Submitted:
05 October 2025
Posted:
06 October 2025
You are already at the latest version
Abstract
Introduction: Mass casualty incidents (MCIs), where casualty numbers exceed available emergency resources, are rising globally due to natural disasters, terrorism, and pandemics. Effective response requires well-trained healthcare professionals, yet training programs vary widely in structure and delivery. Previous reviews, such as Baetzner et al., focused on first responders and training effectiveness but offered limited insight into curriculum design across broader healthcare roles. Similarly, Bahattab et al. reviewed humanitarian health education in low- and middle-income countries but excluded high-income settings and did not examine the pedagogical design of MCI training for clinical professionals. This scoping review aims to map global evidence on how disaster and MCI training curricula are designed and implemented across diverse healthcare groups. Methods: This scoping review is conducted as part of the MCI-PHER project (Mass Casualty Incident – Prehospital Emergency Response), a collaborative initiative to advance disaster medicine education and prehospital preparedness. The review will follow the methodological framework by Arksey and O’Malley, with refinements from Levac et al., and will be reported according to the PRISMA-ScR guidelines. A comprehensive search of seven databases (PubMed, Embase, Scopus, PsycINFO, CINAHL, Cochrane Library, and ClinicalTrials.gov) will be conducted using a combination of MeSH terms and keywords. Studies published in English over the past ten years will be considered. Two independent reviewers will conduct study selection, data extraction, and quality checks, with disagreements resolved by a third reviewer. Data will be charted using a customized extraction tool, refined through piloting five relevant studies. Inclusion criteria will cover all healthcare learners (e.g., paramedics, nurses, physicians, medical students) in prehospital or in-hospital disaster training contexts. Both qualitative and quantitative studies, including grey literature, will be included. Results and Analysis: The review will map and synthesize existing literature on disaster and mass casualty incident (MCI) training curricula across healthcare disciplines. Extracted data will be organized into tables and figures, presenting curriculum structures, learner groups, instructional methods, competency frameworks, assessment strategies, and reported outcomes. Both quantitative findings (e.g., frequencies of approaches and participant characteristics) and qualitative insights (e.g., implementation experiences and contextual factors) will be summarized. This integrated analysis will highlight current practices, innovations, and gaps in disaster training education to inform future curriculum development and policy. Ethics and Dissemination: No ethical approval is required as no human participants are involved. Findings will be disseminated through peer-reviewed publications, conference presentations, policy briefs, and stakeholder engagement.
Keywords:
disaster medicine
; mass casualty incident
; curriculum design
; medical education
; simulation training
; emergency preparedness
; healthcare professionals
; competency-based training
Introduction
Background
A mass casualty incident (MCI) is defined as a situation in which the number and severity of casualties exceed the capacity of emergency medical services, overwhelming the entire system. MCIs can result from both natural and human-made disasters. Common causes include terrorism, mass transportation accidents, fires, and natural disasters. In contrast, a multiple casualty incident involves a high number of casualties but remains within the manageable limits of available resources. However, a multiple casualty incident may escalate into a mass casualty incident if resources become insufficient and the system is overwhelmed [1].
Effective response to an MCI requires a structured approach, beginning with accurate triage and efficient allocation of resources to minimize preventable morbidity and mortality. The World Health Organization (WHO) has developed comprehensive guidelines to support healthcare providers and institutions in preparing for MCIs [2].
Mass Casualty Incidents (MCIs) can be categorized into several types. Planned events, such as large-scale sporting gatherings, fall under one category. Conventional incidents, which occur with some regularity, include transportation accidents, fires, and severe weather events. Another category involves hazardous exposures to chemical, biological, or radiological agents. Nuclear-related incidents, whether accidental or intentional—such as those resulting from acts of terrorism—also constitute a significant category. Lastly, catastrophic public health emergencies, including nuclear detonations, major explosions, large-scale hurricanes, or widespread outbreaks like pandemic influenza, represent some of the most severe forms of MCIs.
The initial step in response is the correct identification of an MCI, typically carried out by the first EMS personnel to arrive on the scene. Effectively navigating the complexity of MCIs hinges on adhering to the structured approach summarized by the five “S’s”:
- Scene safety assessment
- Scene size-up
- Send information
- Scene set-up
- START: Simple Triage and Rapid Treatment
This structured response framework is essential in organizing the chaos and facilitating effective disaster response training [3].
The increasing frequency of disasters, wars, and pandemics highlights the importance of comprehensive mass casualty incident (MCI) preparedness across all sectors, particularly the healthcare sector. An effective humanitarian health response requires interprofessional and interdisciplinary collaboration. Over time, ongoing responses to various crises have shaped and advanced emergency preparedness programs. In the 1970s, the International Committee of the Red Cross (ICRC) began offering training courses in humanitarian health, followed by Médecins Sans Frontières (MSF). In response to growing global crises, academic institutions began introducing humanitarian health courses in the 1990s. After the 9/11 attacks, healthcare systems were increasingly recognized as critical components of national security. This shift led to expanded federal funding and a heightened focus on enhancing public health infrastructure and hospital readiness for large-scale emergencies [4,5,6].
According to the Emergency Management Accreditation Program (EMAP), emergency preparedness programs are structured around four fundamental phases: mitigating the risk or reducing the severity of hazards; developing plans to enhance capability and capacity before an emergency occurs; ensuring a safe and effective response during the event; and facilitating recovery afterward [7]. An integrative review by Almukhlifi et al. found that the majority of emergency healthcare workers are inadequately prepared for disaster situations, though previous disaster experience was shown to have a positive impact on preparedness [8]. Glow et al. emphasized that training scenarios should be tailored to local resources and involve all relevant disciplines. This inclusive approach helps avoid training in “silos,” where different professional groups (such as physicians, nurses, or paramedics) train separately. Siloed training can hinder coordination and obscure role clarity during real emergencies, whereas interdisciplinary training fosters collaboration, mutual understanding, and effective team performance [9].
Objectives and Rationale
While recent literature, such as the systematic review by Baetzner et al., has evaluated the effectiveness of disaster training programs for medical first responders (MFRs), it remains unclear how disaster training curricula are structured and implemented across a broader range of healthcare learners and professionals. Their focus on measurable training outcomes (e.g., RCTs, pre-post testing) excluded a significant portion of the literature that describes curricular content, pedagogical strategies, and context-specific implementation, especially in settings where experimental evaluation may not be feasible. Similarly, only effectiveness indicators with sufficient informative value were considered, further narrowing the scope of their review and potentially overlooking innovative or contextually relevant training approaches that lack formal outcome measures [10].
Another recent scoping review by Bahattab et al. focused on humanitarian health education and training, specifically in the context of low- and middle-income countries (LMICs). While valuable, their review concentrated on international humanitarian response settings and excluded training programs in high-income countries, as well as those outside the humanitarian aid framework. Their scope was broader in terms of interdisciplinary humanitarian content (e.g., WaSH, ethics), but did not delve into the detailed structure or pedagogical strategies of disaster and mass casualty incident (MCI) training curricula aimed at clinical healthcare professionals [6].
This highlights the need for a broader synthesis of evidence that spans all income settings and focuses specifically on how disaster and MCI training curricula are designed, delivered, and evaluated across healthcare roles.
In this review, we aim to examine the existing literature on disaster and mass casualty incident (MCI) training curricula implemented around the world across all levels of prehospital care and in-hospital care, spanning paramedics, nurses, interns, residents, and physicians, with a focus on identifying curricular strategies, educational approaches, target audiences, and gaps. By including descriptive, qualitative, and mixed-methods studies, we seek to:
- Identify common educational approaches across different learner groups
- Highlight innovations such as simulation, VR, interprofessional learning, and community-integrated models
- Expose existing gaps in content coverage, target group inclusion, and training adaptability
- Provide a foundation for future research and curriculum development that supports system-wide disaster preparedness beyond MFRs alone
Methods
Protocol Design
This scoping review protocol was developed within the MCI-PHER (Mass-Casualty Incident—Prehospital Emergency Response) project, which advances a coordinated research agenda to strengthen disaster medicine education, drive training innovation, and enhance prehospital preparedness. The review will follow the Arksey and O’Malley methodological framework, incorporate updates recommended by Levac and colleagues, and adhere to PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) to ensure methodological rigor [11,12,13]. The methodology for this review was registered on Protocols.io in accordance with best practices for open science and research reproducibility [14].
Stage 1: Identifying the Research Question
Definitions
- Disaster medicine: A medical specialty focused on two key areas: delivering healthcare to individuals affected by disasters and leading medically related efforts in disaster preparedness, planning, response, and recovery across all phases of the disaster lifecycle [15].
- Disaster preparedness: This refers to the proactive measures and strategies implemented to minimize the effects of emergencies such as hurricanes, floods, earthquakes, and other disasters on individuals, communities, and institutions. It encompasses creating emergency response plans, preparing disaster-specific kits, maintaining critical supplies, and conducting routine drills and training sessions [16].
- Mass casualty incident (MCI): An MCI is an event in which the number and severity of victims surpass the available resources of emergency medical services, including personnel, equipment, and facilities. For example, a sudden surge of patients at a small rural clinic following a nearby industrial explosion can qualify as an MCI. More commonly recognized scenarios include large-scale disasters such as plane crashes, earthquakes, major traffic collisions, and structural collapses [1].
- Curriculum design: Curriculum design refers to the intentional and structured planning of instructional content within a course or program. It involves organizing what will be taught, determining who will deliver the instruction, and establishing the timeline for implementation; essentially serving as a roadmap for educators to guide the teaching and learning process [17].
- Simulation training: Simulation provides learners with the opportunity to build experience, confidence, and competence in managing specific, often rare conditions or scenarios that are not commonly encountered in real clinical settings [18].
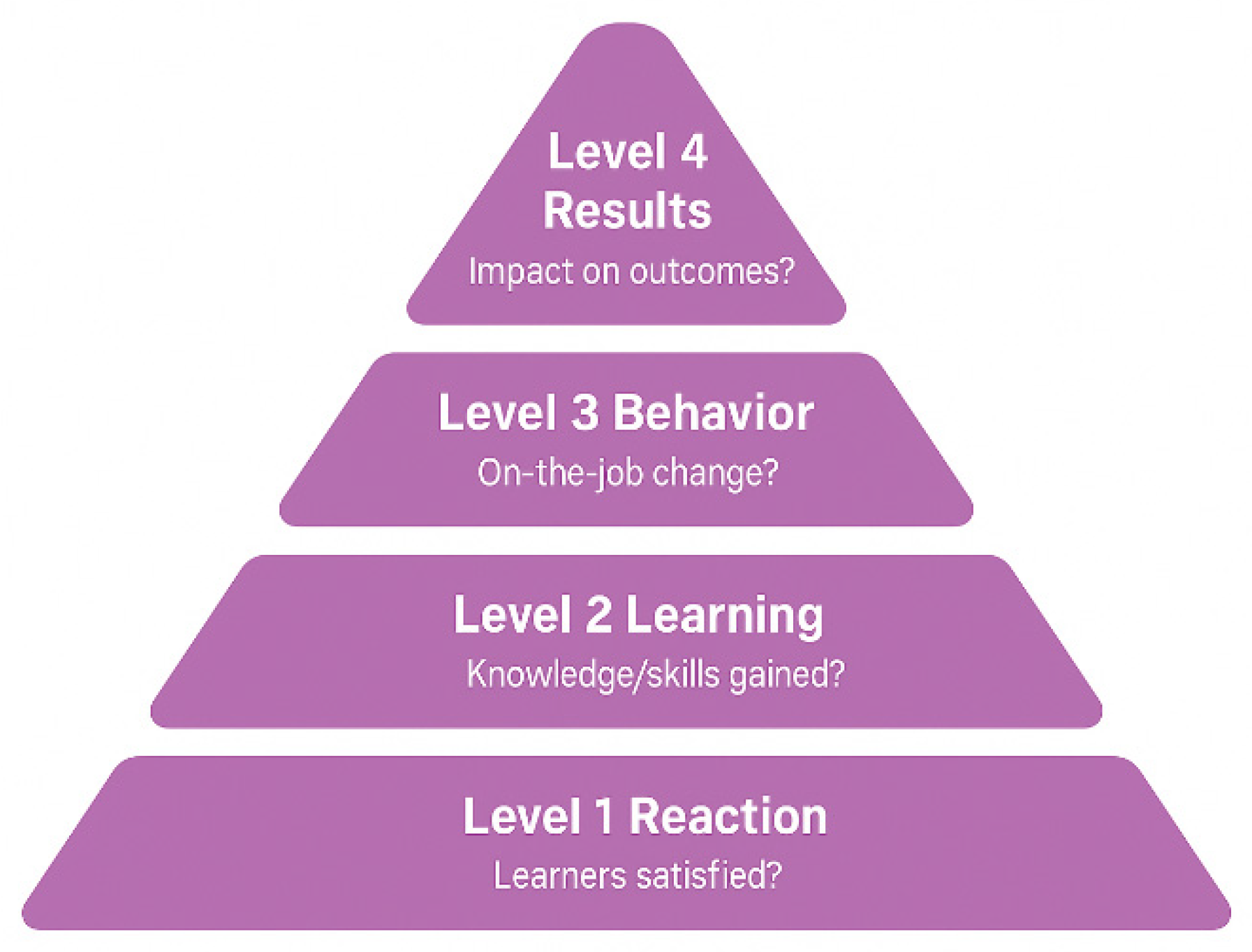
- Kirkpatrick’s model: The Kirkpatrick Model, introduced by Dr. Donald Kirkpatrick in 1959, is one of the most widely used frameworks for evaluating training effectiveness. It breaks down evaluation into four key levels to assess impact and outcomes:
This model helps assess training effectiveness by determining participant satisfaction, learning outcomes, real-world application, and organizational benefits [19].
Figure 1.
The Kirkpatrick Model.
Research Questions
The following are the questions we aim to address in this review:
Primary Research question:
- How are disaster and mass casualty incident (MCI) training curricula designed and implemented across different healthcare professionals globally?
Secondary Research questions:
- What types of educational settings (e.g., undergraduate, in-service) are used to deliver MCI training across healthcare professions?
- Which healthcare roles (e.g., paramedics, nurses, residents, physicians) are targeted in disaster training programs?
- What pedagogical strategies and teaching methods (e.g., simulation, PBL, tabletop exercises) are commonly employed in MCI/disaster training curricula?
- Which disaster competency frameworks (e.g., WHO EMT Standards, NDLS, Core Competencies for Disaster Medicine) are referenced in training programs?
- Which domains or themes (e.g., triage, logistics, leadership, communication) and specific competencies (e.g., PPE use, field triage, incident command) are emphasized in the curricula?
- What types of MCI scenarios (e.g., earthquake, flood, chemical spill, pandemic) are used in training simulations?
- How are training modalities (e.g., in-person, online, hybrid) and pacing models (e.g., fixed schedule vs. self-paced) applied across different programs?
- How is pre-simulation preparation structured (e.g., videos, handouts)?
- What assessment and evaluation methods (e.g., OSCE, pre/post-tests, surveys) are used to measure learning outcomes, and what level of the Kirkpatrick framework do they reach?
Stage 2: Identifying Relevant Studies
Information Sources
A comprehensive range of databases will be searched to ensure thorough coverage of relevant literature across disciplines. These include:
- PubMed – for peer-reviewed publications in the biomedical and life sciences
- Embase – offering broad biomedical coverage, including literature from European and Asian sources
- Scopus – encompassing scientific, technical, and medical research from various disciplines
- PsycINFO (via APA PsycNet) – for studies focusing on the psychological dimensions of training and education
- CINAHL (Cumulative Index to Nursing and Allied Health Literature) – for research related to nursing and allied health fields
- Cochrane Library – for accessing systematic reviews and evidence from clinical trials
- ClinicalTrials.gov – to identify registered clinical trials relevant to our review
- Google Scholar – to capture additional academic and grey literature
Search Strategy
An extensive search strategy was developed on June 12, 2025, using a combination of keywords and Medical Subject Headings (MeSH), identified through the MeSH database on PubMed (refer to Table 1 and Table 2). To ensure thoroughness, the search will be updated prior to final submission. In addition, Google Scholar and the reference lists of included studies and systematic reviews will be manually searched to identify any potentially missed studies.
Search Strategy Refinement
To enhance the accuracy and completeness of the search, the strategy will undergo peer review following the PRESS (Peer Review of Electronic Search Strategies) guidelines [20]. All revisions made during the development process will be recorded and shared with the research team to maintain full transparency.
Search Management
All search results will be imported into Covidence, a web-based platform designed for managing scoping and systematic reviews. Duplicate entries will be automatically detected and removed within the platform [21]. A manual hand-search will also be conducted to ensure no relevant studies are overlooked.
Documentation
A detailed record of the search process will be maintained, including the databases used, search terms applied, changes made to the strategy over time, and the number of records retrieved. This documentation will support transparency, reproducibility, and future updates of the review.
Stage 3: Study Selection
Screening
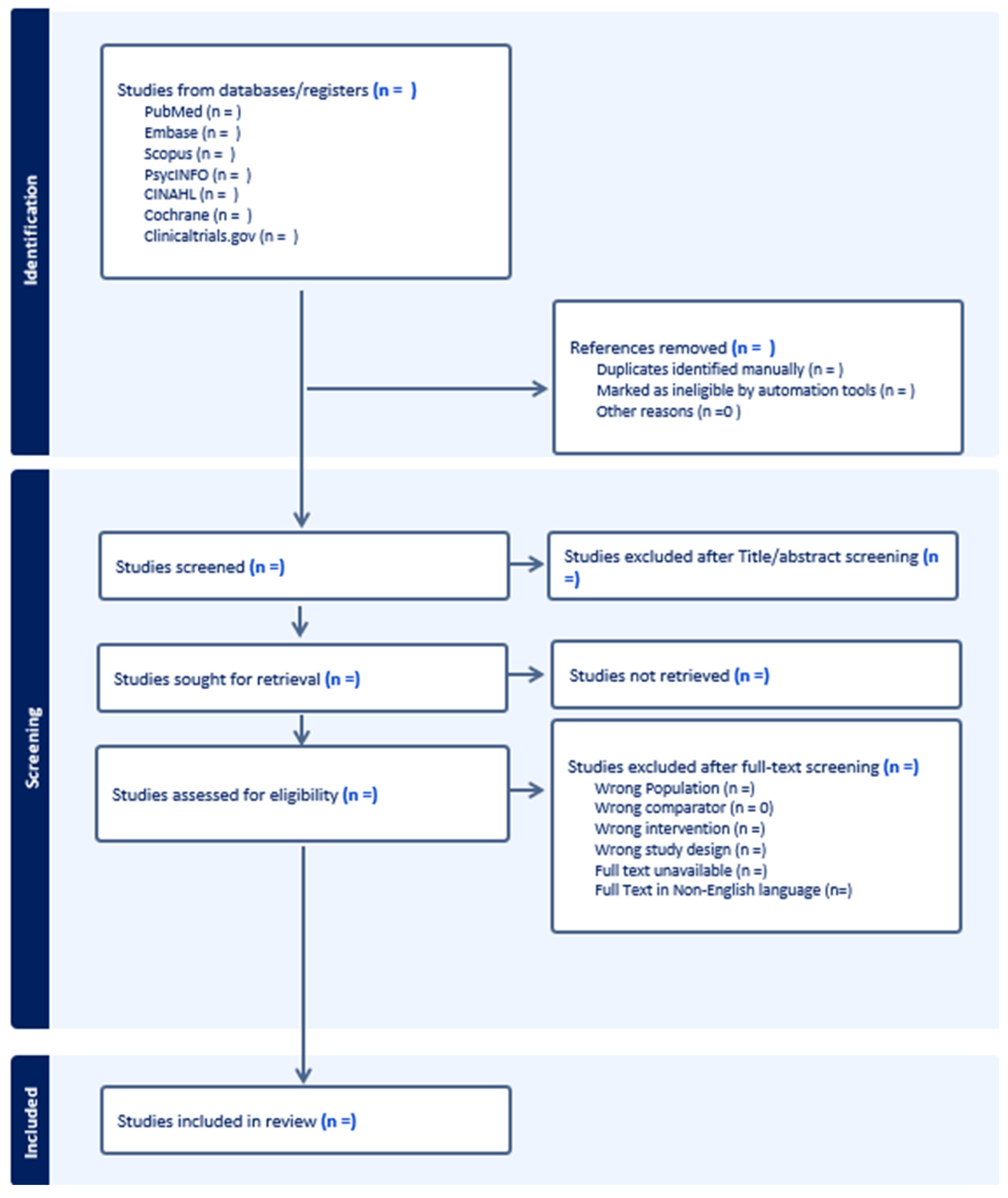
The study screening process will be managed through Covidence. A two-step approach will be employed: an initial review of titles and abstracts, followed by a full-text assessment. Two reviewers will independently evaluate all studies according to the predefined inclusion criteria. Any discrepancies between reviewers will be addressed through discussion, with a third reviewer consulted as needed to reach consensus. The overall selection process will be illustrated using a PRISMA flow diagram providing a clear visual summary of each screening stage (Figure 2).
Figure 2.
Prisma flow diagram.
Inclusion Criteria
Studies will be included if they:
-
Population:
- o
- Involve healthcare providers, including but not limited to physicians, nurses, paramedics, EMTs, residents, and interns.
- o
- Include university or college students enrolled in health-related fields (e.g., medicine, nursing, public health, EMS).
-
Concept:
- o
- Describe or evaluate curricular design strategies in disaster medicine or MCI training.
- o
- Focus on curriculum structure, delivery methods, learning outcomes, or training modalities.
-
Context:
- o
- Focus on disaster medicine or mass casualty incident (MCI) education and training.
- o
- Can include both prehospital and in-hospital training environments.
-
Study Types:
- o
- Include primary studies (quantitative, qualitative, or mixed methods), and curriculum development reports.
- o
- May include grey literature, such as conference abstracts or government/NGO reports, if they provide relevant curriculum detail.
- o
- Studies published in English, with a restriction on publication year to the last 10 years.
Exclusion Criteria
Studies will be excluded if they:
- Do not focus on disaster or MCI training (e.g., general emergency care, trauma surgery without a disaster context).
- Are solely focused on effectiveness evaluations without describing the curriculum structure or instructional design.
- Involve non-healthcare populations (e.g., military, engineers, general public) without a separate analysis for healthcare participants.
- Do not describe any form of curriculum content, strategy, or framework (e.g., focus only on knowledge/attitude assessments or survey perceptions).
- Are editorials, commentaries, or opinion pieces without empirical data or descriptive curriculum details.
- Systematic reviews, literature reviews, and other scoping reviews.
- Are not available in full text.
Stage 4: Data Charting
We will develop a standardized data extraction form by piloting five studies and identifying common variables relevant to curricular design in disaster medicine education. In addition, we will consult two prior reviews on related topics to guide the structure and content of the form [6,10]. This process will allow us to refine the charting tool to ensure it captures key elements across diverse study types and contexts. The data extraction tool will remain adaptable and may be revised iteratively as needed during the review to accommodate emerging themes.
| Field | Description |
| Study ID | Last name of author and year of publication. |
| Paper DOI | Digital Object Identifier of the paper, if available. |
| Country | The country where the study was conducted. |
| Study Design | Type of study (e.g., RCT, Qualitative, Cross-sectional, Review). |
| Target Population | Description of participants (e.g., EMS personnel, paramedics, medical students). |
| Educational Setting | Undergraduate, Postgraduate, In-service, CME. |
| Study Aim / Objective | Primary objective(s) or research question(s) of the study. |
| Duration of the Course | Time frame or length of the educational/training intervention (e.g., 2 weeks, 3 months, 4 sessions). |
| Curriculum Content | Topics covered in the intervention (e.g., triage, communication, first aid, disaster preparedness). |
| Delivery Modality | Format of instruction (e.g., online, face-to-face, blended, workshop, lecture, simulation-based). |
| Teaching Strategies | All instructional strategies used (e.g., role-play, case studies, debriefing, group discussion). |
| Pacing Model: Fixed vs. Self-Paced | Whether the course was scheduled and synchronous (fixed) or flexible and self-directed (self-paced). |
| Simulation Included? (Y/N) | Yes/No – whether simulation was part of the study. |
| Simulation Type | If simulation is included, specify type (e.g., tabletop, high-fidelity mannequin, virtual reality, drill). |
| MCI Type | Type of mass casualty incident used in scenario (e.g., earthquake, pandemic, explosion, chemical spill). |
| Information on Facilitator (if any) | Background or role of facilitators (e.g., clinical instructor, subject expert, external trainer). |
| Outcomes measured | List all measured outcomes (e.g., knowledge, skills, attitudes, confidence, performance). |
| Describe the findings (results) | Key findings reported by the study (quantitative and/or qualitative). |
| Comparator Present? | Yes/No – whether a comparator group or condition was included. |
| Elaborate on the comparator | If present, describe comparator (e.g., traditional lecture vs. simulation-based training). |
| Which disaster frameworks or systems are referenced or applied in the course? | Any disaster competency frameworks or operational protocols (e.g., START, ICS). |
| General Program Frameworks / Standards Referenced | Educational or professional frameworks guiding the curriculum (e.g., Bloom’s taxonomy, Kirkpatrick’s model, CANMEDS). |
| How was the Data Collected? | Methods of data collection (e.g., survey, exam, observation, interview, performance checklist). |
| Framework/model of training design? | If training design is explicitly based on a framework (e.g., ADDIE, Kern’s six-step approach). |
| Framework/model of assessment, if present | If the assessment uses a framework (e.g., Kirkpatrick, Miller’s pyramid, OSCE model). |
| Mention any cognitive support system or other scaffold | Any support structures provided to aid learning (e.g., decision aids, checklists, feedback, e-learning scaffolds). |
Stage 5: Collating, Summarizing, and Reporting the Results
Two independent reviewers will perform data screening to ensure consistency and accuracy by cross-checking key details from each study. Any discrepancies will be resolved through discussion or with input from a third reviewer when needed. Data will be managed and organized using Microsoft Excel.
Extracted data from the included studies will be compiled, summarized, and presented in tables, figures, and other visual formats to enhance clarity and facilitate a comprehensive overview of findings. This structured synthesis will map the existing literature on curriculum design strategies for disaster and mass casualty incident (MCI) training across healthcare disciplines.
Following data charting in Excel, the research team will conduct both systematic and narrative analyses to categorize the studies across key domains relevant to this review, including:
- Curriculum structure and design approaches
- Educational setting and learner level (e.g., undergraduate, in-service)
- Target healthcare populations (e.g., paramedics, nurses, physicians, students)
- Instructional methods and pedagogical strategies (e.g., simulation, PBL, lectures)
- Competency frameworks and disaster-specific standards referenced
- Assessment methods and evaluation levels (e.g., Kirkpatrick Model)
- Use and types of simulation, including roles, tasks, and real-world alignment
- Reported outcomes
Quantitative information (such as study frequencies, participant numbers, or training formats) will be analyzed descriptively. Qualitative data, including implementation experiences and contextual insights, will be examined through categorization and synthesis across domains. This integrated approach will allow us to explore both the scope and depth of how disaster training curricula are developed and delivered globally.
The review will also identify areas where evidence is limited and provide recommendations to guide future research, policy, and educational practice. All stages of the synthesis will be guided by the stated research questions and conducted in alignment with the PRISMA-ScR guidelines [13].
Stage 6: Stakeholder Consultation (Optional Stage)
Stakeholder consultation will be incorporated as a key component of the final reporting phase. This optional step is intended to actively involve relevant stakeholders engaged in disaster preparedness and emergency training. Participants may include EMS educators, emergency physicians, paramedics, disaster management officials, policymakers, and simulation specialists. Their input will help validate the review findings, offer additional insights, and highlight real-world applications and implications for disaster training practices.
Limitations
This review has several limitations. Limiting inclusion to English-language publications may introduce language bias and potentially exclude relevant studies published in other languages. Although the search strategy is designed to be comprehensive, some studies may be overlooked due to inconsistent indexing or limited access to certain sources.
While including grey literature helps reduce publication bias and broadens the evidence base, it may also lead to variation in the quality and reporting standards of the included materials. Additionally, significant differences in curriculum design, educational context, instructional methods, and evaluation approaches may pose challenges to comparing findings across studies. Methodological limitations, such as small sample sizes, lack of rigorous outcome measures, or limited detail on curricular components, may further affect the interpretation and generalizability of the results.
Despite these limitations, the review will provide valuable insights into how disaster and MCI training curricula are designed and implemented across diverse healthcare settings, while highlighting areas in need of further research and development.
Ethics and Dissemination
Ethical Considerations
This scoping review will not involve primary data collection or interaction with human participants and, therefore, does not require ethical approval. Nevertheless, the review will be conducted in line with established ethical research standards. This includes transparency in reporting methods and findings, proper citation of all sources, avoidance of plagiarism and duplicate publication, and impartiality in data synthesis and interpretation. Any potential conflicts of interest within the research team will be disclosed and managed appropriately.
Dissemination Strategy
The results of this review will be widely shared with stakeholders across emergency medicine and prehospital care to maximize their utility.
- Peer-Reviewed Publication
We will submit the final manuscript to a peer-reviewed journal focused on emergency medicine, disaster readiness, or simulation-based education.
- 2.
- Conference Presentations
Major findings will be presented at leading national and international meetings, including:
- World Association for Disaster and Emergency Medicine (WADEM)
- International Conference on Emergency Medicine (ICEM)
- National EMS conferences and simulation education events
- 3.
- Stakeholder Engagement
A concise brief will be distributed to:
- EMS organizations
- Disaster response agencies
- Simulation centers
- Prehospital training programs
We may also host webinars or roundtables with prehospital stakeholders to discuss practical implications and use cases.
- 4.
- Open Access and Preprints
We intend to publish in an open-access venue and may post a preprint of the scoping review on platforms like medRxiv to provide early access and visibility.
- 5.
- Professional Networks and Social Media
Key takeaways and infographics will be shared on LinkedIn, X (formerly Twitter), and ResearchGate to reach EMS professionals, educators, and researchers.
- 6.
- Policy Briefs
Short policy-oriented summaries emphasizing the importance of disaster and MCI curricula for preparedness will be circulated to health organizations and policy leaders.
- 7.
- Implementation and Collaboration
We will seek partnerships with EMS programs and disaster training institutions to pilot or adopt promising approaches identified in the review. A follow-up survey of stakeholders may assess real-world uptake.
- 8.
- Research Gaps and Agenda
Identified gaps will shape a forward research agenda, which we will share with funders and academic networks to catalyze further studies.
- 9.
- Review Updates
We plan to refresh this scoping review every 3–5 years to capture emerging evidence and innovations in tabletop-based prehospital preparedness.
Project Timeline
| Stage | Duration | Weeks |
| Planning & Protocol Development | 4 weeks | Weeks 1–4 |
| - Team meetings & protocol drafting | ||
| - Protocol registration (e.g., OSF) | ||
| Literature Search | 3 weeks | Weeks 5–7 |
| - Finalize and conduct search | ||
| - Grey literature and manual search | ||
| Study Selection | 6 weeks | Weeks 8–13 |
| - Title/abstract screening | ||
| - Full-text screening | ||
| Data Charting | 4 weeks | Weeks 14–17 |
| - Pilot and finalize charting form | ||
| - Extract data from included studies | ||
| Analysis & Synthesis | 6 weeks | Weeks 18–23 |
| - Thematic and descriptive analysis | ||
| - Identify trends, gaps, and insights | ||
| Report Writing | 4 weeks | Weeks 24–27 |
| - Draft, review, and finalize manuscript | ||
| Dissemination Activities | 5+ weeks | Weeks 28–32+ |
| - Prepare journal submission | ||
| - Presentations, briefs, stakeholder outreach |
Ongoing Coordination:
- Weekly team meetings to monitor progress
- Buffer time built into each phase to accommodate unforeseen delays
- Dissemination activities may continue beyond Week 32 due to conference and stakeholder engagement schedules
Funding
This review is supported by the MCI-PHER project (Mass Casualty Incident – Prehospital Emergency Response), funded through the Dubai Health Collaborative Stimulus Research Grant (CSRG) at Mohammed Bin Rashid University of Medicine and Health Sciences. The funding organization had no influence on the study design, data analysis, or manuscript preparation.
Acknowledgments
None to declare.
Conflicts of Interest
None to declare.
References
- World Health Organization. Mass casualty management systems: strategies and guidelines for building health sector capacity. 2007;34.
- Mass Casualty Management [Internet]. Available online: https://www.who.int/teams/integrated-health-services/clinical-services-and-systems/emergency-and-critical-care/mass-casualty-management (accessed on 24 June 2025).
- DeNolf RL, Kahwaji CI. EMS Mass Casualty Management. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available online: http://www.ncbi.nlm.nih.gov/books/NBK482373/ (accessed on 24 June 2025).
- Herstein JJ, Schwedhelm MM, Vasa A, Biddinger PD, Hewlett AL. Emergency preparedness: What is the future? Antimicrob Steward Healthc Epidemiol. 2021;1(1):e29.
- Implementing 9/11 Commission Recommendations | Homeland Security [Internet]. Available online: https://www.dhs.gov/implementing-911-commission-recommendations (accessed on 24 June 2025).
- Bahattab A, Trentin M, Hubloue I, Della Corte F, Ragazzoni L. Humanitarian health education and training state-of-the-art: a scoping review. Front Public Health. 2024 Jul 29;12:1343867.
- EMAP-Policies-Procedures-for-the-Development-of-an-American-National-Standards_March-22-2023_Final.pdf [Internet]. Available online: https://emap.org/wp-content/uploads/2024/08/EMAP-Policies-Procedures-for-the-Development-of-an-American-National-Standards_March-22-2023_Final.pdf (accessed on 1 October 2025).
- Almukhlifi Y, Crowfoot G, Wilson A, Hutton A. Emergency healthcare workers’ preparedness for disaster management: An integrative review. Journal of Clinical Nursing. 2021 Jul 12;jocn.15965.
- Glow SD, Colucci VJ, Allington DR, Noonan CW, Hall EC. Managing Multiple-Casualty Incidents: A Rural Medical Preparedness Training Assessment. Prehosp Disaster med. 2013 Aug;28(4):334–41.
- Baetzner AS, Hill Y, Roszipal B, Gerwann S, Beutel M, Birrenbach T, et al. Mass Casualty Incident Training in Immersive Virtual Reality: Quasi-Experimental Evaluation of Multimethod Performance Indicators. J Med Internet Res. 2025 Jan 27;27:e63241.
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. 2005 Feb;8(1):19–32.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implementation Sci. 2010 Dec;5(1):69.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018 Oct 2;169(7):467–73.
- Yussef HH, Abdelhamied NM, Elmisbah SA, Omayer A, Ali MA, Hubloue I, et al. Curricular Design Strategies in Disaster Medicine Education- A Scoping Review Protocol. 2025 Jul 3. Available online: https://www.protocols.io/view/curricular-design-strategies-in-disaster-medicine-g4fcbytix (accessed on 10 July 2025).
- School of Medicine and Health Sciences [Internet]. Disaster Medicine. Available online: https://ospe.smhs.gwu.edu/disaster-medicine (accessed on 13 August 2025).
- SafetyCulture [Internet]. 2023. Disaster Preparedness: A Guide. Available online: https://safetyculture.com/topics/disaster-preparedness/ (accessed on 25 June 2025).
- ThoughtCo [Internet]. How to Develop Effective Curriculum Design. Available online: https://www.thoughtco.com/curriculum-design-definition-4154176 (accessed on 25 June 2025).
- Davis D, Warrington SJ. Simulation Training and Skill Assessment in Emergency Medicine. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available online: http://www.ncbi.nlm.nih.gov/books/NBK557695/ (accessed on 25 June 2025).
- Falletta, S. Evaluating Training Programs: The Four Levels Donald L. Kirkpatrick, Berrett-Koehler Publishers, San Francisco, CA, 1996, 229 pp. The American Journal of Evaluation. 1998;19(2):259–61.
- McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. Journal of Clinical Epidemiology. 2016 Jul;75:40–6.
- Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org.

Table 1.
Keywords and MeSH terms.
| Population | Concept | Context |
| paramedic* | “Curriculum design” | “Disaster medicine” |
| “First responders” | “Instructional design” | “Disaster preparedness” |
| “Medical student” | “Educational strategies” | “Mass casualty incident” |
| physician* | “Curriculum”[Mesh] | “Emergency preparedness” |
| intern* | “Mass Casualty Incidents”[Mesh] | |
| nurse* | “Disaster Medicine”[Mesh] | |
| “Healthcare provider” | “Disaster Planning”[Mesh] | |
| “Paramedics”[Mesh] | ||
| “Health Personnel”[Mesh] | ||
| “Nurses”[Mesh] | ||
| “Physicians”[Mesh] |
Table 2.
Search Strategy.
| Database | Search strategy |
|---|---|
| PubMed | (“disaster medicine” OR “disaster preparedness” OR “mass casualty incident” OR “emergency preparedness” OR “Mass Casualty Incidents”[MeSH] OR “Disaster Medicine”[MeSH] OR “Disaster Planning”[MeSH]) AND (“curriculum design” OR “instructional design” OR “educational strategies” OR “Curriculum”[MeSH] OR “Education”[MeSH] OR “Simulation Training”[MeSH] OR “Teaching”[MeSH]) AND (“first responders” OR intern* OR “healthcare provider” OR “Paramedics”[MeSH] OR “Health Personnel”[MeSH] OR “Nurses”[MeSH] OR “Physicians”[MeSH]) AND (y_10[Filter]) |
| Scopus | ( TITLE-ABS-KEY ( “disaster medicine” OR “disaster preparedness” OR “mass casualty incident” OR “emergency preparedness” ) AND TITLE-ABS-KEY ( “curriculum design” OR “instructional design” OR “educational strategies” OR “simulation training” OR education* OR teaching OR training ) AND TITLE-ABS-KEY ( paramedic* OR “first responders” OR “medical student” OR physician* OR intern* OR nurse* OR “healthcare provider” ) ) AND PUBYEAR > 2014 AND PUBYEAR < 2026 AND ( EXCLUDE ( DOCTYPE, “re” ) ) AND ( EXCLUDE ( LANGUAGE, “Chinese” ) OR EXCLUDE ( LANGUAGE, “German” ) OR EXCLUDE ( LANGUAGE, “Russian” ) ) |
| Embase | #22 #21 AND (2015:py OR 2016:py OR 2017:py OR 2018:py OR 2019:py OR 2020:py OR 2021:py OR 2022:py OR 2023:py OR 2024:py OR 2025:py) #21 #8 AND #14 AND #20 #20 #15 OR #16 OR #17 OR #18 OR #19 #19 ’emergency preparedness’ #18 ’mass casualty incident’ #17 ’mass disaster’ #16 ’disaster preparedness’ #15 ’disaster medicine’ #14 #9 OR #10 OR #11 OR #12 OR #13 #13 ’teaching’ #12 ’educational model’ #11 ’curriculum development’ #10 ’education program’ #9 ’simulation training’ #8 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 #7 ’health care personnel’ #6 ’nurse’ #5 ’medical intern’ #4 ’physician’ #3 ’medical student’ #2 ’first responder (person)’ #1 ’paramedical personnel’ |
| PsycNET |
((Any Field: (paramedic*) OR Any Field: (“first responders”) OR Any Field: (“medical student”) OR Any Field: (physician*) OR Any Field: (intern*) OR Any Field: (nurse*) OR Any Field: (“healthcare provider”))) AND ((Any Field: (“curriculum design”) OR Any Field: (“instructional design”) OR Any Field: (“educational strategies”) OR Any Field: (“simulation training”) OR Any Field: (education*) OR Any Field: (teaching) OR Any Field: (training))) AND ((Any Field: (“disaster medicine”) OR Any Field: (“disaster preparedness”) OR Any Field: (“mass casualty incident”) OR Any Field: (“emergency preparedness”))) AND Year: 2015 To 2025 |
| CINAHL | (paramedic* OR “first responders” OR “medical student” OR physician* OR intern* OR nurse* OR “healthcare provider” ) AND (“curriculum design” OR “instructional design” OR “educational strategies” OR “simulation training” OR education* OR teaching OR training ) AND (“disaster medicine” OR “disaster preparedness” OR “mass casualty incident” OR “emergency preparedness”) Filter: last 10 years |
| Cochrane | paramedic* OR “first responders” OR “medical student” OR physician* OR intern* OR nurse* OR “healthcare provider”) in Title Abstract Keyword AND (“curriculum design” OR “instructional design” OR “educational strategies” OR “simulation training” OR education* OR teaching OR training) in Title Abstract Keyword AND (“disaster medicine” OR “disaster preparedness” OR “mass casualty incident” OR “emergency preparedness”) in Title Abstract Keyword Filter: last 10 years |
| ClinicalTrials.gov | (paramedic* OR “first responders” OR “medical student” OR physician* OR intern* OR nurse* OR “healthcare provider” ) AND (“curriculum design” OR “instructional design” OR “educational strategies” OR “simulation training” OR education* OR teaching OR training ) AND (“disaster medicine” OR “disaster preparedness” OR “mass casualty incident” OR “emergency preparedness”) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



