
Submitted:
16 October 2025
Posted:
22 October 2025
You are already at the latest version
Abstract
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by an impaired insulin secretion (or action), leading to persistent hyperglycemia. Such a disease, associated with multiple risk factors, can be broadly classified into two major types: Type 1 and type 2 diabetes. In recent years, herbal medicines (HMs) have been gaining significant attention as alternatives or complementary therapeutic options, owing to their rich content of bioactive compounds. These natural agents have been widely investigated for their potential in the prevention and management of several chronic diseases, including (i) cardiovascular disorders, (ii) infections, and notably (iii) diabetes mellitus. In this present state-of-the art review, we highlight the roles and impacts of various medicinal plants originating from diverse families upon emphasizing their active phytoconstituents, and the mechanisms through which they exert antidiabetic effects. Special emphasis is placed on how these bioactive ingredients can modulate glucose metabolism, enhance insulin sensitivity, and ultimately mitigate complications related to diabetes.
Keywords:
diabetes mellitus
; herbal-based medicine
; hyperglycemia
; medicinal plants
; phytochemicals
; anti-diabetic effects
; glucose transporter type 4 (GLUT4)
1. Introduction
Diabetes mellitus (DM) is a well-known (long-lasting) metabolic disorder identified by persistent hyperglycemia resulting from defects in insulin secretion, action or even both. Insulin, an anabolic hormone, plays a central role in the regulation of carbohydrates and lipids, as well as in protein metabolism. It can be then expected that disturbances in insulin activity have widespread consequences on the overall metabolic homeostasis. According to a recent statistical study conducted by the World Health Organization (WHO) [1], data have shown that the global burden of diabetes have increased dramatically between the years 1990 and 2022, from around 200 to 830 million (affected) individuals. In fact, it has been indicated that by the year 2022, approximately 14% of adults (18 years and slightly older) were living with the disease, a percentage that is indeed double the prevalence reported in 1990 (when the percentage was close to 7%). Moreover, a concerning aspect dictates that nearly 59% of adults affected by the disease, 30 years of age and above, were not receiving any form of medication to manage their condition. The rise has been particularly pronounced in low-to middle-income countries, where access to treatment remains critically scarce. Additionally, in the year 2021 alone, diabetes was recognized to be a direct cause of approximatively 1.6 million deaths, with almost half occurring before the age of 70. Furthermore, around 530,000 deaths from kidney disease were found to be directly linked to diabetes, and elevated blood glucose contributed to nearly 11% of all cardiovascular-induced deaths [2]. Concerning the clinical manifestations of diabetes, these can vary, within individuals, depending principally on blood glucose levels and common symptoms include (i) polyuria, (ii) polydipsia, (iii) polyphagia, (iv) unexplained weight loss, (v) recurrent skin, (vi) genital infections, (vii) irritability, (viii) ketonuria, (ix) dysuria, as well as (x) blurred vision [1,3]. If left uncontrolled and/or untreated, diabetes progresses to severe complications including cardiovascular disease, neuropathy, nephropathy, retinopathy and chronic ulceration [4]. Diabetes mellitus is classified into several forms, with the two predominant types being type 1 and type 2. Type 1 diabetes mellitus (termed as T1DM), commonly referred to as insulin-dependent diabetes, results from an autoimmune destruction of pancreatic β-cells in the islets of Langerhans, leading thus to an absolute insulin deficiency. Patients with T1DM are dependent on lifelong insulin therapy [5]. In contrast, type 2 diabetes mellitus (labeled as T2DM), or non-insulin-dependent diabetes, is primarily characterized by an insulin resistance due to defects in insulin receptor signaling, particularly at the tyrosine kinase level [6]. Other forms of diabetes include (a) gestational diabetes mellitus (GDM), a kind that develops during pregnancy, (b) monogenic diabetes, a form that is found linked to genetic defects in β-cell function (or insulin pathways), as well as (c) secondary diabetes resulting from exocrine pancreatic diseases and endocrinopathies as well as from drug- and chemical-induced damages [4,7]. It has been proven that multiple risk factors contribute to diabetes onset and progression, including genetic predisposition, chronic inflammation, obesity, physical inactivity, advancing age, poor dietary habits, ethnicity, stress, history of GDM, and disturbances in cellular redox balance such as reductive and oxidative stress [8,9]. While conventional antidiabetic medications such as metformin, sulfonylureas, insulin and some insulin-derived newer classes, principally GLP-1 receptor agonists and SGLT-2 inhibitors, have been reported effective in managing diabetes; they are unfortunately associated with several limitations and health-related drawbacks. Such adverse effects include (but are not limited to) hypoglycemia, weight gain, gastrointestinal disturbances and in some cases, cardiovascular risks. In fact, the progressive nature of type 2 diabetes often necessitates combination therapy or dose escalation over time, leading thus to increased healthcare costs associated with high risks of drug interaction. Besides such critical health impacts, it should be also mentioned that the global economic burden of diabetes is staggering, with annual direct medical costs exceeding $760 billion worldwide, excluding the indirect costs that are related to productivity loss and disability. This economic impact, combined with the growing prevalence of diabetes, particularly in developing nations with limited healthcare infrastructure, underscores the urgent need for accessible, affordable and most importantly effective therapeutic alternatives [10].
2. Biological Pathways Involved in Diabetes Management
Understanding the physiological role of insulin and its associated signaling pathway is essential for clarifying the mechanisms behind insulin resistance (IR). After a meal, elevated blood glucose stimulates pancreatic β-cells to release insulin. This hormone binds to receptors on target cell membranes, promoting glycogen and lipid storage in the liver, skeletal muscle, and adipose tissue. Insulin also suppresses hepatic glucose production by downregulating genes involved in gluconeogenesis and lipolysis in adipose tissue. The binding of insulin to its receptor tyrosine kinase (IRTK) triggers receptor auto-phosphorylation and activates adaptor proteins such as insulin receptor substrates (IRS), growth factor receptor-bound proteins (GRB-2 and GRB-10), SH2B adapter protein-2, and SHC-transforming protein. Phosphorylated IRS proteins recruit phosphatidylinositol-3-kinase (PI3K), which converts PIP2 into PIP3. This lipid second messenger attracts Akt to the membrane, where it is phosphorylated and activated by PDK1 and mTORC2 (Figure 1).
Akt activation initiates three major cascades: the CAP/Cbl pathway (facilitating GLUT4 translocation), the PI3K-dependent pathway (regulating glucose, lipid, and protein metabolism), and the MAP kinase pathway (controlling cell proliferation). Through these cascades, insulin promotes glucose uptake and nutrient storage in skeletal muscle, adipose tissue, and the liver. Beyond the classical insulin signaling pathway, the incretin system plays a crucial role in glucose homeostasis and represents an important target for both conventional and herbal antidiabetic therapies. The incretin hormones, primarily glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), are released from intestinal L-cells and K-cells respectively in response to nutrient intake. These hormones enhance glucose-dependent insulin secretion, suppress glucagon release, slow gastric emptying, and promote satiety. Importantly, several medicinal plants discussed in this review, including Berberis vulgaris (through berberine) and Gymnema sylvestre, have been shown to modulate incretin hormone levels or enhance their activity. This represents an additional mechanism through which herbal medicines can exert their antidiabetic effects, complementing their direct actions on insulin signaling and glucose metabolism. Understanding these interactions is crucial for developing comprehensive treatment strategies that leverage both conventional incretin-based therapies and herbal medicines. Oxidative stress, caused by an imbalance between reactive oxygen species (ROS) and antioxidant defenses, further disrupts insulin signaling. ROS such as superoxide radicals, hydrogen peroxide, and hydroxyl radicals are generated by mitochondrial activity and NADPH oxidase. Over nutrition and mitochondrial dysfunction enhance ROS production, leading to oxidative damage to lipids, proteins, and DNA, ultimately causing cell apoptosis. In diabetes, elevated ROS levels accelerate harmful pathways including protein kinase C activation, hexosamine flux, advanced glycation end-product (AGE) formation, and polyol pathway activation. These processes amplify inflammation and tissue injury. ROS also impair insulin receptor auto-phosphorylation and activate stress kinases such as JNK and IKKβ, which phosphorylate IRS proteins and block downstream insulin signaling. Additionally, ROS stimulate the release of pro-inflammatory cytokines such as TNF-α, IL-6, and IL-1β. Visceral adipose tissue is a major source of these mediators, which trigger NF-κB activation in insulin-responsive tissues, driving further inflammation and insulin resistance. Antioxidant therapies may help protect pancreatic β-cells from oxidative stress-induced apoptosis and preserve their insulin-secreting function [11].
3. Methodological Considerations and Quality Assessment
The evaluation of herbal medicines for diabetes management presents unique methodological challenges that must be acknowledged when interpreting research findings. Standardization of plant extracts remains a significant issue, as the concentration of bioactive compounds can vary substantially based on factors including geographic origin, harvesting season, extraction methods, and storage conditions. Many studies utilize different extraction protocols, making direct comparisons difficult. Furthermore, the quality of clinical evidence varies considerably, with many studies being small-scale, short-duration, or lacking proper randomization and blinding. While numerous in vitro and animal studies demonstrate promising antidiabetic effects, translation to human clinical outcomes requires more rigorous investigation. Future research should prioritize standardized extraction protocols, well-designed randomized controlled trials with adequate sample sizes, and long-term safety assessments. Additionally, pharmacokinetic studies are needed to understand the bioavailability and metabolism of key bioactive compounds, as this information is crucial for determining optimal dosing regimens and potential drug interactions.
4. Medicinal Herbs: Past and Present Insights
Over the past decades, complementary and alternative medicine, particularly herbal medicine (HM), has gained significant interest in the management of chronic diseases. Herbal preparations are widely utilized across diverse cultures—including China, Japan, New Zealand, Canada, the United States, and Russia—due to their therapeutic value and traditional acceptance [12,13]. Plants contain diverse bioactive secondary metabolites such as alkaloids, terpenes, phenolics, vitamins, and other nitrogenous compounds, which contribute to their defense mechanisms and biological activities [14]. These phytochemicals have been shown to exert antimicrobial [15,16], antioxidant, and anti-inflammatory effects [17], in addition to displaying anti-carcinogenic properties, cardiovascular protection, neuroprotective activity, and regulation of apoptosis and cell cycle processes [18,19,20]. In the context of diabetes, numerous medicinal plants have demonstrated hypoglycemic effects and are increasingly used alongside conventional antidiabetic drugs (Figure 2). Their mechanisms include enhancing glucose uptake by adipose and muscle tissues (ginseng, bitter melon and cinnamon), inhibiting glucose absorption from intestine (myrcia and sanzhi) and inhibiting glucose production from hepatocytes (berberine, fenurgreek leaves) [21,22,23]. Importantly, plant-based therapies are generally considered safer, more affordable, and more accessible than synthetic drugs, with fewer adverse effects [24].
5. Safety Considerations and Drug Interactions
While herbal medicines are generally perceived as safer alternatives to synthetic drugs, their use in diabetes management requires careful consideration of potential adverse effects and drug interactions. Several medicinal plants discussed in this review can potentiate the hypoglycemic effects of conventional antidiabetic medications, potentially leading to dangerous hypoglycemic episodes. For instance, bitter melon (Momordica charantia) and fenugreek (Trigonella foenum-graecum) have been reported to enhance insulin sensitivity and glucose uptake, which may necessitate dose adjustments of concurrent insulin or sulfonylurea therapy. Additionally, some herbal medicines may affect the metabolism of conventional drugs through modulation of cytochrome P450 enzymes. Garlic (Allium sativum) and turmeric (Curcuma longa) have been shown to influence drug-metabolizing enzymes, potentially altering the pharmacokinetics of co-administered medications. Healthcare providers should be aware of these potential interactions and monitor patients closely when herbal medicines are used alongside conventional therapies. Patient education regarding the importance of disclosing herbal medicine to healthcare providers is essential for safe and effective diabetes management.
6. Antidiabetic Medicinal Plants
6.1. Achyranthes aspera
Achyranthes aspera, commonly known as Devil’s horsewhip, is a member of the Amaranthaceae family and is widely distributed as a weed throughout India [25]. Phytochemical screening has revealed that the plant contains a variety of bioactive compounds, including saponins, alkaloids, steroids, flavonoids, and terpenoids [26]. Traditionally, it has been used in the treatment of several conditions such as toothache, rheumatism, inflammation, bronchitis, microbial infections, skin diseases, colds, asthma, piles, rabies, and notably, diabetes [26,27]. Several studies have highlighted its antidiabetic potential. In an in vivo study, ethanolic seed extracts of A. aspera (300 mg/kg and 600 mg/kg body weight) were administered to streptozotocin (STZ)-induced diabetic rats for 28 days. The treatment significantly reduced blood glucose levels in comparison with the standard drug glibenclamide (5 mg/kg body weight) [27]. Similarly, in vitro investigations demonstrated that leaf extracts of A. aspera inhibited the activities of α-amylase and α-glucosidase enzymes in a dose-dependent manner, comparable to standard antidiabetic drugs. Since these enzymes are responsible for carbohydrate digestion and the postprandial rise in blood glucose, their inhibition suggests a promising mechanism for glycemic control [28]. Another study reported that administration of A. aspera as an herbal tea led to a significant reduction in blood glucose and serum triglyceride levels after one week of treatment [29]. Furthermore, experimental evidence in diabetic rats indicated that oral administration of A. aspera not only reduced hyperglycemia and dyslipidemia but also alleviated oxidative stress and enhanced pancreatic insulin protein expression, confirming both its antidiabetic and antilipidemic activities [26].
6.2. Allium sativum
Allium sativum, commonly known as garlic, is a flowering plant belonging to the family Amaryllidaceae and the genus Allium [30]. It is thought to have originated in Southern Europe and Central Asia and is now widely cultivated worldwide, with China being the largest producer. Garlic has been extensively used both as a culinary spice and a medicinal herb due to its broad spectrum of biological activities. It possesses anticancer, antibacterial, antifungal, anti-inflammatory, and antioxidant properties [31]. In addition, it has demonstrated beneficial effects in the management of cardiovascular disease, hypertension, and diabetes. Phytochemically, garlic is rich in a variety of bioactive compounds including fibers, adenosine sulfur, pectin, fructans, lectin, prostaglandins, nicotinic acid, carbohydrates, phospholipids, fatty acids, essential amino acids, selenium, potassium, iron, manganese, calcium, phosphorus, sodium, and vitamins C, E, B1, B2, and B6. Many of these constituents are believed to contribute to its therapeutic potential. In the context of diabetes, garlic has been shown to inhibit the enzyme α-glucosidase, a key enzyme in carbohydrate metabolism, thereby reducing postprandial blood glucose levels [32]. Clinical and experimental evidence also indicates that garlic lowers total cholesterol, triglycerides, and LDL cholesterol, while simultaneously improving insulin sensitivity [33]. Collectively, these effects support the use of A. sativum as a complementary agent in the management of diabetes and its associated metabolic complications.
6.3. Aloe vera
Aloe vera has been used for centuries in cosmetics, traditional medicine, and modern healthcare products. It possesses a wide range of pharmacological properties, including anti-inflammatory, antioxidant, anti-tumor, laxative, wound healing, anti-aging, and antidiabetic activities [34,35]. Taxonomically, Aloe vera belongs to the family Liliaceae. Its bioactive constituents include minerals, lignin, enzymes, vitamins, sugars, amino acids, and salicylic acid [34,35]. Other key compounds such as alprogen and chromium have been shown to lower blood glucose levels, restore pancreatic β-cell function, and enhance insulin activity [36]. Several studies have highlighted its role in diabetes management. One study demonstrated that Aloe vera reduced blood glucose levels by inhibiting the glycation pathway and ameliorating hyperlipidemia [35]. Another comparative study reported beneficial effects in both in vivo and in vitro models: in vivo, Aloe vera treatment increased serum insulin and decreased serum glucose in diabetic rats, while in vitro experiments showed enhanced insulin secretion from isolated pancreatic islets [37]. Moreover, clinical trials revealed that Aloe vera gel improved glycemic control in type 2 diabetic patients without significantly affecting lipid profiles [38].
6.4. Amaranthus tricolor (Lal Chaulai / Joseph’s Coat)
Amaranthus tricolor, also known as Lal Chaulai or Joseph’s coat, belongs to the family Amaranthaceae and is mainly distributed in temperate and tropical regions [25,39]. Traditionally, it has been used to treat piles, leucorrhea, constipation, leprosy, and bronchitis [39]. Pharmacological investigations have confirmed its anti-hyperlipidemic, anti-hyperglycemic, antiviral, anti-proliferative, cyclooxygenase enzyme inhibitory, antioxidant, and antidiabetic activities [25,40,41]. Experimental studies have demonstrated its potential against diabetes. For example, A. tricolor extract significantly reduced pancreatic malondialdehyde (MDA) levels and blood glucose in STZ-induced diabetic rats, suggesting a protective effect against oxidative stress [42]. Another study showed that leaf and stem extracts exhibited anti-diabetic, anti-lipase, anti-α-amylase, anti-α-glucosidase, and anti-acetylcholinesterase (AChE) activities, highlighting its therapeutic role in the prevention and management of diabetes [43].
6.5. Anacardium occidentale (Cashew Tree)
Anacardium occidentale, commonly known as the cashew tree, belongs to the family Anacardiaceae. Native to Brazil and now cultivated worldwide, its nuts are rich in bioactive compounds such as linoleic acid, oleic acid, tannins, tocopherols, flavonoids, anthocyanins, dietary fiber, folate, and unsaturated fatty acids (UFAs). Traditionally, it has been used to treat skin diseases, fever, pain, diarrhea, and arthritis [44,45]. Recent studies on the aerial parts of Anacardium occidentale have highlighted their strong antioxidant properties, which are closely linked to antidiabetic activity. These extracts exhibit potent free radical scavenging capacity while also enhancing the expression and activity of key endogenous antioxidant enzymes, including superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx). Such antioxidant protection is particularly relevant in type 2 diabetes mellitus (T2DM), where oxidative stress is a major driver of insulin resistance and β-cell dysfunction. Elevated reactive oxygen species (ROS) disrupt insulin receptor signaling and stimulate the release of pro-inflammatory cytokines, thereby worsening metabolic imbalance. By counteracting oxidative stress, A. occidentale extracts support insulin signaling, suppress inflammation, and protect pancreatic β-cells against apoptosis [46]. Scientific studies highlight its potential in diabetes management. The inner bark extract of A. occidentale significantly reduced hyperglycemia in alloxan-induced diabetic rats [47]. Similarly, methanolic stem bark extract reduced hyperglycemia, hyperlipidemia, and lipid peroxidation, thereby offering protection against the diabetogenic effects of a high-fructose diet in diabetic rats [48]. Moreover, leaf extract combined with riboceine improved hepatic and renal function, restored β-cell activity, and modulated several diabetes-related genes, contributing to better glycemic control [49].
6.6. Annona squamosa (Custard Apple / Sugar Apple)
Annona squamosa, a tropical tree belonging to the family Annonaceae, is traditionally known as custard apple or sugar apple. Various parts of the plant (roots, bark, seeds, leaves, and fruits) possess anti-ulcer, antiseptic, renoprotective, hepatoprotective, analgesic, antipyretic, anti-inflammatory, antioxidant, and antidiabetic properties. Consequently, it has been widely used in the treatment of gastritis, diarrhea, parasitic infections, rheumatism, splenic disorders, dysentery, and diabetes [50,51]. Experimental evidence supports its antidiabetic role. In streptozotocin (STZ)-induced diabetic rats, Annona squamosa significantly reduced blood glucose levels, lowered cholesterol, VLDL, LDL, triglycerides, and improved liver function markers [52]. Another study in rabbits (non-rodents) and rats (rodents) demonstrated that water extract of Annona squamosa effectively controlled hyperglycemia in both alloxan- and STZ-induced diabetes by stimulating glucose uptake in muscle and intestine, as well as enhancing insulin release from the pancreas [53]. Furthermore, aqueous extract supplementation improved lipid metabolism, increased plasma insulin, and prevented diabetic complications in STZ-induced diabetic rats [54].
6.7. Berberis vulgaris (Barberry)
Berberis vulgaris, commonly known as barberry, belongs to the family Berberidaceae. It is a deciduous, spiny shrub with elliptic leaves. Phytochemical analyses have revealed the presence of vitamins, proteins, lipids, tannins, carotenoids, anthocyanins, alkaloids, and phenolic compounds [55]. Among its bioactive components, the isoquinoline alkaloid berberine (a quaternary ammonium salt) is considered the most potent, with documented effects in preventing and treating several chronic diseases, including cardiovascular disorders, cancer, inflammatory diseases, depression, and diabetes [56]. Experimental studies support the antidiabetic activity of Berberis vulgaris. Aqueous and saponin extracts significantly reduced blood glucose, cholesterol, and triglyceride levels in streptozotocin (STZ)-induced diabetic rats compared with control [57]. Another study demonstrated that berberine prevented fructose-induced insulin resistance in rats by downregulating aldose reductase expression and inhibiting its enzymatic activity, thereby suppressing the polyol pathway that is hyper activated under hyperglycemia [58]. The antidiabetic mechanisms of berberine (BBR) are multifactorial. It enhances glucose-stimulated insulin secretion (GSIS), improves insulin sensitivity, inhibits glucagon release, and stimulates pancreatic β-cell proliferation. Berberine also promotes glucagon-like peptide-1 (GLP-1) secretion, modulates gut microbiota linked to type 2 diabetes, and reduces insulin resistance through upregulation of insulin receptor proteins (InsR) via the protein kinase C (PKC)-dependent pathway. Furthermore, it exerts anti-inflammatory effects by reducing the expression of TNF-α, ROS, IL-6, and IL-1. On a molecular level, berberine inhibits key enzymes such as α-glucosidase, protein tyrosine phosphatase 1B (PTP1B), and dipeptidyl peptidase-4 (DPP-4), leading to reduced intestinal glucose absorption. It also induces glycolysis by stimulating the translocation of glucose transporters GLUT1 and GLUT4 and by activating the AMP-activated protein kinase (AMPK) pathway [55,56,59].
6.8. Cinnamomum zeylanicum
Cinnamomum zeylanicum, also known as “true cinnamon” or “Ceylon cinnamon,” is one of the 250 species belonging to the genus Cinnamomum and family Lauraceae. Traditionally used as a spice and flavoring agent, it has also been widely recognized for its medicinal applications [60]. Phytochemical analyses have revealed that C. zeylanicum contains numerous bioactive constituents with diverse biological activities, including anti-inflammatory, antimicrobial, antibacterial, anti-oxidant, anti-allergic, anti-pyretic, analgesic, and antidiabetic properties. Key components include eugenol (predominantly in the leaves), tannins, β-caryophyllene, linalool, cinnamic acid, weiterhin, mucilage, diterpenes, proanthocyanidins, cinnamaldehyde, cinnamyl acetate, cinnamyl alcohol, methyl chavicol, and methyl-hydroxy chalcone polymer (MHCP) [61]. In diabetic patients, Ceylon cinnamon has demonstrated multiple health benefits such as lowering fasting blood glucose, reducing LDL cholesterol, increasing HDL cholesterol, and contributing to weight loss [62]. The antidiabetic mechanisms of C. zeylanicum are multifaceted: i) inibition of carbohydrate-digesting enzymes: Cinnamon reduces intestinal glucose absorption by inhibiting pancreatic α-amylase and α-glucosidase [62,63,64], ii) regulation of glucose metabolism: It enhances glycogen synthesis and promotes glucose metabolism in peripheral tissues [62], iii) stimulation of glucose transporters: Cinnamon upregulates GLUT-4 expression and facilitates its translocation to the plasma membrane, thereby increasing cellular glucose uptake [65], and iv) insulin-like activity: Extracts of C. zeylanicum have been shown to decrease plasma glucose and increase plasma insulin [64,66]. One active compound, cinnamtannin B1, exhibits insulin-mimetic activity by binding to insulin receptors, triggering auto-phosphorylation, PI3K activation, and subsequent GLUT-4 translocation, which enhances glucose uptake [67]. Together, these findings suggest that C. zeylanicum exerts its hypoglycemic effects through both insulin-sensitizing and insulin-mimetic actions, making it a valuable complementary therapy for diabetes management (Figure 3).
6.9. Curcuma longa (Turmeric)
Curcuma longa, commonly known as turmeric, belongs to the family Zingiberaceae and is widely cultivated in Southeast Asia [68]. Type 2 diabetes mellitus (T2DM) development is strongly associated with oxidative stress, which activates protein kinase C and enhances polyol pathway flux [69]. Curcumin, the principal bioactive compound in Curcuma longa, exhibits strong protective effects on pancreatic islet cells through diverse molecular pathways. It promotes islet cell survival by attenuating reactive oxygen species (ROS) production and inhibiting pro-inflammatory mediators such as TNF-α and IL-1β, partly via suppression of NF-κB nuclear translocation. In diabetic DB/DB mice, curcumin has been shown to activate AMPK and PPARγ signaling, thereby improving metabolic homeostasis, while concurrently reducing NF-κB protein levels, though it does not appear to influence SIRT1 or PGC-1 expression. Beyond these effects, curcuminoids enhance antioxidant defenses by regulating the expression of gamma-glutamyl-cysteine ligase, HO-1, and NAD(P)H: quinone oxidoreductase 1 at both the transcript and protein levels in human pancreatic islets. This modulation results in increased antioxidant enzyme activity and elevated glutathione content, which collectively protect islet cells against oxidative damage. Moreover, curcumin interacts with a wide spectrum of signaling pathways, targeting growth factors, enzymes, transcription factors, cytokines, interleukins, and chemokines, underscoring its broad therapeutic value in diabetes management [68,70,71]. In patients with T2DM, treatment with Curcuma longa extracts has been shown to reduce fasting glucose and insulin levels, lower leptin, resist in, TNF-α, IL-6, and IL-1β, while improving insulin resistance, hyperlipidemia, and hyperglycemia. Additionally, it increases adiponectin secretion and protects against pancreatic islet apoptosis and necrosis [69,72]. These effects confirm that curcumin, the major bioactive compound, plays a central role in diabetes prevention and treatment [72]. Several studies have supported these findings. A randomized, double-blind, placebo-controlled clinical trial demonstrated that curcumin supplementation significantly reduced the risk of developing T2DM in prediabetic individuals and improved β-cells function [73]. Another clinical study reported that in T2DM patients, Curcuma longa significantly decreased HbA1c, fasting blood glucose (FBG), and other metabolic parameters [74].
6.10. Gymnema sylvestre
Gymnema sylvestre, also known as Meshashringi or Madhunashini, belongs to the Asclepiadaceae family [75,76] and is primarily found in tropical Africa, Australia, and central and western India. Traditionally, it has been used to treat inflammation, snakebites, asthma, eye disorders, and microbial infections, and also exhibits anti-obesity, anti-hypercholesterolemic, and hepatoprotective activities. The antidiabetic effects of Gymnema sylvestre are primarily attributed to regeneration of pancreatic islet cells, increased insulin secretion, inhibition of intestinal glucose absorption, inhibition of α-glucosidase enzyme, enhancement of peripheral glucose utilization [75,77,78] (Figure 4). The leaves contain bioactive compounds including gymnemic acids, gurmarin, gymnemagenol, gymnomosides, and gymnemanol, which contribute to these effects [76].
Experimental studies have confirmed its hypoglycemic activity. In hyperglycemic rats, leaf extracts of Gymnema sylvestre increased plasma insulin levels and significantly reduced blood glucose by modulating the expression of key genes involved in glucose metabolism and diabetes control, such as Irs1, Irs2, SREBP1c, Foxo1, Ins-1, Ins-2, and NF-κB [76]. Another study demonstrated that rabbits treated with aqueous extracts of Gymnema sylvestre in combination with metformin showed enhanced hypoglycemic effects, increased insulin secretion, and improved kidney and liver function markers (creatinine, serum urea, and liver enzymes) compared to controls [79].
6.11. Gynostemma pentaphyllum
Gynostemma pentaphyllum is a climbing plant mainly found in the mountainous regions of Vietnam, Japan, North Korea, China, and Southeast Asia. It belongs to the family Cucurbitaceae. The plant exhibits multiple biological activities (Figure 5), including anti-oxidant, anti-apoptotic, anti-hyperlipidemia, anticancer, anti-inflammatory, immunomodulatory, anti-fatigue, cardio protective, neuroprotective, regulating micro flora and hypoglycemic effects [80,81]. Studies in type 2 diabetic mice have demonstrated that Gynostemma pentaphyllum improves insulin sensitivity and reduces hyperglycemia via activation of the AMPK-mediated signaling pathway [82,83]. Additionally, heat-processed extracts of Gynostemma pentaphyllum have been shown to increase GLUT4 expression and decrease liver histological damage in high-fat diet-induced glucose metabolic disorder models, indicating protection against metabolic and hepatic dysfunction [84].
6.12. Momordica charantia
Momordica charantia, commonly known as bitter gourd or bitter melon, is a tropical and subtropical plant belonging to the Cucurbitaceae family. It is widely cultivated in South America, East Africa, Asia, and India [85]. Nutritionally, M. charantia is considered a nutrient-dense plant rich in essential minerals such as potassium, calcium, zinc, magnesium, phosphorus, and iron, as well as antioxidants and vitamins including vitamin C, vitamin A, vitamin E, vitamin B9, and several B-complex vitamins (B1, B2, B3) [27]. In addition, phytochemical analyses have identified various bioactive compounds such as steroids, alkaloids, triterpenes, proteins, phenolics, and lipids, which are believed to contribute to its therapeutic activities [85,86,87]. The antidiabetic properties of M. charantia have been well-documented. Its hypoglycemic effect is mediated through several mechanisms: i) M. charantia reduces the activity of key gluconeogenic enzymes, including glucose-6-phosphatase and fructose-1,6-bisphosphatase, thereby suppressing hepatic glucose production, ii) it promotes glucose transport into skeletal muscle cells and increases the expression of intestinal Na⁺/glucose co-transporters, both of which contribute to lowering postprandial blood glucose levels, and iii) experimental studies suggest that M. charantia helps preserve the morphology and function of pancreatic islet β-cells, which are responsible for insulin secretion. This protective effect supports improved insulin production and overall pancreatic health [87,88,89]. Collectively, these mechanisms highlight M. charantia as a promising antidiabetic medicinal plant with multifaceted actions, including enhancement of peripheral glucose utilization, reduction of hepatic glucose output, and preservation of β-cell integrity (Figure 6).
6.13. Nigella sativa (Black Seed / Black Cumin)
Nigella sativa, commonly known as black seed or black cumin, belongs to the genus Nigella L. in the family Ranunculaceae, order Ranunculales, class Magnoliopsida, division Tracheophyta, kingdom Plantae [90]. It is mainly distributed in Mediterranean countries and Iran. The oil derived from Nigella sativa contains bioactive compounds such as alkaloids, phenolics, and terpenes [91]. Traditionally, Nigella sativa has been used for the treatment of various chronic conditions including cancer, obesity, hypertension, and diabetes (Figure 7) [92]. The most important bioactive constituent is thymoquinone (TQ), which exhibits antidiabetic effects through multiple mechanisms. TQ inhibits α-glucosidase and α-amylase digestive enzymes, stimulate MAPK pathway activation that leads to increase in muscle GLUT-4 levels, inhibits the activity of COX and lipoxygenase (LOX) enzymes, suppresses hepatic gluconeogenesis by targeting fructose-1,6-bisphosphatase and glucose-6-phosphatase, suppress pro-inflammatory cytokines such as IL-6, TNF-α, IFN-γ and IL-1β, inhibits NO production and reduces intestinal glucose absorption by inhibiting sodium-glucose linked transporter 1 (SGLT1). Additionally, since diabetes is associated with increased reactive oxygen species (ROS) that damage pancreatic β-cells, Nigella sativa enhances antioxidant defense by increasing the activity of superoxide dismutase (SOD), glutathione peroxidase (GPx), and catalase (CAT). It also stimulates β-cell proliferation, enhances insulin secretion, and decreases insulin resistance [90,91,92,93,94].
Several experimental and clinical studies have confirmed these effects. For instance, low-dose intraepithelial administration of N. sativa oil protected pancreatic islets and increased serum insulin levels in type 1 diabetes models [95]. In a clinical observation, daily intake of Nigella sativa tea reduced body weight and blood glucose levels in a 72-year-old patient with type 2 diabetes [96].
6.14. Ocimum sanctum
Ocimum sanctum, commonly known as holy basil, belongs to the family Lamiaceae and is predominantly found in the South Asian region. Traditionally, its leaves have been used to manage a wide variety of conditions including chronic fever, helminthiasis, dyspepsia, skin disorders, bronchial asthma, dysentery, catarrhal bronchitis, hemorrhage, and hypoglycemia. The hypoglycemic effect of Ocimum sanctum is attributed primarily to its ability to lower blood glucose levels and stimulate insulin secretion from pancreatic β-cells [97]. Several experimental studies have confirmed the antidiabetic potential of O. sanctum. For example, ethanolic leaf extract of O. sanctum was tested in alloxan-induced diabetic rats, where it demonstrated a significant hypoglycemic effect comparable to that of glibenclamide (a standard sulfonylurea antidiabetic drug). The proposed mechanism involved an increase in intracellular calcium levels within pancreatic β-cells, which in turn enhanced insulin secretion [98]. Another study reported that leaf oil extract of O. sanctum significantly reduced blood glucose and serum lipid levels, while simultaneously increasing serum insulin concentrations in streptozotocin (STZ)-induced diabetic rats [99]. Taken together, these findings suggest that O. sanctum exerts its antidiabetic effects through stimulation of insulin secretion, improvement of lipid profile, and reduction of hyperglycemia, highlighting its potential as a supportive herbal therapy for diabetes management.
6.15. Punica granatum (Pomegranate)
Punica granatum, commonly known as pomegranate, is a medicinal and edible plant belonging to the family Punicaceae (sometimes classified under Lythraceae). It is widely distributed across the Mediterranean region, Southeast Asia, Africa, Europe, and the northwestern provinces of China. Pomegranate leaves are particularly rich in triterpenoids, phenolic compounds, and tannins, which contribute to its pharmacological activities [101,102]. Traditionally, pomegranate has been used for the prevention and treatment of various conditions, including dental disorders, erectile dysfunction, cardiovascular disease, cancer, and diabetes. Its therapeutic value is largely attributed to its potent antioxidant capacity, particularly in scavenging free radicals and reducing oxidative stress, a key factor in the pathogenesis of diabetes [101,102]. The antidiabetic mechanisms of P. granatum include stimulating pancreatic β-cell secretion, enhancing insulin expression, and increasing glucose uptake by upregulating the mRNA expression of IRS-1 and Akt genes [102]. These effects improve insulin signaling and glucose metabolism. Several experimental studies support its antidiabetic potential. In type 2 diabetic rats, flower polyphenol extracts improved blood antioxidant status, lipid profile, liver glycogen storage, and insulin sensitivity, resulting in reduced blood glucose levels [103]. Another study reported that oral administration of fresh juice and peel extract increased catalase (CAT) enzyme activity, improved pancreatic islet health, and exhibited antioxidant and lipid-lowering effects in diabetic male albino rats [104]. Overall, P. granatum exerts its antidiabetic effect by combining antioxidant activity, β-cell protection, enhancement of insulin signaling, and improvement of lipid metabolism, making it a promising natural therapeutic agent for diabetes management.
6.16. Trigonella foenum-graecum
Trigonella foenum-graecum, commonly known as fenugreek, is a medicinal plant belonging to the Fabaceae family. Its leaves and seeds are nutrient-rich, containing essential vitamins, minerals, and macronutrients [104]. Fenugreek has long been recognized for its therapeutic properties, particularly as an antidiabetic herb, owing to its diverse phytochemical composition. The seeds and leaves of fenugreek contain polyphenols, alkaloids, flavonoids, saponins, steroids, lipids, carbohydrates, hydrocarbons, galactomannan fiber, and amino acids [105,106]. Among these, diosgenin (a steroidal saponin) is considered the most bioactive compound, known to improve diabetic status by promoting pancreatic β-cell renewal and stimulating insulin secretion [106]. Another key compound, 4-hydroxyisoleucine, a plant-derived amino acid present in high amounts in fenugreek, has been shown to enhance insulin secretion and reduce insulin resistance in peripheral tissues such as muscle and liver [106,107]. The high fiber content of fenugreek seeds, particularly galactomannan, which constitutes 45–60% of the seed, contributes significantly to its antidiabetic effect. This soluble fiber forms a viscous gel in the intestine, slowing glucose absorption and creating a physical barrier that reduces postprandial glucose spikes [106,107]. Additionally, fenugreek fibers inhibit lipid- and carbohydrate-hydrolyzing enzymes, thereby further supporting glycemic control [107]. Experimental evidence also supports fenugreek’s role in modulating cellular glucose uptake. In HepG2 cells, fenugreek treatment increased glucose uptake through upregulation of glucose transporter-2 (GLUT-2) mRNA levels [108]. Furthermore, studies in cell lines including CHO-HIRc-mycGLUT4eGFP, 3T3-L1-mycGLUT4, 3T3-L1, HepG2, and A431 demonstrated that fenugreek seeds enhanced tyrosine phosphorylation of IRS1 and PI3K proteins, leading to protein kinase C (PKC) activation. This signaling cascade facilitated the translocation of GLUT4 to the plasma membrane, thereby increasing glucose uptake from the blood [109]. Collectively, the diverse bioactive constituents of Trigonella foenum-graecum (fenugreek) exert significant hypoglycemic effects through multiple mechanisms. These include the regeneration of pancreatic β-cells, stimulation of insulin secretion, enhancement of insulin sensitivity, inhibition of carbohydrate-digesting enzymes such as α-amylase and α-glucosidase, and upregulation of glucose transporter activity. Furthermore, T. foenum-graecum promotes insulin signaling by inducing tyrosine phosphorylation of insulin receptor substrate-1 (IRS-1) and phosphoinositide 3-kinase (PI3K), leading to activation of protein kinase C (PKC) and subsequent translocation of glucose transporter type 4 (GLUT4) to the cell membrane, thereby facilitating glucose uptake. These properties highlight T. foenum-graecum as a promising complementary therapeutic agent for diabetes management (Figure 8).
7. Conclusions
Plants have demonstrated significant potential as herbal medicines, serving as natural antioxidants and showing therapeutic value in the treatment of several diseases, including diabetes mellitus. Data regarding the plants with known action against diabetes, including the active part(s) of the plants and the mechanism(s) involved are listed in Table 1. Compared to conventional drugs, they often provide greater availability, lower cost, and favorable safety profiles. Despite the promising results, further research is required to identify additional plant species with antidiabetic potential, clarify their precise molecular mechanisms, and explore the synergistic effects of combining different plant-derived compounds.
A deeper understanding of these interactions and the crosstalk among affected cellular pathways will be essential to fully harness the therapeutic benefits of medicinal plants in diabetes treatment. The integration of herbal medicines into modern diabetes care represents a promising frontier that requires continued research, standardization efforts, and collaborative approaches between traditional and modern medicine. As the global burden of diabetes continues to rise, the development of safe, effective, and accessible herbal therapies may provide valuable complementary options for patients worldwide, particularly in resource-limited settings where conventional treatments may be less available or affordable.
Author Contributions
All authors have read and agreed to the published version of the manuscript..
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Diabetes. WHO 2024, 14 November. https://www.who.int/news-room/fact-sheets/detail/diabetes.
- Antar, S.A.; Ashour, N.A.; Sharaky, M.; Khattab, M.; Ashour, N.A.; Zaid, R.T.; Roh, E.J.; Elkamhawy, A.; Al-Karmalawy, A.A. Diabetes mellitus: Classification, mediators, and complications; A gate to identify potential targets for the development of new effective treatments. Biomed. Pharmacother. 2023, 168, 115734. [CrossRef]
- Shaikh, A.A.; Kolhatkar, M.K.; Sopane, D.K.; Thorve, A.N. Review on: Diabetes mellitus is a disease. Int. J. Res. Pharm. Sci. 2022, 13, 102–109. [CrossRef]
- Bastaki, S. A review diabetes mellitus and its treatment. Int. J. Diabetes Metab. 2005, 13, 111–134. [CrossRef]
- Dey, R.K. Diabetes Mellitus: A comprehensive review of pathophysiology, management, and emerging therapeutic approaches. Diabetes Mellitus 2023.
- Lu, X.; Xie, Q.; Pan, X.; Zhang, R.; Zhang, X.; Peng, G.; Zhang, Y.; Shen, S.; Tong, N. Type 2 diabetes mellitus in adults: pathogenesis, prevention and therapy. Sig. Transduct. Target. Ther. 2024, 9, 262–286. [CrossRef]
- Savan, C.; Viroja, D.; Kyada, A. An updated review on diabetes mellitus: Exploring its etiology, pathophysiology, complications and treatment approach. IJCAAP 2024, 9, 31–36. [CrossRef]
- Tegegne, B.A.; Adugna, A.; Yenet, A.; Yihunie Belay, W.; Yibeltal, Y.; Dagne, A.; Hibstu Teffera, Z.; Amare, G.A.; Abebaw, D.; Tewabe, H.; Abebe, R.B.; Zeleke, T.K. A critical review on diabetes mellitus type 1 and type 2 management approaches: From lifestyle modification to current and novel targets and therapeutic agents. Front. Endocrinol. 2024, 15, 1440456–1440475. [CrossRef]
- Yameny, A.A. Diabetes mellitus overview. J. Biosci. Appl. Res. 2024, 10, 641–645. [CrossRef]
- . [CrossRef] [PubMed]
- Kaur, S.; Gadpayle, D.; Kumari, A.; Kaur, G.; Seen, K.; Bhardwaj, R.; Kumar, A. Antidiabetic potential of underutilized crops: Nutritional, phytochemical insights, and prospects for diabetes management. Appl. Food Res. 2025, 5, 101127. [CrossRef]
- Albahri, G.; Badran, A.; Hijazi, A.; Daou, A.; Baydoun, E.; Nasser, M.; Merah, O. The therapeutic wound healing bioactivities of various medicinal plants. Life 2023, 13, 317. [CrossRef]
- Enioutina, E.Y.; Salis, E.R.; Job, K.M.; Gubarev, M.I.; Krepkova, L.V.; Sherwin, C.M.T. Herbal Medicines: challenges in the modern world. Part 5. Status and current directions of complementary and alternative herbal medicine worldwide. Expert Rev. Clin. Pharmacol. 2016, 1–12. [CrossRef]
- Chanda, S.; Ramachandra, T.V. A review on some therapeutic aspects of phytochemicals present in medicinal plants. Int. J. Pharm. Life Sci. 2019, 10, 6052–6058.
- McEwen, S.A.; Collignon, P.J. Antimicrobial resistance: A one health perspective. Microbiol. Spectr. 2018, 6, 1–22. [CrossRef]
- Huemer, M.; Mairpady Shambat, S.; Brugger, S.D.; Zinkernagel, A.S. Antibiotic resistance and persistence—Implications for human health and treatment perspectives. EMBO Rep. 2020, 21, 51034–51057. [CrossRef]
- Forni, C.; Facchiano, F.; Bartoli, M.; Pieretti, S.; Facchiano, A.; D’Arcangelo, D.; Norelli, S.; Valle, G.; Nisini, R.; Beninati, S.; Tabolacci, T.; Jadeja, R.N. Beneficial Role of Phytochemicals on Oxidative Stress and Age-Related Diseases. Biomed. Res. Int. 2019, 1–16. [CrossRef]
- Al-Ishaq, R.K.; Overy, A.J.; Büsselberg, D. Phytochemicals and Gastrointestinal Cancer: Cellular Mechanisms and Effects to Change Cancer Progression. Biomolecules 2020, 10, 105. [CrossRef]
- Sundaram, M.K.; Khan, M.A.; Alalami, U.; Somvanshi, P.; Bhardwaj, T.; Pramodh, S.; Raina, R.; Shekfeh, Z.; Haque, S.; Hussain, A. Phytochemicals induce apoptosis by modulation of nitric oxide signaling pathway in cervical cancer cells. 2020, 24, 11827–11844. https://doi: 10.26355/eurrev_202011_23840.
- Lin, R.; Hu, X.; Chen, S.; Shi, Q.; Chen, H. Naringin induces endoplasmic reticulum stress-mediated apoptosis, inhibits β-catenin pathway and arrests cell cycle in cervical cancer cells. Acta Biochim. Pol. 2020, 67, 181-186. [CrossRef]
- Kooti, W.; Farokhipour, M.; Asadzadeh, Z.; Ashtary-Larky, D.; Asadi-Samani, M. The role of medicinal plants in the treatment of diabetes: a systematic review. Electron. Physician 2016, 8, 1832–1842. [CrossRef]
- Salleh, N.H.; Zulkipli, I.N.; Mohd Yasin, H.; Ja’afar, F.; Ahmad, N.; Wan Ahmad, W.A.N.; Ahmad, S.R. Systematic Review of Medicinal Plants Used for Treatment of Diabetes in Human Clinical Trials: An ASEAN Perspective. Evid. Based Complement. Alternat. Med. 2021, 1–10. [CrossRef]
- Hui, H.; Tang, G.; Go, V. Hypoglycemic herbs and their action mechanisms. Chin. Med. 2009, 4, 1–11. [CrossRef]
- Mahmoud, V.L.; Shayesteh, R.; Foong Yun Loh, T.K.; Chan, S.W.; Sethi, G.; Burgess, K.; Lee, S.H.; Wong, W.F.; Looi, C.Y. Comprehensive review of opportunities and challenges of ethnomedicinal plants for managing type 2 diabetes. Heliyon 2024, 10, 39699–39714. [CrossRef]
- Zanzabil, K.Z.; Hossain, M.S.; Hasan, M.K. Diabetes mellitus management: An extensive review of 37 medicinal plants. Diabetology 2023, 4, 186–234. [CrossRef]
- Asiago, O.H.; Reddy, K.S. Protective effect of achyranthes aspera against high fat diet and streptozotocin induced diabetes in rats [Adventure]. Journal of Chemical Health Risks, 13(6), 3124–3131. https://www.jchr.org.
- Vijayaraj, R.; Naresh Kumar, K.; Mani, P.; Senthil, J.; Jayaseelan, T.; Dinesh Kumar, G. Hypoglycemic and antioxidant activity of Achyranthes aspera seed extract and its effect on streptozotocin induced diabetic rats. Int. J. Biol. Pharm. Res. 2016, 7, 23–28. [CrossRef]
- Priyamvada, P.M; Mishra, P.; Sha, A.; Mohapatra, A.K. Evaluation of antidiabetic and antioxidant activities of Achyranthes aspera leaf extracts: An in vitro study. Int. J. Pharm. Life Sci. 2021, 10, 103–110. Priyamvada, Mishra, P., Sha, A., & Mohapatra, A. K. (2021). Evaluation of antidiabetic and antioxidant activities of Achyranthes aspera leaf extracts: An in vitro study. Journal of Pharmacognosy and Phytochemistry, 10(4), 103–110. https://www.phytojournal.com/archives/2021/vol10issue4/PartB/10-5-12-481.pdf.
- Njideka, B.E.; Theophilus, A.E.N.; Ugochukwu, N.T. Use of Achyranthes aspera Linn Tea as antidiabetic and hypolipidemic herbal tea. Int. J. Health Sci. Res. 2019, 9, 32–38. Njideka, B. E., Theophilus, A. E. N., & Ugochukwu, N. T. (2019). Use of Achyranthes aspera Linn Tea as Antidiabetic and Hypolipidemic Herbal Tea. International Journal of Health Sciences and Research, 9(2), 32–38. https://www.ijhsr.org/IJHSR_Vol.9_Issue.2_Feb2019/6.pdf.
- Sanie-Jahromi, F.; Zia, Z.; Afarid, M. A review on the effect of garlic on diabetes, BDNF, and VEGF as a potential treatment for diabetic retinopathy. Chin. Med. 2023, 18, 18–31. [CrossRef]
- Xie, C.; Gao, W.; Li, X.; Luo, S.; Wu, D.; Chye, F.Y. Garlic (Allium sativum L.) polysaccharide ameliorates type 2 diabetes mellitus (T2DM) via the regulation of hepatic glycogen metabolism. NFS J. 2023, 31, 19–27. [CrossRef]
- Najafi, N.; Masoumi, S.J. The Effect of garlic (allium sativum) supplementation in patients with type 2 diabetes mellitus: A systematic review. Int. J. Nutr. Sci. 2018, 3, 7–11.
- Abdullah, H.; Miladiyah, I. Garlic (Allium sativum L.) Efficacy as an adjuvant therapy for type 2 diabetes mellitus: A scoping review. In Proceedings of the 3rd International Conference on Cardiovascular Diseases (ICCvD 2021); Nurdiyanto, H.; Miladiyah, I.; Jamil, N.A., Eds.; Atlantis Press International BV: Paris, France, 2023; pp. 419–434. [CrossRef]
- Choo, T.-M. Nigella sativa tea mitigates type-2 diabetes and edema: A case report. Adv. Tradit. Med. 2023, 23, 1249–1254. [CrossRef]
- Zhang, Y.; Liu, W.; Liu, D.; Zhao, T.; Tian, H. Efficacy of Aloe Vera supplementation on prediabetes and early non-treated diabetic patients: A Systematic review and meta-analysis of randomized controlled trials. Nutrients 2016, 8, 388–397. [CrossRef]
- Harshali, Thakur, P.; Mukherjee, G. Aloe Vera as an Antidiabetic and Wound Healing Agent for Diabetic Patients. JPRI 2021, 256–263. [CrossRef]
- Budiastutik, I.; Subagio, H.W.; Kartasurya, M.I.; Widjanarko, B.; Kartini, A.; Soegiyanto, S.; Suhartono, S.S. The effect of aloe vera on fasting blood glucose levels in pre-diabetes and type 2 diabetes mellitus: A systematic review and meta-analysis. J. Pharm. Pharmacogn. Res. 2022, 10, 737–747. [CrossRef]
- Abo-Youssef, A.M.H.; Messiha, B.A.S. Beneficial effects of aloe vera in treatment of diabetes: comparative in vivo and in vitro studies. Bull. Fac. Pharm. Cairo Univ. 2013, 51, 7–11. [CrossRef]
- Pathomwichaiwat, T.; Jinatongthai, P.; Prommasut, N.; Ampornwong, K.; Rattanavipanon, W.; Nathisuwan, S.; Thakkinstian, A. Effects of turmeric (curcuma longa) supplementation on glucose metabolism in diabetes mellitus and metabolic syndrome: An umbrella review and updated meta-analysis. PLoS ONE 2023, 18, 288997–289017. [CrossRef]
- H. M. Mahbubur Rahman, A.; Iffat Ara Gulshana, M. Taxonomy and medicinal uses on amaranthaceae family of rajshahi, Bangladesh. AEES 2014, 2, 54–59. [CrossRef]
- Aneja, S.; Vats, M.; Aggarwal, S.; Sardana, S. Phytochemistry and hepatoprotective activity of aqueous extract of Amaranthus tricolor Linn. Roots. J. Ayurveda Integr. Med. 2013, 4, 211–217. [CrossRef]
- Rahmatullah, M.; Hosain, M.; Rahman, S.; Rahman, S.; Akter, M.; Rahman, F.; Rehana, F.; Munmun, M.; Kalpana, M. antihyperglycemic and antinociceptive activity evaluation of methanolic extract of whole plant of Amaranthus Tricolor L. (Amaranthaceae). Afr. J. Tradit. Complement. Altern. Med. 2013, 10, 408–411. [CrossRef]
- Rahma, K.; Nurcahyanti, O. Therapeutic effect of red spinach (Amaranthus tricolor L.) extract on pancreatic MDA levels rats (Rattus norvegicus) exposed to MLD-STZ. J. Biomed. Transl. Res. 2021, 7, 129–133. [CrossRef]
- Kaleem, M.; Asif M.Bano, B. Antidiabetic and antioxidant activity of Annona squamosa extract in streptozotocin-induced diabetic rats. Singapore Med. J., 2006, 47, 670–675. https://pubmed.ncbi.nlm.nih.gov/16865205/.
- Ajao, F.O.; Iyedupe, M.O.; Akanmu, O.; Kalejaiye N.O.; Adegoke A.L.; Adeniji, L.A. Anti-oxidative, anti-inflammatory and anti-apoptotic efficacy of Anacardium occidentale leaf extract in diabetic rats. Int J Diabetes Clin Res., 2023, 10, 177–188. https://doi: 10.23937/2377-3634/1410177.
- Jaiswal, Y.S.; Tatke, P.A.; Gabhe, S.Y.; Vaidya, A.B. Antidiabetic activity of extracts of Anacardium occidentale Linn. leaves on n-streptozotocin diabetic rats. J. Tradi. Complement. Med., 2017, 7, 421–427. [CrossRef]
- Ponce-Mora, A.; Gimeno-Mallench, L.; Lavandera, J.L.; Giebelhaus, R.T.; Domenech-Bendaña, A.; Locascio, A.; Gutierrez-Rojas, I.; Sauro, S.; De La Mata, P.; Nam, S.L.; Méril-Mamert, V.; Sylvestre, M.; Harynuk, J.J.; Cebrián-Torrejón, G.; Bejarano, E. Systematic characterization of antioxidant shielding capacity against oxidative stress of aerial part extracts of Anacardium occidentale. Antioxidants, 2025, 14, 935–961. [CrossRef]
- Abdullahi, S. and Olatunji, G.A. Antidiabetic activity of Anacardium occidentale in alloxan – diabetic rats. Jnl Sci Tech., 2010, 30, 35–41. [CrossRef]
- Olatunji, L.A.; Okwusidi, J.I.; and Soladoye, A.O. Antidiabetic effect of Anacardium occidentale.Stem-bark in fructose-diabetic rats. Pharm. Biol., 2005, 43, 589–593. [CrossRef]
- Yang, Y.-C.; Mong, M.-C.; Wu, W.-T.; Wang, Z.-H.; Yin, M.-C. Phytochemical profiles and anti-diabetic benefits of two edible amaranthus species. CyTA J. Food 2020, 18, 94–101. [CrossRef]
- Almalki, G.; Alothman, N.; Mohamed, G.; Akeel, M.; El-Beltagy, A.E.-F.B.; Mahmoud, A.M. Amaranthus tricolor L. leaf extracts improve glucose homeostasis and lipid profile in high-fat diet/streptozotocin-induced diabetic rats. Biomed. Pharmacother. 2022, 153, 113372–113381. [CrossRef]
- Sharma, C.P.; Singh, A.; Prasad, R.K.; Mishra, D.K.; Singh, A.K.; Yadav, S. Antidiabetic and antioxidant activity of Annona squamosa bark using successive solvent extraction method. J. Complement. Herb. Res., 2024, 14, 2004–2013.
- Sharma, A.; Chand, T.; Khardiya, M.; Yadav, K.C.; Mangal, R.; Sharma, A.K. Antidiabetic and antihyperlipidemic activity of Annona squamosa fruit peel in streptozotocin induced diabetic rats. Int. J. Pharm. Sci. Res., 2013, 4, 200–208.
- Gupta, R.K.; Kesari, A.N.; Watal, G.; Murthy, P.S.; Chandra, R.; Maithal, K.; Tandon, V. Hypoglycaemic and antidiabetic effect of aqueous extract of leaves of Annona squamosa (L.) in experimental animals. Curr. Sci., 2005, 88, 1192–1196. http://www.jstor.org/stable/24110293.
- Muszalska, A.; Wiecanowska, J. Berberis vulgaris: A natural source of berberine for addressing contemporary health concerns. Herba Pol. 2024, 70, 13–38. [CrossRef]
- Pang, B.; Zhao, L.-H.; Zhou, Q.; Zhao, T.-Y.; Wang, H.; Gu, C.-J.; Tong, X.-L. Application of berberine on treating type 2 diabetes mellitus. Int. J. Endocrinol. 2015, 1–12. [CrossRef]
- Meliani, N.; Dib, M.E.A.; Allali, H.; Tabti, B. Hypoglycaemic effect of Berberis vulgaris L. in normal and streptozotocin-induced diabetic rats. Asian Pac. J. Trop. Biomed. 2011, 1, 468–471. [CrossRef]
- Shidfar, F.; Ebrahimi, S.S.; Hosseini, S.; Heydari, I.; Shidfar, S.; Hajhassani, G. The effects of Berberis vulgaris fruit extract on serum lipoproteins, apoB, apoA-I, homocysteine, glycemic control and total antioxidant capacity in type 2 diabetic patients. Iran J. Pharm.Res. 2012, 11, 643–652.
- Belwal, T.; Bisht, A.; Devkota, H.P.; Ullah, H.; Khan, H.; Pandey, A.; Bhatt, I.D.; Echeverría, J. Phytopharmacology and Clinical Updates of Berberis Species Against Diabetes and Other Metabolic Diseases. Front. Pharmacol. 2020, 11, 41–67. [CrossRef]
- Munguia-Nolan, J.E.; García-Puga, J.A.; Robles-Zepeda, R.E.; Quintana-Zavala, M.O.; Díaz-Zavala, R.G.; Rendón-Domínguez, I.P. Efectos de Cinnamomum zeylanicum en Niveles Glucémicos en Pacientes con Diabetes Tipo 2: Ensayo Clínico Aleatorizado. Enf. Global 2024, 23, 59–82. [CrossRef]
- Senevirathne, B.S.; Jayasinghe, M.A.; Pavalakumar, D.; Siriwardhana, C.G. Ceylon cinnamon: A versatile ingredient for futuristic diabetes management. J. Future Foods 2022, 2, 125–142. [CrossRef]
- Ranasinghe, P.; Jayawardana, R.; Galappaththy, P.; Constantine, G.R.; De Vas Gunawardana, N.; Katulanda, P. Efficacy and safety of ‘true’ cinnamon (Cinnamomum zeylanicum) as a pharmaceutical agent in diabetes: A Systemic review and meta-analysis. Diabet. Med. 2012, 29, 1480–1492. [CrossRef]
- Shihabudeen, H.M.S.; Priscilla, D.H.; Thirumurugan, K. Cinnamon extract inhibits α-glucosidase activity and dampens postprandial glucose excursion in diabetic rats. Nutr. Metab. 2011, 8, 46–56. [CrossRef]
- Medagama, A.B. The glycaemic outcomes of Cinnamon, a review of the experimental evidence and clinical trials. Nutr. J. 2015, 14, 108–119. [CrossRef]
- Shen, Y.; Fukushima, M.; Ito, Y.; Muraki, E.; Hosono, T.; Seki, T.; Ariga, T. Verification of the antidiabetic effects of Cinnamon (Cinnamomum zeylanicum) using insulin-uncontrolled type 1 diabetic rats and cultured adipocytes. Biosci. Biotechnol. Biochem. 2010, 74, 2418–2425. [CrossRef]
- Yaghmoor, S.S.; Khoja, S.M. Effect of Cinnamon on plasma glucose concentration and the regulation of phosphofructo-1-kinase activity from the liver and small intestine of streptozotocin induced diabetic rats. J. Biol. Sci. 2010, 10, 761–766. [CrossRef]
- Taher, M.; Abdul Majid, F.A.; Sarmidi, M.R. A proanthocyanidin from Cinnamomum zeylanicum stimulates phosphorylation of insulin receptor in 3T3–L1 adipocytes. J. Teknol. 2006, 74, 53–68. [CrossRef]
- Fallah Huseini, H.; Kianbakht, S.; Hajiaghaee, R.; Afkhami-Ardekani, M.; Bonakdaran, A.; Dabaghian, F. Aloe Vera leaf gel in treatment of advanced type 2 diabetes mellitus needing insulin therapy: A randomized double-blind placebo-controlled clinical trial. J. Med. Plants 2012, 11, 23–28.
- Rivera-Mancía, S.; Trujillo, J.; Chaverri, J.P. Utility of curcumin for the treatment of diabetes mellitus: evidence from preclinical and clinical studies. J. Nutr. Intermediary Metab. 2018, 14, 29–41. [CrossRef]
- Marton, L.T.; Pescinini-e-Salzedas, L.M.; Camargo, M.E.C.; Barbalho, S.M.; Haber, J.F.D.S.; Sinatora, R.V.; Detregiachi, C.R.P.; Girio, R.J.S.; Buchaim, D.V.; Cincotto Dos Santos Bueno, P. The effects of curcumin on diabetes mellitus: A systematic review. Front. Endocrinol. 2021, 12, 669448–669459. [CrossRef]
- Abbas, W.; Khan, R.A.; Baig, M.T.; Shaikh, S.A.; Kumar, A. Role of Curcuma Longa in Type 2 Diabetes and Its Associated Complications. JPRI 2021, 33, 369–376. [CrossRef]
- Lu, W.; Shahidi, F.K.; Khorsandi, K.; Hossienzadeh, R.; Asma, G.; Balick, V. An update on molecular mechanisms of curcumin effect on diabetes. J. Food Biomech. 2022, 46, 653–669. [CrossRef]
- Zhang, D.; Fu, M.; Gao, S-H.; Liu, J-L. Curcumin and diabetes: A systematic review. Evid. Based Complement. Altern. Med. 2013, 1, 636053–636068. [CrossRef]
- Chuengsamarn, S.; Rattanamongkolgul, S.; Luechapudiporn, R.; Phisalaphong, C.; Jirawatnotai, S. Curcumin extract for prevention of type 2 diabetes. Diabetes Care 2012, 35, 2121–2127. [CrossRef]
- Kanetkar, P.; Singhal, R.; Kamat, M. Gymnema sylvestre: A memoir. J. Clin. Biochem. Nutr. 2007, 41, 77–81. [CrossRef]
- Muzaffar, H.; Qamar, I.; Bashir, M.; Jabeen, F.; Irfan, S.; Anwar, H. Gymnema sylvestre Supplementation Restores Normoglycemia, Corrects Dyslipidemia, and Transcriptionally Modulates Pancreatic and Hepatic Gene Expression in Alloxan-Induced Hyperglycemic Rats. Metabolites 2023, 13, 516–531. [CrossRef]
- Yadav, D.; Kwak, M.; Jin, J.-O. Clinical applications of Gymnema sylvestre against type 2 diabetes mellitus and its associated abnormalities. Prog. Nutr. 2019, 21, 258–269. [CrossRef]
- Gaonkar, V.P.; Hullatti, K. Indian Traditional medicinal plants as a source of potent Anti-diabetic agents: A Review. J. Diabetes Metab. Disord. 2020, 19, 1895–1908. [CrossRef]
- Kashif, M.; Nasir, A.; Gulzaman; Rafique, M.K.; Abbas, M.; Ur Rehman, A.; Riaz, M.; Rasool, G.; Mtewa, A.G. Unlocking the anti-diabetic potential of Gymnema syvestre, Trigonella foenum-graecum, and their combination thereof: An in vivo evaluation. Food Sci. Nutr. 2023, 11, 7664–7672. [CrossRef]
- Huyen, V.T.T.; Phan, D.V.; Thang, P.; Ky, P.T.; Hoa, N.K.; Ostenson, C.G. Antidiabetic effects of add-on Gynostemma pentaphyllum extract therapy with sulfonylureas in type 2 diabetic patients. Evid. Based Complement. Altern. Med. 2012, 1–7. [CrossRef]
- Li, X.; Liu, L.; Wei, S. Gynostemma pentaphyllum: A review on its traditional uses, phytochemistry and pharmacology. J. Funct. Foods 2025, 124, 106651–106674. [CrossRef]
- Song, M.; Tan, D.; Li, B.; Wang, Y.; Shi, L. Gypenoside ameliorates insulin resistance and hyperglycemia via the AMPK-mediated signaling pathways in the liver of type 2 diabetes mellitus mice. Food Sci. Hum. Wellness 2022, 11, 1347–1354. [CrossRef]
- Huyen, V.T.T.; Phan, D.V.; Thang, P.; Hoa, N.K.; Östenson, C.G. Gynostemma pentaphyllum tea improves insulin sensitivity in type 2 diabetic patients. J. Nutr. Metab. 2013, 1–7. [CrossRef]
- Xie, J.-B.; Xie, P.; Guo, M.; Li, F.-F.; Xiao, M.-Y.; Qi, Y.-S.; Pei, W.-J.; Luo, H.-T.; Gu, Y.-L.; Piao, X.-L. Protective effect of heat-processed Gynostemma pentaphyllum on high fat diet-induced glucose metabolic disorders mice. Front. Pharmacol. 2023, 14, 1215150–1215164. [CrossRef]
- Joseph, B.; Jini, D. Antidiabetic effects of Momordica charantia (bitter melon) and its medicinal potency. Asian Pac. J. Trop. Dis. 2013, 3, 93–102. [CrossRef]
- Leung, L.; Birtwhistle, R.; Kotecha, J.; Hannah, S.; Cuthbertson, S. Anti-diabetic and hypoglycaemic effects of Momordica charantia (Bitter Melon): A mini review. Br. J. Nutr. 2009, 102, 1703–1708. [CrossRef]
- Richter, E.; Geetha, T.; Burnett, D.; Broderick, T.L.; Babu, J.R. The effects of Momordica charantia on Type 2 Diabetes Mellitus and Alzheimer’s Disease. Int. J. Mol. Sci. 2023, 24, 4643. [CrossRef]
- Garau, C.; Cummings, E.; Phoenix, D.A.; Singh, J. Beneficial effect and mechanism of action of Momordica charantia in the treatment of diabetes mellitus: A mini review. Int. J. Diabetes Metab. 2003, 11, 46–55. [CrossRef]
- Oyelere, S.F.; Ajayi, O.H.; Ayoade, T.E.; Santana Pereira, G.B.; Dayo Owoyemi, B.C.; Ilesanmi, A.O.; Akinyemi, O.A. A detailed review on the phytochemical profiles and anti-Diabetic mechanisms of Momordica charantia. Heliyon 2022, 8, 9253–9263 . [CrossRef]
- Mashayekhi-Sardoo, H.; Sepahi, S.; Baradaran Rahimi, V.; Askari, V.R. Application of Nigella sativa as a functional food in diabetes and related complications: Insights on molecular, cellular, and metabolic effects. J. Funct. Foods 2024, 122, 106518–106550. [CrossRef]
- Shaukat, A.; Zaidi, A.; Anwar, H.; Kizilbash, N. Mechanism of the antidiabetic action of Nigella sativa and Thymoquinone: a review. Front. Nutr. 2023, 10, 1126272–1126299. [CrossRef]
- Maideen, N.M.P. Antidiabetic activity of nigella sativa (black seeds) and its active constituent (thymoquinone): A review of human and experimental animal studies. Chonnam Med. J. 2021, 57, 169–176. [CrossRef]
- Hamdan, A.; Haji Idrus, R.; Mokhtar, M.H. Effects of nigella sativa on type-2 diabetes mellitus: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 4911–4922. [CrossRef]
- El-Aarag, B.; Hussein, W.; Ibrahim, W.; Zahran, M. Thymoquinone improves anti-diabetic activity of metformin in streptozotocin-induced diabetic male rats. J. Diabetes Metab. 2017, 8, 1000780-1000787. [CrossRef]
- Afaf Jamal Ali Hmza, E.; Omar, A.; Adnan, A.; Osman, M.T. Nigella sativa oil has significant repairing ability of damaged pancreatic tissue occurs in induced type 1 diabetes mellitus. Glob. J. Pharmacol. 2013, 7, 14–19.
- Choo, T.-M. Nigella sativa tea mitigates type-2 diabetes and edema: A case report. Adv. Tradit. Med. 2023, 23, 1249–1254. [CrossRef]
- Hannan, J.M.A.; Marenah, L.; Ali, L.; Rokeya, B.; Flatt, P.R.; Abdel-Wahab, Y.H.A. Ocimum sanctum leaf extracts stimulate insulin secretion from perfused pancreas, isolated islets and clonal pancreatic β-Cells. J. Endocrinol. 2006, 189, 127–136. [CrossRef]
- Abhilash Rao, S.; Vijay, Y.; Deepthi, T.; Sri Lakshmi, C.; Vibha Rani, S.; Swetha Rani, B.; Bhuvaneswara Reddy, Y.; Ram Swaroop, P.; Sai Laxmi, V.; Nikhil Chakravarthy, K.; Arun, P. Anti-diabetic effect of ethanolic extract of leaves of ocimum sanctum in alloxan induced diabetes in rats. Int. J. Basic Clin. Pharmacol. 2013, 2, 613. S, A., Y, V., T, D., Ch, S., Rani, V., Rani, S., Y, B., P, R., V, S., K, N., & P, A. (2013). Anti diabetic effect of ethanolic extract of leaves of Ocimum sanctum in alloxan induced diabetes in rats. International Journal of Basic & Clinical Pharmacology, 2(5), 613. [CrossRef]
- Suanarunsawat, T.; Anantasomboon, G.; Piewbang, C. Anti-diabetic and anti-oxidative activity of fixed oil extracted from Ocimum sanctum L. leaves in diabetic rats. Exp. Ther. Med. 2016, 11, 832–840. [CrossRef]
- Cheurfa, M.; Achouche, M.; Azouzi, A.; Abdalbasit, M.A. Antioxidant and anti-diabetic activity of pomegranate (Punica granatum L.) leaves extracts. Foods Raw Maters, 2020, 8, 329–336. [CrossRef]
- Gharib, E. Kouhsari, S.M. Study of the antidiabetic activity of Punica granatum L. fruits aqueous extract on the alloxan-diabetic wistar rats. Iran. J. Pharm. Res., 2019, 18, 358–368. https://pmc.ncbi.nlm.nih.gov/articles/PMC6487419/.
- Tang, D.; Liu, L.; Ajiakber, D.; Ye, J.; Xu, J.; Xin, X.; Aisa, H.A. Anti-diabetic Effect of Punica granatum Flower Polyphenols Extract in Type 2 Diabetic Rats: Activation of Akt/GSK-3β and Inhibition of IRE1α-XBP1 Pathways. Front. Endocrinol. 2018, 9, 586–596. [CrossRef]
- Mabrouk Gabr, N. Effects of pomegranate (Punica granatum L.) fresh juice and peel extract on diabetic male albino rats. AMJ., 2017, 46, 965–980. [CrossRef]
- Haxhiraj, M.; White, K.; Terry, C. The role of fenugreek in the management of type 2 diabetes. Int. J. Mol. Sci. 2024, 25, 6987–6997. [CrossRef]
- Laila, O.; Murtaza, I.; Muzamil, S.; Imtiyaz Ali, S.; Abid Ali, S.; Ahamad Paray, B.; Gulnaz, A.; Vladulescu, C.; Mansoor, S. Enhancement of nutraceutical and anti-diabetic potential of fenugreek (Trigonella foenum-graecum). Sprouts with natural elicitors. Saudi Pharm. J. 2023, 31, 1–13. [CrossRef]
- Baset, M.E.; Ali, T.I.; Elshamy, H.; El Sadek, A.M.; Sami, D.; Badawy, M.; Abou-Zekry, S.; Heiba, H.; Saadeldin, M.; Abdellatif, A. Anti-Diabetic Effects of Fenugreek (Trigonella foenum-graecum): A Comparison between Oral and Intraperitoneal Administration—An Animal Study. Int. J. Funct. Nutr. 2020, 1, 2–10. [CrossRef]
- Ota, A.; Ulrih, N.P. An overview of herbal products and secondary metabolites used for management of type two diabetes. Front. Pharmacol. 2017, 8, 436–449. [CrossRef]
- Kumar, A.; Aswal, S.; Chauhan, A.; Semwal, R.B.; Kumar, A.; Semwal, D.K. Ethnomedicinal investigation of medicinal plants of Chakrata region (Uttarakhand) used in the traditional medicine for diabetes by Jaunsari tribe. Nat. Prod. Bioprospect. 2019, 9, 175–200. [CrossRef]
- Sarker, D.K.; Ray, P.; Dutta, A.K.; Rouf, R.; Uddin, S.J. Antidiabetic potential of fenugreek (Trigonella foenum-graecum): A magic herb for diabetes mellitus. Food Sci. Nutr. 2024, 12, 7108–7136. [CrossRef]
Figure 1.
An illustration showcasing insulin binding to its receptor activates IRS1 that leads to subsequent Akt pathway activation. Activated Akt initiates three major cascades: 1- Glycogen synthase kinase activation, 2- MAPK/ERK activation, 3- GLUT-4 translocation. Moreover, ROS and AGE inhibit IRS1 activation. and disrupts insulin signaling. Image was created using BioRender.com.
Figure 1.
An illustration showcasing insulin binding to its receptor activates IRS1 that leads to subsequent Akt pathway activation. Activated Akt initiates three major cascades: 1- Glycogen synthase kinase activation, 2- MAPK/ERK activation, 3- GLUT-4 translocation. Moreover, ROS and AGE inhibit IRS1 activation. and disrupts insulin signaling. Image was created using BioRender.com.
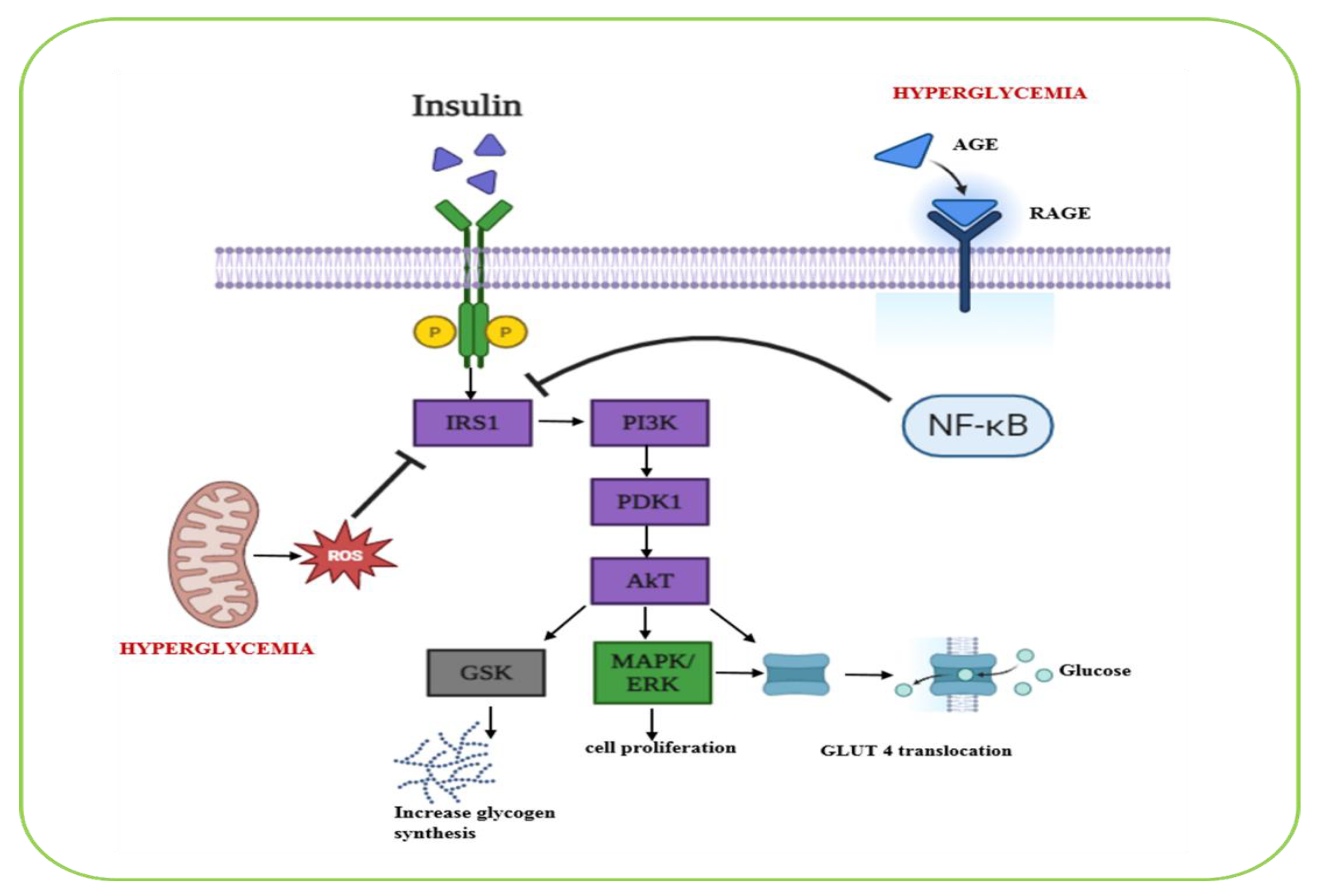
Figure 2.
A graphical illustration showcasing the effect of herbal medicine update on various organs during treatment against diabetes. Image was created using BioRender.com.
Figure 2.
A graphical illustration showcasing the effect of herbal medicine update on various organs during treatment against diabetes. Image was created using BioRender.com.
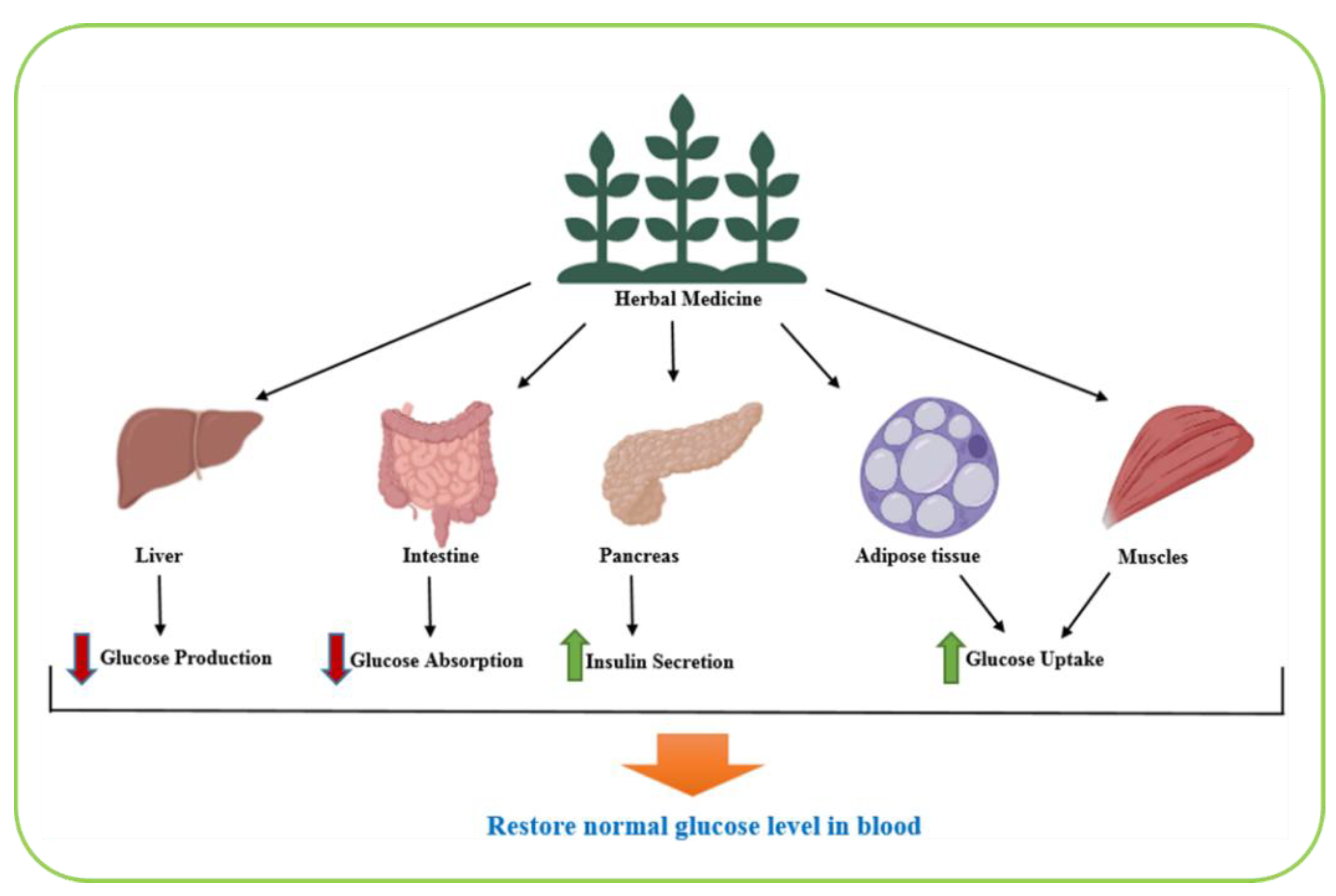
Figure 3.
A graphical representation of the molecular mechanism of cinnamon inhibiting α-amylase, α-glucosidase and plasma glucose and stimulating plasma insulin, glycogen synthesis, glucose metabolism and insulin. receptor phosphorylation. Image was created using BioRender.com.
Figure 3.
A graphical representation of the molecular mechanism of cinnamon inhibiting α-amylase, α-glucosidase and plasma glucose and stimulating plasma insulin, glycogen synthesis, glucose metabolism and insulin. receptor phosphorylation. Image was created using BioRender.com.
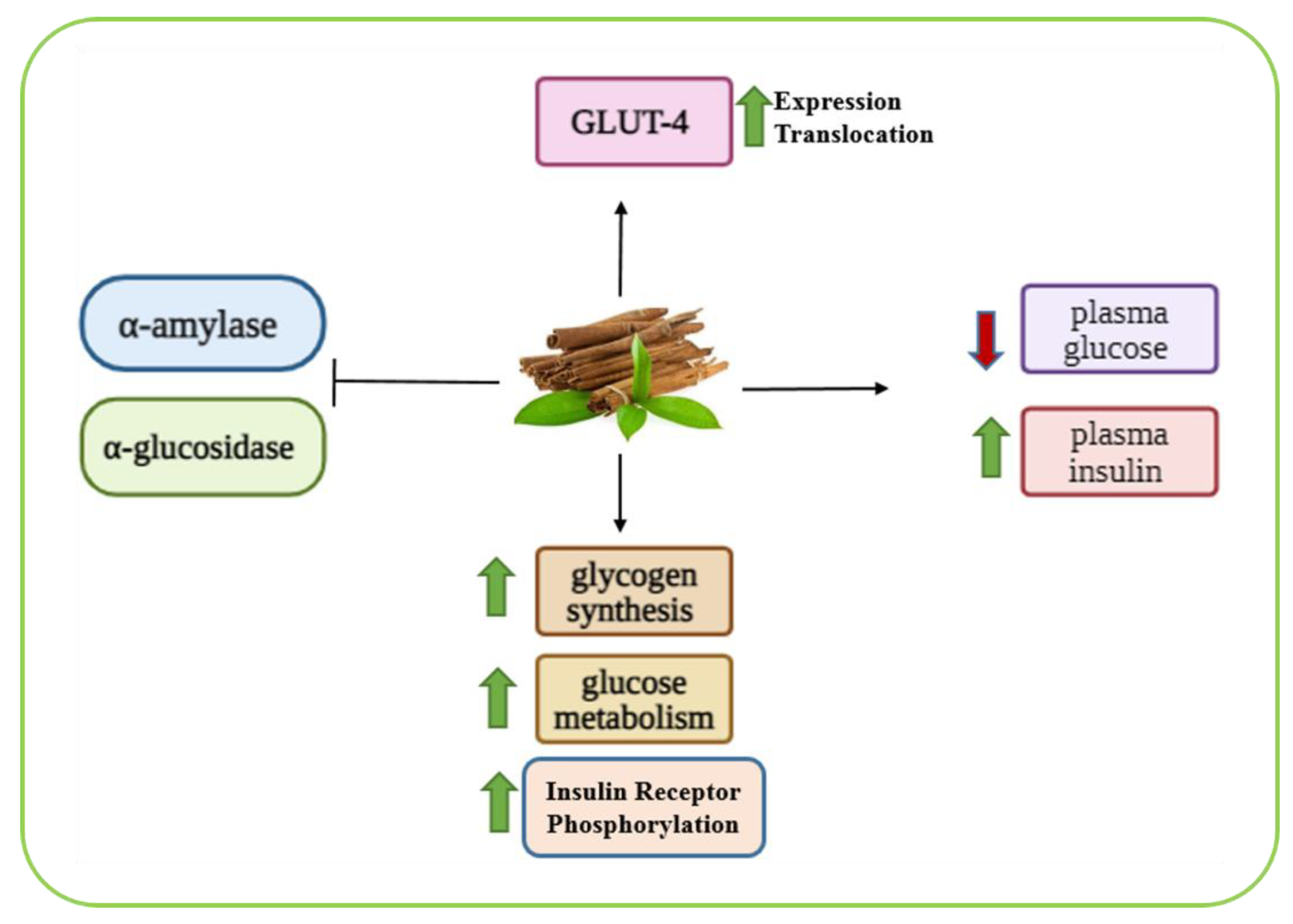
Figure 4.
A graphical representation of a potential (and probable) molecular mechanism associated to the anti-diabetic effect of the gymnema sylvestre plant. Image was created using BioRender.com.
Figure 4.
A graphical representation of a potential (and probable) molecular mechanism associated to the anti-diabetic effect of the gymnema sylvestre plant. Image was created using BioRender.com.
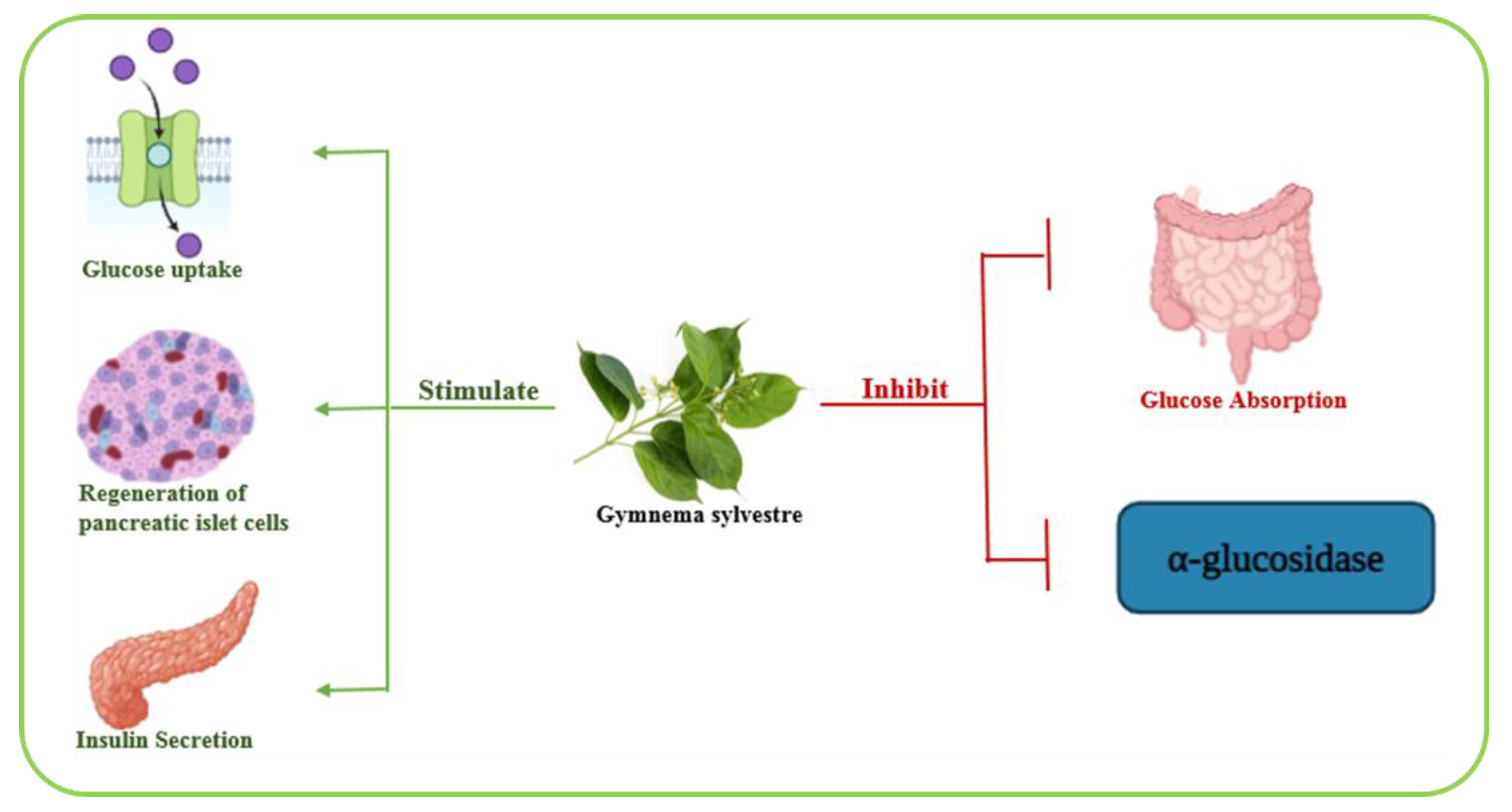
Figure 5.
A schematic illustration summarizing main GPS biological activities. Image was created using BioRender.com.
Figure 5.
A schematic illustration summarizing main GPS biological activities. Image was created using BioRender.com.
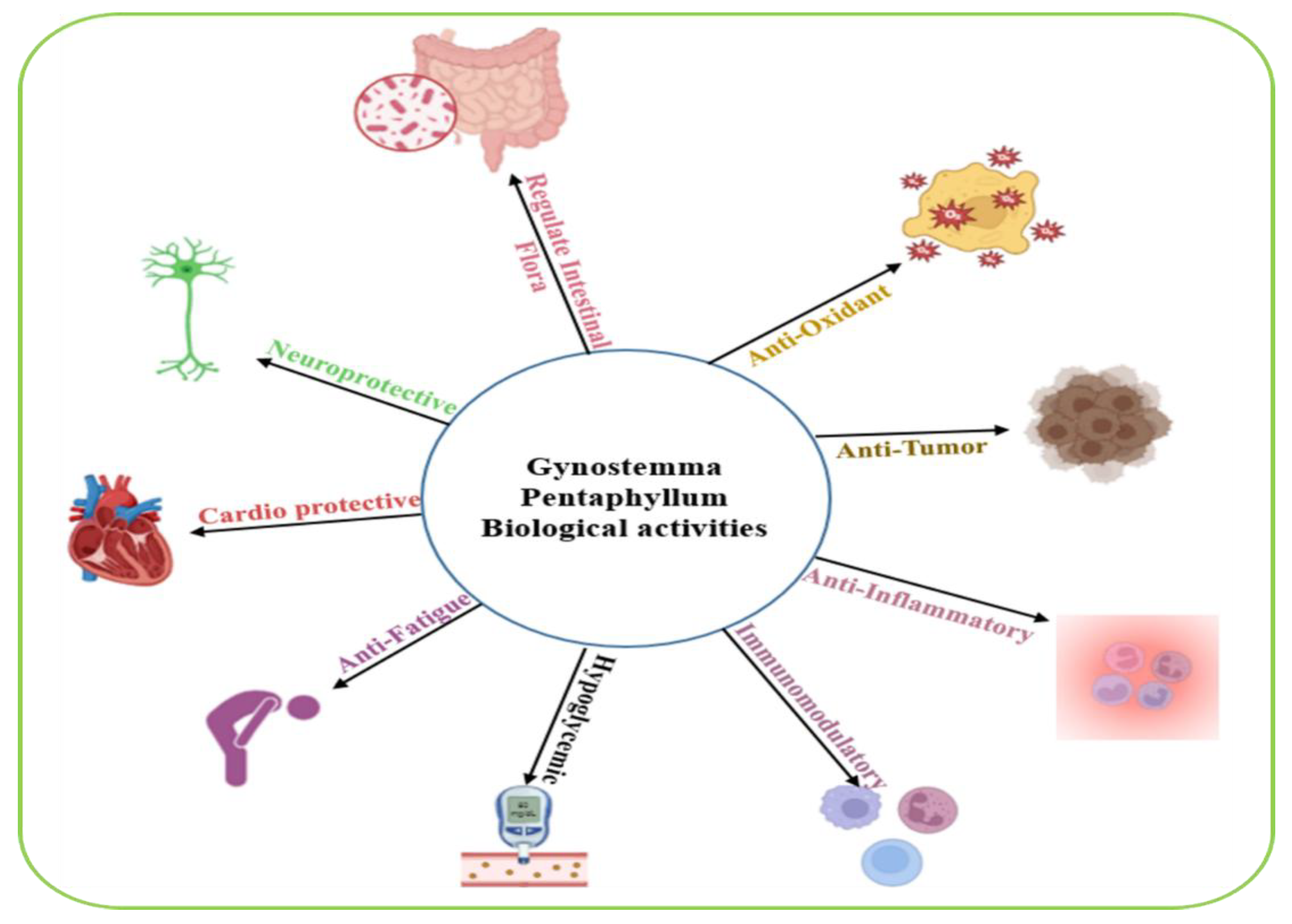
Figure 6.
A graphical representation of the biological effects of Momordica charantia on glucose metabolism and insulin regulation. Image was created using BioRender.com.
Figure 6.
A graphical representation of the biological effects of Momordica charantia on glucose metabolism and insulin regulation. Image was created using BioRender.com.
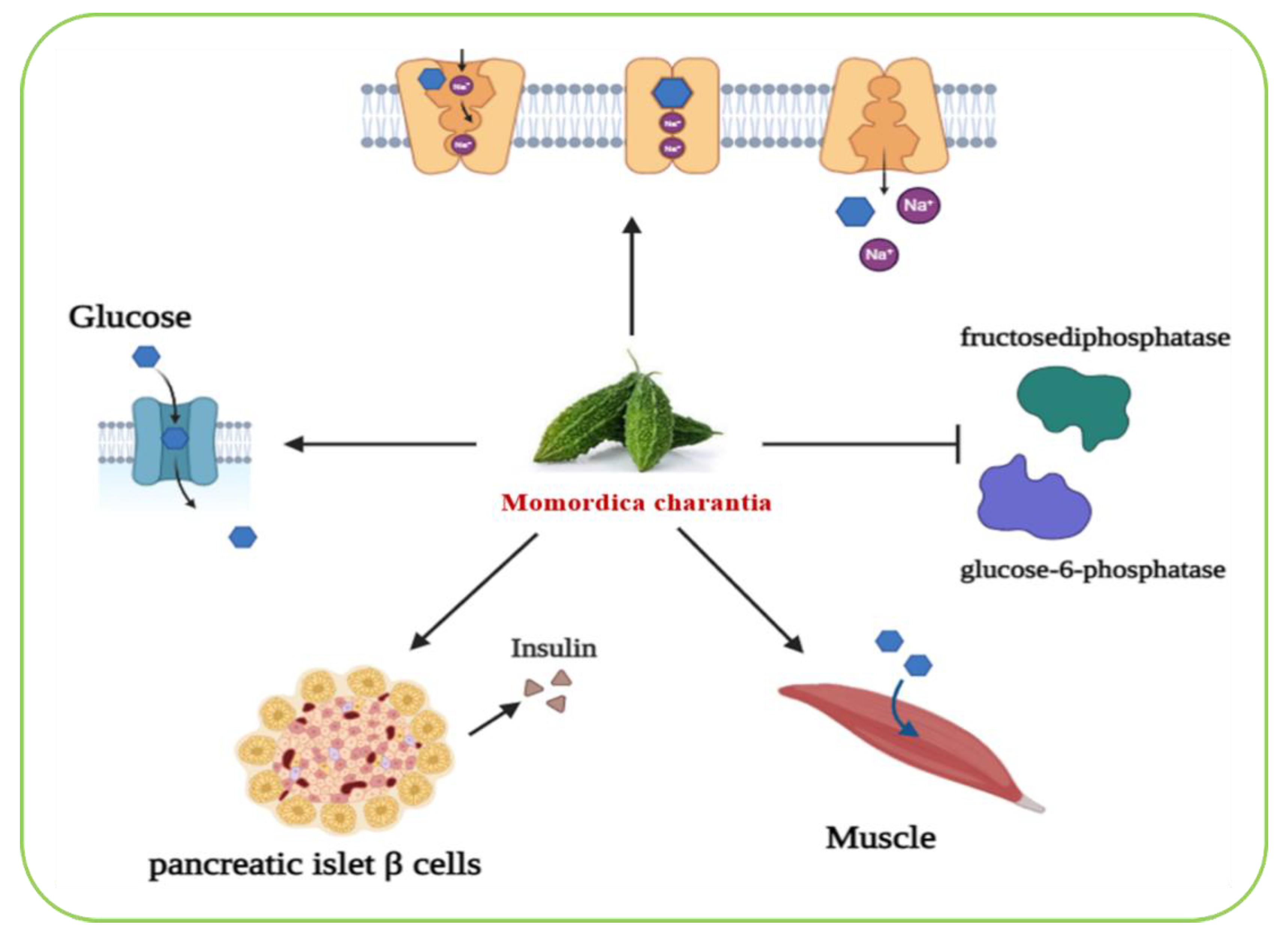
Figure 7.
A graphical illustration of antidiabetic actional mode of the nigella sativa plant. Image was created using BioRender.com.
Figure 7.
A graphical illustration of antidiabetic actional mode of the nigella sativa plant. Image was created using BioRender.com.
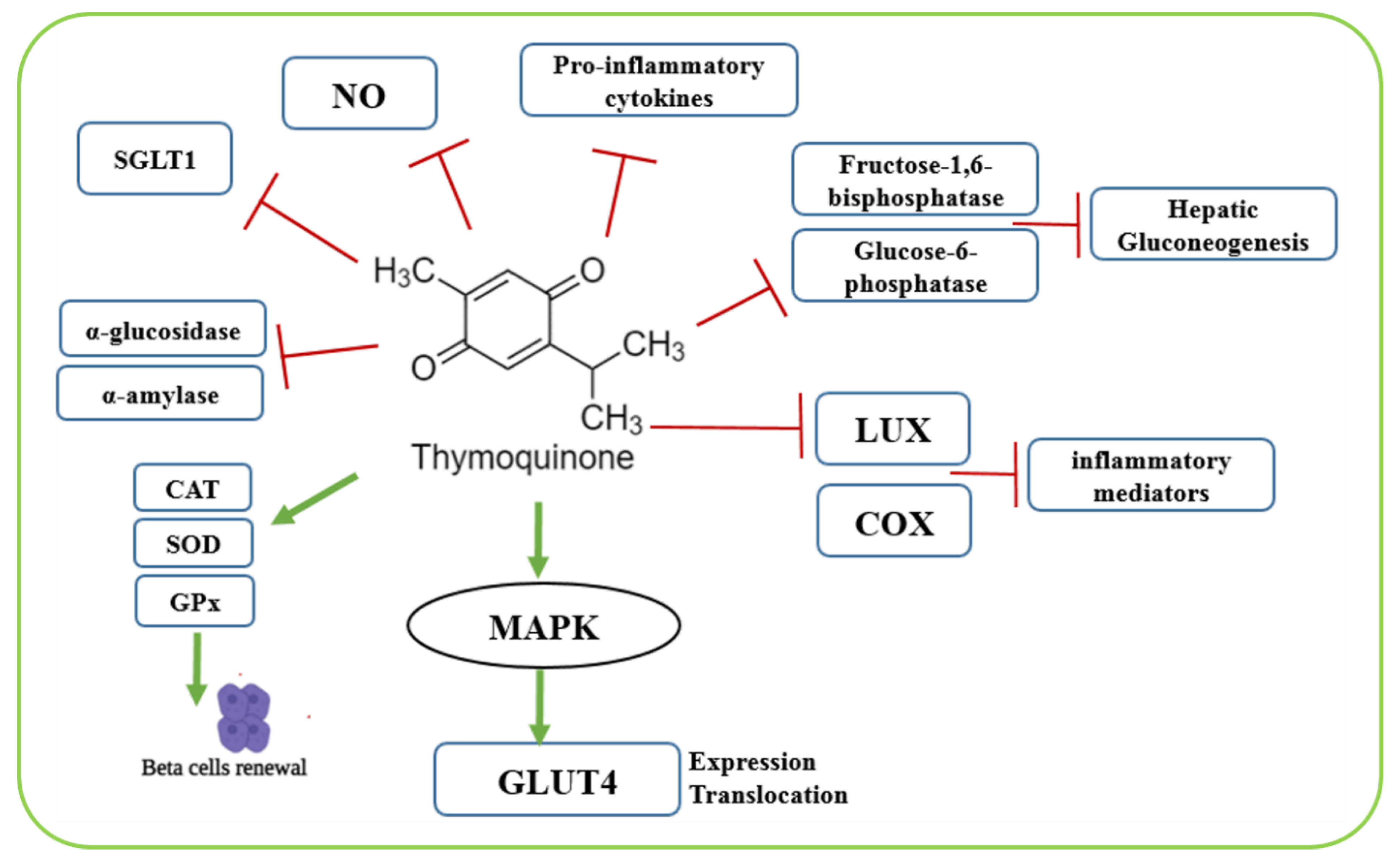
Figure 8.
A schematic representation of the hypoglycemic effects of Trigonella foenum-graecum (also referred to as fenugreek). Image was created using BioRender.com.
Figure 8.
A schematic representation of the hypoglycemic effects of Trigonella foenum-graecum (also referred to as fenugreek). Image was created using BioRender.com.
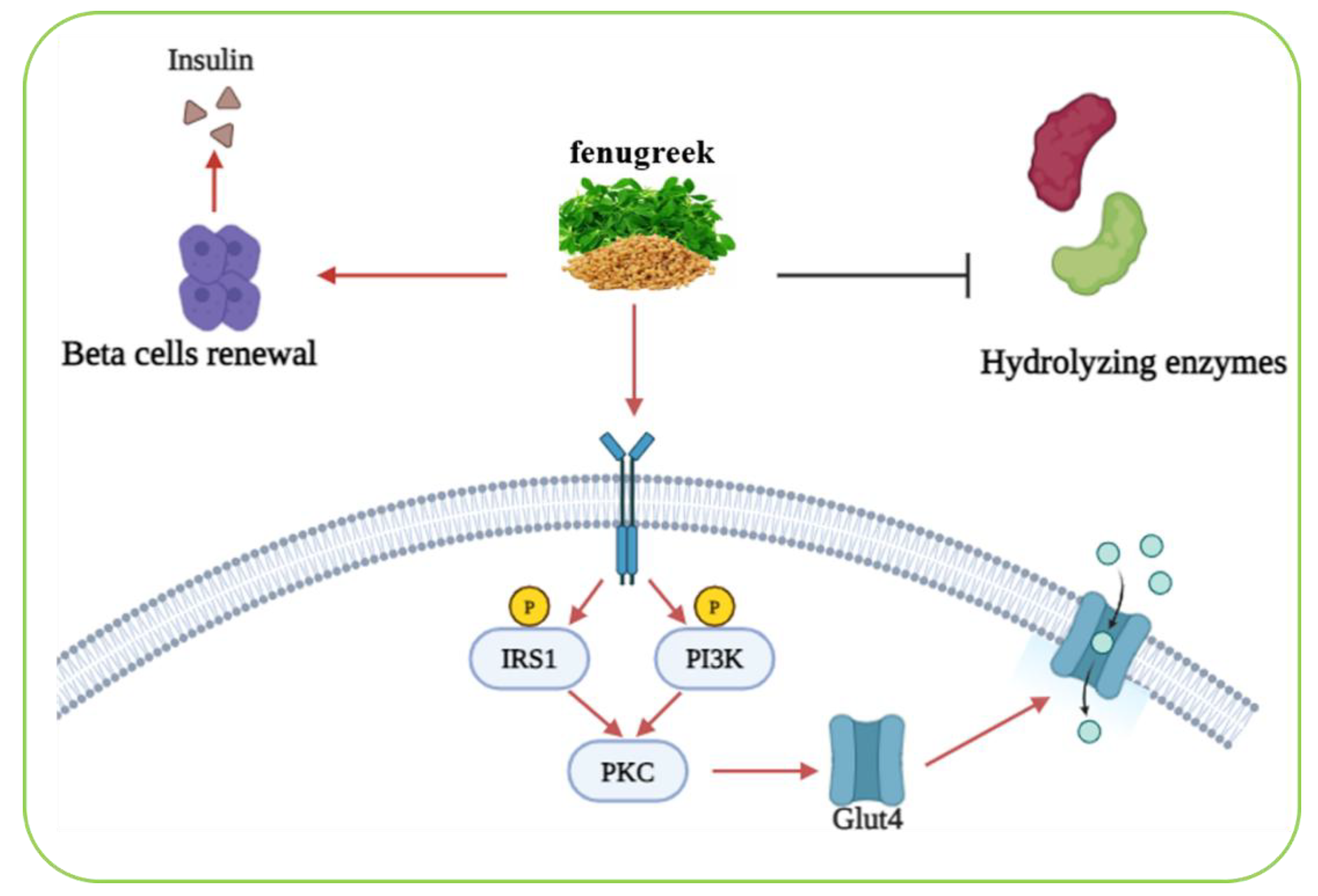

Table 1.
A comprehensive summary of various plants known for their antidiabetic properties including the parts usually used for treatment procedures along with their respective mode of action and their corresponding therapeutic relevance.
Table 1.
A comprehensive summary of various plants known for their antidiabetic properties including the parts usually used for treatment procedures along with their respective mode of action and their corresponding therapeutic relevance.
| Plant name | Family | Used plant parts | Mode of action | Ref. |
|---|---|---|---|---|
| Achyranthes aspera | Amaranthaceae | Seed, Leaf | ● Inhibits the activities of glucosidase enzymes Reduces oxidative damage and increases the expression of the pancreatic insulin protein |
[26,28] |
| Allium sativum |
Amaryllidaceae | Whole plant | ● Inhibits the enzyme alpha glucosidase Increases insulin sensitivity |
[32,33] |
| Aloe vera | Liliaceal | Whole plant | ● Inhibits glycation pathway Affects insulin secretion rate |
[35,37] |
| Amaranthus tricolor | Amaranthaceae | Leaf and stem | Prevents oxidative stress in cells Stimulates anti-α-amylase, anti-α-glucosidase properties |
[42,43] |
| Anacardium occidentale | Anacardiaceous | Leave and stem | ● Improves hepatic and renal functions Enhances β-cell functions |
[49] |
| Annona squamosa | Annonaceae | Roots, seeds, leaves and fruits | ● Stimulates glucose uptake and the release of the insulin hormone | [53] |
| Berberis vulgaris | Berberidaceae | Fruit | ● Inhibits fructose-induced insulin resistance Downregulates the expression of aldose reductase Improves the sensitivity and the secretion of insulin Inhibits the release of glucagon Stimulates the proliferation of pancreatic β-cells and that of the GLP-1 hormone secretion which plays a role in insulin secretion Upregulates the expression of insulin receptor proteins Inhibits key enzymes contribution to glucose regulation |
[55,56,58,59] |
| Cinnamomum zeylanicum | Lauraceae | Whole plant | ● Inhibits pancreatic α-amylase and α-glucosidase by stimulating the synthesis of glycogen and the metabolism of glucose Enhances GLUT-4 production and translocation |
[62,63,65] |
| Curcuma longa |
Zingiberaceae | Root | ● Improves the overall functions of b-cells Reduces the levels of metabolic parameters |
[73,74] |
| Gymnema sylvestre | Asclepiadaceae | leaves | ● Modulates several gene expressions, contributing to diabetes control | [76] |
| Gynostemma pentaphylium |
Cucurbitaceae | ● | ● Improves insulin sensitivity Increases the expression of GLUT4 Decreases the histological liver damage |
[83,84] |
| Momordica charantia |
Cucurbitaceae | Fruit | ● Controls glucose transportation Reduces gluconeogenic enzymes (such as glucose-6-phosphatase and fructosebiphosphatase) Increase the levels of intestinal Na+/glucose co-transporters, protectors of pancreatic islet β cells |
[87,88,89] |
| Nigella sativa |
Ranunculaceae | Whole plant | ● Blocks α-glucosidase and α-amylase digestive enzymes Reduces gluconeogenesis in the liver Inhibits the intestinal glucose transporters Increases the secretion of antioxidant enzymes Stimulates pancreatic-cell proliferation |
[90,91,92,93] |
| Ocimum sanctum | Lamiaceae | Leaves | ● Increases the intra cellular calcium concentration of beta islet cells | [98] |
| Punica granatum |
Lythraceae | Leave and flower | ● Increases the secretion of pancreatic β-cells Stimulates the mRNAs expression of IRS-1 and Akt genes Increases the activity of CAT enzymes and improves the health of pancreatic islets of Langerhans |
[101,103] |
| Trigonella foenum-graecum | Fabaceae | Seeds and leaves | Overexpresses of GLUT2 mRNA Renews β-cell and promotes insulin secretion stimulation Inhibits lipid-and carbohydrate hydrolyzing enzymes Stimulates translocation of GLUT4 to cell membrane |
[106,107,108,109] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



