
Submitted:
05 January 2026
Posted:
08 January 2026
You are already at the latest version
Abstract
Older adults with cancer face disproportionately high rates of severe treatment-related toxicities, yet current prediction tools rarely incorporate biomarkers that capture physiological resilience. The hypothalamic–pituitary–adrenal (HPA) axis—central to stress adaptation, immune regulation, and tissue repair—undergoes pronounced age-related alterations, including elevated basal cortisol, reduced dehydroepiandrosterone (DHEA) and its sulphate form DHEAS, and an increased cortisol:DHEA(S) ratio. These changes may impair immune function, delay recovery, and exacerbate vulnerability to treatment toxicity. This narrative review synthesizes mechanistic and clinical evidence linking HPA-axis dysregulation to treatment tolerance in geriatric oncology. Common patterns include blunted diurnal cortisol slopes, elevated evening cortisol, and low DHEA(S), which are associated with fatigue, functional decline, and reduced survival across cancer types. However, their predictive value for acute treatment toxicities remains underexplored due to methodological heterogeneity, lack of age-specific reference ranges, and absence from existing geriatric toxicity models. This review proposes a translational roadmap that prioritizes (1) standardization of salivary cortisol/DHEA(S) protocols; (2) prospective, age-stratified validation studies using standardized toxicity endpoints; (3) interventional testing of behavioral or pharmacological strategies to modulate HPA function; and (4) integration into oncology workflows and electronic decision-support tools. Incorporating endocrine biomarkers into risk prediction could refine treatment stratification, enable targeted supportive care, and ultimately improve outcomes for older patients with cancer.
Keywords:
cortisol
; hydrocortisone
; dehydroepiandrosterone
; geroscience
; chemotherapy toxicity
; drug-related side effects and adverse reactions
; endocrine system
; hypothalamo-hypophyseal System
; HPA-axis
; aged
; 80 and over
; older adults
Introduction
Cancer predominantly affects older adults, from fewer than 26 cases per 100,000 people in age groups under age 20, to about 350 per 100,000 at ages 45–49, and more than 1,000 per 100,000 people in age groups 60 years and older [1]. Older adults face a disproportionate risk of treatment-related toxicities, exacerbated by age-related physiological changes[2,3,4]. Despite this vulnerability, most current oncology risk stratification tools, such as the Cancer and Aging Research Group (CARG) score [5] and the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH)[6], largely omit endocrine parameters[5,7,8,9], particularly those involving stress-response systems such as the hypothalamic-pituitary-adrenal (HPA) axis. These tools remain the standard for geriatric toxicity prediction. Conceptually, endocrine parameters such as HPA-axis markers might enhance risk stratification in older adults once their predictive value has been robustly established.
The HPA axis is a central regulator of systemic stress responses, inflammation, and immune function[10,11,12,13]. Cortisol, its principal effector hormone, coordinates adaptive responses to physiological and psychological stressors[14,15,16]. Cortisol dysregulation is frequently observed in cancer populations, characterized by elevated basal secretion, blunted diurnal slopes, and impaired reactivity to acute stress[17,18,19,20,21,22,23,24,25,26]. These alterations are found across tumor types and treatment modalities and have been associated with fatigue, cognitive impairment, and reduced physical functioning[17]. However, it remains unclear whether cortisol dysregulation actively contributes to poor outcomes or merely reflects disease burden.
Older adults exhibit specific changes in HPA-axis physiology that may amplify these disruptions[27,28,29]. Age-related endocrine changes include elevated basal cortisol secretion, impaired negative feedback sensitivity[30,31], and a decline in dehydroepiandrosterone (DHEA) (also a steroid hormone produced in the adrenals, often measured in its active sulphated form DHEAS), which counterbalances many of the adverse effects of cortisol[32,33]. These alterations result in an elevated cortisol:DHEA(S) ratio and may compromise immune regulation[34], physical function[35], and treatment tolerance in the context of cancer[36,37]. This convergence of age-related endocrine aging and cancer-related stress burden may amplify physiological risk in this population.
To date, although some studies exist [38,39,40] and the field of biomarkers for toxicity prediction is developing[41,42], no large-scale prospective studies have evaluated whether pre-treatment HPA axis dysregulation features (e.g., diurnal slope, evening elevation, cortisol:DHEA(S) ratio) predict acute treatment-related toxicities—such as Common Terminology Criteria for Adverse Events (CTCAE) grade ≥3 adverse events, dose reductions, or unplanned hospitalizations—in older patients with cancer. While observational studies link cortisol abnormalities to outcomes like survival and fatigue, their predictive value for treatment-specific complications remains uncharacterized.
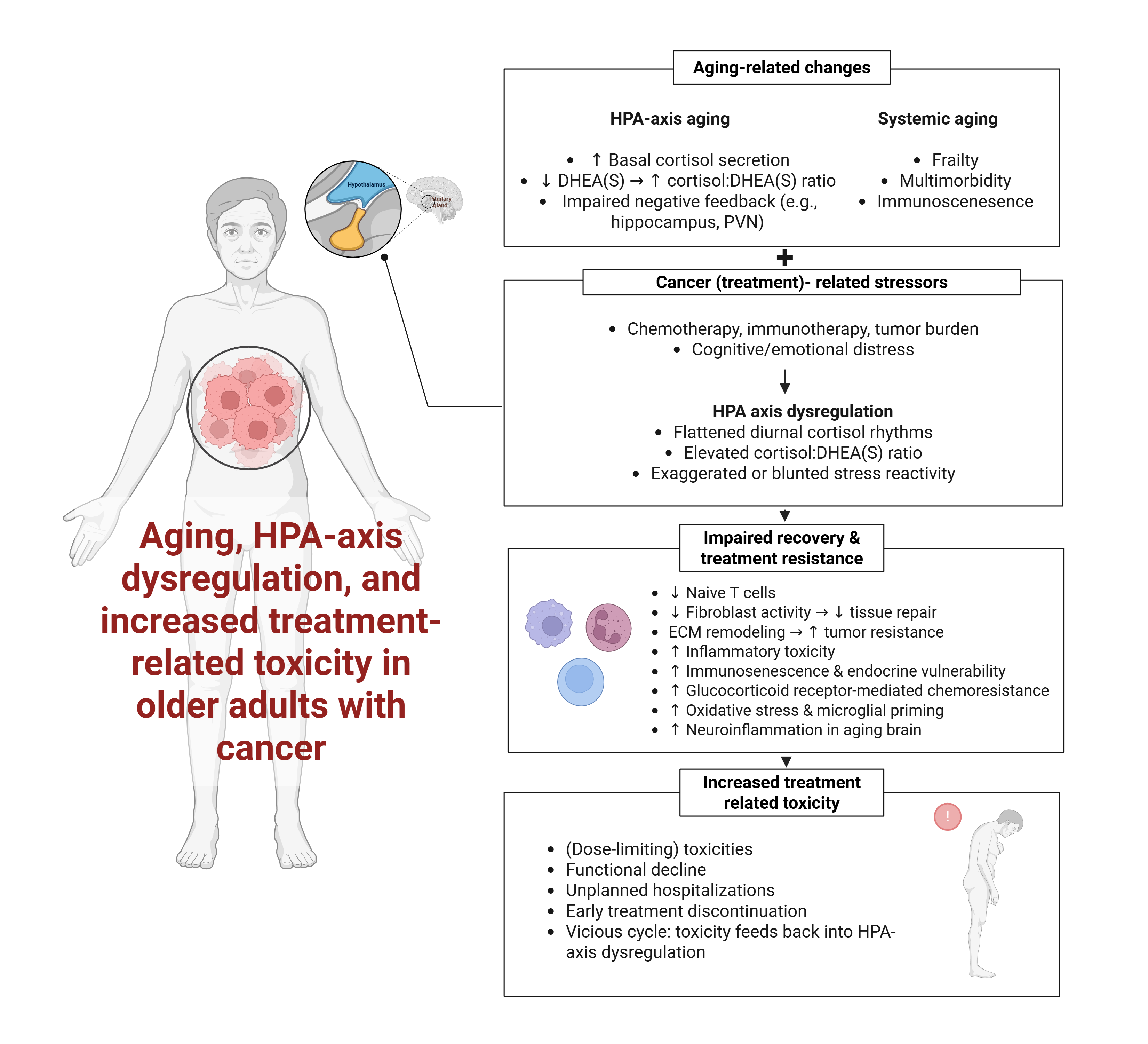
This review argues that HPA-axis dysregulation is a potential biomarker of impaired physiological resilience in geriatric oncology and not merely an incidental correlate of disease burden. It further proposes that cortisol and DHEA(S) may serve as prognostic, predictive, and monitoring biomarkers—each playing a distinct role in improving treatment decision-making and supportive care strategies. Figure 1 illustrates the hypothesized convergence of aging-related endocrine decline and cancer-related stressors in disrupting HPA function and increasing toxicity risk.
This review hypothesizes that age-related HPA-axis dysregulation is a clinically meaningful predictor of treatment-related toxicity in older adults with cancer, and that standardized biomarker assessment could enhance risk stratification in geriatric oncology. To this end, this review aims to: (1) examine how aging and cancer interact to disrupt cortisol and DHEA(S) dynamics; (2) differentiate the prognostic, predictive, and monitoring potential of these biomarkers; (3) map mechanistic pathways linking HPA dysregulation to treatment toxicity phenotypes; (4) critically appraise methodological heterogeneity in biomarker assessment; (5) propose a translational roadmap for integrating HPA-axis biomarkers into geriatric oncology risk models.
HPA-axis dysregulation in patients with cancer: current evidence
Prevalence and patterns of HPA axis dysregulation
Evidence from observational studies consistently demonstrates that HPA-axis dysregulation is highly prevalent among patients with cancer, irrespective of tumor type or treatment modality[17,43]. A systematic review of 17 studies reported altered HPA-axis activity in 16 cohorts compared to cancer-free controls, with 13 identifying elevated baseline cortisol levels or exaggerated stress responses[17]. However, cortisol dysregulation in cancer can manifest as either hyper- or hypocortisolism, depending on tumor type, treatment, and comorbidities[39]. Nevertheless, these findings confirm the widespread disruption of endocrine regulation in oncology populations. Typical patterns of dysregulation include elevated basal cortisol concentrations (often 20–200% higher than controls), blunted diurnal slopes, indicating impaired circadian regulation, and exaggerated or blunted responses to pharmacological or psychosocial stressors. These patterns collectively point to a state of maladaptive neuroendocrine regulation in patients with cancer, marked by sustained cortisol activation without appropriate rhythmicity or stress termination.
These abnormalities suggest a failure of adaptive endocrine regulation under chronic disease stress[44,45,46]. However, most oncology cohorts remain mixed-age, and age is frequently reported descriptively or addressed through age-matched control designs rather than formal age-stratified analyses [17,43]. Accordingly, while the prevalence and severity of cortisol dysregulation appear largely independent of tumor type, stage, or anticancer therapy, underscoring its potential as a non-specific biomarker of systemic vulnerability rather than a cancer-type-specific marker, the extent to which its prevalence or phenotype differs across older age strata remains insufficiently characterized and requires dedicated age-stratified designs (see Section below “Age-Related Changes in Cortisol:DHEA Metabolism”).
Associations with Clinical Outcomes
Cortisol dysregulation—whether reflected in elevated evening levels, blunted diurnal slopes, or reduced awakening responses—has been consistently associated with adverse outcomes in cancer populations. These include both patient-reported symptoms (e.g., fatigue, cognitive dysfunction, sleep disturbance[18,47,48]) and clinical endpoints (e.g., more advanced disease states[23]). Currently, there is scarce prospective evidence connecting pre-treatment cortisol or cortisol:DHEA(S) to acute treatment toxicities (e.g., CTCAE ≥3, dose reductions, hospitalizations). An overview of studies assessing cortisol or cortisol:DHEA(S) in relation to treatment toxicities or toxicity-related outcomes in cancer, specifically in older adults, is shown in Table 1. The following paragraphs further elaborate on associations between cortisol and DHEA(S) in cancer populations, not exclusively in older adults, to provide a rigorous overview of existing literature on topic.
In patients with head and neck cancer (n=50), elevated evening cortisol was associated with worse progression-free survival (HR=1.848, 95% CI=1.057–3.230), while elevated mean cortisol across the day was linked to significantly shorter survival (HR=2.662, 95% CI=1.115–6.355), whereas diurnal slope was not statistically significant[25]. In breast cancer survivors, a blunted diurnal cortisol slope prospectively predicted more severe fatigue and slower psychomotor recovery[24]. Other studies report similar associations in oral cancer and myeloproliferative neoplasms, where cortisol abnormalities correlate with fatigue severity, emotional distress, and poorer quality of life[39,49]. Further, patients with advanced non-small cell lung cancer post-chemotherapy showed reduced salivary DHEAS concentrations compared to age-matched controls, with lower DHEAS concentrations being associated with higher fatigue and depression scores[50].
Despite these consistent associations, the vast majority of studies conceptualize cortisol (and the cortisol:DHEA(S) ratio) as a prognostic biomarker of global health status or survival. Critically, few studies have examined its predictive value for treatment-related toxicity, such as grade ≥3 adverse events (per Common Terminology Criteria for Adverse Events (CTCAE) v.5.0), dose reductions, unplanned hospitalizations, or treatment discontinuations. This represents a significant knowledge gap. No large-scale prospective studies have yet tested whether pre-treatment cortisol features (e.g., blunted slope, high cortisol:DHEA(S) ratio) are associated with acute toxicities during chemotherapy or immunotherapy. Furthermore, the temporal sequence—whether cortisol dysregulation precedes or results from treatment and disease burden—remains insufficiently studied. Only two small longitudinal studies have examined cortisol trajectories across chemotherapy cycles[49,51]. These limitations underscore the urgent need for time-series, mechanistic studies that can differentiate cause from consequence and clarify the monitoring potential of HPA biomarkers.
Importantly, however, most studies linking cortisol or DHEA(S) to clinical outcomes do not formally evaluate whether these associations differ by age. Cohorts are typically mixed-age, and analyses more often rely on age adjustment or age-matched designs rather than age-stratified models or age×biomarker interaction testing. For instance, Cash et al. considered age among candidate confounders in survival models but did not report age-stratified or interaction analyses for cortisol features [25], and Fang et al. used age-matched controls without examining effect modification across age strata [50]. This limits inference on whether HPA-axis dysregulation carries distinct prognostic implications in older adults with cancer and supports the need for prospective, age-stratified validation.
Mechanistic pathways relevant to treatment toxicity
Cortisol’s role
Cortisol dysregulation may contribute to cancer treatment toxicity through multiple, evidence-based biological mechanisms. Mechanisms such as glucocorticoid-receptor-mediated chemoresistance and chemotherapy-induced endocrine disruption are supported by a combination of preclinical and early clinical evidence, whereas other pathways (e.g., interactions between cortisol, immunosenescence, and immunotherapy response in older adults) remain largely hypothetical and require targeted investigation.
Direct disruption of HPA axis function by chemotherapy. Platinum-based agents (e.g., cisplatin, carboplatin) have been shown to suppress serum cortisol levels following infusion, independent of circadian or psychological influences[52]. Whether this transient suppression contributes to symptoms such as nausea or fatigue remains speculative[52]. Further, based on rodent data, cisplatin activates hypothalamic CRH and vasopressin production, possibly exacerbating HPA activation and contributing to the stress burden of treatment[57].
Glucocorticoid receptor (GR)-mediated chemoresistance. Clinical studies show that perioperative dexamethasone increases SGK1 and MKP1/DUSP1 expression in ovarian tumours, suggesting that pharmacologic glucocorticoids can promote chemoresistance[58]. Further, preclinical work demonstrates that physiological cortisol levels can activate GR and induce pro-survival pathways; GR antagonism (e.g., relacorilant) restores chemosensitivity in vitro[59]. Finally, early-phase trials combining relacorilant with nab-paclitaxel improved progression-free and overall survival[60].
Induction of cellular senescence and inflammatory toxicity. Chemotherapy promotes cellular senescence in non-tumor tissues, leading to a persistent pro-inflammatory secretory phenotype that exacerbates tissue damage and impairs recovery[61]. In older adults, this effect is amplified, with biomarkers such as p16INK4a (a cyclin-dependent kinase inhibitor) rising sharply post-treatment, contributing to frailty, fatigue, and reduced treatment resilience[62].
Age-related cortisol accumulation and oxidative stress. With aging, chronic hypercortisolemia enhances chemoresistance via GR-mediated upregulation of metallothioneins, reprogramming cancer cells toward treatment insensitivity[63]. Simultaneously, oxidative stress disrupts HPA axis regulation and hippocampal feedback, particularly in older males, further impairing endocrine-immune homeostasis[64].
Immune suppression and immunotherapy toxicity. Cortisol dysregulation suppresses immune activation by reducing naïve T-cell populations and enhancing T-cell exhaustion, directly undermining responses to immune checkpoint inhibitors[65]. Moreover, anti-CTLA-4 and anti-PD-1/PD-L1 therapies may induce hypophysitis (found in 3.9% of patients)[66], leading to permanent ACTH and cortisol deficiency, further compromising endocrine balance during immunotherapy[67].
Inflammatory amplification in aging brains. In older patients, elevated cortisol synergizes with pro-inflammatory cytokines (IL-6, TNF-α), leading to neuroinflammation, hippocampal atrophy, and impaired cognitive and treatment recovery[68,69]. Microglial priming in aged brains amplifies this response to chemotherapy, shifting the inflammatory response toward damaging oxidative stress[68].
However, it is essential to acknowledge that current evidence is predominantly associative. The extent to which cortisol dysregulation drives downstream pathology—or merely reflects a biomarker of systemic stress—is an open question. Longitudinal studies with repeated sampling across the treatment continuum are critically needed to clarify directionality and causal roles.
DHEA(S)’s role
DHEA(S) exerts immunostimulatory, anti-glucocorticoid, and anabolic effects that counterbalance cortisol’s impact. Notably DHEA promotes interleukin-2 (IL-2) production by CD4⁺ T cells[70], promoting a Th1-type immune response[71]. In doing so, DHEA acts as a physiological antiglucocorticoid, opposing cortisol’s immunosuppressive influence [72,73] and helping to preserve immune function during stress or chemotherapy. DHEA and DHEAS also exert anabolic or protective effects on metabolism and tissues: for instance, DHEAS supplementation in animals reduces visceral fat and improves insulin sensitivity[74], and clinically, low DHEA states are associated with greater frailty and sarcopenia (a condition characterized by loss of muscle mass, strength, and function in older adults)[75]. Therefore, an inadequate DHEA(S) response in patients with cancers – especially in older individuals – may permit unopposed cortisol activity, impairing immune surveillance and tissue recovery. This imbalance can contribute to heightened treatment toxicity and slower recovery, highlighting the need to consider DHEA(S) alongside cortisol in managing HPA axis dysregulation during cancer therapy.
Evidence limitations and unmet needs
While the evidence consistently demonstrates high prevalence and clinical correlates of HPA-axis dysregulation in cancer populations, its translation to clinical practice is hampered by several key limitations: (1) Most studies assess survival, fatigue, or global well-being rather than DLTs, hospitalizations, or treatment adherence—outcomes more directly actionable in oncology[17]. (2) Despite age being a primary modifier of HPA function, few studies stratify by age group or include frail or multimorbid older adults. (3) HPA biomarkers are absent from clinical tools predicting treatment toxicity (e.g., Cancer and Aging Research Group CARG[76], Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH)[6]), despite their plausible biological role[9,77]. (4) Despite growing interest, cortisol remains primarily a research biomarker, lacking standardized protocols and regulatory qualification in oncology.
Thus, while cortisol abnormalities are consistently linked to adverse symptoms and poor survival, their value as predictive biomarkers for treatment-specific toxicities remains underexplored. At present, the potential role of HPA-axis biomarkers in clinical toxicity tools should first be tested in well-designed prospective studies that directly compare the performance of existing models with and without endocrine measures.
Section summary
| - HPA-axis dysregulation is prevalent across tumor types, most commonly manifesting as elevated cortisol levels and blunted circadian rhythms. - These abnormalities correlate with poorer survival and symptom burden but have not been validated as predictors of treatment toxicity. - Most evidence is prognostic and lacks specificity for treatment-related toxicities. - Prospective, age-stratified studies using standardized toxicity endpoints are urgently needed to determine the predictive and monitoring utility of cortisol and DHEA(S) in cancer care. |
Treatment outcomes in older adults
Age-related changes in cortisol:DHEA metabolism
Aging is associated with profound alterations in HPA-axis regulation that shape the endocrine context in which cancer therapy occurs[27,37,45]. These changes include: (1) Elevated basal cortisol secretion, partly driven by increased hypothalamic drive and altered negative feedback at the pituitary and hippocampal levels[78,79]; (2) Impaired glucocorticoid receptor sensitivity, leading to prolonged cortisol exposure and a reduced capacity to terminate stress responses[29,80]; (3) DHEAS declines by approximately 1–2% per year after the third decade, reaching 20–30% of peak concentrations by age 70–80[81]. Thus, in aging, elevated cortisol and this decline in DHEA(S) production reduce the cortisol-buffering effects of DHEA(S) and result in an elevated cortisol:DHEA(S) ratio[32,35].
Together, these changes impair circadian cortisol regulation, yielding blunted diurnal slopes and exaggerated responses to physical or psychological stress. The elevated cortisol:DHEA(S) ratio, in particular, is increasingly recognized as a sensitive marker of endocrine imbalance and systemic vulnerability in older adults. It has been linked to immunosenescence, chronic low-grade inflammation, sarcopenia, and reduced recovery from physiological insults[31,34,35,82,83].
Crucially, these endocrine alterations are not benign background phenomena. Instead, they create a hormonal environment in which physiological resilience is already compromised before treatment begins. This may amplify the impact of cancer-related stressors and therapy-induced toxicity, particularly in the context of multimorbidity, frailty, and functional decline common in geriatric populations[27,63]. Therefore, age-related HPA-axis dysregulation may serve not only as a biomarker of vulnerability but also as a biological modifier that increases susceptibility to adverse treatment outcomes.
Lack of Age-Stratified Analyses and Predictive Models
Despite well-documented aging effects on cortisol dynamics, most oncology studies evaluating HPA-axis biomarkers do not stratify analyses by age or adjust for aging-related endocrine shifts. Research cohorts often span wide age ranges without age-specific reference intervals, leading to potential misclassification of normal aging effects as pathological.
Further, few studies contextualize cortisol abnormalities within geriatric assessment domains such as frailty, comorbidity, or functional reserve—despite these being key determinants of treatment tolerance in older adults[84]. The omission of age-adjusted biomarker interpretation critically limits the relevance of existing research for geriatric oncology.
Current predictive models for chemotherapy toxicity in older adults, including the CARG score[76], the CRASH[6], and the G8 screening tool[85], primarily include demographic, functional, and inflammatory variables, showing poor external validation in predicting the risk of chemotherapy severe toxicities in some cohorts[86]. None incorporates endocrine or HPA-axis biomarkers, despite mounting evidence of their clinical relevance[9,41,77,87,88,89,90].
Integrating cortisol-based biomarkers into these models offers a promising strategy to enhance precision. For example, a blunted cortisol slope or elevated cortisol:DHEA ratio may uncover physiologic risk in patients who otherwise appear fit on functional screening or who fall into intermediate-risk strata based on age and comorbidities alone. This could be especially useful in tailoring chemotherapy dosing, early supportive care, or prehabilitation strategies.
In future predictive frameworks, cortisol metrics could be incorporated as add-on variables to existing tools (e.g., CARG-plus or CRASH-plus), independent biomarkers within new multimodal indices of endocrine resilience, or as dynamic markers tracked over time to reflect evolving tolerance across treatment cycles. To support such integration, normative reference ranges and clinically actionable thresholds must be established in older patients with cancer, ideally through prospective, age-stratified biomarker validation studies (see Section 5). Until then, the omission of endocrine parameters remains a critical blind spot in toxicity prediction for geriatric oncology.
Mechanistic pathways linking cortisol dysregulation to treatment outcomes in older adults
The intersection of aging physiology and cortisol dysregulation may undermine treatment tolerance through several interrelated mechanisms. While human data support some pathways, others remain theoretical or are extrapolated from preclinical models and require cautious interpretation.
Exacerbation of immunosenescence. Aging is characterized by diminished innate and adaptive immune function—marked by thymic involution, T-cell exhaustion, and chronic low-grade inflammation[91,92]. Elevated cortisol levels compound these changes, suppressing immune cell proliferation, altering cytokine profiles, and impairing tumor immune surveillance[80]. Although human data linking cortisol to poor immunotherapy outcomes remain limited, early observational findings suggest that baseline endocrine function may modify immune-related adverse events and treatment efficacy[93].
Glucocorticoid receptor-mediated treatment resistance. Cortisol activates glucocorticoid receptors (GRs), modulating transcription of genes involved in cell survival and proliferation[94]. GR activation enhances PI3K/Akt and NF-κB signaling, promotes anti-apoptotic pathways, and induces drug resistance mechanisms[94,95,96,97]. In cancers exhibiting GR overexpression or glucocorticoid resistance, these effects may reduce chemotherapy efficacy[98]. While these mechanisms have been observed across tumor types—including ovarian, breast, and lung cancers—their translation to older patient populations remains speculative, and human studies evaluating cortisol-GR interactions during treatment are lacking.
Delayed tissue repair.Cortisol impairs fibroblast activity and collagen synthesis[99,100], which could undermine post-treatment recovery. Human studies have documented age-related declines in extracellular matrix turnover and fibroblast responsiveness[101,102], but direct evidence linking cortisol to impaired post-treatment recovery in patients with cancer is limited. The role of DHEA as a counter-regulatory anabolic hormone may be especially relevant here, given its capacity to promote matrix repair and oppose cortisol’s effects[103,104]—though this too remains understudied in clinical oncology.
Together, these mechanisms suggest that cortisol dysregulation may not merely reflect systemic stress but actively contribute to treatment intolerance. Importantly, aging appears to magnify the biological impact of HPA-axis dysregulation, particularly in immune, neuroendocrine, and reparative systems already under strain. Further research is needed to determine the relative contributions of these pathways and whether they can be targeted to enhance resilience and reduce toxicity in geriatric oncology.
Research priorities
To translate these insights into clinical practice, future research should pursue the following directions:
Conduct age-stratified analyses using reference-adjusted cortisol:DHEA(S) data. Future studies should explicitly stratify outcomes by age groups (e.g., 65–74, 75–84, ≥85 years) and apply age-appropriate reference ranges to distinguish normative aging effects from cancer-related dysregulation. Large-scale normative datasets already exist in endocrinology, but few oncology studies leverage this information to contextualize biomarker abnormalities in older patients.
Design longitudinal studies to track cortisol and DHEA(S) trajectories across treatment cycles.Rather than relying on single-time-point measures, research should evaluate temporal changes in cortisol slope, CAR, evening cortisol, and cortisol:DHEA(S) ratio at baseline, mid-treatment, and treatment completion. These trajectories may offer unique insights into dynamic resilience and physiological recovery. Real-time tracking may also support early toxicity detection and anticipatory supportive care.
Integrate endocrine biomarkers into multimodal prediction models. Validated risk scores such as CARG and CRASH could be enhanced by integrating endocrine markers. Alternatively, a new “Endocrine Resilience Index” incorporating salivary cortisol features, DHEA(S) levels, and clinical frailty indicators could be developed and validated in prospective cohorts.
Evaluate feasibility and implementation in vulnerable subgroups. Special attention should be given to frail, multimorbid, or cognitively impaired patients, who are often underrepresented in biomarker research. Studies should report not only biomarker-outcome associations but also feasibility metrics including adherence to sample collection, cost, acceptability, and usability in real-world geriatric oncology settings.
Explore DHEA(S)-specific effects and mechanisms.Compared to cortisol, DHEA(S) remains understudied in cancer populations. Its immuno-enhancing, anti-glucocorticoid, and anabolic properties may confer protective effects that warrant further exploration, especially in the context of sarcopenia, fatigue, and post-treatment recovery.
Section summary
| - Older adults exhibit distinct HPA-axis alterations that increase physiological vulnerability to cancer therapy. - Despite these biological vulnerabilities, most studies do not stratify biomarker data by age or integrate them into predictive models for toxicity. - Mechanistic pathways—including immune suppression, glucocorticoid receptor signaling, and impaired tissue repair—provide a biologically plausible rationale for the role of cortisol in mediating treatment intolerance. - Research priorities include age-adjusted reference use, longitudinal biomarker tracking, model integration, feasibility studies, and greater focus on DHEA(S). - These priorities lay the foundation for the standardization and clinical translation roadmap outlined in Section 5. |
Methodological heterogeneity: A barrier to clinical translation
Despite strong biological plausibility and consistent associations with clinical outcomes, the translation of HPA-axis biomarkers into oncology practice remains limited. A significant barrier is the substantial methodological heterogeneity across studies, which undermines reliability, limits comparability, and impedes regulatory qualification. This section outlines key sources of variability—ranging from matrix selection to endpoint definitions—and offers concrete recommendations to standardize biomarker assessment.
Sampling matrices
The biological matrix used to assess cortisol and DHEA(S) strongly influences the physiological interpretation, feasibility, and clinical relevance of results. Current studies use heterogeneous measurement approaches[105,106].
Salivary cortisol reflects the free, biologically active fraction of circulating cortisol, with strong correlation to serum-free cortisol[107,108,109]. It responds robustly to ACTH and CRH stimulation and is unaffected by cortisol-binding globulin, making it ideal for circadian rhythm profiling and stress reactivity assessment. Given its non-invasiveness, low cost, and ease of repeated sampling, salivary cortisol has become the preferred matrix in psychoneuroendocrinology [107] and is gaining traction in aging and oncology research[38,105,110]. Salivary DHEA, similarly, offers practical advantages: it reflects the bioavailable fraction, correlates well with serum levels (r ≈ 0.86 in a 358-pair cohort[111]), and remains relatively stable across the day[35,111,112,113].
The choice between DHEA and its sulfated form DHEAS depends on study objectives, and they should not be used interchangeably[114]. DHEA fluctuates more rapidly and is preferred in studies of acute stress reactivity[113], while DHEAS is more stable and better suited to long-term health profiling[115]. In the context of cortisol:DHEA(S) ratios and cancer and frailty research, a single, pre-specified DHEA sample in the morning—adjusted for time of awakening[116]—offers a feasible and clinically relevant option.
Recommendation: The choice between serum and saliva measurements depends largely on the available analytical approaches and oncology setting (in- or outpatient). DHEA versus DHEAS sampling depends on the study objectives and is both scientifically defensible.
Sample timing recommendations
Cortisol secretion follows a diurnal rhythm, with a sharp peak upon awakening and gradual decline across the day. Capturing this rhythm requires carefully timed, repeated measurements. However, timing protocols vary widely across studies—from single morning samples to multi-point curves across 1 to 4 days—hindering comparability and interpretation[17,105,117]. Pairing cortisol with DHEA(S) at the same awakening timepoint further stabilizes the cortisol:DHEA(S) ratio against diurnal phase differences[118], as DHEA(S) shows a flatter but still morning-skewed rhythm (mostly DHEA[113]); two-day morning averages reduce random error relative to single-day sampling[119].
Recommendation:Concerning cortisol sampling, adhere to expert consensus guidelines recommending at least five sampling time points per day (upon awakening, +30 min, noon, afternoon, bedtime) over ≥3 consecutive days to improves reliability [105,120,121] and capture key features such as cortisol awakening response (CAR), diurnal slope, evening cortisol, area under the curve (AUC). While full cortisol diurnal profiling adds mechanistic depth, a two-day cortisol:DHEA(S) profile (with strict sample timing, adjusted for awakening time[116]) could provide a pragmatic approach for prognostic studies in geriatric oncology. For longitudinal treatment monitoring, sampling should correspond to clinically meaningful milestones (e.g., baseline, mid-cycle, end-of-cycle) and include a 6-12 months follow-up for long-term pattern evaluation[122,123].
Importantly, feasibility in older adults must be addressed. Cognitive impairment, frailty, or multimorbidity may impair protocol adherence. Pilot studies suggest ~75% compliance in cancer populations[38], though implementation in cognitively impaired or homebound patients requires support (e.g., caregiver assistance, simplified kits)[105].
Heterogeneity in clinical outcomes and confounders
Clinical outcomes used in HPA-axis studies vary substantially—ranging from survival and fatigue to general quality of life[47,124,125,126]. However, few studies evaluate treatment-specific toxicities such as CTCAE grade ≥3 adverse events, dose reductions or discontinuations, unplanned hospitalizations, or functional decline[17]. This limits the ability to evaluate cortisol as a predictive biomarker of treatment intolerance.
Additionally, key age-specific confounders—such as frailty, cognitive function, polypharmacy, and corticosteroid co-medications—are inconsistently reported or adjusted for[76]. This omission may obscure or exaggerate associations between cortisol and outcomes in older adults.
Recommendation:Standardize outcome definitions using CTCAE criteria and integrate geriatric oncology guidelines (e.g., ASCO, SIOG) for confounder control. Report and adjust for variables such as corticosteroid use, multimorbidity, and frailty indices in all predictive analyses.
Lack of reference ranges for older adults
Numerous large population studies—many using gold-standard liquid chromatography tandem mass spectrometry (LC-MS/MS)—have established cortisol and DHEA(S) reference intervals in older adults[127,128,129,130].
In contrast, no authoritative guidelines or peer-reviewed studies have yet been published with universally accepted reference ranges stratified by specific cancer types or discrete treatment phases (e.g., pre-operative vs. adjuvant vs. maintenance). Instead, oncology papers typically report cohort-specific distributions or use general population cut-offs when exploring prognostic associations[25,39,131].
Recommendation: Multi-center validation studies should develop age- and treatment-specific reference intervals for cortisol and DHEA(S), using standardized analytical platforms and harmonized pre-analytical conditions.
Section summary
|
Future research and standardization agenda
Bridging the gap between exploratory cortisol research and clinical application in geriatric oncology requires a comprehensive, staged roadmap. This includes biomarker standardization, predictive validation, interventional testing, and clinical integration. To support clinical translation and address the current gap in biological risk stratification, the 14-item checklist of the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) Test Evaluation Working Group (TE-WG) for test evaluation was applied[132]. The resulting analysis, presented in Supplementary File 1, outlines the unmet clinical needs, intended use, and feasibility of cortisol:DHEA ratio testing in older patients with cancer, offering a roadmap for biomarker development in geriatric oncology. In this section, concrete priorities across these domains are outlined to facilitate the development of cortisol and DHEA as predictive and monitoring biomarkers for treatment-related toxicity.
Standardization priorities for biomarker development
Before cortisol or DHEA(S) can be considered clinically actionable, robust methodological standardization is required. For cortisol, expert consensus supports repeated daily sampling to capture diurnal dynamics, with a minimum of five time points per day (awakening, +30 minutes, midday, afternoon, and bedtime) over at least three consecutive days. In clinical or pragmatic settings, simplified protocols—such as morning and evening sampling—may be acceptable, provided they are prospectively validated. When focusing on the cortisol:DHEA(S) ratio, a standardized two-day morning sampling protocol may offer a feasible compromise that reduces random measurement error relative to single-day assessments. Across all protocols, key pre-analytical variables—including time of awakening, medication use (particularly exogenous corticosteroids), food intake, and sampling adherence—must be systematically recorded and accounted for. Analytical methods should rely on validated assays or platforms with established inter-assay reliability. In parallel, age- and treatment-stratified normative datasets are required to enable valid interpretation in older adults with cancer. Finally, clinical validation studies should adopt uniform and clinically actionable endpoints, such as CTCAE grade ≥3 toxicities, dose reductions, treatment discontinuation, and unplanned hospitalizations.
Prospective validation studies
Once standardized, the predictive validity of cortisol and DHEA(S) must be tested in prospective studies focused on older adults with cancer. These studies should (1) recruit treatment-naïve patients ≥65 years, including those with frailty or multimorbidity, (2) collect serial salivary samples pre-treatment, mid-treatment, and at treatment completion, (3) assess toxicity-related outcomes including dose-limiting toxicities (DLTs), dose reductions or delays, treatment discontinuations, hospitalizations and functional decline, (4) include comprehensive geriatric assessments to evaluate frailty, comorbidities, functional reserve, and polypharmacy, and (5) report implementation outcomes such as feasibility, adherence, patient burden, and cost.
To ensure applicability across the heterogeneous older adult population, validation cohorts should deliberately include patients across the full spectrum of frailty, multimorbidity, cognitive status, and socio-economic backgrounds, rather than only fitter trial-eligible individuals. Stratified analyses by frailty category, comorbidity burden, polypharmacy, corticosteroid use, and functional status, as well as pre-specified subgroup analyses in the oldest-old (≥80 years), will be necessary to determine whether biomarker thresholds and predictive performance are stable across these clinically relevant strata. In addition to testing baseline cortisol features (e.g., blunted slope, elevated evening levels), studies should explore treatment-induced cortisol trajectories as real-time indicators of declining resilience.
Interventional research
To move beyond correlation and test causality, interventional trials that deliberately modify HPA-axis profiles and assess downstream effects on toxicity are necessary. Such studies can determine whether normalizing cortisol:DHEA(S) trajectories improves treatment tolerance, thus establishing whether these biomarkers function as causal mediators or merely as risk indicators.
Establishing causality requires interventional trials targeting cortisol dysregulation to improve treatment tolerance. Two strategies could be pursued, and the potential efficacy and safety of proposed interventions are further expanded upon in Supplementary file 2:
Behavioral interventions: Mind–body interventions (e.g., mindfulness-based stress reduction, yoga, cognitive-behavioral therapy, or exercise interventions) have been shown to improve diurnal cortisol output and rhythmicity[131,133,134,135,136,137,138]. Median participant age across biomarker studies hovers at approximately 55–60 years[137]; frail adults ≥75 years are seldom enrolled, limiting generalizability to the oldest-old. Randomized controlled trials embedding serial cortisol sampling can determine whether such interventions delay the onset or severity of treatment-related toxicity, normalize HPA-axis profiles, and/or improve physical functioning or quality of life.
Pharmacological modulation: Evidence indicates that while some pharmacological options are under investigation for managing HPA axis dysregulation in older patients with cancer (e.g., selective glucocorticoid receptor modulators [60,139] or non-selective glucocorticoid receptor antagonists[140,141]), treatment decisions should be individualized based on the specific type of dysfunction (hyper- vs. hypofunction), underlying cancer type, concurrent treatments, and patient-specific factors. Regular monitoring and multidisciplinary care coordination remain essential for optimal outcomes.
Clinical integration framework
To achieve clinical impact, validated HPA-axis biomarkers must be systematically embedded within oncology care pathways. A staged clinical integration framework is outlined in Table 2. First, cortisol and DHEA(S) sampling can be piloted within pre-treatment geriatric assessments, alongside established functional and inflammatory markers, with parallel evaluation of logistical feasibility, laboratory capacity, and stakeholder acceptance. Second, once predictive validity is established, key HPA-axis features—such as blunted diurnal slope or elevated cortisol:DHEA(S) ratio—could be incorporated into existing toxicity prediction tools (e.g., CARG or CRASH) or combined into new composite indices of endocrine resilience, supported by automated interpretation within electronic health record–based decision-support systems. Finally, clinical utility must be demonstrated through pragmatic trials or hybrid implementation–effectiveness designs assessing whether biomarker-informed care reduces severe toxicity rates, improves treatment adherence and dose intensity, and lowers hospitalization or functional decline.
While this review outlines conceptual pathways for clinical integration, formal evaluation of cost-effectiveness, workflow burden, and stakeholder acceptance will require prospective implementation-effectiveness studies, aligned with biomarker evaluation frameworks (e.g., EFLM TE-WG[132], Supplementary File 1).
Review limitations
While this review offers a translational roadmap, several limitations must be acknowledged. First, most studies cited are observational, cross-sectional, or underpowered to assess treatment-specific toxicity outcomes. Second, evidence on DHEA(S) remains sparse relative to that on cortisol, limiting firm conclusions about the cortisol:DHEA(S) ratio. Third, this is a narrative review, and selection bias may persist despite efforts to prioritize representative and high-quality studies. Fourth, the generalizability of findings to frail, cognitively impaired, or socioeconomically vulnerable older adults is uncertain, as these groups are frequently excluded from primary studies. Finally, the incremental predictive value of HPA-axis biomarkers relative to established geriatric assessment variables and toxicity tools has not yet been quantified. The staged roadmap outlined in this review—including methodological standardization, age-stratified prospective validation, and interventional trials—is specifically designed to address these limitations in future research.
Section summary
| - Translation of HPA-axis biomarkers into geriatric oncology requires standardization, validation, interventional testing, and integration. - Prospective studies should assess predictive accuracy for treatment toxicity, including in frail and multimorbid patients. - Interventions targeting cortisol dysregulation—behavioral or pharmacological—should be tested for modifiability of toxicity risk. - Integration into oncology workflows demands demonstration of clinical utility and interdisciplinary collaboration. |
Conclusions
Older adults with cancer face a disproportionate risk of treatment-related toxicities, however, current oncology risk stratification models largely omit biomarkers that reflect underlying physiological resilience. The hypothalamic-pituitary-adrenal (HPA) axis—particularly through cortisol and DHEA(S) dynamics—represents a promising but underexplored window into this vulnerability.
This review has synthesized evidence showing that age-related alterations in HPA-axis function (e.g., blunted cortisol slope, reduced DHEA(S)) are biologically linked to key mechanisms of treatment intolerance, including immunosenescence, glucocorticoid-mediated chemoresistance, impaired tissue repair, and neuroinflammation. However, the translational potential of these biomarkers is currently limited by methodological heterogeneity, lack of age-stratified validation, and minimal integration into predictive frameworks.
A structured translational agenda is required to advance clinical utility. This includes: (1) biomarker standardization using validated salivary assays; (2) prospective studies with age-specific reference thresholds and clinically actionable endpoints; (3) interventional trials assessing whether targeting cortisol dysregulation improves treatment tolerance; and (4) integration into real-world oncology workflows and decision tools.
If implemented, this roadmap could facilitate a paradigm shift in geriatric oncology—from one-size-fits-all toxicity prediction to precision risk assessment based on endocrine resilience. Cortisol and DHEA(S) have the potential to not only predict who is most vulnerable but also enable personalized interventions that preserve function, reduce toxicity, and optimize cancer care for older adults.
Funding
No funding sources to be declared.
Acknowledgements
During the preparation of this manuscript, the author used the ChatGPT 4o tool to improve academic writing. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
References
- NCI, N.C.I. Age and Cancer Risk. 2025. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/age.
- Bhatt, V.R. Cancer in older adults: understanding cause and effects of chemotherapy-related toxicities. Future Oncol 2019, 15(22), 2557–2560. [Google Scholar] [CrossRef] [PubMed]
- Eochagain, C.M. Management of immune checkpoint inhibitor-associated toxicities in older adults with cancer: recommendations from the International Society of Geriatric Oncology (SIOG). Lancet Oncol 2025, 26(2), e90–e102. [Google Scholar] [PubMed]
- Shahrokni, A. Long-term Toxicity of Cancer Treatment in Older Patients. Clin Geriatr Med 2016, 32(1), 63–80. [Google Scholar] [CrossRef]
- Hurria, A. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicenter study. J Clin Oncol 2011, 29(25), 3457–65. [Google Scholar]
- Extermann, M. Predicting the risk of chemotherapy toxicity in older patients: the Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer 2012, 118(13), 3377–86. [Google Scholar] [CrossRef] [PubMed]
- Loh, K.P. Adequate assessment yields appropriate care-the role of geriatric assessment and management in older adults with cancer: a position paper from the ESMO/SIOG Cancer in the Elderly Working Group. ESMO Open 2024, 9(8), 103657. [Google Scholar]
- Hurria, A. Validation of a Prediction Tool for Chemotherapy Toxicity in Older Adults With Cancer. J Clin Oncol 2016, 34(20), 2366–71. [Google Scholar] [CrossRef]
- Chan, W.L. Prediction models for severe treatment-related toxicities in older adults with cancer: a systematic review. Age Ageing 2025, 54(4). [Google Scholar] [CrossRef]
- Chrousos, G.P. Stress and disorders of the stress system. Nat Rev Endocrinol 2009, 5(7), 374–81. [Google Scholar]
- Herman, J.P. Regulation of the Hypothalamic-Pituitary-Adrenocortical Stress Response. Compr Physiol 2016, 6(2), 603–21. [Google Scholar] [CrossRef]
- Alotiby, A. Immunology of Stress: A Review Article. J Clin Med 2024, 13(21). [Google Scholar] [CrossRef]
- Chrousos, G.P. The hypothalamic-pituitary-adrenal axis and immune-mediated inflammation. N Engl J Med 1995, 332(20), 1351–62. [Google Scholar] [CrossRef]
- Gjerstad, J.K.; Lightman, S.L.; Spiga, F. Role of glucocorticoid negative feedback in the regulation of HPA axis pulsatility. Stress 2018, 21(5), 403–416. [Google Scholar] [CrossRef]
- McEwen, B.S. Central effects of stress hormones in health and disease: Understanding the protective and damaging effects of stress and stress mediators. Eur J Pharmacol 2008, 583(2-3), 174–85. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Protective and damaging effects of stress mediators. N Engl J Med 1998, 338(3), 171–9. [Google Scholar] [PubMed]
- Kanter, N.G. Hypothalamic-Pituitary-Adrenal Axis Dysfunction in People With Cancer: A Systematic Review. Cancer Med 2024, 13(22), p. e70366. [Google Scholar] [CrossRef]
- Weinrib, A.Z. Diurnal cortisol dysregulation, functional disability, and depression in women with ovarian cancer. Cancer 2010, 116(18), 4410–9. [Google Scholar] [CrossRef]
- Rasmuson, T. Increased serum cortisol levels are associated with high tumour grade in patients with renal cell carcinoma. Acta Oncol 2001, 40(1), 83–7. [Google Scholar]
- Ramirez-Exposito, M.J. Circulating levels of beta-endorphin and cortisol in breast cancer. Compr Psychoneuroendocrinol 2021, 100028. [Google Scholar] [CrossRef]
- Cruz, M.S.P. Nighttime salivary cortisol as a biomarker of stress and an indicator of worsening quality of life in patients with head and neck cancer: A cross-sectional study. Health Sci Rep 2022, 5(5), p. e783. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.P.; Lin, C.C. Relationships of salivary cortisol and melatonin rhythms to sleep quality, emotion, and fatigue levels in patients with newly diagnosed lung cancer. Eur J Oncol Nurs 2017, 29, 79–84. [Google Scholar] [CrossRef]
- Bernabe, D.G. Increased plasma and salivary cortisol levels in patients with oral cancer and their association with clinical stage. J Clin Pathol 2012, 65(10), 934–9. [Google Scholar] [CrossRef]
- Zeitzer, J.M. Aberrant nocturnal cortisol and disease progression in women with breast cancer. Breast Cancer Res Treat 2016, 158(1), 43–50. [Google Scholar] [CrossRef]
- Cash, E. Evening cortisol levels are prognostic for progression-free survival in a prospective pilot study of head and neck cancer patients. Front Oncol 2024, 14, 1436996. [Google Scholar] [CrossRef] [PubMed]
- Volden, P.A.; Conzen, S.D. The influence of glucocorticoid signaling on tumor progression. Brain Behav Immun 2013, 30 Suppl(0), S26–31. [Google Scholar] [CrossRef]
- Ayroldi, E. Role of Endogenous Glucocorticoids in Cancer in the Elderly. Int J Mol Sci 2018, 19(12). [Google Scholar] [CrossRef]
- Spindler, M. Dysfunction of the hypothalamic-pituitary adrenal axis and its influence on aging: the role of the hypothalamus. Sci Rep 2023, 13(1), 6866. [Google Scholar] [PubMed]
- Veldhuis, J.D.; Sharma, A.; Roelfsema, F. Age-dependent and gender-dependent regulation of hypothalamic-adrenocorticotropic-adrenal axis. Endocrinol Metab Clin North Am 2013, 42(2), 201–25. [Google Scholar] [CrossRef] [PubMed]
- van den Beld, A.W. The physiology of endocrine systems with ageing. Lancet Diabetes Endocrinol 2018, 6(8), 647–658. [Google Scholar] [CrossRef]
- Ferrari, E. Age-related changes of the hypothalamic-pituitary-adrenal axis: pathophysiological correlates. Eur J Endocrinol 2001, 144(4), 319–29. [Google Scholar] [CrossRef]
- Buoso, E. Opposing effects of cortisol and dehydroepiandrosterone on the expression of the receptor for Activated C Kinase 1: implications in immunosenescence. Exp Gerontol 2011, 46(11), 877–83. [Google Scholar]
- Pluchino, N. Neurobiology of DHEA and effects on sexuality, mood and cognition. J Steroid Biochem Mol Biol 2015, 145, 273–80. [Google Scholar]
- Butcher, S.K. Raised cortisol:DHEAS ratios in the elderly after injury: potential impact upon neutrophil function and immunity. Aging Cell 2005, 4(6), 319–24. [Google Scholar] [CrossRef] [PubMed]
- Heaney, J.L.; Phillips, A.C.; Carroll, D. Ageing, physical function, and the diurnal rhythms of cortisol and dehydroepiandrosterone. Psychoneuroendocrinology 2012, 37(3), 341–9. [Google Scholar] [CrossRef]
- Schwartz, A.G. Dehydroepiandrosterone, Cancer, and Aging. Aging Dis 2022, 13(2), 423–432. [Google Scholar] [CrossRef]
- Bauer, M.E. Stress, glucocorticoids and ageing of the immune system. Stress 2005, 8(1), 69–83. [Google Scholar] [CrossRef]
- Chhabria, K. Feasibility and value of salivary cortisol sampling to reflect distress in head and neck cancer patients undergoing chemoradiation: A proof-of-concept study. Int J Oncol Res 2022, 5(2). [Google Scholar]
- Vizcaino, M. Dysregulation in Cortisol Diurnal Activity among Myeloproliferative Neoplasms Cancer Patients. Open Access Text, 2018. [Google Scholar]
- Lutgendorf, S.K. Interleukin-6, cortisol, and depressive symptoms in ovarian cancer patients. J Clin Oncol 2008, 26(29), 4820–7. [Google Scholar] [CrossRef]
- Abraham, S. Accelerated Aging in Cancer and Cancer Treatment: Current Status of Biomarkers. Cancer Med 2025, 14(9), p. e70929. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, J.M.; Cohen, H.J.; Muss, H.B. Incorporating biomarkers into cancer and aging research. J Clin Oncol 2014, 32(24), 2611–6. [Google Scholar] [CrossRef] [PubMed]
- Sephton, S.E. Diurnal cortisol rhythm as a predictor of breast cancer survival. J Natl Cancer Inst 2000, 92(12), 994–1000. [Google Scholar] [CrossRef]
- Reiche, E.M.; Nunes, S.O.; Morimoto, H.K. Stress, depression, the immune system, and cancer. Lancet Oncol 2004, 5(10), 617–25. [Google Scholar] [CrossRef]
- Sephton, S.; Spiegel, D. Circadian disruption in cancer: a neuroendocrine-immune pathway from stress to disease? Brain Behav Immun 2003, 17(5), 321–8. [Google Scholar] [CrossRef]
- Colon-Echevarria, C.B. Neuroendocrine Regulation of Tumor-Associated Immune Cells. Front Oncol 2019, 9, 1077. [Google Scholar] [PubMed]
- Oh, I.J. Altered Hypothalamus-Pituitary-Adrenal Axis Function: A Potential Underlying Biological Pathway for Multiple Concurrent Symptoms in Patients With Advanced Lung Cancer. Psychosom Med 2019, 81(1), 41–50. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E. Cancer-related fatigue: links with inflammation in cancer patients and survivors. Brain Behav Immun 2007, 21(7), 863–71. [Google Scholar] [CrossRef]
- Figueira, J.A. Predisposing factors for increased cortisol levels in oral cancer patients. Compr Psychoneuroendocrinol 2022, 100110. [Google Scholar]
- Fang, Y.H. Low Concentrations of Dehydroepiandrosterone Sulfate are Associated with Depression and Fatigue in Patients with Non-Small-Cell Lung Cancer After Chemotherapy. Neuropsychiatr Dis Treat 2020, 16, 2103–2109. [Google Scholar] [CrossRef]
- Taub, C.J. Relationships Between Serum Cortisol, RAGE-Associated s100A8/A9 Levels, and Self-Reported Cancer-Related Distress in Women With Nonmetastatic Breast Cancer. Psychosom Med 2022, 84(7), 803–807. [Google Scholar] [CrossRef]
- Morrow, G.R. Reduction in serum cortisol after platinum based chemotherapy for cancer: a role for the HPA axis in treatment-related nausea? Psychophysiology 2002, 39(4), 491–5. [Google Scholar] [CrossRef]
- Hursti, T.J. Endogenous cortisol exerts antiemetic effect similar to that of exogenous corticosteroids. Br J Cancer 1993, 68(1), 112–4. [Google Scholar] [CrossRef]
- Toh, Y.L. Prechemotherapy Levels of Plasma Dehydroepiandrosterone and Its Sulfated Form as Predictors of Cancer-Related Cognitive Impairment in Patients with Breast Cancer Receiving Chemotherapy. Pharmacotherapy 2019, 39(5), 553–563. [Google Scholar] [CrossRef] [PubMed]
- Toh, Y.L. Longitudinal evaluation of dehydroepiandrosterone (DHEA), its sulfated form and estradiol with cancer-related cognitive impairment in early-stage breast cancer patients receiving chemotherapy. Sci Rep 2022, 12(1), p. 16552. [Google Scholar] [CrossRef] [PubMed]
- Lundstrom, S.; Furst, C.J. Symptoms in advanced cancer: relationship to endogenous cortisol levels. Palliat Med 2003, 17(6), 503–8. [Google Scholar] [CrossRef]
- Akiyama, Y. Peripherally administered cisplatin activates a parvocellular neuronal subtype expressing arginine vasopressin and enhanced green fluorescent protein in the paraventricular nucleus of a transgenic rat. J Physiol Sci 2020, 70(1), p. 35. [Google Scholar]
- Melhem, A. Administration of glucocorticoids to ovarian cancer patients is associated with expression of the anti-apoptotic genes SGK1 and MKP1/DUSP1 in ovarian tissues. Clin Cancer Res 2009, 15(9), 3196–204. [Google Scholar] [CrossRef]
- Greenstein, A.E.; Hunt, H.J. Glucocorticoid receptor antagonism promotes apoptosis in solid tumor cells. Oncotarget 2021, 12(13), 1243–1255. [Google Scholar] [CrossRef]
- Olawaiye, A.B. Clinical Trial Protocol for ROSELLA: a phase 3 study of relacorilant in combination with nab-paclitaxel versus nab-paclitaxel monotherapy in advanced platinum-resistant ovarian cancer. J Gynecol Oncol 2024, 35(4), p. e111. [Google Scholar] [CrossRef]
- Demaria, M. Cellular Senescence Promotes Adverse Effects of Chemotherapy and Cancer Relapse. Cancer Discov 2017, 7(2), 165–176. [Google Scholar]
- Hurria, A.; Jones, L. H.B. Muss, Cancer Treatment as an Accelerated Aging Process: Assessment, Biomarkers, and Interventions. Am Soc Clin Oncol Educ Book 2016, 35, e516–22. [Google Scholar] [PubMed]
- Gomes, A. AGE-INDUCED SYSTEMIC REPROGRAMMING DRIVES DRUG RESISTANCE IN LUNG CANCER. Innovation in Aging 2023, 139–140. [Google Scholar] [CrossRef]
- Limberaki, E. Cortisol levels and serum antioxidant status following chemotherapy. Health Psychol 2011. [Google Scholar] [CrossRef]
- Yu, S. Depression decreases immunity and PD-L1 inhibitor efficacy via the hypothalamic-pituitary-adrenal (HPA) axis in triple-negative breast cancer. Biochim Biophys Acta Mol Basis Dis 2025, 1871(2), 167581. [Google Scholar] [CrossRef]
- Patel, N. Immune checkpoint inhibitor induced hypophysitis: a specific disease of corticotrophs? Endocr Connect 2024, 13(11). [Google Scholar] [CrossRef]
- Di Stasi, V. Immunotherapy-Related Hypophysitis: A Narrative Review. Cancers (Basel) 2025, 17(3). [Google Scholar] [CrossRef]
- von Bernhardi, R.; Eugenin-von Bernhardi, L. J. Eugenin, Microglial cell dysregulation in brain aging and neurodegeneration. Front Aging Neurosci 2015, 7, 124. [Google Scholar] [CrossRef]
- Sudheimer, K.D. Cortisol, cytokines, and hippocampal volume interactions in the elderly. Front Aging Neurosci 2014, 153. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T. Dehydroepiandrosterone enhances IL2 production and cytotoxic effector function of human T cells. Clin Immunol Immunopathol 1991, 61 2 Pt 1, 202–11. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Taboada, V. Changes in peripheral blood lymphocyte subsets in elderly subjects are associated with an impaired function of the hypothalamic-pituitary-adrenal axis. Mech Ageing Dev 2002, 123(11), 1477–86. [Google Scholar] [CrossRef] [PubMed]
- Araneo, B.; Daynes, R. Dehydroepiandrosterone functions as more than an antiglucocorticoid in preserving immunocompetence after thermal injury. Endocrinology 1995, 136(2), 393–401. [Google Scholar] [CrossRef]
- Blauer, K.L. Dehydroepiandrosterone antagonizes the suppressive effects of dexamethasone on lymphocyte proliferation. Endocrinology 1991, 129(6), 3174–9. [Google Scholar] [CrossRef]
- Perrini, S. Associated hormonal declines in aging: DHEAS. J Endocrinol Invest 2005, 28(3 Suppl), 85–93. [Google Scholar] [PubMed]
- Erceg, N. The Role of Cortisol and Dehydroepiandrosterone in Obesity, Pain, and Aging. Diseases 2025, 13(2). [Google Scholar] [CrossRef] [PubMed]
- Dale, W. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Systemic Cancer Therapy: ASCO Guideline Update. J Clin Oncol 2023, 41(26), 4293–4312. [Google Scholar] [CrossRef]
- Battisti, N.M.L.; Arora, S.P. An overview of chemotherapy toxicity prediction tools in older adults with cancer: A young international society of geriatric oncology and nursing and allied health initiative. J Geriatr Oncol 2022, 13(4), 521–525. [Google Scholar] [CrossRef]
- Van Cauter, E.; Leproult, R.; Kupfer, D.J. Effects of gender and age on the levels and circadian rhythmicity of plasma cortisol. J Clin Endocrinol Metab 1996, 81(7), 2468–73. [Google Scholar]
- Karlamangla, A.S. Daytime trajectories of cortisol: demographic and socioeconomic differences--findings from the National Study of Daily Experiences. Psychoneuroendocrinology 2013, 38(11), 2585–97. [Google Scholar] [CrossRef] [PubMed]
- Stamou, M.I.; Colling, C.L.E. Dichtel, Adrenal aging and its effects on the stress response and immunosenescence. Maturitas 2023, 168, 13–19. [Google Scholar] [CrossRef]
- Ravaglia, G. The relationship of dehydroepiandrosterone sulfate (DHEAS) to endocrine-metabolic parameters and functional status in the oldest-old. Results from an Italian study on healthy free-living over-ninety-year-olds. J Clin Endocrinol Metab 1996, 81(3), 1173–8. [Google Scholar]
- Phillips, A.C. Cortisol, DHEAS, their ratio and the metabolic syndrome: evidence from the Vietnam Experience Study. Eur J Endocrinol 2010, 162(5), 919–23. [Google Scholar] [CrossRef]
- Phillips, A.C. Cortisol, DHEA sulphate, their ratio, and all-cause and cause-specific mortality in the Vietnam Experience Study. Eur J Endocrinol 2010, 163(2), 285–92. [Google Scholar] [CrossRef]
- Tran Van Hoi, E. Toxicity in Older Patients with Cancer Receiving Immunotherapy: An Observational Study. Drugs Aging 2024, 41(5), 431–441. [Google Scholar] [CrossRef]
- Bouzan, J.; Horstmann, M. G8 screening and health-care use in patients with cancer. Lancet Healthy Longev 2023, 4(7), e297–e298. [Google Scholar] [CrossRef]
- Frelaut, M. External Validity of Two Scores for Predicting the Risk of Chemotherapy Toxicity Among Older Patients With Solid Tumors: Results From the ELCAPA Prospective Cohort. Oncologist 2023, 28(6), e341–e349. [Google Scholar] [CrossRef]
- Al-Danakh, A. Aging-related biomarker discovery in the era of immune checkpoint inhibitors for cancer patients. Front Immunol 2024, 15, 1348189. [Google Scholar] [CrossRef] [PubMed]
- Morse, R.T. Sarcopenia and Treatment Toxicity in Older Adults Undergoing Chemoradiation for Head and Neck Cancer: Identifying Factors to Predict Frailty. Cancers (Basel) 2022, 14(9). [Google Scholar] [CrossRef]
- Menjak, I.B. Predicting treatment toxicity in older adults with cancer. Curr Opin Support Palliat Care 2021, 15(1), 3–10. [Google Scholar] [CrossRef]
- Li, D.; Soto-Perez-de-Celis, E. A. Hurria, Geriatric Assessment and Tools for Predicting Treatment Toxicity in Older Adults With Cancer. Cancer J 2017, 23(4), 206–210. [Google Scholar]
- Salminen, A. Immunosuppressive network promotes immunosenescence associated with aging and chronic inflammatory conditions. J Mol Med (Berl) 2021, 99(11), 1553–1569. [Google Scholar] [CrossRef] [PubMed]
- Yu, W. Immune Alterations with Aging: Mechanisms and Intervention Strategies. Nutrients 2024, 16(22). [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Su, Z.; Xue, J. Targeting T-cell Aging to Remodel the Aging Immune System and Revitalize Geriatric Immunotherapy. Aging Dis 2025. [Google Scholar] [CrossRef]
- Adelaiye-Ogala, R. Targeting the PI3K/AKT Pathway Overcomes Enzalutamide Resistance by Inhibiting Induction of the Glucocorticoid Receptor. Mol Cancer Ther 2020, 19(7), 1436–1447. [Google Scholar] [CrossRef]
- Kaboli, P.J. Chemoresistance in breast cancer: PI3K/Akt pathway inhibitors vs the current chemotherapy. Am J Cancer Res 2021, 11(10), 5155–5183. [Google Scholar]
- Aggarwal, B.B.; Sung, B. NF-kappaB in cancer: a matter of life and death. Cancer Discov 2011, 1(6), 469–71. [Google Scholar] [CrossRef]
- Karin, M. NF-kappaB as a critical link between inflammation and cancer. Cold Spring Harb Perspect Biol 2009, 1(5), p. a000141. [Google Scholar] [CrossRef] [PubMed]
- Beesley, A.H. Glucocorticoid resistance in T-lineage acute lymphoblastic leukaemia is associated with a proliferative metabolism. Br J Cancer 2009, 100(12), 1926–36. [Google Scholar] [CrossRef] [PubMed]
- Niculet, E.; Bobeica, C.; Tatu, A.L. Glucocorticoid-Induced Skin Atrophy: The Old and the New. Clin Cosmet Investig Dermatol 2020, 13, 1041–1050. [Google Scholar] [CrossRef]
- Chae, M. AP Collagen Peptides Prevent Cortisol-Induced Decrease of Collagen Type I in Human Dermal Fibroblasts. Int J Mol Sci 2021, 22(9). [Google Scholar] [CrossRef]
- Varani, J. Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am J Pathol 2006, 168(6), 1861–8. [Google Scholar] [CrossRef]
- Quan, T.; Fisher, G.J. Role of Age-Associated Alterations of the Dermal Extracellular Matrix Microenvironment in Human Skin Aging: A Mini-Review. Gerontology 2015, 61(5), 427–34. [Google Scholar] [CrossRef] [PubMed]
- Fiacco, S.; Walther, A.; Ehlert, U. Steroid secretion in healthy aging. Psychoneuroendocrinology 2019, 105, 64–78. [Google Scholar] [CrossRef]
- Maninger, N. Neurobiological and neuropsychiatric effects of dehydroepiandrosterone (DHEA) and DHEA sulfate (DHEAS). Front Neuroendocrinol 2009, 30(1), 65–91. [Google Scholar] [CrossRef]
- Hulett, J.M. Rigor and Reproducibility: A Systematic Review of Salivary Cortisol Sampling and Reporting Parameters Used in Cancer Survivorship Research. Biol Res Nurs 2019, 21(3), 318–334. [Google Scholar] [CrossRef] [PubMed]
- Subnis, U.B. Psychosocial therapies for patients with cancer: a current review of interventions using psychoneuroimmunology-based outcome measures. Integr Cancer Ther 2014, 13(2), 85–104. [Google Scholar] [CrossRef] [PubMed]
- Vining, R.F. Salivary cortisol: a better measure of adrenal cortical function than serum cortisol. Ann Clin Biochem 1983, 20 Pt 6, 329–35. [Google Scholar] [CrossRef]
- Gozansky, W.S. Salivary cortisol determined by enzyme immunoassay is preferable to serum total cortisol for assessment of dynamic hypothalamic--pituitary--adrenal axis activity. Clin Endocrinol (Oxf) 2005, 63(3), 336–41. [Google Scholar] [CrossRef]
- Aardal-Eriksson, E.; Eriksson, T.E.; Thorell, L.H. Salivary cortisol, posttraumatic stress symptoms, and general health in the acute phase and during 9-month follow-up. Biol Psychiatry 2001, 50(12), 986–93. [Google Scholar] [CrossRef]
- Hulett, J.M. Religiousness, Spirituality, and Salivary Cortisol in Breast Cancer Survivorship: A Pilot Study. Cancer Nurs 2018, 41(2), 166–175. [Google Scholar] [CrossRef]
- Ahn, R.S. Salivary cortisol and DHEA levels in the Korean population: age-related differences, diurnal rhythm, and correlations with serum levels. Yonsei Med J 2007, 48(3), 379–88. [Google Scholar] [CrossRef] [PubMed]
- Izawa, S. Salivary dehydroepiandrosterone secretion in response to acute psychosocial stress and its correlations with biological and psychological changes. Biol Psychol 2008, 79(3), 294–8. [Google Scholar] [CrossRef]
- Hucklebridge, F. The diurnal patterns of the adrenal steroids cortisol and dehydroepiandrosterone (DHEA) in relation to awakening. Psychoneuroendocrinology 2005, 30(1), 51–7. [Google Scholar] [CrossRef]
- Straub, R.H. Serum dehydroepiandrosterone (DHEA) and DHEA sulfate are negatively correlated with serum interleukin-6 (IL-6), and DHEA inhibits IL-6 secretion from mononuclear cells in man in vitro: possible link between endocrinosenescence and immunosenescence. J Clin Endocrinol Metab 1998, 83(6), 2012–7. [Google Scholar] [CrossRef]
- Prom-Wormley, E.C. Genetic and environmental effects on diurnal dehydroepiandrosterone sulfate concentrations in middle-aged men. Psychoneuroendocrinology 2011, 36(10), 1441–52. [Google Scholar] [CrossRef]
- Kudielka, B.M.; Kirschbaum, C. Awakening cortisol responses are influenced by health status and awakening time but not by menstrual cycle phase. Psychoneuroendocrinology 2003, 28(1), 35–47. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R. Use of Salivary Diurnal Cortisol as an Outcome Measure in Randomised Controlled Trials: a Systematic Review. Ann Behav Med 2016, 50(2), 210–36. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.Y. Circadian rhythm characteristics of serum cortisol and dehydroepiandrosterone sulfate in healthy Chinese men aged 30 to 60 years. A cross-sectional study. Steroids 2003, 68(2), 133–8. [Google Scholar] [CrossRef]
- Laudenslager, M.L. Diurnal patterns of salivary cortisol and DHEA using a novel collection device: electronic monitoring confirms accurate recording of collection time using this device. Psychoneuroendocrinology 2013, 38(9), 1596–606. [Google Scholar] [CrossRef] [PubMed]
- Hellhammer, J. Several daily measurements are necessary to reliably assess the cortisol rise after awakening: state- and trait components. Psychoneuroendocrinology 2007, 32(1), 80–6. [Google Scholar] [CrossRef]
- Adam, E.K.; Kumari, M. Assessing salivary cortisol in large-scale, epidemiological research. Psychoneuroendocrinology 2009, 34(10), 1423–36. [Google Scholar] [CrossRef]
- Fenech, A.L. Fear of cancer recurrence and change in hair cortisol concentrations in partners of breast cancer survivors. J Cancer Surviv 2024. [Google Scholar] [CrossRef]
- Lambert, M. Behavioural, physical, and psychological predictors of cortisol and C-reactive protein in breast cancer survivors: A longitudinal study. Brain Behav Immun Health 2021, 10, 100180. [Google Scholar] [CrossRef]
- Andreano, J.M. Effects of breast cancer treatment on the hormonal and cognitive consequences of acute stress. Psychooncology 2012, 21(10), 1091–8. [Google Scholar] [CrossRef]
- Arlt, W. Frequent and frequently overlooked: treatment-induced endocrine dysfunction in adult long-term survivors of primary brain tumors. Neurology 1997, 49(2), 498–506. [Google Scholar] [CrossRef]
- van Waas, M. Adrenal function in adult long-term survivors of nephroblastoma and neuroblastoma. Eur J Cancer 2012, 48(8), 1159–66. [Google Scholar] [CrossRef] [PubMed]
- Kunz, S. Age- and sex-adjusted reference intervals for steroid hormones measured by liquid chromatography-tandem mass spectrometry using a widely available kit. Endocr Connect 2024, 13(1). [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, H. Sex- and age-specific reference intervals of 16 steroid metabolites quantified simultaneously by LC-MS/MS in sera from 2458 healthy subjects aged 0 to 77 years. Clin Chim Acta 2024, 562, 119852. [Google Scholar] [CrossRef]
- Gregory, S. Using LC-MS/MS to Determine Salivary Steroid Reference Intervals in a European Older Adult Population. Metabolites 2023, 13(2). [Google Scholar] [CrossRef]
- Supe-Domic, D. Reference intervals for six salivary cortisol measures based on the Croatian Late Adolescence Stress Study (CLASS). Biochem Med (Zagreb) 2018, 28(1), p. 010902. [Google Scholar] [CrossRef]
- Meszaros Crow, E. Psychosocial interventions reduce cortisol in breast cancer patients: systematic review and meta-analysis. Front Psychol 2023, 14, 1148805. [Google Scholar] [PubMed]
- Monaghan, P.J. Practical guide for identifying unmet clinical needs for biomarkers. EJIFCC 2018, 29(2), 129–137. [Google Scholar]
- De Nys, L. The effects of physical activity on cortisol and sleep: A systematic review and meta-analysis. Psychoneuroendocrinology 2022, 143, 105843. [Google Scholar] [CrossRef] [PubMed]
- Nys, L.D. Physical Activity Influences Cortisol and Dehydroepiandrosterone (Sulfate) Levels in Older Adults: A Systematic Review and Meta-Analysis. Journal of Aging and Physical Activity 2022, 31(2). [Google Scholar]
- Black, D.S. Mindfulness practice reduces cortisol blunting during chemotherapy: A randomized controlled study of colorectal cancer patients. Cancer 2017, 123(16), 3088–3096. [Google Scholar] [CrossRef]
- Phillips, K.M. Stress management intervention reduces serum cortisol and increases relaxation during treatment for nonmetastatic breast cancer. Psychosom Med 2008, 70(9), 1044–9. [Google Scholar] [CrossRef] [PubMed]
- Lengacher, C.A. A Large Randomized Trial: Effects of Mindfulness-Based Stress Reduction (MBSR) for Breast Cancer (BC) Survivors on Salivary Cortisol and IL-6. Biol Res Nurs 2019, 21(1), 39–49. [Google Scholar] [CrossRef]
- Matiz, A. The effect of mindfulness-based interventions on biomarkers in cancer patients and survivors: A systematic review. Stress Health 2024, 40(4), p. e3375. [Google Scholar] [CrossRef]
- Giudice, E. Relacorilant in recurrent ovarian cancer: clinical evidence and future perspectives. Expert Rev Anticancer Ther 2024, 24(8), 649–655. [Google Scholar] [CrossRef]
- Nanda, R. A randomized phase I trial of nanoparticle albumin-bound paclitaxel with or without mifepristone for advanced breast cancer. Springerplus 2016, 5(1), 947. [Google Scholar] [CrossRef]
- Brandhagen, B.N. Cytostasis and morphological changes induced by mifepristone in human metastatic cancer cells involve cytoskeletal filamentous actin reorganization and impairment of cell adhesion dynamics. BMC Cancer 2013, 13, 35. [Google Scholar] [CrossRef]

Table 1.
Studies assessing cortisol or cortisol:DHEA(S) in relation to treatment toxicities or toxicity-related outcomes in older adults with cancer.
Table 1.
Studies assessing cortisol or cortisol:DHEA(S) in relation to treatment toxicities or toxicity-related outcomes in older adults with cancer.
| Study | Study design | Cancer & treatment context | Biomarkers & matrix | Sampling window | Toxicities / AE endpoint | Main toxicity(-related) finding |
| Oh et al., 2019 [47] | Cross-sectional observational | Advanced lung cancer (mixed age; mean 64.3 ± 9.2 → includes ≥65 subset) | Salivary cortisol | Upon awakening (0, +30, +60 min) and nighttime (~21:00–22:00) | Symptom burden (MDASI), performance status (toxicity-related) | Blunted CAR and flatter diurnal slope associated with worse performance status and higher burden of multiple concurrent symptoms (including nausea cluster), indicating HPA dysregulation tracks toxicity-related symptomatology. |
| Fang et al., 2020 [50] | Case–control (post-chemotherapy patients vs age-matched controls) | NSCLC after chemotherapy (population typically older; paper notes lung cancer median diagnosis age ≈70) | Salivary DHEA, DHEA-S, and cortisol | Daytime saliva (single-timepoint per protocol) | Fatigue & depression scores after chemotherapy (toxicity-related) | Patients had reduced salivary DHEA-S vs controls; lower DHEA-S associated with higher fatigue and depression after chemo—supporting relevance of the cortisol/DHEA(S) axis to post-treatment symptom toxicity. |
| Cruz et al., 2022 [21] | Cross-sectional | Head & neck cancer (HNC; adult cohort with older subset) | Nighttime salivary cortisol | Nighttime (single sample per protocol) | Quality of life (UW-QOL) and perceived stress (toxicity-related) | Higher nighttime cortisol associated with worse quality of life and higher perceived stress, consistent with cortisol dysregulation mapping onto toxicity-related well-being impairments in HNC. |
| Morrow et al., 2002 [52] | Repeated-measures within-subject | Ovarian cancer receiving cisplatin/carboplatin (disease predominantly in older women; median diagnosis age ≈63) | Serum cortisol (total) | Serial samples pre-infusion and hourly for 6 h across two chemotherapy cycles | Acute CINV (nausea/vomiting; treatment toxicity) | Serum cortisol fell immediately after platinum infusion (vs control day), supporting a direct chemo–HPA interaction potentially relevant to CINV pathophysiology. |
| Hursti et al., 1993 [53] | Observational | Cisplatin-treated ovarian cancer (adults incl. 65 years or older) | Nocturnal urinary cortisol | Night prior to chemotherapy | CINV (vomiting ± nausea) | Lower pre-chemo nighttime cortisol predicted more severe cisplatin-induced nausea/vomiting in 42 patients |
| Fang et al., 2020 [50] | Cross-sectional case-control | Advanced NSCLC after chemotherapy (adults incl. older) | Salivary DHEA & DHEAS & cortisol | Single post-chemo sampling | Fatigue and depression scores | Lower DHEAS associated with higher fatigue and depression after chemotherapy vs. controls; patients had reduced DHEA/DHEAS post-chemo. |
| Toh et al., 2019 [54] | Prospective cohort | Early breast cancer receiving adjuvant chemotherapy (mixed ages; includes older subset though mean ~49) | Plasma DHEAS & DHEA (UHPLC-MS/MS) | Pre-chemotherapy baseline | CRCI (FACT-Cog domains) during & after therapy | Higher pre-chemo DHEAS predicted lower odds of CRCI (verbal fluency, mental acuity) over treatment; DHEA not predictive. |
| Toh et al., 2022 [55] | Longitudinal cohort | Early breast cancer on anthracycline-based chemo (adults incl. older subset) | DHEA, DHEAS, estradiol (plasma) | Pre-, during, and post-chemo | CRCI trajectories | Within-patient DHEA(S) variations tracked with cognitive symptom trajectories across treatment. |
| Lundström et al., 2003 [56] | Cross-sectional | Advanced cancer, predominantly gastrointestinal canccer (mixed sites; adults incl. older) | Urinary free cortisol | Single timepoint | Symptom scores (fatigue, appetite loss, nausea/vomiting) | Higher endogenous cortisol correlated positively with fatigue, appetite loss, nausea/vomiting—toxicity-related symptom burden in advanced disease. |
| Cash et al., 2024 [25] | Prospective | Head and neck cancer - most patients >50 years (some 65+), late-stage oral/oropharyngeal cancer | Cortisol (salivary) - diurnal slope, mean, waking, evening levels | Twice daily for 6 consecutive days during diagnostic/treatment planning | Progression-free survival (treatment outcomes, not toxicity) | Elevated evening cortisol and diurnal mean cortisol associated with shorter progression-free survival |
Note. CAR = cortisol awakening response; CINV = chemotherapy-induced nausea and vomiting; CRCI: cancer related cognitive impairment; DHEA-S = dehydroepiandrosterone sulfate; HPA = hypothalamic–pituitary–adrenal; MDASI = M.D. Anderson Symptom Inventory; NSCLC = non-small-cell lung cancer; QOL = quality of life; UW-QOL = University of Washington QOL.
Table 2.
Translational roadmap for HPA-axis biomarkers in older adults with cancer.
| Phase | Objective | Key Actions | Expected Outputs |
|---|---|---|---|
| 1. Methodological standardization | Establish uniform, reproducible biomarker protocols | - Select salivary or serum cortisol and DHEA(S) as preferred matrices, depending on analytic tools and study objectives - Define minimum sampling protocol - Standardize pre-analytical variables (e.g., awakening time, corticosteroid use) - Employ validated assays (e.g., LC-MS/MS or calibrated immunoassays) - Stratify data by age, sex, cancer type, and treatment phase |
- Harmonized biomarker assessment protocol - Age- and treatment-specific reference ranges - Enhanced cross-study comparability |
| 2. Prospective Validation | Demonstrate predictive validity for treatment-related toxicity in older adults | - Recruit ≥65-year-old treatment-naïve patients - Collect cortisol and DHEA(S) ratio (baseline, mid-, post-treatment) - Assess toxicity endpoints: DLTs, dose reductions, hospitalizations, functional decline - Adjust for frailty, comorbidities, polypharmacy - Track adherence and patient burden |
- Predictive models incorporating cortisol:DHEA(S) ratio - Risk thresholds for toxicity stratification - Real-world feasibility and compliance data |
| 3. Interventional Trials | Test whether modifying HPA-axis dysregulation improves outcomes | - Identify patients with abnormal HPA profiles - Randomize to behavioural interventions (e.g., CBT, yoga, exercise) or pharmacologic agents - Embed serial biomarker sampling and toxicity tracking - Evaluate toxicity, functional, and QoL outcomes |
- Evidence for causal role of cortisol:DHEA(S) ratio - Demonstration of biomarker-guided toxicity reduction - Interventional proof-of-concept |
| 4. Clinical Integration | Embed biomarkers into oncology care pathways | - Pilot salivary sampling in pre-treatment geriatric assessments - Integrate cortisol/DHEA(S) features into existing tools (e.g., CARG, CRASH) or new endocrine-resilience indices - Develop EHR-integrated decision-support tools - Conduct implementation-effectiveness studies |
- Clinical workflows incorporating HPA-axis assessment - Improved patient stratification and individualized supportive care - Reduced toxicity and treatment discontinuation rates |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



