a higher use of painkiller medications [11], and may benefit from integrated psychosocial-medical management approaches [12].
3. Pain Catastrophizing in Rheumatic Diseases
Osteoarthritis
PC plays a central role in osteoarthritis (OA), influencing pain intensity, physical function, and postoperative recovery. In patients with hip OA, those presenting higher levels of catastrophizing consistently report worse symptoms and poorer quality of life (QoL), even when controlling for structural severity or objective clinical metrics. In a multicentre study of 160 hip OA patients, higher PC scores independently predicted lower physical (β=-0.28, p<0.05) and mental (β=-0.29, p<0.05) QoL indices after adjusting for pain intensity, BMI, and range of motion, underscoring the independent contribution of cognitive-affective processes to disability in OA [13]. Similarly, preoperative catastrophizing has been associated with inferior postoperative outcomes in hip OA: patients with elevated PCS prior to total hip arthroplasty reported greater pain and functional limitations at twelve months independent of baseline characteristics, suggesting that catastrophizing not only reflects distress but can modulate recovery trajectories, probably through facilitating movement-avoidant behaviors [14,15,16,17].
In a study assessing fear-avoidance and PC in hip OA, both constructs showed significant associations with reduced QoL and functional limitation, reinforcing their intertwined role in pain-related outcomes [14]. In this sense, catastrophizing and kinesiophobia frequently co-occur, suggesting shared mechanisms such as hypervigilance toward movement-related pain, anticipatory threat appraisal, and reduced willingness to engage in physical activity, behaviors that may accelerate deconditioning and disability. Evidence in knee OA mirrors hip OA findings. A prospective study demonstrated that higher preoperative PCS scores predicted worse pain and poorer function following total knee arthroplasty, with PC emerging as a stronger determinant of outcomes than radiographic severity [18]. In this patient population, cognitive-emotional burden mediated through PC appears to interact with central pain mechanisms. In another investigation, applying transcranial direct current stimulation as a neuro-modulatory approach in 68 knee OA patients, a greater number of stimulation sessions correlated with reduced pain (r=−0.42, p=0.002) and improved function (r=0.39, p=0.004), and PC mediated these associations, highlighting the mechanistic interplay between cortical modulation and catastrophizing tendencies [19]. Functional performance data further emphasize the behavioral impact of catastrophizing. High-catastrophizing knee OA patients demonstrate slower gait speed and poorer chair-rise performance, indicating that catastrophizing contributes to measurable physical impairment beyond subjective pain reports [18]. Beyond the lower limb, even in hand OA patients PC is markedly elevated versus controls (mean difference ~10.8 points on PCS) [20], and catastrophizing has been shown to impair post-operative outcomes even in shoulder OA patients [17].
Notably, PC is clinically relevant even in patients with modest disease burden. A cross-sectional study of both autoimmune and mechanic musculoskeletal diseases found that higher PC scores were associated with failure to achieve low disease activity even in lower inflammatory states [21]. Taken together, evidence across OA consistently shows that catastrophizing contributes to heightened pain perception, functional impairment, diminished QoL, and poorer surgical recovery.
Inflammatory arthritis
In spondyloarthritis (SpA), PC is increasingly recognized as a key contributor to pain burden, treatment outcomes, and perceived disease activity. In a recent Italian prospective multicenter cohort including PsA and axSpA patients, higher baseline PC predicted treatment discontinuation over two years [22]. The effect was consistent across univariate analyses, where each unit increase in the PC scores helplessness or rumination subscales was associated with a higher risk of drug withdrawal. Importantly the helplessness domain of PC scores showed the strongest signal. Although multivariable confirmation for axSpA was limited by low event numbers, these findings suggest that cognitive-affective dysregulation contributes to poorer treatment persistence, likely via reduced perceived benefit and lower adherence.
Additional evidence comes from a large real-world cohort across multiple autoimmune diseases (n=1,229), where PC showed a disease-specific impact in axSpA (n=255). Specifically a higher PCS significantly reduced the likelihood of achieving low disease activity (OR 0.33, 95% CI 0.12-0.88) [23]. These results underscore a particular vulnerability of axial disease to cognitive amplification of pain and support the concept of a “residual pain” phenotype where symptoms persist despite adequate inflammatory control. Neurophysiological data further delineate this phenotype [23]. In a Quantitative Sensory Testing-based profiling study, patients with PsA demonstrated lower pressure pain thresholds and greater temporal summation compared with healthy controls, along with significantly higher catastrophizing scores amplifying PC and sensory hypersensitivity metrics. These findings reinforce that PC is closely intertwined with central pain sensitization rather than simply responding to nociceptive drive from inflammation [20]. Younger SpA cohorts show aligned trends wherein associations between PC, higher BASDAI scores, and kinesiophobia frequently fall in the low-to-moderate range (r≈0.25-0.40), indicating that catastrophizing co-evolves with movement-related fear and avoidance early in the disease course [24]. These interactions may partially explain why younger patients with limited structural damage can still report substantial disability and pain.
Beyond SpA, PC represents a key modulator of pain severity, emotional distress, and physical functioning also for rheumatoid arthritis (RA), where it often exceeds the explanatory power of inflammatory markers alone. In a cohort of 220 RA patients, 61.8% reported high levels of PC, which showed strong inverse associations with both cognitive flexibility (β=−0.34, p<0.001) and self-efficacy (β=-0.53, p<0.001), together accounting for 51% of the variance in catastrophizing [25].These data underscore the importance of cognitive-affective mechanisms in shaping pain experience and coping capacity in RA. Catastrophizing has been consistently linked to greater pain intensity, increased disease impact, and heightened psychological burden, independent of disease activity [1,26]. Importantly, PC in inflammatory arthritis is closely tied to fear-avoidance behaviors, where fear of movement and anticipation of pain drive avoidance of physical activity [27,28].
Connective tissue diseases
In connective tissue diseases (CTDs), PC plays a central role in modulating pain perception, disability, and emotional burden, frequently exceeding the influence of humoral disease activity biomarkers. In systemic sclerosis (SSc), PC and hopelessness are highly prevalent and clinically meaningful. In one cohort of SSc patients, high catastrophizing was significantly associated with worse physical functioning, higher fatigue, and greater emotional distress, independent of disease severity scores [29]. Furthermore, hopelessness was present in over 40% of patients and strongly correlated with higher pain ratings and disability indices, suggesting that maladaptive cognitive patterns contribute substantially to perceived disease burden and to amplified pain processing pathways [30]. These findings support a cognitive-affective amplification model layered onto microvascular and neuropathic pain mechanisms typical of SSc.
In systemic lupus erythematosus (SLE), catastrophizing is a key determinant of pain and fatigue, despite weak or absent correlations between disease activity and patient-reported pain severity. In a study including SLE patients, high PC scores were associated with greater pain, stiffness, lower positive mood, and significantly worse QoL, while disease activity did not correlate with psychological distress or pain intensity [31]. Importantly, in a study of 104 women with SLE, kinesiophobia, depression, body awareness, and BMI explained 52% of the variance in PC scores, highlighting the central role of psychological and perceptual factors over biological ones [32]. Moreover, 63.2% of SLE patients exhibited clinically significant kinesiophobia, which was directly associated with fatigue, poor function, and reduced quality of life, despite minimal association with inflammatory markers or physician global scores [33]. This underscores a predominant fear-avoidance behavioral phenotype, reinforcing physical inactivity and perpetuating central sensitization and disability.
In primary Sjögren’s syndrome (pSS), PC emerges as one of the strongest predictors of pain outcomes. In a cohort of 92 pSS patients, catastrophizing, along with fibromyalgia comorbidity and negative illness beliefs, explained 55% of the variance in pain severity [34]. Compared to depression and anxiety measures, catastrophizing was a stronger predictor of pain intensity, suggesting that cognitive-emotional mechanisms may outweigh affective symptoms in driving pain amplification in pSS. These findings align with the high prevalence of neuropathic-like pain, fatigue, and centralized pain features observed in the disease [35].
Fibromyalgia
Fibromyalgia (FM), the most comorbid condition in all autoimmune rheumatic diseases, represents a prototypical condition in which PC plays a central pathophysiological and clinical role. Across FM cohorts, catastrophizing consistently correlates with higher pain intensity, emotional distress, disability, and poorer treatment response. Evidence supports a bidirectional model in which catastrophizing not only amplifies nociceptive input and central sensitization, but is also reinforced by persistent pain and hypervigilance. A growing body of work highlights catastrophizing as a key mediator between psychological and clinical variables in FM. In a study of 105 FM patients, PC significantly mediated the relationship between pain self-efficacy and disease severity, indicating that catastrophizing independently predicted symptom burden and accounted for part of the effect of low self-efficacy on FM severity [36].
Cognitive-affective processes further contribute to disability in FM through repetitive negative thinking and rumination. In a cohort of 82 FM patients, the link between pain and anxious-depressive symptoms was doubly mediated by catastrophizing and RNT, suggesting a serial model where maladaptive cognitive loops exacerbate both emotional burden and pain experience [37]. These findings position catastrophizing as part of a broader emotion-regulation deficit in FM. Treatment response data underline the clinical implications of catastrophizing also in FM beyond autoimmunity. A randomized controlled trial assessing dry needling in 96 women with FM reported significant improvements in pressure pain thresholds; however, individuals with moderate baseline PC exhibited diminished immediate post-intervention benefit [38]. This highlights catastrophizing as a moderator of therapy efficacy, reinforcing the need for integrated multimodal approaches. Finally, catastrophizing has been linked to suicidality in FM. In an observational study, higher catastrophizing scores were associated with elevated suicidal ideation, independent of depressive symptoms, underscoring its role as a critical psychological risk marker in FM [39].
4. Hopelessness in Rheumatic Diseases
While research in rheumatic disease remains limited, findings from broader chronic pain population suggest that hopeless exerts a significant influence on long-term pain outcomes and psychological adjustment. For instance, Serafini et al., demonstrated that individuals with chronic pain who reported higher levels of hopelessness experienced greater emotional distress, poorer functional outcomes, and reduced quality of life compared to those without hopelessness [40]. These patterns likely extend to rheumatic disease, where sustained pain and functional limitation can foster pessimistic expectations about recovery. Patients experiencing hopelessness are therefore more likely to disengage from self-management, physical activity or rehabilitation - behaviors that are known to alleviate pain and disability when maintained.
5. Psychological and Developmental Origins
PC does not arise in isolation; rather, it reflects an interaction between early environmental exposures, emotional learning, and cognitive-emotional vulnerability traits. A substantial body of evidence implicates adverse childhood experiences (ACEs), particularly emotional and physical abuse, as key precursors to catastrophizing tendencies later in life. In a chronic pain cohort, childhood trauma - particularly emotional abuse- significantly predicted higher PC even after adjusting for depression and anxiety, whereas trauma exposure in adulthood did not exert the same effect [41]. These findings suggest that a sensitive developmental windows exist during which adverse social environments may shape maladaptive cognitive schemas about threat, control, and vulnerability.
Similarly, childhood trauma and abuse have been repeatedly linked to exaggerated threat perception, heightened emotional reactivity, and impaired stress-regulation circuits, including dysregulation of the Hypothalamic-Pituitary-Adrenal axis and limbic responsivity. These alterations may foster hypervigilance to bodily sensations, persistent anticipatory anxiety about pain, and a reduced sense of coping capacity, providing a neurobiological substrate for catastrophizing to emerge as a default cognitive style.
In FM populations specifically, childhood abuse is highly prevalent and has been associated with greater bodily distress, worse physical functioning, and elevated catastrophizing [42]. While some samples did not find a direct correlation between childhood abuse and pain severity, PC moderated the relationship between early trauma and clinical burden - suggesting that catastrophizing acts as a cognitive amplifier through which early adversity translates into adult pain vulnerability [41]. In other words, individuals exposed to early life stress who also develop maladaptive pain cognitions exhibit worse pain interference and functional impairment than those without such cognitions.
More surprisingly, even across immune-mediated conditions exposure to maltreatment and psychological trauma has been shown to predispose individuals to increased PC, greater emotional dysregulation, and poorer coping resources, reinforcing the notion that catastrophizing represents a learned cognitive and affective response rooted in early adversity and reinforced by subsequent pain experiences [43]. This framework positions PC not simply as a mood-related epiphenomenon, but as a developmentally acquired vulnerability embedded in stress neurobiology and emotional learning systems.
Altogether, these findings underscore that PC often reflects developmentally ingrained cognitive heuristics shaped by trauma, threat exposure, and early stress environments. Recognizing these origins highlights the importance of trauma-informed approaches and targeted interventions (e.g., cognitive restructuring, resilience-building, mindfulness-based strategies) aimed at interrupting maladaptive appraisal cycles and restoring a sense of agency in patients with chronic pain..
6. Clinical Implications and Future Directions
The evidence reviewed indicates that PC and hopelessness are not epiphenomena of disease burden but mechanistic drivers of pain amplification, disability, and suboptimal treatment response in rheumatic diseases [26,41]. Clinically, this supports a paradigm shift away from viewing persistent pain solely through an inflammatory lens, toward recognizing cognitive-affective and behavioral processes as central therapeutic targets.
One key mechanism linking these psychological traits to disability is the fear-avoidance cycle, in which catastrophizing and kinesiophobia fuel movement avoidance, leading to reduced physical activity, progressive deconditioning, and greater disability [27,42]. Over time, physical inactivity can promote weight gain and metabolic dysfunction, particularly relevant in arthritis and other immune-mediated diseases, where excess adiposity contributes to low-grade inflammation and worsened disease control [43,44,45,46,47]. This creates a self-perpetuating cycle of pain sensitization, disability, emotional distress, and heightened inflammatory burden. Breaking this cycle requires timely recognition and targeted intervention (Figure 2).
From a treatment standpoint, it becomes critical to identify patients in whom psychological drivers outweigh inflammatory activity. In these individuals, escalation of immunosuppressive therapy may offer limited benefit and can expose patients to unnecessary risk and healthcare burden. Conversely, appropriately delivered psychological and behavioral interventions - including cognitive-behavioral therapy, pain-coping skills training, acceptance and commitment therapy, motivational interviewing, and behavioral activation - may yield the greatest therapeutic return. These approaches can reduce PC, restore a sense of agency, and support gradual re-engagement in valued physical and social activities (Figure 2) [38,48,49,50]. Integration with exercise-based rehabilitation, graded activity programs, and structured physical therapy may further enhance outcomes by addressing both cognitive-emotional and motor-behavioral components of pain maintenance [51].
Future care models should therefore incorporate systematic screening for catastrophizing, hopelessness, and fear-avoidance profiles early in the disease course, ideally embedded within routine rheumatology pathways. Stratified approaches will allow clinicians to allocate patients to precision psychosocial interventions when these are most needed, rather than reflexively escalating pharmacotherapy. Emerging digital therapeutics, remote behavioral coaching, and blended care models (combining brief clinician-guided sessions with app-based support) may facilitate scalable delivery of these interventions across diverse healthcare systems.
Further research is needed to refine these stratification strategies, define the neurobiological substrates linking cognitive-affective traits and inflammation, and evaluate combined immunomodulatory-psychological pathways as synergistic, rather than competing, treatment modalities. Ultimately, recognizing and treating the psychological architecture of pain alongside immunological drivers represents a key frontier in improving outcomes for patients with rheumatic disease.
The sensory-discriminative component of pain (blue pathway) is transmitted via the ventral posterolateral and ventral posteromedial thalamic nuclei to the primary and secondary somatosensory cortices, supporting localization and intensity processing.
The affective-motivational component of pain (red pathway) is mediated by the mediodorsal thalamic nucleus, which projects to medial prefrontal and cingulate cortices, integrating pain with emotional evaluation, meaning, and behavioral relevance.
The salience and arousal system (green pathway) involves the paraventricular and intralaminar thalamic nuclei, including the centromedian-parafascicular complex, projecting to the anterior cingulate cortex, striatum, and insular cortex. This network modulates vigilance, autonomic reactivity, and detection of behaviorally relevant nociceptive signals.
Together, these thalamo-cortical circuits account for the sensory, emotional, and salience-driven dimensions of pain experience. Dysregulation of affective-motivational and salience pathways contributes to heightened threat appraisal, hypervigilance, and pain persistence typical of chronic rheumatic disease.
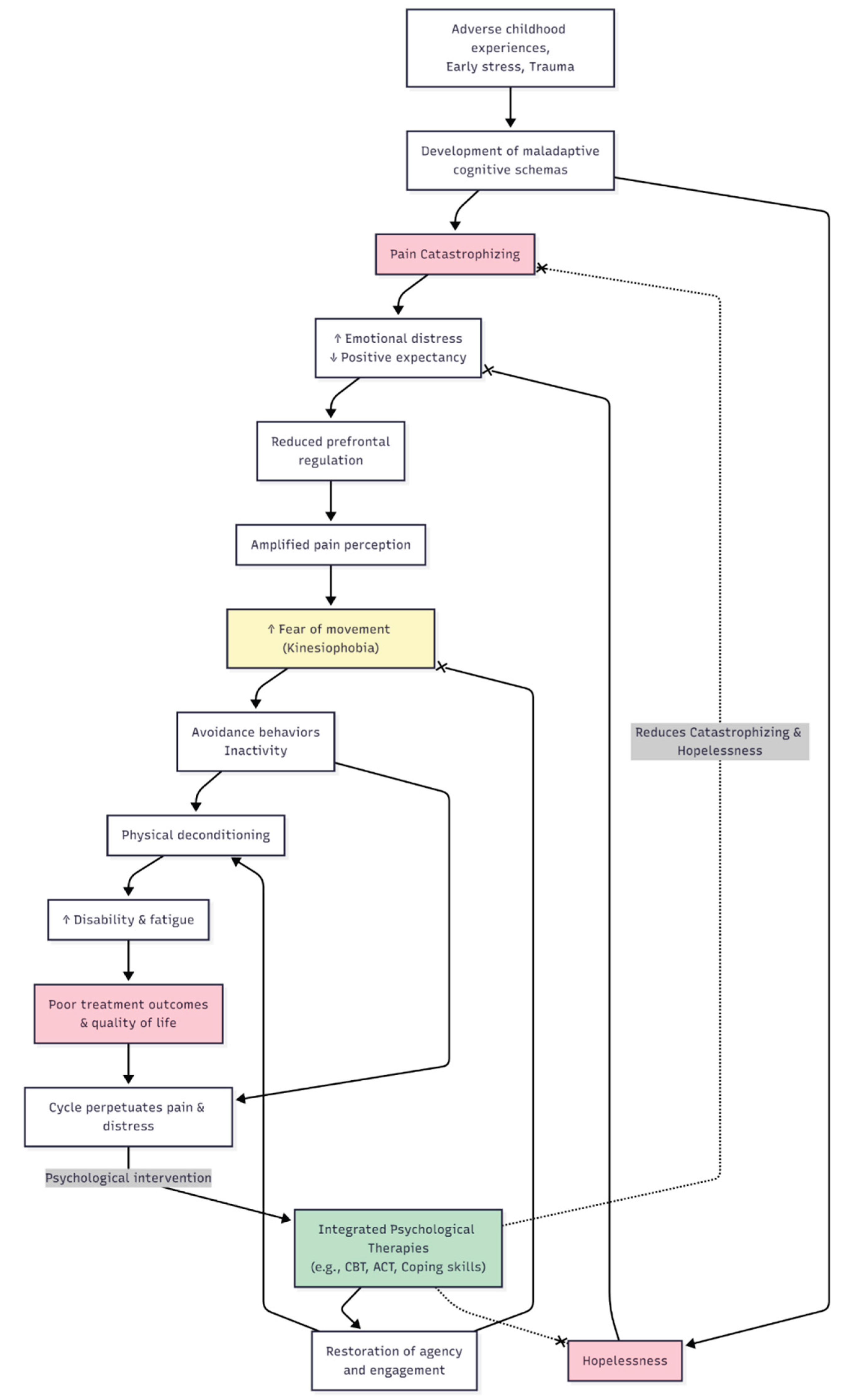
Conceptual model illustrating the developmental and behavioral pathways linking early-life stress to pain catastrophizing, hopelessness, and disability in rheumatic disease. Early adverse experiences foster maladaptive cognitive schemas, predisposing to pain catastrophizing, heightened emotional distress, and impaired prefrontal regulatory control. This amplifies pain perception and increases kinesiophobia, leading to avoidance behaviors, physical inactivity, and deconditioning, ultimately worsening disability and quality of life in a self-reinforcing cycle. Integrated psychological therapies disrupt this cycle by restoring agency and reducing catastrophizing and hopelessness.
Arrow notation: pointed arrow indicates promotion/causal progression; x-ended arrow indicates reduction/inhibition.
Author Contributions
Conceptualization SDD and EOC; methodology, SDD and EOC; writing—original draft preparation, EOC and AM; writing—review and editing, SDD and AM; visualization, SDD and EOC. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACC ACT ACR axSpA BMI CBT FM HPA OA PC PFC PsA QoL RA SLE |
Anterior Cingulate Cortex Acceptance and Commitment Therapy American College of Rheumatology Axial Spondyloarthritis Body Mass Index Cognitive Behavioural Therapy Fibromyalgia Hypothalamic–Pituitary–Adrenal (axis) Osteoarthritis Pain Catastrophizing Prefrontal Cortex Psoriatic Arthritis Quality of Life Rheumatoid Arthritis Systemic Lupus Erythematosus |
References
- Edwards RR, Calahan C, Mensing G, et al. Pain, catastrophizing, and depression in the rheumatic diseases. Nat Rev Rheumatol. 2011;7:216–24. [CrossRef]
- Edwards RR, Bingham CO, Bathon J, et al. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Rheum. 2006;55:325–32. [CrossRef]
- Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing a critical review. Expert Rev Neurother. 2009;9:745–58.
- Cohen EM, Edwards RR, Bingham CO, et al. Pain and Catastrophizing in Patients With Rheumatoid Arthritis: An Observational Cohort Study. J Clin Rheumatol. 2019;25:232–6. [CrossRef]
- Currado D, Biaggi A, Pilato A, et al. The negative impact of pain catastrophising on disease activity: analyses of data derived from patient-reported outcomes in psoriatic arthritis and axial spondyloarthritis. Clin Exp Rheumatol. 2023;41:1856–61. [CrossRef]
- Wilk M, Zimba O, Haugeberg G, et al. Pain catastrophizing in rheumatic diseases: prevalence, origin, and implications. Rheumatol Int. 2024;44:985–1002. [CrossRef]
- Galambos A, Szabó E, Nagy Z, et al. A systematic review of structural and functional MRI studies on pain catastrophizing. J Pain Res. 2019;12:1155–78. [CrossRef]
- Büchel, C. The role of expectations, control and reward in the development of pain persistence based on a unified model. Elife. 2023;12. [CrossRef]
- Wang Y, Wang C, Zhou J, et al. Contribution of resting-state functional connectivity of the subgenual anterior cingulate to prediction of antidepressant efficacy in patients with major depressive disorder. Translational Psychiatry 2024 14:1. 2024;14:1–8. [CrossRef]
- Höflich A, Michenthaler P, Kasper S, et al. Circuit Mechanisms of Reward, Anhedonia, and Depression. Int J Neuropsychopharmacol. 2019;22:105–18. [CrossRef]
- Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, et al. Pain Catastrophizing, Opioid Misuse, Opioid Use, and Opioid Dose in People With Chronic Musculoskeletal Pain: A Systematic Review. Journal of Pain. 2021;22:879–91. [CrossRef]
- Nagy Z, Szigedi E, Takács S, et al. The Effectiveness of Psychological Interventions for Rheumatoid Arthritis (RA): A Systematic Review and Meta-Analysis. Life (Basel). 2023;13. [CrossRef]
- Hayashi K, Morishima T, Ikemoto T, et al. Pain Catastrophizing Is Independently Associated with Quality of Life in Patients with Severe Hip Osteoarthritis. Pain Medicine (United States). 2019;20:2220–7. [CrossRef]
- Hidaka R, Tanaka T, Hashikura K, et al. Association of high kinesiophobia and pain catastrophizing with quality of life in severe hip osteoarthritis: a cross-sectional study. BMC Musculoskelet Disord. 2023;24. [CrossRef]
- Reine S, Xi Y, Archer H, et al. Effects of Depression, Anxiety, and Pain Catastrophizing on Total Hip Arthroplasty Patient Activity Level. Journal of Arthroplasty. 2023;38:1110–4. [CrossRef]
- Wood TJ, Gazendam AM, Kabali CB, et al. Postoperative Outcomes Following Total Hip and Knee Arthroplasty in Patients with Pain Catastrophizing, Anxiety, or Depression. Journal of Arthroplasty. 2021;36:1908–14. [CrossRef]
- Hardy A, Sandiford MH, Menigaux C, et al. Pain catastrophizing and pre-operative psychological state are predictive of chronic pain after joint arthroplasty of the hip, knee or shoulder: results of a prospective, comparative study at one year follow-up. Int Orthop. 2022;46:2461–9. [CrossRef]
- Matsuo H, Kubota M, Naruse H, et al. Association of knee joint performance and gait patterns with pain catastrophizing in patients with severe knee osteoarthritis: a cross-sectional study. BMC Musculoskelet Disord. 2025;26. [CrossRef]
- Reddy RS, Tedla JS, Alshehri SHS, et al. Associations between transcranial direct current stimulation session exposure and clinical outcomes in knee osteoarthritis: a cross-sectional analysis exploring the role of pain catastrophizing. J Orthop Surg Res. 2025;20. [CrossRef]
- Vela J, Dreyer L, Petersen KK, et al. Quantitative sensory testing, psychological profiles and clinical pain in patients with psoriatic arthritis and hand osteoarthritis experiencing pain of at least moderate intensity. Eur J Pain. 2024;28:310–21. [CrossRef]
- Wilk M, Pripp AH, Korkosz M, et al. Exploring pain catastrophizing and its associations with low disease activity in rheumatic inflammatory disorders. Rheumatol Int. 2023;43:687–94. [CrossRef]
- Currado D, Saracino F, Ruscitti P, et al. Pain catastrophizing negatively impacts drug retention rate in patients with Psoriatic Arthritis and axial Spondyloarthritis: results from a 2-years perspective multicenter GIRRCS (Gruppo Italiano di Ricerca in Reumatologia Clinica) study. Arthritis Res Ther. 2024;26. [CrossRef]
- Wilk M, Łosińska K, Pripp AH, et al. Pain catastrophizing in rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis: biopsychosocial perspective and impact on health-related quality of life. Rheumatol Int. 2022;42:669–82. [CrossRef]
- Tekaya A Ben, Said H Ben, Yousfi I, et al. Burden of disease, pain catastrophizing, and central sensitization in relation to work-related issues in young spondyloarthritis patients. Reumatologia. 2024;62:35–42. [CrossRef]
- Gazik AB, Vagharseyyedin SA, Saremi Z, et al. Severity of Pain Catastrophizing and Its Associations With Cognitive Flexibility and Self-Efficacy in Patients With Rheumatoid Arthritis. Musculoskeletal Care. 2024;22:e1923. [CrossRef]
- Alcon C, Bergman E, Humphrey J, et al. The Relationship between Pain Catastrophizing and Cognitive Function in Chronic Musculoskeletal Pain: A Scoping Review. Pain Res Manag. 2023;2023. [CrossRef]
- Karaca NB, Arin-Bal G, Sezer S, et al. Physical Activity, Kinesiophobia, Pain Catastrophizing, Body Awareness, Depression and Disease Activity in Patients With Ankylosing Spondylitis and Rheumatoid Arthritis: A Cross-Sectional Explorative Study. Musculoskeletal Care. 2024;22. [CrossRef]
- Lööf H, Demmelmaier I, Henriksson EW, et al. Fear-avoidance beliefs about physical activity in adults with rheumatoid arthritis. Scand J Rheumatol. 2015;44:93–9. [CrossRef]
- Edwards RR, Goble L, Kwan A, et al. Catastrophizing, pain, and social adjustment in scleroderma: Relationships with educational level. Clinical Journal of Pain. 2006;22:639–46. [CrossRef]
- Bearzi P, Navarini L, Mattioli LC, et al. Hopelessness is associated to severity of both digital vasculopathy and lung disease in systemic sclerosis patients: a prospective one-year study. Clin Exp Rheumatol. 2025;43:1508–15. [CrossRef]
- Yildirim, N. Comparison of kinesiophobia in patients with rheumatoid arthritis and systemic lupus erythematosus. Eur Rev Med Pharmacol Sci. 2023;27:11508–16. [CrossRef]
- Kinikli GI, Bal GA, Aydemir-Guloksuz EG, et al. Predictors of pain catastrophizing in women with systemic lupus erythematosus. Rev Assoc Med Bras (1992). 2022;68:1247–51. [CrossRef]
- Bağlan Yentür S, Karatay S, Oskay D, et al. Kinesiophobia and related factors in systemic lupus erythematosus patients. Turk J Med Sci. 2019;49:1324–31. [CrossRef]
- Segal BM, Pogatchnik B, Rhodus N, et al. Pain in primary Sjögren’s syndrome: The role of catastrophizing and negative illness perceptions. Scand J Rheumatol. 2014;43:234–41. [CrossRef]
- Gebreegziabher EA, Bunya VY, Baer AN, et al. Neuropathic Pain in the Eyes, Body, and Mouth: Insights from the Sjögren’s International Collaborative Clinical Alliance. Pain Pract. 2021;21:630–7. [CrossRef]
- Apriliyasari RW, Chou CW, Tsai PS. Pain Catastrophizing as a Mediator Between Pain Self-Efficacy and Disease Severity in Patients with Fibromyalgia. Pain Management Nursing. 2023;24:622–6. [CrossRef]
- Fonseca Das Neves J, Serra E, Kosinski T, et al. Catastrophizing and rumination mediate the link between functional disabilities and anxiety/depression in fibromyalgia. A double-mediation model. Encephale. 2024;50:162–9. [CrossRef]
- Vicente-Mampel J, Bautista IJ, Salvat I, et al. Dry needling in people with fibromyalgia: A randomized controlled trial of its effects on pain sensitivity and pain catastrophizing influence. PM&R. 2025;17:419–30. [CrossRef]
- Varallo G, Scarpina F, Arnison T, et al. Suicidal ideation in female individuals with fibromyalgia and comorbid obesity: prevalence and association with clinical, pain-related, and psychological factors. Pain Medicine. 2024;25:239–47. [CrossRef]
- Serafini G, Lamis DA, Aguglia A, et al. Hopelessness and its correlates with clinical outcomes in an outpatient setting. J Affect Disord. 2020;263:472–9. [CrossRef]
- Sipilä R, Kalso E, Kemp H, et al. Pain catastrophizing levels differentiate between common diseases with pain: HIV, fibromyalgia, complex regional pain syndrome, and breast cancer survivors. Scand J Pain. 2024;24. [CrossRef]
- Pinto AJ, Roschel H, de Sá Pinto AL, et al. Physical inactivity and sedentary behavior: Overlooked risk factors in autoimmune rheumatic diseases? Autoimmun Rev. 2017;16:667–74.
- Mok CC, Ko GTC, Ho LY, et al. Prevalence of atherosclerotic risk factors and the metabolic syndrome in patients with chronic inflammatory arthritis. Arthritis Care Res (Hoboken). 2011;63:195–202. [CrossRef]
- Feld J, Nissan S, Eder L, et al. Increased Prevalence of Metabolic Syndrome and Adipocytokine Levels in a Psoriatic Arthritis Cohort. Journal of Clinical Rheumatology. 2018;24:302–7. [CrossRef]
- Mallbris L, Ritchlin CT, Ståhle M. Metabolic disorders in patients with psoriasis and psoriatic arthritis. Curr Rheumatol Rep. 2006;8:355–63.
- Azfar RS, Gelfand JM. Psoriasis and metabolic disease: Epidemiology and pathophysiology. Curr Opin Rheumatol. 2008;20:416–22.
- Betancur G, Orozco MC, Schneeberger E, et al. Prevalence of Obesity and Metabolic Syndrome in Patients with Axial Spondyloarthritis - ACR Meeting Abstracts. 2015 ACR/ARHP Annual Meeting. 2015. https://acrabstracts. 6 September.
- Goodwin B, Khan D, Mehta A, et al. Exercise Therapies for Fibromyalgia Pain Catastrophizing: A Systematic Review and Comparative Analysis. Prim Care Companion CNS Disord. 2025;27. [CrossRef]
- Estévez-López F, Álvarez-Gallardo IC, Segura-Jiménez V, et al. The discordance between subjectively and objectively measured physical function in women with fibromyalgia: association with catastrophizing and self-efficacy cognitions. The al-Ándalus project. Disabil Rehabil. 2018;40:329–37. [CrossRef]
- Woolf, CJ. Central sensitization: Implications for the diagnosis and treatment of pain. Pain. 2011;152:S2.
- Angst F, Lehmann S, Sandor PS, et al. Catastrophizing as a prognostic factor for pain and physical function in the multidisciplinary rehabilitation of fibromyalgia and low back pain. European Journal of Pain (United Kingdom). 2022;26:1569–80. [CrossRef]
Figure 1.
Ascending nociceptive input integration systems via different thalamic nuclei distribution of the signal.
Figure 1.
Ascending nociceptive input integration systems via different thalamic nuclei distribution of the signal.
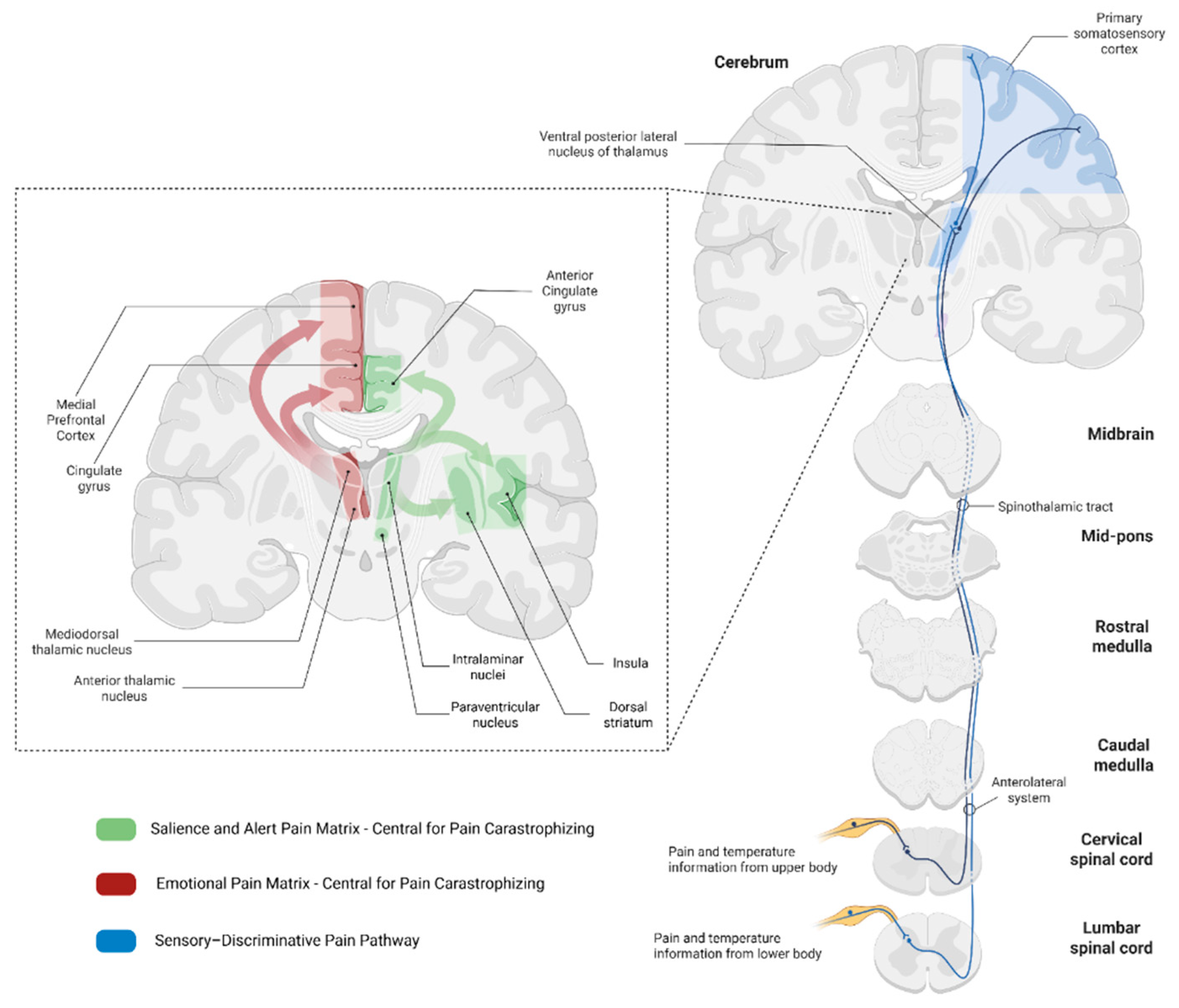
Figure 2.
Clinical implications of Pain Catastrophizing and Hopelessness and potential interventions.
Figure 2.
Clinical implications of Pain Catastrophizing and Hopelessness and potential interventions.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



