
Submitted:
29 October 2025
Posted:
30 October 2025
You are already at the latest version
Abstract
Invasive fungal disease (IFD) is one of the leading causes of morbidity and mortality in immunocompromised pediatric patients. This is a multicenter prospective cohort study with a nested retrospective analysis aimed to identify risk factors for IFD in immunocompromised children with cancer and episodes of persistent high-risk febrile neutropenia (HRFN). One hundred and seventy-four episodes of persistent HRFN were analyzed, of which 34 (19.5%) were confirmed as IFD, 52.9% caused by filamentous fungi and 47.1% by yeasts. Logistic regression and survival analyses identified the following significant risk factors for IFD: male sex (OR 4.04), adolescence (OR 4.65), C-reactive protein ≥ 90 mg/L at admission (OR 3.13), and transfer to a critical care unit (OR 10.73). The predictive model demonstrated strong discriminatory capacity (AUC 0.84), with 79.4% sensitivity and 82.1% specificity. These findings highlight that adolescent, particularly males with severe clinical conditions and elevated inflammatory markers, are at highest risk for IFD during episodes of HRFN. The proposed risk factors-based model may support early risk stratification and guide targeted antifungal prophylaxis or therapy, potentially improving outcomes in this population. Validation in external cohort is required to confirm these results and optimize clinical applicability.
Keywords:
invasive fungal disease
; neutropenia
; children
; cancer
; risk factors
Introduction
Invasive fungal disease (IFD) is one of the leading causes of morbidity and mortality in immunocompromised adult and pediatric patients. There are significant differences between these two groups in terms of epidemiology, diagnosis, treatment, immune reconstitution capacity following chemotherapy, and comorbidities [1,2]. Therefore, it is not appropriate to use data reported in adults to assess pediatric patients.
One of the most important factors for the survival of immunocompromised patients with IFD is early diagnosis and prompt treatment; in many cases, this is difficult given the non-specific nature of the symptoms and the difficulty of establishing an accurate diagnosis [3]. In this context, treatment is often initiated without certainty that the patient has an IFD, unnecessarily exposing them to antifungal drugs that may be associated with high toxicity, drug-drug interactions, and selection for resistance [2,4].
Children with hematologic malignancies are at increased risk of developing IFD. However, the type of cancer is rarely a single risk factor for the onset of this infection [5]; rather, a combination of factors or interactions between them could increase the risk of developing IFD [6]. Knowledge of these risk factors is essential for the prediction, recognition, classification, diagnosis, and early treatment of IFD, which is associated with better clinical outcomes [7].
Despite recent advances in the diagnosis and treatment of IFD, morbidity and mortality remain high in pediatric patients with cancer. Hence, different strategies have been created to address IFD, including empirical therapy, preemptive therapy, and the use of antifungal prophylaxis, each with its own advantages and disadvantages. Empirical antifungal therapy involves the early initiation of antifungal treatment in patients with fever and prolonged neutropenia (>96 hours). In contrast, preemptive therapy consists of identifying children at high risk of IFD, formulating an early detection strategy through comprehensive testing, and implementing a more rational and targeted therapy, which is expected to have reduced toxicity while achieving clinical outcomes equivalent to the empirical strategy [4]. This approach has two essential requirements: a highly specialized healthcare team with early clinical suspicion and a thorough and timely diagnostic strategy encompassing clinical, microbiological, molecular, and imaging aspects, which may in some instances limit its application [8].
Antifungal prophylaxis consists of administering antifungal drugs to populations highly susceptible to contracting IFD, such as children with acute myeloid leukemia (AML), severe aplastic anemia, leukemia relapses, and allogeneic hematopoietic cell transplant (HCT) recipients during periods of profound and prolonged neutropenia [9,10]. Prophylaxis is considered a good strategy because it has been shown to reduce the incidence of IFD [11]; however, it remains controversial due to the increase in opportunistic fungal infections, the diagnosis and management of which are complex and challenging [12,13].
An alternative to the aforementioned therapeutic approaches is to create tools that can predict IFD based on the identification of its risk factors. Some models have been developed to predict IFD in adult patients, but there are few data on pediatric patients [14,15,16,17]. This study aimed to determine the main risk factors for IFD in children with cancer and to evaluate the predictive capacity of these risk factors.
Methods
2.1. Population
Multicenter prospective cohort study with a nested retrospective analysis. Children under the age of 18 undergoing chemotherapy for cancer who were experiencing episodes of high-risk febrile neutropenia (HRFN) were invited to participate in six hospitals belonging to the National Child Program of Antineoplastic Drugs (PINDA): Dr. Luis Calvo Mackenna, Exequiel González Cortés, Sótero del Río, San Juan de Dios, Roberto del Río, and San Borja Arriarán, 2016–2020, in Santiago, Chile. The study was approved by the Human Research Ethics Committee of the Faculty of Medicine at the Universidad de Chile, and patients were enrolled after their parents signed the informed consent form, and children over the age of 8 gave their assent (FONDECYT 1161662). Patients who developed febrile and neutropenic 96 hours after admission were classified as having persistent HRFN and were included in the analyses. According to the Ethics Committee requirements, only one episode of persistent HRFN was selected per patient.
All children with persistent HRFN underwent clinical, microbiological, biomarker, and imaging assessments for the purpose of diagnosing IFD. All episodes of persistent HRFN were evaluated by an infectious disease expert and classified according to the EORTC/MSG definition as proven, probable, possible, and absence of IFD [18]. Episodes of possible IFD and Pneumocystis jirovecii infections were excluded from the analyses.
2.2. Risk Factors for IFD and Statistical Analysis
For the descriptive analysis, categorical variables were expressed as frequency and percentage, while numerical variables were expressed as median and interquartile range (IQR). Risk factors for IFD were assessed using bivariate and multivariate analyses with logistic regression models and survival analysis.
The association between IFD and the different independent variables was evaluated. The association among categorical variables was performed using Fisher's exact test or chi-square test, as appropriate. The association with numerical variables was performed using the non-parametric Wilcoxon or Kruskal Wallis test, as applicable. The crude OR and their respective 95% confidence intervals (CI) were estimated as a measure of effect using bivariate logistic regression. Event-free survival (EFS) was evaluated in episodes of persistent HRFN. The follow-up period was defined as the number of days until the patient overcame neutropenia (ANC > 500 cells/mm³). Only right-censoring was considered, and total EFS was estimated. Survival was calculated according to sociodemographic variables and admission variables (clinical and laboratory evaluation) using the Kaplan-Meier estimator, and the curves were compared using the non-parametric log-rank test. The hazard ratio (HR) and its respective 95% CI was estimated for each variable using Cox proportional hazard model.
Variables with a p-value < 0.1 in the bivariate analyses were used in the multivariate analyses. Logistic regression was performed, and the association between IFD and the different independent variables was estimated (entry model). The significant variables in the input model were used to adjust model 1. Adjusted ORs and their respective 95% CIs were estimated. A second model (model 2) was used, adding variables of biological relevance or interest as predictors of IFD as defined by the research group, which was evaluated and compared with model 1.
Given the low prevalence of IFD, the predictive ability of the models was evaluated using the same cohort. The likelihood of each patient having IFD was estimated, and this data was used to construct a receiver operating characteristic (ROC) curve and calculate the area under the curve (AUC). The cutoff point was determined as the best sensitivity and specificity by calculating the Youden index. A multivariate survival analysis was also performed using the semi-parametric test of Cox proportional hazard model. The magnitude of the effect was measured by obtaining the HR and their respective 95% CI. The proportionality assumptions were evaluated. The IFD predictor variables according to this model were compared with those obtained in the logistic regression model. The RStudio 1.3.1073 program was used for the analyses, and p-value < 0.05 was considered significant.
Results
3.1. Characteristics of the Population
Seven hundred seventy-seven episodes of HRFN were evaluated, of which 257 persisted with fever and neutropenia on day 4 of evolution. Of these, 185 were identified as first episodes and included in the study. Of the 185 persistent HRFN episodes assessed, 140 did not progress to IFD, and 45 were classified as IFD (23 proven, 13 probable, and 9 possible). Eleven patients were excluded from the analyses: 9 with possible IFD and 2 with pneumonia due to Pneumocystis jirovecii, yielding 34 episodes in total with proven and probable IFD and 140 episodes without IFD, out of 174 episodes of persistent HRFN. The median age of patients was 7.0 years (IQR 3-13), while the main type of cancer was hematologic malignancy, 85.6% (N=149 patients), with AML and acute lymphocytic leukemia being the main types of cancer with 35.3% (N=61 patients) and 29.5% (N=51 patients), respectively. Antifungal prophylaxis was used in 5 patients (2.9%) during the study period, 3 with voriconazole and 2 with fluconazole. Other characteristics of the population are described in Table 1.
Of the 34 episodes with IFD, 18 (52.9%) were filamentous fungi and 16 (47.1%) were yeasts. Of the 21 proven IFD, Candida albicans (5 cases), Candida parapsilosis (4 cases), Aspergillus spp (4 cases), and Candida tropicalis (3 cases) predominated, followed by one case each of Scedosporium sp, Candida glabrata, Candida lusitaniae, Candida dubliniensis, and Rhodotorula mucilaginosa (Table 2). Of the 13 probable cases of IFD, all corresponded to suspected filamentous fungal infection; 11 patients had pulmonary involvement, demonstrated by computed tomography scan (CT scan) findings and positive galactomannan (GM) in serum or bronchoalveolar lavage (BAL), and 2 had sinus involvement and compatible biopsy.
3.2. Risk Factors
The bivariate analysis showed that patients with IFD were older than patients who did not develop IFD, with a median age of 9.4 years (IQR 5-13) vs. 6 years (IQR 3.1-10.2), respectively (p=0.020). Furthermore, a trend analysis determined that as the age range increased, so did the IFD (p=0.013), with adolescents developing more IFD, 47.0% (N=16), than the rest of the population (Table 1). Clinical and laboratory assessment on admission showed that patients who subsequently developed IFD were admitted to hospital in a more serious condition than those who did not develop a fungal infection, with a higher percentage of patients with hypotension (p=0.033), sepsis (p=0.020), transfer to an intensive care unit (ICU) (p=0.0001), and CRP ≥90 mg/L (p=0.005) (Table 3).
Variables with a p-value < 0.1 in the bivariate analysis were used to perform a multivariate logistic regression model, defined as the input model. The significant variables in the input model were male sex, adolescent age range compared to infants, CRP ≥ 90 mg/L, transfer to the ICU, sepsis, and hypotension. When the first model (model 1) was adjusted, it was noted that male patients had a higher risk of developing IFD, adjusted OR 4.04 (95% CI 1.58-11.38), while adolescents had a 4.65 times higher risk (95% CI 1.20-21.87) than infants. A CRP ≥ 90 mg/L on admission and transfer to an PICU increases the risk of IFD by 3.13 (95% CI 1.26–8.20) and 10.73 (95% CI 4.26–29.47) times, respectively (Table 3). A second model (model 2) was evaluated by adding the variable type of cancer, considered by the authors as a possible risk factor, with no differences being found in the OR of each variable, as shown in Table 3.
Both models were evaluated for their ability to predict IFD. Model 1, obtained with the significant variables, was able to discriminate 84.7% (95% CI 76.4-92.9) of patients who developed IFD (Figure 1a), with a sensitivity of 79.4% and specificity of 82.1%, correctly classifying 81.6% of patients with a cutoff value of 0.206. Model 2 (Figure 1b), which includes the type of cancer, showed no differences from model 1 (sensitivity: 79.4, specificity: 82.1%, correctly classifying 81.1%).
3.3. Event-Free Survival
The overall EFS was 66.7% (95% CI 57.2-77.9%). The highest risk of IFD was observed in the first 7 days of neutropenia. After this period, the risk of developing IFD decreased, and on day 10 of neutropenia, only 66 patients were at risk of developing IFD with an EFS of 75% (67–83.9%). Furthermore, by day 10, 85.3% (N=29) of the IFD cases had accumulated. Kaplan-Meier curves showed that adolescents had a significantly higher risk of developing IFD, with an EFS of 38.3% (95% CI 21.3-66.8) compared to other age groups (p=0.015). Other demographic variables, such as cancer type or sex, were not associated with a lower EFS, as shown in Figure 2. Patients who developed IFD during their FN episode were admitted in a more serious condition than patients who did not develop IFD. Hypotension, sepsis and CRP ≥ 90 mg/L were associated with lower EFS, results that were statistically significant. (Figure 2)
A multivariate model of Cox proportional hazard was adjusted with the significant variables detected in the survival analyses. It was also adjusted for sex, a variable that was not significant in the survival analyses but was considered important in the onset of IFD according to previous analyses. As the forest plot shows in Figure 3, being an adolescent (aged 10 to 18 years) was an independent risk factor and associated with a 6.3 (95% CI 1.97–20.5) times increased risk of developing IFD compared to younger patients. Being transferred to PICU and having a CRP ≥90 on admission were associated with a 6.9 (3.23–14.8) and 2.4 (95% CI 1.14–5.0) times higher risk of IFD, respectively, while male sex was associated with a 3.0 (95% CI 1.43–6.4) times higher risk of developing IFD. These results are consistent with those obtained in the logistic regression analyses.
4. Discussion
In our study, we were able to establish that being male, adolescent, and presenting with greater severity at the onset of the FN episode are independent risk factors that can discriminate the development of IFD in pediatric patients with cancer in 84.7% of cases.
Currently, a wide variety of risk factors could serve as predictors of IFD [19,20,21,22,23,24]. This may be due mainly to the different study designs and populations used to determine factors that can predict IFD. A systematic review of 22 studies showed considerable heterogeneity among the patient populations studied, including patients with HCT and cancer. In addition, the studies assessed risk at different clinical stages and employed diverse methods to measure each factor [3]. Using two multivariate methods, logistic regression and survival analysis, we determined that male sex and age were non-modifiable risk factors for IFD, while greater severity at the onset of FN, manifested by hypotension, sepsis, admission to an ICU, and CRP ≥90 was independently associated with an increased risk of IFD.
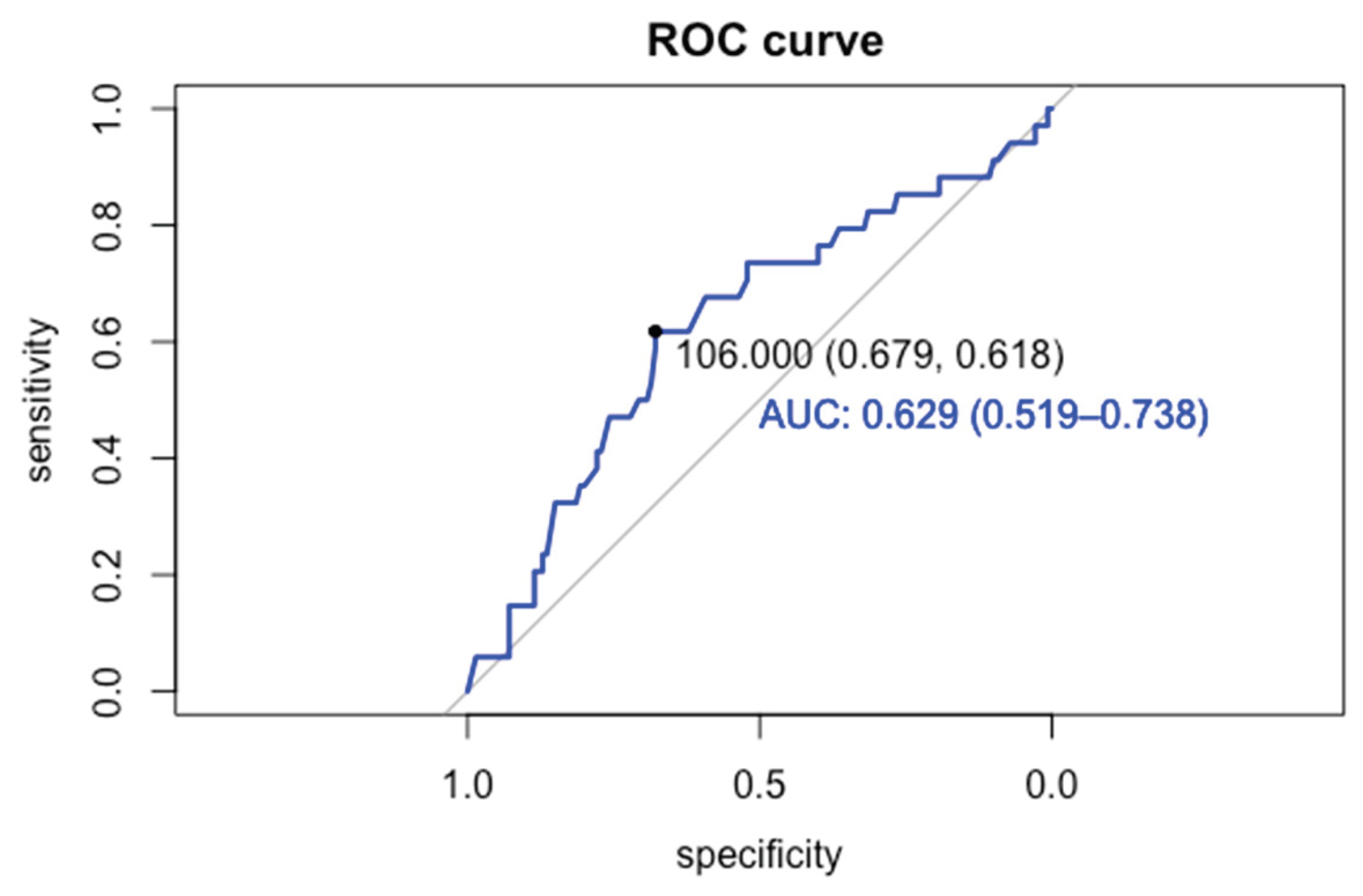
Increasing age has been associated with a higher risk of developing IFD in several articles, identifying 10 years as the cutoff value [5,6,20,21,24,25]. However, this remains a topic of debate, as it is unclear whether age itself is a risk factor or whether it is associated with such factors as the intensity of chemotherapy, depending on the type of cancer, differences in pharmacokinetics, associated comorbidities, or increased colonization by environmental fungi [3,26]. Our study determined that age was related to the onset of IFD, with a cutoff point for this predictor of 8.8 years (Figure A1), which aligns with the findings of other authors, who found an average age in patients with IFD between 8 and 10 years [6,20,21,24,25]. The group at highest risk of developing IFD in our cohort were adolescents, consistent with recent findings by Lehrnbecher et al. [1], where a multivariate analysis showed that the HR for proven/probable IFD increased in patients aged ≥12 years, with a higher proportion of filamentous fungi. These findings align with our results, where the median age of patients with filamentous fungal infections was 11.8 years (IQR 9–13.7), compared to 7.4 years (IQR 2.2–11.5) among children with yeast infections (Table A1). These findings can be explained by children, unlike adolescents, develop a greater adaptive immune response, mainly from T cells (Th17), which are responsible for promoting the elimination of fungi to compensate for an immature innate immune system. This characteristic could make children less likely to develop IFD caused by filamentous fungi compared to adolescents [12].
Concerning gender, there are currently no data indicating that it could be a risk factor for IFD in pediatric patients. In an observational study of adult patients with myeloid leukemia undergoing induction therapy, Ming-Yu Lien et al. showed that being male was significantly associated with developing IFD [27]. A clinical study conducted on pediatric cancer patients in Chile revealed that 14 of 18 cases of IFD in cancer patients were male, mostly adolescents [4]. Moreover, we noted that the risk of IFD in males increased 4-fold (95% CI 1.58–11.38) after the multivariate analyses. These results may be due to the presence of genetic effect-modifying variables, which predispose males to a higher risk of IFD. These findings should be reviewed in future studies.
Increased severity on admission has been reviewed in some pediatric studies evaluating predictors of IFD. Monsereenusorn Ch. et al. determined that respiratory involvement, the need for oxygen, hypotension, and prolonged hospitalization are associated with IFD [19]. Furthermore, Muayad A. et al developed a predictive model for IFD, finding that fever and hypotension are significantly associated with the onset of IFD [16]. In a recent study, Moraitaki E. et al. found that ICU hospitalization was associated with an increased risk of IFD in pediatric patients with hematologic cancer [20]. These data, added to the findings of this study, support the hypothesis that severity on admission is a predictive risk factor for IFD in pediatric patients with cancer.
Most studies describing IFD-related risk factors have determined that these are prolonged neutropenia, AML, and ALL relapse [3,5,19,21,23,28]. We found no significant differences in these variables because we only worked with the population with persistent HRFN, which occurs mainly in children with hematologic cancer, the population at highest risk for IFD.
In a recent systematic review assessing the main predictors of IFD in pediatric patients, a series of individual risk factors for IFD were identified; however, no prediction rules were found that could be useful for establishing prophylaxis and different antifungal therapy strategies [3]. We established a series of independent risk factors mentioned above and used them to develop a predictive model for IFD in children with cancer and persistent HRFN. This is a simple, intuitive model with parameters that are readily available in clinical practice, like age range, sex, having a CRP≥90, and transfer to the ICU to estimate the likelihood of IFD. Our model differentiated 84.7% of patients who develop IFD with good sensitivity and specificity. To date, there are few prediction rules focused on IFD in children with cancer. Muayad A. et al. designed a high-performing IFD risk score (AUC = 0.94), with good sensitivity, specificity, positive predictive value, and negative predictive value [16] using variables as duration of fever, duration of neutropenia, absolute white blood cell count, hypotension on admission, and the presence of graft-versus-host disease. The variables selected differ from ours mainly in terms of the population studied, since, as previously mentioned, the population in this cohort only includes patients with cancer experiencing persistent HRFN. In contrast, the referred study considers a population of children receiving HCT, who have greater immunosuppression and graft-versus-host disease [16].
This study maintained the strengths of a prospective study combined with a nested retrospective design, which offers certain advantages over most retrospective studies. Furthermore, it is a multicenter study, so the likelihood of bias due to factors such as local epidemiology and available diagnostic tools is lower. As a strength, we estimated independent risk factors for IFD using two different methodological approaches, logistic regression and survival analysis, which provide the results obtained with greater robustness and make it possible for us to generate a prediction rule for patients with cancer who develop fever and persistent neutropenia.
An important limitation of this study is that only one episode per patient was used to determine risk factors, which means that relevant information in the cohort may be missing, as intra- and inter-patient variability has been excluded. However, given the low number of cases, the assessment of the model's predictive capacity was performed on the same cohort. This tool must be validated in a cohort other than the one used for its creation, so new prospective studies are needed to validate and use this prediction rule in the population of children with cancer. Finally, due to the low number of cases, it was not possible to determine distinct independent risk factors for yeast and filamentous fungal infections.
5. Conclusions
Identifying risk factors that predict IFD makes it possible to develop tools that can be used as prediction rules. Our study found that patients at highest risk of developing IFD are adolescents, mainly males, who are admitted in serious condition and have persistent HRFN. The findings may enable more personalized antifungal treatment strategies for these patients, potentially reducing inappropriate antifungal use, an issue associated with increased toxicity and selection for resistance. This warrants validation in future studies.
Author Contributions
Conceptualization, M.B. and M.E.S.; methodology, M.B.; M.E.S.; and J.C.; software, M.B.; validation, M.E.S.; R.V.; V.G.; CG; and A.A.; formal analysis, M.B.; investigation, M.B.; R.V; C.G.; V.G; A.A.; M.E.S; resources, M.E.S.; data curation, M.B.; writing—original draft preparation, M.B.; writing—review and editing, R.V; C.G.; V.G; A.A. and M.E.S.; visualization, M.B.; supervision, M.E.S.; project administration, M.E.S.; funding acquisition, M.E.S.
Funding
Please add: This research was funded by FONDECYT (1161662).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Human Research Ethics Committee of the Faculty of Medicine, Universidad de Chile.
Informed Consent Statement
Informed consent and assent were obtained from all subjects involved in the study.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
We thank the patients and their parents for their generous contribution to our study. We thank research nurses of the participant hospitals for their invaluable support in enrolling patients and obtaining samples; and we also thank the FONDECYT Program for its support.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| IFD | Invasive fungal disease |
| CRP | C-reactive protein |
| RF | Risk factor |
| HRFN | high-risk febrile neutropenia |
| PICU | Pediatric Intensive Care Unit |
| AML | Acute myeloid leukemia |
| HCT | Hematopoietic cell transplant |
| PINDA | National Child Program of Antineoplastic Drugs |
| IQR | Interquartile range |
| CI | confidence intervals |
| EFS | Event-free survival |
| HR | Hazard ratio |
| ROC | Receiver operating characteristic |
| CVC | Central venous catheter |
| GM | Galactomannan |
| CT | Computed tomography |
| BAL | Bronchoalveolar lavage |
| FB | Fungus ball |
| UC | Urine culture |
| BC | Blood culture |
Appendix A
Appendix A.1

Table A1.
Comparison between mold and yeast infections in children with cancer and episodes of persistent high-risk febrile neutropenia.
Table A1.
Comparison between mold and yeast infections in children with cancer and episodes of persistent high-risk febrile neutropenia.
| Variables Median (IRQ), N (%) | Mold infections(N=18) | Yeast infections(N=16) | P-Value |
| Age (Years) | 11.8 (9.0-13.7) | 7.4 (2.2-11.5) | 0.0198 |
| Age Range | 0.0929 | ||
| Infant | 0 | 4 (25.0) | |
| Pre-school | 3 (16.7) | 4 (25.0) | |
| Elementary School | 4 (22.2) | 2 (18.8) | |
| Adolescent | 11 (61.1)) | 5 (31.2) | |
| Male sex | 12 (66.7) | 11 (68.8) | 1 |
| Hematologic Malignancies | 17 (94.4) | 11(68.7) | 0.0782 |
| Solid tumors | 1 (5.6) | 5(31.3) | |
| CRP ≥ 90 mg/L | 11 (61.1) | 12 (75.0) | 0.4768 |
| Hypotension | 4 (22.2) | 1(12.5) | 0.6602 |
| Sepsis | 6 (33.3) | 6 (37.5) | 1 |
| PICU admission | 12 (66.7) | 10 (62.5) | 1 |
Figure A1.
ROC curve of age and age cutoff for invasive fungal infection (106 months = 8.8 years).
References
- Lehrnbecher T, Groll AH, Cesaro S, et al (2023) Invasive fungal diseases impact on outcome of childhood ALL – an analysis of the international trial AIEOP-BFM ALL 2009. Leukemia 37:72–78. [CrossRef]
- Lehrnbecher T, Schoning S, Poyer F, et al (2019) Incidence and Outcome of Invasive Fungal Diseases in Children With Hematological Malignancies and/or Allogeneic Hematopoietic Stem Cell Transplantation: Results of a Prospective Multicenter Study. Front Microbiol 10:681. [CrossRef]
- Fisher BT, Robinson PD, Lehrnbecher T, et al (2018) Risk Factors for Invasive Fungal Disease in Pediatric Cancer and Hematopoietic Stem Cell Transplantation: A Systematic Review. J Pediatric Infect Dis Soc 7:191–198. [CrossRef]
- Santolaya ME, Alvarez AM, Acuña M, et al (2018) Efficacy of pre-emptive versus empirical antifungal therapy in children with cancer and high-risk febrile neutropenia: A randomized clinical trial. Journal of Antimicrobial Chemotherapy 73:2860–2866. [CrossRef]
- Ruijters VJ, Oosterom N, Wolfs TFW, et al (2019) Frequency and Determinants of Invasive Fungal Infections in Children With Solid and Hematologic Malignancies in a Nonallogeneic Stem Cell Transplantation Setting: A Narrative Review. J Pediatr Hematol Oncol 41:345–354. [CrossRef]
- Kobayashi R, Hori D, Sano H, et al (2018) Risk Factors for Invasive Fungal Infection in Children and Adolescents With Hematologic and Malignant Diseases: A 10-year Analysis in a Single Institute in Japan. Pediatr Infect Dis J 37:1282–1285. [CrossRef]
- King J, Pana ZD, Lehrnbecher T, et al (2017) Recognition and Clinical Presentation of Invasive Fungal Disease in Neonates and Children. J Pediatric Infect Dis Soc 6: S12–S21. [CrossRef]
- Van Rhijn N, White PL (2025) Antifungal treatment strategies and their impact on resistance development in clinical settings. Journal of Antimicrobial Chemotherapy. [CrossRef]
- Gutiérrez V, Contardo V, De la Maza V, et al (2022) Enfermedad Fúngica Invasora :Experiencia en centros PINDA 2016-2020. Chile. Rev. chil. infectol.. 2023. Vol. 40(4):360-369. [CrossRef]
- Barraza M, Valenzuela R, Villarroel M, et al (2024) Epidemiological changes of invasive fungal disease in children with cancer: Prospective study of the National Child Program of Antineoplastic Drugs network, Chile. Mycoses 67:e13780. [CrossRef]
- Yeoh DK, Blyth CC, Clark JE, et al (2024) Invasive fungal disease and antifungal prophylaxis in children with acute leukaemia: a multicentre retrospective Australian cohort study. Lancet Reg Health West Pac 52:. [CrossRef]
- Jenks JD, Cornely OA, Chen SCA, et al (2020) Breakthrough invasive fungal infections: Who is at risk? Mycoses 63:1021–1032. [CrossRef]
- Boutin CA, Durocher F, Beauchemin S, et al (2024) Breakthrough Invasive Fungal Infections in Patients With High-Risk Hematological Disorders Receiving Voriconazole and Posaconazole Prophylaxis: A Systematic Review. Clinical Infectious Diseases 79:151–160. [CrossRef]
- Kanda Y, Kimura SI, Iino M, et al (2020) D-Index-Guided Early Antifungal Therapy Versus Empiric Antifungal Therapy for Persistent Febrile Neutropenia: A Randomized Controlled Noninferiority Trial. J Clin Oncol 38:815–822. [CrossRef]
- Wang L, Wang Y, Hu J, et al (2019) Clinical risk score for invasive fungal diseases in patients with hematological malignancies undergoing chemotherapy: China Assessment of Antifungal Therapy in Hematological Diseases (CAESAR) study. Front Med 13:365–377. [CrossRef]
- Alali M, Giurcanu M, Elmuti L, Kumar M (2021) Pediatric Invasive Fungal Risk Score in Cancer and Hematopoietic Stem Cell Transplantation Patients With Febrile Neutropenia. J Pediatr Hematol Oncol. [CrossRef]
- Portugal RD, Garnica M, Nucci M (2009) Index to predict invasive mold infection in high-risk neutropenic patients based on the area over the neutrophil curve. Journal of Clinical Oncology 27:3849–3854. [CrossRef]
- Peter Donnelly J, Chen SC, Kauffman CA, et al (2020) Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 71:1367–1376. [CrossRef]
- Monsereenusorn C, Sricharoen T, Rujkijyanont P, et al (2021) Clinical Characteristics and Predictive Factors of Invasive Fungal Disease in Pediatric Oncology Patients with Febrile Neutropenia in a Country with Limited Resources. Pediatric Health Med Ther 12:335–345. [CrossRef]
- Moraitaki E, Kyriakidis I, Pelagiadis I, et al (2024) Epidemiology of Invasive Fungal Diseases: A 10-Year Experience in a Tertiary Pediatric Hematology–Oncology Department in Greece. Journal of Fungi 10:. [CrossRef]
- Gal Etzioni TR, Fainshtain N, Nitzan-Luques A, et al (2024) Invasive Fungal Infections in Children with Acute Leukemia: Epidemiology, Risk Factors, and Outcome. Microorganisms 12:145. [CrossRef]
- Hajri H Al, Al-Salmi W, Hinai K Al, et al (2023) Invasive fungal infections in children with leukemia in a tertiary hospital in Oman: An eight-year review. Curr Med Mycol 9(3), 16–22. [CrossRef]
- Roumani AM, Benmouffok N (2022) Risk Factors for Invasive Fungal Disease in Pediatric Oncology. International Journal of Clinical Research 3:167–172. [CrossRef]
- Sezgin Evim M, Tüfekçi Ö, Baytan B, et al (2022) Invasive Fungal Infections in Children with Leukemia: Clinical Features and Prognosis. Turkish Journal of Hematology 39:94–102. [CrossRef]
- Kobayashi R, Kaneda M, Sato T, et al (2008) The clinical feature of invasive fungal infection in pediatric patients with hematologic and malignant diseases: a 10-year analysis at a single institution at Japan. J Pediatr Hematol Oncol 30:886–890. [CrossRef]
- Lin GL, Chang HH, Lu CY, et al (2018) Clinical characteristics and outcome of invasive fungal infections in pediatric acute myeloid leukemia patients in a medical center in Taiwan. J Microbiol Immunol Infect 51:251–259. [CrossRef]
- Fang W, Wu J, Cheng M, et al (2023) Diagnosis of invasive fungal infections: challenges and recent developments. J Biomed Sci 30 (1), 42. [CrossRef]
- Cesaro S, Tridello G, Castagnola E, et al (2017) Retrospective study on the incidence and outcome of proven and probable invasive fungal infections in high-risk pediatric onco-hematological patients. Eur J Haematol 99:240–248. [CrossRef]
Figure 1.
Kaplan-Meier estimator. The p-value was obtained using the log-rank test.
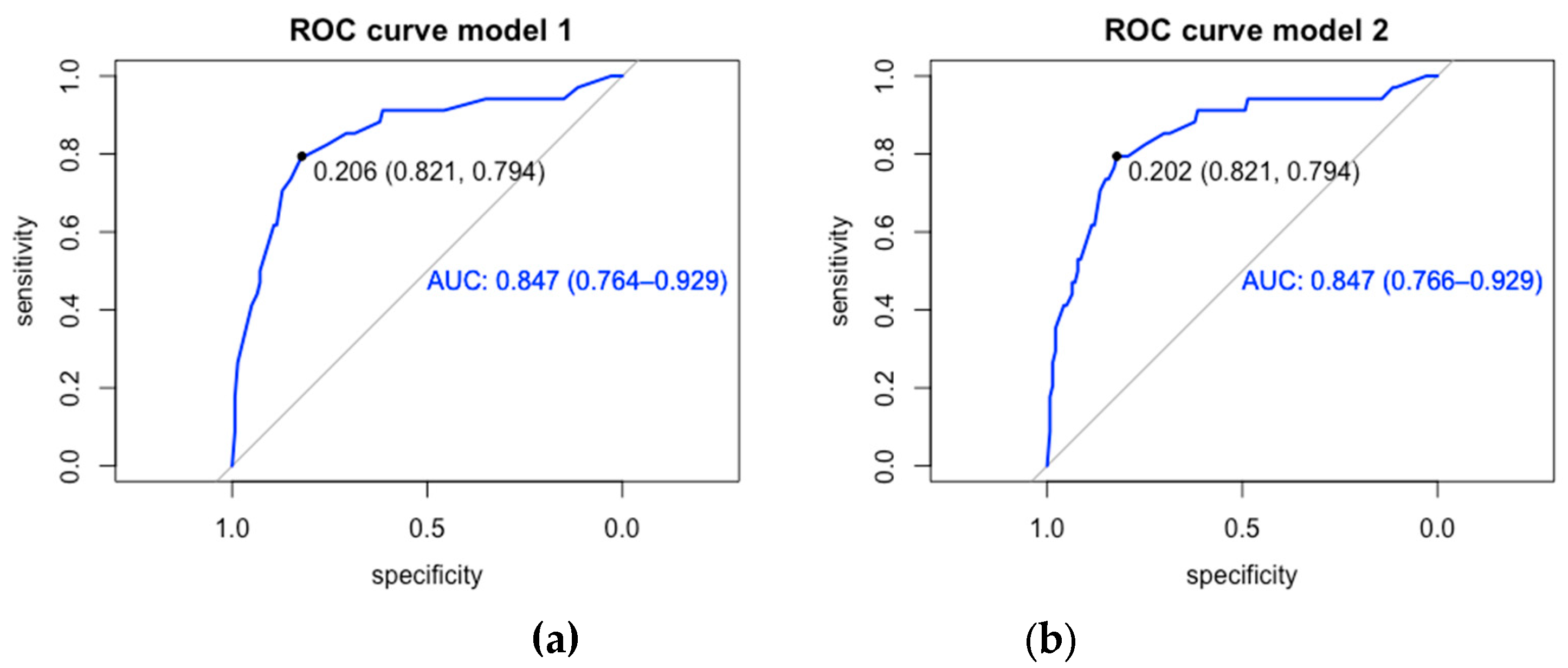
Figure 2.
Forest plot and hazard ratio estimation. Results obtained from the analysis of Cox proportional hazards models.
Figure 2.
Forest plot and hazard ratio estimation. Results obtained from the analysis of Cox proportional hazards models.
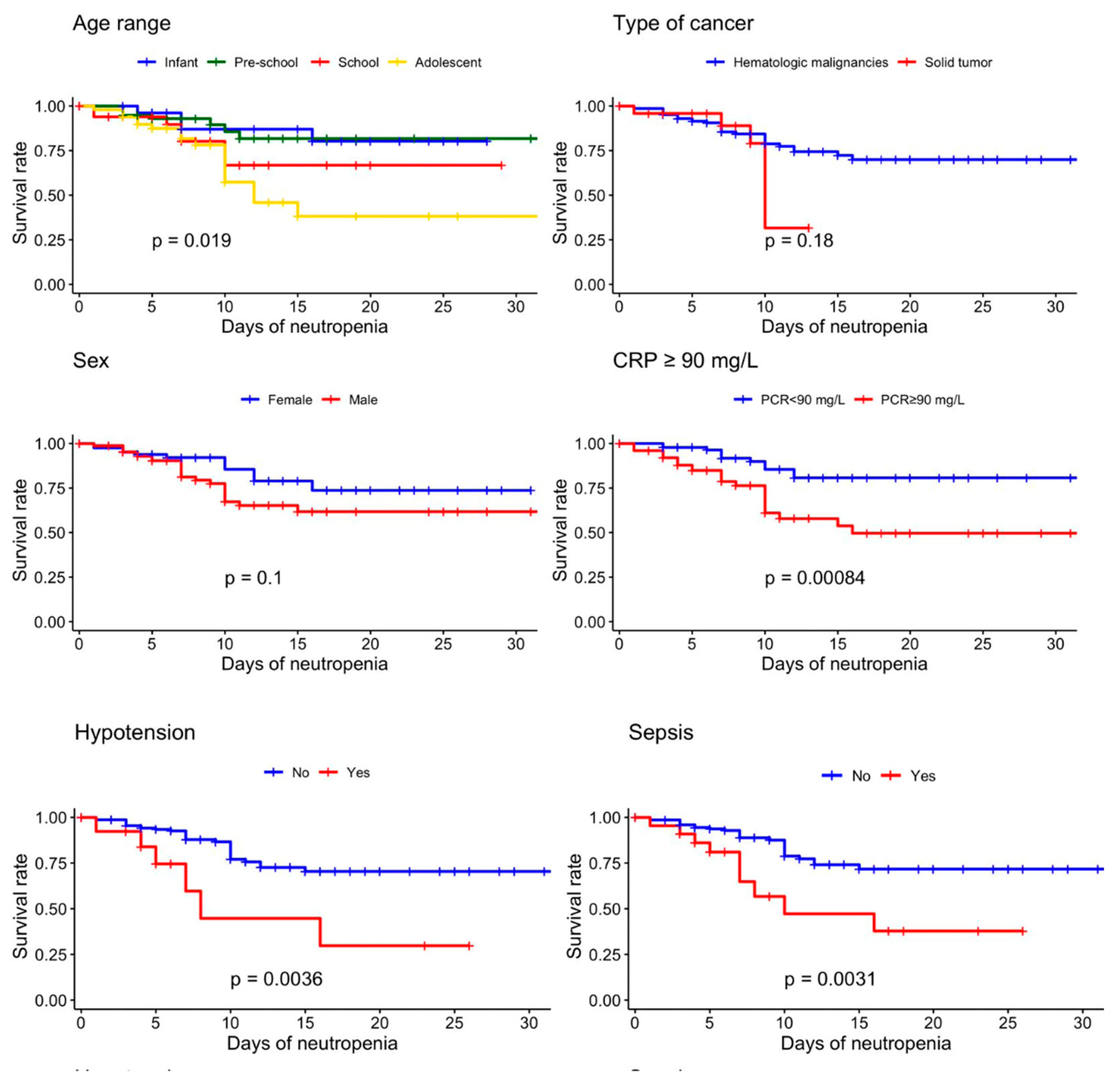
Figure 3.
ROC curve of predictive models for invasive fungal disease in children with cancer and episodes of persistent high-risk febrile neutropenia. (a) Model 1 (b) Model 2.
Figure 3.
ROC curve of predictive models for invasive fungal disease in children with cancer and episodes of persistent high-risk febrile neutropenia. (a) Model 1 (b) Model 2.
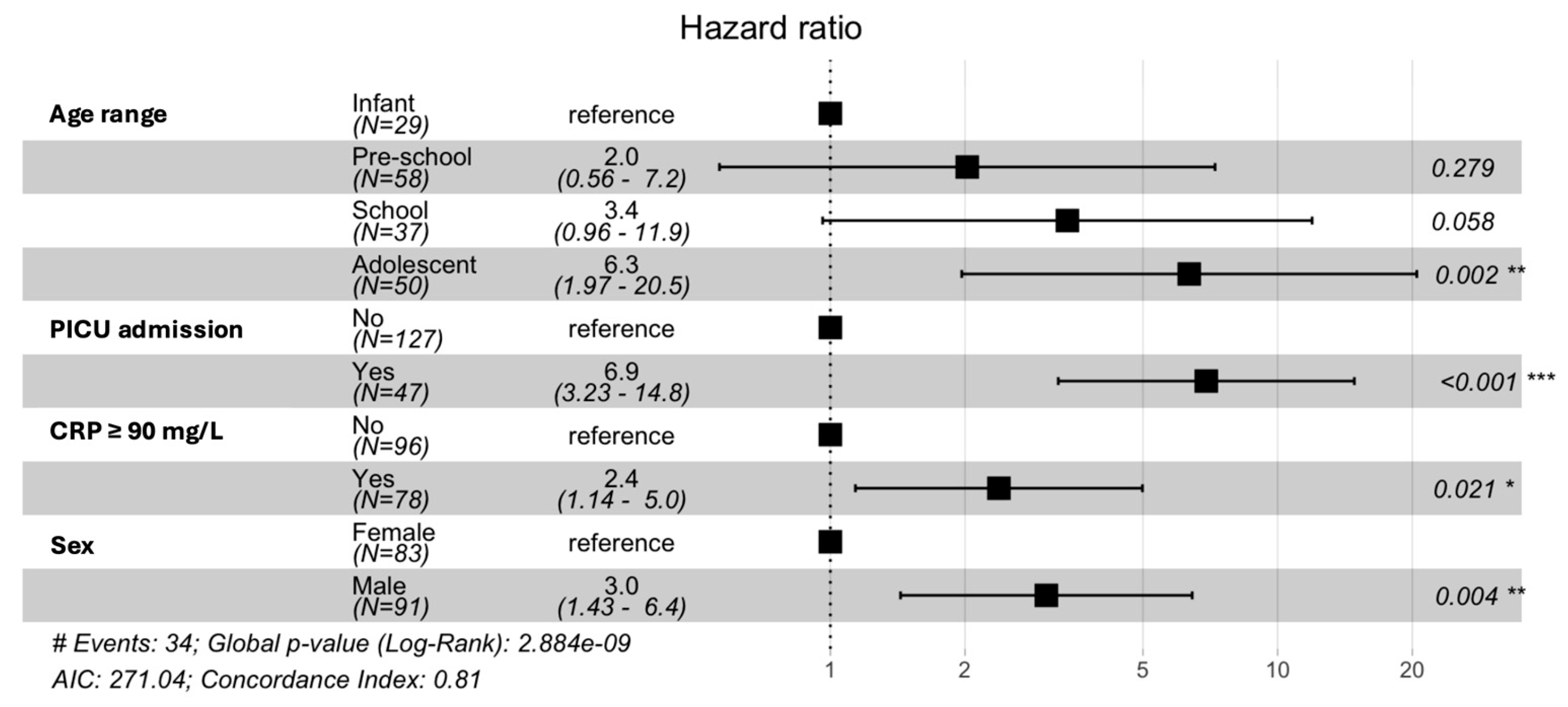
Table 1.
Demographic and clinical characteristics at admission in 174 children with cancer and episodes of persistent high-risk febrile neutropenia, according to the presence or absence of invasive fungal disease.
Table 1.
Demographic and clinical characteristics at admission in 174 children with cancer and episodes of persistent high-risk febrile neutropenia, according to the presence or absence of invasive fungal disease.
| Variable (Median; IQR) (n; %) | IFD (n=34) |
No IFD (n= 140) |
Total (n= 174) |
p-value |
| Demographic | ||||
| Age; years | 9.4 (5-13) | 6 (3.1-10.2) | 7.0 (3-13) | 0.0200* |
| Male sex | 23 (67.7) | 68 (48.6) | 91 (52.3) | 0.0550 |
| Age range | 0.0540** | |||
| Infant | 4 (11.8) | 25 (17.9) | 29 (16.7) | Ref |
| Pre-school | 7 (20.6) | 51 (36.4) | 58 (33.3) | 0.8196 |
| School | 7 (20.6) | 30 (21.4) | 37 (21.3) | 0.5805 |
| Adolescent | 16 (47.0) | 34 (24.3) | 50 (28.7) | 0.0810 |
| Clinical | ||||
| Type of cancer | 0.5868 | |||
| Hematologic malignancies | 28 (82.4) | 121 (86.4) | 149 (85.6) | |
| Solid tumors | 6 (17.6) | 19 (13.6) | 25 (14.4) | |
| Use of CVC | 32 (94.1) | 126 (91.3) | 158 (91.9) | 0.7390 |
| Previous IFD | 2 (5.9) | 5 (3.6) | 7 (4.0) | 0.7390 |
| Bacterial co-infection | 29 (85.3) | 99 (70.7) | 128 (73.6) | 0.1270 |
| CRP ≥ 90 mg/L | 23 (67.6) | 55 (39.3) | 78 (44.8) | 0.0052* |
| Hypotension | 6 (17.6) | 8 (5.7) | 21 (12.1) | 0.0331* |
| Sepsis | 9 (26.5) | 14 (10) | 23 (13.2) | 0.0205* |
| PICU admission | 22(64.7) | 25 (17.9) | 47(27.0) | 0.0001* |
CVC: central venous catheter; IFD: Invasive fungal disease; CRP: C-reactive protein, PICU: Pediatric Intensive Care Unit; ref: reference; *Statistically significant variable, ** Trend test.
Table 2.
Demographic, clinical, imaging, and microbiological characteristics of 34 children with proven or probable Invasive Fungal Disease.
Table 2.
Demographic, clinical, imaging, and microbiological characteristics of 34 children with proven or probable Invasive Fungal Disease.
|
Age (years) |
Gender |
Type of cancer/ Phase of treatment |
Source |
Clinical and microbiological findings |
Outcome |
| Proven IFD | |||||
| 13 | M | Solid Tumor* | Renal | FB, UC (+) C. albicans | Alive |
| 4 | M | Lymphoma* | Renal | FB, UC (+) C. albicans | Alive |
| 0.8 | F | AML/Consolidation | Candidemia | BC (+) C. parapsilosis | Dead |
| 6 | M | ALL relapse/Induction | Spleen | Splenic lesions, UC (+) C. glabrata | Alive |
| 14 | M | AML/Consolidation | Pneumonia | Thin hyphae in lung biopsy. Aspergillus sp. | Alive |
| 11 | F | ALL/Consolidation | Renal | Renal biopsy, abscess, C. lusitaniae | Alive |
| 3 | M | Solid Tumor* | Pneumonia | Serum GM (3.8), pulmonary CT, PCR Aspergillus sp. | Alive |
| 3 | F | ALL/Consolidation | Candidemia | BC (+) C. parapsilosis | Alive |
| 1 | M | AML/Consolidation | Catheter Infection | CVC (+) C. albicans | Alive |
| 8 | M | ALL/Consolidation | Candidemia | BC, UC (+) C. tropicalis | Alive |
| 1 | M | AML/Consolidation | Catheter Infection | CVC (+) C. parapsilosis | Alive |
| 9 | F | Solid Tumor* | Candidemia | BC (+) C. parapsilosis | Alive |
| 8 | M | AML/Consolidation | Hepatosplenic | Hepatosplenic images, UC (+) C. albicans | Alive |
| 12 | M | ALL/Induction | Pneumonia | Pulmonary CT, Biopsy Aspergillus fumigatus | Alive |
| 13 | F | Solid Tumor* | Esophagitis | Esophageal biopsy, C. dublinensis | Alive |
| 13 | M | ALL/Induction | Hepatosplenic | Hepatosplenic images, UC (+) C. albicans | Alive |
| 13 | F | ALL/Induction | Fungal Sinusitis | Nasal biopsy, serum GM (0.7) Scedosporium sp. | Dead |
| 14 | M | ALL relapse/Consolidation | Pneumonia | Pulmonary CT, nasal cavity scab, Aspergillus sp. | Alive |
| 2 | M | Solid Tumor* | Candidemia | BC (+) C. tropicalis | Alive |
| 14 | M | ALL/Maintenance | Fungemia | BC (+) Rhodotorula mucilaginosa | Alive |
| 0.9 | M | Solid Tumor* | Candidemia | BC (+) C. tropicalis | Alive |
| Probable IFD | |||||
| 8 | M | AML/Consolidation | Fungal Sinusitis | Thin septate hyphae in biopsy | Alive |
| 13 | M | AML/Consolidation | Fungal Sinusitis | Sparse septate hyphae with 90-degree bifurcation in biopsy | Alive |
| 18 | F | ALL relapse/Maintenance | Pneumonia | BAL GM (2.1), pulmonary CT | Alive |
| 9 | M | AML/Consolidation | Pneumonia | Serum GM (0.6), pulmonary CT | Alive |
| 4 | M | AML/Consolidation | Pneumonia | Serum GM (0.7), pulmonary CT | Alive |
| 17 | M | AML/Induction | Pneumonia | Serum GM (1.5), pulmonary CT | Alive |
| 9 | M | ALL/Induction | Pneumonia | Serum GM (0.8), pulmonary CT | Alive |
| 9 | F | ALL/Induction | Pneumonia | Serum GM (0.6), pulmonary CT | Alive |
| 14 | F | AML/Consolidation | Pneumonia | Serum (1.9) and BAL (4.9) GM, pulmonary CT | Alive |
| 6 | M | ALL/Consolidation | Pneumonia | BAL GM (4.1), pulmonary CT | Alive |
| 11 | M | AML/Consolidation | Pneumonia | Serum GM (1.1), pulmonary CT | Alive |
| 12 | F | ALL/Consolidation | Pneumonia | Serum (2.8) and BAL (6.5) GM (+), pulmonary CT | Alive |
| 11 | F | ALL/Induction | Pneumonia | Serum GM (0.8), pulmonary CT | Dead |
AML: acute myeloid leukemia; ALL: acute lymphoblastic leukemia; M: male; F: female; CVC: central venous catheter; FB: fungal ball; UC: urine culture; BC: blood culture; GM: galactomannan antigen (serum > 0.5; BAL ≥ 1); BAL: bronchoalveolar lavage; CT: computed tomography; * No specific protocol.
Table 3.
Risk factors for invasive fungal diseases in children with cancer and episodes of persistent high-risk febrile neutropenia obtained by multivariate logistic regression analysis.
Table 3.
Risk factors for invasive fungal diseases in children with cancer and episodes of persistent high-risk febrile neutropenia obtained by multivariate logistic regression analysis.
| Variable | Input model | Model 1 | Model 2 | |||
| CrudeOR | 95% CI | AdjustedOR | 95% CI | AdjustedOR | 95% CI | |
| Male sex | 2.21 | 1.02 - 5.04 | 4.04 | 1.58 - 11.38 | 4.04 | 1.58 – 11.36 |
| Age range (ref Infant) | ||||||
| Adolescent | 2.94 | 0.94 - 11.23 | 4.65 | 1.20 - 21.87 | 4.74 | 1.21 - 22.61 |
| CRP ≥ 90 mg/L | 3.23 | 1.49 - 7.39 | 3.13 | 1.26 - 8.20 | 3.05 | 1.20 – 8.15 |
| Hypotension | 3.54 | 1.09 - 10.98 | ||||
| Sepsis | 3.24 | 1.23 - 8.25 | ||||
| PICU admission | 8.43 | 3.76 -19.81 | 10.73 | 4.26 - 29.47 | 10.65 | 4.35 - 29.28 |
| Type of cancer (ref hematologic malignancy) | 1.36 | 0.46 - 3.57 | 1.18 | 0.32 - 3.97 | ||
CRP: C-reactive protein PICU: Pediatric Intensive Care Unit; ref: reference.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



