
Submitted:
30 October 2025
Posted:
31 October 2025
You are already at the latest version
Abstract
Adolescence is a critical period of vulnerability for the onset of mental health difficul-ties, presenting an urgent need for scalable prevention strategies. Diet is a universal, modifiable factor, yet its evidence base remains inconsistent. This systematic review synthesized evidence from controlled trials and prospective cohort studies investigat-ing the relationship between diet and mental health in adolescents aged 10–19 years. Searches were conducted to July 2025, and risk of bias was assessed. Nineteen studies met inclusion criteria: six intervention trials and thirteen cohort studies. Examined exposures included vitamin D, omega-3s, polyphenol-rich foods, Mediterranean-style diets, and overall diet quality. Across designs, healthier dietary patterns were often associated with fewer depressive symptoms, while poorer diet quality was linked to increased psychological distress. However, the current evidence is constrained by wide variation in assessments, small samples, and significant methodological limita-tions—particularly with high risk or some concerns noted in half of the included in-tervention trials—along with evidence suggesting that associations may differ by sex and are often sensitive to adjustment for socioeconomic status. Despite these chal-lenges, the findings confirm diet as a possible, actionable target for supporting ado-lescent mental health. This review concludes by proposing a detailed roadmap for fu-ture research, prioritizing harmonized symptom-based outcomes, biomarker-verified assessments, explicit analysis of sex and socioeconomic (SES) effects, and adequately powered trials to inform effective public health strategies for youth. Protocols were registered with PROSPERO (CRD42023413970) and archived on the Open Science Framework (https://osf.io/c6xze).
Keywords:
adolescents
; mental health
; depression
; anxiety
; diet quality
; dietary patterns
; micronutrients
; systematic review
1. Introduction
Adolescence is a critical developmental window characterised by rapid social, psychological, and biological change. It is also a period of heightened vulnerability, with early symptoms of mental health difficulties emerging as early as ages 7–11 [1]. Globally, around one in five adolescents experience mental health problems, underscoring the need to identify modifiable risk and protective factors. Within this context, diet has gained increasing attention as a plausible, scalable influence on adolescent mental health [2].
Building on this, the consequences of early-onset mental health problems are profound. Difficulties that emerge in adolescence frequently persist into adulthood, elevating risk for recurrent depression and anxiety, poorer academic attainment e.g., Wickersham et al, 2021 [3], impaired social functioning, and reduced quality of life [4]; see also [5]. These sequelae can derail key developmental milestones and contribute to the intergenerational transmission of risk. Adolescence therefore represents a critical window for prevention and early intervention. Within this context, diet has been highlighted as a modifiable, scalable factor embedded in daily life; however, the evidence base remains heterogeneous and at times inconsistent, motivating a systematic synthesis.
In parallel, traditional interventions e.g., psychotherapy and pharmacotherapy, remain but insufficient to meet the rising burden of adolescent mental health difficulties. These approaches can be costly, carry side-effects, and remain inaccessible for many, particularly in low-resource settings [6]. They also rarely address lifestyle and environmental determinants that may underlie psychological vulnerability. By contrast, dietary patterns offer a promising, scalable target with direct relevance to adolescents - who are simultaneously gaining autonomy over food choices, facing heightened nutritional demands for growth and brain development, and showing susceptibility to unhealthy behaviours that can track into adulthood [7,8]. These developmental features provide a strong rationale for considering diet as a leverage point in adolescent mental health.
Taken together, the evidence supports the plausibility of a diet–mental health relationship in adolescence. Epidemiological studies consistently associate poorer diet quality with greater depressive and anxiety symptoms, whereas healthier dietary patterns are linked to more favourable outcomes [9,10]. Multiple pathways provide biological credibility - including diet-related modulation of inflammation, oxidative stress, gut microbiota, and neurotrophic factors - all implicated in mental health [11]. However, findings remain heterogeneous. Intervention studies - spanning nutrient supplementation and whole-diet modification - report mixed effects, with considerable variability in design, dietary assessment, outcome measures, and effect sizes, as well as differing risks of bias. Collectively, these limitations constrain causal inference and the strength of current conclusions.
Prior syntheses in youth have typically narrowed either the exposure or the outcome. For example, reviews centred on supplementation (omega-3 or vitamin D) in children and adolescents with depression, and diet-as-treatment RCTs targeting depressive symptoms specifically [12]. Likewise, several adolescent reviews restrict outcomes to depression, linking diet quality or healthy patterns with fewer depressive symptoms but offering limited coverage of broader mental-health endpoints [13]. Many also organise evidence by diagnostic categories, which can obscure symptom heterogeneity, underrepresent subclinical distress, and reduce comparability across tools and settings [14,15]. In contrast, this review concentrates on the most rigorous study designs (controlled trials and longitudinal cohorts) and considers a wider range of dimensional outcomes, including depressive and anxiety symptoms, stress, well-being, and internalising/externalising indices. Crucially, we also synthesise available evidence regarding the influence of sex and socioeconomic status on these diet–mental health relationships. This comprehensive approach aims to improve construct coverage and the real-world relevance of findings beyond clinic-defined groups, thereby enhancing applicability for both clinical practice and public-health policy.
2. Materials and Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [16]. Protocols were registered with PROSPERO (CRD42023413970) and archived on the Open Science Framework (https://osf.io/c6xze). PRISMA 2020 checklists are provided (Supplementary Appendix 1a–1b). The review proceeded in two phases. In Phase 1, literature searches were conducted to scope the field using preliminary eligibility criteria. In Phase 2, final research questions and eligibility criteria were applied..
2.1. Search Strategy and Selection Criteria
A systematic search of [List your databases, e.g., Scopus, MEDLINE, PsycINFO] was conducted up to July 2025 to identify relevant literature published in English before 2025. The search strategy combined three core concepts: (1) an adolescent population (e.g., “Adolescents” OR “Adolescence”); (2) nutrition-related exposures (e.g., “Food” OR “Meal” OR “Diet”); and (3) mental health outcomes (e.g., “Mental health” OR “Mood” OR “Depression”). The search was further refined to include only prospective study designs (e.g., longitudinal, cohort, RCT) and to exclude cross-sectional studies, review articles, and studies focused on eating disorders. To identify unpublished studies, we also searched the British Library of Electronic Theses Online Service (EThOS). A full, unabridged example of the search string used for Scopus is available in the Supplementary Information. The strategy was implemented by H.Y. and J.T. Reference lists of included studies and relevant reviews were hand-searched.
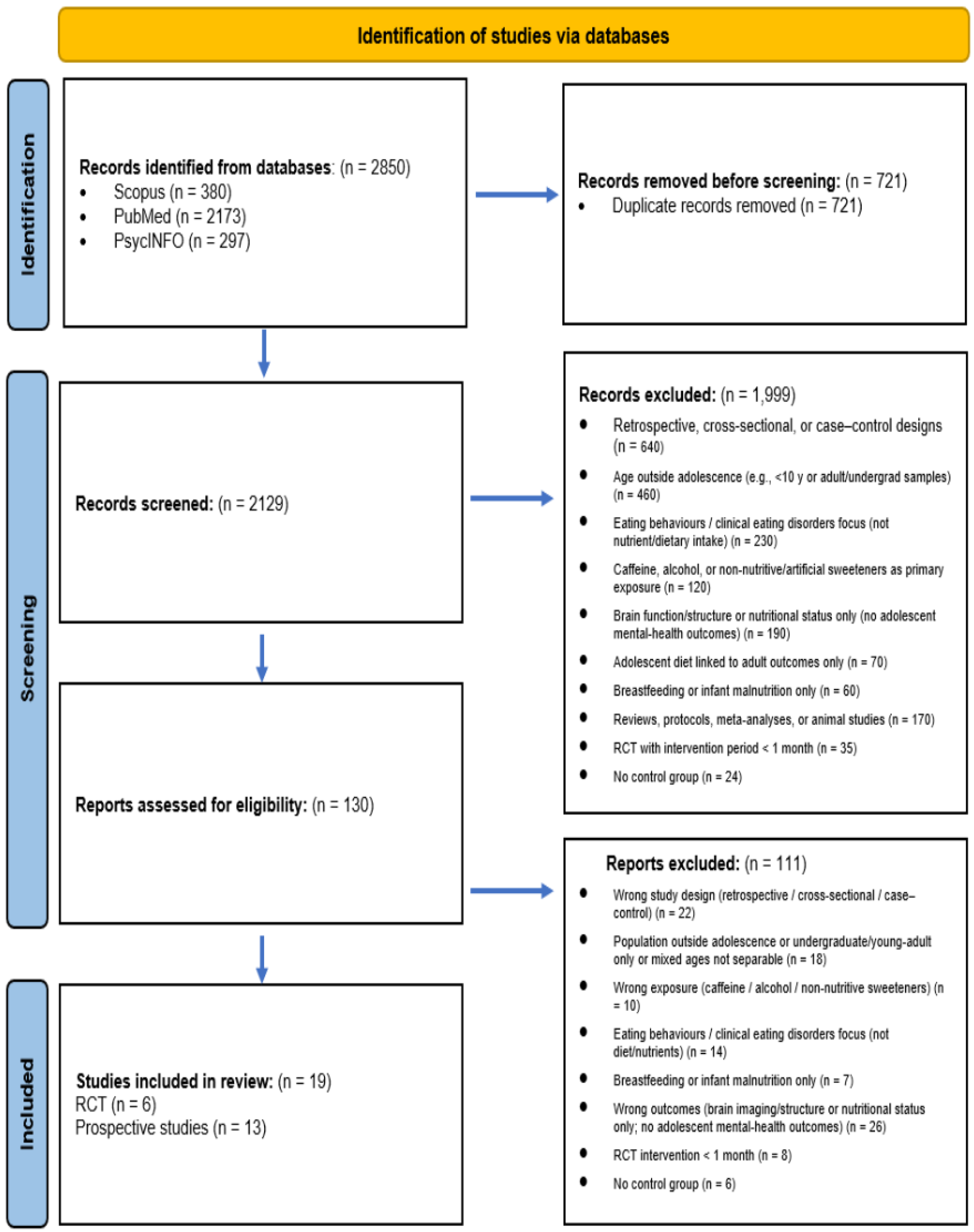
Study selection. Records were de-duplicated and screened independently by the two reviewers (titles/abstracts, then full texts). Disagreements were resolved by discussion or a third reviewer (A.B). Reasons for full-text exclusion were recorded. The selection process is shown in the PRISMA flow diagram (Figure 1).
2.2. Eligibility Criteria
2.2.1. Inclusion
Eligible studies enrolled adolescents aged 10–19 years (World Health Organization definition) drawn from the general population, using the National Academies of Sciences, Engineering, and Medicine definition (i.e., including individuals with, or at risk for, chronic disease such as overweight/obesity unless a nutrient-specific exception applied), or adolescents with nutritional deficiencies. Eligible designs comprised randomised or non-randomised controlled trials and prospective cohort studies, including cluster variants; acute single-consumption trials were excluded, and chronic interventions were defined as lasting one month or longer. Eligible exposures included dietary patterns or nutrient intake assessed during adolescence, or diet assessed in infancy (<3 years) with mental-health outcomes measured during adolescence. Outcomes were required to be assessed using validated mental-health instruments. Only full-text, peer-reviewed articles published in English were considered.
2.2.2. Exclusion
Exclusions were: animal studies, reviews, protocols, and meta-analyses; samples outside adolescence (e.g., <10 years or exclusively undergraduate/young-adult populations); studies focused on eating behaviours or clinical eating disorders rather than nutrient/dietary intake; studies examining caffeine, alcohol, or non-nutritive/artificial sweeteners as the primary exposure (sugar-sweetened beverages were eligible); studies reporting only brain function/structure or nutritional status without adolescent mental-health outcomes; studies relating adolescent diet to adult outcomes only; studies focused solely on breastfeeding or malnutrition in infancy; and retrospective, cross-sectional, or case–control designs.
2.3. Data Extraction
Data were extracted by a single reviewer (J.T.) using a piloted template and independently verified by a second reviewer (H.Y.) for completeness and accuracy. Extracted items included: author and year; country and study setting; exposure definition (dietary intervention and duration for trials; dietary assessment method for cohorts); sample size; participant characteristics (mean age and standard deviation, BMI where reported, sex/gender distribution, location, baseline health status); study design; mental-health measures (instrument and timing); primary outcomes with effect estimates and precision; covariates/adjustment strategy; funding/source of support; and reviewer notes on interpretation. When required information was unclear or missing, study authors were contacted for clarification.
2.4. Outcome Measures
The primary outcome measure was mental health, assessed using validated and standardised tools such as mood and depression scales. Secondary outcome measures included self-reported or clinically observed indicators of psychological wellbeing, emotional regulation, and behavioural health. Additional outcomes comprised objective indicators of nutritional status, dietary intake, or relevant biomarkers, provided these were examined in relation to changes in mental health or psychological outcomes.
2.5. Organisation Process
Studies were organised first by design (randomised controlled trials vs prospective cohort studies) and then by dietary exposure. For trials, categories reflected the intervention type (e.g., vitamin D, omega-3 fatty acids, polyphenol-rich foods such as wild blueberries, multi-component whole-diet modification). For prospective cohorts, categories reflected the exposure assessed (e.g., adherence to Mediterranean-style patterns, macro-/micronutrient intake, sugar-sweetened/soft-drink consumption, overall diet quality indices). Results are presented in this hierarchy to maintain comparability within design and exposure type.
2.6. Risk of Bias
Risk of bias was assessed using design-appropriate, established tools. For randomised controlled trials, the Cochrane Risk of Bias 2 (RoB 2) tool was applied [17], with cluster adaptations used where applicable. For prospective cohort studies, the Joanna Briggs Institute Critical Appraisal Checklist for Cohort Studies was used. All assessments were conducted after data extraction by two independent reviewers (H.Y. and J.T.); disagreements were resolved by discussion or, where necessary, consultation with a third reviewer (A.B.). Additional information was sought from study protocols or by contacting authors when possible. Domain-level judgements and overall ratings (low / some concerns / high for RoB 2; low / moderate / high for JBI) are reported in Supplementary Tables S1–S2.
3. Results
3.1. Study Selection
The PRISMA flow diagram is shown in Figure 1. In total, 2,850 records were identified across databases (Scopus = 380; PubMed = 2,173; PsycINFO = 297). After de-duplication (n = 721), 2,129 titles/abstracts were screened and 1,999 were excluded. 130 full texts were assessed for eligibility, of which 111 were excluded for pre-specified reasons (e.g., wrong design, population, exposure, or outcome; insufficient data), leaving 19 studies for inclusion: six randomised controlled trials and thirteen prospective cohort studies. Full-text exclusion reasons are summarised in Figure 1.
3.2. Randomised Controlled Trials (RCTs)
Six RCTs evaluated dietary interventions in adolescents: vitamin D supplementation [18,19,20], omega-3 fatty acids acids [21,22], and a polyphenol-rich whole food [wild blueberries; 23]. Samples were predominantly mixed-sex, and participants were generally healthy. Adolescent mental-health outcomes were assessed with validated instruments (Table 1).
Depressive symptoms were the most frequently evaluated endpoint, appearing in four trials [18,20,21,23]. Measures included the Beck Depression Inventory [20], the Mood and Feelings Questionnaire [23], the Center for Epidemiologic Studies Depression Scale [21], and YSR/CBCL internalising subscales [18]. Aggressive or externalising behaviours were assessed in one trial [18]. Self-esteem was examined once using the Rosenberg Self-Esteem Scale [21]. Anxiety-related outcomes featured in two trials: one reported RCADS anxiety risk [23], and the other reported DASS anxiety/stress together with WHOQOL-BREF domains [19]. The Isaac et al. trial did not report depression scores as an outcome; in contrast, the Fisk et al. trial did report depression as a primary outcome, measured separately with the MFQ. Transient affect was assessed using PANAS-Now [23] and a 10-item visual analogue mood scale [22].
Across these interventions, effects on mental-health endpoints were heterogeneous. Favourable effects were seen in some, but not all, trials that used high-dose supplementation or targeted populations with potentially low baseline nutrient status [20]. In contrast, some shorter or lower-dose interventions, and one long-term trial hampered by poor adherence, yielded null findings [19,21,22]. Interpretation is further constrained by variation in outcome selection (multiple instruments tapping overlapping constructs), small samples, and variation in adherence or biomarker verification, which together limit comparability across trials. Full intervention characteristics and measurement instruments are summarised in Table 1.
Figure 1.
PRISMA flow diagram of the study selection process.
3.2.1. Vitamin D Supplementation
Three RCTs evaluated vitamin D supplementation. Trials lasted three months [18,19], and were conducted in Norway [18], and India [19,20]. Dosing regimens varied markedly: one trial provided 38 µg/day (≈1,520 IU) versus placebo to 50 adolescents [18]; a school-based study delivered a fortified snack containing 1,000 IU vitamin D₃/day to 71 adolescents [19]; and a cluster-randomised trial provided an effective daily dose of 2,250 IU, while controls received 250 IU plus calcium [20]. Across the three trials, the signal for mental health benefits was mixed. In rural India, a cluster RCT also reported a small-to-moderate reduction in depressive symptoms (mean difference ≈ −3.4 BDI-II points), which was consistent across analyses [20]. In contrast, the snack-fortification trial in India found no change in health-related quality of life (WHOQOL-BREF) or anxiety and stress (DASS-21) [19]. Similarly, the trial in Norway noted that while supplementation corrected vitamin D deficiency, it did not alter internalising or externalising outcomes (YSR-CBCL), although an exploratory analysis suggested a link between low baseline vitamin D and greater externalising problems [18].
In sum, based on the three included RCTs, there is emerging but inconsistent evidence that vitamin D supplementation may reduce depressive symptoms in adolescents. This effect was most apparent in the largest trial which used a relatively higher dose [20], while the two smaller trials using lower doses reported null findings for their primary mental health outcomes. There was minimal evidence from this set of studies for benefits on externalising behaviour, anxiety, stress, or quality of life [18,19]. Confirmation in larger, rigorously designed RCTs – ideally with baseline status stratification, biomarker verification, and standardised outcome batteries – is warranted.
3.2.2. Fatty Acids
Two trials evaluated omega-3 fatty acid supplementation, with intervention durations ranging from 8 weeks [UK; 22] to 12 months [Netherlands; 21]. Although both targeted omega-3, procedures and implementation differed substantially.
In Kennedy, Jackson [22], 90 healthy 10–12-year-olds were randomised to placebo, 400 mg/day DHA (two capsules morning, placebo evening), or 1,000 mg/day DHA (capsules morning and evening); capsules also contained 4 mg EPA and vegetable oil. Compliance exceeded 80% under parental supervision. Outcomes comprised computerised cognitive tasks and a visual-analogue mood scale. Apart from a single effect on relaxation favouring both DHA arms, no consistent benefits for cognition or broader mood were detected, plausibly reflecting the short exposure period and modest per-arm sample sizes (n≈30).
van der Wurff, von Schacky [21] conducted a double-blind, placebo-controlled trial (n=256; age 14–15 years) with krill-oil EPA+DHA. Cohort I escalated from 400 mg/day (260 mg EPA, 140 mg DHA) for three months to 800 mg/day (520 mg EPA, 280 mg DHA); Cohort II commenced at the higher dose. Placebo oils resembled a typical European fatty-acid profile. Adherence was poor: by six months the mean Omega-3 Index (O-3I) in the active group reached only 5.29% (target 8–11%), declining to 4.86% at twelve months, indicating missed doses on ~44% of days between months 6–12. Primary outcomes were depressive symptoms (CES-D) and self-esteem (Rosenberg). Neither intention-to-treat nor O-3I-based analyses showed significant intervention effects. At 12 months, depressive symptoms trended non-significantly lower in the active group (M=10.86, SD=8.92) versus placebo (M=13.60, SD=11.95; p=0.066; d=0.20), and self-esteem was marginally higher (M=23.00, SD=4.96 vs 21.74, SD=6.36; p=0.120; d=0.15).
Taken together, current data are not sufficient to support a robust effect of omega-3 supplementation on adolescent mood outcomes. A short, well-adhered DHA trial yielded at most a modest, isolated improvement in subjective relaxation [22], 2009), whereas a longer trial with suboptimal adherence and sub-target O-3I showed a borderline benefit for depressive symptoms or self-esteem [21]. Future trials should prioritise adequate duration, dose, and exposure verification (e.g., O-3I targets), with sufficient power to detect clinically relevant effects and to test baseline-status moderation.
3.2.3. Polyphenols/Wild Blueberry
A four-week, double-blind, placebo-controlled RCT in the United Kingdom [23] examined daily wild-blueberry (WBB) supplementation in adolescents aged 12–17 years (n=64). Participants consumed either a flavonoid-rich WBB drink delivering ~253 mg anthocyanins/day or a placebo matched for sugars and vitamin C. Baseline depression and anxiety were subclinical in both groups. After four weeks, the WBB group reported lower depressive symptoms than placebo (Cohen’s d=0.65), with no between-group differences for anxiety or positive/negative affect. Although limited by short duration and modest sample size, this study provides preliminary evidence that short-term flavonoid supplementation may reduce self-reported depressive symptoms in adolescents [23]. Replication in larger samples, including clinically elevated cohorts, is warranted.
3.2.4. Summary of Randomized Controlled Trials
Across six RCTs, interventions targeted vitamin D, omega-3 fatty acids, and a polyphenol-rich whole food (wild blueberries), with outcomes spanning depressive symptoms, anxiety, self-esteem, externalising behaviours, and transient mood. The clearest signal concerned depressive symptoms. One larger vitamin D trial reported small-to-moderate improvements [20], while two smaller trials reported no effect on their primary mental health outcomes [18,19]. The single trial of polyphenols (wild blueberries) also reported a positive effect on depressive symptoms [23], whereas the two omega-3 trials yielded null findings for mood [21,22]. Attrition was a notable limitation in several studies, with rates exceeding 20% in some trials [20,21]. Furthermore, short exposure periods [22,23] limited sample sizes in some studies [18,19,22,23], heterogeneity in outcome instruments, and suboptimal adherence [21] constrain inference. Larger, longer, and methodologically rigorous trials - ideally stratified by baseline nutrient status and employing standardised outcome batteries - are required to clarify the efficacy of these interventions for adolescent mental health.
3.3. Prospective Studies
The review’s search identified thirteen prospective cohort studies. Unlike RCTs, these followed participants longitudinally without intervention, evaluating associations between habitual dietary exposures and subsequent adolescent mental health. Exposures encompassed Mediterranean-style adherence [24,25,26], macronutrient intake [27,28], micronutrient intake [29,30], soft-drink consumption [31], and overall dietary pattern/quality indices [32,33,34,35,36]. Most studies recruited mixed-sex community samples; one focused on elite athletes [27].
Outcomes covered multiple domains of adolescent mental health. Depressive symptoms or emotional functioning were the most frequently examined endpoints [26,27,28,30,31,32,33,34], using a range of self-report instruments such as the PedsQL, BDI-Y, MFQ, PHQ-9, and a brief subscale from the DISC. Anxiety and emotional symptoms were assessed with the SCARED [24], while broader externalizing and aggressive behaviours were measured using the YSR [29,35] and a dedicated aggression scale [31]. One study used the validated Flourishing Scale to assess psychological well-being, capturing positive dimensions of positive functioning such as purpose, optimism, and social connectedness [36].
Across cohorts, findings were generally consistent for dietary patterns, where healthier patterns predicted better mental health outcomes [32,33,34,35,36], although one well-controlled study found no prospective association after full adjustment for covariates [26]. For specific exposures, higher soft-drink consumption was prospectively linked to increased aggression [31], while associations for individual nutrients were varied but generally pointed towards a protective effect, including for protein [27], magnesium [29], vitamin D₃ [30], and dietary fibre (though this effect was not independent of the overall dietary pattern) [28]. Overall, while cohort evidence supports a plausible relationship between diet quality and adolescent mental health, comparability is limited by non-aligned dietary indices and outcome instruments, and by residual confounding typical of observational designs.
3.3.1. Adherence to Mediterranean Diet (MD)
Three longitudinal studies examined MD adherence in relation to adolescent psychological outcomes, but differed in direction of analysis, outcome scope, and measurement approach, yielding mixed conclusions. In Spain, a school-based cohort (n=165; mean age 13.5 years) assessed MD adherence using the Krece Plus index (0–11) alongside FFQ-derived dietary patterns and constructed a composite “emotional symptoms” indicator from the SCARED, Children’s Depression Inventory, and Youth’s Inventory-4. Among females, emotional symptoms were associated with lower subsequent MD adherence and a greater likelihood of a sweet/fatty pattern; no associations were observed in males [24]. Notably, the analytic emphasis was on emotional symptoms predicting later diet, rather than diet predicting later symptoms. In Lebanon, a 12-month cohort (n=563; assessments at baseline, 6, and 12 months) tracked MD adherence with the KIDMED index (0–12) and evaluated self-efficacy and academic achievement. Rising MD adherence predicted higher academic achievement at both follow-ups, and self-efficacy independently predicted achievement at 12 months; however, no clinical symptom measures were included, limiting inferences for mental-health endpoints per se [25]. Attrition and reliance on self-report warrant caution.
In the United Kingdom, the ROOTS cohort (n=603; mean age 14.5 to 17.5 years) derived an MD score from a 4-day diet diary and examined depressive symptoms using the MFQ at baseline and follow-up. While higher baseline fruit and vegetable intake correlated with lower concurrent MFQ scores, these associations attenuated after adjustment for smoking, alcohol, and energy intake; neither the MD score nor specific food groups prospectively predicted depressive symptoms after full adjustment [26].
Taken together, longitudinal evidence linking MD adherence to adolescent mental-health outcomes is limited and inconsistent. One study suggests emotional symptoms may precede lower subsequent MD adherence [24], a second links MD adherence to academic (not clinical) outcomes with a socio-cognitive correlate (self-efficacy) [25], and a third finds no prospective association between MD adherence and depressive symptoms after robust adjustment [26]. Variability in dietary indices (KIDMED, Krece Plus, diary-based MD score), outcome definitions, and confounder adjustment, together with attrition and regional sampling, constrains comparability and weakens causal inference for MD adherence and adolescent mental health.
3.3.2. Macronutrient Intake
Two prospective cohorts examined macronutrient intake in relation to adolescent depressive symptoms, focusing on distinct populations and exposures. In Swiss elite athletes, a 10-month longitudinal study (final analytic n=79; 62% male; mean age 16.4 years) assessed diet via a 3-day recall and depressive symptoms with the PHQ-9 at baseline and follow-up [27]. Hierarchical regressions adjusting for baseline symptoms and sex indicated that higher protein intake prospectively predicted lower depressive symptom severity, whereas total fat, polyunsaturated fatty acids, carbohydrate, and sugar were not associated. Relative to DACH reference values, athletes’ energy, carbohydrate, and PUFA intakes were below recommendations and sugar intake exceeded recommendations, with protein adequate. Interpretation is constrained by the modest sample, 3-day recall, and the specificity of an elite-sport cohort.
In a general-population sample from the Western Australian Pregnancy Cohort (Raine) Study, dietary intake was captured with a 212-item FFQ at ages 14 and 17 years, with fibre intake categorised into quartiles; depressive symptoms were measured using the BDI-Y and converted to T-scores [28]. Mixed-effects logistic models adjusting for demographics, energy intake, adiposity, lifestyle, and family factors showed that adolescents in the highest fibre quartile had lower odds of moderate/extreme depressive symptoms than those in the lowest. This association persisted after excluding participants with baseline symptoms and after adjustment for hs-CRP but attenuated when overall dietary patterns (Healthy vs Western) were included, suggesting that fibre’s apparent protective effect may be partly attributable to broader diet quality rather than an independent nutrient effect. Limitations include attrition between assessments and reliance on self-reported diet (Table 2).
Taken together, cohort evidence for macronutrients is selectively supportive. Protein intake predicted fewer depressive symptoms in elite athletes, and higher fibre intake related to lower odds of depressive symptoms in community adolescents, though the latter appeared sensitive to overall diet quality. These findings highlight the need for studies with objective or repeated dietary measures, broader biomarker panels, and samples representative beyond specialised subgroups to clarify whether macronutrient–mood associations are independent of dietary patterns.
3.3.3. Micronutrient Intake
Two longitudinal cohorts examined micronutrients in relation to adolescent mental health, conducted in Australia and the United Kingdom (Table 2). Although exposures, outcomes, and developmental windows differed, both studies provide insight into nutrient-specific associations with externalising and internalising symptoms.
In the Western Australian Pregnancy Cohort (Raine) Study, 684 adolescents were assessed at ages 14 and 17 years [29]. Dietary zinc and magnesium intake were estimated via a semi-quantitative FFQ, and externalising behaviours were measured with the Youth Self-Report (YSR). After adjustment for energy intake and relevant confounders, higher magnesium intake was associated with fewer externalising behaviours at both ages. Zinc showed a similar inverse trend that did not reach statistical significance. Interpretation is tempered by attrition between follow-ups, reliance on self-reported diet, and potential residual confounding.
Using the ALSPAC cohort, Tolppanen, Sayers [30] investigated whether childhood serum 25-hydroxyvitamin D predicted later depressive symptoms. Blood samples were obtained at mean age 9.8 years, and depressive symptoms were assessed with the MFQ at 10.6 years (n = 2,759) and 13.8 years (n = 2,752). Higher 25(OH)D₃ concentrations predicted lower depressive symptoms at age 13.8 (adjusted odds ratio per doubling of 25(OH)D₃ = 0.90, 95% CI 0.86–0.95), but not at age 10.6; 25(OH)D₂ showed no association at either time point. Higher 25(OH)D₃ was also associated with a greater likelihood of symptom improvement between 10.6 and 13.8 years. Limitations include substantial attrition, possible confounding by outdoor activity and related behaviours, and reliance on a single serum measurement.
Taken together, micronutrient findings are nutrient- and outcome-specific: magnesium intake relates to externalising behaviours, and vitamin D₃ status (but not D₂) relates to depressive symptoms in early-to-mid adolescence, with weaker evidence for zinc. Replication in larger cohorts with repeated dietary/biomarker assessments and comprehensive confounder control is needed to clarify directionality and generalisability.
3.3.4. Soft Drink Consumption
A single longitudinal cohort examined soft-drink intake in relation to adolescent mental health, modelling reciprocal associations with aggression and depressive symptoms across three waves spanning five years [31]. Drawing on the Healthy Passages cohort (n=5,147; 51% female; mean age 11.1 years at baseline) with assessments at ages 11, 13, and 16 years, adolescents self-reported soft-drink consumption over the past seven days, aggressive behaviour (Forms and Functions of Aggression), and depressive symptoms (six items from the DISC Predictive Scales). Analyses employed an autoregressive cross-lagged model adjusting for sociodemographic, health, and behavioural covariates (including BMI, overall diet, exercise, substance use, and family factors). Cross-sectionally, higher soft-drink intake correlated with greater aggression at all three ages and with more depressive symptoms at ages 11 and 13. Longitudinally, intake at 11 predicted greater aggression at 13, and intake at 13 predicted greater aggression at 16. Aggression at 13 also predicted higher intake at 16, indicating bidirectional links for aggression. By contrast, no prospective association emerged between soft-drink intake and depressive symptoms; if anything, intake at 13 predicted slightly fewer depressive symptoms at 16. Depressive symptoms did not predict later intake.
The study’s strengths include a large, multi-site, ethnically diverse sample and pre-registered longitudinal modelling; however, exclusive reliance on adolescent self-report for both exposure and outcomes raises the possibility of shared-method variance and correlated error, which may inflate associations. Future work would benefit from objective intake measures (e.g., purchase data, biomarkers) and multi-informant mental-health assessments to reduce common-method bias and strengthen causal interpretation.
3.3.5. Quality of Dietary Patterns
Six longitudinal cohorts examined overall dietary quality in relation to adolescent mental health [26,32,33,34,35,36]. Three were conducted in Australia, one in Canada [36], and two were from the United Kingdom [26,32]. Participants spanned early to late adolescence (11–18 years). Diet was assessed using FFQs, diet diaries, or composite diet-quality indices; outcomes included general mental health, depressive symptoms, anxiety symptoms, psychological well-being, and internalising/externalising behaviours.
In an Australian school-based sample (n≈3,000), higher healthy diet scores predicted better emotional functioning on the PedsQL, and within-person changes in diet quality over two years paralleled changes in mental health, with no evidence for reverse causation [33]. In a socially deprived UK cohort (n≈2,800), an unhealthy diet was cross-sectionally associated with greater odds of SDQ-defined problems (highest quintile OR=2.10, 95% CI 1.38–3.20). Prospective analyses suggested a similar link, although effects attenuated after full adjustment for confounders [33].
Two cohorts focused on depression-related outcomes. In the UK ROOTS study (n=603), no prospective associations were detected between a Mediterranean Diet score and later depressive symptoms after robust adjustment for confounders, leading the authors to suggest previous findings may be due to confounding by lifestyle factors like smoking and alcohol [26]. In contrast, in the Australian Raine cohort (n=843), a ‘Western’ pattern at 14 years predicted higher BMI and inflammatory markers (leptin, hs-CRP) at 17, which in turn predicted higher depressive symptoms (BDI-Y) and internalising/externalising problems (YSR) [34]. Behavioural outcomes were further examined in the Raine cohort by Trapp, Allen et al. [35], linking a ‘Western’ pattern at 14 years to higher externalising problems at 17 in females only.
In a large Canadian cohort (COMPASS; n = 13,887), Dabravolskaj et al. [36] examined specific dietary indicators (fruit and vegetables [F&V], sugar-sweetened beverages [SSBs], junk food, breakfast frequency) in relation to depressive symptoms (CESD-R-10), anxiety symptoms (GAD-7), and psychological well-being (Flourishing Scale) over one year. After adjusting for baseline mental health and numerous covariates, higher baseline SSB consumption predicted greater depressive (β = 0.04) and anxiety symptoms (β = 0.02) and lower psychological well-being (β = -0.03) at follow-up. Higher baseline F&V consumption predicted greater psychological well-being (β = 0.06) but was not significantly associated with depressive or anxiety symptoms after full adjustment. Associations for SSBs were noted to be stronger in males.
Overall, while several cohorts suggest a pattern where poorer diet quality is associated with greater mental health problems [32,33,34,35,36], this finding was not universal. One large UK study found no prospective association after robustly adjusting for confounders [26]. Interpretation across all studies is constrained by attrition, reliance on self-reported diet, and attenuation of effects after adjustment for lifestyle behaviours, suggesting that diet quality may act as part of a broader constellation of health behaviours rather than as an independent causal factor.
3.4. Risk of Bias Assessment
The risk of bias across the six included RCTs was varied. Using the Cochrane RoB 2 tool, three trials were rated as having a low risk of bias, one had ‘some concerns’, and two were rated as high risk of bias. High-risk ratings were primarily driven by concerns about missing outcome data (attrition) and deviations from the intended intervention (e.g., poor adherence). The thirteen prospective cohort studies were generally of low-to-moderate quality. Based on the Joanna Briggs Institute (JBI) checklist, eight studies were rated as having a low risk of bias, and five were rated as having a moderate risk. The most common methodological limitation across nearly all cohorts was incomplete follow-up, with many studies not fully describing or exploring the reasons for participant attrition. Detailed domain-level judgements for all included studies are available in the Supplementary Materials (Tables S1 and S2).
4. Discussion
This systematic review synthesised evidence from six RCTs and thirteen prospective cohort studies examining the relationship between diet and adolescent mental health. Across the RCTs, the evidence was inconsistent: vitamin D supplementation showed mixed effects, a single polyphenol-rich intervention showed a benefit for depressive symptoms, whereas trials of omega-3 fatty acids yielded null findings for mood outcomes. The prospective studies, while heterogeneous, generally supported associations between healthier dietary patterns and better mental health outcomes, particularly fewer depressive symptoms. Together, these findings suggest that diet may play a meaningful role in adolescent mental health, while highlighting both the potential of nutritional approaches and the need for more rigorous, standardised research to strengthen the evidence base.
4.1. Randomised Controlled Trials
Across the six identified RCTs, the evidence for the benefits of nutrient supplementation on adolescent mental health was inconsistent. For vitamin D and polyphenols, findings were mixed, with some trials reporting a reduction in depressive symptoms. In contrast, trials of omega-3 fatty acids yielded null findings for mood outcomes. These inconsistencies reflect the small number of trials, heterogeneous methodologies, and varying outcome measures. Assessment tools ranged from validated depression scales such as the CES-D to broader instruments that included mood as a secondary component, such as the Cognitive Drug Research battery, limiting direct comparability.
Intervention modalities also varied widely, spanning vitamin D [18,19,20], omega-3s [21,22], and polyphenol-rich extracts [23]. Differences in dosage, duration, and the baseline nutrient status of participants likely contributed to the varied outcomes. A key limitation across the field was the inconsistent use of biomarkers to verify nutrient uptake. The van der Wurff et al. [21] study demonstrated the value of this approach, as its biomarker data (Omega-3 Index) revealed that the intervention’s null effect was likely due to poor participant adherence and a failure to reach target blood levels. Furthermore, while some trials had strong retention, attrition was a significant limitation in several others, with rates exceeding 20%. Sample sizes also ranged from as few as 50 participants [18] to over 450 [20], resulting in marked variation in statistical power.
In sum, most of the identified RCTs (four of six; Table 1) focused on depressive symptoms. This likely reflects the high public health burden of adolescent depression and the availability of validated measurement tools, but it means that potential links between diet and other outcomes such as anxiety, stress regulation, and behavioural problems remain comparatively underexplored. Our risk of bias assessment found two of the six trials to be at high risk of bias. Therefore, the positive findings reported in some studies should be interpreted with significant caution.
4.2. Prospective Studies
Thirteen prospective studies explored a wide range of dietary exposures and mental health outcomes. Cohorts generally supported links between healthier diets and fewer depressive symptoms, but results were inconsistent and often attenuated after adjustment for confounders. Dietary assessment tools varied, from custom-made diet quality scores [33] to narrower adolescent-focused measures like the KIDMED [25] or the Krece Plus [24]. Mental health measures were similarly diverse; for example, depression was captured by use of the BDI-Y [28] and the short form of the MFQ [30] contrasted with broader tools such as the SDQ [32] or less directly relevant scales such as self-efficacy [25].
While most studies relied on self-reported diet, an uncovered issue where some studies assessed dietary intake at only one time point [e.g., 27], limiting inference about dietary changes over time. Secondly, follow-up intervals ranged from less than a year [e.g., 27] to two years or more [e.g., 32], with mismatched timings complicating attribution. High attrition was common [e.g., 28> 50% attrition rate], reducing statistical power and risking bias. Generalisability also varied; while some cohorts were large but demographically narrow e.g., predominantly White Australian samples [33], meanwhile others focused on specific groups such as elite Swiss athletes [27], constraining applicability across broader and more general populations.
Although associations sometimes weakened after covariate adjustment [e.g., 26], the repeated observation that healthier dietary patterns predicted fewer depressive symptoms or better wellbeing across diverse cohorts [32,33,34,36] highlights a promising avenue that warrants more rigorous investigation. These studies all operationalised diet using whole-diet indices or dietary pattern approaches (e.g., Healthy/Western dietary patterns, diet quality scores, or Mediterranean diet indices), rather than single nutrient exposures. Whole-diet indices may better capture the synergistic effects of multiple nutrients and eating behaviours, helping to explain their more consistent associations compared with single nutrient measures.
4.2.1. The Influence of Sex and Socioeconomic Status (SES)
A critical finding from this review is that the relationship between diet and adolescent mental health is not uniform and is likely influenced by demographic and social factors, particularly sex and SES.
4.2.2. Sex-Specific Associations
The potential for sex-specific differences in the diet-mental health relationship is an important but underexplored theme. While many included studies did not report sex-stratified analyses or test for interactions by sex, some did explore these differences, yielding varied results. For instance, in some cohort studies, significant associations were found exclusively in females: Trapp et al. [35] found that a ‘Western’ dietary pattern prospectively predicted greater externalising behaviours only in females. Similarly, Aparicio et al. [24] reported that the link between emotional symptoms and poorer diet quality was present only in females. This suggests that adolescent girls may be more vulnerable to the mental health effects of a poor diet. However, this finding was not universal. One well-controlled study that stratified its analysis found no significant associations in either sex after full adjustment [26]. Furthermore, Dabravolskaj, Patte [36] found that the prospective association between higher sugar-sweetened beverage (SSB) consumption and greater depressive and anxiety symptoms was stronger in males. The association between fruit/vegetable intake and well-being did not significantly differ by sex in their study. Future research must prioritise testing for sex differences using interaction analyses to clarify these complex relationships.
4.2.3. Socioeconomic Status
Nearly all the prospective studies adjusted for SES, but they did so using a wide variety of measures, including parental education, household income, and area-level deprivation indices. The effect of this adjustment was not straightforward, revealing the complex role SES plays in the diet-mental health nexus. Our synthesis identified three distinct patterns: (1) Attenuation of Effects: In some of the most rigorously controlled studies, adjusting for SES and related lifestyle factors was crucial in attenuating or eliminating the prospective link between diet and mental health [26,32]. This suggests that dietary habits may be part of a broader cluster of socially patterned behaviours and that SES is a powerful confounder. (2) Strengthening or Revealing Effects: In other studies, the key findings only became statistically significant after adjusting for SES and other covariates [29,35]. This implies that SES can also supress underlying relationships, and that controlling for it is necessary to isolate the independent effect of diet. (3) Robustness to Adjustment: In many studies, the diet-mental health association remained significant even after adjusting for SES [24,25,30,31,33,34]. This provides the strongest evidence for a more direct, independent relationship between what adolescents eat and their psychological well-being. Taken together, these findings show that SES is more than just a simple variable to “control for.” Its inconsistent measurement and complex interplay with diet and mental health is a critical finding and a vital area for future research.
4.3. General Methodological Considerations
Taken together, both RCTs and prospective studies suggest that diet may influence adolescent mental health, although methodological challenges limit certainty. RCTs provide stronger causal inference, but remain few, small, and methodologically inconsistent. Prospective studies draw on larger, naturalistic cohorts yet are vulnerable to residual confounding, self-report bias, and attrition [37]. Additional heterogeneity arises from the wide range of outcome measures used. Some measures, such as the PedsQL emotional functioning scale [38] and the SDQ emotional symptoms subscale [39], capture broader emotional or internalising difficulties, while others, such as the short MFQ [40], BDI-Y [41], and CES-D [42], focus more specifically on depressive symptomatology. These differences in scope and sensitivity likely contribute to variation in observed associations [43].
A growing body of adolescent research demonstrates high symptom heterogeneity and evolving symptom architecture, with only partial cross-cultural measurement equivalence of common scales and evidence of heterotypic continuity from childhood into adolescence - features that mean diagnosis-level or composite endpoints can obscure developmentally specific patterns [44,45,46,47]. This aligns with critiques that retrospective harmonisation and top-down diagnostic taxonomies struggle against intrinsic symptom heterogeneity, incompatible instruments, and cohort biases [14,15,48]. Polythetic DSM criteria allow multiple, non-overlapping symptom constellations to share a label; sum-scores can therefore conflate opposing item-level effects. Instruments also differ in purpose and structure - PHQ-9 (DSM-aligned screener), CES-D (population surveillance), HADS-D (medical settings), HAM-D/HDRS and MADRS (clinician-rated) - and frequently show weak measurement invariance across sex, age, language, country, or time, undermining comparability. Moreover, patient-prioritised domains such as gastrointestinal distress, cognitive difficulties, mental pain, irritability, and emotion regulation are often omitted [49,50]. Therefore, to improve research on the link between nutrition and mental health in adolescents, a symptom-based, dimensional approach is essential. This strategy requires researchers to prespecify primary outcomes, report detailed subscales and key items in addition to total scores, and validate their measurement tools in the relevant population. Furthermore, it is crucial to harmonise core outcome sets across studies and align assessment choices with both the target construct and the priorities of those with lived experience. Employing these practices will reduce outcome misclassification and improve construct validity, making the associations between diet and mental health more interpretable and actionable for adolescents.
Compounding these measurement issues, most studies rely on chronological age instead of pubertal status. Puberty involves significant hormonal shifts (eg, HPG/HPA axis changes) that reshape mood regulation and increase nutrient needs. Ignoring pubertal timing risks confounding (mistaking puberty’s effects for age or diet effects) and effect modification (as diet’s impact may differ by pubertal stage and sex). Future work must measure pubertal development (eg, Tanner stage, age at menarche/voice change), incorporate this into analyses (through adjustment or stratification), report sex-specific findings, and ensure interventions meet growth-related nutrient demands. Few included studies adequately addressed pubertal status, limiting stage-specific understanding of the diet–mental health link
Despite these limitations, a recurring pattern emerges - whole-diet quality and pattern adherence are more consistently associated with favourable adolescent mental-health outcomes than isolated nutrient supplementation. This likely reflects several factors. Mental-health effects may arise from non-additive interactions among co-consumed foods and nutrients; in the future network approaches (e.g., Gaussian graphical, mutual-information, mixed graphical models) may reveal protective synergies and disruptive clusters that single-nutrient models or simple scores may miss, and recent guidance (Minimal Reporting Standard for Dietary Networks (MRS-DN)) sets reporting standards to improve rigour and comparability [51]. Biologically dietary patterns embody synergistic constellations of foods and nutrients - fibre, polyphenols, unsaturated fats, vitamins, and minerals - that co-modulate interconnected pathways (inflammation, glycaemic/insulin homeostasis, gut–microbiome–brain signalling, neurotrophic support) in a coordinated manner, offering greater biological plausibility than single-nutrient effects [52]. Methodologically, pattern/quality indices implicitly capture the food matrix and its “nutritional dark matter” - the millions of unmeasured bioactives and interactions present in whole foods that single-nutrient studies cannot - while also reducing noise from correlated intakes and self-report error, yielding more stable associations across instruments and samples [51]. Notably, advances in untargeted metabolomics and foodomics are revealing new nutrient candidates with potential mental-health relevance - for example, vitamin A5/X (a vegetable- and algae-derived precursor pool for the RXR ligand 9-cis-13,14-dihydroretinoic acid) [53] - further strengthening the rationale for pattern-level approaches.
Beyond methodological considerations, several interpretive insights are noteworthy. Firstly, adolescence may represent a uniquely sensitive period, given rapid brain maturation and developmental transitions that heighten responsiveness to environmental influences [54]. Secondly, the predominance of depressive-symptom outcomes partly reflects the availability of validated tools but may also indicate that depression is particularly nutrition-sensitive in this developmental stage [55]. Thirdly, the weakening of associations after adjustment for covariates indicates that diet is likely embedded within a broader constellation of lifestyle factors rather than acting in isolation [56]. Finally, even modest dietary effects may be meaningful from a public-health perspective, because adolescence is a critical window for the emergence of mental disorders; small improvements in diet at the population level could translate into substantial gains in wellbeing [57], few studies have simultaneously integrated biological and psychological domains; there is a clear need to identify and validate nutrition-linked biomarkers and correlates of mental health (e.g., inflammatory profiles, glycaemic control, lipid and micronutrient status, microbiome-derived metabolites, and neurotrophic indices, heart rate variability, sleep and other interoceptive indices) [58,59,60] alongside symptom-level outcomes, using longitudinal, multi-informant designs to strengthen inference and translational relevance. A concise roadmap translating these priorities into study designs, measures, biomarkers, and implementation steps is provided in Table 3 (Roadmap for future directions in adolescent nutrition–mental health research).
4.4. Limitations and Recommendations
Several limitations warrant consideration, with corresponding recommendations summarised in Table 3. First, applying the WHO definition of adolescence (10–19 years) spans a dynamic developmental period with marked physical, cognitive, and psychosocial change [54]. Such differences may shape responsiveness to dietary exposures. Future work should stratify analyses by developmental stage and employ repeated assessments across adolescence to identify windows of heightened vulnerability or resilience in the diet–mental health relationship.
Second, measurement lacks standardisation. Mental-health outcomes have been captured with a wide range of tools - from broader scales such as the SDQ to more targeted measures (e.g., MFQ, BDI-Y, RADS), with occasional use of constructs less directly aligned to clinical symptoms [e.g., self-efficacy; 25]. Dietary exposures likewise vary, from general diet-quality indices based on national guidelines [33] to adolescent-specific measures such as KIDMED and Krece Plus [25]. Greater use of validated, developmentally appropriate tools - and clearer reporting of their comparability - would improve synthesis and interpretation.
Third, the literature remains dominated by depression outcomes, leaving anxiety, stress, externalising behaviours, self-esteem, and aggression comparatively underexplored. Expanding outcome scope and incorporating biomarkers (e.g., inflammatory profiles, glycaemic regulation, micronutrient status, microbiome-derived metabolites, neurotrophic indices) and repeated dietary assessments to complement self-report would strengthen robustness and comparability. Longer follow-up, more frequent measurement, and advanced longitudinal models (e.g., cross-lagged, structural equation modelling) are needed to clarify causal and bidirectional pathways. Furthermore, the certainty of existing evidence is weakened by key methodological issues. As noted in our risk of bias assessment, incomplete follow-up was a near-universal issue across the cohort studies, increasing the risk of attrition bias and limiting the generalisability of the findings.
Finally, unmeasured contextual factors may contribute to observed associations. Few studies adequately considered parental mental health, family dietary culture, or psychosocial stressors, despite their likely influence on both diet and mental health [61]. More diverse, representative adolescent samples are needed, moving beyond homogeneous or niche groups to include under-resourced and high-risk populations. Quasi-experimental approaches (e.g., school- or community-based interventions) can complement RCTs by enhancing external validity and implementation insight; school-based studies have also demonstrated excellent retention, supporting feasibility for adolescent research [22].
Addressing these methodological, conceptual, and developmental gaps would strengthen the evidence base, support more targeted interventions, and enhance translation to clinical and public-health practice [62]. A major strength of the present review is that it did not confine outcomes to diagnostic categories or composite totals; by synthesising evidence across dimensional symptom domains (e.g., depressive and anxiety symptoms, wellbeing, internalising/externalising), it offers a developmentally sensitive appraisal that is more faithful to adolescent mental-health heterogeneity and more actionable for prevention and intervention.
5. Conclusions
Current evidence suggests that adolescent diet is relevant to mental health, albeit with certainty constrained by methodological inconsistency. Across randomised trials and prospective cohorts, associations are more consistently observed for whole-diet quality and pattern adherence than for isolated nutrient supplementation, a pattern that is biologically plausible and consonant with real-world eating behaviours. Whole diet approaches therefore appear particularly promising for prevention and intervention, though both strategies warrant more rigorous testing.
Progress will depend on methodological standardisation (aligned, developmentally appropriate outcome measures; harmonised diet indices), explicit consideration of how associations differ by sex and socioeconomic status (SES), larger and more diverse samples, and repeated assessments across developmental stages to clarify timing and directionality. Integrating mechanistic perspectives - including inflammatory signalling, glycaemic regulation, gut–brain pathways, micronutrient status, and psychosocial contexts such as family mealtime practices - alongside validated biomarkers will strengthen causal inference. Finally, adopting symptom-based, dimensional outcomes (rather than restricting inference to diagnostic composites) will improve construct validity and translational relevance. Addressing these gaps can move the field from tentative associations toward actionable, nutrition-informed strategies that support adolescent mental health. A phased research agenda to deliver these advances is set out in Table 3.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, H.Y.; methodology, J.T. and H.Y.; software, J.T.; validation, A.B., H.Y. and J.T.; formal analysis, J.T.; investigation, J.T. and H.Y.; resources, J.T. and H.Y.; data curation, J.T.; writing—original draft preparation, J.T.; writing—review and editing, D.B., A.B.; visualization, J.T. and A.B.; supervision, H.Y.; project administration, H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
H.Y. received support for this work via grant IAFNS-SWANSEAU-20230111 from the Institute for the Advancement of Food and Nutrition Sciences (IAFNS). Other authors received no funding. IAFNS is a nonprofit science organization that pools funding from industry and advances science through the in-kind and financial contributions from private and public sector members.
Data Availability Statement
Data are available at available at https://osf.io/c6xze.
Acknowledgments
We would like to thank Swansea University for supporting this research.
Conflicts of Interest
H.Y. has served as a scientific advisor to the Cognitive Health Committee at the Institute for the Advancement of Food and Nutrition Sciences (IAFNS) since 2020; financial support for this work was provided by IAFNS to Swansea University. In the last three years, H.Y. has also received research funding, in-kind support, and/or consultancy, travel, or speaker fees from Beneo GmbH, Mars-Wrigley, GSK, the European Fruit Juice Association, and Wileys. The remaining authors declare no conflicts of interest.
References
- Dimov, S.; Mundy, L.K.; Bayer, J.K.; Jacka, F.N.; Canterford, L.; Patton, G.C. Diet quality and mental health problems in late childhood. Nutr. Neurosci. 2019, 24, 62–70. [CrossRef]
- Orlando, L.; A Savel, K.; Madigan, S.; Colasanto, M.; Korczak, D.J. Dietary patterns and internalizing symptoms in children and adolescents: A meta-analysis. Aust. New Zealand J. Psychiatry 2021, 56, 617–641. [CrossRef]
- Wickersham, A.; Sugg, H.V.; Epstein, S.; Stewart, R.; Ford, T.; Downs, J. Systematic Review and Meta-analysis: The Association Between Child and Adolescent Depression and Later Educational Attainment. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 105–118. [CrossRef]
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Üstün, T.B. Age of onset of mental disorders: a review of recent literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [CrossRef]
- Copeland, W.E., et al., Adult functional outcomes of common childhood psychiatric problems: a prospective, longitudinal study. JAMA psychiatry, 2015. 72(9): p. 892-899.
- Kazdin, A.E.; Rabbitt, S.M. Novel Models for Delivering Mental Health Services and Reducing the Burdens of Mental Illness. Clin. Psychol. Sci. 2013, 1, 170–191. [CrossRef]
- Benton, D. The influence of dietary status on the cognitive performance of children. Mol. Nutr. Food Res. 2010, 54, 457–470. [CrossRef]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [CrossRef]
- O’Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship Between Diet and Mental Health in Children and Adolescents: A Systematic Review. Am. J. Public Health 2014, 104, e31–e42. [CrossRef]
- Lassale, C.; Batty, G.D.; Baghdadli, A.; Jacka, F.; Sánchez-Villegas, A.; Kivimäki, M.; Akbaraly, T. Healthy dietary indices and risk of depressive outcomes: a systematic review and meta-analysis of observational studies. Mol. Psychiatry 2019, 24, 965–986. [CrossRef]
- Lane, M.M.; Gamage, E.; Travica, N.; Dissanayaka, T.; Ashtree, D.N.; Gauci, S.; Lotfaliany, M.; O’neil, A.; Jacka, F.N.; Marx, W. Ultra-Processed Food Consumption and Mental Health: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2022, 14, 2568. [CrossRef]
- Pruneti, C.; Guidotti, S. Need for Multidimensional and Multidisciplinary Management of Depressed Preadolescents and Adolescents: A Review of Randomized Controlled Trials on Oral Supplementations (Omega-3, Fish Oil, Vitamin D3). Nutrients 2023, 15, 2306. [CrossRef]
- da Silva, L.E.M., et al., Dietary Pattern and Depressive Outcomes in Children and Adolescents: Systematic Review and Meta-analysis of Observational Studies. Nutr Rev, 2025. 83(9): p. 1725-1742.
- Fried, E.I. The 52 symptoms of major depression: Lack of content overlap among seven common depression scales. J. Affect. Disord. 2017, 208, 191–197. [CrossRef]
- Fried, E.I.; Flake, J.K.; Robinaugh, D.J. Revisiting the theoretical and methodological foundations of depression measurement. Nat. Rev. Psychol. 2022, 1, 358–368. [CrossRef]
- Page, M.J., et al., The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Revista panamericana de salud pública, 2022. 46.
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [CrossRef]
- Grung, B.; Sandvik, A.M.; Hjelle, K.; Dahl, L.; Frøyland, L.; Nygård, I.; Hansen, A.L. Linking vitamin D status, executive functioning and self-perceived mental health in adolescents through multivariate analysis: A randomized double-blind placebo control trial. Scand. J. Psychol. 2017, 58, 123–130. [CrossRef]
- Isaac, H.A.; Hemamalini, A.J.; Seshadri, K.; Ravichandran, L. Impact of vitamin D fortified food on quality of life and emotional difficulties among adolescents – A randomized controlled trial. Indian J. Child Heal. 2019, 6, 56–60. [CrossRef]
- Satyanarayana, P.T.; Suryanarayana, R.; Ty, S.; Reddy, S.; Ag, N. Does Vitamin D3 Supplementation Improve Depression Scores among Rural Adolescents? A Randomized Controlled Trial. Nutrients, 2024. 16(12): p. 1828.
- van der Wurff, I.; von Schacky, C.; Bergeland, T.; Leontjevas, R.; Zeegers, M.; Kirschner, P.; de Groot, R. Effect of one year krill oil supplementation on depressive symptoms and self-esteem of Dutch adolescents: A randomized controlled trial. Prostaglandins, Leukot. Essent. Fat. Acids 2020, 163, 102208. [CrossRef]
- Kennedy, D.O.; Jackson, P.A.; Elliott, J.M.; Scholey, A.B.; Robertson, B.C.; Greer, J.; Tiplady, B.; Buchanan, T.; Haskell, C.F. Cognitive and mood effects of 8 weeks' supplementation with 400 mg or 1000 mg of the omega-3 essential fatty acid docosahexaenoic acid (DHA) in healthy children aged 10–12 years. Nutr. Neurosci. 2009, 12, 48–56. [CrossRef]
- Fisk, J.; Khalid, S.; Reynolds, S.A.; Williams, C.M. Effect of 4 weeks daily wild blueberry supplementation on symptoms of depression in adolescents. Br. J. Nutr. 2020, 124, 181–188. [CrossRef]
- Aparicio, E.; Canals, J.; Voltas, N.; Valenzano, A.; Arija, V. Emotional Symptoms and Dietary Patterns in Early Adolescence: A School-Based Follow-up Study. J. Nutr. Educ. Behav. 2017, 49, 405–414.e1. [CrossRef]
- Hayek, J.; de Vries, H.; Tueni, M.; Lahoud, N.; Winkens, B.; Schneider, F. Increased Adherence to the Mediterranean Diet and Higher Efficacy Beliefs Are Associated with Better Academic Achievement: A Longitudinal Study of High School Adolescents in Lebanon. Int. J. Environ. Res. Public Heal. 2021, 18, 6928. [CrossRef]
- Winpenny, E.M.; van Harmelen, A.-L.; White, M.; van Sluijs, E.M.; Goodyer, I.M. Diet quality and depressive symptoms in adolescence: no cross-sectional or prospective associations following adjustment for covariates. Public Health Nutr 2018, 21, 2376–2384. [CrossRef]
- Gerber, M.; Jakowski, S.; Kellmann, M.; Cody, R.; Gygax, B.; Ludyga, S.; Müller, C.; Ramseyer, S.; Beckmann, J. Macronutrient intake as a prospective predictor of depressive symptom severity: An exploratory study with adolescent elite athletes. Psychol. Sport Exerc. 2023, 67. [CrossRef]
- Swann, O.G.; Breslin, M.; Kilpatrick, M.; O’sullivan, T.A.; Mori, T.A.; Beilin, L.J.; Lin, A.; Oddy, W.H. Dietary fibre intake and its associations with depressive symptoms in a prospective adolescent cohort. Br. J. Nutr. 2020, 125, 1166–1176. [CrossRef]
- Black, L.J.; Allen, K.L.; Jacoby, P.; Trapp, G.S.; Gallagher, C.M.; Byrne, S.M.; Oddy, W.H. Low dietary intake of magnesium is associated with increased externalising behaviours in adolescents. Public Health Nutr 2014, 18, 1824–1830. [CrossRef]
- Tolppanen, A.M., et al., The association of serum 25-hydroxyvitamin D 3 and D 2 with depressive symptoms in childhood – a prospective cohort study. Journal of child psychology and psychiatry, 2012. 53(7): p. 757-766.
- Mrug, S.; Jones, L.C.; Elliott, M.N.; Tortolero, S.R.; Peskin, M.F.; Schuster, M.A. Soft Drink Consumption and Mental Health in Adolescents: A Longitudinal Examination. J. Adolesc. Heal. 2021, 68, 155–160. [CrossRef]
- Jacka, F.N.; Rothon, C.; Taylor, S.; Berk, M.; Stansfeld, S.A. Diet quality and mental health problems in adolescents from East London: a prospective study. Chest 2012, 48, 1297–1306. [CrossRef]
- Jacka, F.N.; Kremer, P.J.; Berk, M.; De Silva-Sanigorski, A.M.; Moodie, M.; Leslie, E.R.; Pasco, J.A.; Swinburn, B.A. A Prospective Study of Diet Quality and Mental Health in Adolescents. PLOS ONE 2011, 6, e24805. [CrossRef]
- Oddy, W.H.; Allen, K.L.; Trapp, G.S.; Ambrosini, G.L.; Black, L.J.; Huang, R.-C.; Rzehak, P.; Runions, K.C.; Pan, F.; Beilin, L.J.; et al. Dietary patterns, body mass index and inflammation: Pathways to depression and mental health problems in adolescents. Brain, Behav. Immun. 2018, 69, 428–439. [CrossRef]
- Trapp, G.S.A.; Allen, K.L.; Black, L.J.; Ambrosini, G.L.; Jacoby, P.; Byrne, S.; Martin, K.E.; Oddy, W.H. A prospective investigation of dietary patterns and internalizing and externalizing mental health problems in adolescents. Food Sci. Nutr. 2016, 4, 888–896. [CrossRef]
- Dabravolskaj, J.; Patte, K.A.; Yamamoto, S.; Leatherdale, S.T.; Veugelers, P.J.; Maximova, K. Association Between Diet and Mental Health Outcomes in a Sample of 13,887 Adolescents in Canada. Prev. Chronic Dis. 2024, 21, E82. [CrossRef]
- Howe, L.D., et al., Loss to follow-up in cohort studies: bias in estimates of socioeconomic inequalities. Epidemiology, 2013. 24(1): p. 1-9.
- Varni, J.W., M. Seid, and P.S. Kurtin, PedsQL™ 4.0: Reliability and validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in healthy and patient populations. Medical care, 2001. 39(8): p. 800-812.
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [CrossRef]
- Angold, A., et al., Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents: factor composition and structure across development. International journal of methods in psychiatric research, 1996. 5(4): p. 251-262.
- Beck, J.S., Beck youth inventories of emotional & social impairment: Depression inventory for youth, anxiety inventory for youth, anger inventory for youth, disruptive behavior inventory for youth, self-concept inventory for youth: Manual. 2001: Psychological Corporation New York, NY, USA.
- Radloff, L.S., A self-report depression scale for research in the general population. Applied psychol Measurements, 1977. 1: p. 385-401.
- Beck, A.; Dryburgh, N.; Bennett, A.; Shaver, N.; Esmaeilisaraji, L.; Skidmore, B.; Patten, S.; Bragg, H.; Colman, I.; Goldfield, G.S.; et al. Screening for depression in children and adolescents in primary care or non-mental health settings: a systematic review update. Syst. Rev. 2024, 13, 1–15. [CrossRef]
- Mullarkey, M.C.; Marchetti, I.; Bluth, K.; Carlson, C.L.; Shumake, J.; Beevers, C.G. Symptom centrality and infrequency of endorsement identify adolescent depression symptoms more strongly associated with life satisfaction. J. Affect. Disord. 2021, 289, 90–97. [CrossRef]
- Mullarkey, M.C.; Marchetti, I.; Beevers, C.G. Using Network Analysis to Identify Central Symptoms of Adolescent Depression. J. Clin. Child Adolesc. Psychol. 2018, 48, 656–668. [CrossRef]
- Stevanovic, D.; Jafari, P.; Knez, R.; Franic, T.; Atilola, O.; Davidovic, N.; Bagheri, Z.; Lakic, A. Can we really use available scales for child and adolescent psychopathology across cultures? A systematic review of cross-cultural measurement invariance data. Transcult. Psychiatry 2017, 54, 125–152. [CrossRef]
- Duinhof, E.L.; Stevens, G.W.J.M.; van Dorsselaer, S.; Monshouwer, K.; Vollebergh, W.A.M. Ten-year trends in adolescents’ self-reported emotional and behavioral problems in the Netherlands. Eur. Child Adolesc. Psychiatry 2014, 24, 1119–1128. [CrossRef]
- Fried, E.I.; Papanikolaou, F.; Epskamp, S. Mental Health and Social Contact During the COVID-19 Pandemic: An Ecological Momentary Assessment Study. Clin. Psychol. Sci. 2021, 10, 340–354. [CrossRef]
- Young, H.A.; Cousins, A.L.; Byrd-Bredbenner, C.; Benton, D.; Gershon, R.C.; Ghirardelli, A.; Latulippe, M.E.; Scholey, A.; Wagstaff, L. Alignment of Consumers’ Expected Brain Benefits from Food and Supplements with Measurable Cognitive Performance Tests. Nutrients 2024, 16, 1950. [CrossRef]
- Veal, C.; Tomlinson, A.; Cipriani, A.; Bulteau, S.; Henry, C.; Müh, C.; Touboul, S.; De Waal, N.; Levy-Soussan, H.; A Furukawa, T.; et al. Heterogeneity of outcome measures in depression trials and the relevance of the content of outcome measures to patients: a systematic review. Lancet Psychiatry 2024, 11, 285–294. [CrossRef]
- Taylor, R.M.J.; Moore, J.A.; Griffiths, A.R.; Cousins, A.L.; Young, H.A. Unveiling Dietary Complexity: A Scoping Review and Reporting Guidance for Network Analysis in Dietary Pattern Research. Nutrients 2025, 17, 3261. [CrossRef]
- A Young, H.; Geurts, L.; Scarmeas, N.; Benton, D.; Brennan, L.; Farrimond, J.; Kiliaan, A.J.; Pooler, A.; Trovò, L.; Sijben, J.; et al. Multi-nutrient interventions and cognitive ageing: are we barking up the right tree?. Nutr. Res. Rev. 2022, 36, 471–483. [CrossRef]
- Bánáti, D.; Hellman-Regen, J.; Mack, I.; Young, H.A.; Benton, D.; Eggersdorfer, M.; Rohn, S.; Dulińska-Litewka, J.; Krężel, W.; Rühl, R. Defining a vitamin A5/X specific deficiency – vitamin A5/X as a critical dietary factor for mental health. Int. J. Vitam. Nutr. Res. 2024, 94, 443–475. [CrossRef]
- Laube, C.; Bos, W.v.D.; Fandakova, Y. The relationship between pubertal hormones and brain plasticity: Implications for cognitive training in adolescence. Dev. Cogn. Neurosci. 2020, 42, 100753. [CrossRef]
- Opie, R.S.; O’neil, A.; Itsiopoulos, C.; Jacka, F.N. The impact of whole-of-diet interventions on depression and anxiety: a systematic review of randomised controlled trials. Public Health Nutr 2015, 18, 2074–2093. [CrossRef]
- Benton, D.; Young, H.A. Early exposure to sugar sweetened beverages or fruit juice differentially influences adult adiposity. Eur. J. Clin. Nutr. 2024, 78, 521–526. [CrossRef]
- Jacka, F. N.; O'Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M. L. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’trial). BMC Med. 2017, 15, 23.
- Young, H.A.; Benton, D. Heart-rate variability: a biomarker to study the influence of nutrition on physiological and psychological health?. Behav. Pharmacol. 2018, 29, 140–151. [CrossRef]
- A Young, H.; Freegard, G.; Benton, D. Mediterranean diet, interoception and mental health: Is it time to look beyond the ‘Gut-brain axis’?. Physiol. Behav. 2022, 257, 113964. [CrossRef]
- Gaylor, C.M.; Brennan, A.; Blagrove, M.; Tulip, C.; Bloxham, A.; Williams, S.; Tucker, R.; Benton, D.; Young, H.A. Low and high glycemic index drinks differentially affect sleep polysomnography and memory consolidation: A randomized controlled trial. Nutr. Res. 2025, 134, 49–59. [CrossRef]
- Sparling, T.M.; Deeney, M.; Cheng, B.; Han, X.; Lier, C.; Lin, Z.; Offner, C.; Santoso, M.V.; Pfeiffer, E.; Emerson, J.A.; et al. Systematic evidence and gap map of research linking food security and nutrition to mental health. Nat. Commun. 2022, 13, 1–11. [CrossRef]
- Romijn, A.R.; Latulippe, M.E.; Snetselaar, L.; Willatts, P.; Melanson, L.; Gershon, R.; Tangney, C.; Young, H.A. Perspective: Advancing Dietary Guidance for Cognitive Health—Focus On Solutions to Harmonize Test Selection, Implementation, and Evaluation. Adv. Nutr. Int. Rev. J. 2023, 14, 366–378. [CrossRef]

Table 1.
Characteristics and Key Findings of Included Randomized Controlled Trials.
| Author (year) | Country | Sub-Category | Dose & Duration | Sample Size (N) | Sample Characteristics | Measures | Sex-Specific Analysis? | SES/Deprivation Adjusted? | Key Findings | Biomarker Verified? |
| Fisk et al. (2020) | UK | Polyphenols | ~253 mg anthocyanins/day for 4 weeks | 64 | 12–17 y, Mixed sex | MFQ, RCADS, PANAS | No | NR | ↓ Depressive symptoms NS Anxiety & Affect |
No |
| Grung et al. (2017) | Norway | Vitamin D | 1,520 IU/day for ~3 months | 50 | 13–14 y, Mixed sex | YSR-CBCL, ToH, ToL | No | NR | NS Internalising/Externalising ↑ Executive function (ToH) |
Yes (25(OH)D) |
| Isaac et al. (2019) | India | Vitamin D | 1,000 IU/day for 12 weeks | 71 | 11–16 y, Mixed sex, Vit D deficient | WHOQOL-BREF, DASS-21 | No | NR | NS Quality of Life NS Anxiety/Stress |
Yes (25(OH)D) |
| Kennedy et al. (2009) | UK | Omega-3 | 400 or 1,000 mg/day (DHA) for 8 weeks | 90 | 10–12 y, Healthy, Mixed sex | CDR battery, VAS mood | No | NR | NS Mood & Cognition | No |
| Satyanarayana et al. (2024) | India | Vitamin D | ~2,250 IU/day for 9 weeks | 451 | 14–19 y, Rural, Mixed sex | BDI-II | No | NR | ↓ Depressive symptoms | Yes (25(OH)D) |
| van der Wurff et al. (2020) | Netherlands | Omega-3 | 400→800 mg/day (EPA+DHA) for 12 months | 256 | 14–15 y, Low O3I, Mixed sex | CES-D, RSE | No | Yes (parental education). Did not affect results. | NS Depressive symptoms NS Self-esteem |
Yes (O3I) |
BDI-II: Beck Depression Inventory-II; BPAQ: Buss-Perry Aggression Questionnaire; CDR: Cognitive Drug Research; CES-D: Center for Epidemiologic Studies Depression Scale; DASS-21: Depression, Anxiety and Stress Scales-21; DHA: Docosahexaenoic acid; EPA: Eicosapentaenoic acid; IU: International Unit; MFQ: Mood and Feelings Questionnaire; NR: Not Reported; NS: Not Significant; O3I: Omega-3 Index; PANAS: Positive and Negative Affect Schedule; RCADS: Revised Child Anxiety and Depression Scale; RSE: Rosenberg Self-Esteem Scale; ToH: Tower of Hanoi; ToL: Tower of London; VAS: Visual Analogue Scale; Vit D: Vitamin D; WHOQOL-BREF: World Health Organization Quality of Life-BREF; y: years; YSR-CBCL: Youth Self-Report-Child Behavior Checklist; 25(OH)D: 25-hydroxyvitamin D.
Table 2.
Characteristics and Key Findings of Included Prospective Studies.
| Aparicio et al. (2017) | Spain | Mediterranean Diet | MD adherence & patterns; 3-year follow-up | 165 | ~13.5 y, School cohort | SCARED, CDI, YI-4 | Yes. Emotional symptoms linked to poorer diet in females only. | Yes (Hollingshead index). Association remained significant after adjustment; SES was also a predictor. | ↑ Emotional symptoms → ↓ MD adherence (Females only, reverse causality tested) |
| Author (year) | Country | Sub-Category | Dietary Exposure & Follow-up | Sample Size (N) | Sample Characteristics | Measures | Sex-Specific Analysis? | SES/Deprivation Adjusted? | Key Findings |
| Black et al. (2015) | Australia | Micronutrients | Zinc & Magnesium intake; 3-year follow-up | 684 | 14 & 17 y, General pop. | YSR | No (Interactions tested, NS). | Yes (Family income). Association was significant only after adjustment. | ↑ Magnesium → ↓ Externalising problems |
| Dabravolskaj et al. (2024) | Canada | Overall Diet Quality | Frequency of fruit/veg, SSB, junk food, breakfast intake; 1-year follow-up | 13,887 | Adolescents (grades 9–12); mean age 15 y; 52% female; general pop. | “Diet: COMPASS survey items | Yes. SSB associations stronger in males. | Yes (Adjusted for weekly spending money, plus lifestyle & psychosocial factors). | ↑ SSB intake → ↑ Depressive (β=0.04) & Anxiety symptoms (β=0.02), ↓ Well-being (β=-0.03). ↑ F&V intake → ↑ Well-being (β=0.06), NS Depressive/Anxiety symptoms (after full adjustment) |
| Gerber et al. (2023) | Switzerland | Macronutrients | Protein intake from food recall; 10-month follow-up | 79 | ~16.4 y, Elite athletes | PHQ-9 | No. | No. (Measured but excluded from the final model as it was not a significant predictor). | ↑ Protein → ↓ Depressive symptoms |
| Hayek et al. (2021) | Lebanon | Mediterranean Diet | MD adherence (KIDMED); 1-year follow-up | 563 | 15–18 y, School cohort | Academic Grade | No. | Yes (Parental education). Association remained significant after adjustment. | ↑ MD Adherence → ↑ Academic Achievement (Not MH symptoms) |
| Jacka (2013) | UK | Overall Diet Quality | Healthy vs. unhealthy diet; 2-year follow-up | 2,383 | 11–14 y, Socially deprived | SDQ, SMFQ | No (Interactions tested, NS). | Yes (e.g., free school meals). Overall adjustment attenuated the prospective link. | ↑ Unhealthy diet → ↑ MH problems (effect attenuated after full adjustment) |
| Jacka et al. (2011) | Australia | Overall Diet Quality | Healthful vs. unhealthful patterns; 2-year follow-up | 2,915 | 11–18 y, General pop. | PedsQL | No (Interactions tested, NS). | Yes (SEIFA area index). Associations remained significant after adjustment. | ↑ Healthy diet → ↑ Emotional functioning ↑ Unhealthy diet → ↓ Emotional functioning |
| Mrug et al. (2021) | USA | Soft Drinks | Soft drink frequency; 5-year follow-up (3 waves) | 5,147 | 11, 13 & 16 y, Diverse pop. | Aggression/Depression Scales | No. | Yes (Education & income). Associations remained significant after adjustment. | ↑ Soft Drinks → ↑ Aggression (bidirectional link found) |
| Oddy et al. (2018) | Australia | Overall Diet Quality | Western’ vs. ‘Healthy’ patterns; 3-year follow-up | 843 | 14 & 17 y, General pop. | BDI-Y, YSR | No (Interactions tested, NS). | Yes (Income & education). Associations remained significant after adjustment. | ↑ Western diet → ↑ Depressive symptoms & MH problems (mediated by inflammation) |
| Swann et al. (2021) | Australia | Macronutrients | Dietary fibre intake; 3-year follow-up | 1260 | 14 & 17 y, General pop. | BDI-Y | No (Interactions tested, NS). | Yes (Education & income). Association was significant after SES adjustment but was attenuated by overall dietary pattern. | ↑ Fibre → ↓ Depressive symptoms (attenuated by overall diet quality) |
| Tolppanen et al. (2012) | UK | Micronutrients | Serum Vitamin D₃ (biomarker); ~4-year follow-up | 2,752 | ~10 to ~14 y, General pop. | MFQ | No (Interactions tested, NS). | Yes (Occupation & education). Associations remained significant after adjustment. | ↑ Vitamin D₃ → ↓ Depressive symptoms |
| Trapp et al. (2016) | Australia | Overall Diet Quality | Healthy’ vs. ‘Western’ patterns; 3-year follow-up | 746 | 14 & 17 y, General pop. | YSR | Yes. Link between ‘Western’ diet & externalising found in females only. | Yes (Income & education). Association was significant only after full adjustment. | ↑ Western diet → ↑ Externalising problems (Females only) |
| Winpenny et al. (2018) | UK | Mediterranean Diet | MD score from diet diary; 3-year follow-up | 603 | 14.5 & 17.5 y, General pop. | MFQ | Yes. Stratified analysis; no significant associations found in either sex. | Yes (Postcode index). Associations became non-significant after full adjustment. | NS MD Adherence → Depressive symptoms (after full adjustment) |
BDI-Y: Beck Depression Inventory for Youth; CDI: Children’s Depression Inventory; KIDMED: Mediterranean Diet Quality Index (for children and adolescents); MD: Mediterranean Diet; MFQ: Mood and Feelings Questionnaire; MH: Mental Health; NS: Not Significant; PedsQL: Pediatric Quality of Life Inventory; PHQ-9: Patient Health Questionnaire-9; SCARED: Screen for Child Anxiety Related Disorders; SDQ: Strengths and Difficulties Questionnaire; SEIFA: Socio-Economic Indexes for Areas; SES: Socioeconomic Status; SMFQ: Short Mood and Feelings Questionnaire; y: years; YI-4: Youth Inventory-4; YSR: Youth Self-Report.
Table 3.
Roadmap for future directions in adolescent nutrition–mental health research.
| Priority area | Significance | Design implications | Measurement & biomarkers | Equity & implementation | Example research question |
| Symptom-based outcomes (beyond diagnoses) | Captures heterogeneity; avoids masking effects in composite totals | Pre-specify primary symptom domains; analyse subscales/items alongside total using appropriate statistical methods | Check that measures work the same across groups (measurement invariance); use multiple informants (young person, parent/carer, teacher, clinician) | Use culturally adapted, validated tools developed with young people | Does improving diet quality reduce anhedonia or irritability specifically in adolescents? |
| Harmonised core outcome sets | Enables synthesis and comparison across studies | Build a consensus minimal set via Delphi with youth, carers, clinicians, educators to measure priority outcomes | Map existing tools to prioritised outcomes; Determine which priority outcomes lack adequate, validated measurement tools.; Develop and validate measures specifically designed to fill those identified gaps. | Co-produce outcomes that matter in schools, clinics and everyday life. | What minimal battery best balances burden and validity across settings? |
| Better exposure assessment | Reduces misclassification of diet | Combine repeated 24-hour recalls/diaries with food-frequency tools; include calibration subsamples | Add objective markers: vitamin D (25-hydroxyvitamin D), omega-3 index, carotenoids; digital capture (meal photos, receipts) | Choose methods feasible in low-resource schools/ communities | How do repeated objective diet measures change effect estimates versus food-frequency tools alone? |
| Biomarker-informed trials | Strengthens causal inference | Target adolescents with low baseline status; stratify randomisation; ensure adequate duration and contrast | Verify exposure change (e.g., vitamin D and omega-3 indices); include inflammation, glycaemic control, neurotrophic factors, microbiome/metabolites | Low-burden sampling (dried blood spots; postal stool kits) | Do adolescents with low vitamin D show greater mood benefit from diet improvement than replete peers? |
| Dietary network methods (MRS-DN) | Tests synergy rather than single nutrients | Pre-register network models; compare with traditional indices | Report estimation, stability, and sensitivity per the checklist | Build analyst capacity; share code and data | Which food–nutrient constellations most robustly predict symptom improvement? |
| Longitudinal causal modelling | Clarifies direction of effects | Use within-person change or cross-lagged models; emulate target trials when randomisation is infeasibleᶜ | Align timing of diet and outcome waves | Plan for retention; minimise burden | Do changes in sugar-sweetened drink intake precede changes in externalising behaviours within individuals? |
| Mechanistic integration | Links biology to symptoms | Embed mechanistic sub-studies in trials and cohorts | Panels for inflammation, glycaemic control, lipidomics, metabolomics, microbiome, neurotrophic markers | Use affordable, standardised panels; control for batch effects | Are mood benefits mediated by reductions in systemic inflammation? |
| Early-life to adolescence | Tests timing and sensitive periods | Link infancy diet to adolescent outcomes with repeated measures | Include stable markers (e.g., ferritin), growth, and diet trajectories | Maintain diverse cohorts; consider attrition bias | Do infancy diet trajectories interact with adolescent diet to influence mood? |
| Multi-level context | Accounts for confounding and leverage points | Measure family, school, neighbourhood food environments | Include mealtime practices, food insecurity, marketing exposure | Oversample under-resourced and high-risk groups | Does family meal frequency change the effect of diet quality on anxiety? |
| Sex & Gender Analysis | Addresses findings that diet-mental health links may be stronger or exclusive to females; clarifies vulnerability. | Power studies adequately to test for sex/gender interactions; pre-specify stratified analyses rather than adding them post-hoc. | Collect data on sex assigned at birth and gender identity; consider hormonal status/pubertal stage as a potential moderator. | Ensure interventions and recommendations are relevant and communicated effectively to adolescents of all genders. | Is the prospective link between a ‘Western’ diet and externalising behaviours stronger in adolescent girls than in boys? |
| Socioeconomic & Environmental Context | Disentangles the independent effect of diet from the powerful confounding effects of deprivation, stress, and food insecurity. | Use robust, multi-domain SES measures (parental income, education, area-level deprivation); measure the food environment (e.g., food deserts). | Validated SES indices (e.g., SEIFA); household food insecurity scales; geospatial data on local food outlets. | Oversample low-SES and high-risk groups; co-design interventions that are affordable, accessible, and culturally appropriate. | Does the effect of a healthy diet on depressive symptoms persist after fully accounting for family income and food insecurity? |
| Implementation and scale-up | Ensures real-world impact | Hybrid effectiveness-implementation designs | Track fidelity, reach, cost, acceptability, and equity metrics | Co-design with schools and commissioners | What is the cost per meaningful gain in wellbeing for a school diet programme? |
| Open science and standardisation | Improves trust and synthesis | Register protocols; share data and code; use reporting checklists | Common data dictionaries; transparent preprocessing | Capacity building and training | Does pre-registration reduce outcome-reporting bias in diet–mental health trials? |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



