Submitted:
02 October 2025
Posted:
03 October 2025
You are already at the latest version
Abstract
Chronic pain remains a major clinical challenge, with current treatments often providing insufficient relief. Oxytocin, classically recognized for its roles in reproduction and social bonding, has gained increasing attention for its potential involvement in pain modulation. Evidence suggests that oxytocin influences both nociceptive processing and broader dimensions of pain, including stress regulation, emotional appraisal, and coping. Despite this promise, clinical findings remain mixed. In this opinion paper, we summarize and discuss the rationale and current clinical evidence for the role of oxytocin in chronic pain (management), highlighting key research gaps and outlining future directions focused on: endogenous oxytocin system variability, biological modulators of its effects, dosing and timing strategies, and the role of psychosocial context. We propose that oxytocin should be reconceptualized not as a straightforward analgesic, but as a biopsychosocial adjuvant that strengthens resilience and coping. Positioning oxytocin within this framework may clarify for whom, when, and under what conditions oxytocin can be most effective, and ultimately guide its translational potential in chronic pain management.
Keywords:
oxytocin
; chronic pain
; biopsychosocial framework
Introduction
Chronic pain remains one of the most pressing challenges in medicine, not only because of its sheer prevalence, but also because of the suffering it imposes on individuals and its vast socio-economic burden [1,2]. Despite advances in pharmacological, cognitive and behavioral therapies, many patients continue to experience inadequate relief [3]. The ongoing search for new strategies has drawn attention to oxytocin, a neuropeptide commonly known as the “bonding hormone”, but also increasingly considered for its potential to modulate pain, raising the question of how oxytocin might help shape the way pain is processed and managed.
Oxytocin is synthesized in the supraoptic and paraventricular nuclei of the hypothalamus [4]. From there, it is transported to the posterior pituitary, where it can be released into the bloodstream to exert peripheral hormonal effects, including uterine contractions and lactation [5]. Oxytocin also has documented anti-inflammatory and immunomodulatory properties, reducing the production of pro-inflammatory cytokines [6,7]. In addition to its peripheral roles, oxytocin is also released centrally, where it modulates neuronal activity through dendritic secretion and direct axonal projections [4]. This enables diffusion into multiple brain regions, where it plays a role in neurophysiological processes and supports a wide range of social functions including trust, empathy, social bonding, and the recognition of social cues [8,9,10,11].
Beyond its well-established reproductive, anti-inflammatory and social functions, oxytocin has been increasingly implicated in the modulation of pain [12,13]. Preclinical and some human studies suggest that oxytocin exerts analgesic effects by acting on both spinal and supraspinal levels [12,14,15,16]. At the spinal level, oxytocin modulates nociceptive input via projections to the dorsal horn, where oxytocin-receptors are expressed in dorsal root ganglia [15,17,18]. Oxytocin binding can suppress nociceptive signaling and inhibit sensitization, reducing pain transmission [16,19]. In supraspinal circuits, oxytocin modulates activity within regions central to pain perception and emotional appraisal, including the prefrontal cortex, anterior cingulate cortex, and amygdala [20,21,22]. Notably, oxytocin’s role in thalamic modulation of sensory pain remains limited, suggesting its primary effects may be on cognitive and affective dimensions of pain processing [16].
Oxytocin’s role in regulating stress and social behavior provides an additional mechanism through which it may impact pain perception. By promoting prosocial interactions, reducing stress reactivity, and enhancing coping mechanisms, oxytocin contributes to the biopsychosocial regulation of pain, see Figure 1 [10,23]. These findings align with the increasing recognition that chronic pain is best understood through a biopsychosocial framework, a perspective that views pain as the result of dynamic interactions among biological processes (such as tissue injury and neuroplasticity), psychological factors (including cognition, mood, and coping strategies), and social influences (such as support systems) [24,25]. This highlights the importance of addressing emotional and social factors alongside biological factors when assessing and managing pain.
Clinically, interest has grown in exogenous administration of oxytocin, particularly through intranasal delivery, which is non-invasive, allows flexible dosing, and provides a potential pathway for central nervous system effects. However, only few studies to date have investigated the use of intranasal oxytocin in chronic pain conditions and these demonstrated mixed findings on efficacy [26,27]. Despite promising preclinical results, results from human studies remain inconsistent and endogenous oxytocin levels appear to vary across chronic pain conditions [13]. These inconsistencies do not necessarily undermine oxytocin’s potential but rather highlight the complexity of the system: oxytocin not only dampens nociception but also shapes stress responses, emotional appraisal, and coping strategies [7,10,16]. Put differently, oxytocin may matter less for blocking nociceptive signals and more for how pain is experienced and managed [16].
Here we argue that oxytocin represents a biopsychosocial relevant candidate for chronic pain management. We summarize and critically discuss current clinical evidence, highlight key research gaps and outline directions for future research to clarify for whom, when, and under what conditions oxytocin may be most effective.
Current Clinical Evidence of Oxytocin’s Role in Chronic Pain
Over the past decades, clinical studies exploring oxytocin in the context of chronic pain have yielded intriguing but often inconsistent findings. Investigations have examined both endogenous oxytocin levels and the effects of exogenous oxytocin administration across various chronic pain conditions. The following section highlights studies investigating the role of oxytocin in individuals with chronic migraine, chronic musculoskeletal pain, fibromyalgia, and chronic abdominal pain. A summary can be found in Table 1.
Chronic Migraine
In chronic migraine, evidence suggests an elevation of endogenous oxytocin in plasma, saliva, and cerebrospinal fluid compared to healthy controls [28,29]. These studies predominantly involved adults aged between 19 and 65 years, with a majority of female subjects, reflecting the higher prevalence of chronic migraine in women. This increase in oxytocin may reflect a compensatory response to neuroinflammation, supported by findings of elevated cytokines in migraine pathophysiology [30,31]. Experimental work indicates that inflammation can upregulate oxytocin-receptor expression on trigeminal neurons, raising the possibility that higher oxytocin levels represent a feedback mechanism aimed at dampening nociceptive activity [32,33].
Clinical studies of exogenous oxytocin administration in migraine—mostly conducted in adults—are limited, but some demonstrate reduced headache frequency or delayed pain relief after intranasal delivery [29,30]. However, replication has been scarce, sample sizes remain small, and variability in outcomes suggests that endogenous pain states, neuroinflammatory load, and patient-specific oxytocin biology may interact with each other to determine treatment efficacy.
Chronic Musculoskeletal Pain
In the context of chronic musculoskeletal pain, endogenous oxytocin levels have, to our knowledge, only been assessed in one study [34]. This study found that men and women with chronic low back pain exhibited significantly lower oxytocin levels in plasma compared to healthy controls, while simultaneously showing elevated oxytocin concentrations in cerebrospinal fluid [34]. These findings suggest a differential regulation or compartmentalization of oxytocin release between central and peripheral systems.
Studies examining oxytocin administration in chronic musculoskeletal pain—including chronic back pain, pelvic pain, and neck/shoulder pain—typically involved adult participants aged 18 to 65 years, with sex distribution varying by condition; for instance, pelvic pain studies included mostly women, and back pain studies often had a higher proportion of men [20,26,27,34,35]. Intrathecal, intranasal, and systemic oxytocin administration have been associated with pain reduction in some contexts [27,34,35] but paradoxical pain enhancement in others, particularly in women with neck and shoulder pain [26]. Neuroimaging evidence further indicates that oxytocin administration in individuals with chronic low back pain modulates activity within key limbic regions such as the nucleus accumbens and caudate nucleus [20], regions known to integrate reward, stress regulation, and pain salience. Importantly, interindividual variability in pain-related brain responses to oxytocin was high, and psychological factors such as fear of pain and hypervigilance accounted for significant variance [20]. These findings underscore the possibility that oxytocin’s effects are not uniform but instead shaped by ongoing emotional and cognitive appraisal of pain, aligning with oxytocin’s broader role as a modulator of salience and social-emotional integration [8,10].
Fibromyalgia
Oxytocin research in fibromyalgia—a chronic disorder marked by widespread musculoskeletal pain, fatigue, and sleep disturbances—primarily involves adult women aged 18 to 70 years, reflecting its higher prevalence in females and older populations. Endogenous oxytocin levels do not consistently differ between fibromyalgia patients and controls [36,37]. Subgroup analyses reveal both elevated and reduced levels depending on symptom severity, comorbidities, and stress system dysfunction; for example patients with higher symptom burden show significantly lower oxytocin levels [36]. While Otero et al. [37] found that oxytocin levels were elevated in fibromyalgia-only patients compared to controls, with no difference when including those with comorbid chronic fatigue syndrome. Possibly, elevated levels of inflammatory cytokines in fibromyalgia may trigger an oxytocin increase as a compensatory anti-inflammatory response, especially within a disrupted hypothalamic-pituitary-adrenal (HPA) axis, as noted by the authors [37].
On the exogenous side, trials—almost exclusively in adult women—have produced largely negative or null results. For example, intranasal oxytocin often fails to reduce clinical pain or pain intensity scores [38]. Trial results may have been confounded by concurrent NSAID treatment, which could suppress oxytocin-receptor regulation by inflammatory signals [39]. Chronic elevations in endogenous oxytocin, as suggested in some patients, raise the possibility of receptor desensitization and diminished responsiveness to exogenous treatment [40]. A unifying theme emerging in fibromyalgia is the heterogeneity across patients, some show elevated baseline oxytocin possibly as a compensatory anti-stress signal [41], while others show reduced levels in relation to severe symptom burden. This variability complicates any straightforward therapeutic expectations.
Chronic Abdominal Pain
Studies on abdominal pain—including recurrent abdominal pain, irritable bowel syndrome (IBS) and inflammatory bowel disease—consistently report lower endogenous plasma oxytocin levels in affected individuals compared to healthy controls. For instance, Alfvén et al. [42] found that children with recurrent abdominal pain exhibited lower plasma oxytocin levels, a pattern that persisted after three months. Similarly, the same group reported decreased plasma oxytocin levels in children with recurrent abdominal pain or inflammatory bowel disease relative to controls [43]. These findings parallel the reduced oxytocin concentrations observed in chronic musculoskeletal pain populations and contrast with elevated oxytocin levels seen in chronic migraine and sometimes in fibromyalgia [42,43].
The administration of exogenous oxytocin, via intravenous, intranasal, or intrathecal routes, generally resulted in increased pain thresholds and reduced pain sensitivity in visceral pain models. Louvel et al. [44] demonstrated that continuous intravenous oxytocin infusions raised first sensation and pain thresholds during descending colon distension in IBS patients. However, clinical trials addressing daily abdominal pain and discomfort show mixed results. For example, Ohlsson and colleagues [45] observed no significant reductions in abdominal pain or discomfort with twice-daily intranasal oxytocin over 13 weeks, only a trend toward improvement. These results resemble the inconsistencies seen in fibromyalgia oxytocin trials and underscore that oxytocin’s analgesic efficacy in chronic abdominal pain is highly context- and population-dependent [44,45].
Current Clinical Evidence of Oxytocin’s Role in Chronic Pain—Across Studies
Taken together, clinical findings suggest that endogenous oxytocin profiles vary across pain conditions. In chronic migraine and fibromyalgia, elevated plasma oxytocin levels have been reported, possibly reflecting episodic flare-ups accompanied by inflammation that activates compensatory oxytocinergic mechanisms [36,37]. In contrast, chronic musculoskeletal pain has been associated with reduced oxytocin concentrations compared to healthy controls [34], possibly reflecting oxytocin system exhaustion due to the strain of persistent nociceptive input. Interestingly, recurrent abdominal pain has also been linked to lower oxytocin levels, but these findings are based on pediatric populations [42,43]. This raises the possibility that developmental factors play a role, since the oxytocin system is dynamic and known to fluctuate across the lifespan [46]. Indeed, oxytocin signaling appears to peak early in life, drop to lower basal levels during childhood and adolescence, rise again in adulthood, and later show altered receptor sensitivity with aging [46,47,48,49]. Considering these pain-condition and developmental variations, it is essential to account for heterogeneity in pain-related oxytocin outcomes.
Across studies, notable sex differences emerge in oxytocin’s role in pain, likely influenced by interactions with estrogen, which primes oxytocin synthesis, release, and receptor expression, and fluctuates throughout the menstrual cycle [13]. Women generally show higher endogenous oxytocin levels than men, which may partly explain their differential responses to exogenous administration [13,50]. This variability is well captured by an inverted U-shaped dose–response model, where moderate increases are beneficial, but excessive levels, particularly in those with high baseline oxytocin, may result in diminished or adverse effects [51]. For example, Tracy et al. [26] reported that intranasal oxytocin increased pain in women with chronic neck and shoulder pain, illustrating how hormone–oxytocin interactions can lead to counterintuitive results.
In general, findings on exogenous oxytocin administration in chronic pain are indeed mixed, with some studies reporting pain relief (e.g., reduced headache frequency in migraine [29]) while others describe null or even paradoxical effects, such as increased pain sensitivity in women with musculoskeletal pain [26,30]. These inconsistencies likely reflect individual variability in oxytocin system function, including baseline endogenous level, as well as demographic factors such as age and sex, and the influence of psychosocial context. Importantly, several studies indicate delayed onset of analgesia, suggesting that single-dose oxytocin paradigms may overlook optimal therapeutic windows. Neuroimaging work further supports that oxytocin modulates stress- and salience-related brain circuits rather than acting as a direct analgesic. Accordingly, these patterns point to oxytocin’s role as a contextual and modulatory agent, best considered within a biopsychosocial framework rather than as a stand-alone pharmacological treatment.
Research Gaps and Future Directions
Previous research on oxytocin and pain has yielded valuable insights. Clinical and preclinical studies have demonstrated that oxytocin can act at multiple levels of the nervous system, modulate affective and cognitive dimensions of pain, and interact with stress and social processes in ways highly relevant for chronic pain. However, despite this progress, critical mechanistic and translational gaps remain. Addressing these gaps is essential for refining therapeutic strategies and moving toward precision medicine. Below, we highlight key areas requiring attention, outline potential future directions, and propose hypotheses to guide this research.
Characterizing the Endogenous Oxytocin System Across Pain Populations
Most clinical studies investigated endogenous oxytocin within a single pain population, which limits direct comparison across conditions. As a result, meta-analytic findings remain inconsistent or even contradictory—some studies report elevated oxytocin concentrations in chronic migraine and fibromyalgia, while others find reduced levels in chronic musculoskeletal or abdominal pain populations [13]. Without between-condition comparison, it is unclear whether these discrepancies reflect true biological variation, methodological artifacts, or differences in pain type, duration, and extent. In particular, widespread pain conditions (e.g., fibromyalgia) may place different demands on the oxytocin system than more localized conditions (e.g., low back pain), and acute versus chronic pain may involve distinct trajectories of oxytocin signaling.
Future research should adopt comprehensive, comparative designs that evaluate oxytocin across multiple pain populations within the same study framework. Such work should explicitly compare widespread versus localized pain, and acute versus chronic pain states, to determine whether the oxytocin system adapts differently depending on pain extent and duration. In addition, longitudinal designs are needed to track oxytocin dynamics during transitions from acute to chronic pain, clarifying whether oxytocin patterns predict recovery or chronification.
We hypothesize that pain duration and extent shape endogenous oxytocin profiles, with widespread and chronic pain being associated with blunted or depleted oxytocin signaling, whereas acute or episodic pain eliciting compensatory elevations. These oxytocin phenotypes not only distinguish pain populations but also predict clinical course and treatment responsiveness.
Characterizing the Endogenous Oxytocin System Across the Lifespan
Developmental stage introduces an additional layer of complexity. For instance, pediatric studies of abdominal pain show reduced endogenous oxytocin, whereas adult chronic pain patients sometimes present with elevated oxytocin levels. These age-related differences in oxytocin signaling are in line with research showing fluctuations of the oxytocin system throughout the lifespan [46]. Given that pain vulnerability and stress regulation also change across the lifespan, developmental dynamics in oxytocin may be a critical but underexplored determinant of clinical outcomes.
Lifespan-sensitive studies should examine the endogenous oxytocin system in pediatric, adolescent, adult, and aging pain populations, within comparable methodological frameworks. Longitudinal pediatric studies could clarify whether reduced oxytocin contributes to persistence of pain into adulthood, while research in older adults could determine whether age-related decline or receptor-desensitization exacerbate pain vulnerability. Ideally, such work would integrate repeated oxytocin sampling and pain assessments to capture dynamic regulation across development.
We hypothesize that the developmental stage determines oxytocin signaling capacity in relation to pain, with reduced signaling in youth contributes to vulnerability for recurrent pain, while altered receptor sensitivity in aging increases risk of pain persistence and diminished responsiveness to exogenous oxytocin.
Characterizing Biological Modulators of Oxytocin’s Effect on Pain
Despite comprehensive preclinical research, mechanistic understanding of how oxytocin influences pain in humans still remains limited. While spinal and supraspinal actions are established, the contribution of biological modulators such as receptor-level dynamics, inflammation, and hormones (e.g., estrogen and cortisol) remains unclear. Chronic elevations of endogenous oxytocin may induce receptor desensitization [52,53], yet data on oxytocin-receptor expression and sensitivity in human chronic pain are scarce. Conversely, recent findings from children with autism suggest that oxytocin administration can stimulate the endogenous oxytocin system itself, potentially inducing epigenetic modifications of the oxytocin-receptor gene and creating a positive feed-forward loop that enhances long-term oxytocinergic signaling [54]. In parallel, inflammatory cytokines can upregulate oxytocin-receptor expression and promote oxytocin release [32], although these dynamics are still understudied within pain contexts. Sex hormones such as estrogen also shape oxytocin responses, possibly explaining sex-specific effects and paradoxical findings, with an inverted U-shaped dose–response curve suggesting that women with already higher baseline oxytocin levels may experience null or even adverse effects after exogenous administration (e.g., pain increase after oxytocin in women with neck/shoulder pain [26]). Finally, oxytocin and cortisol—a well-known stress hormone—are tightly interconnected as elevated cortisol appears to suppress oxytocin signaling, while oxytocin can attenuate HPA-axis activation and lower cortisol release [55,56]. For example, in healthy children, higher morning oxytocin predicted lower stress-induced cortisol in the afternoon—a protective feedback mechanism absent in children with autism, due to altered oxytocin dynamics [57]. In chronic pain, altered cortisol rhythms have also been described, with both hyper- and hypo-cortisolism linked to heightened pain sensitivity and impaired recovery [58]. This suggests that stress-axis functioning is a critical but still underexplored moderator of oxytocin’s effects in pain.
Future research should adopt advanced multimodal approaches, including receptor quantification (PET ligands when available), and panels of inflammatory, hormonal, and stress biomarkers, combined with clinical phenotyping. Studies should stratify participants by pain phenotype, sex, hormone status, and stress reactivity (e.g., via stress-induction paradigms) to examine how these moderators influence oxytocin’s efficacy.
We hypothesize that oxytocin’s effects on pain are shaped by multiple interacting biological modulators. At the receptor level, intermittent administration or moderate oxytocin dosing may stimulate receptor sensitivity, while sustained high levels risk desensitization. Inflammation is expected to act as a critical trigger, with cytokines promoting oxytocin release and engaging compensatory anti-nociceptive mechanisms. Sex hormones, particularly estrogen, likely influence baseline oxytocin levels and exogenous efficacy: individuals with lower oxytocin levels may benefit most, while those with higher levels may show paradoxical or null responses. Lastly, cortisol may play a dual role, with oxytocin dampening HPA-axis activation during acute stress, while chronic stress and persistently elevated cortisol could blunt oxytocinergic signaling.
Characterizing Dosing and Timing Effects of Oxytocin Administration
The optimal dosing and timing for oxytocin administration still remains unclear. One study in chronic migraine found a delayed analgesic effect, with significant pain reduction emerging only 2–4 hours after administration, pointing to the advantage of multiple-dose administration [30]. However, to date almost all oxytocin trials in pain employ single-dose paradigms. If there is to be a transition towards the therapeutic use of oxytocin administration, there is a critical need for studies on multiple-dose administration. When looking at oxytocin research outside the pain-field, it is apparent that repeated dosing enhances efficacy [54,59,60]. A recent clinical trial in autism suggests that intermittent oxytocin dosing, followed by positive social interaction, can optimize therapeutic effects and minimize the risk of desensitization, supporting the use of less frequent dosing schedules in clinical practice [61]. Furthermore, chronic intranasal oxytocin has been shown to exert anxiolytic effects, reducing neural responses to threat in a dose-frequency-dependent manner [62]. These findings reinforce the idea that not only the dose, but also the timing and context of oxytocin administration are critical for maximizing its therapeutic potential.
Future clinical trials should evaluate multiple-intermittent and context-sensitive dosing schedules. These should be paired with monitoring of stress reactivity, inflammatory and hormonal markers, as well as pain phenotype.
We hypothesize intermittent multiple-dose and context-integrated oxytocin administration (e.g., over weeks in combination with stress-coping interventions) produces more durable analgesic and affective benefits than acute dosing.
Conclusions
Oxytocin is a promising yet underutilized candidate for chronic pain management. Its combined (neuro)physiological, anti-inflammatory, and psychosocial effects align with contemporary biopsychosocial models of chronic pain [24]. Although preclinical evidence is compelling, clinical studies remain inconclusive due to methodological limitations. This opinion paper emphasizes the urgent need for hypothesis-driven, stratified, and translationally oriented research. By advancing our understanding of oxytocin’s mechanisms and clinical applications, we may uncover novel pathways to improve chronic pain treatment and patient well-being.
References
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Breivik, H.; Eisenberg, E.; O’bRien, T. The individual and societal burden of chronic pain in Europe: the case for strategic prioritisation and action to improve knowledge and availability of appropriate care. BMC Public Heal. 2013, 13, 1229–1229. [Google Scholar] [CrossRef] [PubMed]
- Ashcraft, L.E.; Hamm, M.E.; Omowale, S.S.; Hruschak, V.; Miller, E.; Eack, S.M.; Merlin, J.S. The perpetual evidence-practice gap: addressing ongoing barriers to chronic pain management in primary care in three steps. Front. Pain Res. 2024, 5, 1376462. [Google Scholar] [CrossRef] [PubMed]
- Jurek, B.; Neumann, I.D. The Oxytocin Receptor: From Intracellular Signaling to Behavior. Physiol. Rev. 2018, 98, 1805–1908. [Google Scholar] [CrossRef] [PubMed]
- Hermesch, A.C.; Kernberg, A.S.; Layoun, V.R.; Caughey, A.B. Oxytocin: physiology, pharmacology, and clinical application for labor management. Am. J. Obstet. Gynecol. 2023, 230, S729–S739. [Google Scholar] [CrossRef]
- Naeem MY, Alp Arici EC, Abbas S, Selamoglu Z. Current Research on the Relationships between Oxytocin and the Immune System: An Updated Study. Archives of Razi Institute. 2025.
- Carter, C.S. OXYTOCIN, LOVE AND THE COVID-19 CRISIS. 2020, 17, 195–195.
- Knobloch, H.S.; Charlet, A.; Hoffmann, L.C.; Eliava, M.; Khrulev, S.; Cetin, A.H.; Osten, P.; Schwarz, M.K.; Seeburg, P.H.; Stoop, R.; et al. Evoked Axonal Oxytocin Release in the Central Amygdala Attenuates Fear Response. Neuron 2012, 73, 553–566. [Google Scholar] [CrossRef]
- Kendrick KM, Guastella AJ, Becker B. Overview of human oxytocin research. Behavioral pharmacology of neuropeptides: Oxytocin. 2017:321-48.
- Marsh, N.; Marsh, A.A.; Lee, M.R.; Hurlemann, R. Oxytocin and the Neurobiology of Prosocial Behavior. Neurosci. 2020, 27, 604–619. [Google Scholar] [CrossRef]
- Folorunsho, I.L.; Harry, N.M.; Udegbe, D.C.; Jessa, D. Impact of oxytocin on social bonding and its potential as a treatment for social anxiety disorder. World J. Biol. Pharm. Heal. Sci. 2024, 19, 197–204. [Google Scholar] [CrossRef]
- Rash JA, Aguirre-Camacho A, Campbell TS. Oxytocin and pain: A systematic review and synthesis of findings. Clinical Journal of Pain: Lippincott Williams and Wilkins; 2014. p. 453-62.
- Mekhael, A.A.; Bent, J.E.; Fawcett, J.M.; Campbell, T.S.; Aguirre-Camacho, A.; Farrell, A.; Rash, J.A. Evaluating the efficacy of oxytocin for pain management: An updated systematic review and meta-analysis of randomized clinical trials and observational studies. Can. J. Pain 2023, 7, 2191114. [Google Scholar] [CrossRef]
- Zubrzycka, M.; Janecka, A. Interactions of galanin with endomophin-2, vasopressin and oxytocin in nociceptive modulation of the trigemino-hypoglossal reflex in rats. Physiol. Res. 2008, 57, 769–776. [Google Scholar] [CrossRef]
- Yang, J.; Yang, Y.; Chen, J.-M.; Liu, W.-Y.; Wang, C.-H.; Lin, B.-C. Central oxytocin enhances antinociception in the rat. Peptides 2007, 28, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Boll, S.; Almeida de Minas, A.C.; Raftogianni, A.; Herpertz, S.C.; Grinevich, V. Oxytocin and Pain Perception: From Animal Models to Human Research. Neuroscience 2018, 387, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Millan MJ, Schmauss C, Millan MH, Herz A. Vasopressin and oxytocin in the rat spinal cord: analysis of their role in the control of nociception. Brain research. 1984;309(2):382-3.
- Condés-Lara, M.; Rojas-Piloni, G.; Martínez-Lorenzana, G.; Rodríguez-Jiménez, J.; Hidalgo, M.L.; Freund-Mercier, M.J. Paraventricular hypothalamic influences on spinal nociceptive processing. Brain Res. 2006, 1081, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, M.; Sakai, A.; Ueta, Y. Pain modulation by oxytocin. Peptides 2024, 179, 171263. [Google Scholar] [CrossRef]
- Schneider, I.; Schmitgen, M.M.; Boll, S.; Roth, C.; Nees, F.; Usai, K.; Herpertz, S.C.; Wolf, R.C. Oxytocin modulates intrinsic neural activity in patients with chronic low back pain. Eur. J. Pain 2020, 24, 945–955. [Google Scholar] [CrossRef]
- Li, X.-H.; Matsuura, T.; Xue, M.; Chen, Q.-Y.; Liu, R.-H.; Lu, J.-S.; Shi, W.; Fan, K.; Zhou, Z.; Miao, Z.; et al. Oxytocin in the anterior cingulate cortex attenuates neuropathic pain and emotional anxiety by inhibiting presynaptic long-term potentiation. Cell Rep. 2021, 36, 109411. [Google Scholar] [CrossRef]
- Liu, Y.; Li, A.; Bair-Marshall, C.; Xu, H.; Jee, H.J.; Zhu, E.; Sun, M.; Zhang, Q.; Lefevre, A.; Chen, Z.S.; et al. Oxytocin promotes prefrontal population activity via the PVN-PFC pathway to regulate pain. Neuron 2023, 111, 1795–1811.e7. [Google Scholar] [CrossRef]
- Olivera-Pasilio, V.; Dabrowska, J. Oxytocin Promotes Accurate Fear Discrimination and Adaptive Defensive Behaviors. Front. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Holopainen, R. Biopsychosocial framework – pain impacting life on multiple biopsychosocial domains. Eur. J. Physiother. 2021, 23, 268–269. [Google Scholar] [CrossRef]
- Tracy, L.M.; Labuschagne, I.; Georgiou-Karistianis, N.; Gibson, S.J.; Giummarra, M.J. Sex-specific effects of intranasal oxytocin on thermal pain perception: A randomised, double-blind, placebo-controlled cross-over study. Psychoneuroendocrinology 2017, 83, 101–110. [Google Scholar] [CrossRef]
- Flynn, M.J.; Campbell, T.S.; Robert, M.; Nasr-Esfahani, M.; Rash, J.A. Intranasal oxytocin as a treatment for chronic pelvic pain: A randomized controlled feasibility study. Int. J. Gynecol. Obstet. 2020, 152, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Boström, A.; Scheele, D.; Stoffel-Wagner, B.; Hönig, F.; Chaudhry, S.R.; Muhammad, S.; Hurlemann, R.; Krauss, J.K.; Lendvai, I.S.; Chakravarthy, K.V.; et al. Saliva molecular inflammatory profiling in female migraine patients responsive to adjunctive cervical non-invasive vagus nerve stimulation: the MOXY Study. J. Transl. Med. 2019, 17, 53. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-L.; Yuan, Y.; Yang, J.; Wang, C.-H.; Pan, Y.-J.; Lu, L.; Wu, Y.-Q.; Wang, D.-X.; Lv, L.-X.; Li, R.-R.; et al. The interaction between the oxytocin and pain modulation in headache patients. Neuropeptides 2013, 47, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Tzabazis, A.; Kori, S.; Mechanic, J.; Miller, J.; Pascual, C.; Manering, N.; Carson, D.; Klukinov, M.; Spierings, E.; Jacobs, D.; et al. Oxytocin and Migraine Headache. Headache: J. Head Face Pain 2017, 57, 64–75. [Google Scholar] [CrossRef]
- You, D.S.; Haney, R.; Albu, S.; Meagher, M.W. Generalized Pain Sensitization and Endogenous Oxytocin in Individuals With Symptoms of Migraine: A Cross-Sectional Study. Headache: J. Head Face Pain 2017, 58, 62–77. [Google Scholar] [CrossRef]
- Szewczyk, A.K.; Ulutas, S.; Aktürk, T.; Al-Hassany, L.; Börner, C.; Cernigliaro, F.; Kodounis, M.; Cascio, S.L.; Mikolajek, D.; Onan, D.; et al. Prolactin and oxytocin: potential targets for migraine treatment. J. Headache Pain 2023, 24, 1–26. [Google Scholar] [CrossRef]
- Strother, L.C.; Srikiatkhachorn, A.; Supronsinchai, W. Targeted Orexin and Hypothalamic Neuropeptides for Migraine. Neurotherapeutics 2018, 15, 377–390. [Google Scholar] [CrossRef]
- Yang, J. Intrathecal Administration of Oxytocin Induces Analgesia in Low Back Pain Involving the Endogenous Opiate Peptide System. Spine 1994, 19, 867–871. [Google Scholar] [CrossRef]
- Boll, S.; Ueltzhoeffer, K.; Roth, C.; Bertsch, K.; Desch, S.; Nees, F.; Grinevich, V.; Herpertz, S.C. Pain-modulating effects of oxytocin in patients with chronic low back pain. Neuropharmacology 2020, 171, 108105. [Google Scholar] [CrossRef]
- Anderberg, U.M.; Uvnäs-Moberg, K. Plasma oxytocin levels in female fibromyalgia syndrome patients. Z. fur Rheumatol. 2000, 59, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Otero, E.; Gálvez, I.; Ortega, E.; Hinchado, M.D. Influence of Chronic Fatigue Syndrome Codiagnosis on the Relationship between Perceived and Objective Psychoneuro-Immunoendocrine Disorders in Women with Fibromyalgia. Biomedicines 2023, 11, 1488. [Google Scholar] [CrossRef] [PubMed]
- Mameli, S.; Pisanu, G.M.; Sardo, S.; Marchi, A.; Pili, A.; Carboni, M.; Minerba, L.; Trincas, G.; Carta, M.G.; Melis, M.R.; et al. Oxytocin nasal spray in fibromyalgic patients. Rheumatol. Int. 2014, 34, 1047–1052. [Google Scholar] [CrossRef] [PubMed]
- Kwong KK, Chan S-t. Intranasal oxytocin and NSAIDs: comment on: oxytocin nasal spray in fibromyalgic patients (Rheumatol Int. 2014 Aug; 34 (8): 1047-52.). Rheumatology international. 2015;35(5):941-2.
- Clodi, M.; Vila, G.; Geyeregger, R.; Riedl, M.; Stulnig, T.M.; Struck, J.; Luger, T.A.; Luger, A. Oxytocin alleviates the neuroendocrine and cytokine response to bacterial endotoxin in healthy men. Am. J. Physiol. Metab. 2008, 295, E686–E691. [Google Scholar] [CrossRef]
- Kuchenbecker, S.Y.; Pressman, S.D.; Celniker, J.; Grewen, K.M.; Sumida, K.D.; Jonathan, N.; Everett, B.; Slavich, G.M. Oxytocin, cortisol, and cognitive control during acute and naturalistic stress. Stress 2021, 24, 370–383. [Google Scholar] [CrossRef]
- Alfvén, G.; Torre, B.; Uvnäs-Moberg, K. Depressed concentrations of oxytocin and cortisol in children with recurrent abdominal pain of non-organic origin. Acta Paediatr. 1994, 83, 1076–1080. [Google Scholar] [CrossRef]
- Alfvén, G. Plasma oxytocin in children with recurrent abdominal pain. Journal of pediatric gastroenterology and nutrition. 2004;38(5):513-7.
- Louvel, D.; Delvaux, M.; Felez, A.; Fioramonti, J.; Bueno, L.; Lazorthes, Y.; Frexinos, J. Oxytocin increases thresholds of colonic visceral perception in patients with irritable bowel syndrome. Gut 1996, 39, 741–747. [Google Scholar] [CrossRef]
- Ohlsson, B.; Truedsson, M.; Bengtsson, M.; Torstenson, R.; Sjölund, K.; Björnsson, E.S.; Simrèn, M. Effects of long-term treatment with oxytocin in chronic constipation; a double blind, placebo-controlled pilot trial. Neurogastroenterol. Motil. 2005, 17, 697–704. [Google Scholar] [CrossRef]
- Audunsdottir K, Quintana DS. Oxytocin’s dynamic role across the lifespan. Aging Brain. 2022;2:100028.
- Ebner, N.C.; Maura, G.M.; MacDonald, K.; Westberg, L.; Fischer, H. Oxytocin and socioemotional aging: Current knowledge and future trends. Front. Hum. Neurosci. 2013, 7, 487. [Google Scholar] [CrossRef]
- Moerkerke, M.; Peeters, M.; de Vries, L.; Daniels, N.; Steyaert, J.; Alaerts, K.; Boets, B. Endogenous Oxytocin Levels in Autism—A Meta-Analysis. Brain Sci. 2021, 11, 1545. [Google Scholar] [CrossRef]
- Freeman, S.M.; Palumbo, M.C.; Lawrence, R.H.; Smith, A.L.; Goodman, M.M.; Bales, K.L. Effect of age and autism spectrum disorder on oxytocin receptor density in the human basal forebrain and midbrain. Transl. Psychiatry 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Baroni, S.; Mucci, F.; Piccinni, A.; Moroni, I.; Giannaccini, G.; Carmassi, C.; Massimetti, E.; Dell’osso, L. Sex-Related Differences in Plasma Oxytocin Levels in Humans. Clin. Pr. Epidemiology Ment. Heal. 2019, 15, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Borland, J.M.; Rilling, J.K.; Frantz, K.J.; Albers, H.E. Sex-dependent regulation of social reward by oxytocin: an inverted U hypothesis. Neuropsychopharmacology 2018, 44, 97–110. [Google Scholar] [CrossRef]
- Rajagopal, S.; Shenoy, S.K. GPCR desensitization: Acute and prolonged phases. Cell. Signal. 2018, 41, 9–16. [Google Scholar] [CrossRef]
- Robinson, C.; Schumann, R.; Zhang, P.; Young, R.C. Oxytocin-induced desensitization of the oxytocin receptor. Am. J. Obstet. Gynecol. 2003, 188, 497–502. [Google Scholar] [CrossRef]
- Moerkerke, M.; Daniels, N.; Tibermont, L.; Tang, T.; Evenepoel, M.; Van der Donck, S.; Debbaut, E.; Prinsen, J.; Chubar, V.; Claes, S.; et al. Chronic oxytocin administration stimulates the oxytocinergic system in children with autism. Nat. Commun. 2024, 15, 1–10. [Google Scholar] [CrossRef]
- Cardoso, C.; Kingdon, D.; Ellenbogen, M.A. A meta-analytic review of the impact of intranasal oxytocin administration on cortisol concentrations during laboratory tasks: Moderation by method and mental health. Psychoneuroendocrinology 2014, 49, 161–170. [Google Scholar] [CrossRef]
- Brown, C.A.; Cardoso, C.; Ellenbogen, M.A. A meta-analytic review of the correlation between peripheral oxytocin and cortisol concentrations. Front. Neuroendocr. 2016, 43, 19–27. [Google Scholar] [CrossRef]
- Evenepoel, M.; Moerkerke, M.; Daniels, N.; Chubar, V.; Claes, S.; Turner, J.; Vanaudenaerde, B.; Willems, L.; Verhaeghe, J.; Prinsen, J.; et al. Endogenous oxytocin levels in children with autism: Associations with cortisol levels and oxytocin receptor gene methylation. Transl. Psychiatry 2023, 13, 1–9. [Google Scholar] [CrossRef]
- Wyns, A.; Hendrix, J.; Lahousse, A.; De Bruyne, E.; Nijs, J.; Godderis, L.; Polli, A. The Biology of Stress Intolerance in Patients with Chronic Pain—State of the Art and Future Directions. J. Clin. Med. 2023, 12, 2245. [Google Scholar] [CrossRef]
- Horta, M.; Kaylor, K.; Feifel, D.; Ebner, N.C. Chronic oxytocin administration as a tool for investigation and treatment: A cross-disciplinary systematic review. Neurosci. Biobehav. Rev. 2020, 108, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Daniels, N.; Moerkerke, M.; Steyaert, J.; Bamps, A.; Debbaut, E.; Prinsen, J.; Tang, T.; Van der Donck, S.; Boets, B.; Alaerts, K. Effects of multiple-dose intranasal oxytocin administration on social responsiveness in children with autism: a randomized, placebo-controlled trial. Mol. Autism 2023, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Le, J.; Zhang, L.; Zhao, W.; Zhu, S.; Lan, C.; Kou, J.; Zhang, Q.; Zhang, Y.; Li, Q.; Chen, Z.; et al. Infrequent Intranasal Oxytocin Followed by Positive Social Interaction Improves Symptoms in Autistic Children: A Pilot Randomized Clinical Trial. Psychother. Psychosom. 2022, 91, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Kou, J.; Zhang, Y.; Zhou, F.; Gao, Z.; Yao, S.; Zhao, W.; Li, H.; Lei, Y.; Gao, S.; Kendrick, K.M.; et al. Anxiolytic Effects of Chronic Intranasal Oxytocin on Neural Responses to Threat Are Dose-Frequency Dependent. Psychother. Psychosom. 2022, 91, 253–264. [Google Scholar] [CrossRef]
- Rash JA, Campbell TS. The Effect of Intranasal Oxytocin Administration on Acute Cold Pressor Pain: A Placebo-Controlled, Double-Blind, Within-Participants Crossover Investigation. Psychosomatic Medicine. 2014;76(6):422-9.
- Goodin, B.R.; Anderson, A.J.B.B.; Freeman, E.L.B.; Bulls, H.W.B.; Robbins, M.T.; Ness, T.J. Intranasal Oxytocin Administration is Associated With Enhanced Endogenous Pain Inhibition and Reduced Negative Mood States. Clin. J. Pain 2015, 31, 757–767. [Google Scholar] [CrossRef]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef]
- Baettig, L.; Baeumelt, A.; Ernst, J.; Boeker, H.; Grimm, S.; Richter, A. The awareness of the scared - context dependent influence of oxytocin on brain function. Brain Imaging Behav. 2019, 14, 2073–2083. [Google Scholar] [CrossRef]
- Heinrichs, M.; Baumgartner, T.; Kirschbaum, C.; Ehlert, U. Social support and oxytocin interact to suppress cortisol and subjective responses to psychosocial stress. Biol. Psychiatry 2003, 54, 1389–1398. [Google Scholar] [CrossRef]
- Mescouto, K.; Olson, R.E.; Hodges, P.W.; Setchell, J. A critical review of the biopsychosocial model of low back pain care: time for a new approach? Disabil. Rehabilitation 2020, 44, 3270–3284. [Google Scholar] [CrossRef]
- Aygün, O.; Mohr, E.; Duff, C.; Matthew, S.; Schoenberg, P. Oxytocin Modulation in Mindfulness-Based Pain Management for Chronic Pain. Life 2024, 14, 253. [Google Scholar] [CrossRef]
- Adams, S.C.; DeLorey, D.S.; Davenport, M.H.; Stickland, M.K.; Fairey, A.S.; North, S.; Szczotka, A.; Courneya, K.S. Effects of high-intensity aerobic interval training on cardiovascular disease risk in testicular cancer survivors: A phase 2 randomized controlled trial. Cancer 2017, 123, 4057–4065. [Google Scholar] [CrossRef]
Figure 1.
Oxytocin’s role in the biopsychosocial framework of pain.
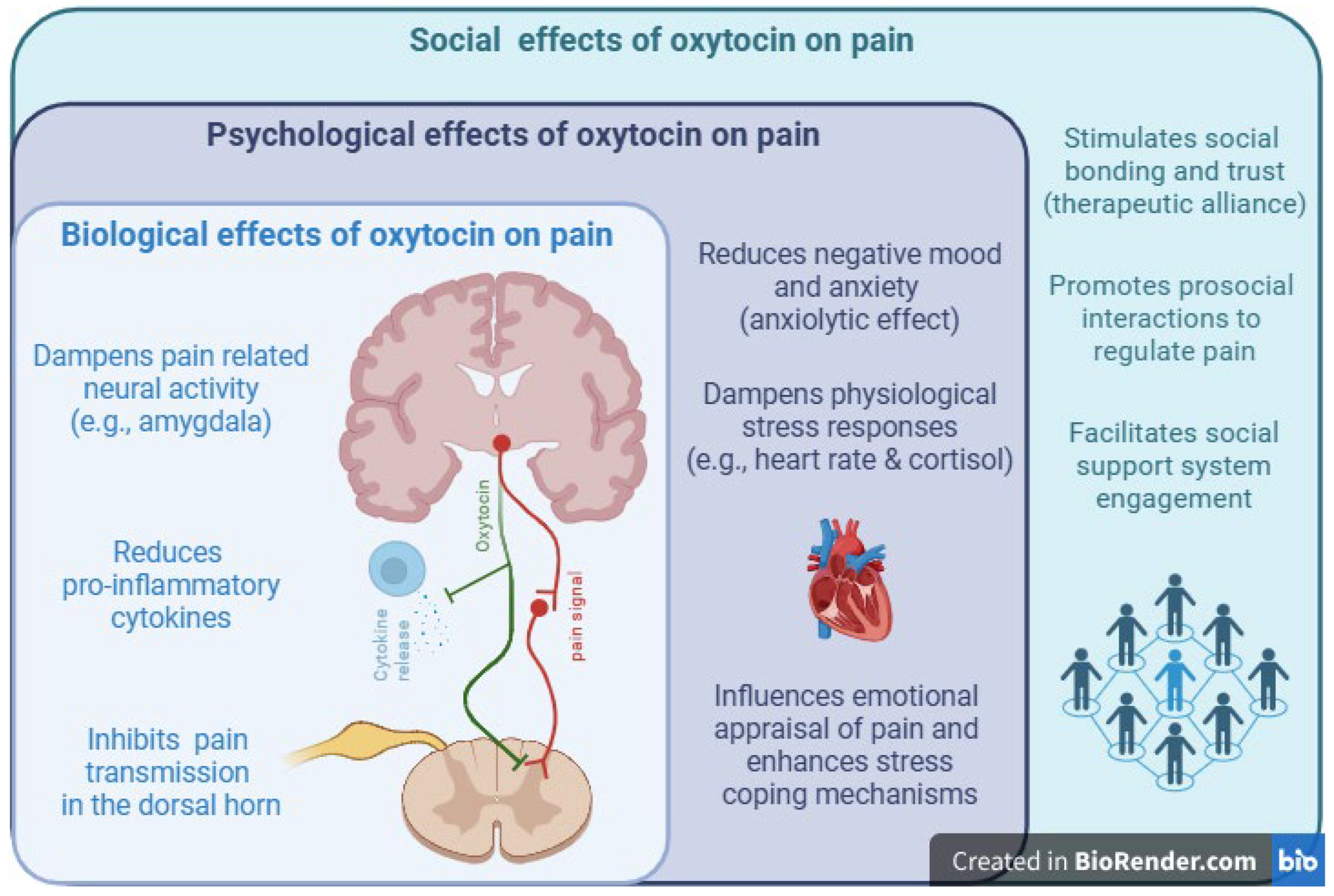

Table 1.
Summary of the current clinical evidence of oxytocin’s role in chronic pain.
| PAIN TYPE | ENDOGENOUS OXYTOCIN FINDINGS | EXOGENOUS OXYTOCIN ADMINISTRATION FINDINGS |
|---|---|---|
| CHRONIC MIGRAINE |
Elevated oxytocin in chronic migraine (♀/♂; aged 19-64; Wang et al., 2013), (♀; aged 22-65; Boström et al., 2019). No significant difference in plasma oxytocin, but trend toward elevation in migraine group (♀/♂; mean age 18.7; You et al., 2017). |
Intranasal oxytocin reduces headache frequency and pain in dose-dependent manner; higher doses yield stronger relief (♀/♂; aged 19-64; Wang et al., 2013), (♀/♂; age not mentioned; Tzabazis et al., 2017). |
| CHRONIC MUSCULOSKELETAL PAIN |
Reduced plasma oxytocin concentrations in chronic low back pain; elevated oxytocin in cerebrospinal fluid (♀/♂; mean age 47.3; Yang et al., 1994). Most studies focus on exogenous oxytocin only. |
Intranasal and intrathecal oxytocin administration yields pain reduction in chronic back pain and pelvic pain (♀; mean age 38; Flynn et al., 2020), (♂; mean age 36.8; Boll et al., 2020), (♀/♂; mean age 47.3; Yang et al., 1994). In women with chronic neck/shoulder pain, oxytocin may increase pain (♀/♂; aged 18-60; Tracy et al., 2017). Dose/sex/context-specific responses are possible, but robust pain attenuation has been shown (♂; aged 18-65; Schneider et al., 2020), (♂; mean age 36.8; Boll et al., 2020). |
| FIBROMYALGIA |
Elevated oxytocin in fibromyalgia, especially in those with high symptom burden (♀; aged 40-65; Otero et al., 2023). No difference to controls—greater variability observed (♀; aged 27-61; Anderberg et al., 2000). |
Intranasal oxytocin does not lead to significant pain reduction; effect possibly masked by concurrent NSAID use and receptor desensitization (♀; aged 18-70; Mameli et al., 2014). |
| CHRONIC ABDOMINAL PAIN | Reduced plasma oxytocin in recurrent abdominal pain; lower oxytocin associated with ongoing pain (♀/♂; aged 6-17; Alfvén et al., 1994; Alfvén, 2004) |
Intranasal oxytocin increased pain thresholds and reduced pain sensitivity (♂; aged 24-63) (Louvel et al. 1996). Oxytocin showed no significant reductions in abdominal pain or discomfort (♀; aged 20-70) (Ohlsson et al. 2005). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



