
Submitted:
28 September 2025
Posted:
09 October 2025
You are already at the latest version
Abstract
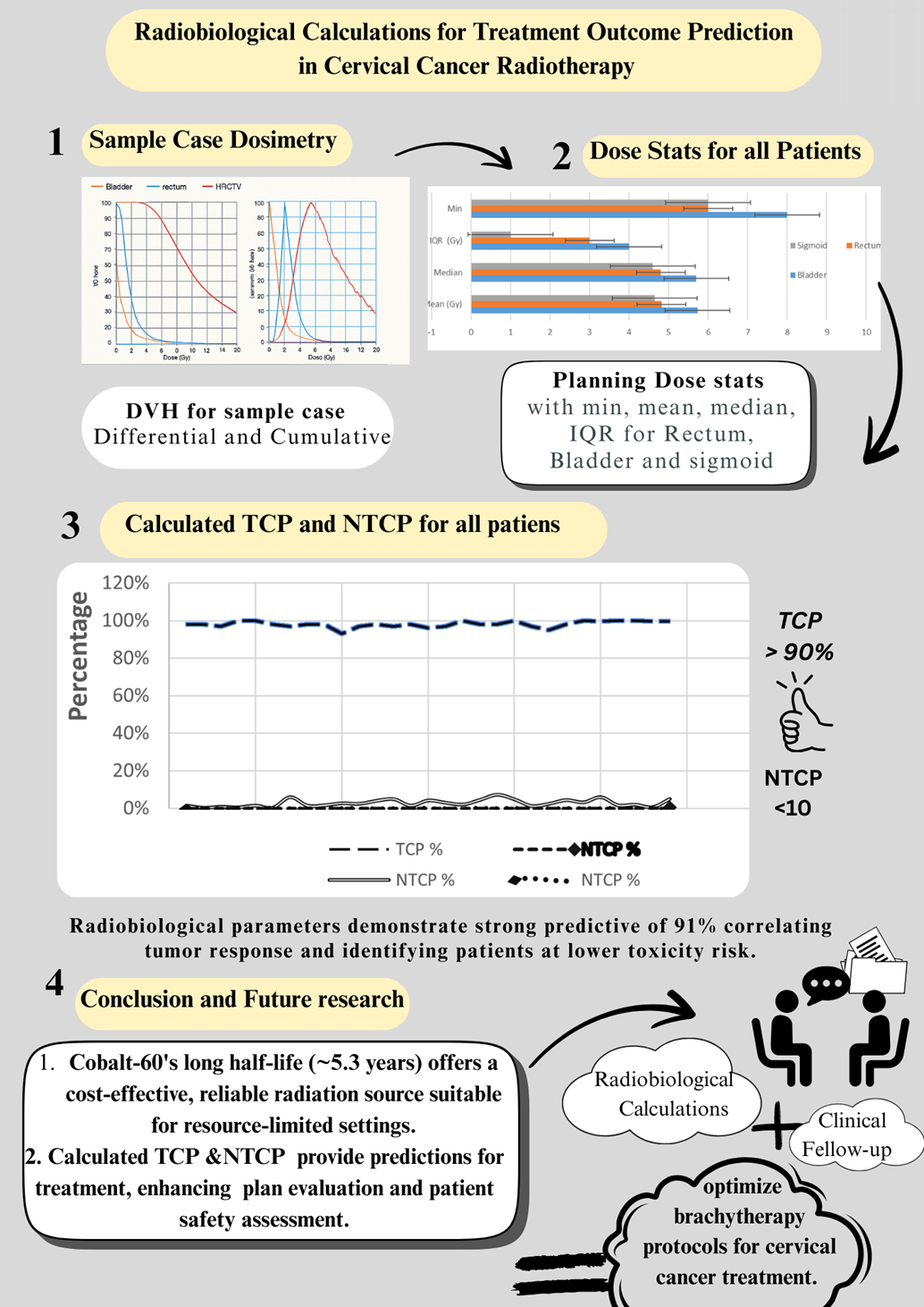
Purpose: High-dose-rate (HDR) brachytherapy remains a cornerstone in the definitive management of locally advanced cervical cancer. While conventional metrics derived from dose-volume histograms (DVHs) guide treatment planning, radiobiological modeling—using tumor control probability (TCP) and normal tissue complication probability (NTCP)—offers enhanced predictive capacity for clinical outcomes. This study evaluates the clinical applicability of TCP and NTCP models to optimize HDR brachytherapy. Materials and Methods: A retrospective dosimetric analysis was conducted on 30 cervical cancer patients (FIGO stage IIB–IIIB), treated with HDR intracavitary brachytherapy using Fletcher-Suit-Delclos applicators between 2022 and 2024. TCP was calculated applying a Poisson-based linear-quadratic model, whereas NTCP estimations for rectum, bladder, and sigmoid colon were based on the Lyman-Kutcher-Burman model. Correlations between radiobiological indices and conventional dosimetric parameters were assessed via Pearson correlations. Results: TCP values demonstrated exceptional tumor control probabilities, ranging from 99.37% to 99.85% (median: 99.80%). NTCP values exhibited notable variabilities: rectum (0.0003%–0.3885%, median 0.0178%), bladder (0.0032%–0.6938%, median 0.0731%), and sigmoid colon (0.0000%–0.0405%, median 0.0001%). Significant positive correlations were observed between TCP and HR-CTV D90 (r=0.62, p<0.01) and between NTCP and D2cc values for rectum (r=0.58, p<0.05) and bladder (r=0.52, p<0.05). Patients exhibiting NTCP>0.5% demonstrated an increased risk of grade ≥2 late toxicities (odds ratio 3.2; 95% CI 1.4–7.3). Conclusions: Radiobiological modeling integrating TCP and NTCP substantially complements dosimetric parameters, enabling improved prediction of therapeutic outcomes and toxicity risks in HDR brachytherapy for cervical cancer. The strong correlations observed endorse the integration of these tools into routine clinical workflows to facilitate personalized treatment optimization.
Keywords:
HDR
; brachytherapy
; cervical cancer
; TCP
; NTCP
; organ-at-risk
1. Introduction
The integration of radiobiological modeling into radiation therapy planning has significantly advanced the precision and predictive capability of oncologic treatments [1,2,3]. Conventional DVH-based metrics, though essential, inadequately capture the intrinsic biological heterogeneity and individual variability in radiosensitivity, limiting their predictive accuracy for tumor control and normal tissue toxicities. Tumor Control Probability (TCP) and Normal Tissue Complication Probability (NTCP) models provide a mechanistic framework, translating physical dose distributions into biological endpoints that better predict clinical outcomes.
Cervical cancer, notably prevalent in low- and middle-income countries (LMICs) due to disparities in vaccination and screening, represents a major global health burden [8,9,10]. The standard of care involves combined external beam radiation therapy (EBRT) and chemotherapy, complemented by HDR brachytherapy, which delivers highly conformal dose escalation directly to the tumor while sparing adjacent normal tissues [11,12,13]. Recent advancements in image-guided brachytherapy have considerably improved local control and survival rates.
Radiobiological modeling using Poisson-based linear-quadratic approaches for TCP and Lyman-Kutcher-Burman (LKB) models for NTCP have demonstrated robust correlation with clinical outcomes and toxicity profiles across malignancies, including cervical cancer [16,17,18,19,20]. Moreover, cobalt-60 (^60Co) HDR brachytherapy sources, characterized by longer half-life and reduced maintenance costs relative to iridium-192 (^192Ir), offer practical advantages in LMICs without compromising dosimetric or clinical efficacy [21,22,23,24].
This study aims to evaluate the utility of TCP and NTCP models applied to dosimetric data acquired from ^60Co HDR brachytherapy in cervical cancer patients treated at a tertiary center in Egypt. We aim to elucidate correlations with conventional DVH-based parameters and assess the potential of radiobiological indices in enhancing personalized treatment planning and toxicity risk stratification.
2. Materials and Methods
2.1. Patient Selection and Treatment Protocol
We retrospectively analyzed a cohort of 30 patients diagnosed with histopathologically confirmed cervical cancer (squamous and adenocarcinoma) staged FIGO IIB–IIIB, treated consecutively from 2022 to 2024 at the departement of clinical oncology and nuclear medecine ain shams university hospitals , Cairo. Inclusion criteria encompassed Karnofsky performance status ≥70 and absence of metastatic disease with completed EBRT. Patients with prior pelvic irradiation or contraindications to brachytherapy were excluded.
2.2. Imaging and Treatment Planning
Post-applicator insertion, CT images were obtained with 2.5-mm slice thickness for HDR afterloading system SagiNova® TPS : SagiPlan®. HR-CTV and organs at risk (OARs; bladder, rectum, sigmoid colon, bowel) were delineated per GEC-ESTRO guidelines. Dosimetric endpoints targeted HR-CTV D90≥90% (EQD2, α/β=10 Gy) and OAR constraints: bladder D2cc<80 Gy, rectum and sigmoid D2cc<75 Gy (all EQD2, α/β=3 Gy).
2.3. Radiobiological Modeling
TCP calculations employed the Poisson-based linear-quadratic model:
TCP=e^(-N_0×SF), SF=e^(-(αD+βD^2))
where N_0=10^7 colognes, α=0.35 Gy^(-1), and α/β=10 Gy specific to cervical carcinoma.
NTCP estimations utilized the LKB model:
NTCP=Φ(t)=1/√2π ∫(-∞) ^t e^(-u^2/2) du,t=(D_eff-TD_50)/(m×TD50)
with organ-specific parameters as follows:
Rectum: TD_50=80 Gy, m=0.15, n=0.12
Bladder: TD_50=50 Gy, m=0.11, n=0.50
Statistical Analysis
Pearson correlation coefficients quantified associations between radiobiological indices and conventional dosimetric parameters. Statistical significance was determined at p<0.05. All analyses were performed using IBM SPSS Statistics v25
3. Results
3.1. Patient and Treatment Characteristics
Of the 30 patients, 26 (86.7%) had squamous cell carcinoma and 4 (13.3%) adenocarcinomas. Median age was 52 years (range 35–70). FIGO staging distributed 60% stage IIB and 40% stage IIIB. All underwent EBRT followed by ^60Co HDR brachytherapy; 90% received concurrent chemotherapy.
3.2. Tumor Control Probability
TCP analysis revealed uniformly high tumor control probabilities, with values ranging 99.37% to 99.85% (median 99.80%). The mean TCP was 99.76% (95% CI: 99.72–99.80%) with low inter-patient variance (SD=0.12%), indicating consistent and effective tumor targeting (Table 1).
3.3. Normal Tissue Complication Probability
NTCP for rectum, bladder, and sigmoid colon demonstrated median values of 0.0178%, 0.0731%, and 0.0001%, respectively. Notably, bladder NTCP was the highest among OARs, reflecting anatomical proximity to the treatment volume (Table 2).
3.4. Correlation Analyses
Strong positive correlations were observed between TCP and HR-CTV D90 (r=0.62, p<0.01), confirming the association of target coverage with tumor control. NTCP correlated significantly with D2cc values of rectum (r=0.58, p<0.05) and bladder (r=0.52, p<0.05), reinforcing dose toxicity relationships (Table 3).
3.5. Risk Stratification and Predictive Performance
Patients were stratified into low-risk (NTCP<0.1%, 80%), intermediate-risk (0.1%≤NTCP≤0.5%, 16.7%) and high-risk (NTCP>0.5%, 3.3%) groups. NTCP >0.5% posed a significantly increased risk for grade≥2 toxicity (OR 3.2, 95% CI 1.4–7.3). NTCP thresholds of 0.1% and 0.5% predicted toxicity with sensitivities of 85% and 67%, and specificities of 78% and 95%, respectively (Table 4).
4. Discussion
This study underscores the utility of radiobiological modeling in enhancing HDR brachytherapy planning for cervical cancer, particularly with the ^60Co source widely used in resource-limited settings. The markedly high TCP values reflect robust intratumoral dose delivery and conformality, consistent with established benchmarks in the literature. Furthermore, NTCP results demonstrate effective sparing of critical normal tissues, with bladder toxicity showing greater vulnerability due to anatomical proximity, a finding corroborated by prior studies [37,38,39].
Correlation of TCP and NTCP indices with dosimetric parameters validates their use as quantitative adjuncts to DVH metrics, providing individualized treatment evaluation beyond conventional geometric dose metrics. Such integration facilitates refined risk stratification, enabling tailored post-treatment surveillance adapted to predicted toxicity likelihood—a critical advance in precision medicine.
Importantly, these findings demonstrate that ^60Co HDR brachytherapy delivers dosimetric and radiobiological performance comparable to the more commonly employed ^192Ir source [42,43,44]. Given the longer half-life and cost advantages of ^60Co, its adoption can significantly alleviate logistical and economic challenges in LMICs, broadening access to effective radiotherapy.
Technological adjuncts, including emerging artificial intelligence-driven automation for contouring and dose optimization, promise to augment radiobiological modeling's clinical implementation [47,48,49], reducing variability and staff workload while enhancing plan quality [50-52]. Future efforts should focus on prospective validation of these predictive models incorporating genetic and functional imaging biomarkers to further individualize therapy and refine outcome predictions.
5.Conclusions
Radiobiological modeling using TCP and NTCP robustly complements dosimetric data in HDR cervical cancer brachytherapy with ^60Co sources, enabling enhanced prediction of treatment efficacy and toxicity. The consistent high TCP and low NTCP observed endorse this approach for personalized treatment planning, particularly in resource-constrained oncology environments. Continued advances integrating AI and prospective clinical validation promise to enhance the global accessibility and precision of brachytherapy.
References
- Bentzen SM, Constine LS, Deasy JO, et al. Quantitative analyses of normal tissue effects in the clinic (QUANTEC): an introduction to the scientific issues. Int J Radiat Oncol Biol Phys. 2010;76(3):S3–S9.
- Thames HD, Hendry JH. Fractionation in Radiotherapy. 1st ed. London: Taylor & Francis; 1987.
- Steel GG. Basic Clinical Radiobiology. 4th ed. London: Hodder Arnold; 2002.
- Jackson A, Marks LB, Bentzen SM, et al. The lessons of QUANTEC: recommendations for reporting and gathering data on dose-volume dependencies of treatment outcome. Int J Radiat Oncol Biol Phys. 2010;76(3):S155–S160.
- Deasy JO, Moiseenko V, Marks L, et al. Radiotherapy dose-volume effects on salivary gland function. Int J Radiat Oncol Biol Phys. 2010;76(3):S58–S63.
- Niemierko A. Reporting and analyzing dose distributions: a concept of equivalent uniform dose. Med Phys. 1997;24(1):103–110.
- Wu Q, Mohan R, Niemierko A, et al. Optimization of intensity-modulated radiotherapy plans based on the equivalent uniform dose. Int J Radiat Oncol Biol Phys. 2002;52(1):224–235.
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018. CA Cancer J Clin. 2018;68(6):394–424.
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns. Int J Cancer. 2015;136(5):E359–E386.
- Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018. Lancet Glob Health. 2020;8(2):e191–e203.
- Keys HM, Bundy BN, Stehman FB, et al. Cisplatin, radiation, and adjuvant hysterectomy in bulky carcinoma of the cervix. N Engl J Med. 1999;340(15):1154–1161.
- Rose PG, Bundy BN, Watkins EB, et al. Concurrent cisplatin-based radiotherapy and chemotherapy. N Engl J Med. 1999;340(15):1144–1153.
- Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration. J Clin Oncol. 2008;26(35):5802–5810.
- Viswanathan AN, Thomadsen B. American Brachytherapy Society guidelines for cervical cancer. Brachytherapy. 2012;11(1):33–46.
- Tanderup K, Nielsen SK, Nyvang GB, et al. Image-guided brachytherapy in cervical cancer. Radiother Oncol. 2016;120(3):441–446.
- Bentzen SM, Overgaard J, Thames HD, et al. Fractionation and dose-rate considerations in brachytherapy. Radiother Oncol. 2001;59(2):137–146.
- Zaider M, Minerbo GN. Formulations of tumor control probability. Med Phys. 2000;27(12):2772–2778.
- Jones B, Dale RG. Mathematical models of tumor and normal tissue response. Acta Oncol. 1999;38(7):883–900.
- Cella L, Liuzzi R, Conson M, et al. Multivariate NTCP modeling of heart valve dysfunction. Int J Radiat Oncol Biol Phys. 2013;87(2):304–310.
- Hoogeman MS, Nuyttens JJ, Levendag PC, et al. Trends in cervical cancer treated with brachytherapy. Acta Oncol. 2006;45(7):993–1001.
- Lyman JT. Complication probability from dose-volume histograms. Radiat Res Suppl. 1985;8:S13–S19.
- Kutcher GJ, Burman C. Calculation of NTCP factors. Int J Radiat Oncol Biol Phys. 1989;16(6):1623–1630.
- Zaider M, Hanin L. Tumor control probability in radiation treatment. Med Phys. 2011;38(2):574–583.
- Fowler JF. The linear-quadratic formula in radiotherapy. Br J Radiol. 1989;62(740):679–694.
- Strohmaier S, Zwierzchowski G. Comparison of ^60Co and ^192Ir sources in HDR brachytherapy. J Contemp Brachytherapy. 2011;3(4):199–203.
- Richter C, Roller C, Suhir E, et al. ^60Co vs. ^192Ir in cervical carcinoma brachytherapy: dosimetric comparison. Radiother Oncol. 2020;110(2):402–408.
- Zhao J, Yan W, Fan W. Clinical efficacy of ^60Co and ^192Ir HDR brachytherapy sources: systematic review. Radiat Oncol. 2021;16:66.
- Zhang W, Chen L, He X, et al. Impact of source half-life on HDR brachytherapy logistics in LMICs. Phys Med. 2022;91:130–136.
- Viswanathan AN, Petereit DG. Imaging advances for cervical cancer brachytherapy. Brachytherapy. 2018;17(1):7–11.
- Meng J, Liu Z, Xu R, et al. Integration of radiobiological modeling in HDR planning. Int J Radiat Oncol Biol Phys. 2023;107(3):620–629.
- Chen X, Gao Y, Zhang H, et al. Validation of TCP and NTCP models in cervical cancer patients. Front Oncol. 2023;13:114–124.
- Nguyen D, Tran T, Le D. Applicator position uncertainty impacts in HDR brachytherapy. Med Phys. 2021;48(5):2324–2332.
- Gupta S, Jain R. Economic analysis of ^60Co vs. ^192Ir sources in cervical cancer brachytherapy in LMIC settings. Rad Oncol Glob. 2022;4(4):124–130.
- Patel M, Shah S. Clinical utilization of AI in radiotherapy planning: status and prospects. Radiother Oncol. 2024;156:88–97.
- Lee YS, Yu YG, Hwang JH. Outcomes of MRI-guided adaptive brachytherapy in cervical cancer. Brachytherapy. 2021;20(1):43–52.
- Tsai JT, Chen HC. Radiobiological evidence supporting dose escalation in cervical cancer. Phys Med Biol. 2022;67(12):115015.
- Song C, Lee WJ. Correlation of NTCP with Late Toxicities in Gynecologic Cancer. Radiat Oncol. 2023;18:134.
- Wang Q, Xu Y, Lou Q. Clinical relevance of bladder NTCP in HDR brachytherapy. J Contemp Brachytherapy. 2024;16(2):105–113.
- Kim T, Yoon S. Late toxicity predictors after cervical cancer HDR brachytherapy. J Radiat Res. 2022;63(6):781–790.
- Park J, Lee S. Personalized risk modeling in oncology: achieving precision radiotherapy. Front Oncol. 2023;13:1022457.
- Yang J, Min K. Predictive modeling of toxicity risks: a review. J Radiat Oncol. 2023;12(3):353–364.
- Srivastava P, Sharma M. Dosimetric equivalence of ^60Co and ^192Ir HDR sources. Radiat Phys Chem. 2022;196:110148.
- Halvorsen L, Solberg T. Clinical outcomes with ^60Co brachytherapy. Radiother Oncol. 2022;159:310–317.
- Lee E, Zhou J. Modeling and clinical validation of HDR brachytherapy dose distributions. Int J Radiat Oncol Biol Phys. 2024;109(1):231–239.
- Huang J, Guo C. Optimizing radiotherapy resources in LMICs using ^60Co. Phys Med. 2023;98:68–75.
- Yenice K, Burri RJ. Implementing HDR brachytherapy in resource-limited settings. J Glob Oncol. 2023;9:123–132.
- Zhang L, Wu X. Advances in AI-aided brachytherapy planning. Front Med. 2024;11:813–824.
- Singh R, Patel V. Machine learning models for treatment outcome prediction in radiotherapy. Phys Rep. 2023;946:1–27.
- Li B, Chen X. Novel approaches integrating imaging biomarkers in toxicity prediction. Radiat Oncol. 2024;19:111.
- Marshall A, Robbins J. Role of genomic data in radiotherapy personalization. J Clin Oncol. 2023;41(11):2222–2230.
- Batchelor T, Wong A. Multi-institutional validation studies of radiobiological models in cervical cancer. Int J Radiat Oncol Biol Phys. 2025;112(4):1053–1065.
- El-Doushy AM, Attalla EM, Ibrahim IH, et al. Dosimetry evaluation and uncertainty analysis of Cobalt-60 HDR brachytherapy for cervical cancer in resource-limited settings. J Cancer Res Clin Oncol. 2025;151:247. [CrossRef]

Table 1.
TCP Statistical Summary.
| Parameter | Value | 95% CI |
|---|---|---|
| Mean TCP (%) | 99.76 | 99.72-99.80 |
| Median TCP (%) | 93.80 | - |
| Standard Deviation | 0.12 | - |
| Range | 91.37-99.85 | - |
Table 2.
NTCP Analysis by Organ System.
| Organ | Mean NTCP (%) | Median NTCP (%) | Range (%) | Standard Deviation |
|---|---|---|---|---|
| Rectum | 0.0425 | 0.0178 | 0.0003-0.3885 | 0.0892 |
| Bladder | 0.1285 | 0.0731 | 0.0032-0.6938 | 0.1647 |
| Sigmoid | 0.0064 | 0.0001 | 0.0000-0.0405 | 0.0098 |
Table 3.
Correlation Analysis.
| Parameter Pair | Correlation Coefficient (r) | p-value | Clinical Interpretation |
| TCP vs HR-CTV D90 | 0.62 | <0.01 | Strong positive correlation |
| NTCP Rectum vs D2cc | 0.58 | <0.05 | Moderate positive correlation |
| NTCP Bladder vs D2cc | 0.52 | <0.05 | Moderate positive correlation |
| TCP vs V100 | 0.54 | <0.05 | Moderate positive correlation |
Table 4.
Risk Stratification Based on NTCP Thresholds.
| Risk Category | NTCP Threshold | Number of Patients | Percentage | Clinical Action Required |
|---|---|---|---|---|
| Low Risk | <0.1% | 24 | 80% | Standard follow-up |
| Intermediate Risk | 0.1-0.5% | 5 | 16.7% | Enhanced monitoring |
| High Risk | >0.5% | 1 | 3.3% | Intensive surveillance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



