
Submitted:
05 October 2025
Posted:
08 October 2025
You are already at the latest version
Abstract
Introduction Emerging technologies have significantly transformed disaster preparedness and training in healthcare, especially for prehospital responders engaged in mass casualty incidents (MCIs). As scenarios grow more complex, traditional training methods alone are insufficient for developing critical skills such as triage, decision-making, and rapid coordination under pressure. Technology-enhanced solutions such as virtual reality (VR), wearable sensors, serious games, and AI-based systems offer immersive, scalable, and repeatable training experiences. While several studies have explored these tools individually, a comprehensive synthesis is lacking to map how diverse technologies are employed in MCI-focused prehospital training. Methods This scoping review is conducted as part of the MCI-PHER project (Mass Casualty Incident – Prehospital Emergency Response), a collaborative initiative to advance disaster medicine education and prehospital preparedness. The review will follow the Arksey and O’Malley framework, refined by Levac et al., and adhere to PRISMA-ScR guidelines. A systematic search will be conducted across databases, including PubMed, Embase, Scopus, CINAHL, PsycINFO, Cochrane Library, and ClinicalTrials.gov. Eligible studies must describe, implement, or evaluate technological training interventions targeted at healthcare professionals or students in simulated or actual prehospital MCI settings. Two independent reviewers will conduct study selection, data extraction, and quality checks, with disagreements resolved by a third reviewer. Data will be charted using a customized extraction tool, refined through piloting five relevant studies. Results and Analysis Studies will be synthesized using a combination of descriptive and narrative approaches. Key domains will include the type of technology and training modality, learning objectives, target professional groups, instructional design models, evaluation strategies, and reported outcomes. Quantitative findings will be summarized using descriptive statistics, while qualitative results, such as user perceptions and contextual insights, will be narratively organized to reflect patterns and diversity across studies. The synthesis will identify common applications, outcome trends, implementation barriers, and evidence gaps to inform future research and practice in prehospital MCI training. Dissemination and Ethics As no human subjects are involved, ethical approval is not required. Results will be disseminated via peer-reviewed publications, conference presentations, stakeholder briefings, and open-access platforms to inform EMS leaders, simulation educators, and health policymakers.
Keywords:
Mass casualty incident
; prehospital training
; emergency responders
; wearable technology
; virtual reality
; serious games
; technology-enhanced learning
; disaster preparedness
; simulation-based education
; scoping review
Introduction
Background
Technology is the application of scientific knowledge for practical purposes. It uses scientific principles to change the environment in which humans live and solve problems, encompassing both the creation of physical tools and the know-how required to use and produce them [1].
Dramatic technological advancements have transformed healthcare. For example, infusion pumps have progressed from simple gravity-fed devices to clockwork mechanisms and now to computerized systems with digital interfaces [2].
Technology continues to reshape healthcare education and improve patient outcomes in innovative ways. With its ability to simulate real-life scenarios, virtual environments now offer online healthcare students immersive training experiences before they engage in actual patient care, such as during surgical residencies. In VR and AR environments, learners can develop not only hands-on skills but also critical thinking and decision-making capabilities that were once acquired primarily through on-the-job training, particularly in trauma or emergency settings. These tech-enabled educational platforms better prepare students for high-stress situations and ultimately contribute to improved patient care [3].
An MCI is an event that leads to a sudden influx of patients, with numbers so high that local healthcare resources and normal procedures become inadequate to manage them. Such situations typically necessitate extraordinary emergency response arrangements and often result from either natural events, like earthquakes or hurricanes, or man-made disasters, such as large-scale accidents or acts of violence [4].
The literature on MCI training highlights the need for specialized, repeated training programs to improve the readiness and effectiveness of emergency medical teams and hospital-based providers [5]. Optimal preparedness involves multiple strategies, including regular drills, clear communication, and integration of disaster response plans. For instance, a study on prehospital preparedness in Sweden revealed low staff familiarity with contingency plans, infrequent follow-up routines, and inadequate training exercises, emphasizing the importance of standardized training and consistent evaluation against national guidelines [6]. The rapid advancement of technology has enabled the integration of modern tools in medical training, such as virtual, augmented, and mixed reality (VR, AR, and MR). These systems provide immersive, realistic environments that accelerate knowledge acquisition and foster the development of high-quality skills [7,8].
Objectives and Rationale
While a recent systematic review has examined the use of extended reality technologies in training first responders for mass casualty incidents (MCIs), it focused narrowly on immersive tools such as virtual and augmented reality. Other important technological modalities, such as wearable sensors, mobile applications, AI-based platforms, and serious games, were not addressed. Additionally, the review did not examine study design quality or implementation challenges. These gaps limit the utility of the findings for guiding future research and practical implementation.
To address this, our scoping review takes a broader perspective. We aim to explore all types of technology-enhanced approaches used to train prehospital responders for MCIs, while also critically analyzing how these tools are applied, what outcomes they report, and what challenges or gaps remain in the literature.
This scoping review aims to explore how technology supports training for prehospital responders in mass casualty incident contexts. It will identify the types of technologies used in MCI-related training; describe the training modalities and pedagogical strategies applied; analyze the reported outcomes and the metrics used to evaluate effectiveness; and synthesize the gaps, barriers, and limitations that affect the design, implementation, and scalability of technology-based training in this domain.
Methods
Protocol Design
Developed under the MCI-PHER (Mass-Casualty Incident—Prehospital Emergency Response) initiative, this scoping review protocol supports a unified research agenda aimed at strengthening disaster medicine education, spurring training innovation, and elevating prehospital preparedness. The review will be guided by the Arksey and O’Malley framework, incorporate enhancements recommended by Levac and colleagues, and align with PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) to maintain methodological rigor [9,10,11]. In line with best practices for transparency and reproducibility, the review methodology was documented and registered on Protocols.io [12].
Stage 1: Identifying the Research Question
Research Questions
Primary Research Question:
What technologies are used to train and assess prehospital responders for mass casualty incidents (MCIs), and what impact do they have on training effectiveness?
Secondary Research Questions:
- How effective are these technologies in improving knowledge, practical skills, decision-making, and response times?
- What measurement instruments (e.g., knowledge tests, OSCEs / checklists, system logs) are used?
- Which training design frameworks (e.g., ADDIE, Kern, mastery learning) and assessment frameworks (e.g., Kirkpatrick, Miller) are reported?
- What levels and determinants of participant satisfaction are reported for technology-enhanced prehospital MCI training?
Stage 2: Identifying Relevant Studies
Information Sources
A comprehensive range of databases will be searched to ensure thorough coverage of relevant literature across disciplines. These include:
- PubMed – for peer-reviewed research in biomedical and life sciences
- Embase – for extensive biomedical literature, including European and Asian sources
- Scopus – for a wide array of scientific, technical, and medical publications
- PsycINFO (via APA PsycNet) – for literature focused on psychological aspects of training and education
- CINAHL (Cumulative Index to Nursing and Allied Health Literature) – for research in nursing and allied health professions
- Cochrane Library – for systematic reviews and evidence from clinical trials
- ClinicalTrials.gov – to review any registered clinical trials related to tabletop exercises or emergency preparedness.
- Google Scholar – to identify additional academic and non-academic sources.
Search Strategy
A thorough search strategy was developed on June 13, 2025, using a combination of keywords and Medical Subject Headings (MeSH), which were identified via the MeSH database on PubMed (Table 1 and Table 2). To ensure completeness, we will rerun the search before submission. Additionally, Google Scholar and the reference lists of included studies and systematic reviews will be manually searched to identify any potentially missed studies.
Search Strategy Refinement
The search strategy will be peer-reviewed using the PRESS (Peer Review of Electronic Search Strategies) guidelines to ensure accuracy and comprehensiveness [13]. All modifications made throughout the development process will be documented and shared with the research team for full transparency.
Search Management
All search results will be directly imported into Covidence, an online platform used for managing systematic and scoping reviews. Duplicate records will be automatically identified and removed within the platform [14].
Documentation
A comprehensive log of the search strategy, including databases searched, search strings used, any iterative changes, and the number of records retrieved, will be maintained to support transparency, reproducibility, and future updates of the review.
Stage 3: Study Selection
Screening
The screening process will be conducted using Covidence. Study selection will follow a two-stage process: initial title and abstract screening, followed by full-text screening. Two reviewers will independently assess all studies based on the pre-established inclusion criteria. Any disagreements between reviewers will be resolved by involving a third reviewer to ensure consensus and consistency. The PRISMA flow diagram will be used to visually represent the review process, clearly outlining each stage of study selection (Figure 1)
Inclusion Criteria
- Population (P): Includes medical first responders (MFRs), paramedics, EMTs, physicians, nurses, medical interns, residents, and students enrolled in health-related university programs (e.g., medicine, nursing, EMS).
- Concept (C): Studies that describe, implement, or evaluate educational or training programs using any form of technology in the context of mass casualty incidents (MCIs).
- Context (C): The training or simulation must replicate prehospital settings, such as field triage, ambulance scenarios, roadside emergencies, or disaster zones.
- Study Design: We will include original research articles and study protocols employing quantitative, qualitative, or mixed-methods designs.
- Other Sources: Grey literature (e.g., conference abstracts, theses, NGO/government reports) will be included if they provide sufficient methodological detail.
Exclusion Criteria
- Studies conducted exclusively in in-hospital environments (e.g., emergency departments, ICUs, or operating rooms).
- Studies that focus on non-disaster emergency care, routine trauma management, or non-MCI clinical procedures.
- Studies focusing only on non-healthcare populations (e.g., firefighters, police, military, laypersons) unless a separate analysis is provided for healthcare professionals.
- Studies published before 2015 or not in English.
- Systematic reviews, literature reviews, and scoping reviews.
Stage 4: Data Charting
We developed a standardized data extraction form by piloting five studies and identifying recurring variables relevant to the assessment of human factors using technology in healthcare and emergency settings. This preliminary testing allowed us to refine the charting tool to ensure it captures essential elements across various technologies, professional roles, and study designs. The data extraction form will remain flexible and may be iteratively updated throughout the review process to accommodate new themes or nuances that emerge from the literature (Table 3).

Table 3.
Data Extraction sheet.
| Field | Description |
| Study ID | Unique identifier (e.g., Author-Year or assigned number). |
| Country | The country where the study was conducted. |
| Study design | Type of study (e.g., experimental, observational, mixed method, etc.). |
| Study aim / objective | Summary of the study’s aim or research questions. |
| Training duration | Total length of the training, including session count, session length, and overall timeframe (e.g., “single 2-hour session,” “daily 1-hour sessions over 1 week,” or “weekly sessions for 2 months”). |
| Study context | Type of disaster or emergency scenario used in the training (e.g., earthquake, flood, mass traffic crash, explosion, terrorist attack, pandemic). Also include the scale of the simulation (e.g., tabletop, functional, full-scale) and whether it was based on a simulated scenario or a real event. |
| Program content | What was taught/practiced: scenario type (e.g., START/SALT, CBRN, MVC), key objectives/tasks, team configuration (single vs interprofessional), and any triage/response algorithms. |
| Framework/model of training design | Any stated instructional design model (e.g., ADDIE, Kern, mastery learning/deliberate practice, TPACK, experiential learning). |
| Framework/model of assessment | Any stated evaluation framework (e.g., Kirkpatrick, Miller’s pyramid, Messick validity, CIPP) or assessment design model (e.g., OSCE blueprinting). |
| Population | Type of healthcare professionals or trainees (e.g., EMTs, paramedics, physicians, nurses, students). |
| Sample size | Total number of participants involved. |
| Setting | Training context (e.g., prehospital field, simulation centre, mobile training unit, hybrid). |
| Technology used | E.g., VR/AR, serious games, mobile apps, wearable tech, haptic simulators, etc. |
| Describe the use of technology | E.g., skills training, scenario replication, triage simulation, decision-making enhancement, etc. |
| Comparator present? | Yes/No. If yes, describe the comparison condition (e.g., traditional training, no intervention, other tech). |
| Data collection method | E.g., performance scores, simulation metrics, surveys, interviews, video analysis, system logs. |
| Outcome measures | Metrics used to assess training effectiveness (e.g., knowledge gain, skill proficiency, response time, accuracy), and participants’ satisfaction. |
| Key findings | Summary of relevant findings about the training outcomes and technology. |
Stage 5: Collating, Summarizing, and Reporting the Results
Two independent reviewers will conduct the screening and data extraction process to ensure accuracy and consistency by verifying key details from each study. Any discrepancies will be addressed through discussion or, if necessary, resolved by a third reviewer. Microsoft Excel will be used to organize and manage the extracted data.
After charting the data in Excel, the research team will employ both systematic and narrative synthesis methods to categorize the studies across key domains relevant to this review, including:
- Technology type and training modality
- Training objectives and focus
- Target learners and professional roles
- Training design
- Assessment and evaluation strategies
- Reported outcomes
Quantitative data (e.g., study frequency, participant numbers, outcome measures) will be summarized using descriptive statistics. Qualitative data (e.g., user perceptions, contextual findings) will be examined through categorization and synthesis across domains to capture nuanced insights. This combined approach will provide a holistic view of how modern technologies are used to evaluate learning and performance outcomes. The entire synthesis process will align with the research objectives and follow the PRISMA-ScR guidelines [11].
Furthermore, in the Discussion, we will examine the studies’ barriers, facilitators, limitations, and strengths, and provide recommendations for future work.
Stage 6: Stakeholder Consultation (Optional Stage)
Stakeholder consultation will be incorporated as a critical component of the final reporting phase. This optional yet valuable step aims to actively engage relevant stakeholders involved in healthcare delivery, emergency response, and workforce development. These stakeholders may include clinical educators, emergency physicians, paramedics, nursing leaders, simulation specialists, health technology developers, and policymakers. Their input will help validate the findings of the scoping review, offer additional insights not captured in the literature, and identify real-world applications and challenges related to the use of emerging technologies in training and evaluating prehospital responders for mass casualty incidents.
Limitations
This review has several limitations. Restricting the inclusion criteria to English-language studies may introduce language bias and result in the exclusion of relevant research published in other languages. Although the search strategy is comprehensive and draws from multiple databases, there remains the possibility of missing pertinent studies due to limited indexing or accessibility.
The inclusion of grey literature helps to minimize publication bias; however, it may lead to variability in the methodological quality of included studies. Heterogeneity in study designs, technological tools used, target populations, and outcome measures may limit comparability across the literature. Additionally, methodological weaknesses such as small sample sizes, lack of control groups, or inconsistent reporting may affect the strength and generalizability of the findings.
Nevertheless, this review will offer valuable insights into the range and application of technologies used to train and evaluate prehospital responders for mass casualty incidents, while also identifying key gaps and opportunities for future research.
Ethics and Dissemination
Ethical Considerations
This scoping review will not involve primary data collection or interaction with human participants and, therefore, does not require ethical approval. Nevertheless, the review will be conducted in line with established ethical research standards. This includes transparency in reporting methods and findings, proper citation of all sources, avoidance of plagiarism and duplicate publication, and impartiality in data synthesis and interpretation. Any potential conflicts of interest within the research team will be disclosed and managed appropriately.
Dissemination Strategy
The review’s findings will be widely disseminated to stakeholders across emergency medicine and prehospital care to maximize impact.
- Peer-Reviewed Publication
We will submit the final manuscript to a peer-reviewed journal in emergency medicine, disaster preparedness, or simulation-based education.
- 2.
- Conference Presentations
Key results will be shared at major national and international meetings, including:
• World Association for Disaster and Emergency Medicine (WADEM)
• International Conference on Emergency Medicine (ICEM)
• National EMS conferences and simulation-training events
- 3.
- Stakeholder Engagement
A brief summary will be distributed to:
• EMS organizations
• Disaster response agencies
• Simulation centers
• Prehospital training institutions
We may also host webinars or roundtables with prehospital stakeholders to discuss implications and applications.
- 4.
- Open Access & Preprint
We aim to publish open access and may post a preprint (e.g., on medRxiv) to provide early visibility.
- 5.
- Professional Networks & Social Media
Key messages and infographics will be shared via LinkedIn, X (formerly Twitter), and ResearchGate to reach EMS professionals, educators, and researchers.
- 6.
- Policy Briefs
Short briefs underscoring the relevance of tech-based training approaches for prehospital preparedness will be provided to health organizations and policy stakeholders.
- 7.
- Implementation & Collaboration
We will pursue partnerships with EMS programs and disaster-training institutions to pilot or adopt promising practices identified in the review, and may conduct a follow-up survey to assess real-world use.
- 8.
- Research Gaps & Agenda
Identified gaps will guide a future research agenda to be shared with funders and academic networks to encourage further work.
- 9.
- Planned Updates
The scoping review will be updated every 3–5 years to incorporate new evidence and innovations in tabletop-based prehospital preparedness.
Ongoing Coordination:
| Stage | Duration | Weeks |
| Planning & Protocol Development | 4 weeks | Weeks 1–4 |
| - Team meetings & protocol drafting | ||
| - Protocol registration (e.g., OSF) | ||
| Literature Search | 3 weeks | Weeks 5–7 |
| - Finalize and conduct a search | ||
| - Grey literature and manual search | ||
| Study Selection | 6 weeks | Weeks 8–13 |
| - Title/abstract screening | ||
| - Full-text screening | ||
| Data Charting | 4 weeks | Weeks 14–17 |
| - Pilot and finalize the charting form | ||
| - Extract data from included studies | ||
| Analysis & Synthesis | 6 weeks | Weeks 18–23 |
| - Thematic and descriptive analysis | ||
| - Identify trends, gaps, and insights | ||
| Report Writing | 4 weeks | Weeks 24–27 |
| - Draft, review, and finalize manuscript | ||
| Dissemination Activities | 5+ weeks | Weeks 28–32+ |
| - Prepare journal submission | ||
| - Presentations, briefs, stakeholder outreach |
Ongoing Coordination:
- Weekly team meetings to monitor progress
- Buffer time built into each phase to accommodate unforeseen delays
- Dissemination activities may continue beyond Week 32 due to conference and stakeholder engagement schedules
Funding
This review is supported by the MCI-PHER project (Mass Casualty Incident – Prehospital Emergency Response), funded through the Dubai Health Collaborative Stimulus Research Grant (CSRG) at Mohammed Bin Rashid University of Medicine and Health Sciences. The funding organization had no influence on the study design, data analysis, or manuscript preparation.
Acknowledgments
None to declare.
Conflicts of Interest
None to declare.
References
- Grubler A. 2.1. From Artifacts to Megamachines.
- Thimbleby H. Technology and the Future of Healthcare. Journal of Public Health Research. 2013 Dec;2(3):jphr.2013.e28.
- Grimwood T, Snell L. The use of technology in healthcare education: a literature review. MedEdPublish. 2020 Jun 25;9:137.
- DeNolf RL, Kahwaji CI. EMS Mass Casualty Management. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Sep 29]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK482373/.
- Hwang KI, Kim J. The Training Effects of Mass Casualty Triage in Radiological Events for 119 Emergency Medical Team. Prehosp Disaster med. 2023 May;38(S1):s129–s129.
- Agri J, Söderin L, Hammarberg E, Lennquist-Montán K, Montán C. Prehospital Preparedness for Major Incidents in Sweden: A National Survey with Focus on Mass-Casualty Incidents. Prehosp Disaster med. 2023 Feb;38(1):65–72.
- Mills B, Dykstra P, Hansen S, Miles A, Rankin T, Hopper L, et al. Virtual Reality Triage Training Can Provide Comparable Simulation Efficacy for Paramedicine Students Compared to Live Simulation-Based Scenarios. Prehospital Emergency Care. 2020 Jul 3;24(4):525–36.
- Duan Y yu, Zhang J yao, Xie M, Feng X bo, Xu S, Ye Z wei. Erratum to: Application of Virtual Reality Technology in Disaster Medicine. CURR MED SCI. 2020 Dec;40(6):1205–1205.
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005 Feb;8(1):19–32.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implementation Sci. 2010 Dec;5(1):69.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2;169(7):467–73.
- Saouli A, Nour R, Farhan H, Omayer A, Yousif A, Hubloue I, et al. Tech-Based Training Approaches for Prehospital Mass Casualty Response: A Scoping Review Protocol. 2025 Jul 5 [cited 2025 Jul 9]; Available from: https://www.protocols.io/view/tech-based-training-approaches-for-prehospital-mas-g4pmbyvk7.
- McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. Journal of Clinical Epidemiology. 2016 Jul;75:40–6.
- Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
Figure 1.
PRISMA flow diagram.
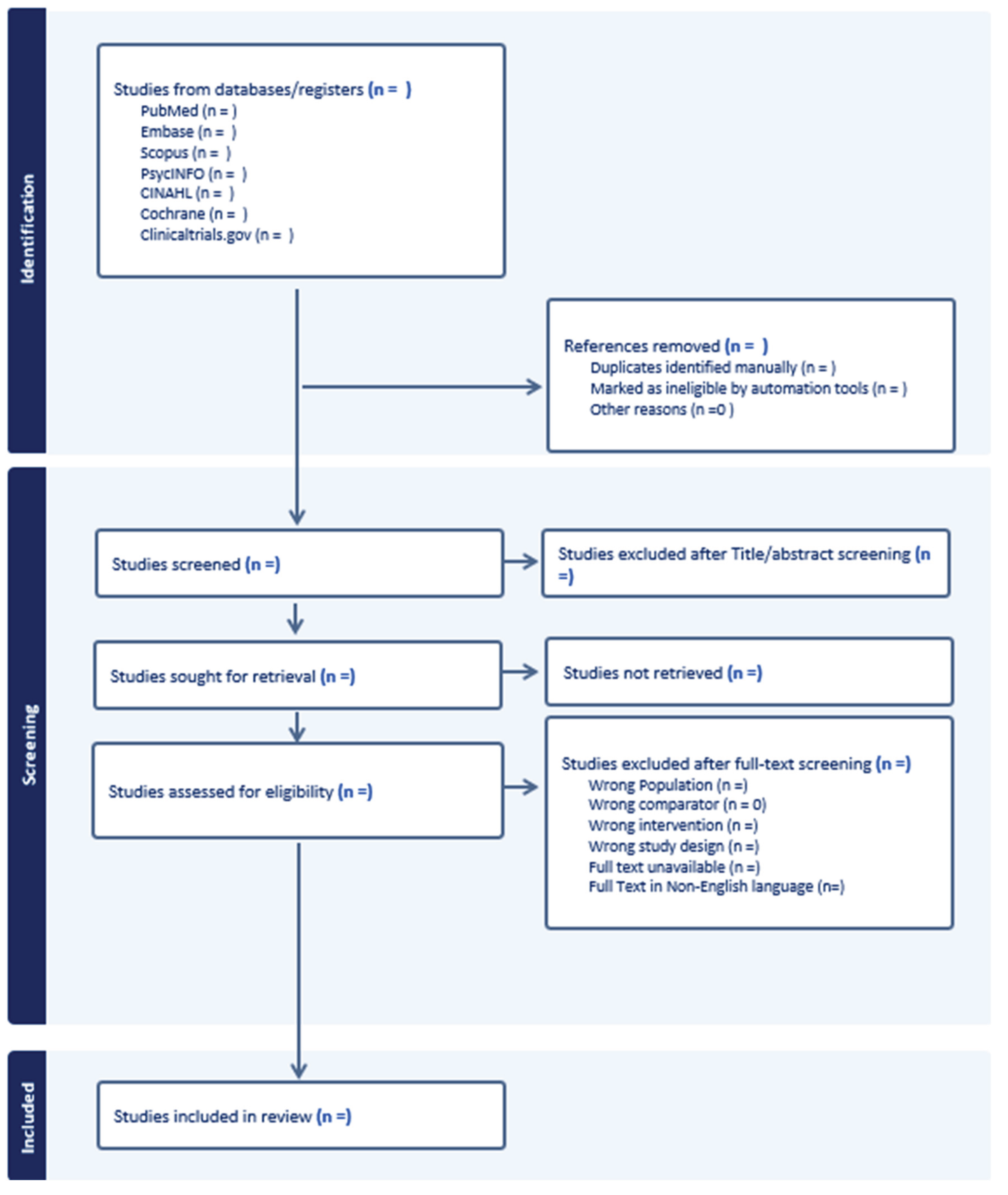
Table 1.
Keywords and MeSH terms.
| Population | First responders, Medical intern, Healthcare Provider, Paramedics[MeSH], Health Personnel[MeSH], Nurses[MeSH], Physicians[MeSH] |
|
Technology (Concept) |
eye-tracking, virtual reality, augmented reality, mixed reality, biometric sensors, electroencephalogram, motion tracking, wearable devices, digital monitoring, performance dashboards, galvanic skin response, pupillometry, psychophysiological tools, heart rate variability, artificial intelligence, AI, human-computer interaction, mobile application, wearable computer, smart glasses, smartphone, wearable electronic devices, smart wearables, GPS, GPS-based, gamification, serious games, video games, immersive virtual environment, 3D environment, virtual scenarios, virtual patient, extended reality, digital tools, augmented virtuality, haptic technology, realistic scenarios, ambient intelligence, user-centered design, user-computer interface, medical informatics applications, data display, game theory, haptic-based, Wearable Proximity Sensors, high-fidelity, close-to-reality, smart electronic devices |
|
Disaster Context |
mass casualty incident, crisis, disaster, pandemic, natural disaster, earthquake, flood, landslide, traffic accident, emergency shelter, nuclear accident, tornado, tidal wave, wildfire, structure collapse, avalanche, CBRN, CBRNe, terrorism, terrorist attack, bioterrorism, bomb, chemical accident, chemical terrorism, radiation accident, radioactive hazard release, chemical hazard release, drought, catastrophe, catastrophic accident, multiple trauma, high-risk situations, human-made disasters |
Table 2.
Search strategy.
| Database | Search strategy |
| PubMed | (“mass casualty incident” OR “Mass Casualty Incidents”[MeSH] OR “crisis” OR “Disasters”[Mesh] OR “aircraft accident” OR “avalanche” OR “biological accident” OR “biohazard release” OR “bioterrorism” OR “bomb” OR “chemical accident” OR “chemical hazard release” OR “chemical terrorism” OR “climate change” OR “cyclonic storm” OR “disaster victim” OR “disaster” OR “drought” OR “earthquake” OR “emergency patient” OR “emergency shelter” OR “flood” OR “landslide” OR “mass-casualty incident” OR “mass disaster” OR “multiple trauma” OR “natural disaster” OR “nuclear accident” OR “pandemic” OR “radioactive hazard release” OR “radiation accident” OR “structure collapse” OR “traffic accident” OR “terrorism” OR “tidal wave” OR “tornado” OR “wildfire” OR “catastrophe” OR “catastrophic accident” OR “CBRN” OR “CBRNe” OR “high-risk situations” OR “human-made disasters” OR “terrorist attack”) AND (“eye-tracking” OR “Technology”[Mesh] OR “virtual reality” OR “augmented reality” OR “mixed reality” OR “biometric sensors” OR “electroencephalogram” OR “digital monitoring” OR “motion tracking” OR “wearable devices” OR “performance dashboards” OR “psychophysiological tools” OR “galvanic skin response” OR “pupillometry” OR “heart rate variability” OR “Eye-Tracking Technology”[Mesh] OR “Virtual Reality”[Mesh] OR “Augmented Reality”[Mesh] OR “Spectroscopy, Near-Infrared”[Mesh] OR “Galvanic Skin Response”[Mesh] OR “artificial intelligence” OR “augmented reality” OR “human computer interaction” OR “human machine interface” OR “microcomputer” OR “mobile application” OR “user-centered design” OR “video game” OR “virtual reality” OR “wearable computer” OR “ambient intelligence” OR “audiovisual aids” OR “data display” OR “game theory” OR “human-computer interaction” OR “medical informatics applications” OR “smartphone” OR “smart glasses” OR “user-computer interface” OR “video games” OR “wearable electronic devices” OR “3D environment” OR “3-D environment” OR “AI” OR “augmented virtuality” OR “close-to-reality” OR “computer environment” OR “digital tools” OR “enhanced realism” OR “enhanced reality” OR “extended reality” OR “game-based” OR “gamification” OR “haptic-based” OR “haptic technology” OR “immersive virtual reality” OR “immersive virtual environment” OR “realistic scenarios” OR “real-world scenarios” OR “smart electronic devices” OR “smart wearables” OR “virtual patient” OR “virtual scenarios” OR “virtual worlds” OR “VR” OR “wearable technologies” OR “Wearable Proximity Sensors” OR Wearable OR GPS OR “GPS-Based” OR “High-Fidelity” OR “Serious games”) AND (“first responders” OR “medical intern” OR “healthcare provider” OR “Paramedics”[MeSH] OR “Health Personnel”[MeSH] OR “Nurses”[MeSH] OR “Physicians”[MeSH]) AND (“Education”[Mesh] OR “Simulation Training”[Mesh] OR Training OR “Feedback training” OR “Simulation-based education” OR “Real-world training” OR “Interprofessional Education” OR “Competency-Based Education”) AND (evaluate OR assess OR train OR outcomes) |
| Scopus | (TITLE-ABS-KEY (“mass casualty incident” OR “crisis” OR “Disasters” OR “aircraft accident” OR “avalanche” OR “biological accident” OR “biohazard release” OR “bioterrorism” OR “bomb” OR “chemical accident” OR “chemical hazard release” OR “chemical terrorism” OR “cyclonic storm” OR “disaster” OR “drought” OR “earthquake” OR “emergency shelter” OR “flood” OR “landslide” OR “mass-casualty incident” OR “mass disaster” OR “multiple trauma” OR “natural disaster” OR “nuclear accident” OR “pandemic” OR “radioactive hazard release” OR “radiation accident” OR “structure collapse” OR “traffic accident” OR “terrorism” OR “tidal wave” OR “tornado” OR “wildfire” OR “catastrophe” OR “catastrophic accident” OR “CBRN” OR “CBRNe” OR “high-risk situations” OR “human-made disasters” OR “terrorist attack”)) AND (TITLE-ABS-KEY (“eye-tracking” OR “Technology” OR “virtual reality” OR “augmented reality” OR “mixed reality” OR “biometric sensors” OR “electroencephalogram” OR “digital monitoring” OR “motion tracking” OR “wearable devices” OR “performance dashboards” OR “psychophysiological tools” OR “galvanic skin response” OR “pupillometry” OR “heart rate variability” OR “Eye-Tracking Technology” OR “Galvanic Skin Response” OR “artificial intelligence” OR “augmented reality” OR “human computer interaction” OR “human machine interface” OR “microcomputer” OR “mobile application” OR “user-centered design” OR “video game” OR “virtual reality” OR “wearable computer” OR “ambient intelligence” OR “audiovisual aids” OR “data display” OR “game theory” OR “human-computer interaction” OR “medical informatics applications” OR “smartphone” OR “smart glasses” OR “user-computer interface” OR “video games” OR “wearable electronic devices” OR “3D environment” OR “3-D environment” OR “AI” OR “augmented virtuality” OR “close-to-reality” OR “computer environment” OR “digital tools” OR “enhanced realism” OR “enhanced reality” OR “extended reality” OR “game-based” OR “gamification” OR “haptic-based” OR “haptic technology” OR “immersive virtual reality” OR “immersive virtual environment” OR “realistic scenarios” OR “real-world scenarios” OR “smart electronic devices” OR “smart wearables” OR “virtual patient” OR “virtual scenarios” OR “virtual worlds” OR “VR” OR “wearable technologies” OR “Wearable Proximity Sensors” OR Wearable OR GPS OR “GPS-Based” OR “High-Fidelity” OR “Serious games”)) AND (TITLE-ABS-KEY (“first responders” OR “medical intern” OR “healthcare provider” OR “Paramedics” OR “Health Personnel” OR “Nurses” OR “Physicians”)) AND (TITLE-ABS-KEY (“Education” OR “Simulation Training” OR Training OR “Feedback training” OR “Simulation-based education” OR “Real-world training” OR “Interprofessional Education” OR “Competency-Based Education”)) AND (TITLE-ABS-KEY (“evaluate” OR “assess” OR “train” OR “outcomes”)) AND (LIMIT-TO (SUBJAREA, “MEDI”) OR LIMIT-TO (SUBJAREA, “NURS”) OR LIMIT-TO (SUBJAREA, “HEAL”) OR LIMIT-TO (SUBJAREA, “NEUR”) OR LIMIT-TO (SUBJAREA, “MULT”)) |
|
Embase #6 #5 #4 #3 #2 #1 |
#1 AND #2 AND #3 AND #4 AND #5 ‘evaluate’ OR ‘assess’ OR ‘train’ OR ‘outcomes’ ‘education’ OR ‘simulation training’ OR training OR ‘feedback training’ OR ‘simulation-based education’ OR ‘real-world training’ OR ‘interprofessional education’ OR ‘competency-based education’ ‘first responders’ OR ‘medical intern’ OR ‘healthcare provider’ OR ‘paramedics’ OR ‘health personnel’ OR ‘nurses’ OR ‘physicians’ ‘eye-tracking’ OR ‘technology’ OR ‘mixed reality’ OR ‘biometric sensors’ OR ‘electroencephalogram’ OR ‘digital monitoring’ OR ‘motion tracking’ OR ‘wearable devices’ OR ‘performance dashboards’ OR ‘psychophysiological tools’ OR ‘pupillometry’ OR ‘heart rate variability’ OR ‘eye-tracking technology’ OR ‘galvanic skin response’ OR ‘artificial intelligence’ OR ‘augmented reality’ OR ‘human computer interaction’ OR ‘human machine interface’ OR ‘microcomputer’ OR ‘mobile application’ OR ‘user-centered design’ OR ‘video game’ OR ‘virtual reality’ OR ‘wearable computer’ OR ‘ambient intelligence’ OR ‘audiovisual aids’ OR ‘data display’ OR ‘game theory’ OR ‘human-computer interaction’ OR ‘medical informatics applications’ OR ‘smartphone’ OR ‘smart glasses’ OR ‘user-computer interface’ OR ‘video games’ OR ‘wearable electronic devices’ OR ‘3d environment’ OR ‘3-d environment’ OR ‘ai’ OR ‘augmented virtuality’ OR ‘close-to-reality’ OR ‘computer environment’ OR ‘digital tools’ OR ‘enhanced realism’ OR ‘enhanced reality’ OR ‘extended reality’ OR ‘game-based’ OR ‘gamification’ OR ‘haptic-based’ OR ‘haptic technology’ OR ‘immersive virtual reality’ OR ‘immersive virtual environment’ OR ‘realistic scenarios’ OR ‘real-world scenarios’ OR ‘smart electronic devices’ OR ‘smart wearables’ OR ‘virtual patient’ OR ‘virtual scenarios’ OR ‘virtual worlds’ OR ‘vr’ OR ‘wearable technologies’ OR ‘wearable proximity sensors’ OR ‘wearable’ OR ‘gps’ OR ‘gps-based’ OR ‘high-fidelity’ OR ‘serious games’ ‘mass casualty incident’ OR ‘crisis’ OR ‘disasters’ OR ‘aircraft accident’ OR ‘avalanche’ OR ‘biological accident’ OR ‘biohazard release’ OR ‘bioterrorism’ OR ‘bomb’ OR ‘chemical accident’ OR ‘chemical hazard release’ OR ‘chemical terrorism’ OR ‘cyclonic storm’ OR ‘disaster’ OR ‘drought’ OR ‘earthquake’ OR ‘flood’ OR ‘landslide’ OR ‘mass-casualty incident’ OR ‘mass disaster’ OR ‘multiple trauma’ OR ‘natural disaster’ OR ‘nuclear accident’ OR ‘pandemic’ OR ‘radioactive hazard release’ OR ‘radiation accident’ OR ‘structure collapse’ OR ‘traffic accident’ OR ‘terrorism’ OR ‘tidal wave’ OR ‘tornado’ OR ‘wildfire’ OR ‘catastrophe’ OR ‘catastrophic accident’ OR ‘cbrn’ OR ‘cbrne’ OR ‘high-risk situations’ OR ‘human-made disasters’ OR ‘terrorist attack’ |
| CINAHL | (“mass casualty incident” OR “crisis” OR “Disasters” OR “aircraft accident” OR “avalanche” OR “biological accident” OR “biohazard release” OR “bioterrorism” OR “bomb” OR “chemical accident” OR “chemical hazard release” OR “chemical terrorism” OR “cyclonic storm” OR “disaster” OR “drought” OR “earthquake” OR “emergency shelter” OR “flood” OR “landslide” OR “mass-casualty incident” OR “mass disaster” OR “multiple trauma” OR “natural disaster” OR “nuclear accident” OR “pandemic” OR “radioactive hazard release” OR “radiation accident” OR “structure collapse” OR “traffic accident” OR “terrorism” OR “tidal wave” OR “tornado” OR “wildfire” OR “catastrophe” OR “catastrophic accident” OR “CBRN” OR “CBRNe” OR “high-risk situations” OR “human-made disasters” OR “terrorist attack”) AND (“eye-tracking” OR “Technology” OR “virtual reality” OR “augmented reality” OR “mixed reality” OR “biometric sensors” OR “electroencephalogram” OR “digital monitoring” OR “motion tracking” OR “wearable devices” OR “performance dashboards” OR “psychophysiological tools” OR “galvanic skin response” OR “pupillometry” OR “heart rate variability” OR “Eye-Tracking Technology” OR “Galvanic Skin Response” OR “artificial intelligence” OR “augmented reality” OR “human computer interaction” OR “human machine interface” OR “microcomputer” OR “mobile application” OR “user-centered design” OR “video game” OR “virtual reality” OR “wearable computer” OR “ambient intelligence” OR “audiovisual aids” OR “data display” OR “game theory” OR “human-computer interaction” OR “medical informatics applications” OR “smartphone” OR “smart glasses” OR “user-computer interface” OR “video games” OR “wearable electronic devices” OR “3D environment” OR “3-D environment” OR “AI” OR “augmented virtuality” OR “close-to-reality” OR “computer environment” OR “digital tools” OR “enhanced realism” OR “enhanced reality” OR “extended reality” OR “game-based” OR “gamification” OR “haptic-based” OR “haptic technology” OR “immersive virtual reality” OR “immersive virtual environment” OR “realistic scenarios” OR “real-world scenarios” OR “smart electronic devices” OR “smart wearables” OR “virtual patient” OR “virtual scenarios” OR “virtual worlds” OR “VR” OR “wearable technologies” OR “Wearable Proximity Sensors” OR Wearable OR GPS OR “GPS-Based” OR “High-Fidelity” OR “Serious games”) AND (“first responders” OR “medical intern” OR “healthcare provider” OR “Paramedics” OR “Health Personnel” OR “Nurses” OR “Physicians”) AND (“Education” OR “Simulation Training” OR Training OR “Feedback training” OR “Simulation-based education” OR “Real-world training” OR “Interprofessional Education” OR “Competency-Based Education”) AND (“evaluate” OR “assess” OR “train” OR “outcomes”) |
| PsycNet | ((Any Field: (“mass casualty incident”) OR Any Field: (“crisis”) OR Any Field: (“Disasters”) OR Any Field: (“aircraft accident”) OR Any Field: (“avalanche”) OR Any Field: (“biological accident”) OR Any Field: (“biohazard release”) OR Any Field: (“bioterrorism”) OR Any Field: (“bomb”) OR Any Field: (“chemical accident”) OR Any Field: (“chemical hazard release”) OR Any Field: (“chemical terrorism”) OR Any Field: (“cyclonic storm”) OR Any Field: (“disaster”) OR Any Field: (“drought”) OR Any Field: (“earthquake”) OR Any Field: (“emergency shelter”) OR Any Field: (“flood”) OR Any Field: (“landslide”) OR Any Field: (“mass-casualty incident”) OR Any Field: (“mass disaster”) OR Any Field: (“multiple trauma”) OR Any Field: (“natural disaster”) OR Any Field: (“nuclear accident”) OR Any Field: (“pandemic”) OR Any Field: (“radioactive hazard release”) OR Any Field: (“radiation accident”) OR Any Field: (“structure collapse”) OR Any Field: (“traffic accident”) OR Any Field: (“terrorism”) OR Any Field: (“tidal wave”) OR Any Field: (“tornado”) OR Any Field: (“wildfire”) OR Any Field: (“catastrophe”) OR Any Field: (“catastrophic accident”) OR Any Field: (“CBRN”) OR Any Field: (“CBRNe”) OR Any Field: (“high-risk situations”) OR Any Field: (“human-made disasters”) OR Any Field: (“terrorist attack”))) AND ((Any Field: (“eye-tracking”) OR Any Field: (“Technology”) OR Any Field: (“virtual reality”) OR Any Field: (“augmented reality”) OR Any Field: (“mixed reality”) OR Any Field: (“biometric sensors”) OR Any Field: (“electroencephalogram”) OR Any Field: (“digital monitoring”) OR Any Field: (“motion tracking”) OR Any Field: (“wearable devices”) OR Any Field: (“performance dashboards”) OR Any Field: (“psychophysiological tools”) OR Any Field: (“galvanic skin response”) OR Any Field: (“pupillometry”) OR Any Field: (“heart rate variability”) OR Any Field: (“Eye-Tracking Technology”) OR Any Field: (“Galvanic Skin Response”) OR Any Field: (“artificial intelligence”) OR Any Field: (“augmented reality”) OR Any Field: (“human computer interaction”) OR Any Field: (“human machine interface”) OR Any Field: (“microcomputer”) OR Any Field: (“mobile application”) OR Any Field: (“user-centered design”) OR Any Field: (“video game”) OR Any Field: (“virtual reality”) OR Any Field: (“wearable computer”) OR Any Field: (“ambient intelligence”) OR Any Field: (“audiovisual aids”) OR Any Field: (“data display”) OR Any Field: (“game theory”) OR Any Field: (“human-computer interaction”) OR Any Field: (“medical informatics applications”) OR Any Field: (“smartphone”) OR Any Field: (“smart glasses”) OR Any Field: (“user-computer interface”) OR Any Field: (“video games”) OR Any Field: (“wearable electronic devices”) OR Any Field: (“3D environment”) OR Any Field: (“3-D environment”) OR Any Field: (“AI”) OR Any Field: (“augmented virtuality”) OR Any Field: (“close-to-reality”) OR Any Field: (“computer environment”) OR Any Field: (“digital tools”) OR Any Field: (“enhanced realism”) OR Any Field: (“enhanced reality”) OR Any Field: (“extended reality”) OR Any Field: (“game-based”) OR Any Field: (“gamification”) OR Any Field: (“haptic-based”) OR Any Field: (“haptic technology”) OR Any Field: (“immersive virtual reality”) OR Any Field: (“immersive virtual environment”) OR Any Field: (“realistic scenarios”) OR Any Field: (“real-world scenarios”) OR Any Field: (“smart electronic devices”) OR Any Field: (“smart wearables”) OR Any Field: (“virtual patient”) OR Any Field: (“virtual scenarios”) OR Any Field: (“virtual worlds”) OR Any Field: (“VR”) OR Any Field: (“wearable technologies”) OR Any Field: (“Wearable Proximity Sensors”) OR Any Field: (Wearable) OR Any Field: (GPS) OR Any Field: (“GPS-Based”) OR Any Field: (“High-Fidelity”) OR Any Field: (“Serious games”))) AND ((Any Field: (“first responders”) OR Any Field: (“medical intern”) OR Any Field: (“healthcare provider”) OR Any Field: (“Paramedics”) OR Any Field: (“Health Personnel”) OR Any Field: (“Nurses”) OR Any Field: (“Physicians”))) AND ((Any Field: (“Education”) OR Any Field: (“Simulation Training”) OR Any Field: (Training) OR Any Field: (“Feedback training”) OR Any Field: (“Simulation-based education”) OR Any Field: (“Real-world training”) OR Any Field: (“Interprofessional Education”) OR Any Field: (“Competency-Based Education”))) AND ((Any Field: (“evaluate”) OR Any Field: (“assess”) OR Any Field: (“train”) OR Any Field: (“outcomes”))) |
| Cochrane | (“mass casualty incident” OR “crisis” OR “Disasters” OR “aircraft accident” OR “avalanche” OR “biological accident” OR “biohazard release” OR “bioterrorism” OR “bomb” OR “chemical accident” OR “chemical hazard release” OR “chemical terrorism” OR “cyclonic storm” OR “disaster” OR “drought” OR “earthquake” OR “emergency shelter” OR “flood” OR “landslide” OR “mass-casualty incident” OR “mass disaster” OR “multiple trauma” OR “natural disaster” OR “nuclear accident” OR “pandemic” OR “radioactive hazard release” OR “radiation accident” OR “structure collapse” OR “traffic accident” OR “terrorism” OR “tidal wave” OR “tornado” OR “wildfire” OR “catastrophe” OR “catastrophic accident” OR “CBRN” OR “CBRNe” OR “high-risk situations” OR “human-made disasters” OR “terrorist attack”):ti,ab,kw AND (“eye-tracking” OR “Technology” OR “virtual reality” OR “augmented reality” OR “mixed reality” OR “biometric sensors” OR “electroencephalogram” OR “digital monitoring” OR “motion tracking” OR “wearable devices” OR “performance dashboards” OR “psychophysiological tools” OR “galvanic skin response” OR “pupillometry” OR “heart rate variability” OR “Eye-Tracking Technology” OR “Galvanic Skin Response” OR “artificial intelligence” OR “augmented reality” OR “human computer interaction” OR “human machine interface” OR “microcomputer” OR “mobile application” OR “user-centered design” OR “video game” OR “virtual reality” OR “wearable computer” OR “ambient intelligence” OR “audiovisual aids” OR “data display” OR “game theory” OR “human-computer interaction” OR “medical informatics applications” OR “smartphone” OR “smart glasses” OR “user-computer interface” OR “video games” OR “wearable electronic devices” OR “3D environment” OR “3-D environment” OR “AI” OR “augmented virtuality” OR “close-to-reality” OR “computer environment” OR “digital tools” OR “enhanced realism” OR “enhanced reality” OR “extended reality” OR “game-based” OR “gamification” OR “haptic-based” OR “haptic technology” OR “immersive virtual reality” OR “immersive virtual environment” OR “realistic scenarios” OR “real-world scenarios” OR “smart electronic devices” OR “smart wearables” OR “virtual patient” OR “virtual scenarios” OR “virtual worlds” OR “VR” OR “wearable technologies” OR “Wearable Proximity Sensors” OR Wearable OR GPS OR “GPS-Based” OR “High-Fidelity” OR “Serious games”):ti,ab,kw AND (“first responders” OR “medical intern” OR “healthcare provider” OR “Paramedics” OR “Health Personnel” OR “Nurses” OR “Physicians”):ti,ab,kw AND (“Education” OR “Simulation Training” OR Training OR “Feedback training” OR “Simulation-based education” OR “Real-world training” OR “Interprofessional Education” OR “Competency-Based Education”):ti,ab,kw AND (“evaluate” OR “assess” OR “train” OR “outcomes”):ti,ab,kw |
| Clinicaltrials.gov | (“mass casualty incident” OR “crisis” OR “Disasters” OR “aircraft accident” OR “avalanche” OR “biological accident” OR “biohazard release” OR “bioterrorism” OR “bomb” OR “chemical accident” OR “chemical hazard release” OR “chemical terrorism” OR “cyclonic storm” OR “disaster” OR “drought” OR “earthquake” OR “emergency shelter” OR “flood” OR “landslide” OR “mass-casualty incident” OR “mass disaster” OR “multiple trauma” OR “natural disaster” OR “nuclear accident” OR “pandemic” OR “radioactive hazard release” OR “radiation accident” OR “structure collapse” OR “traffic accident” OR “terrorism” OR “tidal wave” OR “tornado” OR “wildfire” OR “catastrophe” OR “catastrophic accident” OR “CBRN” OR “CBRNe” OR “high-risk situations” OR “human-made disasters” OR “terrorist attack”) AND (“eye-tracking” OR “Technology” OR “virtual reality” OR “augmented reality” OR “mixed reality” OR “biometric sensors” OR “electroencephalogram” OR “digital monitoring” OR “motion tracking” OR “wearable devices” OR “performance dashboards” OR “psychophysiological tools” OR “galvanic skin response” OR “pupillometry” OR “heart rate variability” OR “Eye-Tracking Technology” OR “Galvanic Skin Response” OR “artificial intelligence” OR “augmented reality” OR “human computer interaction” OR “human machine interface” OR “microcomputer” OR “mobile application” OR “user-centered design” OR “video game” OR “virtual reality” OR “wearable computer” OR “ambient intelligence” OR “audiovisual aids” OR “data display” OR “game theory” OR “human-computer interaction” OR “medical informatics applications” OR “smartphone” OR “smart glasses” OR “user-computer interface” OR “video games” OR “wearable electronic devices” OR “3D environment” OR “3-D environment” OR “AI” OR “augmented virtuality” OR “close-to-reality” OR “computer environment” OR “digital tools” OR “enhanced realism” OR “enhanced reality” OR “extended reality” OR “game-based” OR “gamification” OR “haptic-based” OR “haptic technology” OR “immersive virtual reality” OR “immersive virtual environment” OR “realistic scenarios” OR “real-world scenarios” OR “smart electronic devices” OR “smart wearables” OR “virtual patient” OR “virtual scenarios” OR “virtual worlds” OR “VR” OR “wearable technologies” OR “Wearable Proximity Sensors” OR Wearable OR GPS OR “GPS-Based” OR “High-Fidelity” OR “Serious games”) AND (“first responders” OR “medical intern” OR “healthcare provider” OR “Paramedics” OR “Health Personnel” OR “Nurses” OR “Physicians”) AND (“Education” OR “Simulation Training” OR Training OR “Feedback training” OR “Simulation-based education” OR “Real-world training” OR “Interprofessional Education” OR “Competency-Based Education”) AND (“evaluate” OR “assess” OR “train” OR “outcomes”) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



