
Submitted:
09 October 2025
Posted:
10 October 2025
You are already at the latest version
Abstract
Physiotherapy is a clinical discipline that provides services in healthcare centres, the community, the home, and the school. School Physiotherapy (SP) focuses its practice on children with disabilities or special motor needs during the school period. SP addresses issues of psychomotricity, ergonomics, and posturology in order to improve health and academic performance. The objective of this study is to identify qualitative evidence on the experience/opinions of physiotherapists, children, parents, and teachers regarding SP services. Methods: Metasynthesis of qualitative studies. The search included articles published between 2015 and 2025 on the PubMed, WOS, SCOPUS and CINAHL databases. Results: 698 articles were found through the initial search, of which only 17 were included in the thematic synthesis. Three main themes emerged from this analysis: (1) Clinical and school physiotherapy: separated by a fine line. (2) Ensuring healthcare for children with specific conditions in schools. (3) The challenge of incorporating SP in educational settings. Conclusions: SP plays a vital role in supporting children with disabilities and special needs in schools, but there is a lack of evidence supporting its implementation and its impact on academic performance. The absence of clear guidelines and competencies expose SP to professional intrusion and hinders its integration into educational teams. Understanding the experiences of those involved may help improve SP practice.
Keywords:
physiotherapy
; school health
; special needs
; physiotherapy services
; qualitative research
1. Introduction
Physiotherapy is an autonomous profession whose objective is to prevent, develop, and maintain movement and functional abilities in patients and communities. According to the World Confederation for Physical Therapy, the practice of the profession varies depending on the healthcare system, facilities, regulations, and resources of each country [1]. Although physiotherapy is essentially a clinical discipline, carrying out the assessment, diagnosis, and treatment of patients; it currently forms part of integrated models that also provide services in the home and the school. School physiotherapy (SP) focuses its practice on children with special motor needs during the school period [2], aiming to improve their health and functional performance at school, in connection with the home and the community [3]. Many countries have educational services which include SP for children with disabilities of pre-school and school age [4]. By integrating scientific evidence, clinical experience, and patient preferences, SP provides technical aids and curricular adaptations for children with motor, ergonomic, or postural problems [5,6].
The World Confederation for Physical Therapy recognises that the practise of the profession varies according to the competencies and healthcare system of each country [7,8]. From a paradigm of school inclusion, institutions seek cooperation between the educational, healthcare, and social sectors [9]. Schools provide a unique natural environment for physiotherapists to develop motor learning strategies, neurorehabilitation, or early intervention therapies [6]. Thus, educational centres for children with neurodisabilities usually include physiotherapy, occupational therapy, and speech therapy services [3]. Since the end of the 20th century, Spain has been committed to incorporating SP into educational guidance departments. SP focuses on the care of children with special educational needs, develops physical rehabilitation programmes, physiotherapy assessment, guidance, and treatment of motor problems [10]. Teaching in the classroom is not exempt from problems related to psychomotricity, ergonomics, or posturology, which can be prevented and treated through SP services [11]. The school physiotherapist evaluates psychomotricity, movement disorders, and body structure and function across all educational stages. At the same time, they provide guidance on physical activity [12,13], reduction of sedentary behaviour [14], musculoskeletal disorders, [15], occupational health [11], exercise in specific pathologies [16], postural health, and adapted teaching in special education settings [8,17].
The interaction between healthcare and educational development has evolved in recent years [18]. The application of therapies in schools is key for children with disabilities [19], the educational team decides the frequency, intensity, and type of intervention according to the capacities of the system. The interaction between education and health has a positive impact on the academic success and quality of life of these pupils [20]; however, it is necessary to document the strengths and weaknesses of SP services, the gap between ideal and actual practice [21], and to evaluate the effectiveness of programmes [5]. Although some studies have shown discrepancies regarding SP interventions [22,23], most agree on their benefits, such as improvement in children’s motor and social skills [24]. There is a lack of analysis, guidance, and evidence on SP interventions [25,26]. Clinical practice guides are needed [7], as well as the exploration of training in rehabilitation activities [27] and an understanding of the experiences of those involved in the process. Qualitative methodologies have proved useful in researching the experiences of physiotherapists, families, teachers, or children regarding SP for cerebral palsy [26], the use of standing frames [28], aquatic therapy [29] or spinal health programmes [30]. In order to improve the quality of care in educational settings, there is a need for a synthesis of aggregated data in order to obtain a deeper understanding of the use, development, strengths, and weaknesses of SP services. The objective of this study is to identify qualitative evidence on the experiences/opinions of physiotherapists, children, parents, and teachers concerning SP services.
2. Materials and Methods
2.1. Design
A systematic review, metasynthesis of qualitative studies, was performed.
2.2. Search Methods
Bibliographic searches were conducted on the PubMed, WOS, SCOPUS, and CINAHL databases for qualitative studies in English and Spanish, published between January 2015 and June 2025. The PRISMA 2020 declaration was used in this study [31], and the SPIDER method was used to help formulate the research question [32]. In order to perform the search, the search terms used were divided into three areas. First, the terms "school", "education", “students”, “primary and secondary education”, and “school health services”, were joined with the Boolean operator "OR". This search was performed with "physiotherapy", "physical therapy services", “physical therapist", “physical therapy speciality”, “physical therapy modalities”, and "qualitative research". After performing these searches separately, they were joined using the Boolean operator “AND”(((((((school) OR education)) AND (((((physiotherapy) OR Physical Therapy Services) OR Physical Therapist)) AND ((qualitative research). This search was supplemented by a search of grey literature.
2.3. Inclusion and Exclusion Criteria
Inclusion criteria: primary studies on the experiences and opinions of physiotherapists, parents, teachers, and children regarding SP services. Qualitative research papers or mixed methodology were included. Exclusion criteria: non-primary articles, editorials, or opinion pieces.
2.4. Search Results
A 5-stage selection process was performed: elimination of duplicates, title selection, abstract review, full paper review and reference tracking. A total of 698 studies were identified, however, only 17 articles were included in this review (Figure 1).
2.5. Data Extraction
Three authors (GGH, NSL, and SNN) independently performed data extraction, discussed the controversies found, and reached an agreement; the references of seventeen included papers were reviewed (Figure 1).
2.6. Quality Assessment
Each primary study was assessed using the Joanna Briggs Institute’s Qualitative Assessment Rating Instrument (QARI) [33]. The included articles were considered to be of high quality with respect to objectives, design, analysis, and results, providing useful knowledge on the topic (Table 1). No studies were excluded after quality assessment.
2.7. Data Synthesis and Analysis
The included studies were analysed thematically. The synthesis was undertaken by (GGH and NSL), and verified by (SNN). One independent reviewer with expertise in SP and qualitative research verified the results. The thematic synthesis included three stages [34] (Table 2), characteristics of selected studies can be seen in Table 3.
2.8. Rigour
In order to verify the validity of the review, structured abstracts of the original studies were maintained, and it was verified whether the findings were transferable to other contexts of SP application. After the thematic synthesis, the contributions of the studies to the final analytical themes were examined.
3. Results
The seventeen qualitative studies comprised a total sample of 682 participants, 194 (28.4%) pupils, 65 (9.5%) parents/relatives, 114 (16.7%) teachers, 265 (38.8%) physiotherapists, 7 (1.0%) physiotherapist aides, 10 (1.4%) educational professionals, 10 (1.4%) political positions, and 17 (2.5%) unspecified participants. Regarding their origin, there are 4 studies from South Africa, 3 from the USA, 3 from Spain, 2 from Australia, 2 from Norway, and 1 from Israel, UK, Canada and unspecified countries. Thematic synthesis is an inductive process in which three themes and eighteen sub-themes emerge (Table 4).
3.1. Clinical and School Physiotherapy: Separated by a Fine Line
SP differs from clinical physiotherapy; SP services should represent a potential for educational improvement in pupils with disabilities. Although the whole multidisciplinary team shares the same objective, it is difficult to strike a balance between physical activity, therapy, and academic work. Educators fight for education and, physiotherapists for physiotherapy, but it is a joint task where neither is more important than the other; both must coexist:
Well, what’s the most important thing here? Is it the standing? Is it the education? Is it this bit? Is it that bit?” … It’s a very fine balancing line … constant battle between therapy and education.[28]
Physiotherapists point to a paradigm shift in SP, highlighting the difficulty of moving from a clinical model to an educational one:
I’ve been a PT for 27 years but I’ve only been in the schools for about 14. Certainly, coming from a clinic model, my first couple of years in the schools I had a really hard time to figure out how to make goals that were school-based…[35]
The introduction of physiotherapy in schools involves living with feeling under pressure while not forgetting that the goal is to improve health and education. One therapist explained:
We’re looking at supporting students in special education and benefiting from those services; we’re looking at accessing educational environments and students participating with their peers in motor activities.[35]
There is a lack of interaction, knowledge sharing, and communication between the clinical and academic fields, and this is perceived as a threat to the advancement of SP.
3.1.1. Lack of Specific Guidelines
SP is necessary when disabilities and motor problems negatively affect a pupil’s academic performance. A health problem that interferes with academic performance may require clinical physiotherapy and/or SP. However, as one physiotherapist notes, school settings lack protocols for action or specific tasks for physiotherapists:
I like that it gives nice clarity around the scope of work for a school-based physiotherapist.[8]
Our review highlights the existence of distinct guidelines, competencies, functions, and registries. As one participant states, this situation confuses physiotherapists. There is a need to organise SP practise:
Sometimes because of the wording, complexity and differences between countries, PTs might feel so overwhelmed.[8]
3.1.2. Professional Competencies and Diffuse Responsibility
Defining the professional competencies of SP poses a challenge. The ambiguity with related professions means that some essential functions that define SP are assumed by other professions. While regulations aim to standardise functions of SP, their implementation reveals gaps in accessibility, availability, and professional accountability.
Actually, it is everyone’s responsibility, so when everyone is responsible, no one takes responsibility.[19]
3.1.3. Lack of Support: Feeling Like Outsiders
School physiotherapists report a lack of support from department heads and guidance from educational coordinators. Physiotherapists must be familiar with the school; but they are sometimes forced to adapt by taking on non-clinical activities outside of their profession duties, such as supervising recess or covering shifts for other professionals. There are no job descriptions, positions, training, or specific documentation.
Most of the focus [in our school] is on education and therapists are excluded from the decisions [physiotherapist not consulted to share their views] by the DoE. … To date we do not have job descriptions and are understaffed.[7]
School physiotherapists may feel like outsiders in an educational system where the majority are teaching staff. Physiotherapists perceive insufficient training, fewer opportunities for professional development, and isolation.
Physiotherapy is secondary in the education system, even within the health professions… everyone needs to talk, so they [the students] receive speech therapy… everyone needs to write and hold a pencil, so who will teach them? An occupational therapist… and due to various misconceptions, the OT will also examine motor performance. So why bring in another clinician?[19]
3.1.4. Professional Intrusion
Some policymakers expressed concern about professional boundaries. SP may overlap with occupational therapists, developmental coaches, physical education teachers, or sports coaches. Sometimes these professionals offer physiotherapy treatments for children with motor disabilities.
There is a big problem with physiotherapy professional boundaries: where do they begin and end, who needs physiotherapy, who should be referred to a physiotherapy… I mean, it is unclear to the public but also to therapists, when should a physiotherapy or occupational therapist be consulted?...[19]
3.1.5. Pupil-Centred, Evidence Based
Beyond teachers’ opinions, school physiotherapists are trained to write measurable goals and develop evidence-based activities. As one physiotherapist with 20 years of experience in school states:
And I don’t know that there is really one great way to write goals but making sure that they’re measurable and you can actually keep data on those goals.[35]
SP should focus on the pupil, addressing their access and mobility issues during the school day. The goals are geared toward motor development, independence in movement, gait, balance, and locomotor patterns. As one physiotherapist put it:
So, if it was a clickable link, if it was an interactive document, we could digitally find more of the information in it.[8]
3.2. Ensuring Healthcare for Children with Specific Conditions in Schools
Children with specific conditions such as cerebral palsy, spinal cord problems, anatomical malformations, or recurring pain require physiotherapy support during their daily activities at school.
3.2.1. Care for Pupils with Cerebral Palsy
Children with cerebral palsy attend specialised schools that offer modified curricula along with therapy services. Their experiences with exercise are positive, improving their aerobic capacity, physical endurance, well-being, and participation in school and leisure activities. School physiotherapists state that they perceive improvements in motor skills, communication skills, and improved social relationships:
She was walking longer on the treadmill and riding her bike faster for longer periods.[16]
I think that open friendliness, that it being a little bit social as well as exercise, was a great aspect of it. And so that would make it easier for them to join in.[16]
Teachers and physiotherapists recognise the advantages of children with cerebral palsy participating in these programmes, which focus on addressing pupils’ academic and physical needs and responding to family expectations.
3.2.2. Supervising Pupils Using Standing Frames
Using standing frames for children with specific pathologies requires knowledge of their handling and complications. While classroom staff may have general skills, prolonged use, agitation, or movement of children can cause injuries or burns. Using this technology requires training for students and a multidisciplinary team; this task must be carried out by the SP.
If the children have got a lot of extraneous movement and they’re agitated, you can end up with friction burns … Sometimes it actually depends if they’ve got their second skin (dynamic lycra body suit) on, if they are tired … So you have to really know your children and know what mood they’re in as well.[28]
3.2.3. Implementing Aquatic Therapy Programmes
The inclusion of aquatic therapy programmes in schools and special education centres provides a fun and motivating form of physical activity. Physiotherapists report improvements in muscle tone and strength, motor spasticity, and breathing in children with cerebral palsy. As the physiotherapists explain:
It is an environment where it is easier to mobilize compared to dry land conditions, so, first you see what the person can do regarding mobility in the water, and then this can be applied in the classroom or the dining room, encouraging us to reinforce this.[29]
The sensory experience of being in the water enhances the pupils’ ability to perform other activities.
They pay more attention to conversations as soon as they get into the water, and then they react in the playground when something seems funny or interesting to them, they are more awake than before they get into the water.[29]
3.2.4. Prevention and Treatment of Back Problems/Pain
Knowing the consequences of poor posture helps pupils change habits and motivate them to improve their ergonomics. According to teachers, information provided through physiotherapy activities allow students to improve and prevent back pain. Pupils, parents, teachers, and principals emphasise the benefits of participating in physiotherapy workshops, such as risk awareness, pain reduction, and improved well-being. One pupil expressed the following:
The workshops have helped me to change, I have truly felt that they have been useful. In my daily life, this is noticeable and little by little, the back ache that I had starts to go away.[36]
For the pupils, the physiotherapy activities they applied most were those related to ergonomics, stretching, and proper backpack use.
I have found it very useful because before I would carry my backpack down by my bum and I would struggle, and it was hell and suddenly you said I should raise it higher, and I thought to myself “it doesn’t weigh a thing! I was very surprised.[36]
Teachers are concerned about the lack of attention to the musculoskeletal effects of immobility, excessive technology use, dangerous play, and injury prevention. There is evidence of the effectiveness of SP programmes for this problem, but teachers do not have this training:
The teachers aren’t taught about spinal health and what’s good for children and bad.[30]
3.2.5. Care and Prevention of Complications from Spinal Cord Injuries
Children and adolescents with spinal cord injuries face risks of spinal asymmetry, scoliosis, or hip dislocation, resulting in asymmetrical pressure distribution and an increased risk of pressure ulcers. There is a gap in prevention systems for these problems in schools. Paraplegic pupils are in need of training by physiotherapists for themselves and their peers, along with support from the school administration:
[Assistance through physiotherapists] … there should be the likes of … the help of the hospital physiotherapist, and the school, and other special schools, we will manage.[37]
3.2.6. Applying Mind-Body Therapies
For years, the role of physiotherapy in the care of children with mental health problems has been highlighted. Mindfulness techniques, breathing practices, body awareness, and yoga have all shown benefits for child development. Teachers and pupils report that the mindfulness and body awareness work developed by physiotherapists help children concentrate. As one teacher sees it:
For example, when doing homework, they can focus more; they used to chatter a lot. They can sit better and have a better posture. Like, in sorting out arguments and stuff, they already talk about it differently, and at some point, you gotta say, “F [referring to the physical therapist] comes with this and that…” [referring to the fact that she reminds them of what they’ve learned with the physical therapist, and it’s helped them to chill out].[38]
Guided imagery activities also help develop their imagination of other places outside the classroom. They feel like they can explore other spaces, feel other emotions, and share them in a group or at home.
3.2.7. Addressing Minor Motor Limitations
Children with Developmental Coordination Disorder (DCD) and Autism Spectrum Disorder (ASD) are not considered to have motor disabilities but have unrecognised physiotherapy needs. This represents a gap that school physiotherapists must address:
Children with DCD are not eligible for physiotherapy at school or child development centers after the age of 6.[19]
Participants expressed concern for older children, who do not receive SP treatment beyond a certain age:
I hope older children receive services at school. I hope, but I’m not sure it happens, and I am not sure it’s enough.[19]
3.3. The Challenge of Incorporating SP in Educational Settings
This topic covers the advantages and disadvantages, strengths and weaknesses of incorporating physiotherapists into specialised school settings.
3.3.1. Integrating Therapy Into Curriculum
The availability of specialised staff facilitates physical activity for children with high support needs. Staff shortages limit opportunities for pupils to remain physically active. As one parent notes, physiotherapists are recognised as “physical activity experts” in the school setting.
The most important thing is that the school has specialists . . . because if it didn’t then the opportunity to do physical activity would be limited.[39]
Parents comment that their children participate enthusiastically in activities when directed or suggested by physiotherapists:
. . . if she [physiotherapist] says ‘come on I want you to get up and go and walk around the school seven times’, [name] will go ‘okay, I’ll do it eight times for you’.[39]
3.3.2. Meeting Physiotherapy Needs in Special (and Regular) Education Schools
The school focuses on education; curricular demands prevent teachers from considering pupils’ other needs. Teachers feel they must focus on teaching and learning activities; they lack the time, capacity, or confidence to address the health needs of certain pupils.
Our work has to be done, books has to be marked, assessments have to be done and marked and moderated and all of those so we don’t have time. We can’t worry about their spines because we are worried about what they’re learning.[40]
SP could address these demands, but it is excluded from the department’s decisions. Nor is there a perceived political commitment to change this situation beyond special education. From this premise, our review opens the challenge of incorporating SP into regular education.
Implementing this model to mainstream schools means that physical therapists should be in the general (mainstream schools), and so it’s kind of new thought, so I think it’s going to be challenging.[8]
Policymakers believe that some treatment for children with motor disabilities should be provided in special education settings; they are skeptical about its extension into regular education.
Children with motor disabilities receive physiotherapy in special education schools. I don’t know whether to say that it is full, but certainly in special education schools there are physiotherapists who take care of these children... those in mainstream education should also receive physiotherapy at school, but it doesn’t always happen. And if not in school, then where do they get it, I don’t know.[19]
3.3.3. Training Teachers and Other Professionals
For educational staff, it is important to attend physiotherapy sessions and practise the physiotherapist’s teachings. This way, they feel more motivated to dedicate time to certain techniques in class. For teachers, it would be advisable for the physiotherapist to train the teaching staff, consolidating what they have learned in class.
And it is perfect that in parallel to this, F [the physical therapist] is also training us teachers, so I think it is an action, and the good thing is that it is a very global intervention and that it is not isolated and so on… Yes, so I think it is important. I also think it is important that we can introduce it, as I said, in a transversal way in the curriculum, that teachers are given the tools to be able to do this.[38]
Physiotherapists may also supervise support staff who work with children with special needs in preschools. Support staff face difficulties when handling children to prevent fractures or injuries, assisting with position changes or transferring from a wheelchair to a standing device. Support staff identify training needs for managing children with cerebral palsy, and request the participation and involvement of school physiotherapists.
I conduct 99% of the child’s training, and that doesn’t feel right. But, she’s in massive need of physiotherapy, so I do it for her [the child].[41]
3.3.4. Integrating into Multidisciplinary Teams
The educational teams include pupils, parents, teachers, psychologists, occupational therapists, speech therapists, and physiotherapists. SP is committed to the integration and teamwork of all professionals. For educational team members, holistic care from multidisciplinary teams is the best option for children.
We’ve all got the same goals. I obviously fight for the education, physio fights for the physio, but I’m very mindful that there’s no point just doing 100% education in school. You need to have some therapy as well.[28]
When goals are integrated, the educational team gets involved. They monitor and report on the progress of intervention strategies. As one therapist comments:
We work really hard to integrate goals … so that the teacher … or the staff can do it after we’re gone. So that they’re working on that same goal every day and not just when we’re there.[35]
For school physiotherapists, knowing the opinions of students and parents is a key factor when it comes to involving them, setting goals, and achieving positive results in children’s treatment.
I definitely want their [students’] input [on goal development] because … if they don’t buy into it, you’re not going to go anywhere with it anyway. I like them to come up with ideas of what problems they are having with their disability and … work with them on learning what their disability is … and how we can work on it.[42]
3.3.5. Accompanying, Treating, and Supervising in Natural Settings
Observing adolescents in different settings, such as at home or in school, is an essential part of physiotherapist interventions. SP is offered in a natural setting, with the goal of facilitating the child’s participation in school by integrating therapy into their daily lives. Another advantage is that physiotherapists can monitor the child over time, enabling the early detection of problems.
By working in a school, physiotherapists have the opportunity to monitor the children’s progress over time and detect any signs of decline before they become more serious.[19]
3.3.6. Overcoming Setbacks and Coping with Difficulties
Working with adolescents who are in pain is a challenging and exhausting experience. SPs not only apply techniques, but also establish a therapeutic relationship focused on improving quality of life. When there is not enough time to care for all of the children, they rely on the multidisciplinary team and trained assistants.
I think you really have to collaborate with the other members of the team … we can’t be with a child all day every day. We don’t see the entire school day. We have lots of kids to serve … I think of specifically our kids who have a Physical Needs Assistant. That person is with them all day every day and is focused just on that one student.[42]
For physiotherapists, achieving results is associated with setting goals with children, which makes them more independent and capable of making decisions.
Some of the kids are bigger than I am and they get to the stage where they - if they’ve got knee flexion contractures, if it’s uncomfortable and they don’t want to do it, then they on’t do it.[28]
Therapists mention the need for adaptations and environmental modifications in their interventions with students. This requires quality training, including school physiotherapy in students’ practical rotations.
Related to this, some respondents from academia said it is increasingly difficult to secure good-quality rotations, especially in highly specific or innovative areas.[44]
This quality training involves incorporating new skills and breaking out of the comfort zone that many veteran physiotherapists find themselves in. The inclusion of SPs in educational teams involves a clash of skills with other professionals. Developing specific skills in each area can help address this problem.
There will be staff that will be threatened there will be teachers that are threatened! there will be occupational therapist that is threatened… it will be a real risk to implementation of this model if it’s not done correctly.[8]
Discussion
The objective of this study was to identify qualitative evidence on the experiences/opinions of physiotherapists, children, parents, and teachers regarding SP services. Previous systematic reviews have shown positive results of physical activity on health and academic performance [45]; though it may be useful to the curriculum [46], it is not always indicated for pupils with disabilities or special needs. Hence arises the role of the school physiotherapist, focused on enhancing pupils’ health and academic success [26]. While some studies describe models of SP provision in various countries [8], disparities in regulations, policies, and procedures lead to divergent practices [26,47]. This situation generates a lack of scientific evidence and hinders the capacity of SP to integrate clinical skills within the educational setting [7].
Collaboration between the health and education sector is key to the implementation of global interventions [12]. Teachers acknowledge the importance of physiotherapists’ involvement in the inclusion of pupils with physical disabilities [9]. The reviewed studies indicate that the development of motor and physical skills facilitates the development of language and numerical skills, classroom participation, and children’s interaction with their physical and social environment [48]. Teachers’ cooperation is essential to incorporating therapeutic activities into the classroom [4]; through teamwork in which physiotherapy, occupational therapy, and speech therapy converge [26]. Although most clinical competencies in physiotherapy are relevant for practice in educational settings, our study shows that criteria for practical application need to be unified. In SP, evidence-based practice has been limited by a shortage of research and the complexity of decision-making [26]. The literature corroborates the effectiveness of SP interventions in children’s motor development skills in both the short and long term [24], but institutional support is required for policy change guided by the effectiveness of interventions [25,49].
This review has highlighted the advantages of SP interventions in pupils with specific conditions such as cerebral palsy [16], the use of standing frames [28], spinal pathology and back pain [30,36], spinal cord injury [37], aquatic therapy [29], aerobic exercise [16], or mind-body therapies [38]. However, although some studies agree that SP can prevent musculoskeletal disorders [5], improve motor function, and support academic performance [50]; discrepancies also emerge, such as the use of manipulative therapy in spinal pain [22]. Studies agree that there is a lack of information about which pupils require therapy [3], the cost-effectiveness of interventions [23] and confidence in their routine implementation in schools [6]. Studies show a gap between ideal/actual practice [21]; underlining the need for deep reflection on the impact and empirical basis of SP interventions [25].
The results of this study highlight the need to integrate health promotion and therapy into the curriculum. SP participation is required in the design of services [8], adaptation and promotion of exercise programmes[46], spinal health programmes[30] or school-based sedentary behaviour reduction programmes [14]. This also includes the promotion of teachers’ physical health [11,15], as well as training for teachers, teaching assistants, and other professionals within the educational setting [40]. Research on SP should focus on musculoskeletal health, rehabilitation, pain, ergonomics, and their impact on the teaching-learning process and pupils’ academic performance [17]. Overcoming these challenges implies trust among members of the educational team [51], an increase in physiotherapists, materials, and specific training in SP [19,20]. Teachers and parents agree on the advantages of introducing and integrating SP into the curriculum [39], considering collaboration between health professionals, education, the home, and the school as key [43].
Limitations
The credibility of metasynthesis lies in finding, extracting, and analysing qualitative data from studies using a systematic method of revision. Transferability may be limited because school systems, curriculum, and SP competencies are highly diverse. The authors of this study have worked with children in special needs, but have not carried out the role of school physiotherapist within schools.
5. Conclusions
Although there is evidence supporting various SP interventions, on its own it is insufficient to guide practice. The lack of guidelines, competencies, and clearly defined responsibilities expose SP to professional intrusion, a lack of support, and limited integration into educational teams. SP can ensure healthcare provision for children with specific pathologies and needs within schools; however, studies are needed on its impact on educational improvements and academic performance in the short and long term. The integration of SP services into educational settings continues to be a challenge. Future research should evaluate the effectiveness of most SP approaches and interventions. Understanding the opinions and experiences of participants in SP programmes provides information on the practice, and helps identify the strengths and weaknesses of these services.
Author Contributions
Conceptualization, G.G.H., S.N.N.; methodology, R.F.G., N.S.L.; analysis, J.G.M., L.H.A.R.; resources, J.G.M.; writing—original draft preparation, G.G.H., N.S.L.; writing, review and editing, J.G.M., S.N.N.; project administration, R.F.G., L.H.A.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
Authors thank To Health Science Research Group (CTS-451), Almeria (Spain) for their support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WCPT (World Confederation for Physical Therapy). Policy Statement: Education. Proceedings of World Confederation for Physical Therapy, Geneve, UK, 2019, May 10-13.
- Cánovas, I.M.; Salazar, J. Fisioterapia Educativa: el papel del fisioterapeuta en la mejora de la coordinación óculomanual: un protocolo de intervención”. Fisioterapia y calidad de vida 2002, 1, 26–48. [Google Scholar]
- Llewellyn, G.; Maher, L. Assessment of school students’ needs for therapy services. Au J Physiother 1993, 39, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Sekerak, D.M.; Kirkpatrick, D.B.; Nelson, K.C.; Propes, J.H. Physical therapy in preschool classrooms: successful integration of therapy into classroom routines. Pediatr Phys Ther 2003, 15, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Minghelli, B. School physiotherapy programme: Improving literacy regarding postures adopted at home and in school in adolescents living in the south of Portugal. Work 2020, 67, 95–102. [Google Scholar] [CrossRef]
- Schreiber, J.; Stern, P.; Marchetti, G.; Provident, I.; Turocy, P.S. School-based pediatric physical therapists’ perspectives on evidence-based practice. Pediatr Phys Ther 2008, 20, 292–302. [Google Scholar] [CrossRef]
- Manamela, M.C.; Eksteen, C.A.; Mtshali, B.; Olorunju, S.A.S. South African physiotherapists’ perspectives on the competencies needed to work in special schools for learners with special needs. S Afr J Physiother 2021, 77, 1571. [Google Scholar] [CrossRef]
- Cinar, E.; Anaby, D.; Dostie, R.; PRISE-PT Network, Camden, C. Perspectives of international experts on collaborative tiered school-based physiotherapy service delivery. Phys Occup Ther Pediatr 2022, 42, 595–614. [CrossRef]
- Lins, F.T.; Medeiros, A.P. School inclusion of students with physical disabilities: perceptions of teachers regarding the physiotherapist´s professional cooperation. Rev. Bras. Ed. Esp. 2013, 19, 93–106. [Google Scholar]
- CGCFE (Consejo General de Colegios de Fisioterapéutas de España). Documento Marco de Fisioterapia en Educación. Available online: https://www.consejo-fisioterapia.org/adjuntos/publicaciones/publicacion_3.pdf (accessed on 4 June 2025).
- Figl-Hertlein, A.; Horsak, B.; Dean, E.; Schöny, W.; Stamm, T. A physiotherapy-directed occupational health programme for Austrian school teachers: a cluster randomised pilot study. Physiotherapy 2014, 100, 20–26. [Google Scholar] [CrossRef]
- Beresford, B.; Clarke, S.; Maddison, J. Therapy interventions for children with neurodisabilities: a qualitative scoping study. Health Technol Assess 2018, 22, 1–150. [Google Scholar] [CrossRef]
- Hartikainen, J.; Haapala, E.A.; Poikkeus, AM.; Sääkslahti, A.; Laukkanen, A.; Gao, Y.; Finni, T. Classroom-based physical activity and teachers’ instructions on students’ movement in conventional classrooms and open learning spaces. Learning Environ Res. 2023, 26, 177–198. [Google Scholar] [CrossRef]
- Ronca, F.; Burgess, P.W.; Savage, P.; Senaratne, N.; Watson, E.; Loosemore, M. Decreasing sedentary time during lessons reduces obesity in primary school children: the active movement study. Obes Facts 2024, 17, 243–254. [Google Scholar] [PubMed]
- Temesgen, M.H.; Belay, G.J.; Gelaw, A.Y.; Janakiraman, B.; Animut, Y. Burden of shoulder and/neck pain among school teachers in Ethiopia. BMC Musculoskelet Disord 2019, 20, 18. [Google Scholar] [CrossRef] [PubMed]
- Cleary, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. A qualitative evaluation of an aerobic exercise program for young people with cerebral palsy in specialist schools. Dev Neurorehabil 2017, 20, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Larose, D.; Massie, C.L.; St-Aubin, A.; Boulay-Pelletier, V.; Boulanger, E.; Lavoie, M.D.; Yessis, J.; Tremblay, A.; Drapeau, V. Effects of flexible learning spaces, active breaks, and active lessons on sedentary behaviors, physical activity, learning, and musculoskeletal health in school-aged children: a scoping review. J Act Sedentary Sleep Behav 2024, 3, 30. [Google Scholar] [CrossRef]
- Zajacova, A.; Lawrence, E.M. The relationship between education and health: reducing disparities through a contextual approach. Annu Rev Public Health 2018, 39, 273–289. [Google Scholar]
- Waiserberg, N.; Horev, T.; Feder-Bubis, P. "When everyone is responsible, no one takes responsibility": exploring pediatric physiotherapy services in Israel. Isr J Health Policy Res 2024, 13, 10. [Google Scholar]
- Jeffries, L.M.; McCoy, S.W.; Effgen, S.K.; Chiarello, L.A.; Villasante, A.G. Description of the services, activities, and interventions within school-based physical therapist practices across the United States. Phys Ther 2019, 99, 98–108. [Google Scholar]
- Clevenger, V.D.; Jeffries, L.M.; Effgen, S.K.; Chen, S.; Arnold, S.H. School-Based Physical Therapy Services: predicting the gap between ideal and actual embedded services. Pediatr Phys Ther 2020, 32, 98–105. [Google Scholar]
- Dissing, K.B.; Hartvigsen, J.; Wedderkopp, N.; Hestbæk, L. Conservative care with or without manipulative therapy in the management of back and/or neck pain in danish children aged 9-15: a randomised controlled trial nested in a school-based cohort. BMJ Open 2018, 8, e021358. [Google Scholar] [CrossRef]
- McAnuff, J.; Gibson, J.L.; Webster, R.; Kaur-Bola, K.; Crombie, S.; Grayston, A.; Pennington, L. School-based allied health interventions for children and young people affected by neurodisability: a systematic evidence map. Disabil Rehabil. 2023, 45, 1239–1257. [Google Scholar]
- Yin, X.; Zhang, D.; Shen, Y.; Wang, Y.; Wang, Z.; Liu, Y. Effectiveness of school-based interventions on fundamental movement skills in children: a systematic review and meta-analysis. BMC Public Health. 2025, 25, 1522. [Google Scholar]
- Alexander, K.E.; Clutterbuck, G.L.; Johnston, L.M. Effectiveness of school-based physiotherapy intervention for children. Disabil Rehabil 2025, 47, 1872–1892. [Google Scholar]
- Vialu, C.; Doyle, M. Determining need for school-based physical therapy under idea: commonalities across practice guidelines. Pediatr Phys Ther 2017, 29, 350–355. [Google Scholar] [PubMed]
- Webb, C.; Anderson, J. The relevance of education training for therapists in promoting the delivery of holistic rehabilitation services for young school children with disabilities in Hong Kong. Disabil Rehabil 2003, 25, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, J.; Lecouturier, J.; Smith, J.; Crombie, S.; Basu, A.; Parr, J.R.; Howel, D.; McColl, E.; Roberts, A.; Miller, K.; et al. Understanding frames: A qualitative exploration of standing frame use for young people with cerebral palsy in educational settings. Child Care Health Dev 2019, 45, 433–439. [Google Scholar] [CrossRef]
- Muñoz-Blanco, E.; Merino-Andrés, J.; Aguilar-Soto, B.; García, Y.C.; Puente-Villalba, M.; Pérez-Corrales, J.; Güeita-Rodríguez, J. Influence of aquatic therapy in children and youth with cerebral palsy: a qualitative case study in a special education school. Int J Environ Res Public Health 2020, 17, 3690. [Google Scholar]
- Louw, Q.; Kriel, R.I.; Brink, Y.; van Niekerk, S.M.; Tawa, N. Perspectives of spinal health within the school setting in a South African rural region: A qualitative study. Work 2021, 69, 141–155. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- JBI Manual for Evidence Synthesis; Aromataris, E., Lockwood, C., Porritt, K., Pilla, B., Jordan, Z., Eds.; JBI, 2024. [Google Scholar]
- JBI (Joanna Briggs Institute). Checklist for Qualitative Research. 2020. Available online: https://jbi.global/critical-appraisal-tools (accessed on 12 June 2025).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol 2008, 8, 45. [Google Scholar]
- Wynarczuk, K.D.; Chiarello, L.A.; Fisher, K.; Effgen, S.K.; Palisano, R.J.; Gracely, E.J. School-based physical therapists’ experiences and perceptions of how student goals influence services and outcomes. Phys Occup Ther Pediatr. 2019, 39, 480–501. [Google Scholar] [CrossRef]
- Blanco-Morales, M.; Abuín-Porras, V.; Romero-Morales, C.; de la Cueva-Reguera, M.; De-La-Cruz-Torres, B.; Rodríguez-Costa, I. Implementation of a classroom program of physiotherapy among spanish adolescents with back pain: a collaborative study. Int J Environ Res Public Health. 2020, 17, 4806. [Google Scholar] [CrossRef]
- Rauter, U.S.; Mathye, D. Peer support as pressure ulcer prevention strategy in special school learners with paraplegia. S Afr J Physiother 2024, 80, 2047. [Google Scholar] [CrossRef] [PubMed]
- López-Sierra, Y.; Trapero-Asenjo, S.; Rodríguez-Costa, I.; Granero-Heredia, G.; Pérez-Martin, Y.; Nunez-Nagy, S. Experiences of second-grade primary school children and their teachers in a mind-body activity program: a descriptive qualitative study. Healthcare (Basel) 2024, 12, 2095. [Google Scholar] [CrossRef] [PubMed]
- Cleary, S.; Taylor, N.F.; Dodd, K.J.; Shields, N. Barriers to and facilitators of physical activity for children with cerebral palsy in special education. Dev Med Child Neurol. 2019, 61, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D. & Louw, Q. Primary school learners’ movement during class time: perceptions of educators in the Western Cape, South Africa. BMC Public Health 2023, 23, 2501. [Google Scholar]
- Sørvoll, M.; Obstfelder, A.; Normann, B.; Øberg, G.K. Perceptions, actions and interactions of supervised aides providing services to children with cerebral palsy in pre-school settings: a qualitative study of knowledge application. Eur J Physiother 2018, 20, 198–206. [Google Scholar] [CrossRef]
- Wynarczuk, K.D.; Chiarello, L.A.; Fisher, K.; Effgen, S.K.; Palisano, R.J.; Gracely, E.J. Development of student goals in school-based practice: physical therapists’ experiences and perceptions. Disabil Rehabil. 2020, 42, 3591–3605. [Google Scholar] [CrossRef]
- Kandal, A.; Østerås, B.; Söderström, S. The multifaceted role of physiotherapy - a qualitative study exploring the experiences of physiotherapists working with adolescents with persistent pain. Physiother Theory Pract 2025, 1–12. [Google Scholar] [CrossRef]
- Walton, D.M. physiotherapists’ perspectives on the threats posed to their profession in the areas of training, education, and knowledge exchange: a pan-canadian perspective from the Physio Moves Canada Project, Part 1. Physiother Can 2020, 72, 26–33. [Google Scholar] [CrossRef]
- Daly-Smith, A.J.; Zwolinsky, S.; McKenna, J.; Tomporowski, P.D.; Defeyter, M.A.; Manley, A. Systematic review of acute physically active learning and classroom movement breaks on children’s physical activity, cognition, academic performance and classroom behaviour: understanding critical design features. BMJ Open Sport Exerc Med. 2018, 4, e000341. [Google Scholar] [CrossRef]
- Norris, E.; van Steen, T.; Direito, A.; Stamatakis, E. Physically active lessons in schools and their impact on physical activity, educational, health and cognition outcomes: a systematic review and meta-analysis. Br J Sports Med 2020, 54, 826–838. [Google Scholar] [CrossRef]
- Whitley, J.; Hollweck, T. Inclusion and equity in education: Current policy reform in Nova Scotia, Canada. Prospects 2020, 49, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Kamphorst, E.; Cantell, M.; Van Der Veer, G.; Minnaert, A.; Houwen, S. Emerging school readiness profiles: Motor skills matter for cognitive- and non-cognitive first grade school outcomes. Front Psychol 2021, 12, 759480. [Google Scholar] [CrossRef] [PubMed]
- Fortnum, K.; Furzer, B.; Reid, S.; Jackson, B.; Elliott, C. The physical literacy of children with behavioural and emotional mental health disorders: A scoping review. Ment Health Phys Act 2018, 15, 95–131. [Google Scholar] [CrossRef]
- Effgen, S.K.; McCoy, S.W.; Chiarello, L.A.; Jeffries, L.M.; Starnes, C.; Bush, H.M. Outcomes for students receiving school-based physical therapy as measured by the school function assessment. Pediatr Phys Ther 2016, 28, 371–378. [Google Scholar] [CrossRef]
- Holt, S.L.; Kuperstein, J.; Effgen, S.K. Physical therapists’ perceptions of school-based practices. Physical & Occupational Theraphy Pediatrics 2015, 35, 381–395. [Google Scholar]
Figure 1.
Flow chart.
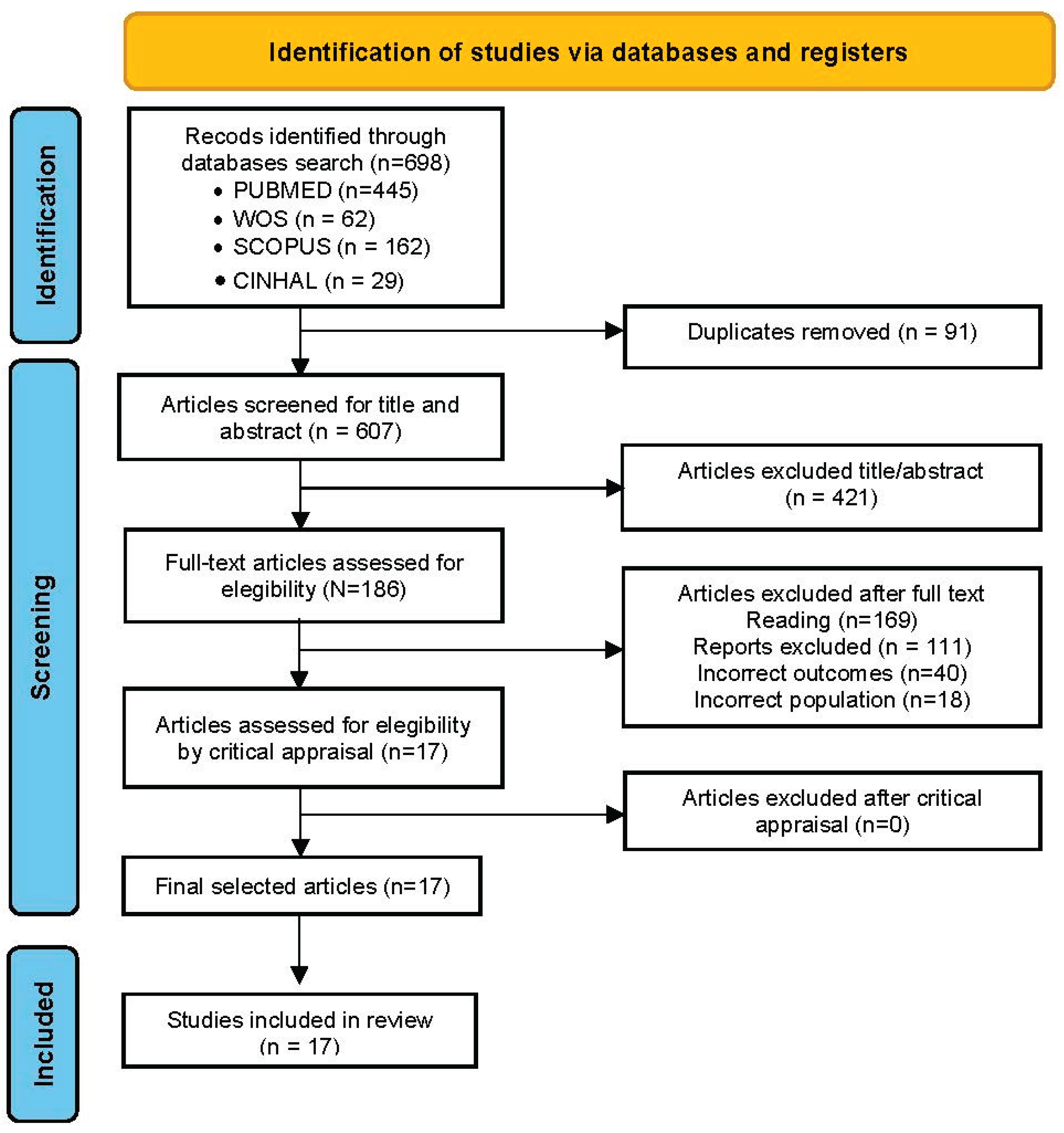

Table 1.
Quality assessment of studies.
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Cleary et al. (2017) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Sørvoll et al (2018) | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ↔ | ✔ |
| Cleary et al. (2019) | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Goodwin et al (2019) | ✔ | ✔ | ✔ | ✔ | ✔ | ✘ | ✔ | ✔ | ✔ | ✔ |
| Wynarczuk et al. (2019) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ |
| Muñoz-Blanco et al. (2020) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Walton (2020) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Blanco-Morales et al (2020) | ✔ | ↔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Wynarczuk et al. (2020) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Manamela et al. (2021) | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Louw et al., (2020) | ✔ | ↔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Cinar et al. (2022) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| López-Sierra et al., (2024) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Fisher & Lown (2023) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Rauter & Mathye (2024) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ |
| Waiserberg et al (2024) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Kandal et al (2025) | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
* ✔ Yes, ↔ Unclear, ✘ No. 1. Congruence of philosophical perspective/methodology 2. Congruence of methodology/objectives 3. Congruence of methodology/data collection 4. Congruence of methodology/data analysis 5. Congruence of methodology/interpretation of results 6. Cultural and theoretical context of the researcher. 7. Influence of the researcher on the research 8. Participants represented. 9. Research Ethics Committee Approval 10. Conclusions from data analysis/interpretation.
Table 2.
Stages in the thematic synthesis process.
| Stage | Description | Steps |
|---|---|---|
| STAGE 1 | Text coding | Recall review question Read/re-read findings of the studies Line-by-line inductive coding Review of codes in relation to the text |
| STAGE 2 | Development of descriptive themes | Search for similarities/differences between codes Inductive generation of new codes Write preliminary and final report |
| STAGE 3 | Development of analytical themes | Inductive analysis of sub-themes Individual/independent analysis Pooling and group review |
Table 3.
Characteristics of selected studies.
| Author and Year | Country | Sample | Design | Data collection |
Data analysis |
Main Theme |
|---|---|---|---|---|---|---|
| Cleary et al. (2017) | Australia | Childs (8), parents (7), teachers (6), PT (7) | Qualitative descriptive study | SSI | Thematic analysis | Benefits of an aerobic exercise programme for children with cerebral palsy |
| Sørvoll et al. (2018) | Norway | PTA (7), PT (7), Child (7) | Qualitative interpretative study | STI, observation | Theme-based content analysis | Delegating formal knowledge to non-professionals is problematic |
| Cleary et al. (2019) | Australia | Child (10), parents (13), teachers (27), PT (23) |
Qualitative descriptive study | FGs | Thematic analysis | Physical activity programmes need to take into consideration complexities |
| Goodwin et al. (2018) | UK | PT (9), EP (8), parents (9), Mixed (17) |
Qualitative study | FGs | Framework method | Training is required to ensure staff are competent in using the standing frame |
| Wynarczuk, et al. (2019) | USA | PT (20) | Qualitative descriptive study | FGs | Thematic analysis | Individualized goals influence services and optimize student outcomes. |
| Muñoz-Blanco et al. 2020 | Spain | Child CP (14), parents (8), EP (2), PT (3) |
Qualitative case study with embedded units | Non-participant observations, IDI, FGs | Thematic analysis | Aquatic therapy is an alternative treatment approach which can be applied in schools |
| Walton (2020) | Canada | PTs (116) | Qualitative study | FGs, IDI | Thematic analysis | Opportunities and threats for the development of physiotherapy |
| Blanco-Morales et al. (2020 | Spain | Child (49) Teachers (9), family (11), PT (9) | Collaborative action research | IDI, FGs, reflexive diaries, field notes | Inductive analysis | Physiotherapy activities o er students new tools to decrease their back pain and improve their health |
| Wynarczuk, et al. (2020) | USA | PT (20) | Qualitative descriptive study | FGs | Thematic analysis |
Help educational teams reflect on goal development processes |
| Manamela et al. (2021) | South Africa |
PT (22) | Mixed method research |
FGs | Thematic analysis |
Educational policies in classroom in the special educational environment |
| Louw et al. (2021) | South Africa |
Child (43), parents (17), Teachers (33) | Qualitative descriptive study | IDIs, FGs | Inductive analysis | There is a need for further engagement on school-based spinal health promotion programs |
| Cinar et al., (2022)] | Different countries (8) | PT (38) | Qualitative study | FGs | Framework method | Perspectives regarding a proposed collaborative tiered school-based PT service |
| López-Sierra et al. (2024) | Spain | Child (43), teachers (2) |
Qualitative descriptive study | IDIs, FGs | Thematic analysis | Importance of physiotherapy interventions in the school environment |
| Fisher & Lown (2023) | South Africa |
Principal (13), teachers (24) |
Qualitative descriptive study | IDIs, FGs | Inductive analysis | Policy should support teachers in implementing movement strategies in-classroom |
| Rauter & Mathye (2024) | South Africa |
Child (12) | Qualitative descriptive study | IDIs, FGs | Thematic analysis | Physiotherapists in special schools should support peer support initiatives among learners with paraplegia |
| Waiserberg et al (2024) | Israel | PT Policymakers health/education (10) | Qualitative descriptive study | IDIs | Inductive analysis | Policymakers question the provision of physiotherapy services in schools |
| Kandal et al (2025) | Norway | PT (13) | Qualitative descriptive study | FGs | Thematic analysis | Need to integrate interventions into the adolescents’ everyday lives |
PTG= Practice Guidelines. PT=physiotherapist. PTA=physiotherapist aides. PTS=physiotherapy student. EP=Educational professionals. STI=semi-structured interview. IDI=in-deep interview. FGs=Focus Group. GDs=Discussion Group. SSI=Semi Structures Interview. CP=cerebral palsy.
Table 4.
Themes and subthemes.
| Themes | Subthemes | Unit of Meaning |
|---|---|---|
| 3.1 Clinical and school physiotherapy: separated by a fine line | 3.1.1 Lack of specific guidelines | Lack of guidelines, organising practice, differences between countries |
| 3.1.2 Professional competencies and diffuse responsibility | Ambiguity of competencies, lack of accountability | |
| 3.1.3 Lack of support: feeling like outsiders | Lack of managerial support, learning by doing, decision-making, lack of laterals and personnel | |
| 3.1.4 Professional intrusion | Professional intrusion, physiotherapy, and sports. | |
| 3.1.5 Pupil-centred, evidence based | Evidence-based physiotherapy, motor skills | |
| 3.2. Ensuring healthcare for children with specific conditions in schools | 3.2.1 Care for pupils with cerebral palsy | Aerobic exercise programme, cerebral palsy, motor and psychological benefits |
| 3.2.2 Supervising pupils using standing frames | Training needs, complications, burns | |
| 3.2.3 Implementing aquatic therapy programmes | Cerebral palsy, aquatic therapy, educational enhancements | |
| 3.2.4 Prevention and treatment of back problems/pain | Ergonomics, stretching, sedentary lifestyle, class backpack | |
| 3.2.5 Care and prevention of complications from spinal cord injuries | Movement, friction, ulcer prevention | |
| 3.2.6 Applying mind-body therapies | Mindfulness, breathing, body awareness, yoga | |
| 3.2.7 Addressing minor motor limitations | Developmental disorders, coordination, autism | |
| 3.3 The challenge of incorporating SP in educational settings | 3.3.1 Integrating therapy into curriculum | Change of status, professional recognition |
| 3.3.2 Meeting physiotherapy needs in special (and regular) education schools | Time, skills, funding, security, severity, doubts, financing | |
| 3.3.3 Training teachers and other professionals | Training teachers and assistants, learning from the physiotherapist | |
| 3.3.4 Integrating into multidisciplinary teams | Educational team, common goals, technology in the classroom | |
| 3.3.5 Accompanying, treating, and supervising in natural settings | School years, identifying problems | |
| 3.3.6 Overcoming setbacks and coping with difficulties | Time, staff, objectives, training, skills |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



