
Submitted:
23 October 2025
Posted:
24 October 2025
You are already at the latest version
Abstract
(1) Background: The squat is a compound exercise used in sports, physiotherapy, and activities of daily living. Posterior pelvic tilt during the squat, commonly referred to as “butt wink” can potentially increase the risk of spine injury when performing a squat with posterior pelvic tilt. The main goal of this study is to objectively assess the immediate effect of the exercise intervention on the total pelvis range of motion in the sagittal plane (mainly posterior pelvic tilt) during squat. The secondary aim is to determine the relationship between the initial pelvic position and the occurrence of posterior pelvic tilt; (2) Methods: The study is a controlled experiment with 42 participants (21 females and 21 males) divided into an experimental group (n = 23) and a control group (n = 19). The division was made according to the incidence of posterior pelvic tilt during the performance of the bodyweight squat. A baseline measurement that included three-dimensional kinematic motion analysis and a physiotherapy examination and an outcome measurement that included only three-dimensional kinematic motion analysis were performed. Both groups underwent a twenty-minute exercise intervention aimed at strengthening stabilizing muscles, improving squat technique and body awareness in space. Data from the three-dimensional kinematic motion analysis were statistically processed using Restricted Maximum Likelihood analysis (REML) of linear mixed models and repeated measures analysis of variance (rANOVA); (3) Results: There was no statistically significant difference in the range of motion of posterior pelvic tilt before and after the exercise intervention (p = 0.89 and p = 0.42). Only the individual repetitions of the squat were statistically significantly different from each other (p < 0.001) and no statistically significant relationship between posterior pelvic tilt and initial pelvic position was found (p = 0.13); (4) Conclusions: The short exercise intervention did not affect the range of motion of posterior pelvic tilt during squatting, but it is still worth investigating this issue further and looking for possible associations between different variables of squat execution and the incidence of posterior pelvic tilt.
Keywords:
butt wink
; exercise intervention
; kinematic motion analysis
; posterior pelvic tilt
; squat
1. Introduction
The squat is considered a compound exercise used in a variety of sports. It is also a part of physiotherapy/rehabilitation for various musculoskeletal conditions and is also a common movement stereotype of the human species [1,2,3]. The squat is commonly used to develop speed, strength and muscle hypertrophy, particularly in the extensor muscles of the knee and hip joints and should therefore be included in training for variety of sports, e.g., basketball, gymnastics, long jump, shot put, swimming etc., because changes in these areas will subsequently show up in improved performance such as sprinting or jumping [1,4,5].
Squat safety involves a number of factors, including warm-up, proper footwear, and most importantly, a proper squat technique [6]. And this is where we have seen a discussion over the last decade or so on the topic of posterior pelvic tilt (PPT) in the squat, colloquially known as the “butt wink” [7,8,9]. The term PPT generally refers to the posterior position or movement of the pelvis in the sagittal plane, with lumbar lordosis flattening or even becoming kyphotic and thoracic kyphosis increasing eventually leading to hyperkyphosis, depending on the degree of PPT [10,11]. In terms of squatting, PTT refers to a movement that occurs during a deep squat, with the pelvis moving below the thigh axis during the descending phase of a squat. It is sometimes reported to be quite common phenomenon, but if the degree of PPT is excessive and/or occurs prior to parallel squat depth, it can potentially increase the risk of lumbar spine injury [9,12].
Lumbar spine injury, specifically the risk of disc herniation is reported to increase, especially during flexion of the entire trunk or the combination of flexion and rotation, when the disc is deformed and the pressure in the lower part of the disc increases, which can lead to herniation. Muscle and ligament strains also occur in these flexion positions [13,14]. However, according to the recommendations of Contreras & Schoenfeld [15], it is not necessary to strictly prohibit any flexion movements/exercise of the spine; in contrast, if performed in a controlled manner and with an adequate loading, they can be beneficial, provided that the athlete does not already have a certain level of degenerative changes (e.g., disc herniation). Yet, the process of developing these degenerative changes is very complex, and in addition to the standard mechanical factors, genetic, age, and nutritional factors also play a role. We also know that regular strength training leads to gradual tissue adaptation and that experienced strength athletes (1–2 years of regular training) have a greater amount of mineralized bone tissue than a comparable population without strength training. Also, there was no higher incidence of degenerative changes or spinal injuries in these strength athletes compared to the non-exercising population [16].
The above opinions are consistent with those of other authors [6,17,18] who claim that squats themselves are no more dangerous than other exercises, but see the main problem, in terms of injury, in the inadequate load used during squat and poor squatting technique, or adding load quickly while not mastering proper squatting technique. We must not also forget the factor of fatigue, especially when trying to determine one repetition maximum (1RM), where the benefit of knowing the 1RM doesn’t necessarily outweigh the potential risk of injury.
The commonly reported causes of PPT during squat are as follow: anatomical predisposition, limited range of motion (ROM) in the hip and ankle joints, impaired function of the core muscles or impaired neuromuscular control in the lumbar spine and pelvis, and a suboptimal starting squat position in terms of excessive anterior pelvic tilt and lumbar hyperlordosis. The cause may also be simply poor instruction given to the athlete on how to hold the trunk and pelvis during squat. At the same time, it is important to remember that not every athlete can achieve full squat depth, mainly due to individual anatomical differences. If we take a very brief look at the individual causes, femoroacetabular impingement syndrome (FAI) is often discussed in relation to anatomical predispositions. It is a condition of the hip joint that occurs as a result of physiological movement in the hip joint, most often caused by an incorrect shape or orientation of the articulating joint surfaces. There is evidence that FAI alters the squat technique. In general, authors agree that FAI causes a change in pelvic positioning, limits ROM in flexion and internal rotation at the hip joint, and decreases squat depth and velocity of the descent phase of the squat [19,20,21,22,23].
Limited hip flexion ROM may be one of the main limiting factors in achieving a technically correct deep squat [24,25,26]. PPT occurs when the maximum possible hip flexion ROM is exhausted and is associated with flexion of the lumbar spine, which increases compression and shear forces in this region [9,27]. Limited dorsiflexion at the ankle can be also a limiting factor in proper squat performance [24,25,26,28,29,30,31]. According to Breen et al. [24] when testing the deep squat within the Functional Movement Screen, individuals with limited dorsiflexion showed lower scores in the quality of squat performance (either inability to perform the squat as instructed or performance with some compensation) than participants with full ROM. Comfort et al. [17] reports, there is a relationship between limited dorsiflexion at the ankle and increased forward leaning of the trunk. Schoenfeld [31] adds, that the ROM for dorsiflexion for full squat performance should be 38.5±5.9°, otherwise this limited ankle dorsiflexion can cause compensatory movements in the knee and hip joints or spine, potentially increasing the risk of injury at higher loads. And finally, according to Kim et al. [26] the dorsiflexion ROM, along with the hip flexion ROM, is one of the main parameters for achieving an appropriate squat depth in males, while in females it is the dorsiflexion ROM and the strength of the dorsal flexors.
The position of the pelvis when squatting is important for both safety and maximum performance. It is advisable to maintain proper pelvic position to maintain neutral lumbar lordosis (to reduce the risk of injury). Excessive anterior pelvic tilt can cause low back pain and excessive PPT can reduce the maximum performance during the squat. Ensuring proper pelvic alignment not only increases the effectiveness of strength training, but also minimizes the risk of injury [32]. Other authors have a similar view and recommend maintaining a neutral or slight anterior pelvic tilt position to minimize excessive lumbar motion, so it is desirable to avoid excessive flexion and extension [9,33,34,35,36,37,38,39,40,41,42,43,44,45,46]. In the deepest squat position, i.e., maximum flexion at the knee and hip joints, the pelvis is indeed in PPT, the lumbar lordosis is flattened (11.7° in squat vs. 32.9° in standing), and the sacrum is vertical [37]. We cannot overlook the anatomical differences between women and men, as we know, that execution of the squat may differ slightly between men and women. The sacrum is slightly longer in men than in women, but not as wide. Overall, the female pelvis is wider and more oval, and the lumbar vertebrae are shorter, allowing women more flexibility in movement. The flexion ROM in the lumbar spine is two times greater in men than in women, likely due to the limited motion of the sacrum in men, who compensate for this limited motion specifically in the lumbar spine [38,39].
As a final note, we would like to mention the pelvifemoral rhythm, which describes that during hip flexion there is not only movement in the hip joint itself (movement of the femur relative to the acetabulum), but also in the pelvis in the sense of PPT. In other words, hip flexion is accompanied by PPT and lumbar flexion [40]. This phenomenon was first reported in 1982 while performing the Straight leg raise test [41]. Since then, several studies have been conducted to further investigate this phenomenon when performing hip flexion in various ways: passive, active, unilateral, bilateral, flexion performed supine, in a hanging position, standing on one lower extremity [42,43,44]. Bohannon et al. [42] state that PPT is evident before the hip flexion range reaches 8°. This finding contradicts the general view that this movement occurs after the maximum hip flexion ROM has been reached. The ratio of PPT is roughly as follows: during the movement into hip flexion, 2.3–2.8° of the movement is due to the femur’s own movement relative to the acetabulum and 1° is due to the PPT, i.e., of the total ROM of 3.3–3.8° of hip flexion, 2.3–2.8° is due to the femur’s own movement and 1° is due to the PPT. Similar conclusions have been reached by authors of other studies [43,44]. A systematic review was conducted in 2017, which included a total of 9 studies on this topic. PPT was found to account for between 13.1% and 37.5% of the total hip flexion ROM, with higher values recorded when the knee joint was in extension and when the participants’ hamstrings were more shortened [45].
Solutions for PPT are often vaguely defined and rather anecdotal, however maintaining a neutral spine and correct pelvic position throughout the squat is a priority. By practicing the squat in this way, we build muscle memory and strength in the correct movement pattern. A comprehensive approach may then be to combine regular strength training with progressive loading and mobility training [46,47]. As a result, it is possible to gradually build strength in the muscles that are activated during the squat, such as the gluteal muscles, hamstrings, quadriceps femoris, and lumbar spine extensors [47,48]. It is advisable to give priority first to achieving technically correct squat depth before increasing the load, leading to long-term progression with minimized risk of injury [7,32,46,49].
It is also a good idea to include mobility training during the warm-up or after strength training that targets the hip and ankle joints. To increase the range of motion of these joints, certain squat variations can be used, such as the goblet squat and the overhead squat. This training allows for proper squat technique and the ability to gradually and safely increase the depth of the squat. Another option may be traditional stretching, whether it is stretching the hip flexors in the lunge, stretching the hip flexors in the 90/90 position, or other variations of static and dynamic stretching [46,50]. Isolated pelvic movements, such as anterior pelvic tilt and PPT, quadruped rocking, etc., are also appropriate for improving body awareness in space and pelvic and lumbar postural control [46]. As a result, the athlete can become aware of the neutral position of the spine and avoid excessive posterior and anterior pelvic tilt when performing squats.
If we target the trunk and pelvic area specifically, then according to the Kushner et al. [51] the excessive forward lean of the trunk and kyphotic lumbar spine can be corrected. It is advisable to start with verbal correction and, if that does not help, to move on to exercises where we teach the athlete to maintain a neutral lumbar spine position (lordosis), first in a standing position and then dynamically (exercises can be aimed at increasing strength, improving neuromuscular control and/or improving mobility). Proper execution of the squat (with moderate lumbar lordosis) requires optimal spinal mobility; when mobility is not present, compensatory, excessive forward leaning of the trunk increases the load on the intervertebral discs.
Finally, it is important to note that due to individual anatomical differences (e.g., acetabulum position, femur length, tibia length and rotation) it is not possible for every athlete to achieve maximum squat depth while maintaining proper technique [7,46]. Hence, it is necessary to find a squatting setup that does not force the athlete into unnatural positions that could lead to compensatory movements or subjectively unpleasant sensations such as excessive flexion of the lumbar spine or a pinching sensation in the hip joint.
As can be seen from the previous text, the correct execution of the squat and its depth is determined by a number of variables, which are often anatomical. Also, opinions on the potential risk of injury are not uniform, but in summary, if the squat is performed technically correctly, given the capabilities of the athlete and with progressive loading, it is a safe and very effective exercise for developing strength and hypertrophy, especially in the lower limbs. Since it is absolutely essential to master technically correct execution of the bodyweight squat (with no external load), the research will deal with the bodyweight squat and the occurrence of the phenomenon of PPT during this type of squat. The main goal of this study is to objectively assess the immediate effect of the exercise intervention on the total pelvis ROM in the sagittal plane (mainly PPT) during squat. The secondary aim of this research is to determine the relationship between the initial pelvic position and the occurrence of PPT. With our main hypothesis being as follows: The exercise intervention will have a statistically significant effect on reducing the PPT ROM during the descending phase of the squat. And our secondary hypothesis is the following: Participants with increased anterior pelvic tilt in the standing position will exhibit a statistically significant greater PPT ROM.
2. Materials and Methods
2.1. Study Design
This reserach is a controlled experiment with the participants divided into experimental and control groups. As the immediate effect of the exercise intervention was investigated, the participants were only monitored during the data collection period. The data collection included the initial physiotherapy examination, three-dimensional (3D) kinematic motion analysis of the squat, exercise intervention and 3D kinematic motion analysis of the squat. The total time required was approximately 1.5–2 hours per participant. Data collection took place at the Faculty of Health Studies, Jan Evangelista Purkyne University in Usti nad Labem from January 2023 to May 2023.
2.2. Research Sample
Volunteers from the students of the faculty were included in the experiment. The students were approached via a group email sent from the study system. A total of 42 participants (n = 42), 21 men (n = 21) and 21 women (n = 21), were included in the experiment. Inclusion criteria for the experiment were as follows: regular squat training at least once a week and good health condition (i.e., not contraindicated by a physician to perform squats). Exclusion criteria were as follows: back pain in the last three months, acute illness, infectious disease, injury or recovery from injury. The division into experimental (n = 23) and control (n = 19) groups was determined by the incidence of PPT at the initial physiotherapy examination. If the participants showed PPT during bodyweight squats before or exactly in parallel squat depth, they were assigned to the experimental group; if PPT appeared later, they were assigned to the control group.
2.3. Physiotherapy Examination
The aim of the initial physiotherapy examination was primarily to detect significant pathologies in the musculoskeletal system that would exclude volunteers from participating in the study.
Palpatory examination of bony landmarks on the pelvis—the following palpable landmarks are important: anterior superior iliac spine (ASIP), posterior superior iliac spine (PSIP) and iliac crest. Palpation of the landmarks was performed according to standard recommendations, i.e., the participant stands in the underwear, the examiner kneels so that his hands and eyes are at the level of the palpated landmarks [11,52,53]. The location of these landmarks is then used to determine the position of the pelvis in the sagittal plane. Despite the fact that palpatory examination has low specificity and repeatability, this method of examination is still a complete necessity and is necessary to evaluate and find the etiology of the patient’s symptoms [54].
Hip and ankle joint ROM—measurements were performed with a metal goniometer according to the general recommendations [55]. Seven movements were measured in the hip joint: flexion with the knee extended, flexion with the knee flexed, extension, abduction, adduction, external and internal rotation, and in the ankle dorsal and plantar flexion. Although the validity and reliability of this method of testing joint ROM is controversial, it can be said that if the assessment is performed by an experienced and the same therapist, under the same conditions and with the same instrument, it is a relatively reliable tool for measuring ROM [56,57,58].
Knee to wall test—is a reliable tool for assessing dorsiflexion ROM in the ankle. Performed against a wall, the athlete is instructed to attempt to touch the wall with the knee while keeping the heel on the ground, and the distance between the toe and the wall is measured with tape measure [59]. According to Horschig et al. [60], the result of this test must be at least 5 inches (12.7 cm) for the athlete to reach full squat depth.
Examination of the pelvic ligaments—the sacroiliac, iliolumbar, and sacrotuberous ligaments are examined. During the examination, the ligaments are stretched over the lever of the lower limb, and in the case of the sacrotuberous ligament, direct palpation is performed. The purpose of the examination is to rule out pain in the ligaments, which is often associated with other disorders of the lumbar spine, pelvis, sacroiliac joint and hip joints [61].
The Sacroiliac Joint Special Test Cluster (Cluster of Laslett)—the purpose of this testing is to rule out structural pathology in the pelvis/sacroiliac joint. The battery includes five specific tests, and if three or more are positive, this indicates dysfunction in the pelvis/sacroiliac joint. Sensitivity of this cluster is 88% and specificity is 78% [62,63].
Assessing Muscle Length—the following muscles were assessed according to Janda et al. [64]: hip flexors, hamstrings, hip adductors, piriformis muscle, and triceps surae muscle. Scoring is on a three-point scale of 0–2, 0 = no shortening, 1 = mild shortening, 2 = severe shortening.
Muscle Strength Testing—flexion and extension movements of the hip joint have been tested in accordance with Janda et al. [64] and Trendelenburg sign, and its difficult variant (standing with feet together, holding participant’s shoulders) was used to identify the weakness of the hip abductors. Scoring of Janda test is on a six-point scale of 0–5, 0 = no movement or flicker, 1 = flicker of movement, 2 = full ROM actively with gravity counterbalanced, 3 = full ROM actively against gravity, 4 = full ROM actively against some resistance, 5 = full ROM actively against strong resistance. The purpose of this testing was to rule out neurological deficits in the enrolled participants [65,66]. Both muscle length and muscle strength must be performer by skilled clinician in order to improve the reliability of the testing [56].
Diagnostic Tests of the Deep Stabilization System (core)—are part of the Dynamic Neuromuscular Stabilization concept and their goal is to detect dysfunction or imbalance in the human body’s stabilization system, or to find pathology in the area of so-called trunk stabilization [67,68]. The following tests were used: the diaphragm test, the hip flexion test, the hip extension test, and the squat test to detect inadequate trunk stabilization function. In the squat test, the following parameters were also monitored: squat depth, occurrence of PPT (used to divide the participants into experimental and control groups), occurrence of varus/valgus knee position, and heel off the ground.
2.4. Kinematic Motion Analysis
3D kinematic motion analysis using Qualisys system and Functional Assessment module was utilized for objective assessment. Objective assessment of complex movements such as the squat is essential, as unbiased results cannot be achieved by mere visual or verbal assessment [8,69,70]. For example, according to Falk et al. [69], PPT during squatting must be at least 34° to be visually detectable, and it is not possible to determine how much PPT is already above or below the physiological norm based on visual inspection alone. Maclachlan et al. [71] also adds that, when squats are performed slowly and in a controlled manner and only dichotomous verbal scores are used, a sensitivity of 88% and a specificity of 85% can be achieved. It is also important to define the body segments correctly, as if they are defined in different ways, this can lead to an overestimation of the data obtained by up to 30–50%, as has been found for hip extensor force moments with two differently defined hip joints [72]. The Qualisys system has also been used in others squat related research [4,8,73,74]. A total of 38 markers were applied to the participant’s body and an additional 3 markers were placed on the hat (Figure 1).
The markers were applied according to the recommendations of the Functional Assessment Module and the palpation and marking of the bony landmarks was performed according to Sint Jan [75]. To ensure that the markers could be applied in the same location, the position of each marker was labeled with three dots using a pen prior to removal (Figure 2).
Eleven Oqus cameras were used for data capture (specifically: 5× Oqus 300, 4× Oqus 300+, 2× Oqus 310+) with 100 Hz capture rate. Data collection was performed exactly as recommended in the Functional Assessment module. First was the static and functional session, which consisted of two assessments: standing and standing with repeated mild knee flexion. This was followed by a squat session in which each participant performed two sets of bodyweight squats of seven repetitions each. The first set was used for familiarization with the data capture and was not included in the data analysis. The second set was already included in the data analysis, but the first repetition of the squat was not included. Thus, a total of six preintervention and six postintervention squat repetitions were processed. There was a 45 second rest period between each trial.
The instructions for the participants to perform the squat were as follows: stand at pelvic width, squat smoothly to the maximum depth the participant can comfortably manage, do not bounce or pause at the bottom, and then return to the starting position. The arms were held at shoulder level at all times.
2.5. Characteristics of the Exercise Intervention
The exercise intervention was identical for both groups and was adapted from Kushner et al. [51]. A total of six exercises were performed (Table 1), three sets of 6 repetitions of each, with 20 seconds of duration in the plank and with a pause of 45 seconds between sets. The intervention time was approximately 15–20 minutes.
2.6. Data Collection
The data collection included the initial physiotherapy examination, 3D kinematic motion analysis of the squat, exercise intervention and 3D kinematic motion analysis of the squat. The total time required was approximately 1.5–2 hours per participant. Data collection took place at the Faculty of Health Studies, Jan Evangelista Purkyne University in Usti nad Labem from January 2023 to May 2023.
2.7. Data Analysis
The first stage was to tag all the markers in the software Qualisys Tracking Manager (version 2023.3). This was followed by starting the automatic processing in the Visual3D Professional software (version 2024.09.1). A pipeline was then manually created to mark the following points on the pelvic curve (Figure 3) in the sagittal plane:
- Blue point—initial position of the pelvis before squat;
- Red point—maximum anterior pelvic tilt during the descending phase of the squat;
- Khaki point—pelvic position at maximum squat depth;
- Green point—pelvic position at 90° right hip flexion;
- Pink point—pelvic position at 90° of left hip flexion.
The pelvic curve is defined as the motion of a pelvis segment (Figure 4) relative to the global coordinate system of the laboratory (in Figure 4, this is the y-axis called „Pelvis_wrt_Lab::X”). The CODA pelvis segment model is used and is defined by using the anatomical locations of both ASIS and the midpoint of the PSIS location.
Thus, a total of six values (six squat repetitions) were obtained for each participant before exercise intervention and another six after exercise intervention. The following data were used for statistical analysis:
- Initial position of the pelvis before squat (blue point);
- PPT ROM during descending phase of the squat (difference between pelvic position at maximum squat depth—khaki point, and maximum anterior pelvic tilt during the descending phase of the squat—red point).
Descriptive statistics (mean, standard error, median, mode, standard deviation, minimum, maximum, count) and frequency distribution (frequency, percent, cumulative percent) was used to analyze the data from the initial physiotherapy examination. These basic analyses were performed in Microsoft Excel (version: Professional Plus 2019).
The R software (version: 4.4.0) was used to analyze the 3D kinematic motion analysis data and to test the hypotheses. Restricted Maximum Likelihood (REML) analysis of linear mixed models was performed both for fixed (time = pre- and post-intervention condition, group = experimental and control) and random effects (participant), residuals normality analysis was performed after each REML analysis, and these results are displayed with in Q-Q plot and histogram. Repeated measures analysis of variance (rANOVA) was also use in specific cases. Statistical significance was set at the conventional 0.05 level.
The first analysis carried out was a mixed model for the dependent variable (PPT ROM) with no difference in squat repetition order with the random effect (participant), first with interaction and then without interaction.
Subsequently, rANOVA with differentiation of squat repetition order was performed (works with all independent variables as factors, so it is not possible to examine a linear dependence on squat repetition order; used factors: time, group, repetition, group:time, group:repetition, time:repetition, group:time:repetition) and then a mixed model was implemented. This model considers repetition as a numerical variable and follows a linear dependence on it.
Lastly, mixed model with random effect (participant) was used to assess the dependence of the PPT ROM on the initial pelvic position (first without the time factor). And then the same model was used for the values obtained before the exercise intervention only, for both groups.
3. Results
3.1. Participants
Twenty-three participants were assigned to the experimental group, including 14 men and 9 women. The average age was 25.65 ± 8.07 years, height 176.83 ± 10.19 cm, and weight 76.87 ± 13.41 kg. Squat depth was slightly below parallel for all participants. The occurrence of PPT was at exactly parallel squat depth in 19 participants and in 4 participants it was before reaching the parallel position. The initial position of the pelvis was very diverse, with 9 participants exhibiting physiological anterior pelvic tilt, 3 increased anterior pelvic tilt, 2 posterior pelvic tilt, 1 torsion, 5 physiological anterior pelvic tilt with obliquity, 2 increased anterior pelvic tilt with pelvis obliquity, and 1 posterior pelvic tilt with pelvis obliquity.
Nineteen participants were assigned to the control group, including 7 men and 12 women. The average age was 27.05 ± 9.44 years, height 170.95 ± 6.64 cm, and weight 67.32 ± 11.30 kg. Squat depth was below parallel for all participants, some (n = 10) even achieved a full deep squat (glutes almost touching the ground). The occurrence of PPT was below parallel in 12 participants and in 7 participants it was slightly above the ground. The initial position of the pelvis was also very diverse, with 10 participants exhibiting physiological anterior pelvic tilt, 1 posterior pelvic tilt, 6 physiological anterior pelvic tilt with obliquity, and 2 increased anterior pelvic tilt with pelvis obliquity.
3.2. Results of Physiotherapy Examination
Hip joint range of motion—all participants (regardless of group) showed physiological ROM. Only flexion and abduction movements showed values at the lower limits of physiological ROM. Ankle joint range of motion—all participants (regardless of group) showed physiological ROM. Only plantar flexion movement showed values at the lower limits of physiological ROM.
Examination of the pelvic ligaments—the results of this examination are virtually free of adverse findings, with 85–100% of participants, regardless of group, being free of any pathology.
The Sacroiliac Joint Special Test Cluster (Cluster of Laslett)—pelvic/sacroiliac joint dysfunction was ruled out in all participants, because no participant had three or more positive tests. Only one participant in experimental group had two positive tests.
Assessing Muscle Length—in both groups, the hamstrings and rectus femoris muscle showed the greatest shortening (80–85% of participants), followed by the tensor fasciae latae (40–50% of participants). The remaining muscles, the hip adductors, piriformis muscle, triceps surae muscle, and iliopsoas muscle, showed almost no shortening.
Muscle Strength Testing—nearly all participants demonstrated hip flexion and extension strength at levels 4+ and 5. There was no pathology in the Trendelenburg sign, but in its more difficult version, 50–75% of participants showed poor execution regardless of group.
Diagnostic Tests of the Deep Stabilization System (core)—virtually every participant, regardless of group, had some amount of pathology in these tests. The biggest problem was the hip flexion test (up to 85% of participants had poor execution), followed by the diaphragm test (40–60% of participants with poor execution) and the hip extension test (25–50% of participants with poor execution). Supporting statistics for these points are provided in Supplementary Materials of this article.
3.3. Results of the 3D Kinematic Motion Analysis
Main hypothesis—no statistically significant difference was found in the mixed model with interaction (p = 0.89) nor in the mixed model without interaction (p = 0.42). In other words, the exercise intervention did not affect the total PPT ROM during the descending phase of the squat for individual participants. This fact is well illustrated in Figure 5, where the individual participants, the means for the groups (experimental and control), and the differences between before and after the exercise intervention are shown. A borderline of statistical significance was found between the groups (p = 0.06).
The results of rANOVA with squat repetition order distinction show a significant difference in the repetitions (p < 0.001) and a borderline of statistical significance was found between the groups (p = 0.06). No other factors were found to be statistically significant. Using a mixed model that takes into account the order of repetition, the effect of repetition is again found to be statistically significant (p < 0.001), and the significance of the group is again borderline (p = 0.07). Figure 6 and Figure 7 show very well the differences in individual squat repetitions, distinguishing between experimental and control groups and between pre- and post-intervention conditions.
Secondary hypothesis—using a mixed model with random effect (participant) and looking at the relationship between PPT ROM and initial pelvic position, no statistically significant relationship was found (p = 0.13). Using the same model, but only with data from before the exercise intervention, the relationship between the PPT ROM and the initial pelvic position is even smaller, i.e., again not statistically significant (p = 0.77), and the significance of the group is again borderline (p = 0.06). To give an idea of the data distribution, the following scatter plot is used (Figure 8).
4. Discussion
The main goal of this research was to objectively assess the immediate effect of the exercise intervention on the total pelvis ROM in the sagittal plane with the assumption that the exercise intervention will reduce PPT ROM during the descending phase of the squat. Unfortunately, the results of this study do not support this main hypothesis, nor do they support the secondary hypothesis. For this reason, we will focus primarily on the limitations of this research and recommendations for future research in this area.
If we look at the Figure 6 and Figure 7, we can see a trend where PPT ROM decreases in the experimental group after the intervention and also in the control group, but to a lesser extent. However, these changes of about 0.5° are obviously not statistically significant and we dare say that they are at the limit of measurement uncertainty. This brings us to the first limitation of this study, which is the use of 3D kinematic motion analysis. Although this is a relatively widely used [4,8,73,74] valid and reliable tool for motion objectification [71], some errors cannot be completely avoided. The reliability of the measurements was ensured by labeling the marker placement with a pen (Figure 2). The main concern could be poor palpation of the bony landmarks (ASIP, PSIP, and iliac crest) necessary to define the CODA pelvis segment. Although the palpation was performed according to the generally accepted recommendations [11,52,53,75] and the author is quite experienced in this palpation, one can never completely exclude the possibility of an incorrect palpation of the given landmarks. Because, as stated in Malanga & Mautner [54], this examination has low specificity and repeatability (this negative was eliminated by the fact that the palpation was done only once), but it is still an absolute basis in the examination of the patient. Even if the palpation was off by a few millimeters, this could change the defining the pelvic segment and therefore affect the PPT ROM data obtained (but probably in the lower units of angular degrees). A theoretical recommendation for further research could be the use of other objectification methods that do not rely on subjective perceptions but are truly objective—e.g., x-ray or dynamic magnetic resonance imaging, but the disadvantage of these methods is the high cost and radiation exposure to the patient.
The second limitation could be in the squat initial settings and its execution. Several authors suggest that a wider stance during squatting can alter PPT ROM [8,38,76,77]. However, since it is commonly stated that the typical execution of the squat is a pelvic/hip/shoulder level stance width [36], the pelvic width stance execution of the squat was investigated for this reason. Since participants were not measured for pelvic width and were only verbally instructed to stand at pelvic width, it could theoretically be that stance width was narrower than pelvic width, resulting in greater PPT ROM. However, based on visual inspection of stance width we would venture to say that all participants were indeed standing at pelvic width. Therefore, in future research, it would be desirable to measure participants’ pelvic width to avoid potential errors in the initial squat stance. There is also the question of whether simply changing the stance width during squatting is the right solution/approach to PPT without further investigation/clarification of the causes of this phenomenon. Related to the execution of the squat is the fact that individual repetitions were not consistent, as can be seen in Figure 6 and Figure 7, respectively, that there was even an increase in PPT ROM with each subsequent repetition. The reason for this may be that the instructions to perform the squat were only verbal: stand at pelvic width, squat smoothly to the maximum depth that you can comfortably manage, do not bounce or pause at the bottom, then return to the starting position and the arms must be held at shoulder level at all times. This may have caused each squat depth to be different, each starting position to be different, and the duration of each descending/ascending phase to be different. A possible solution for future research on this topic is the use of metronome-like aids (which was used e.g., in the study by Erman et al. [78] to standardize execution or introduce a specific pause between each repetition, and possibly the use of a box or other aid to accurately define the squat depth. This should make the repetitions and the data obtained more consistent. On the other hand, this is an artificial interference with the participant’s own squat execution, and it is a matter of consideration whether to study a precisely defined squat execution or a natural way of performing the squat. Also, when we look at the PPT ROM in the experimental and control groups, we see that paradoxically, the control group has a greater PPT ROM than the experimental group. The likely reason for this could be that a significant number of participants in the control group had a greater squat depth than the experimental group. Thus, this finding may support our point above that squat execution should be clearly standardized in terms of squat depth.
Motor learning and the effect of fatigue might be the third limitation of this research. Motor learning, or sensorimotor learning, is generally defined as a four-step process associated with practice or experience that results in relatively permanent changes in a skill. Another definition describes motor learning as an activity designed to learn or modify a previously learned movement [79]. Thus, the exercise intervention used may have failed for two reasons. The first is the fact that it was not checked whether the participants had completely mastered the included exercises. This fact is very important because the first step in motor learning is the generalization phase, which is characterized by high expenditure of energy and concentration. Therefore, in theory, fatigue could increase during/after the exercise intervention and consequently affect the execution of the squat. On the other hand, if we look at the research by Weeks et al. [80], fatigue only occurred to alter the execution of the squat after several hundred repetitions of bodyweight lunges. A similar study was conducted by Erman et al. [78], where fatigue that significantly altered joint kinematics occurred after performing 72±27 bodyweight squats. It is probably very unlikely that a total of 28 squat repetitions (14 before the intervention and 14 after the intervention) and 15–20 minutes exercise intervention would cause such a significant increase in fatigue to alter the execution of the squat. Thus, a future solution might be to first have a few days of familiarization with the exercise intervention in order to teach the exercises to the participants, but the question is whether these few days of familiarization are not a targeted intervention itself and will not affect the results of the immediate effect of the exercise intervention. The second fact may be that only two exercises directly applicable to squat execution (ball wall squat and overhead squat) were included in the exercise intervention, the rest was aimed more at influencing posture or awareness of one’s body in space. We know that performance in the squat is to some extent transferable to other sports such as sprinting or jumping [1,4,5]. However, the question is whether the exercise intervention included is transferable to squat performance/technique. According to Mang et al. [81], both bilateral exercises (hip thrusts) and unilateral exercises (rear foot elevated split squat) are transferable to squat performance. In this context, it is possible to mention the intensity of the included exercise intervention. As can be seen from Table 1 and the following description of the exercises, these are bodyweight exercises. Therefore, it can be concluded that this is a relatively low intensity exercise intervention and it is questionable whether this low intensity can produce any immediate changes.
And this brings us to the fourth limitation of this work, and that is the intensity of used exercise intervention and the time for which the effect of the exercise intervention has been studied. When we look at studies that address pelvic and trunk issues and the immediate effects of exercise interventions, we find mostly positive results outcomes regardless of the level of training of the participants. These studies have used a wide range of exercise interventions, from stretching to isometric exercises to traditional dynamic exercises [82,83,84,85,86]. However, the vast majority of research has used at least four and usually up to eight weeks of exercise intervention at a frequency of three times per week. In terms of intensity, there is research that looks at low-intensity, high-repetition exercise interventions. However, the intensities used are often in the range of 30–50% of 1RM and few use pure bodyweight equivalent loads. The results of such research suggest that even low intensity can affect the outcome in 1RM, increasing isometric strength and increasing the amount of muscle mass [87,88]. However, all of these studies followed participants again for several weeks. Other studies have examined an exercise intervention using bodyweight squats in the elderly population. The results of these studies suggest that performing several bodyweight squats per day for 3–4 months could improve lower limb function, as well as performance in physical functional tests related to daily activities and could slightly change neural activation [89,90]. Thus, it can be concluded that low-intensity exercise intervention has an effect, but usually with a longer time interval, and although immediate changes can occur even after a short exercise intervention, it is probably necessary to make the exercise intervention more specific to squatting, and this is what we would recommend for further research.
And it is the group of participants that brings us to the next, fifth limitation of this thesis. The research sample consisted of a relatively small number of participants who were also completely free of health problems, but more importantly, had at least one year of squatting experience, which could have significantly influenced the results of this study. If these were beginners just starting out with strength training, the results may have been different. The same can be said if participants have health problems, typically low back pain, as there is a huge amount of research on this topic and we know that changes in movement behavior/stereotypes do occur after interventions. Where we know, for example, that stabilization exercises targeting the trunk and pelvic area can reduce pain, increase muscle strength and improve stability [91], we also know that low-intensity aerobic activity along with strength training and mobility training is an appropriate treatment for chronic non-specific low back pain [92], and stabilization exercise intervention can also reduce kinesiophobia [93]. This leads to a very cautious recommendation for further research, namely to compare the pelvic segment behavior of healthy participants (control group) with the pelvic segment behavior of participants with back pain (experimental group).
There is also a sixth limitation related to the participants and that is the way the participants were divided into experimental and control groups. When participants were divided based on the occurrence of PPT during squatting, there were still significant differences in pelvic position during standing. Therefore, it may have been more appropriate to divide the participants not only on the basis of the occurrence of PPT, but also on the basis of their pelvic position during standing and possibly by gender (man/woman). This is because the general recommendation is that participant groups should be as homogeneous as possible [94], and in the case of this thesis, homogeneity was only partially established based on the distribution according to the occurrence of PPT. A second factor in why the results of the thesis came out this way may be that sample size calculation and power analysis were not performed, which some authors have stated is necessary in biological research [95,96]. However, due to the very limited amount of research available on our topic, it was not possible to calculate the parameters from. Thus, a possible flaw in this research is the fact that pilot study was not conducted to determine sample size and power analysis, so for future research we would recommend that pilot study be conducted on a smaller number of participants and then use these results to determine sample size and power analysis, or the results of our study could also be used to determine sample size and power analysis.
A secondary hypothesis was that participants with greater anterior pelvic tilt in standing would also have greater PPT ROM. This hypothesis is based on the opinion of several authors [7,35,50]. Why this hypothesis was not confirmed is difficult to determine. A possible explanation may be found in one of the concepts of manual medicine, which states that if we have a starting joint position that is moved in one direction (in our case, greater anterior pelvic tilt in standing position), the overall ROM in the joint does not change, but the sub-movements do, by increasing the ROM in the direction of the misalignment (in our case, increasing the anterior pelvic tilt ROM in the descending phase of the squat) and decreasing the ROM in the other direction (in our case, decreasing the PPT ROM in the descending phase of the squat) [97]. In the results, we only reported the mixed model result for this secondary hypothesis (p = 0.13 and p = 0.77 using only the data before intervention), but a simple correlation was also performed with a result of -0.26, and using the Spearman rank correlation coefficient (due to the non-normality of the data) the result was similar at -0.29. These negative values actually say that there is a relationship between initial pelvic position and PPT ROM, but it is exactly the opposite of what was hypothesized in our study, i.e., as the value of pelvic curvature increases (greater anterior pelvic tilt), PPT ROM decreases. Again, we have no explanation for this phenomenon, but one study found similar results, only in patients after total hip arthroplasty, where PPT at maximum hip flexion was significantly correlated with pelvic tilt at minimum hip flexion (standing position) [98].
The second to last thing we want to mention are the anatomical predispositions of the individual participants. Several authors [7,46,47,50] state that not everyone is capable of performing the deep squat correctly. Due to the fact that the participants did not undergo radiographic examination, changes in the femoral angles, which can significantly affect ROM and the way of the movements are performed [40], cannot be ruled out with certainty. Therefore, we would consider including imaging examinations (typically x-rays) to rule out congenital changes in the femoral angle and possibly to rule out FAI, which is known to alter the movement pattern of the squat [19,20,21,22,23]. There are clinical tests to rule out FAI that were not used in this thesis, which may be another limitation in this study. However, the included participants showed almost physiological ROM in all hip movements, so it is questionable whether the inclusion of these tests is entirely necessary. Nevertheless, we believe that the initial physiotherapy examination carried out in this research is more than sufficient and could theoretically serve as a model examination for further research or clinical practice.
The last thing we want to address is whether PPT exists at all. In the theoretical background it is said that PPT is a phenomenon that accompanies the hip flexion practically from the beginning [41,42,43,44,45] and some might argue that it is a normal thing that belongs to the execution of the squat or hip flexion itself. In our opinion, this is quite possible, because the pelvis shows a movement into anterior pelvic tilt and then into PPT during the descending phase of the squat (and during the ascending phase, the pelvic movements are in reverse order, as can be seen in Figure 3). A similar finding, i.e., that the pelvis exhibits both movement into anterior pelvic tilt and PPT, has been reported in other research [34,73,80,99,100,101] but because each time a different data collection system (3D kinematic motion analysis from various manufacturers or x-ray) and a different squat variant is used (e.g., squatting on one leg, standing up from a squat, etc.), the results are very heterogeneous and practically incomparable to the results of this thesis. The pelvic kinematic curves of this thesis most closely match those of the following research: Edington [34], Sinclair et al. [73], Weeks et al. [80]. However, because the effect of the exercise intervention on PPT ROM was not primarily investigated in these studies, no definitive conclusion can be drawn. And since nowhere is it defined what PPT ROM is physiological and what is not, the research question of how PPT ROM is affected and its consequences is still valid in our opinion.
5. Conclusions
The short exercise intervention did not affect the range of motion of PPT during squatting, but it is still worth investigating this issue further and looking for possible associations between different variables of squat execution and the incidence of PPT. Nevertheless, we still believe that proper exercise intervention for PPT during squatting is a possible solution, provided the athlete is not limited by innate anatomical predispositions and a comprehensive examination has been performed to uncover the possible cause of PPT. This study is, in our opinion, one of the few publications that have addressed the issue of PPT during squatting, and we would be very pleased if someone else would build on this work and clearly identify the causes and solutions to PPT during squatting.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, O.K. and J.J.T.; methodology, O.K., L.L. and A.Č.; software, M.J.; validation, L.L. and A.Č.; formal analysis, O.K.; investigation, O.K., V.K. and M.J.; resources, O.K.; data curation, K.H., M.J., L.L. and A.Č.; writing—original draft preparation, O.K.; writing—review and editing, O.K.; visualization, O.K.; supervision, J.J.T.; project administration, O.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Faculty of Physical Education and Sport at Charles University in Prague (protocol code 245/2021 with the approval date of 8 November 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PPT | Posterior pelvic tilt |
| 1RM | One repetition maximum |
| ROM | Range of motion |
| 3D | Three-dimensional |
| ASIP | Anterior superior iliac spine |
| PSIP | Posterior superior iliac spine |
| REML | Restricted Maximum Likelihood |
| rANOVA | Repeated measures analysis of variance |
| cm | Centimeter |
| FAI | Femoroacetabular impingement syndrome |
References
- Chelly, M.S.; Fathloun, M.; Cherif, N.; Amar, M.B.; Tabka, Z.; Van Praagh, E. Effects of a Back Squat Training Program on Leg Power, Jump, and Sprint Performances in Junior Soccer Players. J. Strength Cond. Res. 2009, 23, 2241–2249. [Google Scholar] [CrossRef]
- Liebenson, C. Rehabilitation of the Spine: A Patient-Centered Approach, 3rd ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2019. [Google Scholar]
- Garcia-Fernandez, A.; Petros, P.E. A four month squatting-based pelvic exercise regime cures day/night enuresis and bowel dysfunction in children 7–11 years. Cent. Eur. J. Urol. 2020, 73, 307–314. [Google Scholar] [CrossRef]
- Choe, K.H.; Coburn, J.W.; Costa, P.B.; Pamukoff, D.N. Hip and Knee Kinetics During a Back Squat and Deadlift. J. Strength Cond. Res. 2021, 35, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Styles, W.J.; Matthews, M.J.; Comfort, P. Effects of Strength Training on Squat and Sprint Performance in Soccer Players. J. Strength Cond. Res. 2016, 30, 1534–1539. [Google Scholar] [CrossRef]
- Myer, G.D.; Kushner, A.M.; Brent, J.L.; Schoenfeld, B.J.; Hugentobler, J.; Lloyd, R.S.; Vermeil, A.; Chu, D.A.; Harbin, J.; McGill, S.M. The Back Squat: A Proposed Assessment of Functional Deficits and Technical Factors That Limit Performance. Strength Cond. J. 2014, 36, 4–27. [Google Scholar] [CrossRef]
- The Bottom Position of Your Squat: A Defining Characteristic of Your Human Existence. Juggernaut Training Systems. Available online: https://www.jtsstrength.com/bottom-position-squat-defining-characteristic-human-existence/ (accessed on 14 October 2025).
- Nielsen, S.R. Posterior Pelvic Tilt in Barbell Back Squats: A Biomechanical Analysis. Master’s Thesis, Norwegian School of Sport Sciences, Oslo, Norway, 2015. [Google Scholar]
- Todoroff, M. Dynamic Deep Squat: Lower-Body Kinematics and Considerations Regarding Squat Technique, Load Position, and Heel Height. Strength Cond. J. 2017, 39, 71–80. [Google Scholar] [CrossRef]
- Vašíčková, L. Sezení ve Vozíku: Zvýšení Pohybového Potenciálu a Prevence Komplikací, 1st ed.; Grada: Prague, Czech Republic, 2024. [Google Scholar]
- Gross, J.M.; Fetto, J.; Rosen, E. Musculoskeletal Examination, 4th ed.; Wiley: Hoboken, NJ, USA, 2015. [Google Scholar]
- What is Pelvic Tilt & How Do You Fix it? National Academy of Sports Medicine. Available online: https://blog.nasm.org/what-is-pelvic-tilt-how-do-you-fix-it (accessed on 14 October 2025).
- McGill, S. Back Mechanic: The Step-By-Step McGill Method to Fix Back Pain, 1st ed.; Stuart McGill: Waterloo, Canada, 2015. [Google Scholar]
- Sedláková, S. Záda, Která Cvičí, Nebolí: Cvičíme Podle Ludmily Mojžíšové, 5th ed.; Vyšehrad: Prague, Czech Republic, 2023. [Google Scholar]
- Contreras, B.; Schoenfeld, B. To Crunch or Not to Crunch: An Evidence-Based Examination of Spinal Flexion Exercises, Their Potential Risks, and Their Applicability to Program Design. Strength Cond. J. 2011, 33, 8–18. [Google Scholar] [CrossRef]
- Hartmann, H.; Wirth, K.; Klusemann, M. Analysis of the Load on the Knee Joint and Vertebral Column with Changes in Squatting Depth and Weight Load. Sports Med. 2013, 43, 993–1008. [Google Scholar] [CrossRef]
- Comfort, P.; McMahon, J.J.; Suchomel, T.J. Optimizing Squat Technique-Revisited. Strength Cond. J. 2018, 40, 68–74. [Google Scholar] [CrossRef]
- Schoenfeld, B.J. Squatting Kinematics and Kinetics and Their Application to Exercise Performance. J. Strength Cond. Res. 2010, 24, 3497–3506. [Google Scholar] [CrossRef]
- Bagwell, J.J.; Snibbe, J.; Gerhardt, M.; Powers, C.M. Hip kinematics and kinetics in persons with and without cam femoroacetabular impingement during a deep squat task. Clin. Biomech. 2016, 31, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Catelli, D.S.; Kowalski, E.; Beaulé, P.E.; Smit, K.; Lamontagne, M. Asymptomatic Participants With a Femoroacetabular Deformity Demonstrate Stronger Hip Extensors and Greater Pelvis Mobility During the Deep Squat Task. Orthop. J. Sports Med. 2018, 6, 2325967118782484. [Google Scholar] [CrossRef]
- Catelli, D.S.; Kowalski, E.; Beaulé, P.E.; Lamontagne, M. Muscle and Hip Contact Forces in Asymptomatic Men With Cam Morphology During Deep Squat. Front. Sports Act. Living 2021, 3, 716626. [Google Scholar] [CrossRef]
- Kolber, M.J.; Feldstein, A.P.; Masaracchio, M.; Liu, X.; Hanney, W.J. Influence of Femoral Acetabular Impingement on Squat Performance. Strength Cond. J. 2018, 40, 47–53. [Google Scholar] [CrossRef]
- Yoshimoto, K.; Hamai, S.; Higaki, H.; Gondo, H.; Ikebe, S.; Nakashima, Y. Pre- and post-operative evaluation of pincer-type femoroacetabular impingement during squat using image-matching techniques: A case report. Int. J. Surg. Case Rep. 2018, 42, 121–127. [Google Scholar] [CrossRef]
- Breen, E.O.; Howell, D.R.; Borg, D.R.; Sugimoto, D.; Meehan, W.P. Functional Deep Squat Performance is Associated with Hip and Ankle Range of Motion. J. Athl. Enhanc. 2016, 5, 3. [Google Scholar] [CrossRef]
- Contreras, B. Bodyweight Strength Training Anatomy, 1st ed.; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Kim, S.-H.; Kwon, O.-Y.; Park, K.-N.; Jeon, I.-C.; Weon, J.-H. Lower Extremity Strength and the Range of Motion in Relation to Squat Depth. J. Hum. Kinet. 2015, 45, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Straub, R.K.; Powers, C.M. A Biomechanical Review of the Squat Exercise: Implications for Clinical Practice. Int. J. Sports Phys. Ther. 2024, 19, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Carr, K.; Feit, M.K. Functional Training Anatomy, 1st ed.; Human Kinetics: Champaign, IL, USA, 2021. [Google Scholar]
- Comfort, P.; McMahon, J.J.; Suchomel, T.J. Optimizing Squat Technique-Revisited. Strength Cond. J. 2018, 40, 68–74. [Google Scholar] [CrossRef]
- Ishida, T.; Samukawa, M.; Kasahara, S.; Tohyama, H. The center of pressure position in combination with ankle dorsiflexion and trunk flexion is useful in predicting the contribution of the knee extensor moment during double-leg squatting. BMC Sports Sci. Med. Rehabil. 2022, 14, 127. [Google Scholar] [CrossRef]
- Schoenfeld, B.J. Squatting Kinematics and Kinetics and Their Application to Exercise Performance. J. Strength Cond. Res. 2010, 24, 3497–3506. [Google Scholar] [CrossRef]
- Butt Wink. Available online: https://startingstrength.com/training/butt-wink (accessed on 14 October 2025).
- Braidot, A.A.; Brusa, M.H.; Lestussi, F.E.; Parera, G.P. Biomechanics of front and back squat exercises. J. Phys. Conf. Ser. 2007, 90, 012009. [Google Scholar] [CrossRef]
- Edington, C.P. Lumbar Spine Kinematics and Kinetics During Heavy Barbell Squat and Deadlift Variations. Master’s Thesis, University of Saskatchewan, Saskatoon, Canada, 2017. [Google Scholar]
- Masi, M. Hack Your Squat: Learn how to identify fundamental flaws in the back squat and fix them so you and your clients can get back to safely training and performing at maximum potential!, 1st ed.; 2020.
- Stoppani, J. Jim Stoppani’s Encyclopedia of Muscle & Strength, 1st ed.; Human Kinetics: Champaign, IL, USA, 2023. [Google Scholar]
- Moon, M.S.; Kim, S.T.; Shin, S.; Jeon, S.M. Squat Posture and Spinopelvic parameters—Radiographic Assessment. J. Musculoskelet. Res. 2021, 24, 2150001. [Google Scholar] [CrossRef]
- McKean, M.R.; Dunn, P.K.J.; Burkett, B. The Lumbar and Sacrum Movement Pattern During the Back Squat Exercise. J. Strength Cond. Res. 2010, 24, 2731–2741. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, F.; Waschke, J. Sobotta Atlas of Anatomy: General Anatomy and Musculoskeletal System, 16th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Pirola, V. Handbook of Kinesiology: Functional Anatomy, Biomechanics, Assessment of Joints and Muscles, 1st ed.; Edra Publishing: Palm Beach Gardens, FL, USA, 2024. [Google Scholar]
- Bohannon, R.W. Cinematographic Analysis of the Passive Straight-Leg-Raising Test for Hamstring Muscle Length. Phys. Ther. 1982, 62, 1269–1274. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Gajdosik, R.L.; LeVeau, B.F. Relationship of Pelvic and Thigh Motions During Unilateral and Bilateral Hip Flexion. Phys. Ther. 1985, 65, 1501–1504. [Google Scholar] [CrossRef]
- Dewberry, M.J.; Bohannon, R.W.; Tiberio, D.; Murray, R.; Zannotti, C.M. Pelvic and femoral contributions to bilateral hip flexion by subjects suspended from a bar. Clin. Biomech. 2003, 18, 494–499. [Google Scholar] [CrossRef]
- Murray, R.; Bohannon, R.; Tiberio, D.; Dewberry, M.; Zannotti, C. Pelvifemoral rhythm during unilateral hip flexion in standing. Clin. Biomech. 2002, 17, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Bass, A. Research describing pelvifemoral rhythm: A systematic review. J. Phys. Ther. Sci. 2017, 29, 2039–2043. [Google Scholar] [CrossRef]
- Pelvic Tilt and Squats: Butt Winking and Posterior Pelvic Tilt. Available online: https://theprehabguys.com/pelvic-tilt-and-squat-depth/ (accessed on 14 October 2025).
- How Anterior Pelvic Tilt Influences Your Squat Depth. Available online: https://www.primalmobility.com/blog/how-anterior-pelvic-tilt-affects-squat-depth (accessed on 14 October 2025).
- Petr, M.; Šťastný, P. Funkční Silový Trénink, 1st ed.; Univerzita Karlova v Praze, Fakulta Tělesné Výchovy a Sportu: Prague, Czech Republic, 2012. [Google Scholar]
- Tlapák, P. Tvarování Těla pro Muže a Ženy, 11th ed.; ARSCI: Prague, Czech Republic, 2022. [Google Scholar]
- Beat Butt Wink: Squat Big Without Hurting Your Back. Available online: https://www.bodybuilding.com/content/beat-butt-wink-squat-big-without-hurting-your-back.html (accessed on 14 October 2025).
- Kushner, A.M.; Brent, J.L.; Schoenfeld, B.J.; Hugentobler, J.; Lloyd, R.S.; Vermeil, A.; Chu, D.A.; Harbin, J.; McGill, S.M.; Myer, G.D. The Back Squat: Targeted Training Techniques to Correct Functional Deficits and Technical Factors That Limit Performance. Strength Cond. J. 2015, 37, 13–60. [Google Scholar] [CrossRef]
- Chaitow, L. Palpation and Assessment in Manual Therapy: Learning the Art and Refining Your Skills, 4th ed.; Handspring Publishing: London, UK, 2017. [Google Scholar]
- Lewit, K. Manipulační Léčba, 6th ed.; Euromedia: Prague, Czech Republic, 2024. [Google Scholar]
- Malanga, G.A.; Mautner, K. Musculoskeletal Physical Examination: An Evidence-Based Approach, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Haladová, E.; Nechvátalová, L. Vyšetřovací Metody Hybného Systému, 3rd ed.; Národní Centrum Ošetřovatelství a Nelékařských Zdravotnických Oborů: Brno, Czech Republic, 2010. [Google Scholar]
- Berryman Reese, N.; Bandy, W.D. Joint Range of Motion and Muscle Length Testing, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2024. [Google Scholar]
- Boone, D.C.; Azen, S.P.; Lin, C.-M.; Spence, C.; Baron, C.; Lee, L. Reliability of Goniometric Measurements. Phys. Ther. 1978, 58, 1355–1360. [Google Scholar] [CrossRef]
- Gandbhir, V.N.; Cunha, B. Goniometer; StatPearls Publishing: Treasure Island, CA, USA, 2020. https://www.ncbi.nlm.nih.gov/books/NBK558985/.
- Powden, C.J.; Hoch, J.M.; Hoch, M.C. Reliability and minimal detectable change of the weight-bearing lunge test: A systematic review. Man. Ther. 2015, 20, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Horschig, A.; Sonthana, K.; Neff, T. The Squat Bible: The Ultimate Guide to Mastering the Squat and Finding Your True Strength; CreateSpace Independent Publishing Platform: Scotts Valle, CA, USA, 2017. [Google Scholar]
- Kališko, O.; Ježková, A. Metody kinezioterapie I: Učební Text, 1st ed.; Univerzita, J.E., Ed.; Purkyně v Ústí nad Labem, Fakulta Zdravotnických Studií: Ústí nad Labem, Czech Republic, 2019. [Google Scholar]
- Laslett, M. Evidence-Based Diagnosis and Treatment of the Painful Sacroiliac Joint. Arch. Phys. Med. Rehabil. 2008, 16, 142–152. [Google Scholar] [CrossRef]
- van der Wurff, P.; Buijs, E.J.; Groen, G.J. A Multitest Regimen of Pain Provocation Tests as an Aid to Reduce Unnecessary Minimally Invasive Sacroiliac Joint Procedures. Arch. Phys. Med. Rehabil. 2006, 87, 10–14. [Google Scholar] [CrossRef]
- Janda, V.; Herbenová, A.; Jandová, J.; Pavlů, D. Svalové Funkční Testy. Grada: Prague, Czech Republic, 2004. [Google Scholar]
- Hardcastle, P.; Nade, S. The significance of the Trendelenburg test. J. Bone Jt. Surg. 1985, 67-B, 741–746. [Google Scholar] [CrossRef] [PubMed]
- 66. Naqvi, U.; Sherman, A.L. Muscle Strength Grading; StatPearls Publishing: Treasure Island, CA, USA, 2023. https://www.ncbi.nlm.nih.gov/books/NBK436008/.
- Kolář, P.; Bitnar, P.; Horáček, O.; Dyrhonová, O.; Kříž, J. Rehabilitace v Klinické Praxi, 2nd ed.; Galén: Prague, Czech Republic, 2020. [Google Scholar]
- Schlegel, P. Hluboký Stabilizační Systém Páteře a Bolest Zad, 1st ed.; Grada: Prague, Czech Republic, 2024. [Google Scholar]
- Falk, J.; Aasa, U.; Berglund, L. How accurate are visual assessments by physical therapists of lumbo-pelvic movements during the squat and deadlift? Phys. Ther. Sport 2021, 50, 195–200. [Google Scholar] [CrossRef]
- O’Reilly, M.A.; Whelan, D.F.; Ward, T.E.; Delahunt, E.; Caulfield, B.M. Technology in Strength and Conditioning: Assessing Bodyweight Squat Technique With Wearable Sensors. J. Strength Cond. Res. 2017, 31, 2303–2312. [Google Scholar] [CrossRef]
- Maclachlan, L.; White, S.G.; Reid, D. Observer Rating Versus Three-Dimensional Motion Analysis of Lower Extremity Kinematics During Functional Screening Tests: A Systematic Review. Int. J. Sports Phys. Ther. 2015, 10, 482–492. [Google Scholar]
- Blache, Y.; Bobbert, M.; Argaud, S.; de Fontenay, B.P.; Monteil, K.M. Measurement of Pelvic Motion Is a Prerequisite for Accurate Estimation of Hip Joint Work in Maximum Height Squat Jumping. J. Appl. Biomech. 2013, 29, 428–434. [Google Scholar] [CrossRef]
- Sinclair, J.; Brooks, D.; Atkins, S. An examination of the hamstring and the quadriceps muscle kinematics during the front and back squat in males. Balt. J. Health Phys. Act. 2017, 9, 37–45. [Google Scholar] [CrossRef]
- Southwell, D.J.; Petersen, S.A.; Beach, T.A.C.; Graham, R.B. The effects of squatting footwear on three-dimensional lower limb and spine kinetics. J. Electromyogr. Kinesiol. 2016, 31, 111–118. [Google Scholar] [CrossRef]
- Sint Jan, S.V. Color Atlas of Skeletal Landmark Definitions: Guidelines for Reproducible Manual and Virtual Palpations; Churchill Livingstone: London, UK, 2007. [Google Scholar]
- Swinton, P.A.; Lloyd, R.; Keogh, J.W.L.; Agouris, I.; Stewart, A.D. A Biomechanical Comparison of the Traditional Squat, Powerlifting Squat, and Box Squat. J. Strength Cond. Res. 2012, 26, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Fleisig, G.S.; Lowry, T.M.; Barrentine, S.W.; Andrews, J.R. A three-dimensional biomechanical analysis of the squat during varying stance widths. Med. Sci. Sports Exerc. 2001, 33, 984–998. [Google Scholar] [CrossRef] [PubMed]
- Erman, B.; Vural, F.; Dopsaj, M.; Ozkol, M.Z.; Kose, D.E.; Aksit, T.; Cè, E. The effects of fatigue on linear and angular kinematics during bilateral squat. PLoS ONE 2023, 18, e0289089. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.A.; Lee, T.D.; Winstein, C.; Wulf, G.; Zelaznik, H.N. Motor Control and Learning: A Behavioral Emphasis, 6th ed.; Human Kinetics: Champaign, IL, USA, 2018. [Google Scholar]
- Weeks, B.K.; Carty, C.P.; Horan, S.A. Effect of sex and fatigue on single leg squat kinematics in healthy young adults. BMC Musculoskelet. Disord. 2015, 16, 271. [Google Scholar] [CrossRef]
- Mang, Z.; Kravitz, L.; Beam, J. Transfer Between Lifts: Increased Strength in Untrained Exercises. Strength Cond. J. 2022, 44, 101–106. [Google Scholar] [CrossRef]
- Kadono, N.; Tsuchiya, K.; Uematsu, A.; Kamoshita, H.; Kiryu, K.; Hortobágyi, T.; Suzuki, S. A Japanese Stretching Intervention Can Modify Lumbar Lordosis Curvature. Clin. Spine Surg. A Spine Publ. 2017, 30, 297–300. [Google Scholar] [CrossRef]
- Akçay, B.; Çolak, T.K.; Apti, A.; Çolak, İ. The Immediate Effect of Hanging Exercise and Muscle Cylinder Exercise on the Angle of Trunk Rotation in Adolescent Idiopathic Scoliosis. Healthcare 2024, 12, 305. [Google Scholar] [CrossRef]
- Lee, B.; McGill, S. The effect of short-term isometric training on core/torso stiffness. J. Sports Sci. 2016, 35, 1724–1733. [Google Scholar] [CrossRef]
- Huang, T.-Z.; Kim, S.-Y. Immediate effect of trunk flexion and extension isometric exercise using an external compression device on electromyography of the hip extensor and trunk range of motion of healthy subjects. BMC Sports Sci. Med. Rehabil. 2022, 14, 116. [Google Scholar] [CrossRef]
- Imai, A.; Kaneoka, K.; Okubo, Y.; Shiraki, H. Immediate Effects of Different Trunk Exercise Programs on Jump Performance. Int. J. Sports Med. 2016, 37, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Ikezoe, T.; Kobayashi, T.; Nakamura, M.; Ichihashi, N. Effects of Low-Load, Higher-Repetition vs. High-Load, Lower-Repetition Resistance Training Not Performed to Failure on Muscle Strength, Mass, and Echo Intensity in Healthy Young Men: A Time-Course Study. J. Strength Cond. Res. 2020, 34, 3439–3445. [Google Scholar] [CrossRef] [PubMed]
- Usui, S.; Maeo, S.; Tayashiki, K.; Nakatani, M.; Kanehisa, H. Low-load Slow Movement Squat Training Increases Muscle Size and Strength but Not Power. Int. J. Sports Med. 2016, 37, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Hirono, T.; Kunugi, S.; Yoshimura, A.; Ueda, S.; Goto, R.; Akatsu, H.; Watanabe, K. Effects of home-based bodyweight squat training on neuromuscular properties in community-dwelling older adults. Aging Clin. Exp. Res. 2023, 35, 1043–1053. [Google Scholar] [CrossRef]
- Yoshiko, A.; Watanabe, K. Impact of home-based squat training with two-depths on lower limb muscle parameters and physical functional tests in older adults. Sci. Rep. 2021, 11, 6855. [Google Scholar] [CrossRef]
- Mun, D.-J.; Oh, H.-J.; Lee, S.-H. Effects of Sling Exercise on Pain, Trunk Strength, and Balance in Patients with Chronic Low Back Pain. J. Korean Phys. Ther. 2022, 34, 110–115. [Google Scholar] [CrossRef]
- Gordon, R.; Bloxham, S. A Systematic Review of the Effects of Exercise and Physical Activity on Non-Specific Chronic Low Back Pain. Healthcare 2016, 4, 22. [Google Scholar] [CrossRef]
- Filipczyk, P.; Filipczyk, K.; Saulicz, E. Influence of Stabilization Techniques Used in the Treatment of Low Back Pain on the Level of Kinesiophobia. Int. J. Environ. Res. Public Health 2021, 18, 6393. [Google Scholar] [CrossRef]
- Martínez-Mesa, J.; González-Chica, D.A.; Duquia, R.P.; Bonamigo, R.R.; Bastos, J.L. Sampling: How to select participants in my research study? An. Bras. Dermatol. 2016, 91, 326–330. [Google Scholar] [CrossRef]
- Suresh, K.; Thomas, S.V.; Suresh, G. Design, data analysis and sampling techniques for clinical research. Ann. Indian Acad. Neurol. 2011, 14, 287–290. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Medica 2021, 31, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Tichý, M. Dysfunkce Kloubu: Podstata Konceptu Funkční Manuální Medicíny, 2nd ed.; Miroslav Tichý: Prague, Czech Republic, 2014. [Google Scholar]
- Harada, S.; Hamai, S.; Gondo, H.; Higaki, H.; Ikebe, S.; Nakashima, Y. Squatting After Total Hip Arthroplasty: Patient-Reported Outcomes and In Vivo Three-Dimensional Kinematic Study. J. Arthroplast. 2022, 37, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Grant, T.M.; Saxby, D.J.; Pizzolato, C.; Savage, T.; Bennell, K.; Dickenson, E.; Eyles, J.; Foster, N.; Hall, M.; Hunter, D.; et al. Squatting biomechanics following physiotherapist-led care or hip arthroscopy for femoroacetabular impingement syndrome: A secondary analysis from a randomised controlled trial. PeerJ 2024, 12, e17567. [Google Scholar] [CrossRef] [PubMed]
- Hara, D.; Nakashima, Y.; Hamai, S.; Higaki, H.; Ikebe, S.; Shimoto, T.; Hirata, M.; Kanazawa, M.; Kohno, Y.; Iwamoto, Y. Kinematic Analysis of Healthy Hips during Weight-Bearing Activities by 3D-to-2D Model-to-Image Registration Technique. BioMed Res. Int. 2014, 2014, 457573. [Google Scholar] [CrossRef]
- Hoogenboom, B.J.; May, C.J.; Alderink, G.J.; Thompson, B.S.; Gilmore, L.A. Three-Dimensional Kinematics and Kinetics of the Overhead Deep Squat in Healthy Adults: A Descriptive Study. Appl. Sci. 2023, 13, 7285. [Google Scholar] [CrossRef]
Figure 1.
Location of markers front and back.
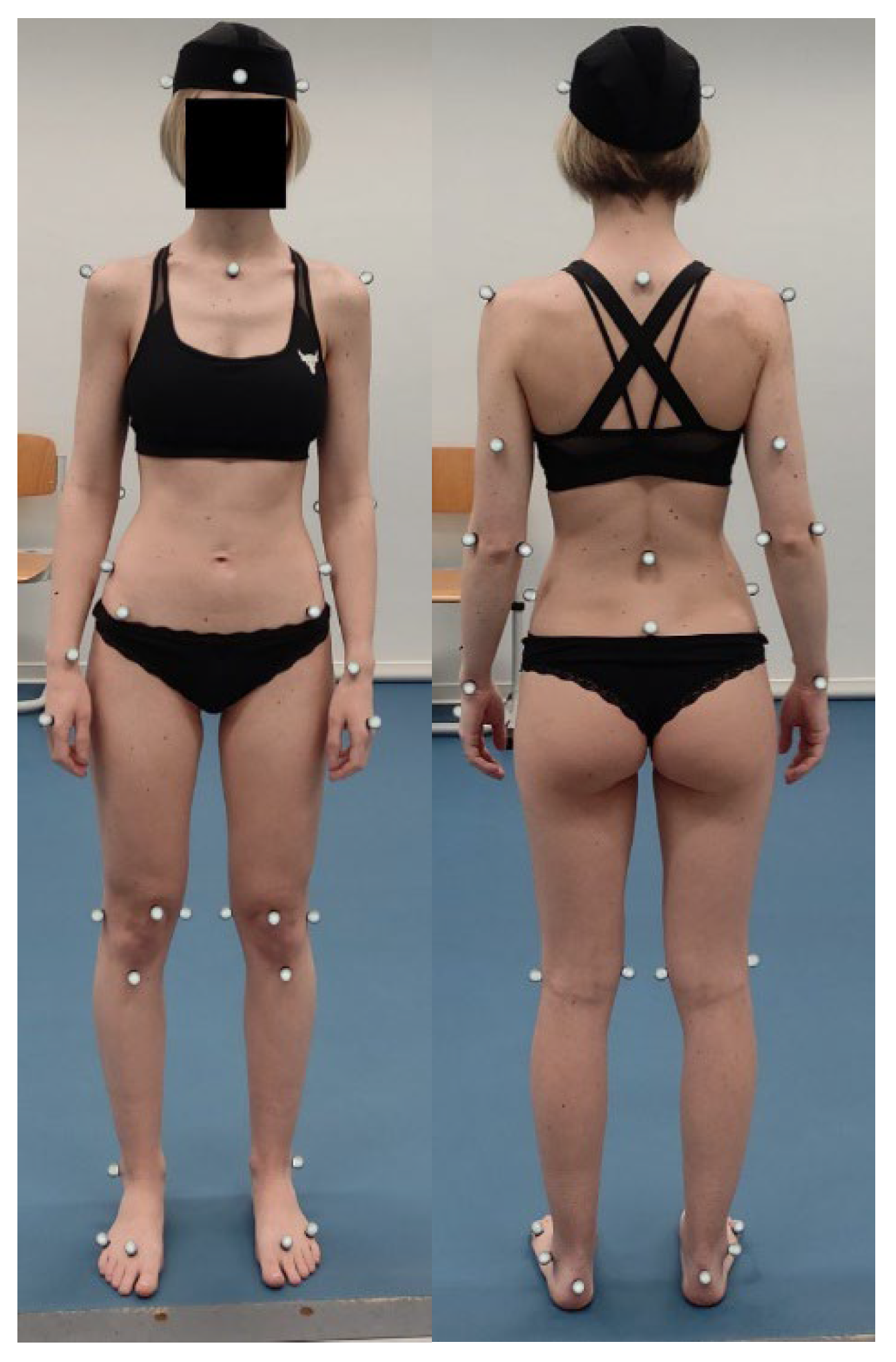
Figure 2.
Markers labeling.
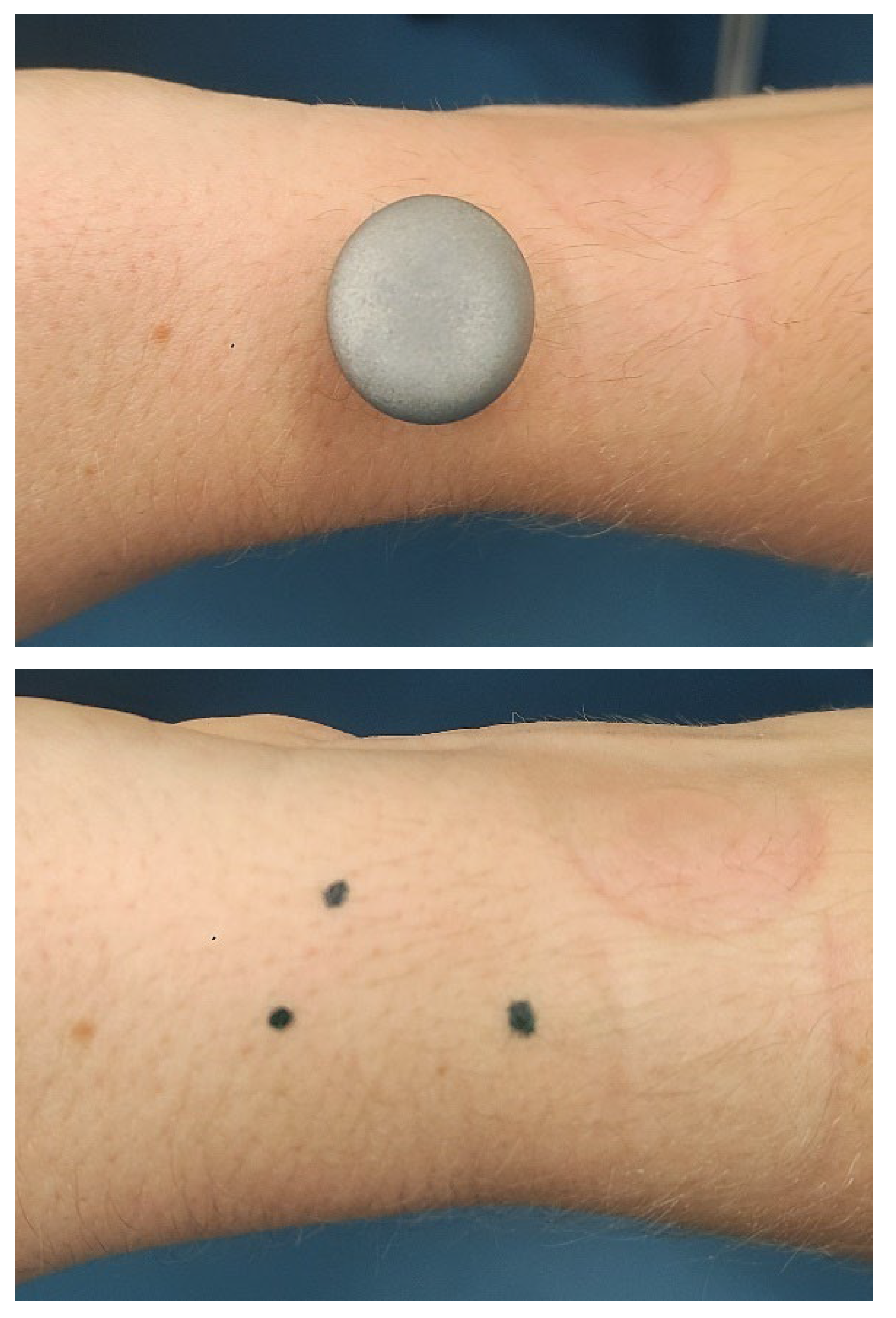
Figure 3.
Pelvic curve in the sagittal plane.
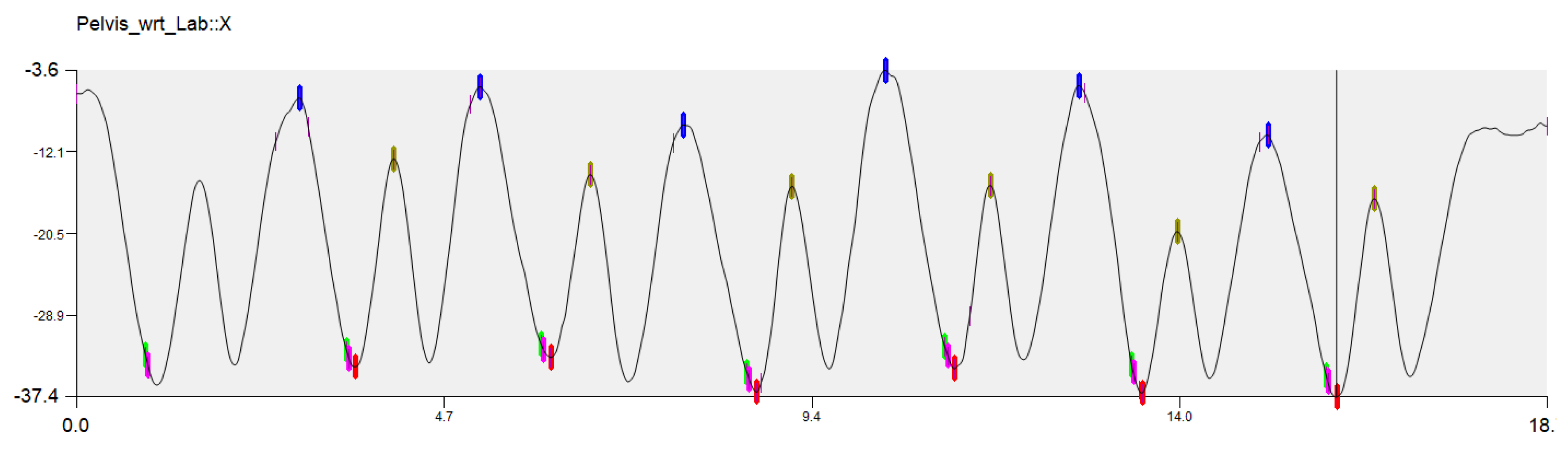
Figure 4.
CODA pelvis segment.
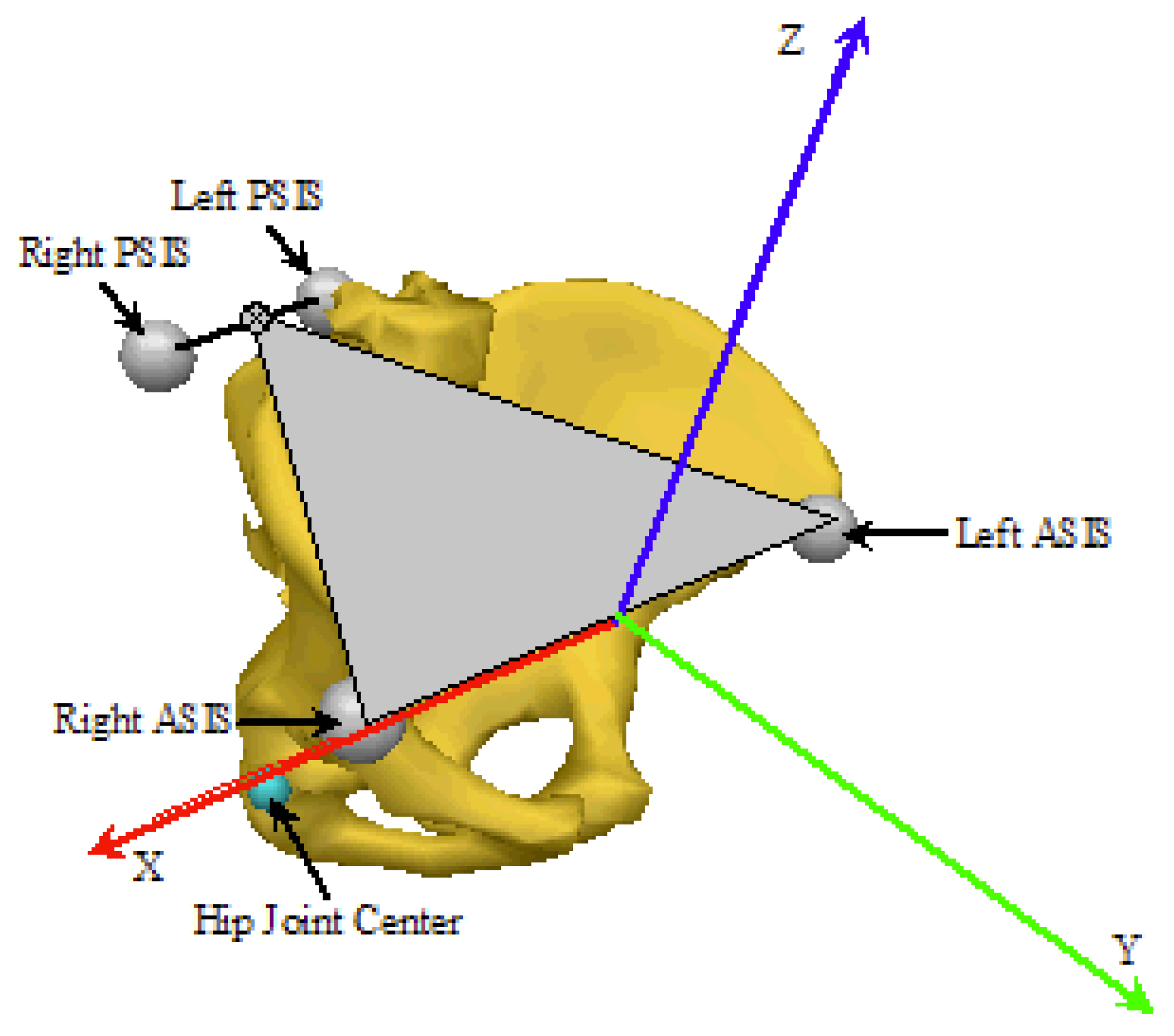
Figure 5.
Overall results for both groups.
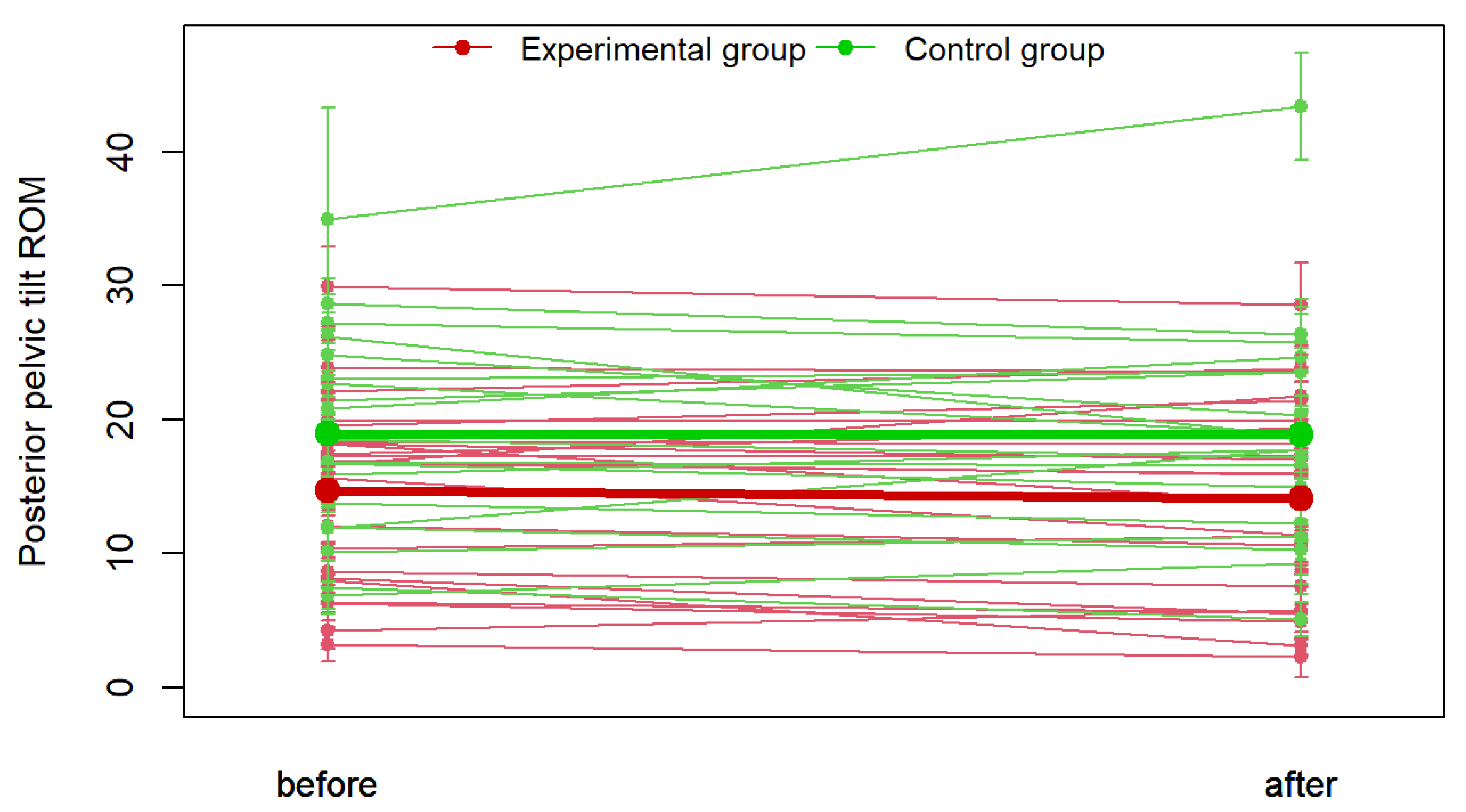
Figure 6.
Differences in individual repetitions of squats—Control and experimental group.
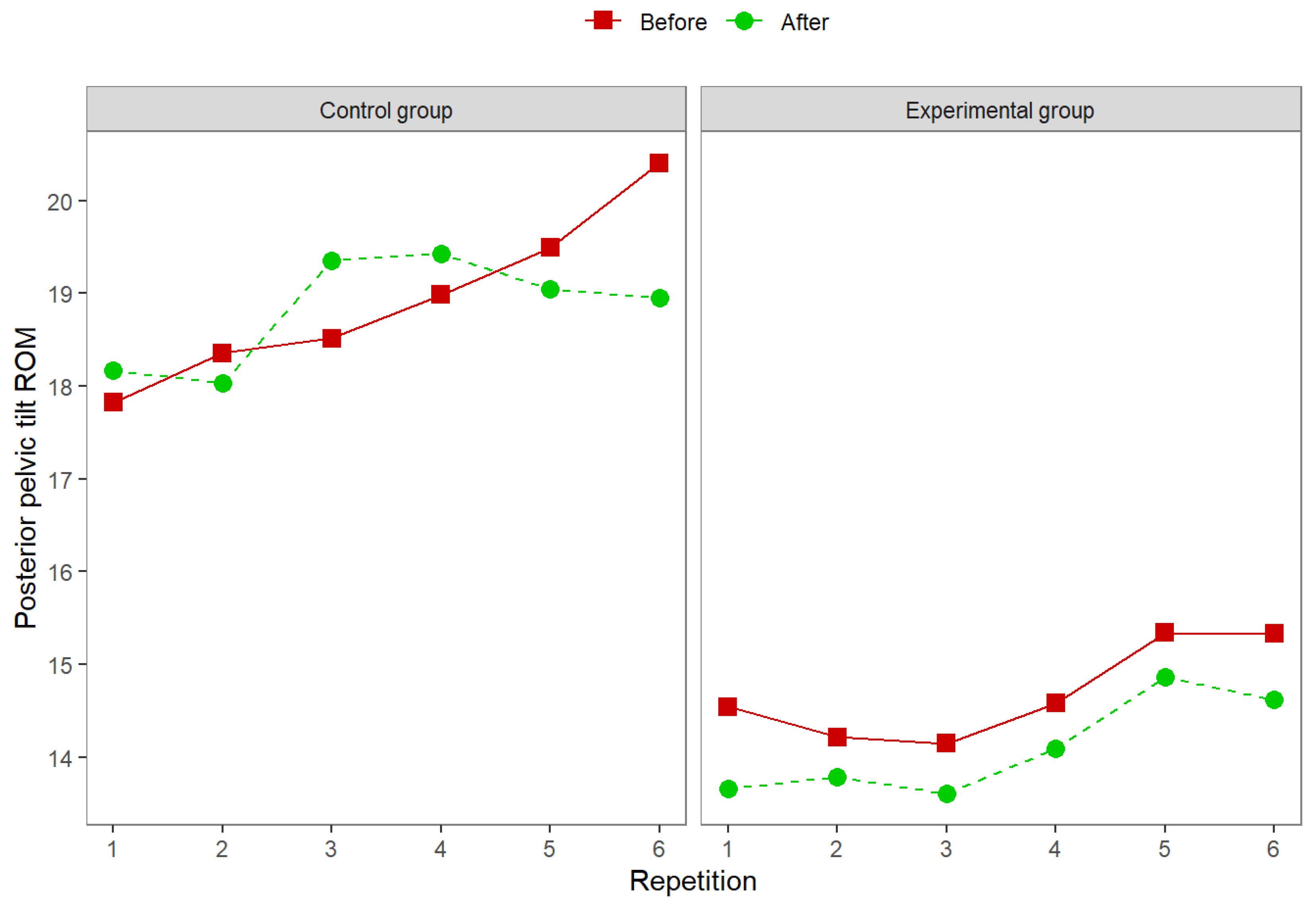
Figure 7.
Differences in individual repetitions of squats—Before and after the exercise intervention.
Figure 7.
Differences in individual repetitions of squats—Before and after the exercise intervention.
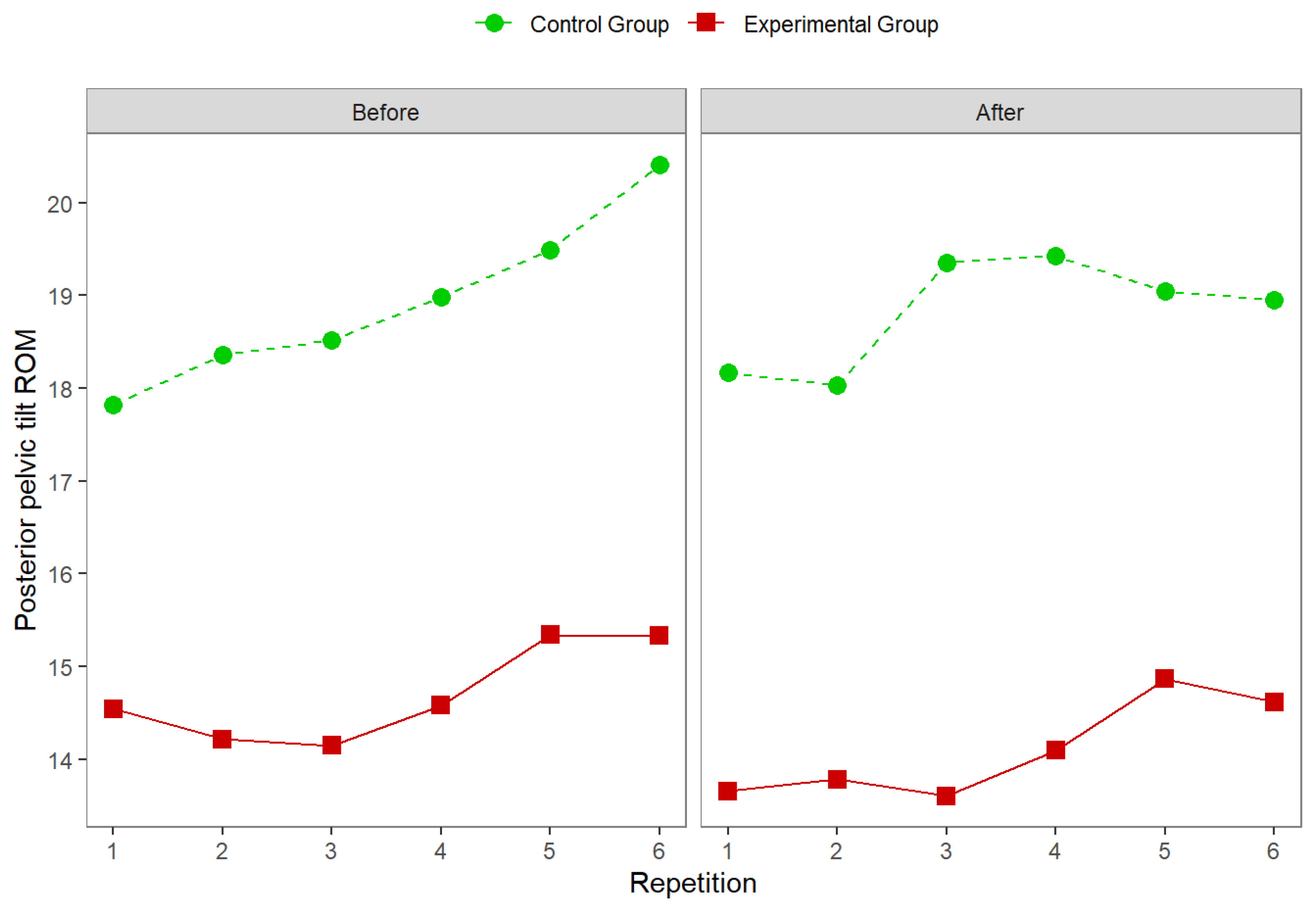
Figure 8.
Relationship between initial pelvic position and total PPT ROM before exercise intervention.
Figure 8.
Relationship between initial pelvic position and total PPT ROM before exercise intervention.
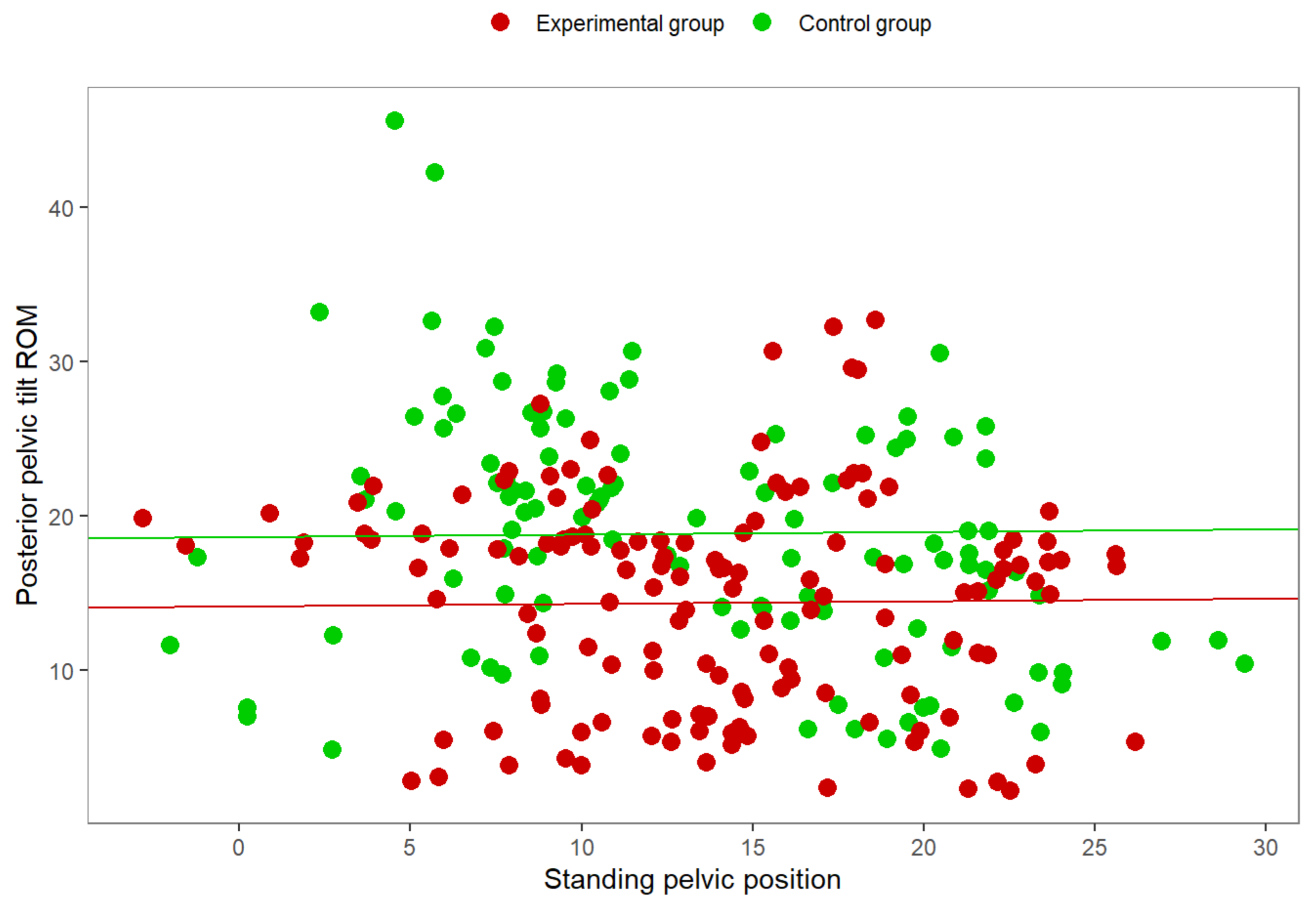

Table 1.
The exercise intervention.
| Exercise | Description | Goal |
|---|---|---|
| Cat/Cow | Assume quadruped position on knees and hands. Practice alternating from rounded back posture to arched back posture. | Identify difference between lordotic and kyphotic positions. |
| Ball Wall Squat | Pin a ball (similar to small Swiss ball) between the lower back and wall. Squat down while keeping ball pinned against the wall. The ball will roll up to the shoulder blades. Ascend and repeat. | Exercise facilitates a more vertical trunk position because horizontal force from wall serves as assistance. Ball rolling encourages the correct spinal curve. |
| Pole Squat and Fix | Perform squat near a sturdy pole or column. At apex of squat, use column as assistance to pull torso into correct position and hold. Heels must remain on the ground. | Assistance to help athlete self-generate and learn correct deep hold position. |
| Plank | Hold plank position with emphasis on maintaining lordosis throughout exercise. | Improve isometric strength of the back musculature and promote correct lumbar spine position. |
| Superman | Lay flat on stomach with your arms straight out in front and legs straight out behind. Keep arms and legs shoulder-width apart for the duration of the exercise. Lift your legs and arms simultaneously at least 6 inches off the ground. Keep each movement slow and controlled to prevent pulling muscles. | Strengthen the lower back musculature. |
| Overhead Squat | Perform squat with dowel in overhand grip overhead with elbows extended. | Strengthen back musculature and promote erect trunk during squat. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



