
Submitted:
20 October 2025
Posted:
21 October 2025
You are already at the latest version
Abstract
Malaria remains one of the most pressing public health challenges in Africa, a continent that bears a significant percentage of the global malaria morbidity and mortality. From the earliest microscopic discoveries of Plasmodium to the era of genomics and vaccine innovations, Africa has stood both as the epicentre of the disease, and the focal point of global research and control efforts. The continent’s unique ecological, genetic, and socio-political contexts have also shaped the evolution of the parasite, the host, and the mosquito vector. African scientists, institutions, and communities have progressively transitioned from being subjects of investigations to active contributors in malaria research; advancing studies in epidemiology, molecular biology, pharmacogenomics, and vaccine development. This review traces the journey of malaria science from its microscopic origins to genomic breakthroughs; emphasising how Africa’s contributions, challenges, and innovations have redefined global understanding. It also highlights the importance of locally-driven research, surveillance, and policy frameworks to translate genomic data into practical solutions, aiming towards equitable and sustainable malaria elimination on the continent.
Keywords:
Africa
; genomics
; malaria
; plasmodium
; research
; vaccine
1. Introduction
Malaria is a life-threatening yet preventable and curable mosquito-borne disease. Malaria infection arises from the transmission of a protozoan parasite to humans following the bite of an infected female Anopheles mosquitoes (Siao et al., 2020; Sato, 2021; Gozalo et al., 2024; Long et al., 2024). The typical symptoms of malaria include headaches, fever, chills, and muscle aches, progressing to severe complications including anaemia, cerebral malaria, multiorgan failures and coma if not treated rapidly (Sypniewska et al., 2017; Mamudu et al., 2025). Despite being curable and preventable, it remains a major global health problem particularly in Africa and other tropical regions (Doumbia et al., 2022; Ounjaijean and Somsak, 2025). In sub-Saharan Africa, malaria remains a major health challenge accounting for a vast majority of infections and mortality, disproportionately affecting children aged zero to five, and pregnant women (Anjorin et al., 2023). While the sub-Saharan African region continues to face persistent challenges including poverty, weak healthcare systems, climate change, drug resistance and the emergence of new vectors; significant progress has been achieved in malaria prevention and cure through interventions like the provision of insecticide-treated bed nets, insecticides, artemisinin-based combination therapies, and intermittent prophylactic treatment in high-risk groups, which resulted in a significant reduction in malaria incidence and mortality rates within the region (World Health Organization, 2023; Li et al., 2024).
The African subregion is intricately linked to the history of malaria; indeed, no other infectious disease has shaped Africa’s health, history, and development as profoundly as malaria (Bashir et al., 2025). Endemic across much of sub-Saharan Africa, malaria has not only imposed a staggering public health burden but has also influenced patterns of settlement, agricultural productivity, trade, and colonial enterprise. Over centuries, recurrent malaria epidemics have curtailed population growth, impeded economic progress, and strained fragile health systems (Badmos et al., 2021; Merga et al., 2025). The persistence of Plasmodium falciparum transmission, coupled with ecological and socio-economic vulnerabilities, continue to define the continent’s epidemiological landscape. Thus, malaria in Africa is not merely a biomedical problem; it is a developmental, historical, and psychosocial challenge intertwined with the region’s evolution and well-being (Msellemu et al., 2016; Nkumama et al., 2017; Li et al., 2024).
The history of malaria research is also inextricably linked with the African subregion, and the high burden of malarial infection in the region led to several foundational discoveries, advancing our understanding of the parasite’s co-evolution with human populations (Cox, 2010; Drouin et al., 2024). This history began with the first microscopic observation of Plasmodium parasite by Alphonse Laveran in Algeria in 1880, to the 1890s research by Ronald Ross that associated the Anopheles mosquito with transmission of the parasite, and the completion in 2002 of the first draft sequence of the plasmodium falciparum genome (Laveran, 1978; Rajakumar and Weisse, 1999; Gardner et al., 2002; Hoffman et al., 2002; Institute of Medicine, 2004; Sinden, 2007; Tan and Ahana, 2009; Su et al., 2019;Talapko et al., 2019; Pande et al., 2024). For more than a century, the African continent has served simultaneously as the laboratory of malaria science and the frontline of global control efforts, shaping and being shaped by every major advance in parasitology, vector biology, and therapeutic discovery (Institute of Medicine, 2004; Li et al., 2024). In recent decades, however, this narrative has evolved, with sustained capacity building and experience resulting in African institutions, scientists, and regional networks shifting from being peripheral contributors to central architects in the areas of malaria genomics, epidemiology, and translational research (Ghansah et al., 2014, 2019; Ishengoma et al., 2019; Tessema et al., 2019). In this narrative review, malaria’s scientific evolution (Table 1) is examined through an African lens, exploring the historical milestones, genomic breakthroughs, local innovations, and enduring challenges that continue to define the continent’s path from microscope to genome.
2. From Microscopic Discovery to Molecular Technologies
The microscopic era of malaria research began in 1880, when French military physician, Charles Louis Alphonse Laveran who was stationed in Algeria, first identified motile pigmented parasites in the blood of soldiers; this marked the discovery of Plasmodium as the causative agent of the disease (Cox, 2010; Pande et al., 2024). This breakthrough, achieved through meticulous light microscopy, was significant in transforming previously-held believes that malaria was a mysterious “miasmatic” illness, and entrenching its place as a parasitic infection (Awoyemi, 2005; Hempelmann and Krafts, 2013; Lalchandama, 2014). In the decades that followed, improvements in microscopic and histological techniques, most notably the introduction of the Romanowsky–Giemsa staining methods aided the characterisation of the biology and life cycle of different members of the plasmodium species, and also increased diagnostic accuracy of the infection. (Barcia, 2007; Wongsrichanalai et al., 2007; Krafts et al., 2011). Since the early 1900s when the German chemist, Gustav Giemsa introduced the stain that bore his name (which is a mixture of methylene blue and eosin stains), the microscopic examination of Giemsa-stained blood smears has remained a standard diagnostic technique for malaria infection.
These early discoveries not only enabled the diagnosis of malaria but also established the taxonomic foundation of malaria science, allowing the identification of four species of the Plasmodium parasite including Plasmodium falciparum (P. falciparum), Plasmodium vivax, Plasmodium malariae, and Plasmodium ovale. These species have now been confirmed to predominate across different geographical regions, with P. falciparum prevailing in Africa (Zekar and Sharman, 2023). Across Africa, microscopy also became the cornerstone of malaria diagnosis, surveillance, and research, remaining a primary method for diagnosis in most parts for more than a century (Nkrumah et al., 201; Ugah et al., 2017; Comfort et al., 2024); and till today, it continues to remain indispensable in clinical and field settings across Africa (Dhorda et al., 2020; Prah et al., 2021; Aninagyei et al., 2024; Tegegn et al., 2024).
In recent times, while microscopy remains the gold standard for malaria diagnosis, it is increasingly being complemented and, in some settings, surpassed by molecular and imaging technologies. These advanced methods offer greater speed, specificity, and sensitivity; enabling the detection of low-density parasitaemia and the identification of parasite genotypes associated with drug resistance (Calderaro et al., 2024). Techniques such as polymerase chain reaction (PCR), quantitative PCR (qPCR), loop-mediated isothermal amplification (LAMP), and next-generation sequencing (NGS) have expanded diagnostic capacity and deepened understanding of parasite diversity and evolution. In parallel, innovations in digital microscopy and artificial intelligence–assisted image analysis are transforming diagnostic accuracy and workflow efficiency (Maturana et al., 2023; Dantas de Oliveira et al., 2024; Fong Amaris et al., 2024; Rubio Maturana et al., 2024), particularly in resource-limited African laboratories. Collectively, these advances underscore the fact that while the microscope era established the cornerstone of malaria diagnosis, the field is fast transitioning toward a new phase of molecular precision and genomic insight, with Africa increasingly positioned to benefit from and contribute to this transformation.
3. The Transmission Revolution: Vector Discovery and Control in the African Context
At the turn of the 20th century, the discovery of the mosquito vector involved in the transmission of malaria marked a significant milestone in malaria research (Table 1). Sir Ronald Ross, working in Secunderabad, India, demonstrated that Anopheles mosquitoes transmit Plasmodium parasites, confirming the disease’s vector-borne nature (Capana, 2006; Cox, 2010; Raele et al., 2024). Almost simultaneously, Giovanni Battista Grassi, an Italian medical doctor/zoologist and his colleagues identified the specific Anopheles species responsible for human transmission, providing conclusive evidence of the parasite’s complex life cycle between mosquito and human hosts (Institute of Medicine, 1991; Capana, 2006; Gachelin, et al., 2018; Chaudhury, 2021; Raele et al., 2024). Though the mosquito transmission cycle was established through research in India and Italy, the field observation centres established across West and Central Africa were important in confirming the ecological link between mosquitoes, swamps, and seasonal fevers (Ferroni et al., 2012). Colonial medical services during the early 20th century documented extensive microscopic surveys in regions that are now Nigeria, Sierrea Leone, the Gambia, and the Congo; laying the foundation for modern malariology in Africa (Bump and Aniebo, 2022). Though these early efforts were led largely by colonial scientists, they produced enduring data on the distribution, vector behaviour, and parasite species diversity of the Anopheles mosquito. The earliest foundational public health institutions in Africa including the Yaba Malaria Research Station in Nigeria (Now placed within Nigerian Institute for Medical Research) and Kampala’s East African Malaria Institute were centres for training and surveillance, nurturing the first generation of African parasitologists and entomologists (Talisuna et al 2015; Nankabirwa et al., 2022; Namuganga et al., 2022). Today, these institutions were the foundation of the various centres of excellence for malaria research across sub-Saharan Africa.
The paradigm shift from considering malaria as a disease resulting from “bad air” to discovering the mosquito vector charted the path for malaria control and eradication. For the first time, prevention strategies could target the mosquito vector rather than only treating human infection. The implications for Africa, a region disproportionately affected by malaria were profound (Wilson et al., 2020; Kaura et al., 2023). The continent’s ecology, characterised by diverse Anopheles species, favourable climatic conditions, and extensive breeding habitats, provided ideal environments for sustained transmission (Ayala et al., 2009; Mattah et al., 2017; Getachew et al., 2020; Msugupakulya et al., 2023; Ebhodaghe et al., 2024). The recognition of Anopheles gambiae as the primary African vector later became a cornerstone for malaria entomology and control initiatives. Detailed understanding of the life cycle and ecological characteristics of the Anopheles gambiae provided a cornerstone for the scientific field of malaria vector entomology and the practical application of malaria control programs across sub-Saharan Africa (Killen et al., 2002; Alves et al., 02024; Takken et al., 2024).
Early vector control efforts, which included environmental management, larva source reduction, and the use of insecticides such as DDT (dichloro-diphenyl-trichloroethane) were implemented during the colonial and early postcolonial periods. These interventions which achieved variable levels of success were also constrained by socioeconomic inequities, limited infrastructure, and resistance to insecticides. Nonetheless, they laid the groundwork for modern integrated vector management programs (van den Berg, 2009; Raghavendra et al., 2011; Maheu-Giroux et al., 2021).
In post-independence Africa, the transmission era also brought scientific and institutional evolution. Field stations such as the Garki Project in Nigeria provided critical epidemiological data and modeling tools that informed global malaria strategies. The Garki Project which was conducted in northern Nigeria immediately after independence, was a landmark field study aimed at understanding malaria transmission and control in real-world African settings. From 1969 to 1976, researchers gathered extensive epidemiological data that culminated in the development of a mathematical model of malaria transmission that was far more reflective of African realities than earlier theoretical models (Nedelman, 1988). This project jointly implemented by the World Health Organisation (WHO) and the Nigerian government, tested interventions such as indoor residual spraying and mass drug administration strategies, offering critical evidence that these strategies alone were insufficient to achieve long-term malaria elimination under local ecological and social conditions (Molineaux and Gramiccia, 1980). The findings demonstrated that, despite aggressive vector control and chemotherapy, malaria elimination in high-transmission African settings required sustained, multifaceted interventions, a lesson that continues to shape policy today (Abeku et al., 2019).
The understanding of malaria transmission also stimulated behavioural and socio-environmental research, linking human activity, housing quality, and agricultural practices to transmission risk. This intersection between entomology, ecology, and social science paved the way for community-based interventions such as insecticide-treated nets (ITNs) and indoor residual spraying (IRS), that would later dominate control efforts in the late 20th and early 21st centuries (Hershey et al. 2017; Thwing et al., 2019; Kayentao et al., 2018; van den Berg et al., 2018; Win Han et al., 2019; Karemere et al., 2021). Thus, the transmission revolution not only clarified malaria’s biological ecology but also redefined its public health identity, establishing Africa as both the epicentre of the disease and the testing ground for innovation in vector control, community engagement, and policy formulation.
4. The Vector and the Environment: Africa’s Ecological Uniqueness
Malaria transmission in Africa is shaped by an intricate interplay of vector biology, environmental factors, and human behaviour; creating conditions that are both unique and challenging for control efforts. The African landscape, with its diverse climate zones from humid rainforests to dry savannahs and highlands provides optimal breeding habitats for Anopheles mosquitoes, the most efficient malaria vectors in the world. Understanding this ecological uniqueness is key to designing context-specific interventions.
Africa hosts more than 140 species of Anopheles, but only a few dominate malaria transmission. The predominant ones are Anopheles gambiae sensu stricto, Anopheles arabiensis, and Anopheles funestus, who’s exceptional anthropophily and endophilic behaviour make them highly effective vectors (Msugupakulya et al., 2023). Anopheles gambiae, in particular, is often described as “the most efficient malaria vector known to man,” capable of transmitting Plasmodium with remarkable precision and adaptability (Shaw et al., 2021). This efficiency, coupled with genetic plasticity, contributes to persistent malaria transmission even in areas of high intervention coverage.
The ecological settings of Africa foster continual malaria transmission. Rainfall patterns, temperature, and humidity directly influence mosquito breeding and parasite development rates. In tropical regions, the perennial availability of stagnant water ranging from puddles and rice paddies to urban drainages ensures sustained vector populations (Chaptoterera et al., 2025). In contrast, semi-arid zones experience seasonal transmission, with peaks corresponding to the rainy season. Climate change, through rising temperatures and altered precipitation patterns, is increasingly expanding the geographic range of vectors into previously non-endemic highland regions of East Africa and southern Africa (Chaptoterera et al., 2025).
Rapid and often unplanned urban growth in African cities introduces new ecological dynamics. Poor drainage, overcrowding, and intermittent water supply create artificial breeding habitats, while shifts in housing structures and human activity patterns affect exposure risk. Meanwhile, agricultural practices such as irrigation and deforestation alter local ecologies, expanding vector habitats and changing species composition (Aliyu and Amadu, 2017). The overlap of rural and peri-urban transmission patterns complicates vector control, requiring integrated approaches that consider local livelihood systems.
Addressing Africa’s ecological complexity requires interventions tailored to local environmental and social contexts. Current strategies include the deployment of dual-insecticide nets, larva source management, biological control agents (e.g., larvivorous fish, Bacillus thuringiensis israelensis), and environmental engineering. Additionally, innovative tools such as gene-drive mosquitoes, developed with contributions from African research institutions, aim to suppress or modify vector populations in the long term. Africa’s ecological uniqueness defined by its biodiversity, climatic diversity, and socio-environmental interactions makes malaria control both a biological and ecological challenge. Recognising and leveraging these unique conditions are essential for sustainable malaria elimination. As vector ecology continues to evolve under the pressures of climate change and human development, Africa’s environmental research will play a pivotal role in shaping adaptive, eco-smart malaria control strategies.
5. Chemotherapeutic Advances and Roadblocks: From Quinine to Artemisinin Resistance in Africa
The history of malaria therapy is deeply intertwined with the global evolution of the science of pharmacology and Africa’s colonial and postcolonial experience (Table 2). For centuries, the use of traditional herbal remedies, including using the bark of the cinchona tree (which contains the antimalarial drug quinine) and the neem tree were used to treat malaria. The successful extraction of quinine from the bark of the cinchona tree in the 17th century provided the first antimalarial agent (Baird et al., 1996; Garforth, 2007; Nosten and White, 2007; Dkarani et al., 2008; Butler et al., 2010; Permin et al., 2016; Kokori et al., 2024). The discovery of quinine would go on to shape both military and colonial expansion into tropical Africa by providing a means to survive in endemic regions once deemed the “white man’s grave” (Brockway, 1979; (Fredj, 2016; Ratschiller Nasim, 2023). However, while quinine saved countless lives, it also symbolised the uneven power dynamics of colonial medicine, as its availability and use were often restricted to colonial officials and elites, leaving local populations with limited access. Quinine remained the only known antimalarial agent until the 19th century. The global shortage of quinine prompted an urgent scientific drive to develop synthetic alternatives (Goss, 2014; Cassauwers, 2015). This effort accelerated the discovery of novel compounds such as chloroquine in 1934, and its official adoption in 1946 as the drug of choice for malaria treatment worldwide, capable of replacing quinine as the principal antimalarial therapy (US Institute of Medicine, 2004; MMV, 2025). Nonetheless, quinine has retained its therapeutic relevance as a secondary or backup medicine, particularly in severe malaria cases.
The mid-twentieth century witnessed the rise of other synthetic antimalarials, including amodiaquine, and sulfadoxine-pyrimethamine (SP), which were affordable and widely distributed across Africa during the 1950s–1970s (Vestergaad and Ringwald, 2007; Onaolapo et al., 2018). Chloroquine in particular, became a mainstay of malaria control and was considered at the time a “miracle drug.” Yet, by the 1980s, resistance of Plasmodium falciparum to chloroquine had spread rapidly across Africa, undermining decades of progress (von Seidlein et al.,1997, Baird, 2004; Wurtz et al., 2012; Tse et al., 2019; Pandey et al., 2023). This wave of resistance was later traced to mutations in two transmembrane transporter including P. falciparum multidrug resistance protein 1 (PfMDR1) and P. falciparum chloroquine resistance transporter (PfCRT) genes, which have provided some of the earliest molecular insights into the adaptive capacity of the parasite (EANMAT, 2003; Viega et al., 2006; Zhou et al., 2020; Silva et al., 2022). Moreover, the persistent burden of malaria, coupled with the emergence of chloroquine resistance has led to sustained global efforts to develop more effective chemotherapeutic agents and consider multidrug therapy for malaria infections.
In response to the failure of monotherapies, the late twentieth and early twenty-first centuries saw the global adoption of artemisinin-based combination therapies (ACTs), derived from Artemisia annua, a plant long used in traditional Chinese medicine (Eastman and Fidock, 2009; Su and Miller, 2015; Morua et al., 2025). Artemisinin-based combination therapies quickly became the first-line treatment for P. falciparum malaria, and their deployment in Africa dramatically reduced malaria morbidity and mortality, particularly among children under five (Bhattarai et al., 2007; Nosten and White, 2007; Maiga et al., 2021). Africa became both the largest consumer and the primary testing ground for ACT efficacy. The emergence of partial artemisinin resistance, a phenomenon first observed in Southeast Asia and now appearing in countries like Rwanda, Uganda, and Eritrea (Mihreteab et al., 2023, 2025; Agaba et al., 2024) underscores another urgent threat to the continent’s malaria control achievements. This resistance, caused by mutations in the parasite’s k13 gene, means that artemisinin-based drugs take longer to clear parasites from the blood, increasing the risk of treatment failure and further spread of resistance (Agaba et al., 2024; Milong et al., 2024; Zheng et al., 2024; Oyegbade et al., 2025)
Molecular surveillance has become a cornerstone of contemporary malaria pharmacology. African researchers are at the forefront of monitoring resistance-associated mutations in pfkelch13, pfcrt, and pfmdr1 genes using genomic and molecular diagnostic tools (Zhou et al., 2019; Cheng et al., 2021; Zhao et al., 2021; Martín Ramírez et al., 2025). The monitoring of resistance patterns assists in the understanding of the prevalence and spread of drug resistance; enabling informed public health policies and the development of more effective treatment strategies, especially as new mutations emerge and spread (Zhao et al., 2021; Wang et al., 2022; Alruwaili et al., 2025; Dakorah et al., 2025; Martín Ramírez et al., 2025). These efforts are supported by regional initiatives such as the Malaria Genomic Epidemiology Network, West African Network for Clinical Trials of Antimalarial Drugs, the Pathogenic Diversity Network Africa, and the Plasmodium Diversity Network Africa, which are strengthening genomic surveillance capacity and promoting data sharing across national borders. The rise of multidrug-resistant Plasmodium strains and emerging partial resistance to newer drugs have further intensified the urgency for continuous research and innovation in antimalarial therapy.
Beyond conventional chemotherapy, renewed attention is being directed toward traditional medicinal plants, reflecting a shift towards Afrocentric pharmacognosy which is driven by the need to combat drug-resistant malaria, the high cost, and accessibility problems of modern drugs, and the rich biodiversity of the continent (Onukansi et al., 2025). Several African botanicals including Azadirachta indica (neem), Cryptolepis sanguinolenta, Morinda lucida, Vernona Amygdalina, Markhamia tomentosa, Polyalthia longifolia, and Trichilia heudelotii are being systematically evaluated for their antiplasmodial and immunomodulatory properties, integrating indigenous knowledge into contemporary drug discovery pipelines (Osunderu, 2009; Alebie et al., 2017; Onukansi et al., 2025). Thus, the history of malaria therapeutics in Africa represents more than a pharmacological evolution; it is a chronicle of adaptation, resistance, and rediscovery. From quinine to artemisinin, Africa has not only endured the shifting tides of drug efficacy but has also increasingly become a critical contributor to global malaria pharmacogenomics, policy, and innovation.
6. The African Genomic Awakening
The decoding of the P. falciparum genome in 2002 opened new possibilities for understanding malaria biology; however, it also revealed a crucial reality that most genomic data were derived from African isolates (Mobegi et al 2014; Ajibaye et al., 2020; Kassegne et al., 2020; Metoh et al., 2020), where the infrastructure to analyse this data was lacking. This created a bottleneck, limiting the ability of local researchers to participate in and benefit from advancements, although significant efforts have since been made to improve sequencing and data analyses capabilities in Africa. Also, Africa, being the heart of P. falciparum diversity, became central to understanding parasite evolution and resistance mechanisms. Subsequent initiatives such as the MalariaGEN Consortium, Human, Heredity and Health (H3) Africa, and Plasmodium Diversity Network Africa (PDNA) to mention a few have continued to empower African researchers to generate and analyse high-quality genomic data locally (MalariaGEN et al., 2023, 2025). These platforms have uncovered patterns of drug resistance gene spread (e.g., pfcrt, pfmdr1, kelch13) and mapped regional population structures of Plasmodium and Anopheles species (MalariaGEN, 2008).
African scientists now leverage next-generation sequencing to lead malaria research, monitor parasite adaptation, vector evolution, and host–parasite genetic interactions. Studies in Ghana, Mali, Uganda, and Nigeria are decoding how local immunity and genetic traits (e.g., sickle cell haemoglobin, G6PD deficiency, Duffy negativity) influence malaria susceptibility and treatment outcomes. This genomic renaissance marks Africa’s transition from data scarcity to data leadership in malaria research.
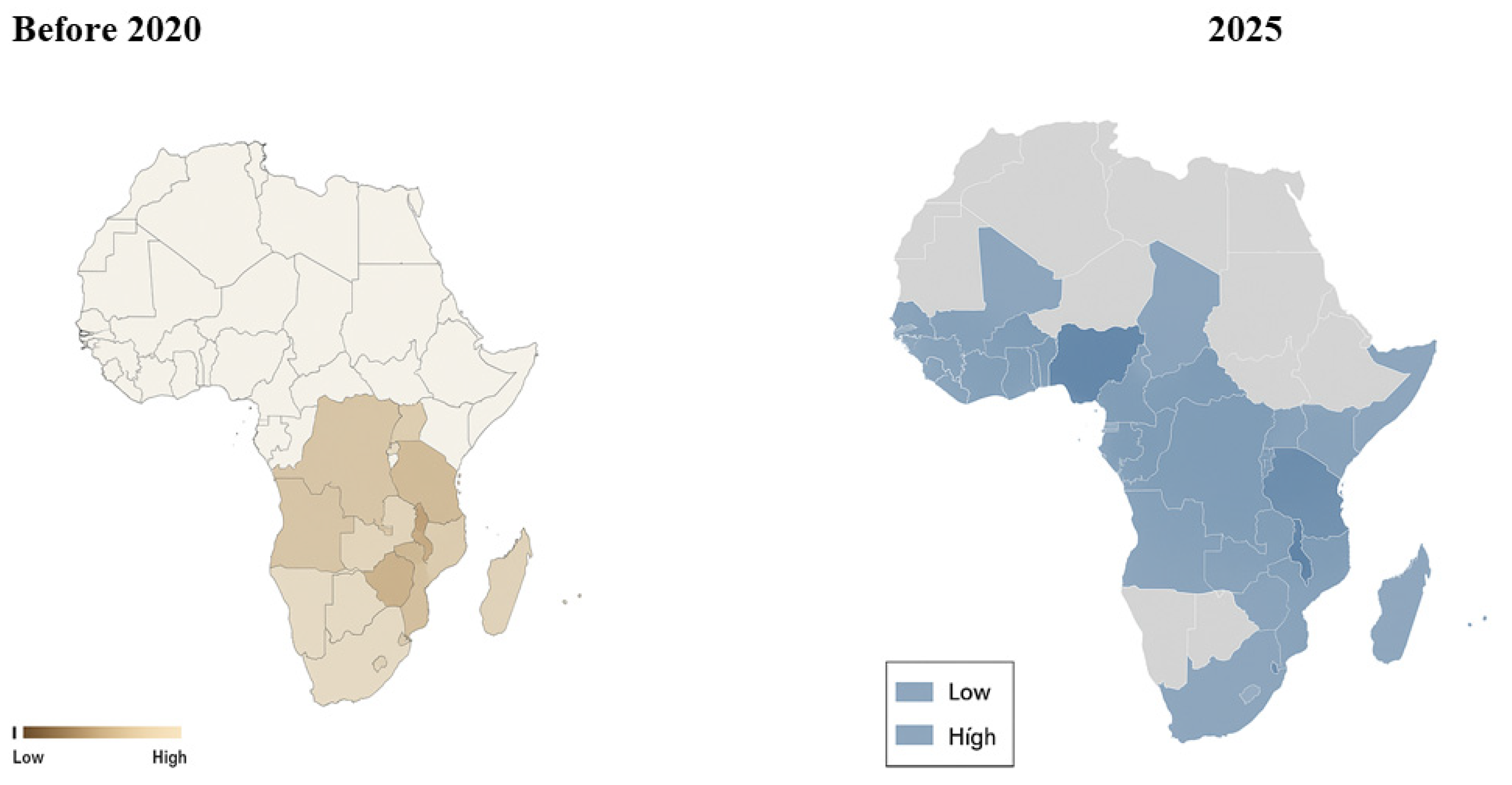
Figure 1.
Genomic Surveillance Networks for Malaria across Africa, then and now. Image generated using ChatGPT. The image was generated in response to this prompt: ‘Create an image that shows genomic surveillance networks for Malaria across Africa before the year 2020 and now in the year 2025.
Figure 1.
Genomic Surveillance Networks for Malaria across Africa, then and now. Image generated using ChatGPT. The image was generated in response to this prompt: ‘Create an image that shows genomic surveillance networks for Malaria across Africa before the year 2020 and now in the year 2025.
7. Vaccines and Immunity: African Contributions to the Next Frontier in Malaria Control
The quest for an effective malaria vaccine represents one of the most ambitious endeavours in global health, and Africa has been central to every phase of this journey (Effiong et al., 2022; Alum et al., 2025). Given that the continent bears over 90% of the global malaria burden, African populations, scientists, and institutions have been both the recipients and the drivers of vaccine innovation, immune profiling, and clinical evaluation (Table 3). African scientists and institutions are actively driving innovation, with initiatives like the African Malaria Network Trust (AMANET) focusing on vaccine research and capacity building (Sibomana et al., 2025). Unlike many other infectious diseases, malaria presents a formidable immunological challenge owing to the complex life cycle of Plasmodium species, their capacity for antigenic variation, and the parasite’s co-evolution with the human immune system in endemic regions (Crutcher and Hoffman, 1996; Crompton et al., 2014; Pikor et al., 2016; Gross et al., 2021). For centuries, efforts to understand natural immunity in African populations have informed global vaccine design, reflecting Africa’s centrality to malaria immunology and translational research (Crutcher and Hoffman, 1996; Crompton et al., 2014; Pikor et al., 2016; Gross et al., 2021; Kalkal et al., 2022).
The early recognition that individuals in endemic regions develop partial immunity to malaria after repeated exposure provided the conceptual foundation for vaccine development (Dolan et al., 2009; Barry and Hansen, 2016; Chan et al., 2020; Opi et al., 2021). African epidemiological studies including those conducted in The Gambia, Nigeria, and Tanzania assisted in defining the dynamics of naturally-acquired immunity, distinguishing between protection against severe disease, and sterile immunity (Pinkevych et al., 2012; Deroost et al.,2016). Observations of asymptomatic parasitaemia, age-dependent immunity, and protection conferred by genetic traits such as the sickle-cell mutation and the glucose-6-phosphate dehydrogenase deficiency offered profound insights into host–parasite interactions (Moormann et al., 2003; Awah et al., 2012; Gong et al., 2012). These findings not only explained regional variations in malaria burden but also guided vaccine development strategies targeting pre-erythrocytic and blood-stage antigens. These insights guided the identification of immunogenic parasite antigens, including circumsporozoite protein, merozoite surface (MSP), and apical membrane antigens (AMA), which remain key targets for subunit vaccine development (Woehlbier et al., 2010; El-Moamly and El-Sweify, 2023).
Malaria vaccines are broadly classified based on the developmental stage of the parasite they are designed to target. These include pre-erythrocytic vaccines, which aim to prevent infection at the liver stage; erythrocytic or blood-stage vaccines, which seek to limit parasite multiplication and disease severity; and transmission-blocking vaccines, which interrupt the parasite’s transmission from humans to mosquitoes (El-Moamly and El-Sweify, 2023). While most candidates focus on a single stage, a few are being developed to act across two or more phases of the parasite’s life cycle (El-Moamly and El-Sweify, 2023). A landmark breakthrough in the field was the RTS, S/AS01 (Mosquirix™) vaccine, the first vaccine candidate to achieve regulatory approval for use in humans (Laurens, 2022; Egbewande, 2022; Praet et al., 2022). Developed through collaboration between GlaxoSmithKline (GSK) and PATH, RTS, S was extensively evaluated in phase II and III clinical trials conducted in several African countries, including Ghana, Kenya, Malawi, and Tanzania (Laurens, 2022; Egbewande, 2022; Praet et al., 2022). The vaccine, which targets the circumsporozoite protein (CSP) of Plasmodium falciparum, offered modest yet meaningful protection, particularly among African children. With an efficacy of approximately 30–50% against clinical malaria, these pivotal trials provided the scientific basis for its pilot introduction in 2019 under the coordination of the World Health Organisation (WHO), a milestone in global and African malaria control efforts (Laurens, 2022; Egbewande, 2022; Praet et al., 2022). The R21/Matrix-M vaccine, developed by Oxford University and the Centre National de Recherche et de Formation sur le Paludisme (CNRFP), is a malaria vaccine that has shown similar or better efficacy than RTS, S, with a lower cost and acceptable safety profile; it also achieved over 75% efficacy in Phase II trials (Oduoye et al., 2024; Schmit et al., 2024; Venkatraman et al., 2025; WHO, 2025). African institutions and scientists played a pivotal role at every stage from its clinical evaluation to implementation. The large-scale pilot trials in these countries provided the decisive data on vaccine safety, efficacy, and feasibility that underpinned the WHO’s 2021 recommendation for widespread use (WHO, 2021). This represents a profound paradigm shift with Africa as the epicentre of both discovery and validation in global vaccine science. In 2023, the WHO endorsed R21 for broad use, marking not only a scientific breakthrough but also a symbolic achievement for African-led research capacity. This success reflects a shift from dependency to partnership, where African laboratories, data systems, and ethics frameworks now underpin the next generation of vaccine innovation and deployment strategies.
African immunologists and epidemiologists have also provided invaluable insights into host–parasite interactions and immune correlates of protection (Kibwana et al., 2024; Ogwang et al., 2025). Studies conducted in endemic areas revealed that antibody-mediated and T-cell–dependent mechanisms vary with transmission intensity, age, and genetic background. Moreover, research from institutes such as KEMRI-Wellcome Trust (Kenya), MRC Unit in The Gambia, and Noguchi Memorial Institute (Ghana) has refined understanding of how immunity develops over time, and how vaccine responses differ among African populations (Mannan et al., 2003; Shelton et al., 2015; Odhiambo et al., 2025).
As parasite diversity and antigenic variation continue to challenge vaccine durability, African laboratories are increasingly participating in genomic and immune epidemiological research to design next-generation vaccines (Gunawardena and Karunaweera, 2015; Shelton et al., 2015; Hafalla et al., 2025). Multi-stage formulations combining pre-erythrocytic, blood-stage, and transmission-blocking components are now under evaluation in African sites, reflecting a shift toward integrated, locally-relevant vaccine strategies (Tachibana et al., 2025). Africa’s role in malaria vaccine research has evolved from that of a passive testing ground to that of a scientific collaborator and innovator. The continent’s immunological diversity, clinical research infrastructure, and growing cadre of trained vaccine scientists position it at the forefront of the next phase in malaria control and elimination. As the world moves toward more durable, multi-stage vaccines, Africa’s sustained leadership will remain indispensable in ensuring that immunological discoveries translate into equitable, context-sensitive public health gains.
8. From Policy to Practice: Translating Science into Sustainable Malaria Control in Africa
Scientific advances in malaria research, spanning diagnostics, therapeutics, and vector control—have significantly shaped global and regional malaria policies. However, translating these scientific insights into sustainable, community-level impact across Africa has remained a persistent challenge. The success of malaria control depends not only on innovation but on the effective integration of research outcomes into national health systems, policies, and behavioural practices (Table 4).
Following the Roll Back Malaria (RBM) Initiative launched in 1998, African governments, through partnerships with the World Health Organisation (WHO), African Union (AU), and local research networks, began implementing evidence-based strategies such as insecticide-treated nets (ITNs), indoor residual spraying (IRS), and intermittent preventive treatment (IPT). These interventions were guided by data from entomological and epidemiological studies that demonstrated their cost-effectiveness and population-level benefits (Pyrce et al., 2022; Obembe et al., 2024). Yet, varying ecological conditions, resource limitations, and health system disparities across the continent often determined the degree of implementation success.
Recent years have seen a shift towards data-driven and adaptive malaria control policies, integrating insights from genomic surveillance, real-time mapping of vector resistance, and community-based participatory approaches (Obeagu and Obeagu, 2024). Countries such as Ghana, Rwanda, and Zambia have incorporated national malaria control programmes (NMCPs) with continuous feedback mechanisms linking researchers, policymakers, and frontline health workers. This approach has strengthened accountability, resource allocation, and response to local transmission dynamics.
Nevertheless, sustainable malaria control in Africa must extend beyond biomedical interventions to address socioeconomic, behavioural, and environmental determinants. Poverty, inadequate housing, and weak infrastructures perpetuate malaria transmission cycles, while climate change and population displacement introduce new ecological pressures. As a result, future policy frameworks must embrace a One Health perspective, integrating human, environmental, and animal health for comprehensive resilience. Ultimately, bridging the gap between scientific discovery and practical implementation requires capacity building, local innovation, and sustained investment. Empowering African scientists, expanding regional manufacturing of diagnostics/ vaccines, and ensuring equitable access to preventive tools are critical steps toward self-reliant and sustainable malaria control across the continent.
9. The Future of Malaria Research in Africa
Africa’s scientific landscape is rapidly changing. The integration of artificial intelligence, metabolomics, and spatial genomics is transforming malaria surveillance and control. Regional networks are developing AI-driven early warning systems and portable sequencing platforms capable of field-level resistance monitoring. Innovations such as gene drive mosquitoes, microbiome engineering, and precision medicine approaches hold promise, but must be guided by ethical frameworks rooted in African contexts. Ultimately, malaria elimination in Africa will require more than biomedical tools, it demands an integrated approach combining molecular science, socio-economic reform, community engagement, and environmental management.
10. Conclusions
Africa’s malaria story has been one of pain, persistence, and progress. From the first microscopic discovery of Plasmodium in Algeria to the sequencing of African parasite genomes, the continent has transitioned from a passive subject of research to a leading voice in global malaria science. The journey from microscope to genome mirrors Africa’s broader scientific awakening characterised by resilience, innovation, and self-determination. As genomic and molecular tools become increasingly accessible, Africa’s greatest opportunity lies in translating knowledge into context-specific solutions that save lives, strengthen systems, and ultimately end malaria’s centuries-long reign. The next chapter of malaria control will not be written in foreign laboratories alone; it will also be authored in African research centres, field stations, and communities, where science and survival continue to meet.
Funding
None declared.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abeku TA, Helinski ME, Kirby MJ, Kefyalew T, Awano T, Batisso E, Tesfaye G, Ssekitooleko J, Nicholas S, Erdmanis L, Nalwoga A, Bass C, Cose S, Assefa A, Kebede Z, Habte T, Katamba V, Nuwa A, Bakeera-Ssali S, Akiror SC, Kyomuhangi I, Tekalegne A, Magumba G, Meek SR. Monitoring changes in malaria epidemiology and effectiveness of interventions in Ethiopia and Uganda: Beyond Garki Project baseline survey. Malar J. 2015 Sep 4;14:337. Erratum in: Malar J. 2019 Nov 25;18(1):373. 10.1186/s12936-019-3006-5. [CrossRef]
- Agaba BB, Travis J, Smith D, Rugera SP, Zalwango MG, Opigo J, Katureebe C, Mpirirwe R, Bakary D, Antonio M, Khalid B, Ngonzi J, Kamya MR, Kaleebu P, Piot P, Cheng Q. Emerging threat of artemisinin partial resistance markers (pfk13 mutations) in Plasmodium falciparum parasite populations in multiple geographical locations in high transmission regions of Uganda. Malar J. 2024 Nov 5;23(1):330. [CrossRef]
- Ajibaye O, Osuntoki AA, Balogun EO, Olukosi YA, Iwalokun BA, Oyebola KM, Hikosaka K, Watanabe YI, Ebiloma GU, Kita K, Amambua-Ngwa A. Genetic polymorphisms in malaria vaccine candidate Plasmodium falciparum reticulocyte-binding protein homologue-5 among populations in Lagos, Nigeria. Malar J. 2020 Jan 6;19(1):6. [CrossRef]
- Alebie G, Urga B, Worku A. Systematic review on traditional medicinal plants used for the treatment of malaria in Ethiopia: trends and perspectives. Malar J. 2017 Aug 1;16(1):307. [CrossRef]
- Aliyu AA, Amadu L. Urbanization, cities, and health: The challenges to Nigeria - A review. Ann Afr Med. 2017 Oct-Dec;16(4):149-158. [CrossRef]
- Alruwaili M, Elderdery A, Manni E, Mills J. A Narrative Review on the Prevalence of Plasmodium falciparum Resistance Mutations to Antimalarial Drugs in Rwanda. Trop Med Infect Dis. 2025 Mar 29;10(4):89. [CrossRef]
- Alum EU, Ainebyoona C, Egwu CO, Onohuean H, Ugwu OP, Uti DE, Alum BN, Echegu DA. Mitigation of Malaria in Sub-Saharan Africa through Vaccination: A Budding Road Map for Global Malaria Eradication. Ethiop J Health Sci. 2025 May;35(3):205-217. [CrossRef]
- Alves G, Troco AD, Seixas G, Pabst R, Francisco A, Pedro C, Garcia L, Martins JF, Lopes S. Molecular and entomological surveillance of malaria vectors in urban and rural communities of Benguela Province, Angola. Parasit Vectors. 2024 Mar 6;17(1):112. [CrossRef]
- Aninagyei E, Deku JG, Yemofio KT, Quainoo E, Ntiri KA, Yaro E, Essandoh P, Agbogli HK, Asmah RH. Comparative evaluation of the diagnostic accuracies of four different malaria rapid diagnostic test kits available in Ghana. PLoS One. 2024 May 7;19(5):e0302840. [CrossRef]
- Anjorin, S., Okolie, E. & Yaya, S. Malaria profile and socioeconomic predictors among under-five children: an analysis of 11 sub-Saharan African countries. Malar J 22, 55 (2023). [CrossRef]
- Awah FM, Nwanedo CG., Salami IO, Azeke AE, Mbaike N A possible protective role of glucose-6-phosphate dehydrogenase deficiency and sickle haemoglobin genes against severe malaria in Madonna University, Elele Community. Journal of Medicine and Medical Sciences 2012;3(6) pp. 375-381. Available online: http://www.interesjournals.org/JMMS.
- Awoyemi A.O ‘Miasma’ theory and the possibility of malaria eradication. African Journal of Clinical and Experimental Microbiology, 2005, Vol. 6, No. 2, 153-158.
- Ayala D, Costantini C, Ose K, Kamdem GC, Antonio-Nkondjio C, Agbor JP, Awono-Ambene P, Fontenille D, Simard F. Habitat suitability and ecological niche profile of major malaria vectors in Cameroon. Malar J. 2009 De.
- Badmos AO, Alaran AJ, Adebisi YA, Bouaddi O, Onibon Z, Dada A, Lin X, Lucero-Prisno DE 3rd. What sub-Saharan African countries can learn from malaria elimination in China. Trop Med Health. 2021 Oct 24;49(1):86. [CrossRef]
- Baird J K, Caneta-Miguel E, Masba S, Bustos D G, Abrenica J A, Layawen A V, Calulut J M, Leksana B, Wignall F S. Survey of resistance to chloroquine of falciparum and vivax malaria in Palawan, The Philippines. Trans Roy Soc Trop Med Hyg. 1996;90:413–414. [CrossRef]
- Baird, JK. Chloroquine resistance in Plasmodium vivax. Antimicrob Agents Chemother. 2004;48:4075–4083.
- Barcia, JJ. The Giemsa stain: its history and applications. Int J Surg Pathol. 2007 Jul;15(3):292-6. [CrossRef]
- Barry A, Hansen D. Naturally acquired immunity to malaria. Parasitology. 2016 Feb;143(2):125–128.
- Bashir, S.G., Ahmed, N.I., Abdullahi, Y.B. et al. The burden of malaria in East Africa: prevalence, risk factors, and control strategies. Malar J 24, 255 (2025). [CrossRef]
- Berzosa P, Esteban-Cantos A, García L, González V, Navarro M, Fernández T, Romay-Barja M, Herrador Z, Rubio JM, Ncogo P, Santana-Morales M, Valladares B, Riloha M, Benito A. Profile of molecular mutations in pfdhfr, pfdhps, pfmdr1, and pfcrt genes of Plasmodium falciparum related to resistance to different anti-malarial drugs in the Bata District (Equatorial Guinea). Malar J. 2017 Jan 13;16(1):28. [CrossRef]
- Bhattarai A, Ali AS, Kachur SP, Mårtensson A, Abbas AK, Khatib R, Al-Mafazy AW, Ramsan M, Rotllant G, Gerstenmaier JF, Molteni F, Abdulla S, Montgomery SM, Kaneko A, Björkman A. Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar.
- Brockway L ’Science and Colonial Expansion: The Role of the British Royal Botanic Gardens’, American Ethnologist, vol.6, p.449–465, 1979.
- Bump JB, Aniebo I. Colonialism, malaria, and the decolonization of global health. PLOS Glob Public Health. 2022 Sep 6;2(9):e0000936. [CrossRef]
- Bump JB, Aniebo I. Colonialism, malaria, and the decolonization of global health. PLOS Glob Public Health. 2022 Sep 6;2(9):e0000936. [CrossRef]
- Butler AR, Khan S, Ferguson E. A brief history of malaria chemotherapy. J R Coll Physicians Edinb. 2010 Jun;40(2):172-7. [CrossRef]
- Calderaro A, Piccolo G, Chezzi C. The Laboratory Diagnosis of Malaria: A Focus on the Diagnostic Assays in Non-Endemic Areas. Int J Mol Sci. 2024 Jan 5;25(2):695. [CrossRef]
- Capanna, E. Grassi versus Ross: who solved the riddle of malaria? Int. Microbiol. 2006; 9(1).
- Cassauwers T. The global history of quinine, the world’s first anti-malaria drug. Medium, 2015, available online at. Available online: https://medium.com/@tcassauwers/the-global-history-of-the-world-s-first-anti-malaria-drug-d1e11f0ba729.
- Chan JA, Loughland JR, de Labastida Rivera F, SheelaNair A, Andrew DW, Dooley NL, Wines BD, Amante FH, Webb L, Hogarth PM, McCarthy JS, Beeson JG, Engwerda CR, Boyle MJ. Th2-like T Follicular Helper Cells Promote Functional Antibody Production during Plasmodium falciparum Infection. Cell Rep Med. 2020 Dec 22;1(9):100157. [CrossRef]
- Chapoterera B, Naidoo K, Marume A. Impact of climate change on malaria transmission in Africa: A scoping review of literature. J Public Health Afr. 2025 Aug 28;16(1):1346. [CrossRef]
- Chaudhury, A. The forgotten malariologist: Giovanni Battista Grassi (1854-1925). Trop Parasitol. 2021 Jan-Jun;11(1):16-18. [CrossRef]
- Cheng W, Song X, Tan H, Wu K, Li J. Molecular surveillance of anti-malarial resistance pfcrt, pfmdr1, and pfk13 polymorphisms in African Plasmodium falciparum imported parasites to Wuhan, China. Malar J. 2021 May 1;20(1):209. [CrossRef]
- Comfort DT, Ombugadu R.J, YakO AB, Tongjura JDC, Olayinka MD, Gloria E. Adeniyi KA Comparison of Microscopy and Rapid Diagnostic Techniques in Malaria Detection Among Children Attending Federal Medical Centre, Keffi, Nasarawa State, Nigeria. Dutse Journal of Pure and Applied Sciences (DUJOPAS), 2024; 10(4a).
- Cox, F.E. History of the discovery of the malaria parasites and their vectors. Parasites Vectors 3, 5 (2010). [CrossRef]
- Crompton PD, Moebius J, Portugal S, Waisberg M, Hart G, Garver LS, Miller LH, Barillas-Mury C, Pierce SK. Malaria immunity in man and mosquito: insights into unsolved mysteries of a deadly infectious disease. Annu Rev Immunol. 2014;32:157-87. [CrossRef]
- Crutcher JM, Hoffman SL. Malaria. In: Baron S, editor. Medical Microbiology. 4th edition. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 83. Available online: https://www.ncbi.nlm.nih.gov/books/NBK8584/.
- Dakorah MP, Aninagyei E, Attoh J, Adzakpah G, Tukwarlba I, Acheampong DO. Profiling antimalarial drug-resistant haplotypes in Pfcrt, Pfmdr1, Pfdhps and Pfdhfr genes in Plasmodium falciparum causing malaria in the Central Region of Ghana: a multicentre cross-sectional study. Ther Adv Infect Dis. 2025 Feb 17;12:20499361251319665.
- Dantas de Oliveira A, Rubio Maturana C, Zarzuela Serrat F, Carvalho BM, Sulleiro E, Prats C, Veiga A, Bosch M, Zulueta J, Abelló A, Sayrol E, Joseph-Munné J, López-Codina D. Development of a low-cost robotized 3D-prototype for automated optical microscopy diagnosis: An open-source system. PLoS One. 2024 Jun 21;19(6):e0304085. [CrossRef]
- Deroost K, Pham T-T, Opdenakker G,. Van den Steen PE. The immunological balance between host and parasite in malaria, FEMS Microbiology Reviews, Volume 40, Issue 2, March 2016, Pages 208–257. [CrossRef]
- Dharani N., Rukunga G., Yenesew A., Mbora A., Mwaura L. and Jamnadass R. (2008): Common Antimalarial Trees and Shrubs of East Africa. World Agroforestry Centre. ISBN: 978-92-9059-238-.
- Dhorda M, Ba EH, Kevin Baird J, Barnwell J, Bell D, Carter JY, Dondorp A, Ekawati L, Gatton M, González I, Guérin PJ, Incardona S, Lilley K, Menard D, Nosten F, Obare P, Ogutu B, Olliaro PL, Price RN, Proux S, Ramsay AR, Reeder JC, Silamut K, Sokhna C; Research Malaria Microscopy Working Group. Towards harmonization of microscopy methods for malaria clinical research studies. Malar J. 2020 Sep 4;19(1):324. [CrossRef]
- Doolan DL, Dobano C, Baird JK. Acquired immunity to malaria. Clin Microbiol Rev. 2009 Jan;22(1):13–36.
- Doumbia S, Toure M, Sogoba N, Alifrangis M, Diakite M, Diarra A, Keita M, Konaté D, Diawara SI, Thiam SM, Keita S, Tounkara M, Cissé I, Sanogo V, Magassa MH, Barry AE, Winch PJ, Marker HC, Shaffer JG, Traoré SF, Müller GC, Cui L, Beier JC, Mihigo J. The West Africa ICEMR Partnerships for Guiding Policy to Improve the Malaria Prevention and Control. Am J Trop Med Hyg. 2022 Oct 11;107(4_Suppl):84-89. [CrossRef]
- Drouin, E., Hautecoeur, P. & Markus, M. Who was the first to visualize the malaria parasite?. Parasites Vectors 17, 184 (2024). [CrossRef]
- East African Network for Monitoring Antimalarial Treatment (EANMAT). The efficacy of antimalarial monotherapies, sulphadoxine–pyrimethamine and amodiaquine in East Africa: implications for sub-regional policy. Trop Med Int Health. 2003;8:860–867.
- Eastman RT, Fidock DA. Artemisinin-based combination therapies: a vital tool in efforts to eliminate malaria. Nat Rev Microbiol. 2009 Dec;7(12):864-74. [CrossRef]
- Ebhodaghe FI, Sanchez-Vargas I, Isaac C, Foy BD, Hemming-Schroeder E. Sibling species of the major malaria vector Anopheles gambiae display divergent preferences for aquatic breeding sites in southern Nigeria. Malar J. 2024 Feb 27;23(1):60. [CrossRef]
- Effiong FB, Makata VC, Elebesunu EE, Bassey EE, Salachi KI, Sagide MR, Abdulameed HT, Uwishema O. Prospects of malaria vaccination in Nigeria: Anticipated challenges and lessons from previous vaccination campaigns. Ann Med Surg (Lond). 2022 Aug 17;81:104385. [CrossRef]
- Egbewande, OM. The RTS,S malaria vaccine: Journey from conception to recommendation. Public Health Pract (Oxf). 2022 Jun 17;4:100283. [CrossRef]
- El-Moamly AA, El-Sweify MA. Malaria vaccines: the 60-year journey of hope and final success-lessons learned and future prospects. Trop Med Health. 2023 May 17;51(1):29. [CrossRef]
- Ferreira MU, da Silva Nunes M, Wunderlich G. Antigenic diversity and immune evasion by malaria parasites. Clin Diagn Lab Immunol. 2004 Nov;11(6):987-95. [CrossRef]
- Ferroni E, Jefferson T, Gachelin G. Angelo Celli and research on the prevention of malaria in Italy a century ago. J R Soc Med. 2012 Jan;105(1):35-40. [CrossRef]
- Fong Amaris WM, Suárez DR, Cortés-Cortés LJ, Martinez C. CAM: a novel aid system to analyse the coloration quality of thick blood smears using image processing and machine learning techniques. Malar J. 2024 Oct 7;23(1):299. [CrossRef]
- Fredj C Treating a Young Colony: Doctors in the French Army of Africa, Fevers and Quinine, 1830-1870 Le Movement Social 2016;4:257 . [CrossRef]
- Gachelin, G., Garner, P., Ferroni, E. et al. Evidence and strategies for malaria prevention and control: a historical analysis. Malar J 17, 96 (2018). [CrossRef]
- Gardner MJ, Hall N, Fung E, White O, Berriman M, Hyman RW, Carlton JM, Pain A, Nelson KE, Bowman S, Paulsen IT, James K, Eisen JA, Rutherford K, Salzberg SL, Craig A, Kyes S, Chan MS, Nene V, Shallom SJ, Suh B, Peterson J, Angiuoli S, Pertea M, Allen J, Selengut J, Haft D, Mather MW, Vaidya AB, Martin DM, Fairlamb AH, Fraunholz MJ, Roos DS, Ralph SA, McFadden GI, Cummings LM, Subramanian GM, Mungall C, Venter JC, Carucci DJ, Hoffman SL, Newbold C, Davis RW, Fraser CM, Barrell B. Genome sequence of the human malaria parasite Plasmodium falciparum. Nature. 2002 Oct 3;419(6906):498-511. [CrossRef]
- Garforth, V. The neem tree, a wonder tool against Malaria Environment, 2007 Federation of American Women’s Club overseas. Available online: https://www.fawco.org/global-issues/environment/environment-articles/289-the-neem-tree-a-wonder-tool-against-malaria.
- Getachew D, Balkew M, Tekie H. Anopheles larval species composition and characterization of breeding habitats in two localities in the Ghibe River Basin, southwestern Ethiopia. Malar J. 2020 Feb 11;19(1):65. [CrossRef]
- Ghansah A, Amenga-Etego L, Amambua-Ngwa A, et al.: Monitoring parasite diversity for malaria elimination in sub-Saharan Africa. Science. 2014; 345(6202): 1297–8.
- Ghansah A, Kamau E, Amambua-Ngwa A, Ishengoma DS, Maiga-Ascofare O, Amenga-Etego L, Deme A, Yavo W, Randrianarivelojosia M; Plasmodium Diversity Network Africa; Ochola-Oyier LI, Helegbe GK, Bailey J, Alifrangis M, Djimde A. Targeted Next Generation Sequencing for malaria research in Africa: current status and outlook. Malar J. 2019 Sep 23;18(1):324. [CrossRef]
- Gong L, Maiteki-Sebuguzi C, Rosenthal PJ, Hubbard AE, Drakeley CJ, Dorsey G, Greenhouse B. Evidence for both innate and acquired mechanisms of protection from Plasmodium falciparum in children with sickle cell trait. Blood. 2012 Apr 19;119(16):3808-14. [CrossRef]
- Goss A, “Building the world’s supply of quinine: Dutch colonialism and the origins of a global pharmaceutical industry”, Endeavour, 2014;38(1): 8–.
- Gozalo AS, Robinson CK, Holdridge J, Mahecha OFL, Elkins WR. Overview of Plasmodium spp. and Animal Models in Malaria Research. Comp Med. 2024 Aug 1;74(4):205-230. [CrossRef]
- Gross MR, Hsu R, Deitsch KW. Evolution of transcriptional control of antigenic variation and virulence in human and ape malaria parasites. BMC Ecol Evol. 2021 Jul 8;21(1):139. [CrossRef]
- Gunawardena S, Karunaweera ND. Advances in genetics and genomics: use and limitations in achieving malaria elimination goals. Pathog Glob Health. 2015 May;109(3):123-41. [CrossRef]
- Hafalla JCR, Borrmann S, Matuschewski K. Genetically attenuated parasites show promise as a next-generation malaria vaccine. Trends Parasitol. 2025 Feb;41(2):75-77. [CrossRef]
- Hempelmann E, Krafts K. Bad air, amulets and mosquitoes: 2,000 years of changing perspectives on malaria. Malar J. 2013 Jul 9;12:232. [CrossRef]
- Hershey CL, Florey LS, Ali D, Bennett A, Luhanga M, Mathanga DP, Salgado SR, Nielsen CF, Troell P, Jenda G, Yé Y, Bhattarai A. Malaria Control Interventions Contributed to Declines in Malaria Parasitemia, Severe Anemia, and All-Cause Mortality in Children Less Than 5 Years of Age in Malawi, 2000-2010. Am J Trop Med Hyg. 2017 Sep;97(3_Suppl):76-88. [CrossRef]
- Hoffman SL, Subramanian GM, Collins FH, Venter JC. Plasmodium, human and Anopheles genomics and malaria. Nature. 2002 Feb 7;415(6872):702-9. [CrossRef]
- Institute of Medicine (US) Committee for the Study on Malaria Prevention and Control; Oaks SC Jr., Mitchell VS, Pearson GW, et al., editors. Malaria: Obstacles and Opportunities. Washington (DC): National Academies Press (US); 1991. 3, Overview.
- Institute of Medicine (US) Committee on the Economics of Antimalarial Drugs; Arrow KJ, Panosian C, Gelband H, editors. Saving Lives, Buying Time: Economics of Malaria Drugs in an Age of Resistance. Washington (DC): National Academies Press (US); 2004. 5, A Brief History of Malaria. Available online: https://www.ncbi.nlm.nih.gov/books/NBK215638.
- Ishengoma DS, Saidi Q, Sibley CH, Roper C, Alifrangis M. Deployment and utilization of next-generation sequencing of Plasmodium falciparum to guide anti-malarial drug policy decisions in sub-Saharan Africa: opportunities and challenges. Malar J. 2019 Sep 3;18(1):267. [CrossRef]
- Kalkal M, Kalkal A, Dhanda SK, Das E, Pande V, Das J. A comprehensive study of epitopes and immune reactivity among Plasmodium species. BMC Microbiol. 2022 Mar 11;22(1):74. [CrossRef]
- Karemere J, Nana IG, Andrada A, Kakesa O, Mukomena Sompwe E, Likwela Losimba J, Emina J, Sadou A, Humes M, Yé Y. Associating the scale-up of insecticide-treated nets and use with the decline in all-cause child mortality in the Democratic Republic of Congo from 2005 to 2014. Malar J. 2021 May 29;20(1):241. [CrossRef]
- Kassegne K, Komi Koukoura K, Shen HM, Chen SB, Fu HT, Chen YQ, Zhou XN, Chen JH, Cheng Y. Genome-Wide Analysis of the Malaria Parasite Plasmodium falciparum Isolates From Togo Reveals Selective Signals in Immune Selection-Related Antigen Genes. Front Immunol. 2020 Oct 23;11:552698. [CrossRef]
- Kaura T, Sylvia Walter N, Kaur U, Sehgal R. Different Strategies for Mosquito Control: Challenges and Alternatives [Internet]. Mosquito Research - Recent Advances in Pathogen Interactions, Immunity, and Vector Control Strategies. IntechOpen; 2023. [CrossRef]
- Kayentao K, Florey LS, Mihigo J, Doumbia A, Diallo A, Koné D, Doumbo O, Eckert E. Impact evaluation of malaria control interventions on morbidity and all-cause child mortality in Mali, 2000-2012. Malar J. 2018 Nov 14;17(1):424. [CrossRef]
- Kibwana E, Kapulu M, Bejon P. Controlled Human Malaria Infection Studies in Africa-Past, Present, and Future. Curr Top Microbiol Immunol. 2024;445:337-365. [CrossRef]
- Killeen GF, Fillinger U, Kiche I, Gouagna LC, Knols BG. Eradication of Anopheles gambiae from Brazil: lessons for malaria control in Africa? Lancet Infect Dis. 2002 Oct;2(10):618-27. [CrossRef]
- Kokori E, Olatunji G, Akinboade A, Akinoso A, Egbunu E, Aremu SA, Okafor CE, Oluwole O, Aderinto N. Triple artemisinin-based combination therapy (TACT): advancing malaria control and eradication efforts. Malar J. 2024 Jan 18;23(1):25. [CrossRef]
- Krafts K, Hempelmann E, Oleksyn BJ. In search of the malarial parasite: biographical sketches of the blood stain contributors. Parasitol Res. 2011 Sep;109(3):521-9. [CrossRef]
- Lalchandama K. The making of modern malariology: from miasma to mosquito-malaria theory Science Vision 2014; 14(1):2-17.
- Laurens MB. RTS,S/AS01 vaccine (Mosquirix™): an overview. Hum Vaccin Immunother. 2020 Mar 3;16(3):480-489. Epub 2019 Oct 22. [CrossRef]
- Laveran CLA. 1978. A newly discovered parasite in the blood of patients suffering from malaria. Parasitic etiology of attacks of malaria. 1880. Translated from the French and reprinted in: Kean BH, editor; Mott KE, editor; Russell AJ, editor, eds. Tropical Medicine and Parasitology. Classic Investigations. Vol. 1. 1st ed. Ithaca, New York: Cornell University Press.
- Li J, Docile HJ, Fisher D, Pronyuk K, Zhao L. Current Status of Malaria Control and Elimination in Africa: Epidemiology, Diagnosis, Treatment, Progress and Challenges. J Epidemiol Glob Health. 2024 Sep;14(3):561-579. [CrossRef]
- Long B, MacDonald A, Liang SY, Brady WJ, Koyfman A, Gottlieb M, Chavez S. Malaria: A focused review for the emergency medicine clinician. Am J Emerg Med. 2024 Mar;77:7-16. [CrossRef]
- Maheu-Giroux M, Castro MC. Impact of community-based larviciding on the prevalence of malaria infection in Dar es Salaam, Tanzania. PLoS One. 2013 Aug 14;8(8):e71638. [CrossRef]
- Maiga FO, Wele M, Toure SM, Keita M, Tangara CO, Refeld RR, Thiero O, Kayentao K, Diakite M, Dara A, Li J, Toure M, Sagara I, Djimdé A, Mather FJ, Doumbia SO, Shaffer JG. Artemisinin-based combination therapy for uncomplicated Plasmodium falciparum malaria in Mali: a systematic review and meta-analysis. Malar J. 2021 Aug 30;20(1):356. [CrossRef]
- Malaria Genomic Epidemiology Network (MalariaGEN) Wellcome Open Research 2023, 8:22. [CrossRef]
- Malaria Genomic Epidemiology Network (MalariaGEN), Muzamil Mahdi Abdel Hamid, Mohamed Hassan Abdelraheem, Desmond Omane Acheampong, Ishag Adam, Pedro Aide, Olusola Ajibaye, Mozam Ali, Jacob Almagro-Garcia, Alfred Amambua-Ngwa, Lucas Amenga-Etego, Ifeyinwa Aniebo, Enoch Aninagyei, Felix Ansah, Tobias O Apinjoh, Cristina V Ariani, Sarah Auburn, Gordon A Awandare, et al Pf8: an open dataset of Plasmodium falciparum genome variation in 33,325 worldwide samples Wellcome Open Access Jun 2025, 10:325. [CrossRef]
- Malaria Genomic Epidemiology Network: A global network for investigating the genomic epidemiology of malaria. Nature. 2008; 456(7223): 732–7.
- Mamudu CO, Polidoro R, Gallego-Delgado J. Animal Models of Malaria-Associated Acute Kidney Injury. Semin Nephrol. 2025 May;45(3):151616. [CrossRef]
- Mannan BA, Patel K, Malhotra I, Ravindran B, Sharma S. How specific is the immune response to malaria in adults living in endemic areas? J Vector Borne Dis. 2003 Sep-Dec;40(3-4):84-91.
- Martín Ramírez A, Akindele AA, González Mora V, García L, Lara N, de la Torre-Capitán Matías E, Molina de la Fuente I, Nassar SA, Ta-Tang TH, Benito A, Berzosa P. Mutational profile of pfdhfr, pfdhps, pfmdr1, pfcrt and pfk13 genes of P. falciparum associated with resistance to different antimalarial drugs in Osun state, southwestern Nigeria. Trop Med Health. 2025 Apr 8;53(1):49. [CrossRef]
- Mattah PA, Futagbi G, Amekudzi LK, Mattah MM, de Souza DK, Kartey-Attipoe WD, Bimi L, Wilson MD. Diversity in breeding sites and distribution of Anopheles mosquitoes in selected urban areas of southern Ghana. Parasit Vectors. 2017 Jan 13;10(1):25. [CrossRef]
- Maturana CR, de Oliveira AD, Nadal S, Serrat FZ, Sulleiro E, Ruiz E, Bilalli B, Veiga A, Espasa M, Abelló A, Suñé TP, Segú M, López-Codina D, Clols ES, Joseph-Munné J. iMAGING: a novel automated system for malaria diagnosis by using artificial intelligence tools and a universal low-cost robotized microscope. Front Microbiol. 2023 Nov 24;14:1240936. [CrossRef]
- Merga, H., Degefa, T., Birhanu, Z. et al. Urban malaria in sub-Saharan Africa: a scoping review of epidemiologic studies. Malar J 24, 131 (2025). [CrossRef]
- Metoh TN, Chen JH, Fon-Gah P, Zhou X, Moyou-Somo R, Zhou XN. Genetic diversity of Plasmodium falciparum and genetic profile in children affected by uncomplicated malaria in Cameroon. Malar J. 2020 Mar 18;19(1):115. [CrossRef]
- Mihreteab S, Anderson K, Fuente IM, Sutherland CJ, Smith D, Cunningham J, Beshir KB, Cheng Q. The spread of molecular markers of artemisinin partial resistance and diagnostic evasion in Eritrea: a retrospective molecular epidemiology study. Lancet Microbe. 2025 Feb;6(2):100930. [CrossRef]
- Mihreteab S, Platon L, Berhane A, Stokes BH, Warsame M, Campagne P, Criscuolo A, Ma L, Petiot N, Doderer-Lang C, Legrand E, Ward KE, Zehaie Kassahun A, Ringwald P, Fidock DA, Ménard D. Increasing Prevalence of Artemisinin-Resistant HRP2-Negative Malaria in Eritrea. N Engl J Med. 2023 Sep 28;389(13):1191-1202. [CrossRef]
- Milong Melong CS, Peloewetse E, Russo G, Tamgue O, Tchoumbougnang F, Paganotti GM. An overview of artemisinin-resistant malaria and associated Pfk13 gene mutations in Central Africa. Parasitol Res. 2024 Jul 18;123(7):277. Erratum in: Parasitol Res. 2024 Aug 23;123(8):309. doi: 10.1007/s00436-024-08315-w. [CrossRef]
- MMV: Medicine for malaria venture History of antimalarial drugs. 2025. Available online: https://www.mmv.org/.
- Mobegi VA, Duffy CW, Amambua-Ngwa A, Loua KM, Laman E, Nwakanma DC, MacInnis B, Aspeling-Jones H, Murray L, Clark TG, Kwiatkowski DP, Conway DJ. Genome-wide analysis of selection on the malaria parasite Plasmodium falciparum in West African populations of differing infection endemicity. Mol Biol Evol. 2014 Jun;31(6):1490-9. [CrossRef]
- Molineaux L., Gramiccia G The Garki Project: Research on the Epidemiology and Control of Malaria in the Sudan Savanna of West Africa. World Health Organization 1980, ISBN 92 4 156061 4.
- Moormann AM, Embury PE, Opondo J, Sumba OP, Ouma JH, Kazura JW, John CC. Frequencies of sickle cell trait and glucose-6-phosphate dehydrogenase deficiency differ in highland and nearby lowland malaria-endemic areas of Kenya. Trans R Soc Trop Med Hyg. 2003 Sep-Oct;97(5):513-4. [CrossRef]
- Morua E, Cuyas L, Matías-Hernández L. The Beneficial Use of Artemisia annua, Artemisinin, and Other Compounds in Animal Health. Animals (Basel). 2025 May 8;15(10):1359. [CrossRef]
- Msellemu D, Namango HI, Mwakalinga VM, Ntamatungiro AJ, Mlacha Y, Mtema ZJ, Kiware S, Lobo NF, Majambere S, Dongus S, Drakeley CJ, Govella NJ, Chaki PP, Killeen GF. The epidemiology of residual Plasmodium falciparum malaria transmission and infection burden in an African city with high coverage of multiple vector control measures. Malar J. 2016 May 23;15(1):288. [CrossRef]
- Msugupakulya BJ, Urio NH, Jumanne M, Ngowo HS, Selvaraj P, Okumu FO, Wilson AL. Changes in contributions of different Anopheles vector species to malaria transmission in east and southern Africa from 2000 to 2022. Parasit Vectors. 2023 Nov 7;16(1):408. [CrossRef]
- Msugupakulya BJ, Urio NH, Jumanne M, Ngowo HS, Selvaraj P, Okumu FO, Wilson AL. Changes in contributions of different Anopheles vector species to malaria transmission in east and southern Africa from 2000 to 2022. Parasit Vectors. 2023 Nov 7;16(1):408. [CrossRef]
- Muzaki S. Africa launches historic malaria vaccine rollout amid funding uncertainty. Nature Africa, 2025. [CrossRef]
- Namuganga JF, Nankabirwa JI, Maiteki-Ssebuguzi C, Gonahasa S, Opigo J, Staedke SG, Rutazaana D, Ebong C, Dorsey G, Tomko SS, Kizza T, Mawejje HD, Arinaitwe E, Rosenthal PJ, Kamya MR. East Africa International Center of Excellence for Malaria Research: Impact on Malaria Policy in Uganda. Am J Trop Med Hyg. 2022 Oct 11;107(4_Suppl):33-39. [CrossRef]
- Nankabirwa JI, Rek J, Arinaitwe E, Namuganga JF, Nsobya SL, Asua V, Mawejje HD, Epstein A, Greenhouse B, Rodriguez-Barraquer I, Briggs J, Krezanoski PJ, Rosenthal PJ, Conrad M, Smith D, Staedke SG, Drakeley C, Bousema T, Andolina C, Donnelly MJ, Kamya MR, Dorsey G. East Africa International Center of Excellence for Malaria Research: Summary of Key Research Findings. Am J Trop Med Hyg. 2022 Oct 11;107(4_Suppl):21-32. [CrossRef]
- Nedelman, J. The prevalence of malaria in Garki, Nigeria: double sampling with a fallible expert. Biometrics. 1988 Sep;44(3):635-55.
- Nkrumah B, Acquah SE, Ibrahim L, May J, Brattig N, Tannich E, Nguah SB, Adu-Sarkodie Y, Huenger F. Comparative evaluation of two rapid field tests for malaria diagnosis: Partec Rapid Malaria Test® and Binax Now® Malaria Rapid Diagnostic Test. BMC Infect Dis. 2011 May 23;11:143. [CrossRef]
- Nkumama IN, O’Meara WP, Osier FHA. Changes in Malaria Epidemiology in Africa and New Challenges for Elimination. Trends Parasitol. 2017 Feb;33(2):128-140. [CrossRef]
- Nosten F, White NJ. Artemisinin-Based Combination Treatment of Falciparum Malaria. In: Breman JG, Alilio MS, White NJ, editors. Defining and Defeating the Intolerable Burden of Malaria III: Progress and Perspectives: Supplement to Volume 77(6) of American Journal of Tropical Medicine and Hygiene. Northbrook (IL): American Society of Tropical Medicine and Hygiene; 2007 Dec. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1713/.
- Obeagu EI, Obeagu GU. Emerging public health strategies in malaria control: innovations and implications. Ann Med Surg (Lond). 2024 Sep 20;86(11):6576-6584. [CrossRef]
- Obembe A, Oduola AO, Adeogun A, Inyang U, Oyeniyi T, Olakiigbe A, Babalola A, Inyama P, Lazarus S, Okeke I, Esema M, Okoko OO, Omo-Eboh M, Uhomoibhi P, Bala M, Awolola S. Implementation of malaria vector surveillance and insecticide resistance monitoring interventions in Nigeria. Glob Health Res Policy. 2024 Dec 31;9(1):55. [CrossRef]
- Odhiambo EO, Mellencamp KA, Ondigo BN, Hamre KES, Beeson JG, Opi DH, Narum DL, Ayodo G, John CC. Antibody correlates of risk of clinical malaria in an area of low and unstable malaria transmission in western Kenya. Malar J. 2025 Mar 4;24(1):73. [CrossRef]
- Oduoye MO, Haider MU, Marsool MDM, Kareem MO, Adedayo AE, Abdulkarim AS, Adegoke AA, Kaushik I, Irfan H, Yusuf HA, Shah HH, Karim KA. Unlocking the potential of novel RTS, S/AS01, and R21/Matrix-M™ malaria vaccines in African nations. Health Sci Rep. 2024 Jan 4;7(1):e1797. [CrossRef]
- Ogwang R, Adan M, Bejon P, Kapulu MC. Controlled human malaria infection studies: insights into recent advances and key immunological and ethical implementation lessons. Front Immunol. 2025 Sep 18;16:1672945. [CrossRef]
- Onaolapo AY Onaolapo OJ, Adeyeba AO Malaria, Antimalaria Drugs, Drug/Parasite Interactions, and the Brain: A Review of Impacts on Behaviour, Neurochemistry and Structure. Cent Nerv Syst Agents Med Chem. 2018;18(3):173-192. [CrossRef]
- Onukansi FO, Anokwuru CC, Eneh SC, Odey GO, Onah DO, Sokunbi T, Innocent DC, Dozie UW, Umoke PC, Ojo TO, Ezejindu CN. Investing in traditional medicine: leveraging evidence and innovative research to strengthen the fight against malaria in Nigeria. Malar J. 2025 Jul 15;24(1):232. [CrossRef]
- Opi, D. H., Kurtovic, L., Chan, J. A., Horton, J. L., Feng, G., Beeson, J. G. Multi-functional antibody profiling for malaria vaccine development and evaluation. Expert Review of Vaccines, 2021; 20(10), 1257–1272. [CrossRef]
- Osunderu, O.A. (2009). Sustainable Production of Traditional Medicines in Africa. In: Yanful, E.K. (eds) Appropriate Technologies for Environmental Protection in the Developing World. Springer, Dordrecht. [CrossRef]
- Ounjaijean S, Somsak V. Evaluating the Antiplasmodial Activity of Picrasma javanica Stem Bark Extract and Its Synergy With Artesunate in Rodent Malaria Models. Scientifica (Cairo). 2025 Jun 4;2025:7344444. [CrossRef]
- Oyegbade SA, Mameh EO, Balogun DO, Aririguzoh VO, Akinduti PA. Emerging Plasmodium falciparum K13 gene mutation to artemisinin-based combination therapies and partner drugs among malaria-infected population in sub-Saharan Africa. Parasites Hosts Dis. 2025 May;63(2):109-122. [CrossRef]
- Pande V, Bahal M, Dua J, Gupta A. Ronald Ross: Pioneer of Malaria Research and Nobel Laureate. Cureus. 2024 Aug 2;16(8):e65993. [CrossRef]
- Pandey SK, Anand U, Siddiqui WA, Tripathi R. Drug Development Strategies for Malaria: With the Hope for New Antimalarial Drug Discovery-An Update. Adv Med. 2023 Mar 14;2023:5060665. [CrossRef]
- Permin H, Norn S, Kruse E, Kruse PR. On the history of Cinchona bark in the treatment of Malaria. Dan Medicinhist Arbog. 2016;44:9-30.
- Pikor D, Hurla M, Drelichowska A, Paul M. Evolutionary Trajectory of Plasmodium falciparum: From Autonomous Phototroph to Dedicated Parasite. Biomedicines. 2025; 13(9):2287. [CrossRef]
- Pinkevych M, Petravic J, Chelimo K, Kazura JW, Moormann AM, Davenport MP. The dynamics of naturally acquired immunity to Plasmodium falciparum infection. PLoS Comput Biol. 2012;8(10):e1002729. [CrossRef]
- Praet N, Asante KP, Bozonnat MC, Akité EJ, Ansah PO, Baril L, Boahen O, Mendoza YG, Haine V, Kariuki S, Lamy M, Maleta K, Mungwira R, Ndeketa L, Oduro A, Ogutu B, Olewe F, Oneko M, Orsini M, Roman F, Bahmanyar ER, Rosillon D, Schuerman L, Sing’oei V, Terlouw DJ, Wéry S, Otieno W, Pirçon JY. Assessing the safety, impact and effectiveness of RTS,S/AS01E malaria vaccine following its introduction in three sub-Saharan African countries: methodological approaches and study set-up. Malar J. 2022 Apr 25;21(1):132. [CrossRef]
- Prah JK, Amoah S, Yartey AN, Ampofo-Asiama A, Ameyaw EO. Assessment of malaria diagnostic methods and treatments at a Ghanaian health facility. Pan Afr Med J. 2021 Aug 19;39:251. [CrossRef]
- Pryce J, Medley N, Choi L. Indoor residual spraying for preventing malaria in communities using insecticide-treated nets. Cochrane Database Syst Rev. 2022 Jan 17;1(1):CD012688. [CrossRef]
- Raele DA, Severini F, Toma L, Menegon M, Boccolini D, Tortorella G, Di Luca M, Cafiero MA. Anopheles sacharovi in Italy: first record of the historical malaria vector after over 50 years. Parasit Vectors. 2024 Apr 10;17(1):182. [CrossRef]
- Raghavendra K, Barik TK, Reddy BP, Sharma P, Dash AP. Malaria vector control: from past to future. Parasitol Res. 2011 Apr;108(4):757-79. [CrossRef]
- Rajakumar K, Weisse M. Centennial year of Ronald Ross’ epic discovery of malaria transmission: an essay and tribute. South Med J. 1999 Jun;92(6):567-71. [CrossRef]
- Ratschiller Nasim, L.M. (2023). Shaping Colonial Science: Missionary Challenges, Racial Segregation and the Locality of Science. In: Medical Missionaries and Colonial Knowledge in West Africa and Europe, 1885-1914. Cambridge Imperial and Post-Colonial Studies. Palgrave Macmillan, Cham. [CrossRef]
- Rubio Maturana C, de Oliveira AD, Zarzuela F, Mediavilla A, Martínez-Vallejo P, Silgado A, Goterris L, Muixí M, Abelló A, Veiga A, López-Codina D, Sulleiro E, Sayrol E, Joseph-Munné J. Evaluation of an Artificial Intelligence-Based Tool and a Universal Low-Cost Robotized Microscope for the Automated Diagnosis of Malaria. Int J Environ Res Public Health. 2024 Dec 31;22(1):47. [CrossRef]
- Sato, S. Plasmodium-a brief introduction to the parasites causing human malaria and their basic biology. J Physiol Anthropol. 2021 Jan 7;40(1):1. Erratum in: J Physiol Anthropol. 2021 Jan 29;40(1):3. 10.1186/s40101-021-00254-0. [CrossRef]
- Schmit N, Topazian HM, Natama HM, Bellamy D, Traoré O, Somé MA, Rouamba T, Tahita MC, Bonko MDA, Sourabié A, Sorgho H, Stockdale L, Provstgaard-Morys S, Aboagye J, Woods D, Rapi K, Datoo MS, Lopez FR, Charles GD, McCain K, Ouedraogo JB, Hamaluba M, Olotu A, Dicko A, Tinto H, Hill AVS, Ewer KJ, Ghani AC, Winskill P. The public health impact and cost-effectiveness of the R21/Matrix-M malaria vaccine: a mathematical modelling study. Lancet Infect Dis. 2024 May;24(5):465-475. [CrossRef]
- Shaw WR, Marcenac P, Catteruccia F. Plasmodium development in Anopheles: a tale of shared resources. Trends Parasitol. 2022 Feb;38(2):124-135. [CrossRef]
- Shelton JM, Corran P, Risley P, Silva N, Hubbart C, Jeffreys A, Rowlands K, Craik R, Cornelius V, Hensmann M, Molloy S, Sepulveda N, Clark TG, Band G, Clarke GM, Spencer CC, Kerasidou A, Campino S, Auburn S, Tall A, Ly AB, Mercereau-Puijalon O, Sakuntabhai A, Djimdé A, Maiga B, Touré O, Doumbo OK, Dolo A, Troye-Blomberg M, Mangano VD, Verra F, Modiano D, Bougouma E, Sirima SB, Ibrahim M, Hussain A, Eid N, Elzein A, Mohammed H, Elhassan A, Elhassan I, Williams TN, Ndila C, Macharia A, Marsh K, Manjurano A, Reyburn H, Lemnge M, Ishengoma D, Carter R, Karunaweera N, Fernando D, Dewasurendra R, Drakeley CJ, Riley EM, Kwiatkowski DP, Rockett KA; MalariaGEN Consortium. Genetic determinants of anti-malarial acquired immunity in a large multi-centre study. Malar J. 2015.
- Siao MC, Borner J, Perkins SL, Deitsch KW, Kirkman LA. Evolution of Host Specificity by Malaria Parasites through Altered Mechanisms Controlling Genome Maintenance. mBio. 2020 Mar 17;11(2):e03272-19. [CrossRef]
- Sibomana O, Bukuru J, Saka SA, Uwizeyimana MG, Kihunyu AM, Obianke A, Damilare SO, Bueh LT, Agbelemoge BOG, Oveh RO. Routine malaria vaccination in Africa: a step toward malaria eradication? Malar J. 2025 Jan 5;24(1):1. [CrossRef]
- Silva M, Malmberg M, Otienoburu SD, Björkman A, Ngasala B, Mårtensson A, Gil JP, Veiga MI. Plasmodium falciparum Drug Resistance Genes pfmdr1 and pfcrt In Vivo Co-Expression During Artemether-Lumefantrine Therapy. Front Pharmacol. 2022 May 24;13:868723. [CrossRef]
- Sinden RE. Malaria, mosquitoes and the legacy of Ronald Ross. Bull World Health Organ. 2007 Nov;85(11):894-6. [CrossRef]
- Su XZ, Lane KD, Xia L, Sá JM, Wellems TE. Plasmodium Genomics and Genetics: New Insights into Malaria Pathogenesis, Drug Resistance, Epidemiology, and Evolution. Clin Microbiol Rev. 2019 Jul 31;32(4):e00019-19. [CrossRef]
- Su XZ, Miller LH. The discovery of artemisinin and the Nobel Prize in Physiology or Medicine. Sci China Life Sci. 2015 Nov;58(11):1175-9. [CrossRef]
- Sypniewska P, Duda JF, Locatelli I, Althaus CR, Althaus F, Genton B. Clinical and laboratory predictors of death in African children with features of severe malaria: a systematic review and meta-analysis. BMC Med. 2017;15:147. 10.1186/s12916-017-0906-5.
- Tachibana M, Takashima E, Torii M, Wu Y, Sattabongkot J, Tsuboi T (Advances in transmission-blocking vaccines against Plasmodium falciparum and Plasmodium vivax, Expert Review of Vaccines, 2025. [CrossRef]
- Takken W, Charlwood D, Lindsay SW. The behaviour of adult Anopheles gambiae, sub-Saharan Africa’s principal malaria vector, and its relevance to malaria control: a review. Malar J. 2024 May 23;23(1):161. [CrossRef]
- Talapko J, Škrlec I, Alebić T, Jukić M, Včev A. Malaria: The Past and the Present. Microorganisms. 2019 Jun 21;7(6):179. [CrossRef]
- Talisuna AO, Noor AM, Okui AP, Snow RW. The past, present and future use of epidemiological intelligence to plan malaria vector control and parasite prevention in Uganda. Malar J. 2015 Apr 15;14:158. [CrossRef]
- Tan S.Y., Ahana A. Charles Laveran (1845–1922), Nobel laureate pioneer of malaria. Singap. Med. J. 2009;50:657–658.
- Tegegn G, Gnanasekaren N, Gadisa E, Getie M, Molla A, Meharie T, Debash H, Berhan A, Almaw A, Hussien A, Abeje G. Comparative assessment of microscopy, malaria rapid diagnostic test and polymerase chain reaction as malaria diagnostic tools in Adama Woreda, East shoa zone of Ethiopia: a cross-sectional study. BMC Infect Dis. 2024 Nov 28;24(1):1363. [CrossRef]
- Tessema SK, Raman J, Duffy CW, Ishengoma DS, Amambua-Ngwa A, Greenhouse B. Applying next-generation sequencing to track falciparum malaria in sub-Saharan Africa. Malar J. 2019 Sep 3;18(1):268. [CrossRef]
- Thwing J, Eckert E, Dione DA, Tine R, Faye A, Yé Y, Ndiop M, Cisse M, Ndione JA, Diouf MB, Ba M. Declines in Malaria Burden and All-Cause Child Mortality following Increases in Control Interventions in Senegal, 2005-2010. Am J Trop Med Hyg. 2017 Sep;97(3_Suppl):89-98. [CrossRef]
- Tse, E.G., Korsik, M. & Todd, M.H. The past, present and future of anti-malarial medicines. Malar J 18, 93 (2019). [CrossRef]
- Ugah UI, Alo MN, Owolabi JO, Okata-Nwali OD, Ekejindu IM, Ibeh N, Elom MO. Evaluation of the utility value of three diagnostic methods in the detection of malaria parasites in endemic area. Malar J. 2017 May 6;16(1):189. [CrossRef]
- US Institute of Medicine (IOM) from the report, Saving Lives, Buying Time: Economics of Malaria Drugs in an Age of Resistance, 2004, pp. 126-128.
- van den Berg H, van Vugt M, Kabaghe AN, Nkalapa M, Kaotcha R, Truwah Z, Malenga T, Kadama A, Banda S, Tizifa T, Gowelo S, Mburu MM, Phiri KS, Takken W, McCann RS. Community-based malaria control in southern Malawi: a description of experimental interventions of community workshops, house improvement and larval source management. Malar J. 2018 Jul 16;17(1):266. [CrossRef]
- van den Berg H. Global status of DDT and its alternatives for use in vector control to prevent disease. Environ Health Perspect. 2009 Nov;117(11):1656-63. [CrossRef]
- Veiga MI, Ferreira PE, Björkman A, Gil JP. Multiplex PCR-RFLP methods for pfcrt, pfmdr1 and pfdhfr mutations in Plasmodium falciparum. Mol Cell Probes. 2006 Apr;20(2):100-4. [CrossRef]
- Venkatraman N, Tiono AB, Bowyer G, Bellamy DG, Stockdale LK, Powlson J, Collins KA, Coulibaly S, Datoo MS, Silman D, Ouedraogo A, Nébié I, Imoukhuede EB, Brod F, Folegatti P, Dickinson-Craig E, Jamieson S, Bougouma EC, Wright D, Diarra A, Bliss CM, Morter R, Glenn G, Fries LF, Reimer JM, Lövgren-Bengtsson K, Baker M, Poulton I, Moyle S, Berrie E, Green N, Mukhopadhyay E, Viebig NK, Angus B, Lawrie A, Roberts R, Gilbert SC, Lewis DJM, Sirima SB, Ewer KJ, Hill AVS. Evaluation of a novel malaria anti-sporozoite vaccine candidate, R21 in Matrix-M adjuvant, in the UK and Burkina Faso: two phase 1, first-in-human trials. Lancet Microbe. 2025 Mar;6(3):100868. [CrossRef]
- Vestergaard LS, Ringwald P. Responding to the Challenge of Antimalarial Drug Resistance by Routine Monitoring to Update National Malaria Treatment Policies. In: Breman JG, Alilio MS, White NJ, editors. Defining and Defeating the Intolerable Burden of Malaria III: Progress and Perspectives: Supplement to Volume 77(6) of American Journal of Tropical Medicine and Hygiene. Northbrook (IL): American Society of Tropical Medicine and Hygiene; 2007 Dec. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1708/.
- von Seidlein L, Duraisingh MT, Drakeley CJ, Bailey R, Greenwood BM, Pinder M. Polymorphism of the Pfmdr1 gene and chloroquine resistance in Plasmodium falciparum in The Gambia. Trans R Soc Trop Med Hyg. 1997 Jul-Aug;91(4):450-3. [CrossRef]
- Wang X, Zhang X, Chen H, Zhang J, Lu Q, Ruan W, Ling F. Molecular Epidemiology of Drug Resistance Genes in Plasmodium falciparum Isolates Imported from Nigeria between 2016 and 2020: Continued Emergence of Fully Resistant Pfdhfr-Pfdhps Alleles. Microbiol Spectr. 2022 Oct 26;10(5):e0052822. [CrossRef]
- WHO: World Health Organisation Malaria vaccines (RTS,S and R21) 2025. Available online: https://www.who.int/news-room/questions-and-answers/item/q-a-on-rts-s-malaria-vaccine#.
- WHO: World Health Organisation recommends groundbreaking malaria vaccine for children at risk, 2021. Available online: https://www.who.int/news/item/06-10-2021-who-recommends-groundbreaking-malaria-vaccine-for-children-at-risk.
- Wilson AL, Courtenay O, Kelly-Hope LA, Scott TW, Takken W, Torr SJ, Lindsay SW. The importance of vector control for the control and elimination of vector-borne diseases. PLoS Negl Trop Dis. 2020 Jan 16;14(1):e0007831. [CrossRef]
- Win Han Oo, Gold L, Moore K, Agius PA, Fowkes FJI. The impact of community-delivered models of malaria control and elimination: a systematic review. Malar J. 2019 Aug 6;18(1):269. [CrossRef]
- Woehlbier U, Epp C, Hackett F, Blackman MJ, Bujard H. Antibodies against multiple merozoite surface antigens of the human malaria parasite Plasmodium falciparum inhibit parasite maturation and red blood cell invasion. Malar J. 2010 Mar 18;9:77. [CrossRef]
- Wongsrichanalai C, Barcus MJ, Muth S, et al. A Review of Malaria Diagnostic Tools: Microscopy and Rapid Diagnostic Test (RDT) In: Breman JG, Alilio MS, White NJ, editors. Defining and Defeating the Intolerable Burden of Malaria III: Progress and Perspectives: Supplement to Volume 77(6) of American Journal of Tropical Medicine and Hygiene. Northbrook (IL): American Society of Tropical Medicine and Hygiene; 2007 Dec. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1695/.
- World Health Organization. World malaria report 2023. WHO; 2023. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2023.
- Wurtz N, Fall B, Pascual A, Diawara S, Sow K, Baret E, Diatta B, Fall KB, Mbaye PS, Fall F, Diémé Y, Rogier C, Bercion R, Briolant S, Wade B, Pradines B. Prevalence of molecular markers of Plasmodium falciparum drug resistance in Dakar, Senegal. Malar J. 2012 Jun 13;11:197. [CrossRef]
- Zekar L, Sharman T. Plasmodium falciparum Malaria. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555962/.
- Zhao D, Zhang H, Ji P, Li S, Yang C, Liu Y, Qian D, Deng Y, Wang H, Lu D, Zhou R, Zhao Y. Surveillance of Antimalarial Drug-Resistance Genes in Imported Plasmodium falciparum Isolates From Nigeria in Henan, China, 2012-2019. Front Cell Infect Microbiol. 2021 Apr 23;11:644576.
- Zheng D, Liu T, Yu S, Liu Z, Wang J, Wang Y. Antimalarial Mechanisms and Resistance Status of Artemisinin and Its Derivatives. Trop Med Infect Dis. 2024 Sep 20;9(9):223. [CrossRef]
- Zhou R, Yang C, Li S, Zhao Y, Liu Y, Qian D, Wang H, Lu D, Zhang H, Huang F. Molecular Surveillance of Drug Resistance of Plasmodium falciparum Isolates Imported from Angola in Henan Province, China. Antimicrob Agents Chemother. 2019 Sep 23;63(10):e00552-19. [CrossRef]
- Zhou W, Wang H, Yang Y, Chen ZS, Zou C, Zhang J. Chloroquine against malaria, cancers and viral diseases. Drug Discov Today. 2020 Sep 16;25(11):2012–22.

Table 1.
Timeline of Malaria Research Milestones in Africa (1880–2025).
| Year / Period | Milestone / Event | Significance (with African Focus) |
|---|---|---|
| 1880 | Charles Louis Alphonse Laveran observes Plasmodium parasites in Algeria. | Marks the first identification of a protozoan parasite in humans; discovery occurred on African soil. |
| 1897 | Sir Ronald Ross demonstrates mosquito transmission of malaria. | Foundation for vector control strategies later applied extensively in Africa. |
| 1898–1900 | Giovanni Battista Grassi confirms mosquito transmission of P. falciparum in humans. | Clarifies parasite life cycle, directly relevant to African Anopheles species. |
| 1900–1950 | Expansion of malaria research and control under colonial health systems. | Establishment of early laboratories in Nigeria, Ghana, Sudan, and Kenya; focus on vector ecology and habitat management. |
| 1940s | Introduction of chloroquine and DDT. | Synthetic antimalarials and insecticides revolutionise malaria treatment and control across tropical Africa. |
| 1955 | WHO launches the Global Malaria Eradication Programme (GMEP). | Africa largely excluded due to logistical, ecological, and infrastructural challenges. |
| 1950s–1960s | Creation of regional research institutes. | Establishment of tropical medicine centres (e.g., East African Institute of Malaria, Nigeria’s Trypanosomiasis Institute). |
| 1969–1976 | The Garki Project (Nigeria). | WHO–Nigeria collaboration providing realistic mathematical models of malaria transmission; exposed limits of vector spraying and mass drug administration in African settings. |
| 1970s–1980s | Widespread chloroquine resistance. | Resistance of P. falciparum spreads across Africa; drives the search for new drug therapies. |
| 1980s | Strengthening of African research institutions. | Growth of KEMRI (Kenya), Noguchi Memorial Institute (Ghana), and Ifakara Health Institute (Tanzania). |
| 2002 | Plasmodium falciparum genome sequenced. | Major genomic breakthrough; African samples and scientists contributed to understanding drug resistance genes. |
| 2005 | Roll Back Malaria & President’s Malaria Initiative (PMI) expanded. | Renewed global and African focus on malaria funding, control, and elimination strategies. |
| 2010 | Scale-up of insecticide-treated nets (ITNs). | Significant reduction in malaria morbidity and mortality across sub-Saharan Africa, especially among children. |
| 2015 | African Union’s “Catalytic Framework to End AIDS, TB, and Eliminate Malaria by 2030.” | Integration of malaria control within Africa’s broader health and development agenda. |
| 2018 | RTS,S/AS01 (Mosquirix) pilot vaccine rollout in Ghana, Kenya, and Malawi. | First large-scale real-world vaccine trials conducted in Africa; pivotal step toward immunological control. |
| 2020 | WHO recognises Africa as the global epicentre of malaria research and challenge. | Over 90% of global malaria cases and deaths occur in Africa, making it central to global policy and innovation. |
| 2021 | WHO recommends RTS,S for widespread use. | Historic milestone in malaria vaccination; evidence driven by African trial data. |
| 2022 | Reports of pfkelch13 mutations in East Africa. | Confirms partial artemisinin resistance in P. falciparum strains from Rwanda and Uganda. |
| 2023 | R21/Matrix-M vaccine approved and endorsed by WHO. | Developed with major African participation (notably Burkina Faso); efficacy surpasses 75%. |
| 2024–2025 | Expansion of genomic surveillance networks (PDNA, MalariaGEN Africa Hub). | African-led genomic initiatives enable cross-border tracking of parasite evolution, drug resistance, and vector genomics. |
From Laveran’s 1880 discovery in Algeria to Africa’s leadership in malaria genomics and vaccine development by 2025, this timeline illustrates the continent’s transformation from a site of colonial experimentation to a global driver of innovation, policy, and molecular research in the fight against malaria.
Table 2.
Timeline of Malaria Chemotherapy in Africa (1880–2025).
| Period / Year | Therapeutic Milestone | Significance in the African Context |
|---|---|---|
| Pre-1880s | Traditional African Antimalarial Remedies | Indigenous use of plants such as Cryptolepis sanguinolenta, Azadirachta indica (neem), Morinda lucida, and Vernonia amygdalina for treating fever and malaria-like symptoms; foundation for later pharmacognostic studies. |
| 17th–19th Century | Introduction of Quinine from Cinchona bark | Used by colonial powers and missionaries in Africa; first effective therapy against malaria; limited access for native populations during colonial expansion. |
| 1880–1930s | Refinement of Quinine Therapy | Quinine becomes standard treatment across Africa; issues of cost, supply, and resistance begin to emerge. |
| 1940s | Synthesis of Chloroquine (CQ) | Affordable, potent antimalarial; rapidly adopted across Africa as a first-line therapy; marked a new era in mass treatment. |
| 1950s–1970s | Golden Age of Antimalarial Chemotherapy | Introduction of amodiaquine, pyrimethamine and sulfadoxine-pyrimethamine (SP); widespread prophylaxis and treatment programmes implemented during and after colonial rule. |
| 1960s–1970s | Mass Drug Administration Trials (e.g., Garki Project, Nigeria) | Evaluated large-scale CQ and SP distribution; revealed challenges of sustainability and resistance in high-transmission African settings. |
| 1980s | Emergence of Chloroquine Resistance in Africa | Chloroquine resistance spreads from Southeast Asia to Africa; genetic basis later linked to pfcrt and pfmdr1 mutations; marks beginning of drug- resistance era. |
| 1990s | Transition to Sulfadoxine-Pyrimethamine (SP) and Other Alternatives | SP temporarily replaces CQ; resistance soon follows; combination therapies explored to delay resistance. |
| 2000s | Adoption of Artemisinin-Based Combination Therapies (ACTs) | ACTs became WHO-recommended first-line treatment; Africa leads global implementation through national malaria control programmes; major decline in mortality observed. |
| 2010s | Widespread Distribution and Policy Integration of ACTs | Rollout supported by Roll Back Malaria, Global Fund, and PMI; local studies validate safety and efficacy; artemisinin resistance monitoring begins in East Africa. |
| 2012–2020 | Integration of Pharmacovigilance and Molecular Surveillance | African researchers identify key resistance markers (pfkelch13 mutations); routine genotyping incorporated into surveillance systems. |
| 2021–2023 | Emergence of Artemisinin Partial Resistance in East Africa | Reports from Rwanda, Uganda, and Eritrea confirm reduced susceptibility; renewed emphasis on surveillance and combination therapy refinement. |
| 2023–2025 | Renewed Focus on Traditional and Nutraceutical Antimalarials | Growing research on African botanicals (e.g., Spondias mombin, Cryptolepis sanguinolenta) and their molecular targets; integration of ethnomedicine with modern pharmacology. |
| 2025 and beyond | Toward Personalised and Genomic-Guided Malaria Therapy | Africa’s genomic networks (e.g., PDNA, MalariaGEN Africa Hub) enable tracking of resistance alleles and design of tailored treatment policies; exploration of host-genetic factors guiding therapy and vaccine response. |
From quinine’s introduction to the continent-wide deployment of ACTs and genomic surveillance, Africa’s therapeutic landscape reflects both the burden and brilliance of adaptation. Each stage of antimalarial therapy has been shaped by Africa’s unique ecology, parasite evolution, and growing research independence. Today, with African scientists leading genomic, pharmacological, and ethnomedicinal investigations, the continent stands poised to redefine the next generation of precision antimalarial therapies.
Table 3.
Key African Malaria Vaccine Trials and Their Outcomes.
| Vaccine Candidate | Target Antigen / Platform | Trial Locations (Africa) | Trial Phase / Period | Efficacy / Key Findings | Lead Institutions / Partners |
|---|---|---|---|---|---|
| RTS, S/AS01 (Mosquirix™) | Circumsporozoite protein (Plasmodium falciparum) + Hepatitis B surface antigen; AS01 adjuvant | Ghana, Kenya, Malawi, Mozambique, Tanzania, Gabon | Phase III (2009–2014); Pilot Implementation (2019–2023) | ~30–50% efficacy against clinical malaria in children (5–17 months); protection wanes over time; reduced severe malaria | GSK, PATH, WHO, African research consortia |
| R21/Matrix-M | Circumsporozoite protein (modified RTS,S antigen) with Matrix-M adjuvant | Burkina Faso, Mali, Ghana | Phase IIb (2019–2021); Phase III (2021–2024 ongoing) | Up to 75% efficacy over 12 months; high antibody titrers; favourable safety profile | University of Oxford, Serum Institute of India, African clinical trial partners |
| SPf66 | Synthetic multi-epitope peptide | The Gambia, Tanzania | Phase II (1990s) | Low and inconsistent efficacy (<30%); abandoned | Colombian and African collaborators |
| DELVAC/AMA1-C1 | Apical Membrane Antigen-1 (AMA1) recombinant protein | Mali | Phase I–II (2005–2010) | Safe; induced strong antibody response but limited protective efficacy | NIH, Malaria Vaccine Initiative (MVI), African trial sites |
| PfSPZ Vaccine | Attenuated whole sporozoite vaccine (IV route) | Mali, Tanzania, Burkina Faso, Kenya | Phase I–II (2015–2023 ongoing) | 40–55% efficacy in field trials; durable immune memory in controlled settings | Sanaria Inc., NIH, African collaborators |
| Transmission-Blocking Vaccines (TBVs) | Pfs25 / Pfs230 antigens (gametocyte stages) | Tanzania | Phase I (ongoing) | Safe and immunogenic; target parasite transmission rather than infection | PATH, NIH, African research institutions |
Africa’s involvement in malaria vaccine trials has progressed from passive participation to active scientific leadership. The continent has hosted pivotal efficacy trials, developed clinical and immunological infrastructure, and contributed critical data that informed global malaria vaccine policy. Current research continues to expand into multi-stage, transmission-blocking, and next-generation vaccines, with African scientists increasingly steering design and implementation.
Table 4.
Major Policy Milestones and Implementation Outcomes in African Malaria Control (1955–2025).
Table 4.
Major Policy Milestones and Implementation Outcomes in African Malaria Control (1955–2025).
| Period / Year | Policy or Initiative | Key Objectives / Focus | African Context & Implementation Outcomes |
|---|---|---|---|
| 1955 | WHO Global Malaria Eradication Programme (GMEP) | Eradicate malaria globally through vector control and drug treatment. | Limited success in Africa due to weak infrastructure, resistance to DDT, and poor healthcare systems; many regions excluded. |
| 1969–1976 | The Garki Project (Nigeria) | Develop realistic models of malaria transmission and evaluate IRS and MDA interventions. | Revealed challenges of eradication in high-transmission settings; established basis for integrated malaria control models. |
| 1988 | African Malaria Control Strategy (OAU/WHO) | Strengthen national malaria control programmes (NMCPs). | Marked Africa’s renewed regional ownership of malaria response post-GMEP failure. |
| 1998 | Roll Back Malaria (RBM) Initiative | Global partnership to reduce malaria burden through ITNs, IRS, and access to treatment. | Expanded ITN use, improved treatment access, but uneven national implementation. |
| 2000 | Abuja Declaration (AU Summit) | Commit African leaders to halve malaria deaths by 2010. | Catalysed political commitment, increased donor funding, and national strategic plans. |
| 2005–2010 | Scaling Up for Impact (SUFI) | Universal coverage of prevention and treatment interventions. | Notable reductions in malaria mortality; emphasis on ITN distribution and IPT in pregnancy. |
| 2015 | WHO Global Technical Strategy (GTS) 2016–2030 | Reduce malaria incidence and mortality by ≥ 90%. | Guided by data from African surveillance networks; adaptation to local epidemiology. |
| 2018–2021 | RTS,S Pilot Implementation (Ghana, Kenya, Malawi) | Evaluate first malaria vaccine in real-world settings. | Demonstrated feasibility, modest efficacy, and community acceptance of vaccination. |
| 2022–2025 | R21/Matrix-M Vaccine Roll-out & Genomic Surveillance Expansion | Strengthen immunity and integrate molecular tools into control strategies. | Improved vaccine coverage; genomic data guiding resistance monitoring and localised interventions. |
| Ongoing (2020s) | One Health & Climate-Resilient Malaria Policies | Integrate environmental, vector, and human health frameworks. | Focus on sustainability, adaptation to ecological change, and Africa-led research networks (e.g., MARA, PAMAfrica). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



