
Submitted:
09 October 2025
Posted:
11 October 2025
You are already at the latest version
Abstract
Lamivudine/dolutegravir (3TC/DTG) is effective and safe for most people with HIV infection (PWH) who are virologically suppressed, but specific individual’s characteristics, such as previous detection of archived resistance-associated mutations (RAMs) to 3TC and prior HBV infection, could represent a risk for virological failure (VF). We conducted a retrospective monocentric cohort study to assess rates and predictors of treatment discontinuation (TD) and VF in PWH switched to 3TC/DTG after reaching virological suppression (HIV-RNA<50 cp/mL). Overall, 188 PWH were included. Over 5145 patient-years follow-up (PYFU), 16 (8.5%) PWH experienced TD (2.87 per 1000 PYFU), whereas over 5082 PYFU, 8 (4.3%) experienced VF (1.45 per 1000 PYFU). Probabilities of TD and VF were 1.3%, 2.8%, 7.5%, 12.9%, 34.5% and 0.6%, 2.7%, 2.7%, 4.2%, 22.3% after 1, 2, 3, 4 and 5 years respectively. Independent predictors of VF were a detectable baseline HIV-RNA of 20-49 copies/ml (versus<20 copies/ml, aHR 9.11, 95 % CI 1.05-79.40; p= 0.046), and a higher GSS-score for 3TC (per 10 points more, aHR 1.57, 95 % CI 1.07-2.29; p= 0.023), with a borderline significance for anti-HBcAg positive serostatus (versus negative, aHR 8.88, 95 % CI 0.89-88.45; p= 0.062). After adjustment for age and gender, those with anti-HBcAg positivity who switched from a tenofovir-containing regimen had the highest risk of VF (versus negative anti-HBcAg and no prior tenofovir use, aHR 15.06, 95% CI 1.40-161.38; p-value= 0.025).
Keywords:
HIV infection
; antiretroviral therapy
; occult HBV infection
; dual ART
; virological failure
1. Introduction
Dual antiretroviral (ART) regimen with dolutegravir (DTG) and lamivudine (3TC) represents a favourable option both as a first line regimen and as a simplification strategy in selected people living with Human Immunodeficiency Virus (PWH) [1]. For ART-naïve PWH, contraindications to this regimen are high viral load and previous failure with tenofovir/emtricitabine Pre-Exposure Prophylaxis (PrEP), while, for treatment experienced patients, 3TC/DTG should only be considered in PWH with no history of resistances to nucleoside reverse transcriptase inhibitors (NRTI) and/or integrase strand transfer inhibitors (INSTI) [1,2]. Current guidelines recommend against this regimen in case of Hepatitis B Virus (HBV) coinfection, defined by HBsAg-positivity, while isolated anti-HBcAg positivity, marker of a previous exposure to HBV infection, is not an absolute contraindication [3,4]. The synergistic effect of HIV and active HBV coinfection is widely recognized, and is characterized by worse immune recovery, higher rates of virological failures on ART, increased signs of chronic immune activation and more frequent undesirable HBV related outcomes [3,4,5,6]. Some authors have also been consistently describing worse control of HIV infection with 3TC/DTG in PWH with isolated anti-HBcAg positivity [3,4]. Due to conflicting data [7,8,9,10,11,12,13,14,15], the relevance of archived resistance associated mutations (RAMs) to 3TC on 3TC/DTG effectiveness is also debated.
Our goal was to assess rates and predictors of virological failure (VF) and treatment discontinuation (TD) with 3TC/DTG in our cohort of PWH, with particular focus on the role of resistance mutations and anti-HBcAg serostatus.
2. Materials and Methods
We conducted a retrospective cohort study in a 3rd level University hospital in Pisa, Italy. Adult (≥18 years-old) PWH on stable ART were considered eligible for study participation if they underwent a switch to 3TC/DTG after reaching virological suppression (HIV-RNA<50 copies/mL) from the 1st of January 2015 to 31st of December 2023. Exclusion criteria were a positive HBsAg serostatus, previous exposure to 3TC/DTG and lack of at least one follow-up measurement of serum HIV-RNA. The main study objectives were time to VF (defined as two consecutive HIV-RNA>50 copies/mL, a single HIV-RNA≥200 copies/mL, or a single HIV-RNA between 50 and 200 copies/mL followed by TD and regimen intensification) and time to TD for any cause. Predictors of VF were subsequently investigated, particularly considering the role of a previous HBV infection (defined as the presence of anti-HBcAg antibodies) and the presence of archived resistance-associated mutations (RAMs) to 3TC, based on Stanford algorithm mutations scores (version 9.7). The included population was followed from the moment of the switch to 3TC/DTG (baseline, BL) up to VF and to treatment discontinuation for any cause (TD). For the virological outcome, participants were censored at the last available viral load measurement, TD, or loss to follow-up (absence of at least one HIV-RNA measurement for more than one year). Probability of VF and TD over time were evaluated by Kaplan-Meier estimator. Predictors of VF were subsequently analysed by multivariable Cox regression analysis (including all factors associated with the outcome at univariable analysis at a p-value<0.05). A post-hoc analysis was then conducted to understand if a causal role of potential occult HBV infection on time to VF was present. We analysed differences in demographical and viro-immunological characteristics among PWH with and without anti-HBcAg positive serostatus, by using Chi-square test for categorical variables and Student T-test for independent samples for continuous variables. A multivariable Cox regression model was then fitted to assess the independent role of anti-HBc positivity on VF.
3. Results
A total of 188 patients were included in our study: most were male (141, 75%), Caucasians (174, 92.5%), with a median age of 54 years (IQR 44-61 years). Sexual transmission was the most common route of HIV acquisition, with similar proportions among individuals reporting heterosexual (70, 37.2%) and same-sex sexual contacts (84, 44.7%). Median time since HIV diagnosis was 11 years (IQR 5-17 years), with a median of 9 years since ART initiation (IQR 5-16 years), and 5 years of virological suppression (IQR 3-9). Thirty-five PWH (18.6%) had a history of a previous AIDS defining condition. Complete characteristics of study population are summarized in Table 1.
The reason for treatment change was proactive switch in all cases, with 129 (68.6%) patients switching from a 2NRTIs+InSTI regimen. One hundred and twenty-eight PWH (68.1%) had experienced at least one previous VF, while 127 (67.6%) were previously exposed to five or less regimens.
Among participants with at least one genotypic resistance test available before BL (137, 72.9%), 14 (10.1%) had at least one RAM to NRTIs; RAMs to 3TC were detected in 5 (3.6%) participants, with one (0.7%) case of M184V.
Concerning HBV serostatus, most patients (74, 39.4%) were HBV-seronegative, 51 (27.1%) had an isolated anti-HBsAg positivity, 35 (18.6%) showed positivity for both anti-HBsAg and anti-HBcAg. Ten patients (5.3%) showed isolated positivity for anti-HBcAg, 18 (9.6%) had an unknown HBV serostatus.
Sixteen patients (2.87 per 1000 patient-years of follow-up or PYFU) discontinued treatment with 3TC/DTG (Figure 1a). Reasons for TD included: VF (6/16, 37.5%), switch to a long-acting regimen (2/16, 12.5%), drug-related toxicity (5/16, 31.3%), other/unknown cause (3/16, 18.7%). VF was found in 8 (1.45 per 1000 PYFU) patients (Figure 1b).
Estimated probability of time to treatment discontinuation was 1.3% (0.3-5.0) at 12 months of follow-up, 2.8% (1.1-7.4) at 24 months, 7.5% (3.7-14.8) at 36 months, 12.9% (7.0-23.3) at 48 months and 34.5% (18.2-58.9) at 60 months (Figure 1a). Estimated probability of time to virological failure was 0.6% (0.1-0.4) at 12 months, 2.7% (1.0-7.1) at 24 and 36 months, 4.2% (1.7-10.7) at 48 months and 22.3% (7.9-54.3) at 60 months (Figure 1b).
Factors independently associated with VF at multivariable analysis were a baseline HIV-RNA between 20 and 49 copies/mL (versus<20 copies/mL, aHR 9.11, 95 % CI 1.05-79.40; p-value= 0.046), and a higher GSS-score for 3TC (per 10 points more, aHR 1.57, 95 % CI 1.07-2.29; p= 0.023); a borderline significant association was found for anti-HBcAg positive serostatus (versus negative, aHR 8.88 95% CI 0.89-88.45; p= 0.062). Table 2 summarizes explored associations among other potential predictors and the virological outcome (Table 2).
Among PWH with and without anti-HBcAg positive serostatus, gender and age were significantly different, with a higher proportion of men with older age in the anti-HBcAg-positive group. Interestingly, fewer PWH in the anti-HBcAg-positive group switched from a tenofovir-containing strategy (see Table 3).
After stratifying anti-HBcAg serostatus for prior tenofovir exposure we found a 15 times fold higher risk of VF for PWH with anti-HBcAg positivity and previous exposure to tenofovir (versus negative anti-HBcAg and no prior tenofovir use, aHR 15.06, 95% CI 1.40-161.38; p-value= 0.025), whereas the effect of anti-HBcAg serostatus was markedly reduced in those not switching from a tenofovir-based therapy and did not reach statistical significance (Table 4).
4. Discussion
Dual ART regimen with 3TC/DTG was highly effective in our cohort of virologically suppressed PWH undergoing antiretroviral therapy optimization. The most recent European guidelines underline the possibility of switching to 3TC/DTG in the setting of previous VF and/or in the presence of M184I/V, whereas, concerning HBV serological status, a switch should be considered in the presence of anti-HBs antibodies (even if no absolute contraindications have been provided concerning isolated anti-HBcAg positivity). [1,2].
In our study, anti-HBcAg was associated with an almost 9-time higher risk of VF, and 15-times higher for those who discontinued tenofovir.
To date, no evidence has emerged of an increased risk of VF with 3TC/DTG in the setting of prior HBV infection. However, a large study from the Italian ICONA cohort by Malagnino et al. did find an excess of risk of VF in case of isolated anti-HBcAg positivity, irrespectively of ART regimen, even if this risk was lower compared with active HBV infection [4]. Also, another work by Malagnino et al. reported significantly fewer anti-HBcAg-positive PWH reaching the target not detected-level of HIV-RNA, compared with anti-HBcAg-negative subjects, in a cohort of people switching to 3TC/DTG; moreover, anti-HBcAg positivity was the only factor associated with an increased risk of suboptimal HIV suppression [16]. Conversely, a similar study conducted in China on 601 PWH switching to 3TC/DTG showed no differences in the proportion of PWH with non-detectable viremia after 24 months from switch [17]. Finally, in another Italian cohort of 606 virologically suppressed PWH switching to 3TC/DTG, no significant differences by HBV serostatus were observed regarding the risk of virological failure or viral blips; however, the effect of HBV serology was not adjusted for potential confounders [18].
Another unresolved issue is represented by the absence of a confirmed biological explanation for a reduction of antiretroviral therapy efficacy in the context of prior HBV exposure. Recently, replication of cryptic serum HBV-DNA was demonstrated in a cohort of anti-HBc-positive/HBsAg-negative PWH despite present tenofovir exposure [19]. However, after switching to a tenofovir-sparing regimen (mostly based on 3TC), the rate of PWH experiencing HBV-DNA>10 IU/mL increased from 12.9% at T1 to 42.6% at T2 and was predicted by a lower nadir CD4 count and the presence of cryptic HBV-DNA at baseline. Even if failure in HIV control was not specifically reported during follow-up, this study seems to support a previously proposed hypothesis [16,20] concerning the synergistic viral interplay of HIV-HBV coinfection, with the reduction of selective antiviral drug pressure or development of HBV-resistance to 3TC, causing HBV to rebound and/or replicate at low levels which, in turn, could activate HIV transcription through HBx activity [20].
In the present study, a higher risk of VF was also predicted by the presence of RAMs to 3TC at previous genotypic resistance tests. This topic has been object of extensive debate in last few years, with no definite proof of a causal effect of the most important mutation to 3TC, M184I/V, on virological outcomes. In the pilot ART-PRO clinical trial, no signal of increased VF risk at 144 week was found in a cohort of PWH with past M184I/V, but with the demonstrated absence of the mutation at screening GRT performed on HIV-DNA [21]. More recently, the SOLAR-3D clinical trial, enrolling individuals with and without a history of M184I/V (some of whom with mutation also detected at baseline genotypic test on HIV-DNA), confirmed the lack of differences in the rate of virological suppression and viral rebound at 144 weeks [22]. In contrast with these trials, one retrospective study underlined the effect of M184I/V in increasing the risk of viral rebound, especially when the mutation was present in association with at least one TAM, independently from the time of virological suppression before switch [23]. Moreover, an emulated trial from the Italian ARCA cohort showed an increased risk of failing with the dual regimen if the switch occurred within the first 6 months from virological suppression and in the presence of historical RAMs (both TAMs and isolated M184I/V), with also a non-statistically significant superior efficacy of triple therapy being reported in this setting [24]. Despite the discrepancy in these results, that could be partly attributed to the different study populations and methods, it is not possible to completely exclude the role of previously found-RAMs on the efficacy of the two-drug regimen, and caution is still advisable when considering this strategy for people with a previous history of failure, even if the overall risk of failure, especially with resistance development, remains very low [25].
Our study has clearly some limitations, primarily due to the low incidence of the virological outcome and the possibility of overfitted statistical models. Another limitation lies in the retrospective design of the study and the impossibility of capturing important data, such as patients’ adherence or, importantly, the determination of HBV-DNA at baseline and at failure (that could have supported the presence of occult HBV infection as the cause of VF). Finally, given the monocentric design, results lack generalizability.
Despite these limitations, this study partly confirms results from other cohorts about the role of RAMs on VF and adds further evidence of a potential concern on the effect of prior HBV infection when switching to a tenofovir-sparing regimen. Considering that most of next-generation treatment strategies won’t have antiviral activity on HBV infection, further evidence on this topic is now mandatory.
5. Conclusions
We found that 3TC/DTG was safe and effective coherently with the available literature. In the few cases in which VF was encountered, predictors for VF were a detectable viremia at baseline, archived RAMs to 3TC, and a positive anti-HBcAg serostatus; the latter was particularly relevant in case of pre-switch exposure to tenofovir. Despite the limitations of our study, we think that reasoning on specific viro-immunological characteristics (e.g., time of viral suppression, persistence of RAMs over time, detection of occult HBV infection) is still fundamental when considering optimization to 3TC/DTG.
Author Contributions
Conceptualization, A.B.; methodology, A.B.; validation, M.F., A.B., ML.V., L.D., M.P., and R.I.; formal analysis, A.B.; investigation, S.O., T.M., A.P.; resources, M.F. and A.B.; data curation, SO., T.M., A.P., A.B., ML.V., L.D., M.P. and R.I.; writing—original draft preparation, T.M.; writing—review and editing, A.B., T.M.; visualization, A.B.; supervision, M.F.; project administration, M.F. and A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Pisa University Hospital (protocol AHCS, version 1.0, approval date 4th of July, 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
A.B. participated in Advisory boards for ViiV Healthcare, Gilead Sciences and Merck Sharp and Dhome. M.F. received unconditional grants from Gilead and speaker honoraria from Pfizer, Menarini, Gilead, GSK, and TermoFisher. The remaining authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| HIV | Human Immunodeficiency Virus |
| HBV | Hepatitis B Virus |
| 3TC | Lamivudine |
| 3TC/DTG | Lamivudine/Dolutegravir |
| PWH | People Living with HIV |
| ART | Antiretroviral Therapy |
| VF | Virological Failure |
| RAMs | Resistance Associated Mutations |
| OBI | Occult HBV Infection |
| TD | Treatment Discontinuation |
| PYFU | Patient Year of Follow-Up |
| HR | Hazard Ratio |
| CI | Confidence Interval |
| GSS | Genotypic Susceptibility Score |
| PrEP | Pre-Exposure Prophylaxis |
| MSM | Males who have Sex with Males |
| HCV | Hepatitis C Virus |
| IDU | Intravenous Drug Users |
| NRTI | Nucleoside Reverse Transcriptase Inhibitor |
| INSTI | Integrase Strand Transfer Inhibitor. |
References
- EACS Guidelines version 12.1, November 2024. Available at https://eacs.sanfordguide.com/. Last accessed 20/04/2025. 20 November.
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. Year. Available at https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv. Last accessed 20/04/2025.
- Sarmati, Loredana, and Vincenzo Malagnino. “HBV Infection in HIV-Driven Immune Suppression.” Viruses vol. 11,11 1077. 19 Nov. 2019. [CrossRef]
- Malagnino, Vincenzo et al. “Association between markers of hepatitis B virus infection and risk of virological rebound in people with HIV receiving antiretroviral therapy.” HIV medicine vol. 25,10 (2024): 1101-1111. [CrossRef]
- Thornton, Alicia C et al. “Hepatitis B, hepatitis C, and mortality among HIV-positive individuals.” AIDS (London, England) vol. 31,18 (2017): 2525-2532. [CrossRef]
- Rajbhandari R, Jun T, Khalili H, Chung RT, Ananthakrishnan AN. HBV/HIV coinfection is associated with poorer outcomes in hospitalized patients with HBV or HIV. J Viral Hepat. 2016 Oct;23(10):820-9. Epub 2016 Jun 13. PMCID: PMC5028254. [CrossRef] [PubMed]
- Soo-Yon Rhee, Matthew J. Gonzales, Rami Kantor, Bradley J. Betts, Jaideep Ravela, and Robert W. Shafer (2003) Human immunodeficiency virus reverse transcriptase and protease sequence database. Nucleic Acids Research, 31(1), 298-303.
- Osiyemi, Olayemi et al. Efficacy and Safety of Switching to Dolutegravir/Lamivudine Versus Continuing a Tenofovir Alafenamide-Based 3- or 4-Drug Regimen for Maintenance of Virologic Suppression in Adults Living With Human Immunodeficiency Virus Type 1: Results Through Week 144 From the Phase 3, Noninferiority TANGO Randomized Trial. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America vol. 75,6 (2022): 975-986. [CrossRef]
- Underwood M, et al. Archived resistance and response to <40 c/mL & TND – DTG/3TC FDC at week 48 in SALSA. Presented at the 29th Conference on Retroviruses and Opportunistic Infections (CROI), February 12-16, 2022, Virtual Event. Poster.
- SOLAR-3D: Wk 144 Results of Switching to DTG/3TC in Virologically Suppressed Heavily Treatment–Experienced People With HIV. Presented at CCO Official Conference Coverage of AIDS 2024, the 25th International AIDS Conference; July 22-26, 2024; Munich, Germany.
- Kabra M, Barber TJ, Allavena C, Marcelin AG, Di Giambenedetto S, Pasquau J, Gianotti N, Llibre JM, Rial-Crestelo D, De Miguel-Buckley R, Blick G, Turner M, Harrison C, Wynne T, Verdier G, Parry CM, Jones B, Okoli C, Donovan C, Priest J, Letang E. Virologic Response to Dolutegravir Plus Lamivudine in People With Suppressed Human Immunodeficiency Virus Type 1 and Historical M184V/I: A Systematic Literature Review and Meta-analysis. Open Forum Infect Dis. 2023 Oct 27;10(11):ofad526. PMCID: PMC10686367. [CrossRef] [PubMed]
- Borghetti, Alberto et al. “Efficacy of Lamivudine Plus Dolutegravir vs Dolutegravir-Based 3-Drug Regimens in People With HIV Who Are Virologically Suppressed.” Open forum infectious diseases vol. 11,5 ofae198. 10 Apr. 2024. [CrossRef]
- Gagliardini, Roberta et al. “Impact of resistance mutations on efficacy of dolutegravir plus rilpivirine or plus lamivudine as maintenance regimens: a cohort study.” Journal of global antimicrobial resistance vol. 28 (2022): 274-281. [CrossRef]
- Borghetti, A et al. “Virological outcomes with dolutegravir plus either lamivudine or two NRTIs as switch strategies: a multi-cohort study.” The Journal of antimicrobial chemotherapy vol. 77,3 (2022): 740-746. [CrossRef]
- Santoro, Maria Mercedes et al. “Virological efficacy of switch to DTG plus 3TC in a retrospective observational cohort of suppressed HIV-1 patients with or without past M184V: the LAMRES study.” Journal of global antimicrobial resistance vol. 31 (2022): 52-62. [CrossRef]
- Malagnino, Vincenzo et al. “HbcAb Positivity as a Risk Factor for Missing HIV RNA Undetectability after the 3TC+DTG Switch.” Viruses vol. 16,3 348. 23 Feb. 2024. [CrossRef]
- Fu J, Biao R, Liu Y, Chen J, Zhao H. 24-month outcomes after switching to Dolutegravir/Lamivudine in people living with HIV and HbcAb positivity at the Beijing Ditan Hospital in China. Ann Med. 2025 Dec;57(1):2470957. Epub 2025 Feb 24. PMCID: PMC11852214. [CrossRef] [PubMed]
- Salvo PF, Ciccullo A, Visconti E, Lombardi F, Torti C, Di Giambenedetto S, Baldin G. Impact of HBV serological status on HIV virological efficacy of two-drug antiretroviral regimens: A retrospective observational study on virologically suppressed people with HIV switching to lamivudine/dolutegravir. HIV Med. 2025 Feb 5. Epub ahead of print. [CrossRef] [PubMed]
- Salpini, Romina et al. “Kinetics of hepatitis B virus replication in anti-HBc positive/HbsAg-negative people with HIV switching to tenofovir sparing therapy.” International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases vol. 150 (2025): 107294. [CrossRef]
- Gómez-Gonzalo, M et al. “The hepatitis B virus X protein induces HIV-1 replication and transcription in synergy with T-cell activation signals: functional roles of NF-kappaB/NF-AT and SP1-binding sites in the HIV-1 long terminal repeat promoter.” The Journal of biological chemistry vol. 276,38 (2001): 35435-43. [CrossRef]
- De Miguel Buckley R, Rial-Crestelo D, Montejano R, Pinto A, Jimenez-Gonzalez M, Lagarde M, Esteban-Cantos A, Aranguren-Rivas P, Cadiñanos J, Bisbal O, Castro JM, Santacreu-Guerrero M, Bermejo-Plaza L, Moreno V, Hernando A, Martín-Carbonero L, Rubio R, Delgado R, Arribas JR, Pulido F; Antiretroviral Treatment Guided by Proviral Genotype (ART-PRO) Study Group. Long-term Evaluation of Residual Viremia in a Clinical Trial of Dolutegravir Plus Lamivudine as Maintenance Treatment for Participants With and Without Prior Lamivudine Resistance. Open Forum Infect Dis. 2022 Nov 8;9(11):ofac610. PMCID: PMC9697602. [CrossRef] [PubMed]
- Blick G, Cerreta-Dial E, Mancini G, Cosenza A, Fang L. No confirmed virological failures (CVF) for 144 weeks when switching 2-/3-/4-drug ART to DTG/3TC in heavily treatment-experienced PLWHA with prior M184V/I and multiple virological failures in the prospective SOLAR-3D study. Slides presented at: International AIDS Conference; July 22–26, 2024; Munich, Germany. 22 July.
- Borghetti A, Giacomelli A, Borghi V, Ciccullo A, Dusina A, Fabbiani M, Rusconi S, Zazzi M, Mussini C, Di Giambenedetto S. Nucleoside Reverse-Transcriptase Inhibitor Resistance Mutations Predict Virological Failure in Human Immunodeficiency Virus-Positive Patients During Lamivudine Plus Dolutegravir Maintenance Therapy in Clinical Practice. Open Forum Infect Dis. 2021 Mar 6;8(7):ofab103. PMCID: PMC8314943. [CrossRef] [PubMed]
- Borghetti A, Ciccullo A, Lombardi F, Giannarelli D, Passerotto RA, Lamanna F, Carcagnì A, Farinacci D, Dusina A, Baldin G, Zazzi M, Di Giambenedetto S. Efficacy of Lamivudine Plus Dolutegravir vs Dolutegravir-Based 3-Drug Regimens in People With HIV Who Are Virologically Suppressed. Open Forum Infect Dis. 2024 Apr 10;11(5):ofae198. PMCID: PMC11055392. [CrossRef] [PubMed]
- Marcelin AG, Soulie C, Wirden M, Barriere G, Durand F, Charpentier C, Descamps D, Calvez V. Emergent resistance-associated mutations at first- or second-line HIV-1 virologic failure with second-generation InSTIs in two- and three-drug regimens: the Virostar-1 study. J Antimicrob Chemother. 2025 Jan 3;80(1):95-101. PMCID: PMC11695916. [CrossRef] [PubMed]
Figure 1.
Estimated probability of time to treatment discontinuation (a) and time to virological failure (b).
Figure 1.
Estimated probability of time to treatment discontinuation (a) and time to virological failure (b).
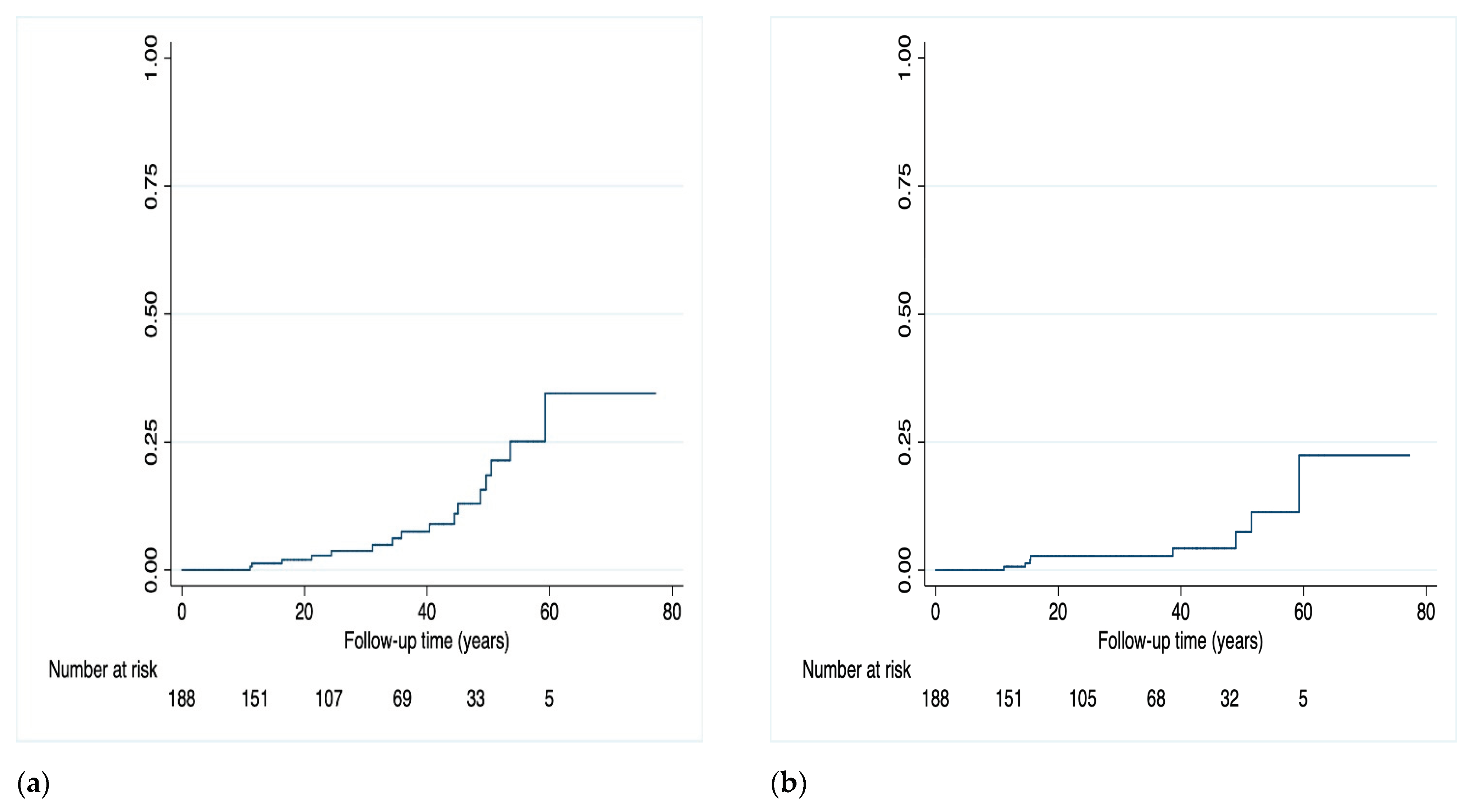

Table 1.
Cohort demographic and immunological and virological data.
| Population | N=188 (% or IQR) |
|---|---|
| Male gender (%) | 141 (75.0) |
| Age, years (IQR) | 54 (44-61) |
|
Ethnicity (%) Caucasians Africa-Sub-Saharan South America Asians |
174 (92.5) 4 (2.1) 7 (3.7) 3 (1.6) |
|
HIV acquisition, risk factor (%) Heterosexual men and women MSM People who inject drugs (PWID) Other/unknown |
70 (37.2) 84 (44.7) 14 (7.5) 20 (10.6) |
| Time since HIV diagnosis, years (IQR) | 11 (5-17) |
| Time since ART initiation, years (IQR) | 9 (5-16) |
| Years of virological suppression (IQR) | 5 (3-9) |
| Previous AIDS event, at least one (%) | 35 (18.6) |
| Nadir CD4+ count (cells/μL), (IQR) | 270 (144-385) |
| Baseline CD4+ count (cells/μL), (IQR) | 716 (538-920) |
|
Zenith HIV-RNA (%) <100.000 copies/mL 100,000-499.999 copies/mL ≥500.000 copies/mL |
86 (47.2) 54 (29.7) 42 (23.1) |
|
Baseline HIV-RNA (%) Target not detected Target detected <20 copies/mL 20-49 copies/mL |
110 (58.5) 62 (33.0) 16 (8.5) |
| Positive HCV-Ab serostatus (%) | 19 (10.1) |
| Number of previous therapeutic lines (IQR) | 4 (3-6) |
Table 2.
Cox regression: predictors of time to virological failure.
| HR (95% CI) | p-value | aHR (95% CI) | p-value | |
|---|---|---|---|---|
| Age (per 10 years more) | 1.02 (0.54-1.91) | 0.953 | - | - |
| Sex (female vs male) | 0.44 (0.05-3.60) | 0.440 | - | - |
| Nadir CD4 count | 0.99 (0.99-1.00) | 0.110 | - | - |
| Zenith HIV-RNA | 0.99 (0.99-1.00) | 0.607 | - | - |
| Years with HIV | 1.00 (0.92-1.08) | 0.919 | - | - |
| Years of virological suppression | 0.88 (0.72-1.07) | 0.205 | - | - |
| Baseline HIV-RNA 20-49 copies/ml (versus <20 copies/mL) | 5.67 (1.10- 9.39) | 0.039 | 9.11 (1.05-79.40) | 0.046 |
| GSS*-3TC** (per 10 points more) | 1.74 (1.23-2.48) | 0.002 | 1.57 (1.07-2.29) | 0.023 |
| Pre-switch tenofovir exposure | 1.87 (0.44-7.84) | 0.395 | - | - |
| Anti-HBcAg + (vs negative) | 5.76 (1.26-26.24) | 0.024 | 8.88 (0.89-88.45) | 0.062 |
|
HBV serology: - AntiHBcAg-/AntiHBsAg- - AntiHBcAg-/AntiHBsAg+ - AntiHBcAg+/AntiHBsAg+ - AntiHBcAg+/Anti HBsAg- |
- 1.43 (0.41-5.02) 1.71 (0.41-7.23) 2.69 (0.31-3.30) |
- 0.574 0.466 0.368 |
- - - - |
- - - - |
* GSS: genotypic susceptibility score.
Table 3.
Population characteristics according to anti-HBcAg serostatus and risk of virological failure.
Table 3.
Population characteristics according to anti-HBcAg serostatus and risk of virological failure.
| Anti-HBcAg + n=45 (%) | Anti-HBcAg - n=135 (%) | p-value | |
|---|---|---|---|
| Sex (male) | 41 (91.1) | 95 (70.3) | 0.005 |
| Age (years, IQR) | 58 (55-61) | 52 (50-54) | 0.002 |
|
Risk factor Hetero MSM IDU Other/Unknown |
11 (24.4) 23 (28.1) 3 (6.6) 8 (1.7) |
55 (40.7) 59 (43.7) 10 (7.4) 11 (8.1) |
0.120 |
| Years with HIV (IQR) | 14.43 (11.64-17.23) | 11.74 (10.31-13.18) | 0.072 |
| Years of suppression (IQR) | 7.27 (5.37-9.18) | 5.85 (5.09-6.62) | 0.101 |
| CD4 baseline (IQR) | 644 (493-857) | 734 (548-947) | 0.109 |
| HIV-RNA detectable (20-49 copies/mL) | 4 (8.8) | 11 (8.1) | 0.987 |
| Tenofovir exposure pre-switch | 15 (33.3) | 72 (53.3) | 0.020 |
| Previous virological failure | 13 (28.8) | 32 (23.7) | 0.651 |
| 3TC* resistance associated mutations | 2 (4.4) | 3 (2.2) | 0.695 |
Table 4.
Cox regression for risk of virological failure per anti-HBcAg serostatus and previous tenofovir exposure.
Table 4.
Cox regression for risk of virological failure per anti-HBcAg serostatus and previous tenofovir exposure.
| aHR (95% CI) | p-value | |
|---|---|---|
|
Previous tenofovir use and occult infection: - No prior tenofovir plus anti-HBcAg– - Prior tenofovir plus anti-HBcAg – - No prior tenofovir plus anti-HBcAg+ - Prior tenofovir plus anti-HBcAg+ |
Reference 1.51 (0.13-16.92) 2.62 (0.14-47.41) 15.06 (1.40-161.38) |
Reference 0.738 0.513 0.025 |
| Age (per 10 years more) | 0.93 (0.43-2.04) | 0.859 |
| Sex (female vs. male) | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



