
Submitted:
14 March 2024
Posted:
15 March 2024
You are already at the latest version
Abstract
Research indicates that painful experiences can significantly affect the fear of cancer recurrence among cancer survivors, which is a distressing concern that influences both physiological and psychological recovery. Yet, the role of potential factors and mechanisms in these relationships is not fully known. This cross-sectional study aimed to advance our comprehension of the associa-tions between total pain and the fear of recurrence in post-treatment cancer patients by examining two potential mediators: psychological flexibility and mentalization. Three hundred and thirty-five participants (aged 22 to 88, 49.1% female) who had finished their cancer treatment completed self-report assessments of total pain, fear of recurrence, psychological flexibility, and mentalization. The serial mediation analysis showed that all dimensions of total pain were positively related to the fear of recurrence indirectly through psychological flexibility and mentalization, in serial. Additionally, gender moderated these serial mediational effects. In line with the psychological flexibility model, personal capacities to face difficult internal/external problems and interpret one’s behaviour in motivational terms can counterbalance patients’ negative emotions and feelings related to the illness.
Keywords:
total pain
; fear of recurrence
; psychological flexibility
; mentalization
; post-treatment cancer patients
1. Introduction
Cancer is affecting an increasing number of people worldwide [1], with approximately 35% of patients experiencing significant psychological distress [2]. Previous studies have shown that a significant proportion of patients who have completed cancer treatment report that managing the fear of cancer recurrence (FCR) is one of their key psychological problems [3,4]. This is mainly due to the chronic nature of cancer, the course and development of which is largely unpredictable. Pain is a frequent problem in cancer survivors, which strongly affects not only their physical health but also their overall psychological functioning [5]. Therefore, it is particularly important to examine how such factors as pain and personal resources (e.g., psychological flexibility and mentalization) may increase vs decrease FCR among those with a history of cancer.
1.1. Associations between Total Pain and Fear of Recurrence
Previous research suggests that cancer pain is a serious health problem among both cancer patients and survivors [6,7]. It affects not only the physical dimensions of the individual but also psychological, social, and existential ones. The multidimensional nature of pain is represented by the concept of total pain, which was introduced by Saunders as the suffering that encompasses physical, psychological, social, and spiritual sensations interacting upon one another [8,9]. Total pain thus tends to affect cancer patients in various essential spheres of their physiological and psychosocial functioning.
Research has shown that the dimensions of total pain were negatively related to meaning in life, coping, and psychological well-being in abdominal and pelvic cancer patients undergoing treatment [10], psychosocial functioning and quality of life in palliative cancer patients, and [11] self-efficacy and illness acceptance in pelvic cancer patients receiving radiotherapy treatment [12]. In addition, associations between the particular dimensions of total pain and psychological outcomes were found. For example, stronger physiological and psychological pain symptoms were associated with lower levels of physical, social, and emotional well-being among patients treated for cancer pain [13]; greater emotional and social pain were related to lower quality of life and increasing disease severity in haematological malignancies [14]; and more intense spiritual pain was related to poorer coping abilities and higher levels of depression, anxiety, and worry [15]. On the other hand, total pain was positively associated with stress and personal activities aimed at searching for meaning [10,12].
Given that total pain is closely related to the cognitive and emotional processes responsible for patients’ well-being, it is therefore plausible to expect associations between total pain and FCR. Among cancer survivors, experiencing new or ongoing symptoms of pain was associated with greater FCR [16]. Pain intensity and pain catastrophizing were also explicitly responsible for heightened FCR in childhood cancer survivors even if they had not had a relapse for many years [17]. Psychological distress, which is closely related to psychological pain, was found to relate positively to FCR in patients who had experienced different types of cancer [18,19]. Although there have not been any studies to date on the relationship between total pain and FCR, given the psychosocial determinants of FCR [20], such relations seem very plausible. In addition, research has not examined potential intervening mechanisms by which total pain may lead to the fear of recurrence among post-treatment cancer patients.
1.2. Psychological Flexibility and Mentalization as Intervening Variables
There is empirical evidence suggesting that the relationship between total pain and the fear of recurrence may be mediated by factors that enhance patients’ psychological resilience and facilitate reinterpretation of the disease. Psychological flexibility and mentalization, whose functional utility in cancer patients has been validated [21,22], offer potentially promising results. Psychological flexibility, which reflects one’s ability to remain in contact with thoughts and emotions during daily activities, was found to mediate the relationships between pain-related disability and life satisfaction among patients suffering from whiplash-associated disorder [23] and health conditions and emotional distress in a group of cancer survivors who were undergoing ACT-based therapy [24]. Psychological flexibility also mediated the relationship between pain intensity and depression in people with chronic pain, which confirms its role as a resilience factor [25]. Similarly, mentalization was found to mediate relationships between stressful life events and emotional dysregulation in a general population [26] and between distress and mental health symptoms in patients with psychosomatic problems; a higher level of mentalization was significantly associated with lower depression, anxiety, and somatization [27]. These findings suggest that psychological flexibility and mentalization may underlie the associations between cancer-related pain and the fear of recurrence. However, research has not examined the mediating effects of psychological flexibility and mentalization in post-treatment cancer patients.
The psychological flexibility model, which was proposed within acceptance and commitment therapy (ACT) [28] and proved its usefulness in cancer research [21,24], may advance our conceptualization and provide a theoretical foundation for understanding the complex relations. The model assumes that detrimental internal experiences (e.g., cognitions, feelings, and pain) are an inevitable part of human life and strongly affect psychosocial functioning. However, people have the ability to productively manage these unfavourable experiences and construct healthy and durable behaviour changes on the basis of their psychological skills. As a consequence, they can reduce distress and anxiety through using constructive thoughts and behaviour. The model includes six core elements, i.e., acceptance, cognitive defusion, present-focused attention, self as context, values, and committed action, which form a coherent process-oriented structure [29].
Within the psychological flexibility model, painful cognitions and emotions can be positively counteracted and attenuated by the ability to recognize and adapt to various situational demands and interpret one’s behaviour in terms of intentionally motivated states, which, in turn, will lead to less distress and anxiety. In other words, psychological flexibility and functional mentalization can serve as intervening factors by which global perceptions of cancer-related pain to a lesser extent affect the potential fear of recurrence. This assumption is supported by empirical studies that showed that psychological flexibility was a mediator in the association of both anxiety and depression with the fear of recurrence in cancer patients [30] and between fatigue and quality of life in people with a cancer diagnosis (current or previous) [31]. Although to date there has not been any research directly testing mentalization as a mediator in cancer patients, mentalization was proved to be a frequent mediator in other clinical groups; it mediated the relationship between psychological symptom severity and disabilities in activities and participation in psychotherapy patients who experienced severe traumatic problems [32] and the association between traumatic experiences and depressive symptoms in people suffering from various psychiatric disorders [33].
In addition, gender has been shown to influence the impact of pain on psychological functioning and emotional processes in cancer patients, which may partly be a consequence of women reporting higher FCR [36] and psychological distress [37] than men. Examining people with different types of cancer, Zajac and al. [38] found that gender moderated the relationship between risk perceptions and cancer worry; absolute risk scores in women were a stronger predictor of worry than in men. Gender was also a moderator of the association between cancer screening and perceived risk of colon cancer, with the association being stronger among women than among men [39] and between disease stage and anxiety and depressive symptoms, with the female gender being associated with higher levels of anxiety and depressive symptoms in advanced disease [40]. However, it should be acknowledged that the number of these studies is relatively small, and that some studies did not confirm the moderating role of gender in the relationship of pain with anxiety or worry [41], which may be due to the lack of differences in cancer-related pain between men and women [42].
These findings, although inconclusive, suggest that the moderating role of gender in the relationship between pain and FCR may depend on cognitive and emotional factors that influence the way in which cancer patients perceive pain-related symptoms and interpret their potential consequences for their future well-being. Given that both psychological flexibility and mentalization are increasingly recognized as playing a significant role in emotional well-being among cancer patients [34,35], it is highly plausible that they may also attenuate the negative symptoms related to total pain and the fear of recurrence.
The current study aimed to broaden our understanding of the relation between total pain and FCR by testing potential intervening variables (i.e., psychological flexibility, mentalization, and gender) (Figure 1). Based on previous findings and the psychological inflexibility model, we hypothesized that the dimensions of total pain would be negatively related to psychological flexibility and mentalization, and positively related to the fear of recurrence. We also hypothesized that psychological flexibility and mentalization would serially mediate the relationship between total pain and fear of relapse; moreover, this relationship would be moderated by gender.
2. Method
2.1. Participants and Procedure
The participants comprised 335 adult outpatients diagnosed with cancer between the ages of 22 and 88 (M = 59.78, SD = 13.28) in southern parts of Poland. The sample included 164 female (49.0%) and 171 male (51.0%) patients. All patients were in the post-treatment stage of cancer. Participants reported numerous types of cancer, with oral cavity and pharynx (N = 75, 22.4%), digestive system (N = 71, 21.2%), and genital and urinary system (N = 52, 15.5%) cancer being the most frequently endorsed. Most participants reported receiving radiotherapy (N = 151, 45.1%), followed by combined therapy (N = 11, 33.1%) and chemotherapy (N = 73, 21.8%). The majority of the sample identified are white or Caucasian (95.6%) and married (81.7%).
Participants were recruited at cancer treatment clinics during visits with their physician. The following inclusion criteria were set: (1) confirmed stages of cancer from I to III; (2) completion of cancer treatment; (3) lack of serious medical conditions that could significantly distort responses; and (4) sufficient cognitive abilities to complete the questionnaire. Eligible participants were provided with an informed consent form before being invited to complete the questionnaire. A total of 386 patients were approached by research assistants, of whom 29 were not eligible due to inclusion criteria, 12 refused to participate, and nine patients returned incomplete tests. A final sample of 335 (86.7%) participants was included in the study. All procedures were conducted in accordance with the approved Institutional Ethics Committee protocol at the first author’s university.
2.2. Measures
2.2.1. Total Pain
The Total Pain Questionnaire (TPQ) [43] is a 20-item self-report assessment of pain and consists of four subscales: physical pain (5 items, “As a result of my treatment so far, I am experiencing physical pain”); psychological pain (5 items, “I experience a sense of helplessness and anxiety due to illness”); social pain (5 items, “Being dependent on other people causes me pain”); and spiritual pain (5 items, “I feel an inner, spiritual suffering”). Participants rate each item on a 10-point scale ranging from 1 (not at all) to 10 (very strong), with higher scores indicating greater pain. The TPQ has demonstrated adequate concurrent validity [44]. In the current study, the Cronbach’s alphas for physical pain, psychological pain, social pain, and spiritual pain were 0.85, 0.84, 0.87, and 0.85, respectively.
2.2.2. Psychological Flexibility
The Acceptance and Action Questionnaire [45] is a seven-item measure of psychological flexibility that represents one’s capacity to function in accordance with core goals and values, even while facing difficult internal and external problems (e.g., “My painful experiences and memories make it difficult for me to live a life that I would value”). Participants rate each item on a seven-point scale ranging from 1 (never true) to 7 (always true), with higher scores indicating greater psychological flexibility. In the current study, Cronbach’s alpha was 0.90.
2.2.3. Mentalization
The Reflective Functioning Questionnaire (RFQ) is an eight-item scale measuring mentalization, which is understood as the capacity to perceive and interpret a person’s own and others’ behaviour in terms of intentionally motivated states (e.g., “People’s thoughts are a mystery to me”) [46]. The items are rated on a seven-point Likert scale ranging from 1 (completely disagree) to 7 (completely agree). The Polish version of the RFQ [47] was used, which measures mentalization only as a unidimensional construct (the original scale includes two subscales: the degree of uncertainty and certainty concerning mental states). Higher scores indicate greater mentalization. In the current study, Cronbach’s alpha was 0.78.
2.2.4. Fear of Recurrence
The Cancer Worry Scale (CWS) [48] is an eight-item scale that assesses concerns about developing cancer again and the effect of these concerns on daily life (e.g., “How often have you thought about your chances of getting cancer again?”). Participants rate each item on a four-point scale from 1 (never) to 4 (almost always). Higher scores represent stronger worries about cancer. The Cronbach’s alpha for the current study was 0.87.
2.3. Statistical Analysis
Analyses were conducted using SPSS version 28 with the PROCESS macro [49]. A priori power analysis was conducted to assess a sufficient number of participants; G*Power was used in accordance with Faul et al.’s recommendations [50] (a test power of 1-β = 0.80, α = 0.05). The results indicated that 304 participants would be required to obtain an effect size of .04. Adding a 10% non-response rate, the final sample size was 335.
Statistical analyses were conducted in several steps. First, as our study was based on mediation analysis, Harman’s single-factor test was used to check the possibility of common method variance [51]. Its results demonstrated satisfactory indicators: 18 different factors with the first unrotated factor explaining only 18.48% of the variance, which precludes the common method variance error. Second, the variance inflation factor (VIF) was 1.24, which excludes any potential multicollinearity. Third, descriptive statistics and bivariate correlations were calculated for all variables. Finally, mediation analysis (Model 4) with two parallel mediators (psychological flexibility and mentalization) and moderated mediation analysis (gender as a moderator) (Model 92) were applied to examine the direct and indirect effects of total pain on the fear of recurrence (bootstrapping with 10,000 samples; 95% bias-corrected confidence intervals) [49]. Four different chains for the dimensions of total pain, namely physical, psychological, social, and spiritual, were explored in these models.
3. Results
3.1. Descriptive and Preliminary Statistics
First, descriptive and bivariate statistics were calculated (Table 1). Age was negatively correlated only with physical and social pain, and psychological flexibility. All dimensions of total pain, i.e., physical, psychological, social, and spiritual, were positively associated with the fear of recurrence but negatively associated with psychological flexibility. Physical and psychological pain, but not social and spiritual pain, were negatively associated with mentalization. Both psychological flexibility and mentalization were negatively associated with the fear of recurrence.
3.2. Serial Mediation Model
Serial mediation analysis (Model 6) was conducted to examine whether psychological flexibility and mentalization would mediate the relationships between the dimensions of total pain and fear of recurrence, respectively (Table 2).
The examination of direct effects revealed that physical, psychological, social, and spiritual pain were negatively related to psychological flexibility but were unrelated to mentalization (Figure 2a–d). Psychological flexibility was positively related to mentalization and negatively related to fear of recurrence, while mentalization was negatively related to fear of recurrence. In contrast, the four dimensions of total pain, namely physical, psychological, social, and spiritual, were positively related to fear of recurrence.
As hypothesized, there were significant serial mediational effects of psychological flexibility and mentalization on the relations between the dimensions of total pain and fear of recurrence (Table 2). Specifically, the examination of direct effects showed that lower levels of physical, psychological, social, and spiritual pain were related to a higher level of psychological flexibility and consequently to higher mentalization, which in turn was related to a lower fear of recurrence (Figure 2a–d). In addition, some single mediational effects turned out to be significant. All single mediational effects of psychological flexibility in associations between the dimensions of total pain and fear of recurrence were significant, but the mediational effects of mentalization were found to be non-significant. This reflects the stronger mediating effect of psychological flexibility compared to mentalization.
The results of the indirect effects contrast showed that for physical and psychological pain, the indirect effect through psychological flexibility was significantly stronger than the indirect effect through mentalization and the serial indirect effect through psychological flexibility and mentalization. In addition to these differences, for social and spiritual pain, the serial indirect effect through psychological flexibility and mentalization was stronger than the indirect effect through mentalization.
As our study utilized a cross-sectional design, the alternative models including reverse orders of mediators, in serial (i.e., total pain → mentalization → psychological flexibility → fear of recurrence), were tested. However, the results of indirect effects turned out to be mostly non-significant (e.g., for physical and psychological pain, the indirect effects through mentalization and psychological flexibility on fear of recurrence were IE = -.01; CI = -.04 to -.03, and IE = -.007; CI = -.03 to .07, respectively).
3.3. Moderated Mediation Model: Gender Moderation
The current analysis tests whether the relationship between total pain and the fear of recurrence through psychological flexibility and mentalization is moderated by gender. Model 92 (moderation effect on all pathways) was chosen as the most advanced because it allows us to examine whether all the indirect effects of total pain on fear of recurrence – in both single (X→M1→Y, X →M2→Y) and serial mediations (X→M1→M2→Y) – are contingent on gender [49]. The statistical significance of the ‘Index of Moderated Mediation’ effect is assessed along with the conditional indirect effects across all four dimensions of total pain.
The results showed some significant indirect effects and moderated mediation indices (Table 3). Gender did not moderate any mediational effect of physical pain on fear of recurrence, although three of the six indirect effects (IE) were significant: the effect of physical pain through psychological flexibility on the fear of recurrence for both females (IE = .02; CI = .01 to .03) and males (IE = .04; CI = .02 to .06), and the effect of physical pain through psychological flexibility and mentalization on the fear of recurrence for males (IE = -.02; CI = -.02 to -.01). For psychological pain as an independent variable, gender significantly moderated its mediational effect on the fear of recurrence through mentalization. Specifically, for men, the conditional IE was non-significant (IE = .001; CI = -.01 to .01), whereas for women, the conditional IE was stronger and statistically significant (IE = -.03; CI = -.04 to -.01). Gender also moderated the serial mediational effect of psychological pain on the fear of recurrence through psychological flexibility and mentalization. The conditional IE was only significant for women (IE = -.02; CI = -.02 to -.01). For social pain, gender moderated the single mediational effect through psychological flexibility, with women having stronger conditional IE (IE = .05; CI = .03 to .07) than men (IE = .01; CI = .01 to .03). Gender also moderated the serial mediational effect of social pain on the fear of recurrence through psychological flexibility and mentalization. Specifically, for men, the conditional IE was non-significant (IE = -.002; CI = -.01 to .002), whereas for women, the conditional IE was stronger and statistically significant (IE = -.04; CI = -.03 to -.01). Finally, gender moderated the serial mediational effect of spiritual pain through psychological flexibility and mentalization; the conditional IE for women was stronger and more significant (IE = -.04; CI = -.03 to -.01) than for men (IE = -.002; CI = -.01 to .01).
In general, psychological flexibility and mentalization were more significant mediators in the relationship of psychological, social, and spiritual pain with the fear of recurrence in men than in women. However, there was no meaningful difference in the mediating effects of psychological flexibility and mentalization in the relationship between physical pain and the fear of recurrence between men and women. Gender was found to moderate the serial mediational effect of psychological, social, and spiritual pain on the fear of recurrence through psychological flexibility and mentalization.
4. Discussion
Cancer-related pain and FCR are significant problems among patients who have completed their treatment. To date, our understanding of the variables and psychological mechanisms underlying these relations, which is crucial for the improvement of effective therapeutic interventions, has been limited. The aim of this study was to investigate the mediating role of psychological flexibility and mentalization as serial mediators as well as the moderating function of gender among post-treatment cancer patients in the relationship between total pain and FCR.
4.1. Participants and Procedure
In our sample, all dimensions of total pain, i.e., physical, psychological, social, and spiritual, were positively related to the fear of recurrence. These results are consistent with previous studies in which symptoms of pain (new or ongoing) were related to higher levels of FCR in cancer survivors [16], and pain intensity and pain catastrophizing were predictors of greater FCR in childhood cancer survivors [17]. Our study extends the previous findings by showing that in post-treatment cancer patients, not only do physical or psychological aspects of pain influence the fear of potential recurrence, but also the social or spiritual experiences of pain activate such negative feelings of anxiety. In people with cancer, suffering thus encompasses all of the person’s physical, psychological, social, and spiritual struggles, generating thoughts and emotions related to the potential development of this disease.
In addition, all dimensions of total pain were negatively related to psychological flexibility, and physical and psychological pain were negatively related to mentalization. Our results are in line with previous research that demonstrated that cancer patients with higher levels experienced less emotional distress [24], and patients with psychosomatic problems with higher mentalization had lower depression, anxiety, and somatization [27]. These relationships seem particularly interesting as they indicate that various dimensions of cancer-related pain tend to undermine patients’ capacity to face challenging internal/external problems and to efficiently understand their own mental states as well as those of others. This interpretation is supported by research showing that painful physical and psychological feelings associated with cancer affect the way patients think about their ability to maintain internal integration and cope with adversity [24,52]. In patients with advanced, chronic illness, pain is thus a multidimensional symptom that compromises not only their quality of life but also the personal resources responsible for their current cognitive and emotional functioning.
4.2. The Mediating and Moderating Effects of Psychological Flexibility, Mentalization, and Gender
The key findings of the current study showed the serial mediational effects of psychological flexibility and mentalization in relationships between the dimensions of total pain and fear of recurrence. Specifically, patients who experience more pain in physical, psychological, social, and spiritual domains as a result of their cancer or cancer treatment are characterized by a higher ability to manage problematic internal/external situations and interpret their behaviour in terms of motivational states, which in turn is associated with less concern about developing cancer again. The serial nature of this mediation means that recognizing and adapting to various situational demands precedes interpreting one’s own actions. Additionally, the indirect effects contrast showed that individuals who experience more cancer-related total pain tend to rely more on their capacity to handle adverse problems on the basis of core goals and values (psychological flexibility) than to cognitively understand their own and others’ mental states (mentalization). Although they are independent factors, examining both in relation to FCR provides more information than studying either alone.
These findings highlight the role of personal abilities based on motivational and cognitive states as potential mechanisms underlying the association between cancer-related total pain and FCR. They are consistent with previous studies that showed the conceptual utility of psychological flexibility and mentalization in cancer patients [21,22] as well as the mediating role of psychological flexibility in the association between pain intensity and depression in non-cancer patients [25], and of mentalization in the association between distress and mental health symptoms in patients with psychosomatic problems [27]. They also offer support for the notion that associations between total pain and FCR have an indirect rather than a direct character, especially for individuals who have completed their cancer treatment.
At the same time, taken together, these results expand our understanding of the complex relationship between total pain and FCR as they reveal two significant aspects of emotional anxiety and adversity associated with cancer. First, for post-treatment cancer patients, different dimensions of total pain and fear of relapse do not occur as separate entities in an “existential vacuum” but are rather functionally interconnected on the basis of the ability to manage challenging or adverse situations and comprehend one’s own mental states. This notion is supported by earlier research that showed the mediating effects of psychological flexibility and mentalization between pain outcomes and detrimental emotional and health symptoms in cancer [24] and non-cancer [26] patients. In other words, what determines the final character of the relationship between total pain and FCR are flexible and mentalizing approaches.
Second, the serial character of the mediation (i.e., psychological flexibility–mentalization) suggests that, despite the cross-sectional nature of our study, identifying and adapting to challenging illness conditions precedes the modes of interpreting patients’ own behaviour. Consequently, patients who experience a high level of total pain will first try to maintain a balance among important life domains and then to construe their own actions in terms of intentional motivation, which in turn will lead to a reduced fear of relapse. This interpretation receives some confirmation within the psychological flexibility model, which assumes that individuals can alleviate painful cognitions and emotions – first, by recognizing and harmonizing the various situational demands of life, and then, by developing patterns of effective action related to chosen values [21,29]. Psychological flexibility and mentalization may thus serve as intermediary mechanisms through which post-treatment cancer patients are able to counterbalance their negative emotions and feelings related to the illness. This seems especially important as patients with higher psychological flexibility and mentalization experienced a lower fear of recurrence.
Extending previous studies on the moderating role of gender in the relationship between pain and emotional processes in cancer patients [36,37], this study specifies that gender moderated the serial mediational effect of three dimensions of total pain (i.e., psychological, social, and spiritual) on the fear of recurrence through psychological flexibility and mentalization. In all cases, the effect was stronger for women than men. These results confirm prior research on cancer patients in which gender was a moderator in the relationship between risk perceptions and cancer worry, with women obtaining stronger effects than men [38], and in the association between disease stage and anxiety, with women reporting higher levels of anxiety [40]. This may be due to a greater tendency in women to react emotionally and worry about the disease and its potential consequences [36], as well as experiencing a statistically higher level of FCR than men [36]. Another, additional explanation for this may relate to women’s greater ability to be aware of unfavourable thoughts and emotions about cancer and a greater tendency to self-analyse. In this sense, the results highlight an important role of gender-related ability to manage difficult internal health problems and respond to challenging and emotionally charged events.
Despite this study’s contribution to the current research on pain and FCR, there are some limitations that need to be formulated. First, our study applied a cross-sectional design that precludes any temporal relationships; yet, the alternative models with a reversed sequence of mediators, in serial, were not significant. Future research should consider examining longitudinal relations among the variables tested in our study in order to definitely confirm their direction. Second, the current study measured mentalization conceptualized as a unidimensional construct [36]. Given the existence of other multidimensional measures of mentalization as well [53], their future use could expand our knowledge about the mediating role of mentalization. Next, due to hospital restriction policies, we did not have access to strictly cancer-related medical data (e.g., number of radiation doses, hormonal indicators, blood tests), so estimating their potential impact on the relationship between pain and FCR was not possible. Lastly, the current study relied on a single tool measuring FCR, which may not fully detect all aspects of cancer recurrence anxiety; therefore, future research should also consider utilizing measures that assess constructs such as distress and mental health concerns.
5. Conclusions
Notwithstanding these limitations, the present study broadens our understanding of mediating factors and psychological mechanisms in the relation between cancer-related total pain and the fear of cancer recurrence. Importantly, it established the significant role of psychological flexibility and mentalization in the association between total pain and FCR in post-treatment cancer patients. The study also has practical, clinical implications as it provides clinicians and therapists with additional knowledge about considering different dimensions of pain in coping with the fear of cancer, designing relevant post-treatment interventions based on personal and motivational factors, and prioritizing patients’ concerns about their painful sensations and emotional responses. In providing health services, appropriate and effective fulfilment of the needs of cancer survivors experiencing FCR is indeed paramount.
Author Contributions
Conceptualization, D.K., E.T., M. Sz., and A.F.; methodology, D.K., E.T., M. Sz., and A.F.; formal analysis, D.K., E.T., M. Sz., and A.F.; investigation, D.K., E.T., M. Sz.; data curation, D.K. and E.T.; writing ‒ original draft, D.K., E.T., M. Sz., and A.F.; writing ‒ review and editing, D.K., E.T., M. Sz., and A.F.; project administration, D.K.; funding acquisition, D.K., E.T., M. Sz., and A.F. All authors have read and agreed on the published version of the manuscript.
Funding
The Article Processing Charge was funded by the University of Opole, University of Szczecin, and Maria Sklodowska-Curie National Research Institute of Oncology, Gliwice Branch.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of University of Opole, KOJBN nr 6/2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available at OSF Home: https://osf.io/5j2hd/
Acknowledgments
The authors would like to thank the medical personnel and patients for their contribution to this study.
Conflicts of Interest
The authors declare no conflict of interest
References
- Chhikara, B.S.; Parang, K. Global Cancer Statistics 2022: the trends projection analysis. Chem. Biol. Lett. 2023, 10, 451–451. [Google Scholar]
- Momenimovahed, Z.; Salehiniya, H.; Hadavandsiri, F.; Allahqoli, L.; Günther, V.; Alkatout, I. Psychological distress among cancer patients during COVID-19 pandemic in the world: a systematic review. Front. Psychol. 2021, 12, 682154. [Google Scholar] [CrossRef] [PubMed]
- Luigjes-Huizer, Y.L.; Tauber, N.M.; Humphris, G.; Kasparian, N.A.; Lam, W.W.; Lebel, S. . van der Lee, M.L. What is the prevalence of fear of cancer recurrence in cancer survivors and patients? A systematic review and individual participant data meta-analysis. Psycho-Oncol. 2022, 31, 879–892. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sun, D.; Qin, N.; Liu, M.; Jiang, N.; Li, X. Factors correlated with fear of cancer recurrence in cancer survivors: a meta-analysis. Cancer Nurs. 2022, 45, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Glare, P.A.; Davies, P.S.; Finlay, E.; Gulati, A.; Lemanne, D.; Moryl, N. ;... Syrjala, K.L. Pain in cancer survivors. J Clin Oncol. 2014, 32, 1739. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.R.; Ramirez, J.D.; Farquhar-Smith, P. Pain in cancer survivors. Br. J. Pain 2014, 8, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Evenepoel, M.; Haenen, V.; De Baerdemaecker, T.; Meeus, M.; Devoogdt, N.; Dams, L. ; ... De Groef, A. Pain prevalence during cancer treatment: a systematic review and meta-analysis. J. Pain Symptom. Manage. 2022, 63, e317–e335. [Google Scholar] [CrossRef] [PubMed]
- Saunders, D.C.M. The management of terminal illness; Hospital Medicine Publications: London, 1967. [Google Scholar]
- Saunders, C. The evolution of palliative care. Patient Educ. Counsel. 2000, 41, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Krok, D.; Telka, E.; Zarzycka, B. Modeling psychological well-being among abdominal and pelvic cancer patients: The roles of total pain, meaning in life, and coping. Psycho-Oncol. 2022, 31, 1852–1859. [Google Scholar]
- Mehta, A.; Chan, LS. Understanding of the concept of ‘total pain’: a prerequisite for pain control. J Hospice Palliat. Nurs. 2008, 10, 26–32. [Google Scholar] [CrossRef]
- Krok, D.; Telka, E.; Zarzycka, B. Total pain and illness acceptance in pelvic cancer patients: exploring Self–Efficacy and stress in a moderated mediation model. Int. J. Environ. Res. Public Health. 2022, 19, 9631. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Brubaker, A.; Meghani, S.H.; Bruner, D.W.; Yeager, K.A. Spirituality and quality of life in black patients with cancer pain. J Pain Symptom Manag. 2018, 56, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Quinn, B.; Ludwig, H.; Bailey, A.; Khela, K.; Marongiu, A.; Carlson, K.B. ;... Seesaghur, A. Physical, emotional and social pain communication by patients diagnosed and living with multiple myeloma. Pain Manag. 2021, 12, 59–74. [Google Scholar] [CrossRef]
- Delgado–Guay, M.O.; Palma, A.; Duarte, E.; Grez, M.; Tupper, L.; Liu, D.D.; Bruera, E. Association between spirituality, religiosity, spiritual pain, symptom distress, and quality of life among Latin American patients with advanced cancer: a multicenter study. J. Palliat. Med. 2021, 24, 1606–1615. [Google Scholar] [CrossRef] [PubMed]
- Crist, J.V.; Grunfeld, E.A. Factors reported to influence fear of recurrence in cancer patients: a systematic review. Psycho-Oncol. 2013, 22, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Tutelman, P.R.; Chambers, C.T.; Noel, M.; Heathcote, L.C.; Fernandez, C.V.; Flanders, A. ;... Urquhart, R. Pain and fear of cancer recurrence in survivors of childhood cancer. Clin. J. Pain 2022, 38, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Lebel, S.; Rosberger, Z.; Edgar, L.; Devins, G.M. Emotional distress impacts fear of the future among breast cancer survivors not the reverse. J. Cancer Surviv. 2009, 3, 117–127. [Google Scholar] [CrossRef]
- Rincones, O.; Smith, A.B.; Naher, S.; Mercieca–Bebber, R.; Stockler, M. An updated systematic review of quantitative studies assessing anxiety, depression, fear of cancer recurrence or psychological distress in testicular cancer survivors. Cancer Manag. Res. 2021, 3803–3816. [Google Scholar] [CrossRef]
- Myers, S.B.; Manne, S.L.; Kissane, D.W.; Ozga, M.; Kashy, D.A.; Rubin, S. ;... Graff, J.J. Social–cognitive processes associated with fear of recurrence among women newly diagnosed with gynecological cancers. Gynecol. Oncol. 2013, 128, 120–127. [Google Scholar] [CrossRef]
- Hulbert-Williams, N.J.; Storey, L.; Wilson, K.G. Psychological interventions for patients with cancer: psychological flexibility and the potential utility of Acceptance and Commitment Therapy. Eur. J. Cancer Care 2015, 24, 15–27. [Google Scholar] [CrossRef]
- Cieślak, M.; Kozaka, J.; Golińska, P.B.; Bidzan, M. Mentalization and its relation to life satisfaction and the level of mental adjustment to illness in women with breast cancer – A pilot study. Int. J. Environ. Res. Public Health 2022, 19, 10323. [Google Scholar] [CrossRef] [PubMed]
- Wicksell, R.K.; Olsson, G.L.; Hayes, S.C. Psychological flexibility as a mediator of improvement in Acceptance and Commitment Therapy for patients with chronic pain following whiplash. Eur. J. Pain. 2010, 14, 1059–e1. [Google Scholar] [CrossRef]
- González-Fernández, S.; Fernández-Rodríguez, C.; Paz-Caballero, M.D.; Pérez-Álvarez, M. Treating anxiety and depression of cancer survivors: Behavioral activation versus acceptance and commitment therapy. Psicothema 2018, 30, 14–20. [Google Scholar] [PubMed]
- Gentili, C.; Rickardsson, J.; Zetterqvist, V.; Simons, L.E.; Lekander, M.; Wicksell, R.K. Psychological flexibility as a resilience factor in individuals with chronic pain. Front. Psychol. 2019, 10, 2016. [Google Scholar] [CrossRef]
- Parada-Fernández, P.; Herrero-Fernández, D.; Oliva-Macías, M.; Rohwer, H. Stressful life events and hopelessness in adults: the mediating role of mentalization and emotional dysregulation. Braz. J. Psychiatry 2020, 43, 385–392. [Google Scholar] [CrossRef]
- Riedl, D.; Rothmund, M.S.; Grote, V.; Fischer, M.J.; Kampling, H.; Kruse, J. ;... Lampe, A. Mentalizing and epistemic trust as critical success factors in psychosomatic rehabilitation: results of a single center longitudinal observational study. Front. Psychiatry 2023, 14, 1150422. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and commitment therapy: the process and practice of mindful change; Guilford Press: New York, 2012. [Google Scholar]
- McCracken, L.M.; Morley, S. The psychological flexibility model: a basis for integration and progress in psychological approaches to chronic pain management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef]
- Seltzer, J.D. Fear of Cancer Recurrence: The Roles of Psychological Flexibility and Social Support as Possible Protective Factors. Doctoral dissertation, Kean University, 2020. [Google Scholar]
- Duarte, J.; Björkstrand, F.K.; McCracken, L.; Perrin, S. The contribution of psychological flexibility to functioning in people living with cancer-related pain. Eur. J. Pain 2023, 27, 413–423. [Google Scholar] [CrossRef]
- Probst, T.; Dehoust, M.; Brütt, A.L.; Schulz, H.; Pieh, C.; Andreas, S. Mentalization and self–efficacy as mediators between psychological symptom severity and disabilities in activities and participation in psychotherapy patients. Psychopathology 2018, 51, 38–46. [Google Scholar] [CrossRef]
- Belvederi Murri, M.; Ferrigno, G.; Penati, S.; Muzio, C.; Piccinini, G.; Innamorati, M. ;... Amore, M. Mentalization and depressive symptoms in a clinical sample of adolescents and young adults. Child Adolesc. Ment. Health 2017, 22, 69–76. [Google Scholar] [CrossRef]
- Smith, E.; Gow, A.; Forsyth, L.; Bryne, B.; Howells, L.; Anderson, A. ; Maggie’s Centres. The relationship between psychological flexibility, value-based living and emotional well-being in people affected by cancer. J. Glob. Oncol. 2018, 4 Supp 2, 115s-115. [Google Scholar]
- Lo, C.; Hales, S.; Chiu, A.; Panday, T.; Malfitano, C.; Jung, J. ;... Rodin, G. Managing Cancer And Living Meaningfully (CALM): randomised feasibility trial in patients with advanced cancer. BMJ Support. Palliat. Care 2019, 9, 209–218. [Google Scholar] [CrossRef]
- Simard, S. , Savard, J. Fear of cancer recurrence inventory: development and initial validation of a multidimensional measure of fear of cancer recurrence. Support. Care Cancer 2009, 17, 241–251. [Google Scholar] [CrossRef]
- Yang, Y.; Li, W.; Wen, Y.; Wang, H.; Sun, H.; Liang, W. ;... Humphris, G. Fear of cancer recurrence in adolescent and young adult cancer survivors: a systematic review of the literature. Psycho-Oncol. 2019, 28, 675–686. [Google Scholar] [CrossRef]
- Zajac, L.E.; Klein, W.M.; McCaul, K.D. Absolute and comparative risk perceptions as predictors of cancer worry: Moderating effects of gender and psychological distress. J. Health Com. 2006, 11, 37–49. [Google Scholar] [CrossRef] [PubMed]
- McQueen, A.; Vernon, S.W.; Meissner, H.I.; Rakowski, W. Risk perceptions and worry about cancer: does gender make a difference? J. Health Com. 2008, 13, 56–79. [Google Scholar] [CrossRef] [PubMed]
- Vodermaier, A.; Linden, W.; MacKenzie, R.; Greig, D.; Marshall, C. Disease stage predicts post-diagnosis anxiety and depression only in some types of cancer. Br. J. Cancer 2011, 105, 1814–1817. [Google Scholar] [CrossRef] [PubMed]
- Markfelder, T.; Pauli, P. Fear of pain and pain intensity: Meta-analysis and systematic review. Psychol. Bull. 2020, 146, 411. [Google Scholar] [CrossRef]
- Ahmed, Y.; Popovic, M.; Wan, B.A.; Lam, M.; Lam, H.; Ganesh, V. ;... Chow, E. (2018). Does gender affect self-perceived pain in cancer patients? A meta-analysis. Ann. Palliat. 2018, 6 Suppl 2, S177–S184. [Google Scholar] [CrossRef] [PubMed]
- Krok, D.; Telka., E. Kwestionariusz Bólu Totalnego [The Total Pain Questionnaire (TPQ)]. Instytut Psychologii UO, Opole, 2021.
- Krok, D.; Telka, E.; Zarzycka, B. Modeling psychological well-being among abdominal and pelvic cancer patients: The roles of total pain, meaning in life, and coping. Psycho-Oncol. 2022, 31, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Bond, F.W.; Hayes, S.C. , Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.;... Zettle, R.D. Preliminary psychometric properties of the acceptance and action questionnaire–ii: A revised measure of psychological inflexibility and experiential avoidance. Beh. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef]
- Fonagy, P.; Luyten, P.; Moulton-Perkins, A.; Lee, Y.W.; Warren, F.; Howard, S. ;... Lowyck, B. Development and validation of a self-report measure of mentalizing: The reflective fun.;ctioning questionnaire. PloS One 2016, 11, e0158678. [Google Scholar] [CrossRef]
- Woźniak-Prus, M.; Gambin, M.; Cudo, A.; Sharp, C. Investigation of the factor structure of the Reflective Functioning Questionnaire (RFQ-8): One or two dimensions? J. Per. Assess. 2022, 104, 736–746. [Google Scholar] [CrossRef] [PubMed]
- Custers, J.A.; van den Berg, S.W.; van Laarhoven, H.W.; Bleiker, E.M.; Gielissen, M.F.; Prins, J.B. The Cancer Worry Scale: detecting fear of recurrence in breast cancer survivors. Cancer Nurs. 2014, 37, E44–E50. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach; Guilford Publications: New York and London, 2018. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Beh. Res. Meth. 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Redaei, S.; Goodarzi, M.A.; Imani, M. The prediction of experienced pain based on mediating role of psychological flexibility in the relationship between meta cognition and meta emotion in patients with blood cancer. J. Res. Psychol. Health 2023, 18, 31–45. [Google Scholar]
- Gori, A.; Topino, E. Exploring and deepening the facets of mentalizing: the integration of network and factorial analysis approaches to verify the psychometric properties of the Multidimensional Mentalizing Questionnaire (MMQ). Int. J. Environ. Res. Public Health 2023, 20, 4744. [Google Scholar] [CrossRef]
Figure 1.
A conceptual model of the serial mediation of psychological flexibility and mentalization in associations between total pain and fear of recurrence and moderated mediation by gender.
Figure 1.
A conceptual model of the serial mediation of psychological flexibility and mentalization in associations between total pain and fear of recurrence and moderated mediation by gender.
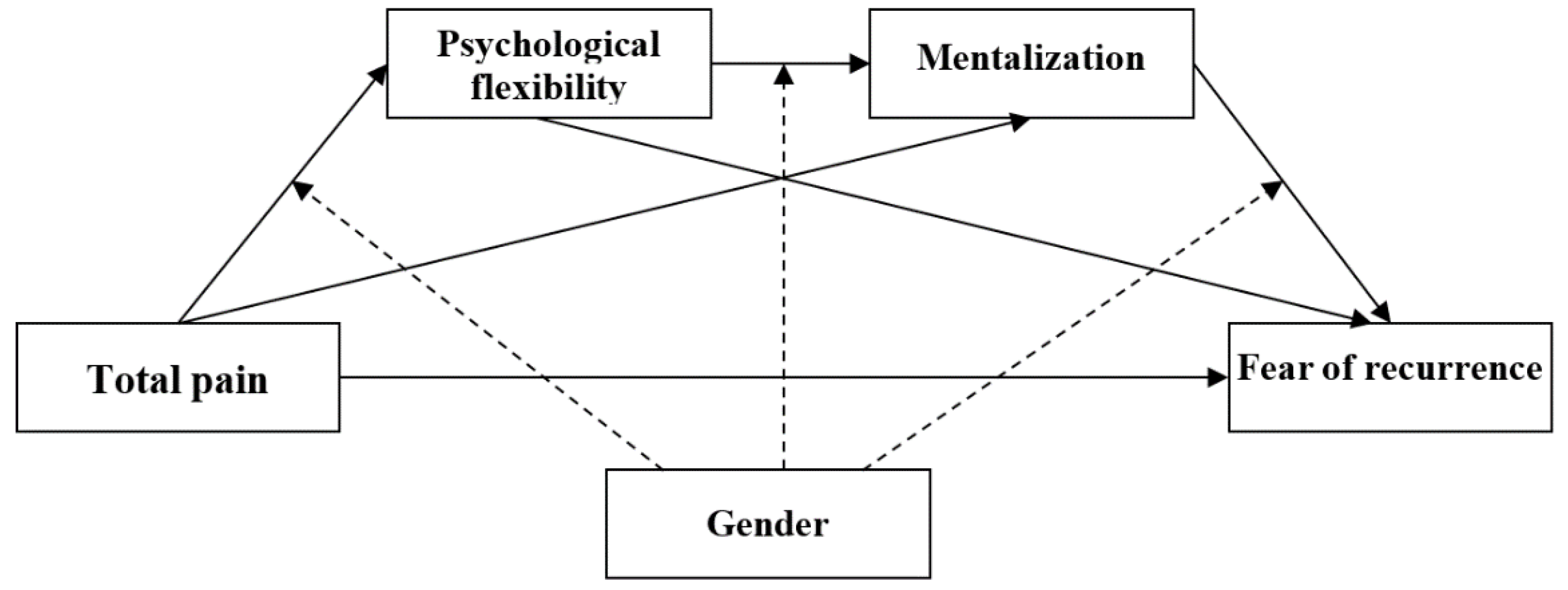
Figure 2.
(a-d) Serial mediation models for psychological flexibility and mentalization in associations between the physical dimension of total pain and fear of recurrence.
Figure 2.
(a-d) Serial mediation models for psychological flexibility and mentalization in associations between the physical dimension of total pain and fear of recurrence.
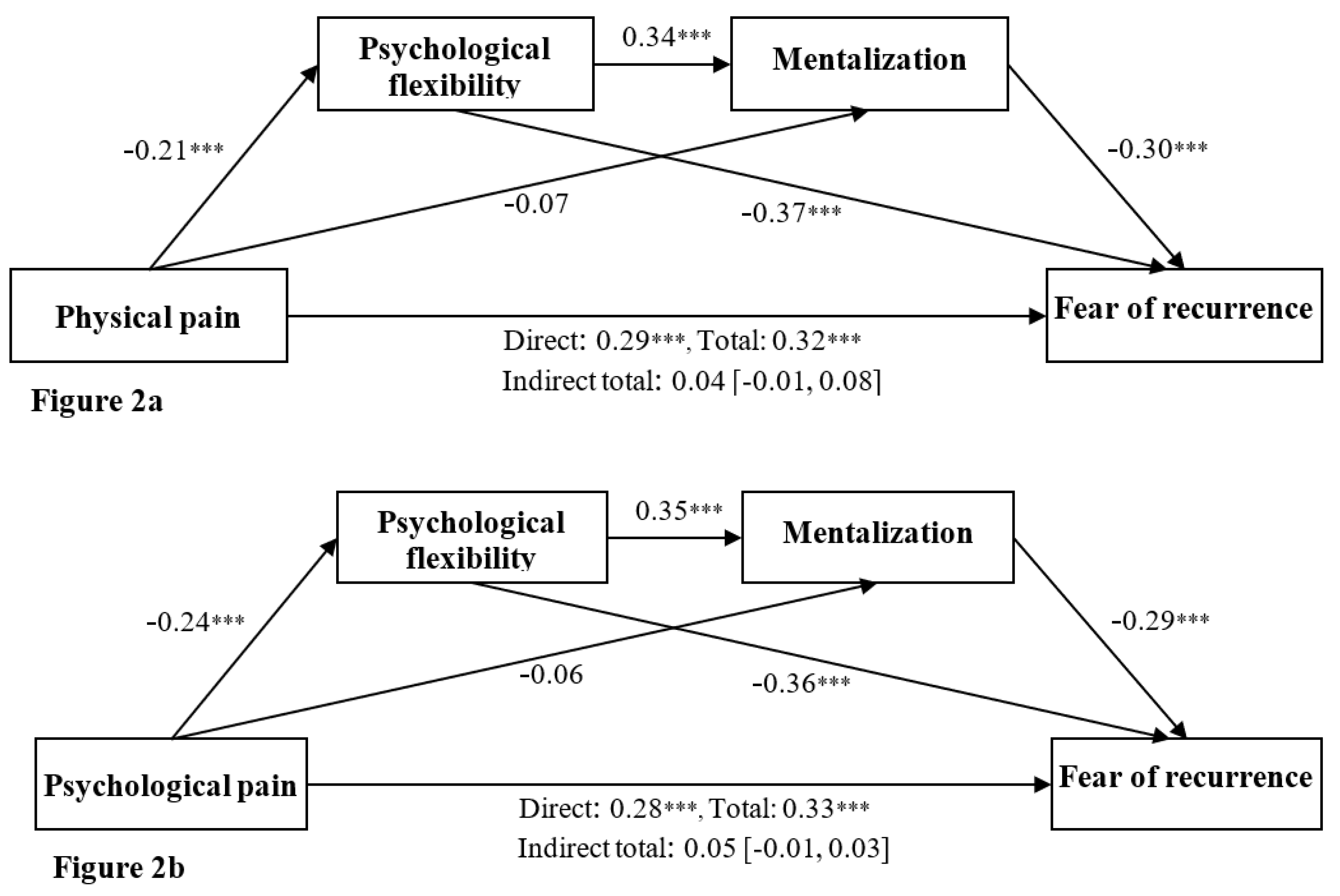
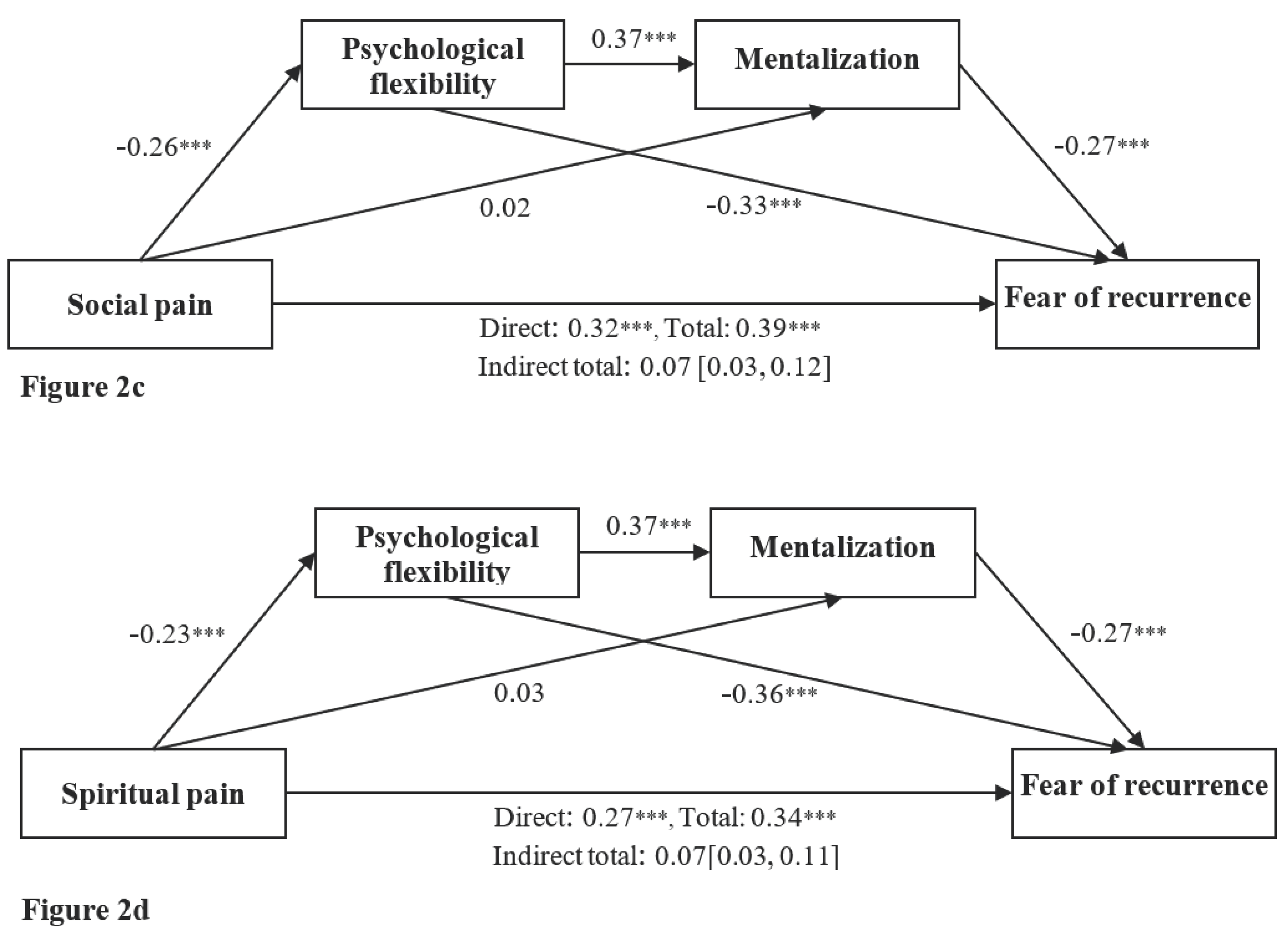

Table 1.
Correlations among age, total pain, fear of recurrence, psychological flexibility, and mentalization.
Table 1.
Correlations among age, total pain, fear of recurrence, psychological flexibility, and mentalization.
| Variables | M | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. |
|
59.78 | 13.28 | ‒ | ||||||
|
3.03 | 2.18 | -0.20*** | ||||||
|
3.31 | 2.16 | -0.10 | 0.50*** | ‒ | ||||
|
2.61 | 1.95 | -0.12* | 0.57*** | 0.70*** | ‒ | |||
|
2.15 | 1.99 | -0.10 | 0.47*** | 0.58*** | 0.76*** | ‒ | ||
|
1.98 | 0.70 | -0.09 | 0.32*** | 0.33*** | 0.39*** | 0.34*** | ||
|
4.92 | 1.06 | -0.11* | -0.21*** | -0.24*** | -0.26*** | -0.23*** | -0.32*** | |
|
4.62 | 0.91 | -0.09 | -0.14** | -0.14** | -0.07 | -0.05 | -0.13* | 0.36*** |
* p < 0.05; ** p < 0.01; *** p < 0.001.
Table 2.
Standardized indirect effects of the dimensions of total pain on fear of recurrence through psychological flexibility and mentalization, and specific indirect effect contrasts for the paths.
Table 2.
Standardized indirect effects of the dimensions of total pain on fear of recurrence through psychological flexibility and mentalization, and specific indirect effect contrasts for the paths.
| Variables | ||||
| Indirect effects for physical pain | Effect | SE | LLCI | ULCI |
| PhP → PF → FoR (Ind 1) | .08 | .02 | .04 | .12 |
| PhP → Me → FoR (Ind 2) | -.02 | .02 | -.05 | .01 |
| PhP → PF → Me → FoR (Ind 3) | -.02 | .01 | -.04 | -.01 |
| Total | .04 | .02 | -.01 | .08 |
| Indirect effects contrast | ||||
| C 1 = Ind 1 – Ind 2 | .10 | .03 | .05 | .16 |
| C 2 = Ind 1 – Ind 3 | .10 | .03 | .05 | .15 |
| C 3 = Ind 2 – Ind 3 | .01 | .02 | -.04 | .04 |
| Indirect effects for psychological pain | ||||
| PsP → PF → FoR (Ind 1) | .09 | .02 | .05 | .13 |
| PsP → Me → FoR (Ind 2) | -.02 | .02 | -.05 | .01 |
| PsP → PF → Me → FoR (Ind 3) | -.03 | .01 | -.04 | -.01 |
| Total | .05 | .02 | -.01 | .09 |
| Indirect effects contrast | ||||
| C 1 = Ind 1 – Ind 2 | .10 | .03 | .05 | .17 |
| C 2 = Ind 1 – Ind 3 | .11 | .03 | .05 | .17 |
| C 3 = Ind 2 – Ind 3 | .01 | .02 | -.03 | .05 |
| Indirect effects for social pain | ||||
| SoP → PF → FoR (Ind 1) | .03 | .02 | .05 | .14 |
| SoP → Me → FoR (Ind 2) | .01 | .01 | -.02 | .04 |
| SoP → PF → Me → FoR (Ind 3) | -.03 | .01 | -.04 | -.01 |
| Total | .07 | .02 | .03 | .12 |
| Indirect effects contrast | ||||
| C 1 = Ind 1 – Ind 2 | .08 | .03 | .03 | .14 |
| C 2 = Ind 1 – Ind 3 | .11 | .03 | .06 | .17 |
| C 3 = Ind 2 – Ind 3 | .04 | .02 | .01 | .07 |
| Indirect effects for spiritual pain | ||||
| SpP → PF → FoR (Ind 1) | .08 | .02 | .04 | .13 |
| SpP → Me → FoR (Ind 2) | .01 | .01 | -.02 | .04 |
| SpP → PF → Me → FoR (Ind 3) | -.02 | .01 | -.04 | -.01 |
| Total | .07 | .02 | .03 | .11 |
| Indirect effects contrast | ||||
| C 1 = Ind 1 – Ind 2 | .07 | .03 | .02 | .13 |
| C 2 = Ind 1 – Ind 3 | .10 | .03 | .05 | .16 |
| C 3 = Ind 2 – Ind 3 | .03 | .02 | .01 | .07 |
PhP – physical pain; PsP – psychological pain; SoP – social pain; SpP – spiritual pain; PF – psychological flexibility; Me – mentalization; FoR – fear of recurrence.
Table 3.
Moderated mediation estimates for fear of recurrence outcomes.
| Moderated mediation index | Effect (SE) | LLCI | ULCI |
| PhP → PF → FoR | .02 (.01) | -.01 | .04 |
| PhP → Me → FoR | -.01 (.01) | -.02 | .01 |
| PhP → PF → Me → FoR | -.01 (.01) | -.02 | .001 |
| PsP → PF → FoR | .02 (.01) | -.01 | .04 |
| PsP → Me → FoR | -.04 (.01) | -.05 | -.01 |
| PsP → PF → Me → FoR | -.05 (.01) | -.02 | -.01 |
| SoP → PF → FoR | .05 (.02) | .01 | .05 |
| SoP → Me → FoR | -.01 (.01) | -.02 | .02 |
| SoP → PF → Me → FoR | -.06 (.01) | -.03 | -.01 |
| SpP → PF → FoR | .02 (.01) | -.01 | .05 |
| SpP → Me → FoR | .01 (.01) | -.01 | .03 |
| SpP → PF → Me → FoR | -.05 (.01) | -.02 | -.01 |
physical pain – PhP; psychological pain – PsP; social pain – SoP; spiritual pain – SpP; psychological flexibility – PF; mentalization – Me; Fear of recurrence – FoR.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



