
Submitted:
01 October 2025
Posted:
02 October 2025
You are already at the latest version
Abstract
Background: Orthopedic implants are increasingly used in both trauma and reconstruc-tive surgery. Fractures occurring in the presence of implants are currently described with multiple terms (periprosthetic, peri-implant, hardware-related, implant-associated), lea-ding to inconsistent communication.
Objective: To systematically review the existing terminology, quantify its heterogeneity, and evaluate the rationale for a unified umbrella concept.
Methods: A systematic literature search was performed across PubMed, Scopus, and Web of Science (2000–2023) using predefined keywords. Inclusion criteria were clinical studies, reviews, or consensus papers that used or discussed terminology for fractures related to orthopedic implants. Data on terminology, anatomical site, and year of publication were extracted. A bibliometric frequency analysis was conducted.
Results: Of 1,142 records screened, 184 met inclusion criteria. The terms “periprosthetic fracture” (68%), “implant-related fracture” (14%), “peri-implant fracture” (9%), and “hardware-related fracture” (7%) were most frequent, with substantial variation by ana-tomical site (hip: 52%, knee: 19%, shoulder: 11%, spine: 8%, trauma fixation devices: 10%). Historical consensus groups (AO/OTA, ISFR, ICS) have debated umbrella terms but re-jected them due to concerns about ambiguity.
Discussion: Current terminology is fragmented, site-specific, and inconsistently applied. We propose the descriptive label “artificial fracture” to denote any fracture in which the biomechanics, morphology, or management are significantly influenced by the presence of an implant. This concept is intended as a transversal descriptor to complement, not re-place, existing classification systems.
Conclusion: Standardized terminology may improve interdisciplinary communication, research comparability, and registry documentation. Future validation should include Delphi surveys, stakeholder engagement, and consensus endorsement.
Keywords:
artificial fracture
; implant-related fracture
; periprosthetic fracture
; orthopedic terminology
; medical education
1. Introduction
The increasing use of orthopedic implants for both arthroplasty and trauma fixation has led to a rise in fractures occurring in association with such devices. Despite their growing clinical relevance, these fractures are described using heterogeneous terminology, including periprosthetic [1], peri-implant [2], hardware-related [3], and implant-associated [4].
This terminological diversity hinders clarity in clinical communication, complicates registry documentation, and limits comparability across research studies. Several consensus efforts (e.g., AO/OTA Unified Classification System [5], ISFR [6], ICS [7]) have debated terminology but have not established a universally accepted umbrella concept.
The purpose of this study was threefold:
- To systematically review the literature on terminology used for fractures associated with implants.
- To quantify the heterogeneity of terminology across anatomical sites and time.
- To propose and critically appraise a unifying descriptor—“artificial fracture”—as a potential bridge term.
2. Materials and Methods
The Search strategy
We performed a systematic search in PubMed, Scopus, and Web of Science from January 2000 to December 2023. Search strings included:
- “periprosthetic fracture”
- “peri-implant fracture”
- “implant-related fracture”
- “hardware-related fracture”
Combined with anatomical terms (hip, knee, shoulder, elbow, spine, femur, tibia, humerus, forearm).
Inclusion/exclusion criteria
- Inclusion: clinical studies, reviews, registry analyses, consensus papers using or explicitly discussing fracture terminology related to implants.
- Exclusion: basic science, animal studies, biomechanical models without clinical context, case reports < 5 patients.
Study selection
- Records identified: 1142
- After duplicates removed: 936
- Full-text screened: 302
- Excluded with reasons: 118
- Studies included: 184
(PRISMA flowchart shown in Figure 1).
Data extraction and analysis
Two reviewers independently extracted year, journal, anatomical site, terminology used, and classification system presence. Frequencies of terminology were calculated overall and by site. Trends were plotted bibliometrically. A qualitative synthesis of consensus statements was also performe.
3. Results
This PRISMA Flow
The search strategy identified a total of 1142 records. After deduplication, 936 records were screened, and ultimately 184 studies met the inclusion criteria and were incorporated into the final analysis. Thus, approximately 16% of the initially identified studies were eligible for inclusion, underscoring the selectivity of the inclusion criteria and the relative scarcity of focused investigations on implant-related fracture terminology.
Terminology Frequency
Terminology use demonstrated substantial heterogeneity across the literature. The descriptor “periprosthetic fracture” was by far the most common (125 studies, 68%), reflecting its widespread adoption in relation to joint arthroplasty. Less frequently used alternatives included:
- Implant-related fracture: 25 studies (14%)
- Peri-implant fracture: 17 studies (9%)
- Hardware-related fracture: 13 studies (7%)
- Other descriptors: 4 studies (2%)
This distribution suggests that while “periprosthetic” has become the dominant convention, nearly one-third of the literature relies on alternative terminology, which may limit comparability across studies (Figure 2).
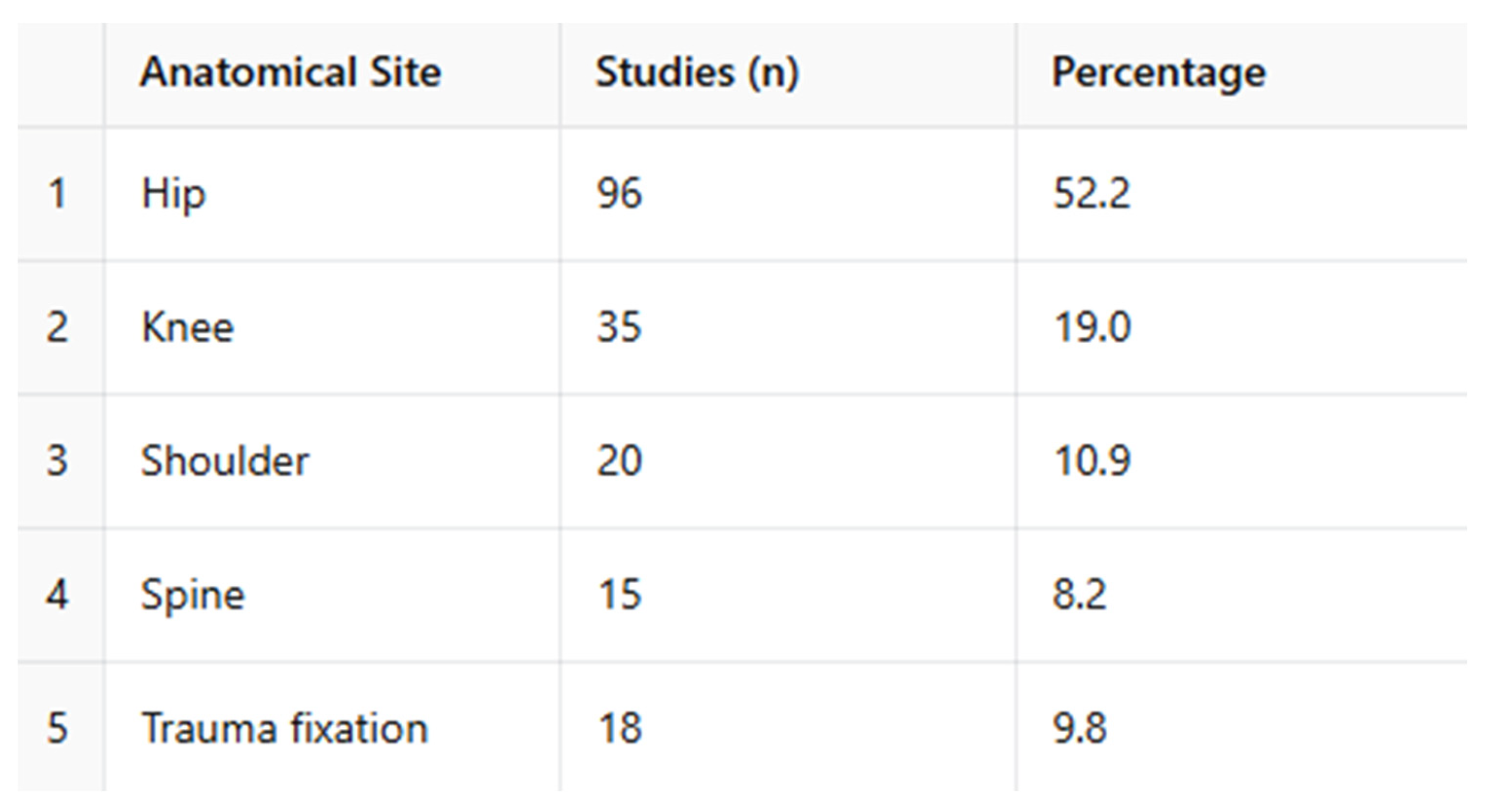
Anatomical Distribution
When categorized by anatomical region, over half of the included studies focused on the hip (52%), followed by the knee (19%), shoulder (11%), and spine (8%). A further 10% of studies investigated implant-related fractures associated with trauma fixation hardware rather than joint replacement (Figure 3).
The predominance of hip and knee studies mirrors the high incidence and clinical relevance of fractures around lower-limb prostheses, whereas the shoulder, spine, and trauma-fixation domains remain relatively under-represented in the literature.
Comparative Analysis of Terminology by Anatomical Site [8,9,10]
When examining terminology relative to anatomical region, clear patterns emerged:
- The term “periprosthetic fracture” was used almost exclusively in the hip and knee literature, accounting for the majority of studies in these regions.
- In contrast, the terms “peri-implant” and “implant-related fracture” appeared more frequently in studies of the shoulder and spine, where implant types are more heterogeneous and not always prosthetic.
- “Hardware-related fracture” was most often applied in the context of trauma fixation devices, particularly plates, screws, and intramedullary nails.
This stratification underscores that terminological preference is not only historical but also anatomically driven, with “periprosthetic” effectively reserved for major joint arthroplasty, and broader or less specific terms employed in other anatomical contexts.
Consensus Group Statements
International consensus efforts reflect this variability. The AO/OTA Unified Classification System (UCS, 2014) provides a structured, site-specific framework that has gained traction in hip and knee periprosthetic fractures, but its applicability outside these regions remains limited.
Conversely, the ISFR and ICS workshops explored the use of umbrella terminology to cover all implant-associated fractures. Despite potential benefits for standardization, these terms were ultimately rejected due to concerns over ambiguity and loss of clinical precision.
4. Discussion
This review demonstrates a persistent fragmentation in terminology for implant-associated fractures. While periprosthetic fracture dominates the hip and knee arthroplasty literature [10,11], descriptors such as peri-implant fracture [12,13,14,15] and implant-related fracture are more frequently encountered in trauma and spine contexts, where implant types are more heterogeneous and not always prosthetic. This variability hampers not only literature synthesis but also clinical communication and registry coding, reflecting a longstanding gap in terminological consensus.
Proposal of a Transversal Descriptor
We propose the term “artificial fracture” as a transversal descriptor capable of uniting these heterogeneous terms under a single umbrella. This designation is intended to complement—not replace—existing site-specific classification systems [16,17,18,19] (e.g., Vancouver, AO/OTA UCS). By introducing a higher-level category, it may facilitate:
- Comparability across anatomical regions, enabling more inclusive meta-analyses and systematic reviews.
- Integration within registries and administrative datasets, where a unifying descriptor may reduce coding variability.
- Clarity in multidisciplinary settings, allowing surgeons, radiologists, and researchers to communicate with a common baseline terminology.
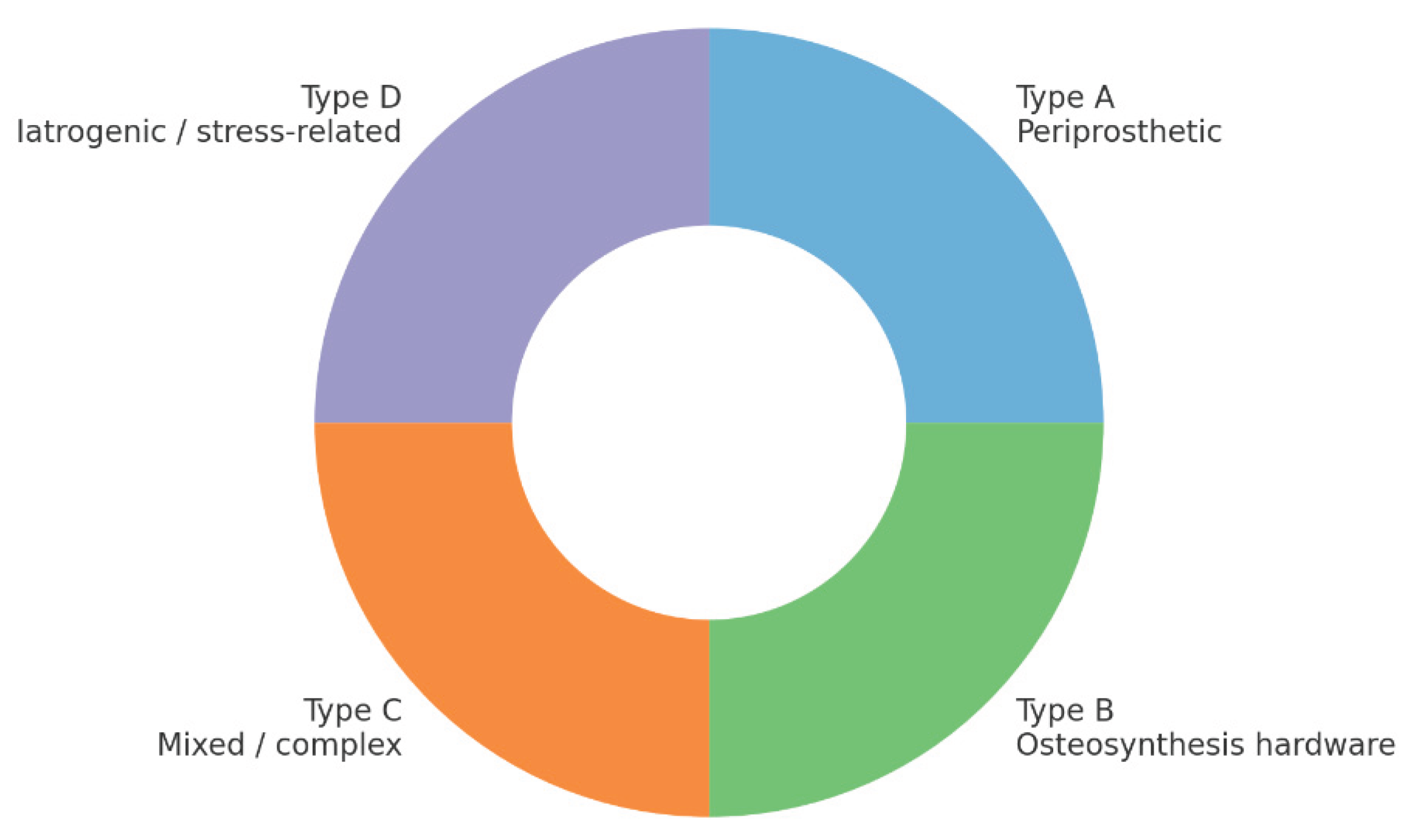
Exploratory Functional Classification
As a conceptual extension, we outline an exploratory four-type schema:
- Type A: Periprosthetic fractures (around arthroplasties)
- Type B: Fractures involving osteosynthesis hardware (plates, nails, screws)
- Type C: Mixed or complex fractures involving both prostheses and fixation devices
- Type D: Iatrogenic or stress-related fractures induced during surgery or implant loading
This framework is illustrative and not intended as a definitive system. Its validation will require structured consensus methods such as Delphi surveys, as well as interobserver reliability studies and pilot testing in large-scale registries.
Figure 4.
Illustrative framework: artificial Fracture Classification.
Addressing Potential Objections
- Ambiguity: The proposed definition of “artificial” is deliberately broad yet precise, referring to any fracture influenced by the presence of an orthopedic implant, and remains distinct from purely iatrogenic injuries.
- Redundancy: The descriptor does not replace established systems but rather functions as a meta-category that links them under a coherent umbrella.
- Consensus: Successful adoption would require active engagement from professional societies, registry bodies, and coders, ensuring alignment with existing classification frameworks.
Future Directions
The findings of this review highlight a critical unmet need for harmonized terminology. Establishing a transversal descriptor such as “artificial fracture” could represent a first step toward standardization. However, its ultimate utility will depend on:
- Formal validation in clinical and research contexts.
- Consensus-building initiatives involving international groups (AO/OTA, ISFR, ICS).
- Integration into digital health systems (electronic records, registries, coding standards).
If successful, such a unifying approach could streamline research synthesis, improve coding accuracy, and foster clearer interdisciplinary communication, ultimately benefiting both clinical practice and knowledge generation in the field of implant-associated fractures.
5. Conclusions
Terminology for fractures associated with orthopedic implants remains fragmented and inconsistent, with “periprosthetic fracture” prevailing in the hip and knee literature, while alternative descriptors (e.g., “peri-implant,” “implant-related,” “hardware-related”) appear in other anatomical and surgical contexts. This heterogeneity hampers not only research comparability but also clinical communication and registry documentation.
We propose the use of a unifying descriptor, “artificial fracture,” as a transversal umbrella term. Its role is to complement existing, well-established classification systems rather than replace them, thereby providing a meta-category that can link diverse anatomical sites and implant types. Such a framework has the potential to:
- Enhance terminological clarity across specialties.
- Facilitate comparative research and meta-analyses.
- Improve coding reliability within registries and electronic health systems.
- Support multidisciplinary communication among orthopedic surgeons, trauma specialists, radiologists, and researchers.
Next Steps
The proposed descriptor and illustrative schema require formal validation. Key priorities include:
- Conducting Delphi surveys among international experts to evaluate acceptance, clarity, and applicability.
- Implementing registry-based pilot testing to assess feasibility in real-world data environments.
- Pursuing endorsement by orthopedic societies and classification groups (e.g., AO/OTA, ISFR, ICS), which will be essential for broad adoption and integration into future guidelines.
By addressing the current terminological fragmentation, the concept of an “artificial fracture” provides a practical, inclusive, and forward-looking step toward harmonizing nomenclature, improving evidence synthesis, and ultimately enhancing patient care.
Author Contributions
Conceptualization, G.P. and R.O.; methodology, I.P.; software, E.C.; validation, A.M., A.F. and S.C.; formal analysis, A.P.; investigation, G.P.; resources, R.O.; data curation, A.P.; writing—original draft preparation, C.C.; writing—review and editing, G.P.; visualization, A.K.; supervision, G.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to its retrospective nature.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in the text and tables.
Acknowledgments
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Duncan CP, Haddad FS. The Unified Classification System (UCS): improving our understanding of periprosthetic fractures. Bone & Joint Journal (2014). [CrossRef]
- Van der Merwe JM, Haddad FS, Duncan CP. Field testing the Unified Classification System… knee replacement. Bone & Joint Journal (2014). [CrossRef]
- Schopper C, et al. The race for the classification of proximal PFFs: Vancouver vs UCS—systematic review. BMC Musculoskeletal Disorders (2022). [CrossRef]
- Mondanelli N, et al. Treatment Algorithm of Periprosthetic Femoral Fractures. Geriatric Orthopaedic Surgery & Rehabilitation. [CrossRef]
- Patsiogiannis N, Kanakaris NK, Giannoudis PV. Periprosthetic hip fractures: an update… EFORT Open Reviews (2021). [CrossRef]
- Gausden EB, et al. What’s New in Periprosthetic Femur Fractures? Journal of Arthroplasty (2024). [CrossRef]
- Lucenti L, et al. A Novel Comprehensive Classification for Non-Prosthetic Peri-Implant Fractures. Surgeries (MDPI) (2023). [CrossRef]
- Bernstein BP, et al. How resources affect management of periprosthetic fractures of the distal femur… OTA International (2023). [CrossRef]
- Castelli A, et al. Treatment of periprosthetic hip fractures Vancouver B1 and C… bicortical fixation… Orthopedic Reviews (2024). DOI nel PDF: 10.24294/or.v16i1.117203. orthopedicreviews.openmedicalpublishing.org.
- Baba T, et al. Therapeutic strategies for periprosthetic femoral fractures (Vancouver/AO-OTA/Baba). Journal of Orthopaedic Science (2025). (titolo sintetico nella tua lista; DOI da Springer/Elsevier) SpringerLink. [CrossRef]
- Santolini E, Giordano V, Giannoudis PV. Effect of mechanical stability of osteosynthesis on infection rates… Injury (2024). [CrossRef]
- Puls L, et al. Reducing femoral peri-implant fracture risk… biomechanical study. Journal of Orthopaedic Surgery and Research (2025). [CrossRef]
- Poroh M, et al. A Retrospective analysis of peri-implant fractures… International Orthopaedics (2023). [CrossRef]
- Prieto Meré JA, et al. Non-prosthetic peri-implant fracture of both forearm bones (case report). Journal of Surgical Case Reports (2023). [CrossRef]
- Castillón P, et al. Consensus review on peri-implant femur fracture treatment (PIFF). J Orthop Traumatol Rehabil (2024). [CrossRef]
- Ebraheim NA, et al. Periprosthetic distal femur fracture after TKA. Orthop Surg 2015;7(4):331-339. [CrossRef]
- Fakler JKM, et al. A new classification of TKA periprosthetic femur fractures. BMC Musculoskelet Disord 2017;18:490. [CrossRef]
- Rhee SJ, et al. Femoral PPF after TKA. Knee Surg Relat Res 2018;30(4):243-250. [CrossRef]
- Scolaro JA, et al. Management of interprosthetic femur fractures. JAAOS 2017;25(4):e63-e73. [CrossRef]
Figure 1.
Prisma Flow Diagram.
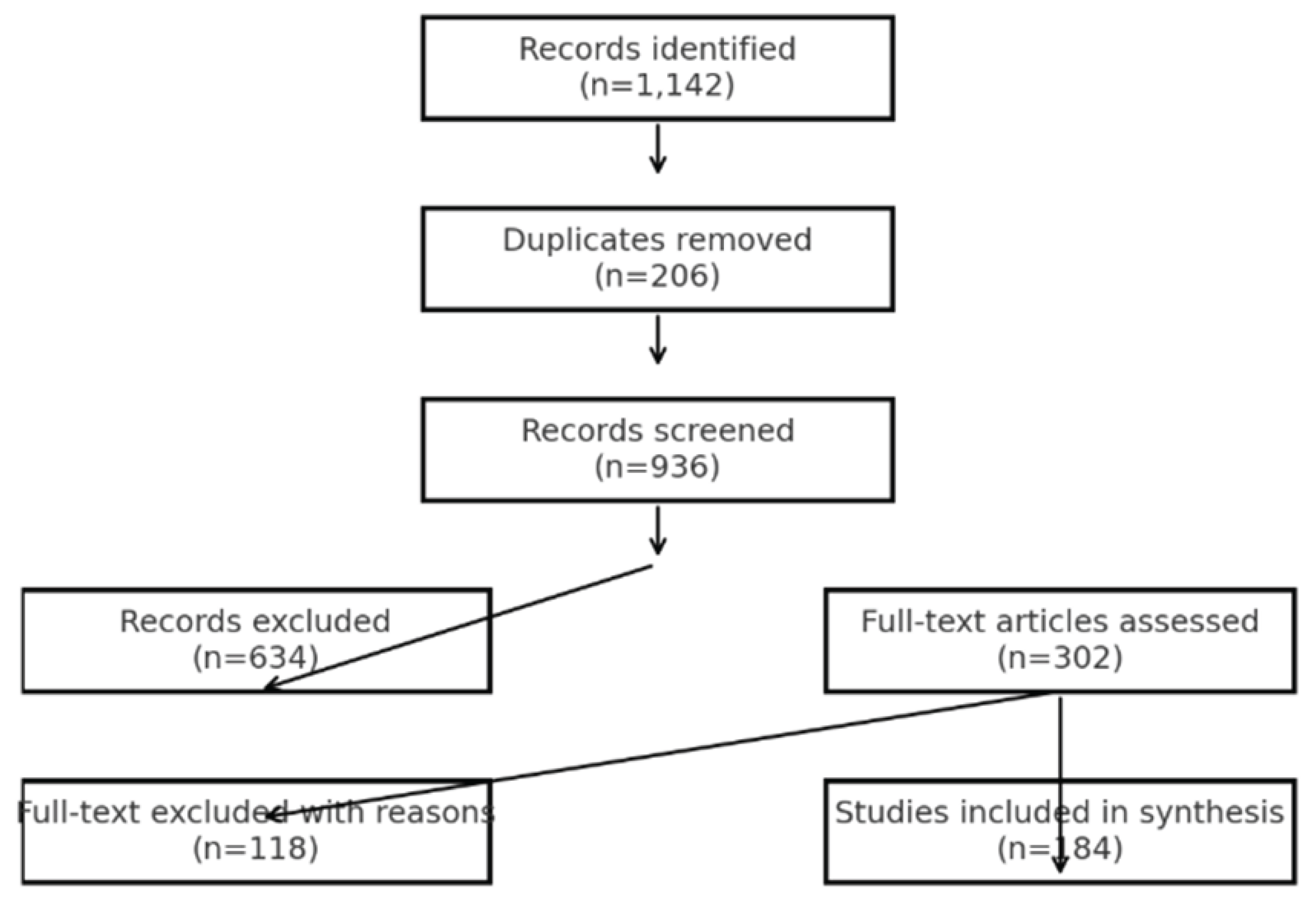
Figure 2.
Terminology frequency.
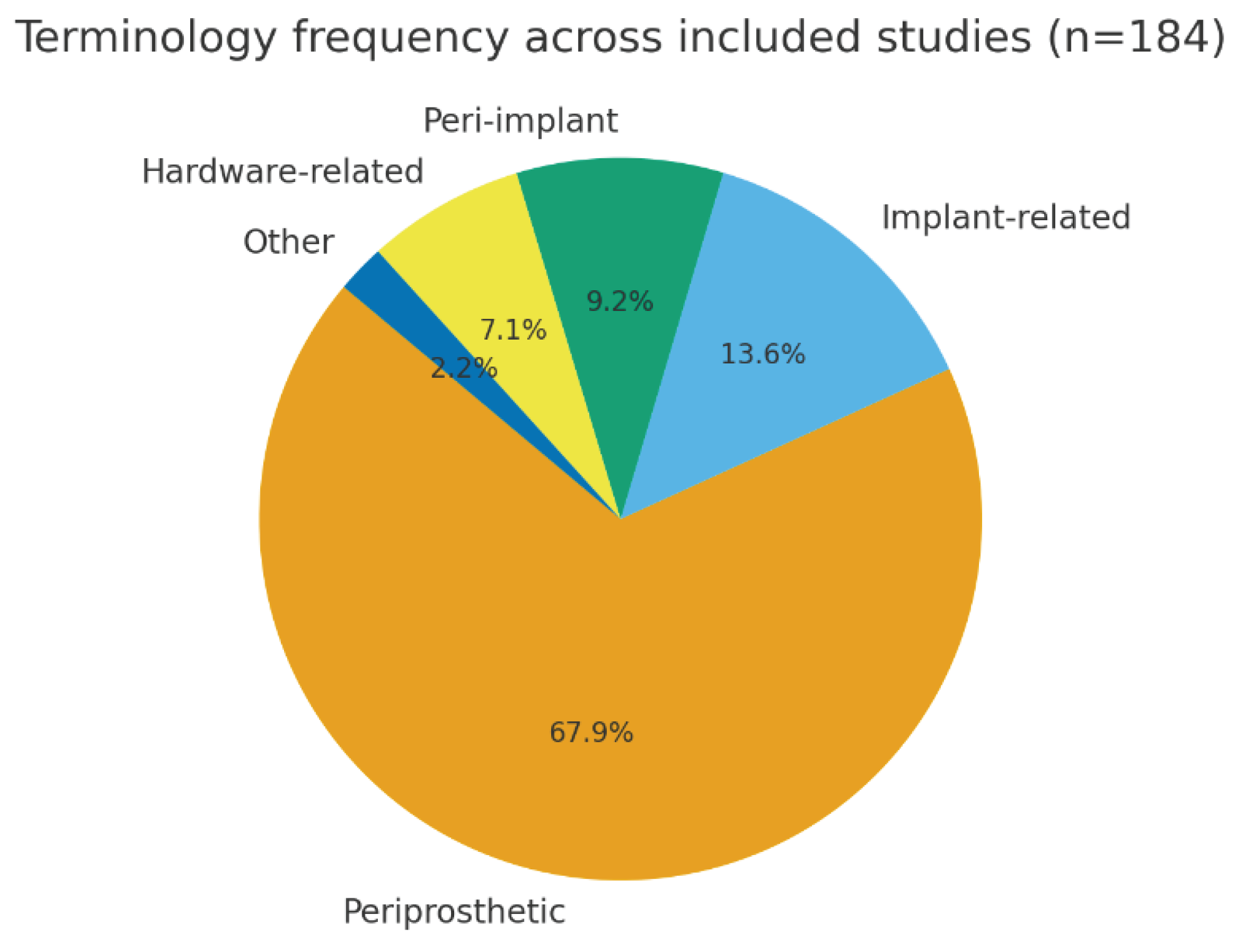
Figure 3.
Terminology by anatomical Site.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



