
Submitted:
25 October 2025
Posted:
27 October 2025
You are already at the latest version
Abstract
Circumduction gait in stroke patients, a compensatory movement involving pelvic hike and femoral abduction, increases energy cost. However, longitudinal studies on its mechanism during the acute phase are lacking. This study longitudinally investigated changes in the paretic femoral abduction angle during gait in acute stroke patients and identified related factors. Twenty-two acute stroke patients were assessed twice: at gait in-itiation and 10-14 days later. Gait kinematics during a 3m walk were measured using a depth sensor, and physical functions (SIAS) were evaluated. Changes were analyzed us-ing paired t-tests and correlation analyses. Spatiotemporal parameters improved signifi-cantly. Kinematically, paretic femoral abduction (p = 0.049) and paretic pelvic hike (p = 0.025) significantly decreased, while maximum paretic knee flexion during swing (p = 0.026) increased. The decrease in femoral abduction correlated positively with the de-crease in pelvic hike (r=0.55) and negatively with the improvement in paretic ankle motor function (SIAS) (ρ=-0.49). The decrease in pelvic hike correlated negatively with the im-provement in paretic knee motor function (SIAS) (ρ=-0.43). These results suggest that in acute stroke patients, the recovery of paretic ankle and knee motor functions leads to a re-duction in compensatory femoral abduction and pelvic hike, respectively. This study pro-vides insights for re-evaluating compensatory movements as an adaptive phenomenon during recovery, not merely as abnormal movements.
Keywords:
circumduction
; acute stroke
; abnormal gait pattern
; longitudinal change
1. Introduction
Stroke-related hemiparesis impairs gait through deficits in lower-limb sensation and motor control, reducing daily activity and health-related quality of life (QOL) [1,2,3,4,5]. Elevated metabolic cost is a key contributor, and so-called circumduction has been implicated as an inefficient yet common compensation [4,5,6,7]. Rather than a single pattern, circumduction is typically expressed through two surrogate kinematic behaviors during paretic swing: thigh (femoral segment) abduction and pelvic hike [8]. In this study, we define thigh abduction angle as the angle between the global vertical and the thigh segment, and pelvic hike angle as the angle between the horizontal and the line connecting both anterior superior iliac spines; positive values indicate elevation of the paretic hemipelvis [8]. Prior work shows both metrics are larger in persons with chronic stroke than in healthy adults during mid-swing [8].
Intervention studies targeting circumduction-related mechanics have yielded inconsistent results. Assistive ankle exosuits have reduced pelvic hike while increasing knee flexion in chronic stroke [10], whereas high-intensity stepping in subacute stroke improved speed and hip range of motion yet increased hip abduction during swing [11]; ankle–foot orthoses have shown no consistent effect on circumduction or pelvic hike [12]. Beyond interventions, mechanical perturbation of pre-swing knee flexion can increase paretic thigh abduction, possibly via abnormal rectus femoris–gluteus medius coupling [13]. Kinematic correlates also appear to vary with walking speed and impairment severity—faster walkers may show greater hip abduction, whereas slower walkers often exhibit reduced knee flexion/dorsiflexion and smaller abduction [14]; pelvic hike is frequently observed with limited paretic knee flexion or more severe paresis [15,16,17]. Collectively, cross-sectional evidence links circumduction surrogates to both segmental motor control and global spatiotemporal context, but causality and longitudinal behavior remain unresolved [12,15,16,17,18].
Clinically scalable motion analysis is essential to study these compensations during the acute phase. Markerless depth sensors estimate joint centers from depth images and allow low-cost, preparation-light 3D gait assessment suitable for wards and early rehabilitation [19,20,21,22]. Multiple studies—across healthy adults and neurologic populations—support acceptable agreement with optical motion capture for hip and knee kinematics relevant to stance and swing [23,24,25]. Our prior work further demonstrated concurrent validity for thigh abduction and pelvic hike in individuals with hemiparesis after brain injury, supporting the use of a depth sensor to track these compensations in clinical settings [26].
However, no longitudinal study has quantified how thigh abduction and pelvic hike change over time in the acute stage of stroke recovery, nor identified which segmental motor functions are associated with their attenuation [11,14,15,16,17,18]. Addressing this gap could help reframe these behaviors not merely as “abnormalities,” but as adaptive strategies that recede with recovery.
The objectives in this study were to quantify short-term longitudinal changes in paretic thigh abduction and pelvic hike during gait in acute stroke, and to identify their associations with lower-limb motor functions.
We hypothesized the followings: (i) Both thigh abduction and pelvic hike will decrease at follow-up compared with the initial assessment. (ii) Reductions in thigh abduction will be negatively associated with improvements in paretic ankle motor function, and reductions in pelvic hike will be negatively associated with improvements in paretic knee motor function.
2. Materials and Methods
2.1. Participants
This longitudinal observational study included patients with m admitted to the Departments of Neurology and Neurosurgery at Sendai Medical Center between May 2024 and September 2025. A total of 22 patients were enrolled.
The initial assessment was conducted once the patient was able to walk safely with minimal assistance, and the follow-up assessment was performed 10–14 days later, including gait and physical function evaluations.
The inclusion criteria were: 1) First-ever acute stroke patients aged 20–90 years; 2) Diagnosed with first-ever stroke (cerebral infarction or hemorrhage) by a physician based on Magnetic Resonance Imaging (MRI) or Computed Tomography (CT); 3) Ability to walk 3 meters with handrail use and minimal assistance; 4) Ability to understand verbal instructions. Exclusion criteria for patients with hemiparesis were: 1) presence of diabetic neuropathy, 2) motor paralysis symptoms in the non-paretic lower limb, 3) decreased sensory function in the non-paretic lower limb, 4) decreased or absent Achilles tendon reflex in the non-paretic side, 5) a history of bone or joint disease in the lower limbs, 6) presence of lesions in the cerebellum or brainstem, 7) symptoms of hemispatial neglect with a score of 2 or lower on the visuospatial cognitive test of the Stroke Impairment Assessment Set (SIAS), and 8) a Mini Mental State Examination (MMSE) score of 19 or lower[27,28,29].
All participants provided written informed consent prior to participation.
The study protocol was approved by the Ethics Committees of Tohoku University Graduate School of Medicine (approval no. 2024-1-032) and Sendai Medical Center (approval no. 24-12) and conducted in accordance with the Declaration of Helsinki.
2.2. Measuring Equipment
Gait data were collected using a depth sensor (Azure Kinect DK; Microsoft Corporation, Redmond, WA, USA), identical to the setup in our previous validation study (Figure 1a) [26].
The device captured skeletal joint coordinates at 30 Hz using the Azure Kinect Body Tracking SDK (v1.4.1).
The sensor was mounted on a tripod at a height of 1.0 m, positioned 4.5 m in front of the gait initiation point with a 0° frontal view.
The effective measurement range was 0.5–3.86 m [31].
This configuration has previously demonstrated excellent concurrent validity with optical motion capture for hip and knee kinematics (r ≥ 0.9) under comparable conditions [30].
2.3. Gait Assessment
Before gait measurement, physical function was assessed using the Stroke Impairment Assessment Set (SIAS).
Participants rolled up their trouser cuffs to expose the ankle and knee joints, tucked in shirts to visualize hip movement, and walked barefoot to improve motion tracking.
From a standing start 4 m from the sensor, participants walked 3 m at a self-selected comfortable speed while lightly holding a handrail with the non-paretic upper limb (Figure 1b).
When minimal assistance was required, the evaluator used a cardboard shield to prevent self-detection by the sensor and provided minimal manual support under the paretic axilla (Figure 3).
Each participant completed five valid trials (maximum of eight, including repetitions).
Rest periods were allowed to avoid fatigue.
If a trial was invalid (e.g., tracking loss), it was immediately repeated.
To ensure consistency across sessions, handrail and orthosis use were standardized: patients who used a handrail or ankle–foot orthosis (AFO) during the initial test used the same aid during the follow-up assessment.
2.4. Data Processing
Python (version 3.10, Python Software Foundation, Wilmington, DE, USA) was used for gait analysis processing. The time-series data of each body coordinate obtained from the depth sensor were resampled to 60 Hz and smoothed using a fourth-order Butterworth low-pass filter with a 6 Hz cutoff frequency.
Gait events (initial contact and toe-off) were detected using the depth sensor data. Initial contact was defined as the point of maximum anteroposterior distance between the pelvis and ankle points. Toe-off was defined as the point of maximum anteroposterior distance between the pelvis and foot points [32].
Spatiotemporal parameters were calculated according to the methods of Rose et al. [33]. Based on previous studies [8,34], kinematic parameters were calculated, including: H1 (hip flexion angle at initial contact), H2 (hip flexion angle during loading response), H3 (minimum hip flexion angle), H4 (hip flexion angle at toe-off), H5 (maximum hip flexion angle during swing), H6 (total hip range of motion), K1 (knee flexion angle at initial contact), K2 (knee flexion angle during loading response), K3 (minimum knee flexion angle), K4 (knee flexion angle at toe-off), K5 (maximum knee flexion angle during swing), K6 (total knee range of motion), maximum paretic femoral abduction angle, and maximum paretic pelvic hike angle during 25-75% of the paretic swing phase(Figure 4).
The paretic femoral abduction angle was defined as the angle formed by the vertical axis of the laboratory and the line connecting the hip and knee joints. Paretic pelvic hike was defined as the angle formed by the horizontal axis of the laboratory and the line connecting left and right hip joints. Furthermore, a positive value was defined when the paretic hip joint was higher than the non-paretic hip joint, and a negative value when it was lower. Our previous research on the concurrent validity between 3D motion analysis and the depth sensor in hemiplegic gait confirmed moderate or higher concurrent validity for these kinematic parameters, excluding H4, H5, and K1 [26].
2.5. Statical Analysis
First, the Shapiro-Wilk test was used to assess the normality of distribution for all continuous variables, including gait parameters. To examine the relationship between baseline paretic femoral abduction and pelvic hike angles and other gait and functional parameters, either Pearson's product-moment correlation coefficient or Spearman's rank correlation coefficient was used, depending on the data distribution. Comparisons of gait parameters between the initial and second assessments were conducted. A paired t-test was used for normally distributed continuous variables, while the Wilcoxon signed-rank test was used for variables that were not normally distributed. Correlations between the changes in paretic femoral abduction and pelvic hike angles and the changes in other gait and functional parameters were also analyzed using Pearson's or Spearman's correlation.
As part of the primary analysis, we calculated the effect size (Cohen’s dz) and the correlation analysis effect size (r) for each comparison to quantify the magnitude of the results. These procedures were positioned as sensitivity analyses included in the primary analysis to verify the robustness and clinical significance of the results.
Correlation coefficients were interpreted as follows: 0.80 or higher as "very strong"; 0.50 to less than 0.80 as "moderate"; 0.30 to less than 0.50 as "somewhat weak"; and less than 0.30 as "weak" [35]. All statistical analyses were performed using SPSS Statistics version 20.0 (IBM, Armonk, NY, USA). The significance level was set at 0.05.
3. Results
3.1. Participant Characteristics
Twenty-two patients with first-ever acute stroke were enrolled (17 male; mean age 66.05 years, SD 15.44). The mean time from stroke onset to the initial assessment was 8.77 days (SD 5.27). The mean interval between the initial and follow-up assessments was 12.95 days (SD 1.15). Mean daily physical therapy time was 22.06 minutes (SD 7.05) before the initial assessment and 25.72 minutes (SD 7.68) during the interval period (Table 1).
3.2. Correlations Between Compensatory Movements and Gait/Functional Parameters at Initial Assessment
At the initial assessment, the paretic femoral abduction angle showed a somewhat weak positive correlation with step width (r = 0.46, p = 0.031) (Table 2).The paretic pelvic hike angle showed moderate positive correlations with double support time (r = 0.66, p = 0.001), paretic swing time (r = 0.57, p = 0.002), and gait cycle time (r = 0.51, p = 0.016). It also showed a somewhat weak negative correlation with gait speed (r = -0.46, p = 0.031). Furthermore, paretic pelvic hike showed a moderate negative correlation with the paretic knee flexion angle at toe-off (r = -0.50, p = 0.018).Regarding physical functional assessments, the paretic femoral abduction angle showed a moderate negative correlation with paretic ankle motor function (r = -0.56, p = 0.007) and a somewhat weak negative correlation with superficial sensation (r = -0.45, p = 0.034) (Table 2). The paretic pelvic hike angle showed a somewhat weak negative correlation with hip motor function (r = -0.44, p = 0.041).

Table 2.
Correlations between compensatory movements and gait parameters at initial assessment.
| Spatiotemporal and kinematic variables |
Paretic side femoral abduction angle |
Paretic side pelvic hike angle |
|||||
| Correlation | p-value | Correlation | p-value | ||||
| Gait speed (m/sec) a | -0.17 | 0.446 | -0.46 | 0.031 | |||
| Gait cycle time (sec) b | 0.22 | 0.326 | 0.51 | 0.016 | |||
| Double stance time (sec) a | 0.13 | 0.569 | 0.66 | 0.001 | |||
| Paretic stance time (sec) a | 0.14 | 0.544 | 0.56 | 0.006 | |||
| Paretic swing time (sec) b | 0.42 | 0.053 | 0.57 | 0.002 | |||
| Non-paretic swing time (sec) b | -0.26 | 0.234 | -0.04 | 0.875 | |||
| Stride length on the paretic side (m) a | -0.09 | 0.686 | -0.25 | 0.253 | |||
| Step length on the paretic side (m) a | 0.11 | 0.615 | -0.02 | 0.927 | |||
| Step length on the non-paretic side (m) a | -0.05 | 0.818 | -0.38 | 0.080 | |||
| Step width (m)a | 0.46 | 0.031 | 0.36 | 0.095 | |||
| Paretic pelvic hike angle (°) a | 0.33 | 0.131 | - | - | |||
| H1 (°) a | 0.06 | 0.796 | -0.21 | 0.349 | |||
| H2 (°) a | 0.11 | 0.639 | -0.19 | 0.388 | |||
| H3 (°) a | -0.02 | 0.917 | 0.01 | 0.950 | |||
| H4 (°) a | -0.09 | 0.698 | -0.17 | 0.452 | |||
| H5 (°) a | 0.10 | 0.671 | -0.19 | 0.391 | |||
| H6 (°) a | 0.26 | 0.234 | -0.22 | 0.332 | |||
| K1 (°) a | 0.17 | 0.452 | -0.04 | 0.866 | |||
| K2 (°) a | 0.34 | 0.119 | 0.11 | 0.636 | |||
| K3 (°) b | -0.19 | 0.391 | -0.10 | 0.669 | |||
| K4 (°) a | -0.32 | 0.145 | -0.50 | 0.018 | |||
| K5 (°) a | -0.09 | 0.703 | -0.35 | 0.108 | |||
| K6 (°) a | -0.03 | 0.903 | -0.28 | 0.210 | |||
|
a Pearson's correlation coefficient (p < 0.05) b Spearman's rank correlation coefficient (p < 0.05) | |||||||
Table 3.
Correlations between compensatory movements and functional parameters at initial assessment.
Table 3.
Correlations between compensatory movements and functional parameters at initial assessment.
| SIAS evaluation items |
Paretic side femoral abduction angle |
Paretic side pelvic hike angle |
|||||
| Correlation | p-value | Correlation | p-value | ||||
| Hip joint b | -0.10 | 0.654 | -0.44 | 0.041 | |||
| Knee joint b | -0.32 | 0.149 | -0.38 | 0.078 | |||
| Ankle joint b | -0.56 | 0.007 | -0.40 | 0.064 | |||
| L/E deep tendon reflex b | -0.20 | 0.372 | 0.02 | 0.939 | |||
| L/E muscle tone b | -0.06 | 0.791 | 0.05 | 0.833 | |||
| L/E superficial sensation b | -0.45 | 0.034 | -0.11 | 0.634 | |||
| L/E deep sensation b | -0.20 | 0.368 | 0.11 | 0.623 | |||
| Ankle joint range of motion b | -0.05 | 0.822 | -0.18 | 0.417 | |||
| Abdominal strength b | 0.17 | 0.444 | 0.01 | 0.957 | |||
| L/E: Lower extremity | |||||||
| b Spearman's rank correlation coefficient (p < 0.05) | |||||||
3.3. Longitudinal Changes in Gait Parameters
From baseline to follow-up, spatiotemporal metrics improved: gait speed increased (p < 0.001), gait cycle time (p < 0.001), double support time (p < 0.001), and paretic stance time (p < 0.001) decreased; paretic stride length (p < 0.001) and both step lengths (paretic p = 0.003; non-paretic p < 0.001) increased (Table 4).
Compensatory angles declined: thigh abduction (mean from 6.71° to 5.79°, p = 0.049) and pelvic hike (3.82° to 2.90°, p = 0.025). Segmental kinematics improved: hip ROM (H6) (p = 0.039), maximum knee flexion in swing (K5) (p = 0.026), and knee ROM (K6) (p = 0.036) increased (Table 4).
3.4. Longitudinal Changes in SIAS Scores
Motor scores improved at follow-up for the hip (p < 0.001), knee (p = 0.006), and ankle (p < 0.001), as did deep sensation (p = 0.046) and abdominal strength (p = 0.002). Deep tendon reflex (p = 0.153), muscle tone (p = 0.160), superficial sensation (p = 0.083), and ankle ROM (p = 0.317) showed no significant change (Table 5).
3.5. Correlations Between Changes in Compensatory Movements and Changes in Gait Parameters and Physical Function Assessment Items
Reductions in thigh abduction and pelvic hike were moderately coupled (r = 0.55, p = 0.008). No other gait Δ-parameters showed significant associations (Table 6).
Functionally, the reduction in thigh abduction correlated negatively with improvement in paretic ankle motor function (ρ = −0.49, p = 0.021), and the reduction in pelvic hike correlated negatively with improvement in paretic knee motor function (ρ = −0.43, p = 0.046) (Table 7).
Discussion
This longitudinal study quantified short-term changes in paretic thigh (femoral segment) abduction and pelvic hike during gait in acute post-stroke hemiparesis and examined their associations with segmental motor recovery. At baseline, larger thigh abduction was linked to poorer paretic ankle motor function and wider step width, whereas greater pelvic hike was linked to slower and more asymmetrical spatiotemporal patterns and to poorer knee/hip motor function. Over ~13 days, both compensatory angles decreased, and their reductions were negatively associated with improvements in ankle (for thigh abduction) and knee (for pelvic hike) motor function, respectively. Taken together, these findings support the view that these behaviors are distinct compensatory strategies that tend to recede as segmental control recovers, especially at the ankle and knee.
4.1. Relationship Between Compensatory Movements and Gait/Physical Function at Initial Assessment
At the initial assessment, greater thigh abduction co-occurred with poorer ankle motor function (SIAS) and wider step width. This pattern is consistent with a lateral stability strategy when distal control is compromised: stroke survivors have reduced accuracy of hip abduction and tend to widen step width to stabilize the stance phase [36]. In contrast, pelvic hike aligned with slower gait and longer double-support, stance, and swing times—patterns characteristic of more severe lower-limb paresis [37]. This suggests that pelvic hike functions as a compensatory elevation to overcome functional limb shortening from limited knee flexion [38].
Little et al. classified post-stroke patients by vertical and lateral pelvic displacement and reported that those with greater displacement had poorer lower-limb motor function and greater asymmetry in hip extension and ankle plantarflexion [39]. These individuals generated less paretic propulsion in late stance, resulting in reduced knee flexion in swing and greater reliance on pelvic hike to ensure foot clearance. The present findings are consistent with this compensatory pattern observed in more severe cases, reflecting an adaptive strategy to maintain foot clearance and stance stability when paretic propulsion and knee flexion are limited.
4.2. Longitudinal Changes in Gait: Context for Compensation Attenuation
Across the cohort, gait speed, stride length, and step length increased, whereas gait cycle time, double-support time, and paretic stance time decreased. These changes coincide with improvements in hip, knee, and ankle motor function and range of motion, suggesting a transition toward more typical gait patterns as paresis recovers.
Similar trends have been reported during 2–12 months post-stroke: gait speed and step length increase alongside rising Fugl-Meyer lower-limb scores, reflecting parallel gains in walking ability and motor recovery [40,41]. Continuous gait assessments during hospitalization have also linked increased trunk acceleration regularity and improved lower-limb extension in late stance with enhanced gait speed [42,43].
However, greater speed does not always signify true paretic-side recovery—improvement may arise from non-paretic propulsion [44]. Hence, frameworks distinguishing quantitative recovery (speed gain) from qualitative recovery (paretic-side functional return) have been proposed, emphasizing paretic propulsion as a key indicator [45]. In this context, our observed increases in speed and reduction in double-support time likely mark functional progress that forms the background for the concurrent attenuation of compensatory behaviors.
4.3. Temporal Changes in Paretic Femoral Abduction Angle and Its Relationship with Physical Function
Thigh abduction decreased over time and showed a negative association with improvements in paretic ankle motor function. This can be explained by two interacting mechanisms: Firstly, propulsive recovery – Improved plantar flexor activity enhances late-stance push-off, reducing the need for lateral abduction to achieve swing-phase clearance. Secondly, coordination recovery – Abnormal reflex coupling between the rectus femoris and gluteus medius can promote excessive abduction when ankle propulsion is weak [13,47]. With better ankle control, such abnormal synergy diminishes, and lateral compensation becomes unnecessary.
Thus, the attenuation of thigh abduction reflects both mechanical sufficiency and coordination refinement—a biomechanical normalization accompanying distal recovery.
4.4. Temporal Changes in Paretic Pelvic Hike and Its Relationship with Physical Function
Pelvic hike also decreased, and its change magnitude correlated negatively with improvement in paretic knee motor control. Interestingly, the pelvic hike was more strongly related to knee control than to static flexion amplitude, implying that hike compensates not just for limited knee flexion angle but for difficulties coordinating flexion–extension timing.
Previous research showed that functional limb shortening depends on both hip and knee contributions [15], and that circumduction cannot be fully explained by reduced knee flexion or ankle dorsiflexion alone [15,17]. Akbas et al. also reported that hip circumduction is not simply a substitute for limited knee flexion, emphasizing the role of intersegmental coordination [15]. Our results—linking pelvic hike more to motor function than to angle magnitude—concur with this view.
Additionally, the depth sensor used has known proportional error in knee flexion angle [26]; this may have weakened the angle-based correlations but does not negate the stronger link to motor recovery. Altogether, improvement in knee control likely facilitates smoother foot clearance, reducing reliance on pelvic elevation.
4.5. Limitation
This study has several limitations. First, the gait measurement was conducted within parallel bars, meaning the walking distance was short and potentially influenced by handrail use. Handrail use has been reported to increase paretic lower limb propulsion [49], and gait patterns might differ under free-walking conditions. Future studies should control for the effects of gait aids or measure gait without handrails.
Second, compensatory movements of the non-paretic lower limb were not fully considered. Stroke patients may compensate for foot clearance using non-paretic ankle plantarflexion or hip extension, the extent of which could alter the magnitude of paretic-side compensation [17]. Combining quantitative evaluation of non-paretic propulsion would clarify the overall picture of compensatory movements.
Third, the physical therapy content and frequency during the observation period were not standardized. The tendency for compensatory movements to increase or decrease may differ depending on the treatment content, highlighting the need for prospective longitudinal studies that control for intervention effects.
Fourth, due to the characteristics of the depth sensor used, proportional error exists in the paretic knee flexion angles [26]. Using an optical 3D motion analysis system would improve joint angle accuracy and enable a more precise evaluation of changes over time.
Fifth, we did not perform a kinetic assessment and thus did not directly examine kinetic factors such as propulsion or ground reaction forces. While kinetic evaluation poses challenges regarding safety and equipment constraints in acute patients, future research should consider introducing simplified measurement methods using wearable sensors or force plates.
Sixth, ankle joint angles were not quantitatively assessed. It is possible that recovery of paretic ankle dorsiflexion and plantarflexion improved foot clearance, consequently contributing to the decrease in paretic femoral abduction. Future studies should conduct multi-joint analyses including ankle angles to elucidate the factors behind compensatory movements in greater detail.
5. Conclusions
This study longitudinally investigated the changes over time in paretic femoral abduction and pelvic hike angles during gait in patients with acute stroke hemiparesis and clarified the relationship between these angles and lower limb motor function.
The results showed that both the paretic femoral abduction angle and paretic pelvic hike angle significantly decreased over time, confirming a reduction in compensatory movements during gait. Furthermore, the improvement in paretic ankle motor function showed a significant negative correlation with the decrease in the femoral abduction angle, and the improvement in paretic knee motor function showed a significant negative correlation with the decrease in the pelvic hike angle.
These results suggest that in patients with acute stroke hemiparesis, the recovery of paretic ankle and knee motor functions leads to a reduction in compensatory paretic femoral abduction and pelvic hike during gait. In other words, this indicates that as the functional propulsive force and knee flexion/extension control ability of the paretic lower limb recover, the dependence on compensatory movements such as femoral abduction and pelvic hike naturally decreases.
Author Contributions
Conceptualization, Y.S. and S.E.; methodology, R.S., Y.S., K.H., M.M. and S.E.; software, R.S., Y.S, K.H., D.O., and M.H.; validation, R.S., Y.S., and K.H.; formal analysis, R.S., Y.S., and K.H.; investigation, R.S., Y.S., and K.H.; resources, R.S., Y.S., D.O., and M.H.; data curation, R.S., Y.S., and K.H.; writing—original draft preparation, R.S., Y.S., and K.H.; writing—review and editing, R.S., Y.S., K.H., M.M., D.O.,M.H., and S.E.; supervision, S.E.; project administration, S.E.; funding acquisition, R.S. and Y.S.; All authors have read and agreed to the published version of the manuscript.
Funding
The Article Processing Charge (APC) for this publication was supported by the Tohoku University APC Support Project for Open Access Promotion, and this work was also supported by the Michinoku GAP Fund.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved in advance by the Ethics Committee of Tohoku university graduate school of medicine (approval number: 2024-1-032) and the Ethics Committee of the National Hospital Organization Sendai Medical Center (approval number: 24-12).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data, including graphs, within this paper are available from the corresponding author upon reasonable request.
Acknowledgments
We extend our deepest gratitude to the Department of Rehabilitation Medicine, Tohoku University Graduate School of Medicine, for their valuable advice and guidance throughout this study. We are also profoundly grateful to the members of the Neuro-Robotics Lab, Department of Robotics, Graduate School of Engineering, Tohoku University, for their assistance with the measurement and the Depth sensor activation and recording program, and for their support with the analysis program. Finally, we wish to thank the staff of the Department of Rehabilitation at Sendai Medical Center and all the participants who generously volunteered their time for this measurement.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Imanawanto, K., Andriana, M., & Satyawati, R. (2021). Correlation Between Joint Position Sense, Threshold To Detection of Passive Motion of The Knee Joint And Walking Speed of Post-Stroke Patient. International Journal of Research Publications, 83(1). [CrossRef]
- Mizuta, N., Hasui, N., Nakatani, T., Takamura, Y., Fujii, S., Tsutsumi, M., Taguchi, J., & Morioka, S. (2020). Walking characteristics including mild motor paralysis and slow walking speed in post-stroke patients. Scientific Reports, 10(1). [CrossRef]
- Odetunde, M. O., Makinde, A. F., Jimoh, O. M., Mbada, C. E., Niyi-Odumosu, F., & Fatoye, F. (2025). Physical activity, fatigue severity, and health-related quality of life of community-dwelling stroke survivors: a cross-sectional study. Bulletin of Faculty of Physical Therapy, 30(1). [CrossRef]
- Balbinot, G., Schuch, C. P., Oliveira, H. B., & Peyré-Tartaruga, L. A. (2020). Mechanical and energetic determinants of impaired gait following stroke: segmental work and pendular energy transduction during treadmill walking. Biology Open, 9(7). [CrossRef]
- Fulk, G. D., He, Y., Boyne, P., & Dunning, K. (2017). Predicting Home and Community Walking Activity Poststroke. Stroke, 48(2), 406–411. [CrossRef]
- Ribeiro, J. A. M., Oliveira, S. G., di Thommazo-Luporini, L., Phillips, S. A., Catai, A. M., Borghi-Silva, A., Ribeiro, J. A. M., Oliveira, S. G., di Thommazo-Luporini, L., Monteiro, C. I., Phillips, S. A., Catai, A. M., Borghi-Silva, A., & Russo, T. L. (2019). Energy Cost During the 6-Minute Walk Test and Its Relationship to Real-World Walking After Stroke: A Correlational, Cross-Sectional Pilot Study. https://academic.oup.com/ptj.
- Ardestani, M. M., Kinnaird, C. R., Henderson, C. E., & Hornby, T. G. (2019). Compensation or Recovery? Altered Kinetics and Neuromuscular Synergies Following High-Intensity Stepping Training Poststroke. Neurorehabilitation and Neural Repair, 33(1), 47–58. [CrossRef]
- Kerrigan, D. Casey, Frates, Elizabeth P, Rogan, Shannon BS; Riley, Patrick O.(2000). Hip Hiking and Circumduction Quantitative Definitions. American Journal of Physical Medicine & Rehabilitation, 79 (3) 247-252.
- Chen, G., Patten, C., Kothari, D. H., & Zajac, F. E. (2005). Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait and Posture, 22(1), 51–56. [CrossRef]
- Awad, L. N., Bae, J., Kudzia, P., Long, A., Hendron, K., Holt, K. G., OʼDonnell, K., Ellis, T. D., & Walsh, C. J. (2017). Reducing Circumduction and Hip Hiking During Hemiparetic Walking Through Targeted Assistance of the Paretic Limb Using a Soft Robotic Exosuit. American Journal of Physical Medicine & Rehabilitation, 96(10), S157–S164. [CrossRef]
- Mahtani, G. B., Kinnaird, C. R., Connolly, M., Holleran, C. L., Hennessy, P. W., Woodward, J., Brazg, G., Roth, E. J., & Hornby, T. G. (2017). Altered Sagittal-and Frontal-Plane Kinematics Following High-Intensity Stepping Training Versus Conventional Interventions in Subacute Stroke Background. Common locomotor deficits observed in people poststroke include. In Original Research (Vol. 320). https://academic.oup.com/ptj.
- Zissimopoulos, A., Fatone, S., & Gard, S. (2015). Effects of ankle-foot orthoses on mediolateral foot-placement ability during post-stroke gait. Prosthetics and Orthotics International, 39(5), 372–379. [CrossRef]
- Akbas, T., Neptune, R. R., & Sulzer, J. (2019). Neuromusculoskeletal simulation reveals abnormal rectus femoris-gluteus medius coupling in post-stroke gait. Frontiers in Neurology, 10(APR). [CrossRef]
- Stanhope, V. A., Knarr, B. A., Reisman, D. S., & Higginson, J. S. (2014). Frontal plane compensatory strategies associated with self-selected walking speed in individuals post-stroke. Clinical Biomechanics, 29(5), 518–522. [CrossRef]
- Akbas, T., Prajapati, S., Ziemnicki, D., Tamma, P., Gross, S., & Sulzer, J. (2019). Hip circumduction is not a compensation for reduced knee flexion angle during gait. Journal of Biomechanics, 87, 150–156. [CrossRef]
- Tamaya, V. C., Wim, S., Herssens, N., van de Walle, P., Willem, D. H., Steven, T., & Ann, H. (2020). Trunk biomechanics during walking after sub-acute stroke and its relation to lower limb impairments. Clinical Biomechanics, 75. [CrossRef]
- Lee, J., Seamon, B. A., Lee, R. K., Kautz, S. A., Neptune, R. R., & Sulzer, J. S. (2025). Post-stroke Stiff-Knee gait: are there different types or different severity levels? Journal of NeuroEngineering and Rehabilitation, 22(1). [CrossRef]
- Akbas, T., Kim, K., Doyle, K., Manella, K., Lee, R., Spicer, P., Knikou, M., & Sulzer, J. (2020). Rectus femoris hyperreflexia contributes to Stiff-Knee gait after stroke. Journal of NeuroEngineering and Rehabilitation, 17(1). [CrossRef]
- Han, X., Guffanti, D., & Brunete, A. (2025). A Comprehensive Review of Vision-Based Sensor Systems for Human Gait Analysis. In Sensors (Vol. 25, Issue 2). Multidisciplinary Digital Publishing Institute (MDPI). [CrossRef]
- Microsoft. Available online:https://www.microsoft.com/ja-JP/d/azure-kinect-dk/8pp5vxmd9nhq?activetab=pivot:%E6%A6%82%E8%A6%81tab (accessed on 20 October 2025).
- Bawa, A., Banitsas, K., & Abbod, M. (2021). A Review on the Use of Microsoft Kinect for Gait Abnormality and Postural Disorder Assessment. Journal of Healthcare Engineering, 2021, 1–19. [CrossRef]
- Sugai, R., Maeda, S., Shibuya, R., Sekiguchi, Y., Izumi, S. I., Hayashibe, M., & Owaki, D. (2023). LSTM Network-Based Estimation of Ground Reaction Forces during Walking in Stroke Patients Using Markerless Motion Capture System. IEEE Transactions on Medical Robotics and Bionics, 5(4), 1016–1024. [CrossRef]
- Koo, T. K., & Li, M. Y. (2016). A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. Journal of Chiropractic Medicine, 15(2), 155–163. [CrossRef]
- Eltoukhy, M., Oh, J., Kuenze, C., & Signorile, J. (2017). Improved kinect-based spatiotemporal and kinematic treadmill gait assessment. Gait and Posture, 51, 77–83. [CrossRef]
- Eltoukhy, M., Kuenze, C., Oh, J., Jacopetti, M., Wooten, S., & Signorile, J. (2017). Microsoft Kinect can distinguish differences in over-ground gait between older persons with and without Parkinson’s disease. Medical Engineering and Physics, 44, 1–7. [CrossRef]
- Shibuya, R. (2023). Verification of the reliability of gait data for patients with hemiparesis measured by a depth sensor [Unpublished master's thesis]. Department of Disability Science, Graduate School of Medicine, Tohoku University.
- Kazuhisa Domen (1995) Consistency and validity of the Stroke Impairment Assessment Set (SIAS) in hemiplegic stroke patients (1) -Motor function, muscle tone, tendon reflexes, and healthy side function on the paretic side Rehabilitation Medicine, 32(2), 113-122.
- Sonoda, Shigeru (1995) Consistency and validity of the Stroke Impairment Assessment Set (SIAS) for functional assessment of hemiplegic stroke patients (2) - Trunk, higher brain function, sensory items and outcome prediction Rehabilitation Medicine, 32(2), 123-132.
- Yeh, T. ting, Chang, K. chou, & Wu, C. yi. (2019). The Active Ingredient of Cognitive Restoration: A Multicenter Randomized Controlled Trial of Sequential Combination of Aerobic Exercise and Computer-Based Cognitive Training in Stroke Survivors With Cognitive Decline. Archives of Physical Medicine and Rehabilitation, 100(5), 821–827. [CrossRef]
- Kharazi, M. R., Memari, A. H., Shahrokhi, A., Nabavi, H., Khorami, S., Rasooli, A. H., Barnamei, H. R., Jamshidian, A. R., & Mirbagheri, M. M. (2016). Validity of microsoft kinectTM for measuring gait parameters. 2015 22nd Iranian Conference on Biomedical Engineering, ICBME 2015, 375–379. [CrossRef]
- Tölgyessy, M., Dekan, M., Chovanec, Ľ., & Hubinský, P. (2021). Evaluation of the azure kinect and its comparison to kinect v1 and kinect v2. Sensors (Switzerland), 21(2), 1–25. [CrossRef]
- J. Zeni, J. Richards, J. Higginson, Two simple methods for determining gait events during treadmill and overground walking using kinematic data, Gait Posture 27 (2008) 710–714.
- Rose, J., Gamble, J.G., 2006. Human walking. Lippincott Williams & Wilkins, Philadelphia, pp. 33–51.
- Kinsella, S., & Moran, K. (2008). Gait pattern categorization of stroke participants with equinus deformity of the foot. Gait and Posture, 27(1), 144–151. [CrossRef]
- Chan, Y. H. (2003). Biostatistics 104: Correlational analysis. Singapore Medical Journal, 44(12), 614–619.
- Dean, J. C., Embry, A. E., Stimpson, K. H., Perry, L. A., & Kautz, S. A. (2017). Effects of hip abduction and adduction accuracy on post-stroke gait. Clinical Biomechanics, 44, 14–20. [CrossRef]
- Wang, Y., Mukaino, M., Ohtsuka, K., Otaka, Y., Tanikawa, H., Matsuda, F., Tsuchiyama, K., Yamada, J., & Saitoh, E. (2020). Gait characteristics of post-stroke hemiparetic patients with different walking speeds. International Journal of Rehabilitation Research, 43(1), 69–75. [CrossRef]
- Haruyama, K., Kawakami, M., Okada, K., Okuyama, K., Tsuzuki, K., & Liu, M. (2021). Pelvis-toe distance: 3-dimensional gait characteristics of functional limb shortening in hemiparetic stroke. Sensors, 21(16). [CrossRef]
- Little, V. L., McGuirk, T. E., Perry, L. A., & Patten, C. (2018). Pelvic excursion during walking post-stroke: A novel classification system. Gait and Posture, 62, 395–404. [CrossRef]
- Kwakkel, G., van Peppen, R., Wagenaar, R. C., Dauphinee, S. W., Richards, C., Ashburn, A., Miller, K., Lincoln, N., Partridge, C., Wellwood, I., & Langhorne, P. (2004). Effects of augmented exercise therapy time after stroke: A meta-analysis. Stroke, 35(11), 2529–2536. [CrossRef]
- Patterson, K. K., Parafianowicz, I., Danells, C. J., Closson, V., Verrier, M. C., Staines, W. R., Black, S. E., & McIlroy, W. E. (2008). Gait Asymmetry in Community-Ambulating Stroke Survivors. Archives of Physical Medicine and Rehabilitation, 89(2), 304–310. [CrossRef]
- Mizuike, C., Ohgi, S., & Morita, S. (2009). Analysis of stroke patient walking dynamics using a tri-axial accelerometer. Gait & Posture, 30(1), 60–64. [CrossRef]
- Kettlety, S. A., Finley, J. M., Reisman, D. S., Schweighofer, N., & Leech, K. A. (2023). Speed-dependent biomechanical changes vary across individual gait metrics post-stroke relative to neurotypical adults. Journal of NeuroEngineering and Rehabilitation, 20(1). [CrossRef]
- Awad, L. N., Palmer, J. A., Pohlig, R. T., Binder-Macleod, S. A., & Reisman, D. S. (2015). Walking speed and step length asymmetry modify the energy cost of walking after stroke. Neurorehabilitation and Neural Repair, 29(5), 416–423. [CrossRef]
- Balasubramanian, C. K., Bowden, M. G., Neptune, R. R., & Kautz, S. A. (2007). Relationship Between Step Length Asymmetry and Walking Performance in Subjects With Chronic Hemiparesis. Archives of Physical Medicine and Rehabilitation, 88(1), 43–49. [CrossRef]
- Awad, L. N., Lewek, M. D., Kesar, T. M., Franz, J. R., & Bowden, M. G. (2020). These legs were made for propulsion: advancing the diagnosis and treatment of post-stroke propulsion deficits. In Journal of NeuroEngineering and Rehabilitation (Vol. 17, Issue 1). BioMed Central Ltd. [CrossRef]
- Little, V. L., McGuirk, T. E., & Patten, C. (2014). Impaired Limb Shortening following Stroke: What’s in a Name? PLoS ONE, 9(10), e110140. [CrossRef]
- Sánchez, N., Acosta, A. M., López-Rosado, R., & Dewald, J. P. A. (2018). Neural constraints affect the ability to generate hip abduction torques when combined with hip extension or ankle plantarflexion in chronic hemiparetic stroke. Frontiers in Neurology, 9(JUL). [CrossRef]
- Hinton, E. H., Bierner, S., Reisman, D. S., Likens, A., & Knarr, B. A. (2024). Paretic propulsion changes with handrail Use in individuals post-stroke. Heliyon, 10(5). [CrossRef]
Figure 1.
(a) Depth sensor; (b) Measurement environment and analysis section.
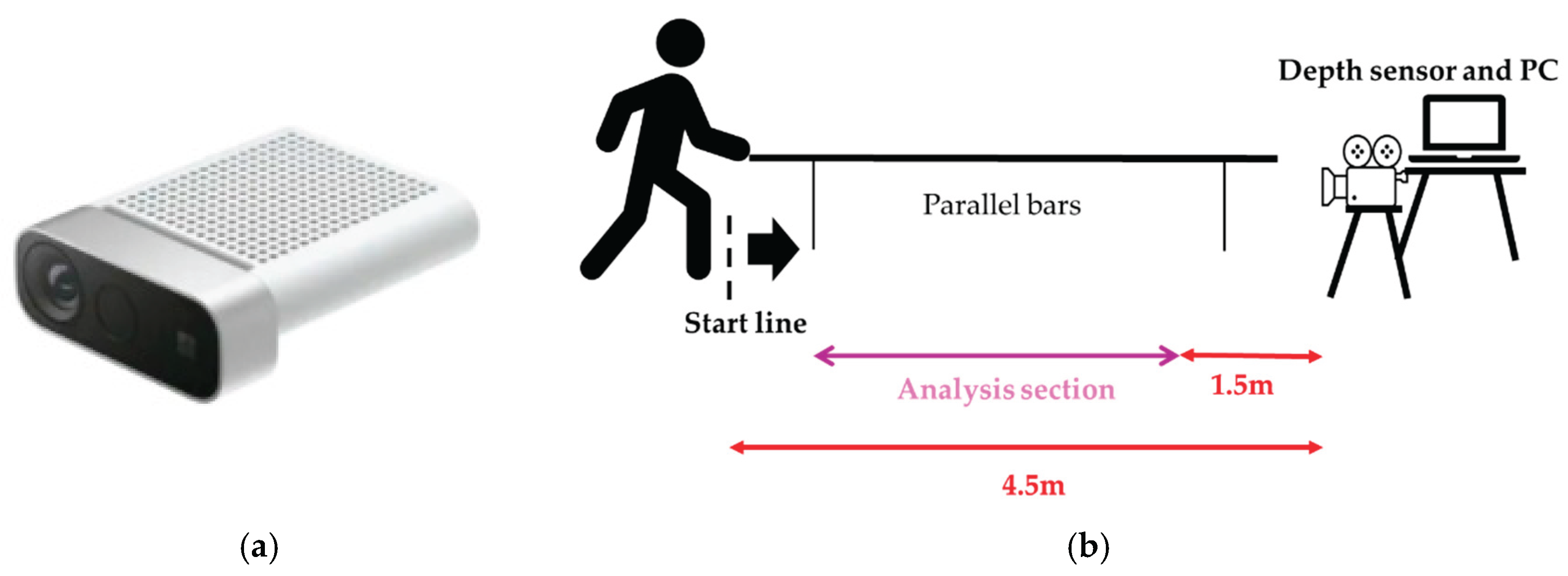
Figure 3.
(a) The figure shows the evaluator holding a shielding plate as viewed from the frontal plane.; (b) This is a diagram showing the evaluator holding a shielding plate as viewed from the sagittal plane.
Figure 3.
(a) The figure shows the evaluator holding a shielding plate as viewed from the frontal plane.; (b) This is a diagram showing the evaluator holding a shielding plate as viewed from the sagittal plane.
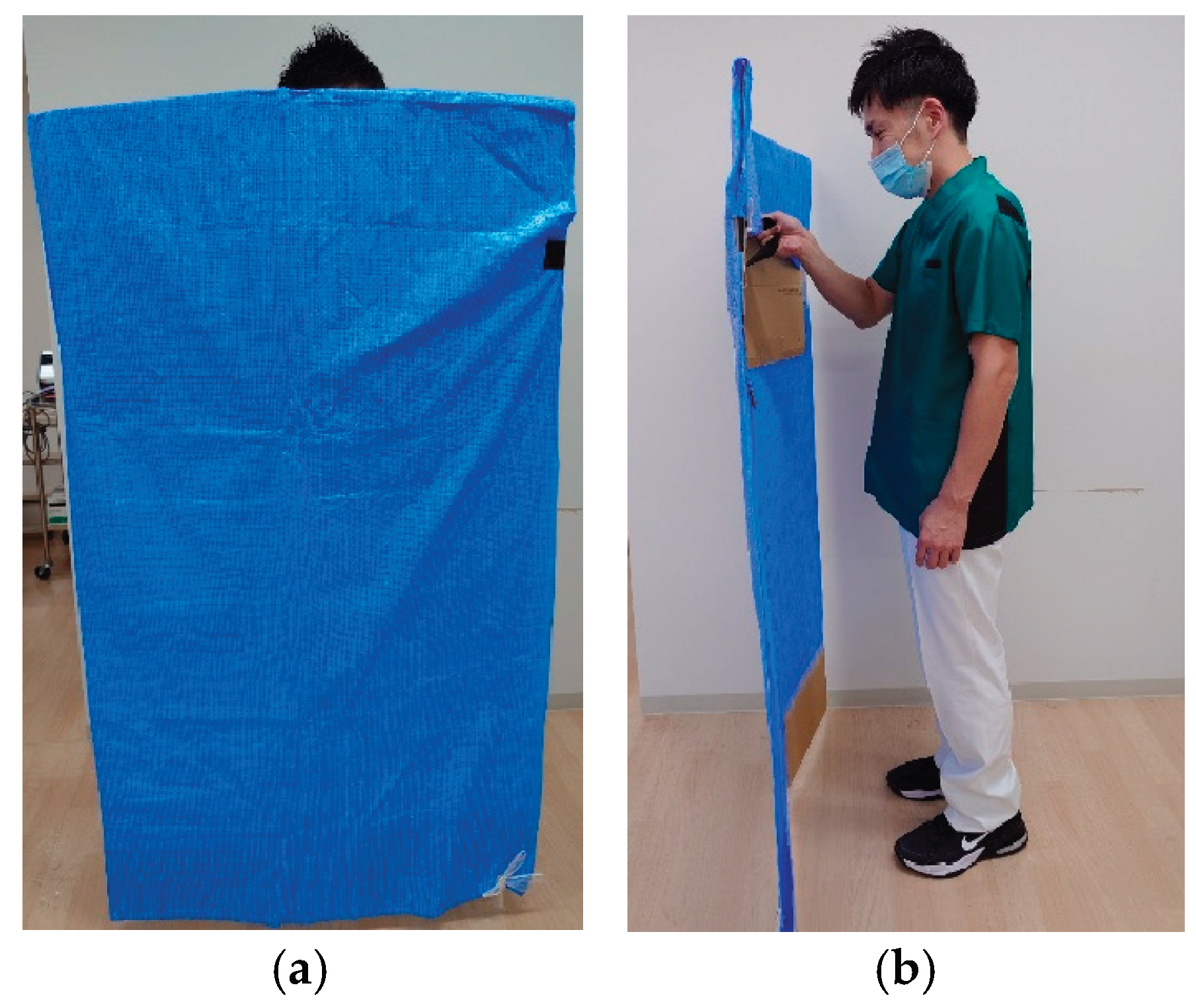
Figure 4.
Representative temporal changes in the paretic femoral abduction angle during one gait cycle in an acute stroke patient. The blue and orange lines indicate data from the initial and second assessments, respectively. Solid line segments represent the mid-swing phase, while dashed line segments represent other phases.
Figure 4.
Representative temporal changes in the paretic femoral abduction angle during one gait cycle in an acute stroke patient. The blue and orange lines indicate data from the initial and second assessments, respectively. Solid line segments represent the mid-swing phase, while dashed line segments represent other phases.
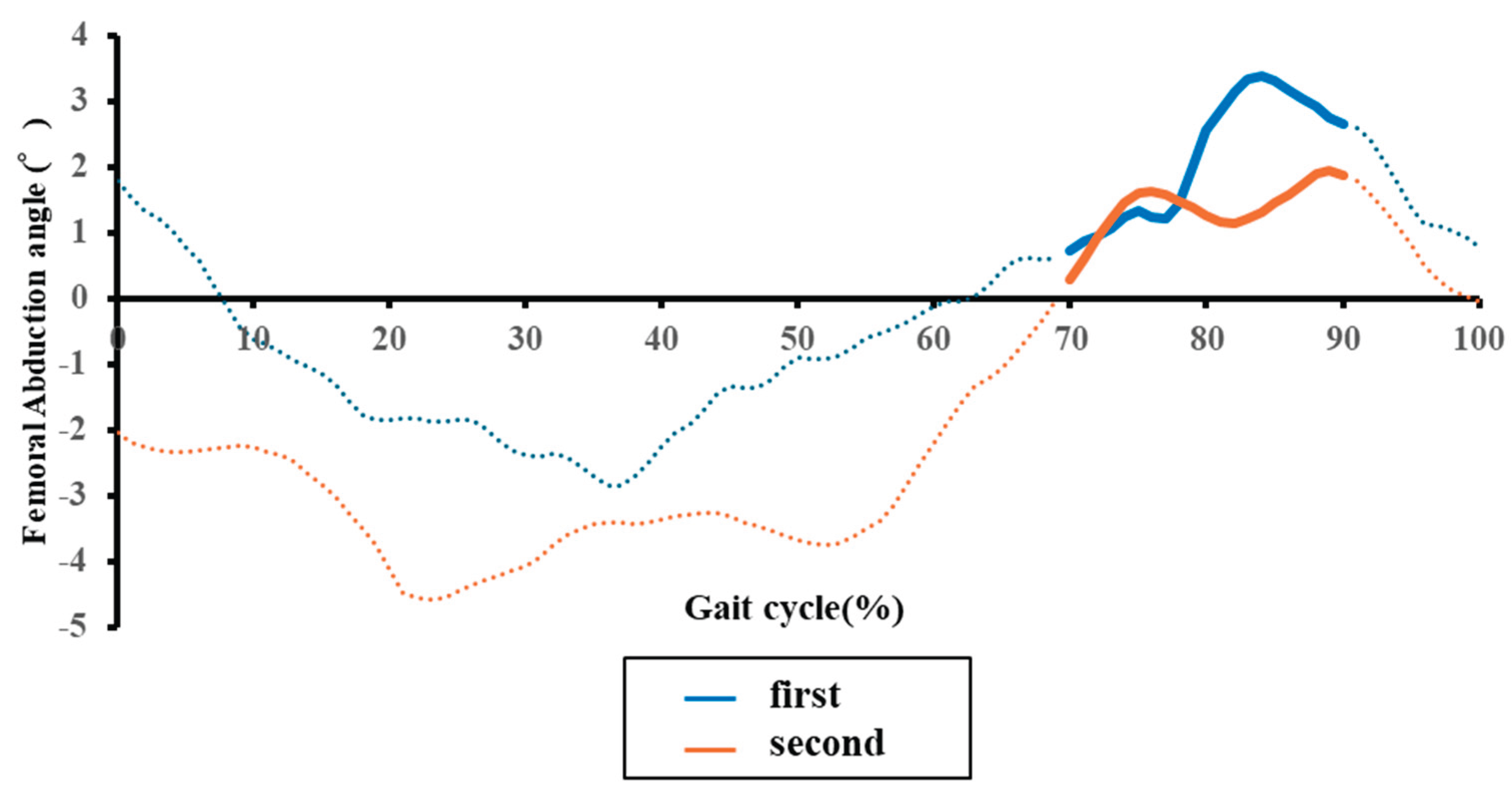
Table 1.
Characteristics of stroke patients.
| Stroke patients | |||||
|---|---|---|---|---|---|
| Gender (male/female) a | 17/5 | ||||
| Age (year)b | 66.05 | (15.44) | |||
| Height (m)b | 1.65 | (0.08) | |||
| Weight (kg)b | 68.43 | (15.43) | |||
| Diagnosis (Hemorrhage/Infarction) a | 5/17 | ||||
| Paretic side (left/right) a | 14/8 | ||||
| Time since onset (days)b | 8.77 | (5.27) | |||
| Physical therapy time during longitudinal period (minutes) |
25.72 | (7.68) | |||
| a Number of people | |||||
| b Mean (Standard deviation) | |||||
Table 4.
Changes in gait parameters over time.
| Spatiotemporal parameters | Initial assessment | Second assessment | Effect size | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Gait speed (m/sec) a | 0.38 | (0.16) | 0.53 | 0.18 | -1.181 | < 0.001 | |||
| Gait cycle time (sec)a | 1.99 | (0.68) | 1.60 | 0.42 | 0.882 | < 0.001 | |||
| Double stance time (sec)b | 0.49 | (0.23) | 0.35 | 0.18 | 0.878 | < 0.001 | |||
| Paretic stance time (sec)a | 1.44 | (0.54) | 1.10 | 0.34 | -0.792 | < 0.001 | |||
| Paretic swing time (sec)b | 0.53 | (0.16) | 0.48 | 0.11 | -0.415 | 0.051 | |||
| Non-paretic swing time (sec)b | 0.45 | (0.08) | 0.42 | 0.05 | -0.391 | 0.067 | |||
| Stride length on the paretic side (m)a | 0.66 | (0.15) | 0.78 | 0.14 | -1.081 | < 0.001 | |||
| Step length on the paretic side (m)a | 0.31 | (0.08) | 0.36 | 0.07 | -0.720 | 0.003 | |||
| Step length on the non-paretic side (m)a | 0.29 | (0.08) | 0.35 | 0.08 | -1.022 | < 0.001 | |||
| Step width (m)a | 0.13 | (0.03) | 0.12 | 0.04 | 0.2999 | 0.174 | |||
| Paretic femoral abduction angle (°) a | 6.71 | (3.78) | 5.79 | 3.47 | 0.513 | 0.049 | |||
| Paretic pelvic hike angle (°) a | 3.82 | (2.34) | 2.90 | 2.35 | 0.513 | 0.025 | |||
| H1 (°) b | 23.18 | (5.67) | 23.93 | 4.30 | -0.174 | 0.424 | |||
| H2 (°) a | 23.20 | (5.40) | 24.02 | 4.29 | -0.197 | 0.367 | |||
| H3 (°) a | -3.89 | (6.17) | -5.91 | 5.13 | 0.417 | 0.064 | |||
| H4 (°) a | 5.52 | (7.12) | 4.69 | 5.76 | 0.139 | 0.521 | |||
| H5 (°) a | 24.28 | (6.79) | 25.55 | 5.49 | -0.245 | 0.263 | |||
| H6 (°) a | 29.59 | (5.42) | 32.32 | 5.43 | -0.469 | 0.039 | |||
| K1 (°) a | 9.93 | (5.16) | 8.58 | 5.23 | 0.342 | 0.124 | |||
| K2 (°) a | 15.15 | (4.80) | 15.09 | 6.20 | 0.010 | 0.963 | |||
| K3 (°) a | 5.65 | (3.16) | 5.96 | 4.40 | -0.132 | 0.543 | |||
| K4 (°) a | 35.24 | (10.95) | 37.74 | 8.89 | -0.358 | 0.108 | |||
| K5 (°) a | 46.65 | (11.67) | 50.87 | 10.82 | -0.513 | 0.026 | |||
| K6 (°) a | 41.82 | (10.73) | 45.84 | 9.77 | -0.479 | 0.036 | |||
| Mean (Standard deviation) a Paired t-test (p < 0.05) b Wilcoxon signed-rank test (p < 0.05) | |||||||||
Table 5.
Changes in physical function assessment over time.
| SIAS evaluation items | First assessment | Second assessment | Effect size | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Hip joint (0/1/2/3/4/5) a | 1/0/6/7/8/0 | (4-2) | 0/0/3/3/9/7 | (5-3.25) | -0.82 | < 0.001 | |||
| Knee joint (0/1/2/3/4/5) a | 1/1/3/5/9/3 | (4-3) | 0/0/2/5/8/7 | (5-3) | -0.58 | 0.006 | |||
| Ankle joint (0/1/2/3/4/5) a | 2/2/5/4/5/4 | (4-2) | 1/3/0/3/6/9 | (5-3) | -0.74 | < 0.001 | |||
| L/E Deep tendon reflex (0/1/2/3) a | 2/13/6/1 | (2-1) | 3/6/11/2 | (2-1) | -0.30 | 0.153 | |||
| L/E muscle tone (0/1/2/3) a | 0/4/10/8 | (3-2) | 0/2/9/11 | (3-2) | -0.30 | 0.160 | |||
| Superficial sensation (0/1/2/3) a | 2/0/2/18 | (3-3) | 0/2/1/19 | (3-3) | -0.37 | 0.083 | |||
| Deep sensation (0/1/2/3) a | 2/0/2/18 | (3-3) | 0/2/0/20 | (3-3) | -0.42 | 0.046 | |||
| Ankle joint range of motion (0/1/2/3) a | 0/0/13/9 | (3-2) | 0/0/10/12 | (3-2) | -0.21 | 0.317 | |||
| Abdominal strength (0/1/2/3) a | 8/7/6/3 | (2-0) | 0/5/8/9 | (3-2) | -0.66 | 0.002 | |||
| SIAS: Stroke impairment assessment set (Interquartile range) L/E: Lower extremity a Wilcoxon signed-rank test (p < 0.05) | |||||||||
Table 6.
Correlations between changes in compensatory movements and gait parameters.
| Spatiotemporal and kinematic variables | Mean (SD) | Paretic side femoral abduction angle |
Paretic side pelvic hike angle |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Correlation | p-value | Correlation | p-value | |||||||
| Gait speed Δ (m/sec) a | 0.15 | (0.13) | 0.09 | 0.701 | 0.03 | 0.886 | ||||
| Gait cycle time Δ (sec)b | -0.39 | (0.44) | -0.05 | 0.809 | 0.23 | 0.299 | ||||
| Double stance time Δ (sec)a | -0.14 | (0.16) | -0.24 | 0.290 | 0.12 | 0.609 | ||||
| Paretic stance time Δ (sec)b | -0.34 | (0.34) | -0.19 | 0.393 | 0.10 | 0.661 | ||||
| Paretic swing time Δ (sec)b | -0.05 | (0.13) | 0.32 | 0.148 | 0.41 | 0.058 | ||||
| Non-paretic swing time Δ (sec)b | -0.03 | (0.07) | -0.18 | 0.428 | -0.05 | 0.828 | ||||
| Paretic stride length Δ (m)a | 0.12 | (0.11) | 0.03 | 0.881 | 0.00 | 0.996 | ||||
| Paretic step length Δ (m)a | 0.04 | (0.06) | -0.03 | 0.892 | 0.15 | 0.517 | ||||
| Non-paretic step length Δ (m)a | 0.05 | (0.05) | 0.12 | 0.586 | -0.02 | 0.935 | ||||
| Step width Δ (m) a | -0.01 | (0.03) | -0.22 | 0.332 | 0.12 | 0.604 | ||||
| Paretic pelvic hike Δ (°) a | -0.91 | (1.74) | 0.55 | 0.008 | - | - | ||||
| H1Δ (°) b | 0.75 | (4.33) | -0.31 | 0.154 | -0.32 | 0.148 | ||||
| H2Δ (°) a | 0.83 | (4.20) | -0.34 | 0.118 | -0.27 | 0.221 | ||||
| H3Δ (°) a | -2.02 | (4.84) | -0.03 | 0.886 | -0.14 | 0.545 | ||||
| H4Δ (°) a | -0.83 | (5.99) | 0.02 | 0.938 | -0.14 | 0.540 | ||||
| H5Δ (°) a | 1.27 | (5.19) | -0.13 | 0.557 | -0.13 | 0.557 | ||||
| H6Δ (°) a | 2.73 | (5.82) | -0.09 | 0.679 | 0.02 | 0.936 | ||||
| K1Δ (°) a | -1.35 | (3.94) | -0.09 | 0.690 | -0.25 | 0.271 | ||||
| K2Δ (°) a | -0.06 | (5.98) | -0.23 | 0.311 | -0.13 | 0.569 | ||||
| K3Δ (°) a | 0.31 | (2.38) | -0.36 | 0.096 | -0.22 | 0.324 | ||||
| K4Δ (°) a | 2.49 | (6.96) | 0.26 | 0.247 | 0.03 | 0.894 | ||||
| K5Δ (°) a | 4.22 | (8.24) | 0.10 | 0.660 | 0.09 | 0.700 | ||||
| K6Δ (°) a | 4.02 | (8.40) | 0.19 | 0.388 | 0.13 | 0.573 | ||||
| SD: Standard deviation a Pearson's correlation coefficient (p < 0.05) b Spearman's rank correlation coefficient (p < 0.05) | ||||||||||
Table 7.
Correlations between changes in compensatory movements and physical function assessment items.
Table 7.
Correlations between changes in compensatory movements and physical function assessment items.
| SIAS evaluation items | Median (IQR) |
Paretic side femoral abduction angle |
Paretic side pelvic hike angle |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Correlation | p-value | Correlation | p-value | |||||||
| Hip joint Δ b | 1 | (1-1) | 0.42 | 0.050 | -0.20 | 0.371 | ||||
| Knee joint Δ b | 0 | (1-0) | -0.28 | 0.203 | -0.43 | 0.046 | ||||
| Ankle joint Δ b | 1 | (1-0) | -0.49 | 0.021 | -0.01 | 0.962 | ||||
| L/E deep tendon reflex Δ b | 0 | (1-0) | -0.34 | 0.121 | -0.13 | 0.566 | ||||
| L/E muscle tone Δ b | 0 | (0.00) | 0.01 | 0.969 | -0.31 | 0.161 | ||||
| L/E superficial sensation Δ b | 0 | (0.00) | -0.16 | 0.487 | -0.03 | 0.888 | ||||
| L/E deep sensation Δ b | 0 | (0.00) | 0.02 | 0.935 | 0.13 | 0.559 | ||||
| Ankle joint range of motion Δ b | 0 | (0.75-0) | 0.32 | 0.149 | 0.09 | 0.681 | ||||
| Abdominal strength Δ b | 1 | (1.75-0) | -0.11 | 0.614 | -0.20 | 0.365 | ||||
| IQR: Interquartile range L/E: Lower extremity b Spearman's rank correlation coefficient (p < 0.05) | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



