
Submitted:
28 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Objective: CDK4/6 inhibitors are the standard first-line treatment for hormone receptor (HR)-positive, HER2-negative metastatic breast cancer (MBC). However, treatment response shows heterogeneity among patients. The objective of this multicentre, retrospective study is to investigate real-world parameters affecting overall survival (OS) in patients receiving CDK4/6 inhibitor therapy, particularly the effect of high oestrogen receptor (ER) expression (≥90%). Methods: A total of 603 HR-positive/HER2-negative MMK patients treated with a CDK4/6 inhibitor (ribociclib or palbociclib) from five centres were retrospectively reviewed. Age, menopausal status, metastatic status, metastatic sites, pathological subtype, HER2 status (low/negative), ER expression level (< 90% vs ≥90%), progesterone receptor (PR) status, and prior endocrine therapy (ET) or chemotherapy (CT) before CDK4/6 inhibitor were evaluated for their impact on OS using univariate and multivariate Cox regression analyses. Results: In the univariate analysis, OS was significantly longer in patients who did not receive ET prior to CDK4/6 inhibitor treatment (median OS: 51.0 months vs. 33.3 months; p< 0.01). OS was also better in patients without liver metastases (50.0 months vs. 34.0 months; p=0.019), those with bone metastases only (57.7 months vs. 40.5 months; p=0.022), and PR-positive patients (50.0 months vs. 36.0 months; p=0.037) also had better OS. OS was numerically longer in patients with ER expression ≥90% compared to those with < 90% (49.0 months vs. 41.0 months; p=0.072). In multivariate analysis, not having received ET prior to CDK4/6 inhibitor therapy (p=0.045) and high ER expression (≥90%) (p=0.031) were independently associated with better OS. Conclusion: Our study demonstrates that HR-positive/HER2-negative MBC patients who are naive to endocrine therapy prior to CDK4/6 inhibitor treatment and have high ER expression (≥90%) in their tumours derive greater OS benefit from this treatment. The ER expression level threshold of ≥90% may be proposed as a potential biomarker for predicting response to CDK4/6 inhibitor therapy. These findings necessitate further prospective studies to improve patient selection.
Keywords:
breast cancer
; ER high positivity
; hormonotherapy
; CDK 4/6 Inhibitors
1. Introduction
Breast cancer is the most commonly diagnosed malignancy worldwide and the leading cause of cancer deaths in women globally [1].
Hormone receptor (HR)-positive tumors without HER2 overexpression are the most common form of metastatic breast cancer, and endocrine therapy has long been the primary treatment method for these patients [2]. CDK4/6 inhibitors have been shown to significantly improve outcomes in patients diagnosed with HR-positive, HER2-negative metastatic breast cancer when used in combination with endocrine therapy.[3].
In estrogen receptor (ER)-positive breast cancer, activation of the ER signaling pathway upregulates the ER-cyclin D-CDK4/6pathway. Cyclin-CDKs pathway plays a pivotal role in cell-cycleregulation [4]. When bound and activated by cyclin D, CDK4/6phosphorylates the retinoblastoma protein (Rb), leading to therelease of the transcription factor E2F. This promotes thetranscription of genes related to the cell cycle, driving the transition of cells [5,6,7,8,9]. Therefore, the inhibition of both CDK4/6 and ER have shown clinical efficacy in ER+ advanced breast cancer [10].
Ribociclib, one of the CDK 4/6 inhibitors, demonstrated an OS benefit in patients with metastatic breast cancer who were ER-2 negative and hormone negative when used with AI or AI with an ovary suppressor in the MONALEESA-2 and MONALEESA-7 studies [11].
Palbociclib, another CDK 4/6 inhibitor, demonstrated an OS benefit in these patients in the combined analysis of the PALOMA-1 and PALOMA-2 trials [12,13].
MONARCH 3 trial demonstrated significant improvements in progression-free survival and objective response rate when combining abemaciclib with a nonsteroidal AI as initial therapy for patients with HR-positive, HER2-negative advanced breast cancer [14,15,16].
CDK 4/6 inhibitors are the gold standard first-line treatment for patients diagnosed with metastatic breast cancer who are hormone-positive and do not overexpress HER-2; however, endocrine resistance develops in almost all patients. Furthermore, there are patient groups who do not derive the expected benefit from this gold standard treatment. Therefore, it is important to identify subgroups that will not benefit or will benefit less from CDK 4/6 inhibitors. Studies have been conducted in this regard, such as comparisons of certain subgroups. In our study, we designed this study with the aim of combining many different parameters in the patient group using CDK 4/6 inhibitors to show in which patient group CDK 4/6 inhibitors would be more beneficial and in which groups less benefit would be seen.
2. Method
Our study is a multicentre, retrospective study. Patients who presented to the Medical Oncology outpatient clinics at Selçuk University Faculty of Medicine Hospital, Necmettin Erbakan University Faculty of Medicine, İzmir City Hospital, Ege University Faculty of Medicine Hospital, and Manisa Celal Bayar University Faculty of Medicine between May 2020 and June 2024 were included in the study after reviewing their files.
Inclusion criteria were: 1) Diagnosis of metastatic breast cancer 2) Hormone-positive breast cancer pathology and absence of Her-2 overexpression 3) Documented pathology report (de novo metastatic or early-stage surgical pathology) 4) The patient having used a CDK 4/6 inhibitor at some stage of their breast cancer treatment, 5) Being female (male breast cancer patients were not included in the study)
To investigate the efficacy of CDK 4/6 inhibitors, the overall survival (OS) of patients was calculated and compared. OS was calculated as the time from the start of CDK 4/6 inhibitor treatment to death or the date of the last visit.
In these patients: age (over 65 years, between 65 and 35 years, and under 35 years), Her-2 status, menopausal status (pre/perimenopausal, postmenopausal), metastatic status (de novo or systemic recurrence), metastatic sites (visceral, bone-only, and liver metastasis presence), pathological subtype, use of Ribociclib or Palbociclib among CDK 4/6 inhibitors, prior use of hormone therapy or chemotherapy before CDK 4/6 inhibitor treatment, ER status (below 90% or 90% and above), PR status (negative or positive) were determined to affect survival using univariate analysis. Subsequently, multivariate analysis was performed using data with p<0.1 in the univariate analysis to determine the independent effect of these variables.
Tumour progression was assessed according to RECIST criteria.
Our study was conducted in accordance with the Helsinki Declaration and was reviewed and approved by the Ethics Committee of Selçuk University Faculty of Medicine.
All analyses were performed using the SPSS version 20.0 statistical software package for Windows. We used the chi-square test to analyse differences in clinical characteristics between the two groups. Overall survival was calculated using the log-rank test. We then used the Kaplan-Meier method to plot survival curves and the Cox proportional hazards model to identify statistically significant variables related to overall survival. Differences were considered significant when p < 0.05.
3. Result
A total of 603 patients were included in our study. Patient characteristics are shown in Table 1.
| Characteristic | Patients |
|
HER-2 Status HER-2 Low HER-2 Negative |
297 301 |
|
Median age > 65 years <35 years |
56,5 168 29 |
|
Menopausal status Pre/perimenopausal Postmenopausal |
201 401 |
|
ER status < 90% ≥ 90% Unknown |
259 310 34 |
|
PR status Negative Positive Unknown |
139 430 29 |
|
Pathology Invasive ductal Invasive lobular Other Unknown |
525 51 19 7 |
|
Metastatic status De-novo Recurrent |
308 295 |
|
Metastasis Visceral metastasis Only bone metastasis Liver metastasis Unknown |
316 135 136 16 |
|
CDK 4/6 Inhibitors Ribosiclib Palbosiclib |
422 181 |
|
Tretatment before CDK 4/6 Inhibitors Hormonotherapy before CDK 4/6 Inhibitors Yes No Chemotherapy before CDK 4/6 Inhibitors Yes No |
144 458 181 418 |

Table 2.
The effects of the parameters on survival (univaryant analysis).
| Variables | P |
| Her-2 status Her-2 low Her-2 negative |
0,479 |
| Metastasis Visceral metastasis Only bone metastasis Liver metastasis |
0,025 0,022 0,019 |
| ER status < %90 ≥ %90 |
0,072 |
| PR status Negative Positive |
0,037 |
| Menopausal status Pre/perimenopausal Postmenopausal |
0,775 |
| Pathology Invasive ductal Invasive lobular Other |
0,723 |
| Metastatic status De-novo Recurrent |
0,757 |
| CDK 4/6 Inhibitors Ribosiclib Palbosiclib |
0,267 |
| Treatment before CDK 4/6 Inhibitors Hormonotherapy before CDK 4/6 Inhibitors Chemotheray before CDK 4/6 Inhibitors |
<0,01 0,01 |
| Age < 35 years >65 years |
0,848 0,695 |
Table 3.
The effects parameters on survival were investigated by Cox regression analysis (multivariant analysis).
Table 3.
The effects parameters on survival were investigated by Cox regression analysis (multivariant analysis).
| Variables | P |
| Metastasis Visceral metastasis Only bone metastasis Liver metastasis |
0,237 0,586 0,332 |
| ER status < %90 ≥ %90 |
0,031 |
| PR status Negative Positive |
0,231 |
| Metastatic status De-novo Recurrent |
0,813 |
| CDK 4/6 Inhibitors Ribosiclib Palbosiclib |
0,127 |
| Treatment before CDK 4/6 Inhibitors Hormonotherapy before CDK 4/6 Inhibitors Chemotherapy before CDK 4/6 Inhibitors |
0,045 0,530 |
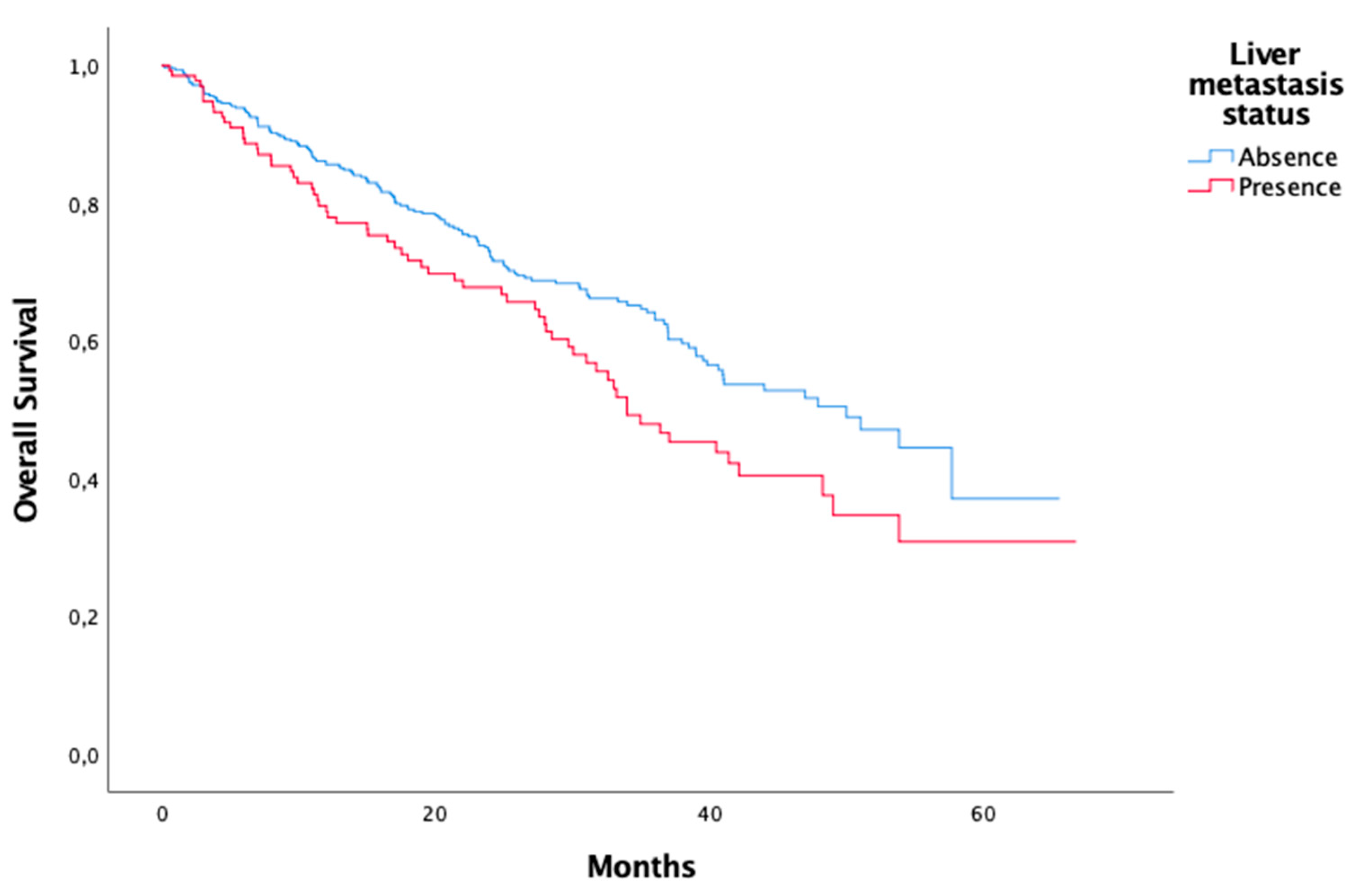
Figure 1.
Liver metastasis status, univaryant analysis.
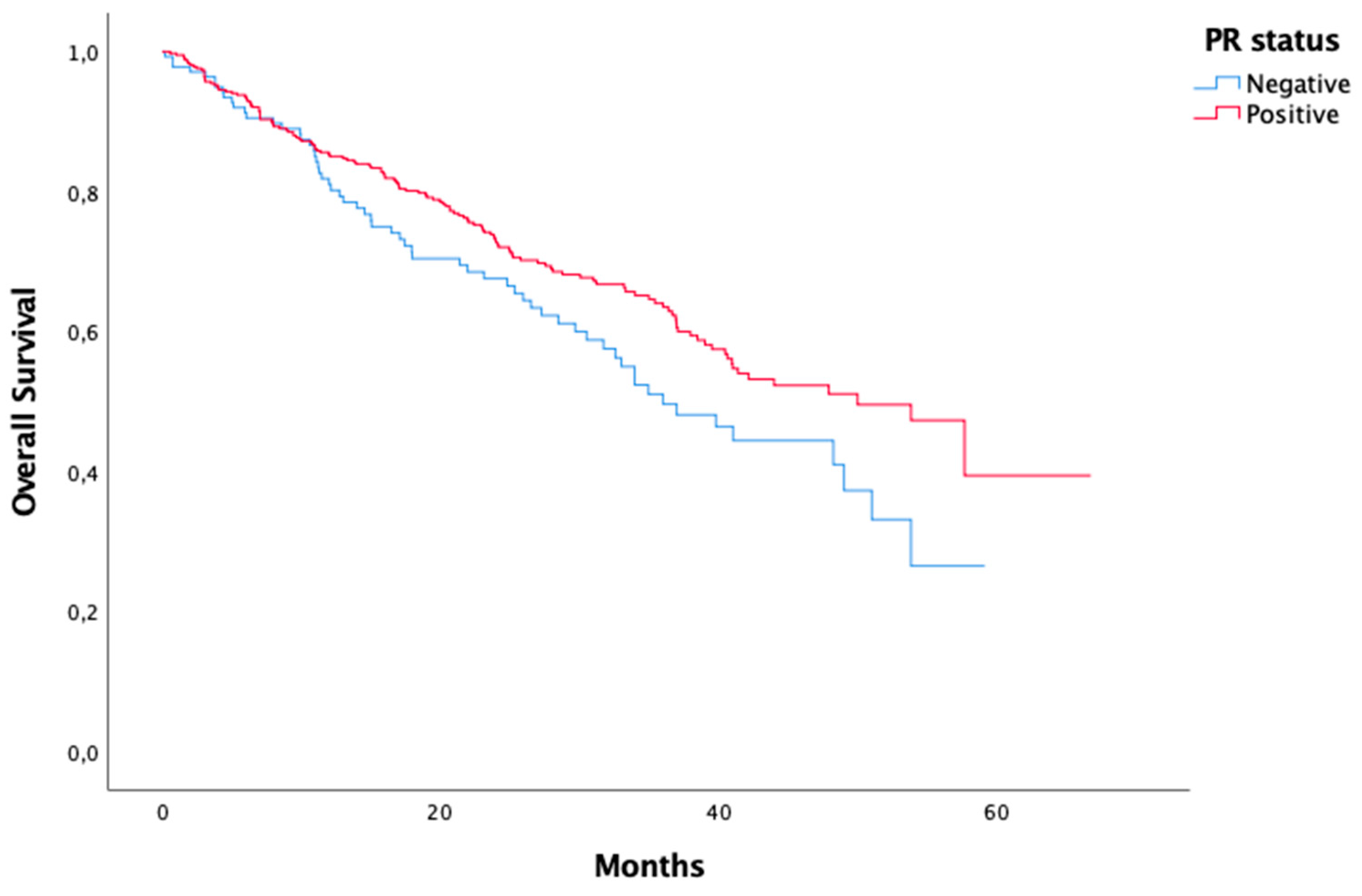
Figure 2.
PR status, univaryant analysis.
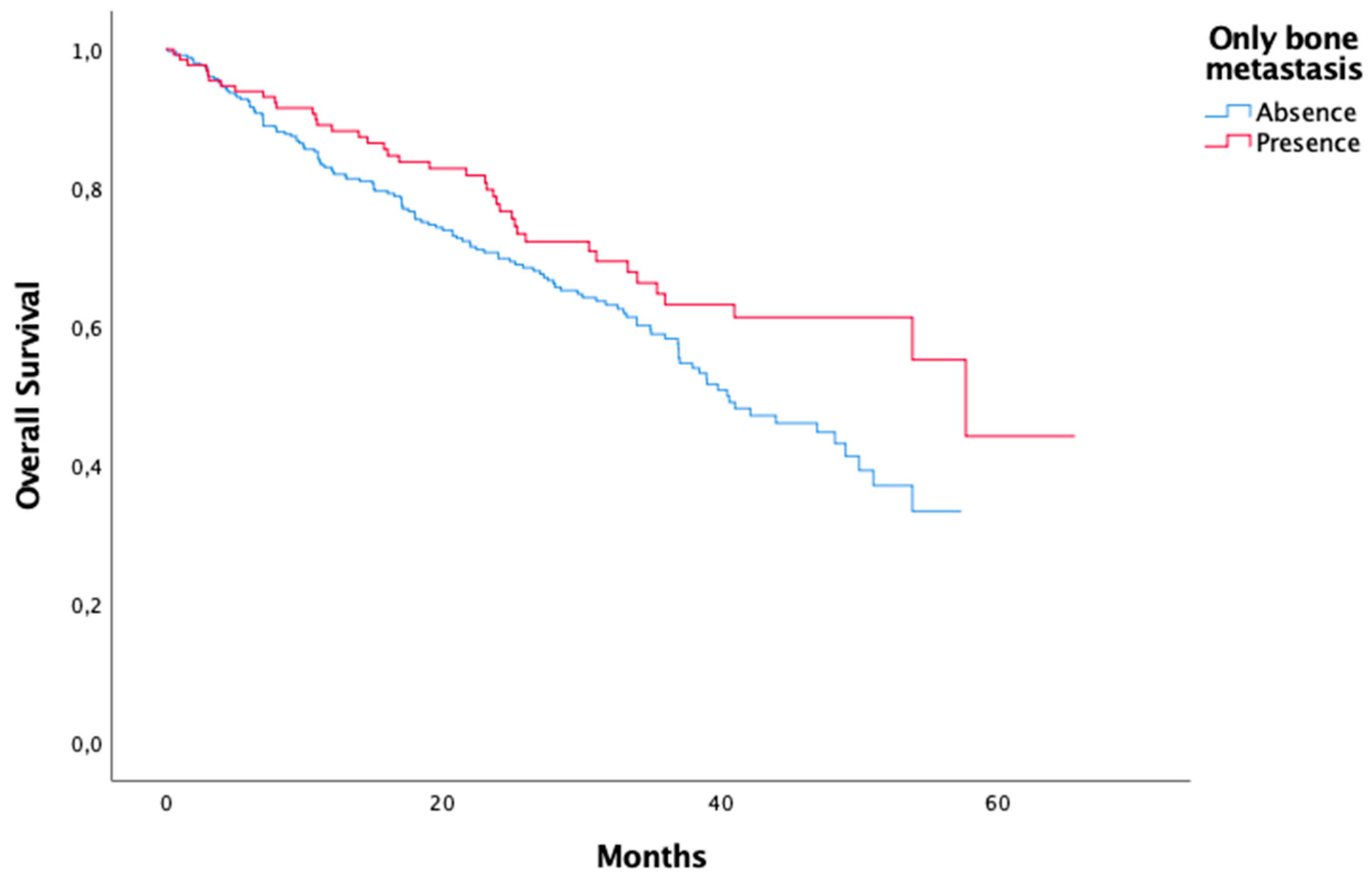
Figure 3.
Only bone metastasis status, univaryant analysis.
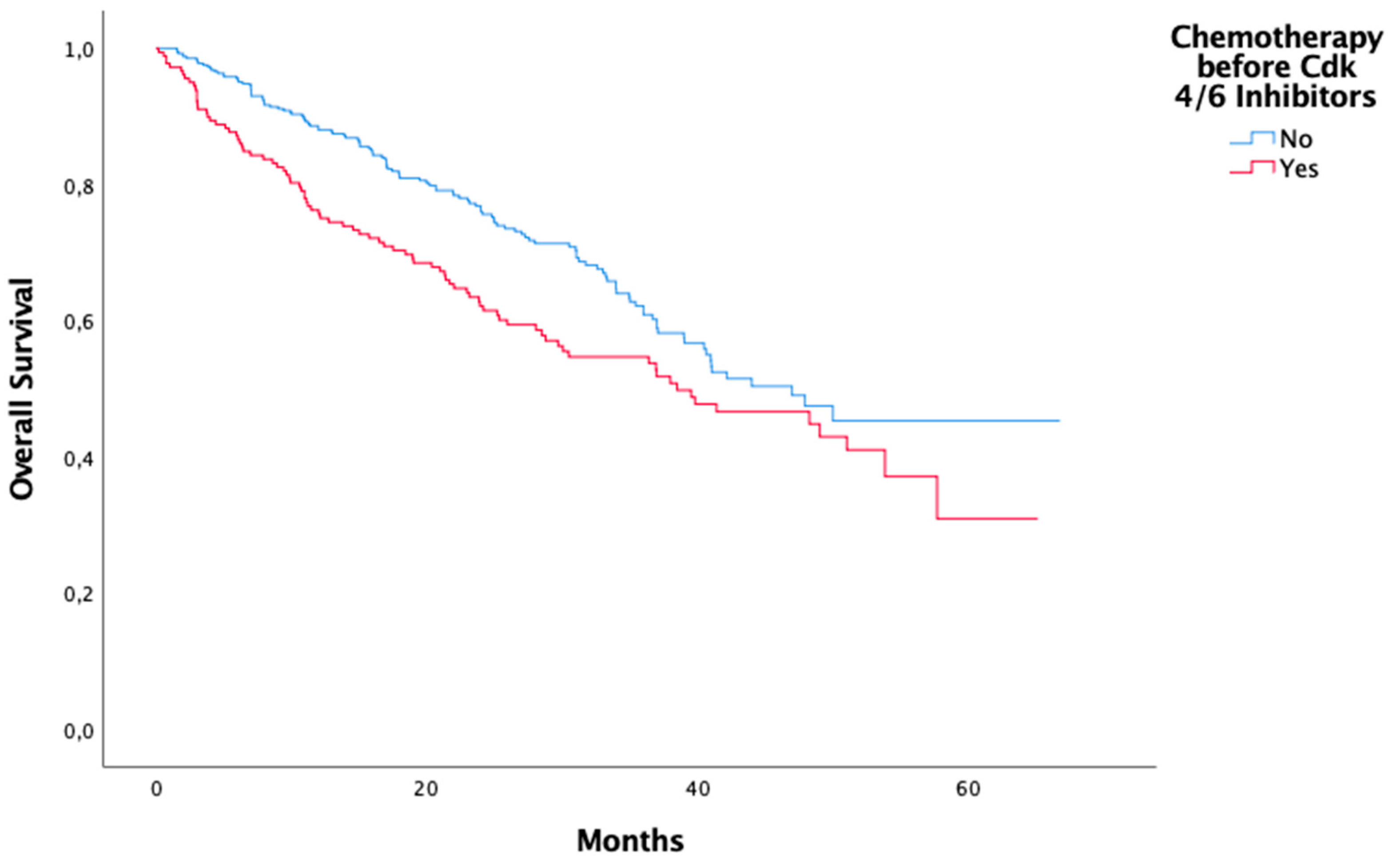
Figure 4.
Chemotherapy before CDK 4/6 Inhibitors, univaryant analysis.
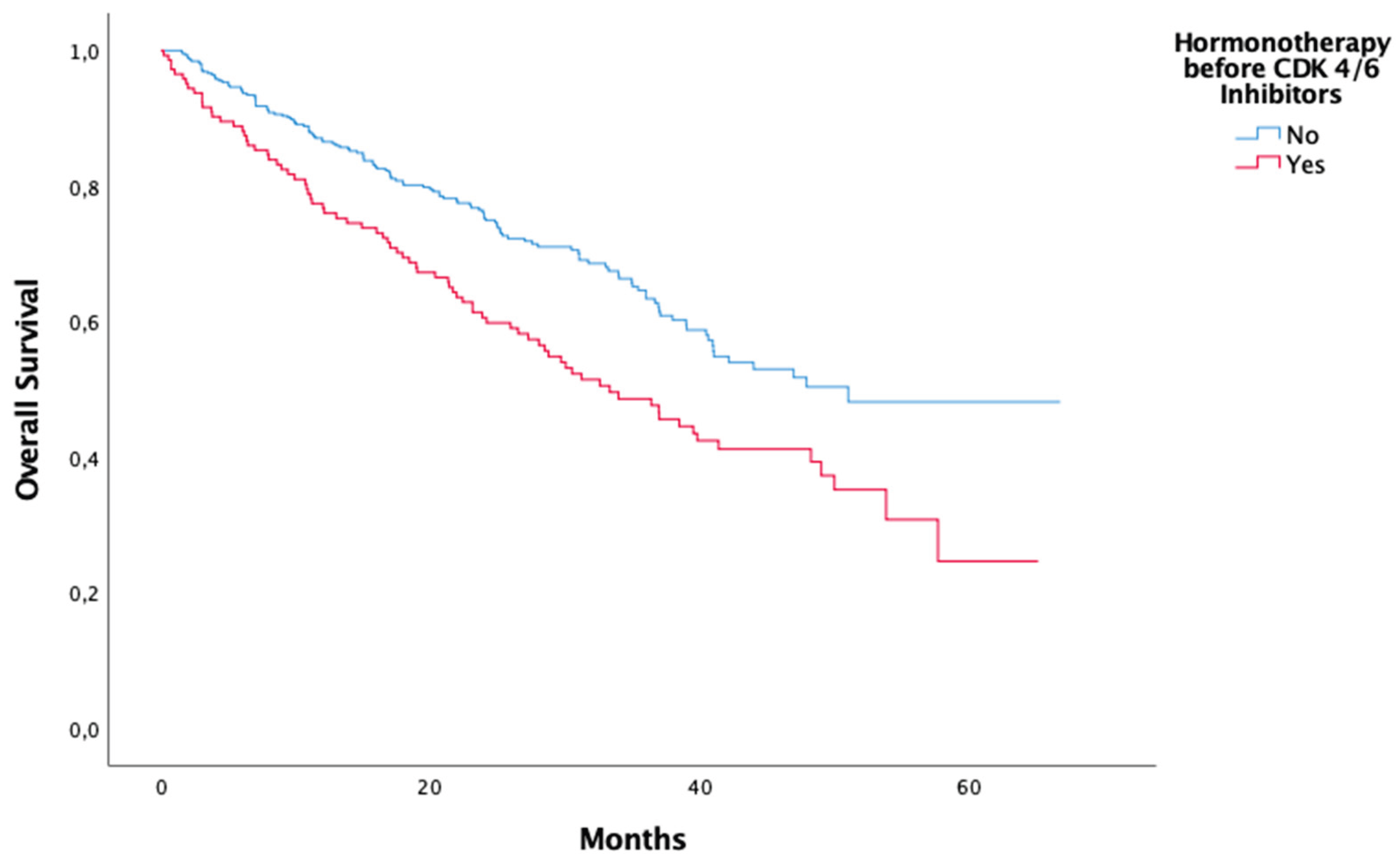
Figure 5.
Hormonotherapy before CDK 4/6 Inhibitor, univaryant analysis.
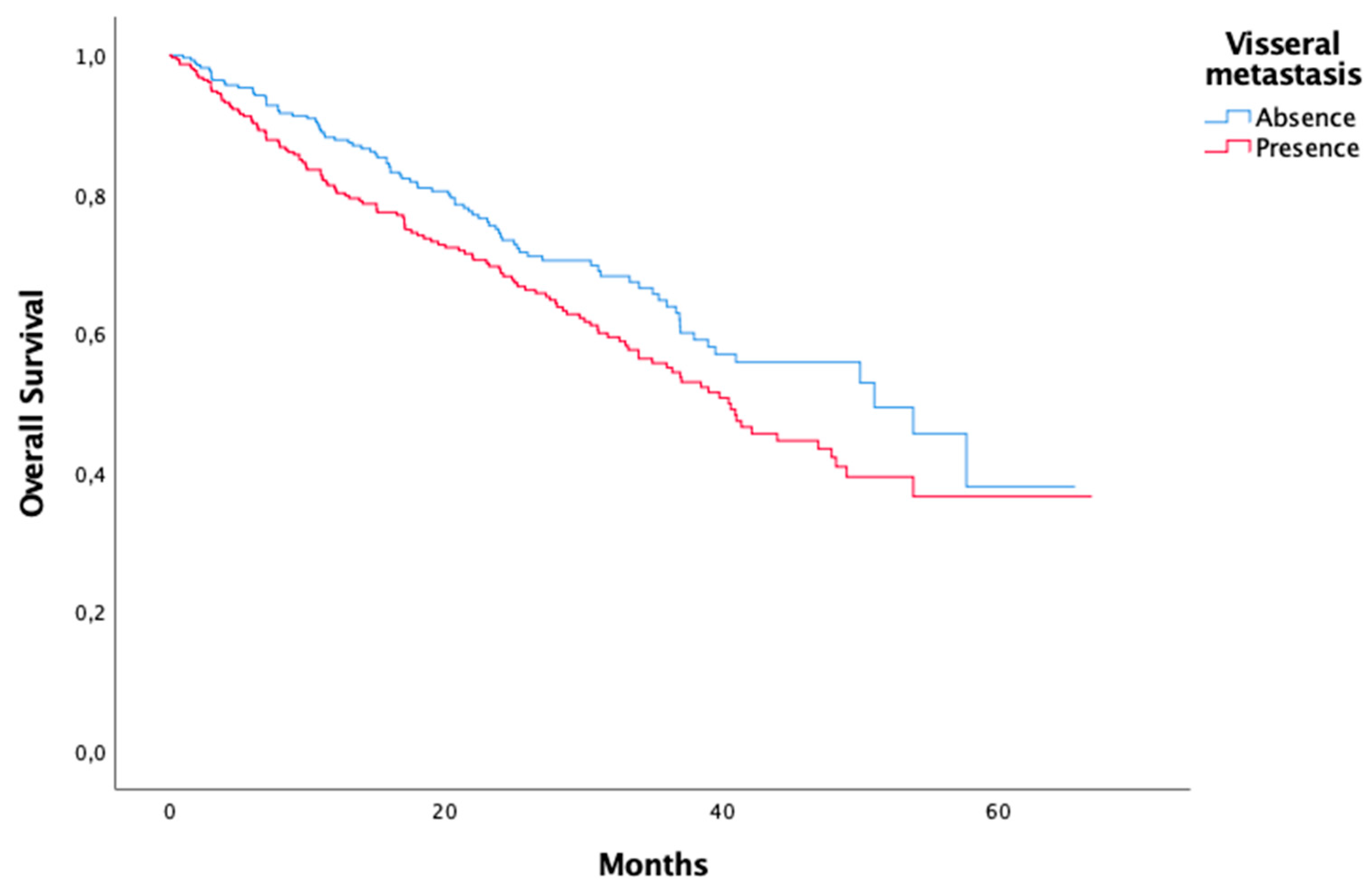
Figure 6.
Visseral metastasis status, univaryant analysis.
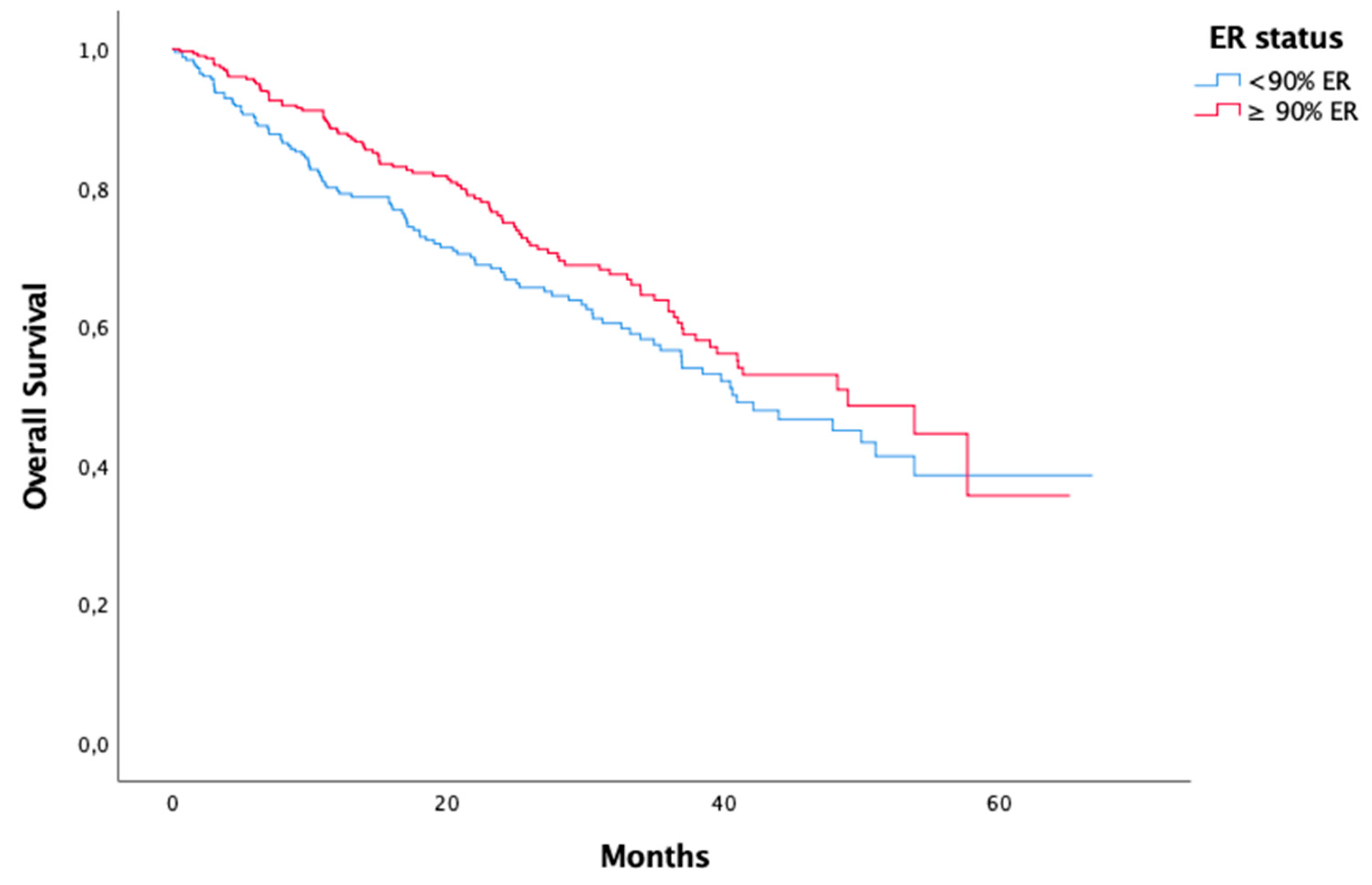
Figure 7.
ER status, univaryant analysis.
Age, pathology (invasive ductal, invasive lobular, and others), menopausal status (pre/perimenopausal, postmenopausal), ER status (below 90%, 90% and above), PR status (negative or positive), metastatic status (systemic recurrence or de novo), metastasis sites (visceral metastasis, presence of liver metastasis, bone metastasis only), which CDK 4/6 inhibitor was used (Palbociclib or Ribociclib), and whether hormone therapy or chemotherapy was used prior to CDK 4/6 inhibitor are presented in Table 2 (univariate analysis).
In the univariate analysis, a statistically significant difference was found between patients who did not receive hormone therapy prior to CDK 4/6 inhibitor use and those who did. The median OS was 51.023 months in patients who did not receive hormone therapy prior to CDK 4/6 inhibitor use and 33.314 months in patients who received hormone therapy prior to CDK 4/6 inhibitor use (p:<0.01).
Similarly, in the univariate analysis, a statistically significant difference was found between patients who did not receive chemotherapy prior to CDK 4/6 inhibitor use and patients who received chemotherapy prior to CDK 4/6 inhibitor use. The median OS was 46.982 months in patients who did not receive chemotherapy prior to CDK 4/6 inhibitor use and 38.472 months in patients who received chemotherapy prior to CDK 4/6 inhibitor use, showing a statistically significant difference (p: 0.01).
In the univariate analysis, the median OS was 33.971 months in the presence of liver metastases and 50.004 months in the absence of liver metastases, and a statistically significant difference was found (p:0.019).
Furthermore, in univariate analysis, the median OS was 50.004 months in PR-positive patients and 36.008 months in PR-negative patients, showing a statistically significant difference (p=0.037).
Among patients with metastatic breast cancer, OS was 57.692 months only in the presence of bone metastases, while the median OS in the group outside this group was 40.476 months (p: 0.022). Furthermore, in the univariate analysis comparing patients without visceral metastases to those with visceral metastases, the median OS was 51.023 months in patients without visceral metastases, while the median OS was 40.476 months in patients with visceral metastases (p=0.025).
In a univariate analysis comparing strong ER positivity with patients whose ER ratio was below 90%, the median OS was 49.018 months in patients with strong ER positivity (ER value ≥90%) and 40.969 months in patients with an ER value below 90% (p=0.072).
Other parameters evaluated in univariate analysis, including which CDK 4/6 inhibitor was used, HER-2 low or negative status, menopausal status, metastatic status, and pathological subtype analysis, did not show statistical significance.
In the multivariate analysis (Table 3), statistically significant results were obtained in patients who did not receive hormone therapy prior to CDK 4/6 inhibitor treatment (p=0.045). Furthermore, a statistically significant difference was observed in cases of strong ER positivity, i.e., ER values of 90% or higher (p: 0.031). In univariate analysis, the absence of liver metastasis showed a statistically significant difference, while in multivariate analysis, although a numerical difference was observed, statistical significance could not be demonstrated.
4. Discussion
In the treatment of metastatic breast cancer, CDK 4/6 inhibitors constitute first-line therapy in cases where there is no hormone positivity or HER-2 overexpression. However, treatment responses to CDK 4/6 inhibitors vary in this heterogeneous patient group. In this study, we designed a study to investigate factors affecting OS in the use of CDK 4/6 inhibitors. ER high positivity (90% and above or below 90%), PR positivity (positive or negative), age, menopausal status, pathological subtype, Her-2 status (negative or low), presence of liver metastases, presence of visceral metastases, presence of bone metastases only, history of hormone therapy or chemotherapy prior to CDK 4/6 inhibitor use, metastatic status at diagnosis (de novo or systemic recurrence), and which CDK 4/6 inhibitor was used (ribociclib or palbociclib).
In breast cancer, ER positivity is an important parameter in evaluating the response to endocrine therapy. A study by Allison et al. [17] suggests that using a 1% threshold for ER may be insufficient and that higher ER expression levels are associated with a better prognosis and possibly a better response to endocrine therapy. In their study [18] on the bioanalysis of the PALOMA-2 and PALOMA-3 trials, Finn et al. performed subgroup analyses [18] and found that the CDK4/6 inhibitor palbociclib was associated with a better response to endocrine therapy in patients with higher ER expression levels. -3 trials [18] demonstrated that the benefit of the CDK4/6 inhibitor palbociclib was more pronounced in tumours with high ER positivity (≥50% by IHC).
MONALEESA-2 trial [11] demonstrated that the superiority of the letrozole + palbociclib combination on PFS (Progression-Free Survival) was observed in all ER-positive/HER2-negative patients, but this benefit was further increased in the group with the highest ER expression level (Allred score 7-8 or 80-100% positivity).
There are no studies on high ER positivity (≥90%). In our study, a significant difference was found in multivariate analyses regarding the use of CDK 4/6 inhibitors in high ER positivity.
The use of CDK 4/6 inhibitors is common in the first line of treatment for patients diagnosed with metastatic breast cancer who are hormone-positive and do not overexpress Her-2, as their contribution to overall survival (OS) and progression-free survival (PFS) is well established. Subgroup analyses are being conducted to determine in which subgroups of these patients the use of CDK 4/6 inhibitors provides greater benefit or in which patient groups early recurrence is observed. In our study, the contribution of CDK 4/6 inhibitors was lower in patients who had received hormone therapy prior to CDK 4/6 inhibitor use, and significant results were obtained in both univariate and multivariate analyses in hormone therapy-naive patients. However, when analysing patients in this group who had received chemotherapy prior to CDK 4/6 inhibitor use, statistically significant results were obtained in univariate analysis, but not in multivariate analysis.
While patients with PR-positive tumours also experience improved outcomes with ET, PR is considered a functional indicator of the ER pathway [19]. It is established that PR status can divide ER-positive tumours into different prognostic categories. Evidence suggests that PR positivity, independent of ER status, predicts ET response, and it is recommended that PR be considered when making ET decisions for patients [20].
In a single-centre study by Öner and colleagues [21] involving 244 patients, it was demonstrated that PR positivity, in addition to ER positivity, contributed significantly to PFS in metastatic breast cancer patients using CDK 4/6 inhibitors. Similarly, in our study, PR-positive patients showed a significant difference in univariate analysis compared to PR-negative patients when using CDK 4/6 inhibitors; however, in multivariate analysis, although a numerical difference was observed, no statistically significant difference was detected.
In a multicentre retrospective study by Toss and colleagues, it was demonstrated that the presence of bone metastases alone in patients diagnosed with metastatic breast cancer who were hormone-positive and HER-2 low or negative contributed significantly to OS compared to the presence of external visceral metastases [22]. Similarly, a study by Niikula et al. obtained similar results [23]. In our study, although it was numerically demonstrated that the presence of bone metastases alone in patients diagnosed with metastatic breast cancer contributed significantly to OS, no statistically significant results were obtained.
Approximately 20% of breast cancer patients will experience relapse, and 50–70% of metastatic breast cancer cases involve the liver [24]. Prognosis is poor following metastasis to the liver, with the median survival rate being only 2–3 years [25]. In our study, the effect of liver metastasis on OS was demonstrated numerically but not statistically
Patients with de novo MBC tend to have a better prognosis compared with those with recurrent MBC [26,27]. Being naïve to treatment, they may respond better to systemic therapy, whereas inherent biological differences could also explain this phenomenon [28,29]. In a multicentre study of 10,655 patients conducted by Barcenas et al. [30], systemic and targeted therapy was shown to contribute to better OS and PFS in patients diagnosed with metastatic breast cancer with de novo disease compared to those with recurrent disease. However, in our study, although OS was numerically better in de novo disease, no statistically significant difference was demonstrated.
HER2-low tumours constitute a heterogeneous population that includes both hormone receptor-positive and hormone receptor-negative breast cancers with varying prognosis and sensitivity to systemic therapies [31]. In a multicentre study of 423 patients with HER2-low and HER2-negative breast cancer conducted by Kahraman and colleagues [32] on the treatment efficacy of CDK 4/6 inhibitors, no difference in OS and PFS was observed between HER2-low and HER2-negative biology with the use of CDK 4/6 inhibitors. A similar study was conducted by Önder and colleagues [33] in a single centre with 258 patients, and similarly, no significant OS difference was demonstrated in HER-2 low and HER-2 negative patients with CDK 4/6 inhibitor use. Similarly, in our study, no difference in OS was demonstrated with the use of CDK 4/6 inhibitors in HER-2 low and HER-2 negative patients.
The use of CDK 4/6 inhibitors is common in patients diagnosed with metastatic breast cancer. In a study by Thrill and colleagues [34] involving 623 patients, which compared OS and PFS with the use of the CDK 4/6 inhibitors ribociclib and palbociclib, no difference in OS and PFS was demonstrated between ribociclib and palbociclib. Similarly, in our study, no statistically significant difference was observed between the use of the two CDK 4/6 inhibitors.
Various studies exist on whether there is a difference in the contribution of CDK 4/6 inhibitor use to OS in premenopausal and postmenopausal patients diagnosed with breast cancer. In a study by Schettini et al. [35], which included a pooled analysis of six studies, no difference in OS was demonstrated between postmenopausal and premenopausal patients. Similarly, in our study, no statistically significant difference in OS was demonstrated between postmenopausal and premenopausal patients using CDK 4/6 inhibitors. The same study also examined the effects of CDK 4/6 inhibitor use on the age factor, and no difference in OS and PFS was demonstrated in the analysis between patients under and over 65 years of age. In the MONALEESA-7 study, a subgroup analysis based on age was performed for ribociclib and endocrine therapy [36], and efficacy was found to be consistent across all age groups (≤25, 25-39, 40-59 years). Similarly, in our study, the age analysis showed no statistically significant difference in OS between patients aged 65 years and older and those aged 35 years and younger.
Although treatment options vary according to pathological subgroups in breast cancer, CDK 4/6 inhibitors are preferred as first-line therapy in metastatic disease in cases of hormone-positive and HER-2 non-overexpression ductal carcinoma, lobular carcinoma, and other subgroups. In a multicentre study of 1,213 patients with metastatic breast cancer diagnosed with ductal carcinoma or lobular carcinoma, Toda and colleagues [37] conducted a multicentre study involving 1,213 patients to investigate the use of CDK 4/6 inhibitors in patients with metastatic breast cancer diagnosed with ductal carcinoma and lobular carcinoma, and to examine the difference in OS and PFS. Similar PFS results were obtained for lobular carcinoma and ductal carcinoma, but OS was found to be lower in patients diagnosed with lobular carcinoma. However, in this study, the mean age of patients diagnosed with lobular carcinoma was higher than that of patients diagnosed with ductal carcinoma. In our study, when comparing CDK 4/6 inhibitor use in ductal carcinoma, lobular carcinoma, and other pathological subgroups, no significant difference was observed in terms of OS.
CDK 4/6 inhibitors are among physicians' first choices as they contribute to meaningful PFS and OS in metastatic breast cancer in the first line of treatment. However, some patient groups experience progression earlier than expected, and although the reason for this is not fully understood, it is thought to be due to factors such as differences in tumour biology, patient clinical status at diagnosis, and areas of metastasis.
With our study, we aimed to highlight the factors affecting OS in the use of CDK inhibitors in a heterogeneous group of breast cancer patients. It was found that not having used hormone therapy prior to CDK inhibitor treatment contributed to OS, and that strong ER positivity similarly contributed to OS.
As a multicentre retrospective study, our work aimed to demonstrate the effect of CDK inhibitors in this heterogeneous patient group and to guide patient selection. Several limiting factors were present in our study; the retrospective nature of the study and the heterogeneity of the patient groups were the most important of these. Further multicentre studies involving more patients are needed in this area.
5. Conclusions
In metastatic breast cancer, CDK 4/6 inhibitors are the gold standard treatment for hormone-positive disease without HER-2 overexpression; however, due to the heterogeneous nature of breast cancer, the benefit of CDK4/6 inhibitors in some subgroups is considerably less than expected. Our study aimed to analyse these subgroups and identify those that would benefit from CDK4/6 inhibitors. Our findings are valuable as this is the first study in the literature to focus on strong ER positivity. We demonstrated the contribution of CDK4/6 inhibitor use to overall survival (OS) in patients with ER 90% and above, and the contribution of CDK4/6 inhibitor use to OS in patients who had not received hormone therapy prior to CDK4/6 inhibitor treatment. Our study is noteworthy as it is the first to investigate the efficacy of CDK4/6 inhibitor use in ER high positivity and has yielded statistically significant results.
Despite various limiting factors, our study is important due to the data obtained being indicative in this regard, as it is a multicentre and comprehensive study on the use of CDK 4/6 inhibitors. Multicentre studies involving larger patient groups are needed.
References
- Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends: an update. Cancer Epidemiol Biomarkers Prev 2016;25(1):16–27.
- Reinert, T., de Paula, B., Shafaee, M. N., Souza, P. H., Ellis, M. J., & Bines, J. (2018). Endocrine therapy for ER-positive/HER2-negative metastatic breast cancer. Chinese Clinical Oncology, 7(3), 25–25. [CrossRef]
- Cardoso F, Costa A, Senkus E, et al. 3rd ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 3). Ann Oncol 2017;28:3111.
- Sherr CJ, Roberts JM. CDK inhibitors: positive and negative regulators of G1-phase progression. Genes Dev. 1999;13:1501–12.
- Bertoli C, Skotheim JM, de Bruin RA. Control of cell cycle transcription during G1and S phases. Nat Rev Mol Cell Biol. 2013;14:518–28.
- Spring LM, Wander SA, Andre F, Moy B, Turner NC, Bardia A. Cyclin-dependentkinase 4 and 6 inhibitors for hormone receptor-positive breast cancer: past,present, and future. Lancet. 2020;395:817–27.
- Ding L, Cao J, Lin W, Chen H, Xiong X, Ao H, et al. The roles of cyclin-dependentkinases in cell-cycle progression and therapeutic strategies in human breastcancer. Int J Mol Sci. 2020;21:1960.
- Roskoski R Jr. Cyclin-dependent protein serine/threonine kinase inhibitors asanticancer drugs. Pharm Res. 2019;139:471–88.
- Pernas S, Tolaney SM, Winer EP, Goel S. CDK4/6 inhibition in breast cancer:current practice and future directions. Ther Adv Me Oncol.2018;10:1758835918786451.
- Alves CL, Ehmsen S, Terp MG, Portman N, Tuttolomondo M, Gammelgaard OL,et al. Co-targeting CDK4/6 and AKT with endocrine therapy prevents progres-sion in CDK4/6 inhibitor and endocrine therapy-resistant breast cancer. NatCommun. 2021;12:5112.
- Im SA, Lu YS, Bardia A, et al. Overall Survival with Ribociclib plus Endocrine Therapy in Breast Cancer. N Engl J Med 2019; 381:307.
- Slamon DJ, Diéras V, Rugo HS, et al. Overall Survival With Palbociclib Plus Letrozole in Advanced Breast Cancer. J Clin Oncol 2024; 42:994.
- Rugo H, et al. Overall survival with first-line palbociclib plus an aromatase inhibitor(AI) vs AI in metastatic breast cancer: A large real-world database analysis. Ann Oncol 2022; 33 (S3): S194-S223.
- Finn RS, Martin M, Rugo HS, et al: Palbociclib and letrozole in advanced breast cancer. N Engl J Med375:1925-1936, 2016.
- Cristofanilli M, Turner NC, Bondarenko I, et al: Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol 17:425-439, 2016.
- Hortobagyi GN, Stemmer SM, Burris HA, et al: Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med 375:1738-1748, 2016.
- llison, K. H., Hammond, M. E. H., Dowsett, M., McKernin, S. E., Carey, L. A., Fitzgibbons, P. L., Hayes, D. F., Lakhani, S. R., Chavez-MacGregor, M., Perlmutter, J., Perou, C. M., Regan, M. M., Rimm, D. L., Symmans, W. F., Torlakovic, E. E., Varella, L., Viale, G., Weisberg, T. F., McShane, L. M., & Wolff, A. C. (2020). Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology, 38(12), 1346–1366. [CrossRef]
- Finn, R., Jiang, Y., Rugo, H., Moulder, S. L., Im, S.-A., Gelmon, K. A., Dieras, V., Martin, M., Joy, A. A., Toi, M., Gauthier, E., Lu, D. R., Bartlett, C. H., & Slamon, D. (2016). late-breaking and deferred publication abstracts LBA15 Biomarker analyses from the phase 3 PALOMA-2 trial of palbociclib (P) with letrozole (L) compared with placebo (PLB) plus L in postmenopausal women with ER + /HER2-advanced breast cancer (ABC). Abstract Book of the 41st ESMO Congress (ESMO 2016), 7-11 October 2016, Copenhagen, Denmark, 27, vi554. [CrossRef]
- Fang H, Huang D, Yang F, Guan X. Potential biomarkers of CDK4/6 inhibitors in hormone receptor-positive advanced breast cancer. Breast Cancer Res Treat. 2018;168(2):287-297. [CrossRef]
- Pandey K, An HJ, Kim SK, et al. Molecular mechanisms of resistance to CDK4/6 inhibitors in breast cancer: a review. Int J Cancer. 2019;145(5): 1179-1188. [CrossRef]
- Öner, İ., İnci, K., Tolunay, K., Karabuğa, B., Türkel, A., Ateş, Ö., & Karaçin, C. (2025). ANATOLIAN CURRENT MEDICAL Predictive value of progesterone receptor in advanced-stage breast cancer patients treated with CDK 4/6 inhibitors. Anatolian Curr Med J, 7(3), 375–383. [CrossRef]
- Toss A, Venturelli M, Sperduti I, et al. First-line treatment for endocrine-sensitive bone-only metastatic breast cancer: systematic review and meta-analysis. Clin Breast Cancer. 2019;19(6):e701-e716.
- Niikura N, Liu J, Hayashi N, et al. Treatment outcome and prognostic factors for patients with bone-only metastasesof breast cancer: a single-institution retrospective analysis.Oncologist. 2011;16(2):155-164.
- Cummings MC et al. (2014) Metastatic progression of breast cancer: insights from 50 years of autopsies. J Pathol 232(1):23–31. 10.1002/path.4288.
- Zhao HY, Gong Y, Ye FG, Ling H, Hu X (2018) Incidence and prognostic factors of patients with synchronous liver metastases upon initial diagnosis of breast cancer: a population-based study. Cancer Manag Res 10:5937–5950. [CrossRef]
- Dawood S, Broglio K, Ensor J, et al: Survival differences among women with de novo stage IV and relapsed breast cancer. Ann Oncol 21:2169-2174, 2010.
- Lobbezoo D, Van Kampen R, Voogd A, et al: Prognosis of metastatic breast cancer: Are there differences between patients with de novo and recurrent metastatic breast cancer? Br J Cancer112:1445, 2015.
- Den Brok WD, Speers CH, Gondara L, et al: Survival with metastatic breast cancer based on initial presentation, de novo versus relapsed. Breast Cancer Res Treat 161:549-556, 2017.
- Yardley DA, Kaufman PA, Brufsky A, et al: Treatment patterns and clinical outcomes for patients with de novo versus recurrent HER2-positive metastatic breast cancer. Breast Cancer Res Treat 145:725-734, 2014.
- Barcenas, C. H., Song, J., Murthy, R. K., Raghavendra, A. S., Li, Y., Hsu, L., Carlson, R. W., Tripathy, D., & Hortobagyi, G. N. (2021). Prognostic Model for De Novo and Recurrent Metastatic Breast Cancer. JCO Clinical Cancer Informatics, 5, 789–804. https://doi.org/10.1200/CCI.21.00020/SUPPL_FILE/DS_CCI.21.00020.PDF.
- Modi, S., Jacot, W., Yamashita, T., Sohn, J., Vidal, M., Tokunaga, E., Tsurutani, J., Ueno, N. T., Prat, A., Chae, Y. S., Lee, K. S., Niikura, N., Park, Y. H., Xu, B., Wang, X., Gil-Gil, M., Li,W., Pierga, J.-Y., Im, S.-A., … Cameron, D. A. (2022). Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. The New England Journal of Medicine, 387(1),9. [CrossRef]
- Kahraman, S., Hızal, M., Gümüşay, Ö., Başaran, G., Seyyar, M., Sahin, E., Çabuk, D., Yaşar, A., Bayoğlu, V., Bayram, E., Paydaş, S., Gülbağcı, B., Hacıbekiroğlu, İ., Demirel, B. Ç., Yaren, A., Özçelik, M., Yılmaz, F., Doğan, M., Paksoy, N., … Şendur, M. A. (2025). HER2-low expression in patients with hormone receptor positive and HER2 negative advanced breast cancer treated with ribociclib or palbociclib in combination with endocrine therapy. Turkish Journal of Clinics and Laboratory. [CrossRef]
- Önder, T., Ateş, Öner, & Karaçin, C. (2024). Relationship between HER2-low status and efficacy of CDK4/6 inhibitors in advanced breast cancer: a real-world study. International Journal of Clinical Oncology, 29(7), 972–984. [CrossRef]
- Thill, M., Zahn, M. O., Welt, A., Nusch, A., Zaiss, M., Engelken, K., Kaltenecker, G., Ringwald, K., Gratzke, K., Dille, S., Kruggel, L., Jänicke, M., Schulz, H., Hagen, V., Fricker, R., Stickeler, E., Harbeck, N., Wöckel, A., & Decker, T. (2025). Head-to-head comparison of palbociclib and ribociclib in first-line treatment of HR-positive/HER2-negative metastatic breast cancer with real-world data from the OPAL registry. International Journal of Cancer, 156(9), 1770–1782. [CrossRef]
- Schettini F, Giudici F, Giuliano M, Cristofanilli M, Arpino G, Del Mastro L, Puglisi F, De Placido S, Paris I, De Placido P, Venturini S, De Laurentis M, Conte P, Juric D, Llombart-Cussac A, Pusztai L, Prat A, Jerusalem G, Di Leo A, Generali D. Overall Survival of CDK4/6-Inhibitor-Based Treatments in Clinically Relevant Subgroups of Metastatic Breast Cancer: Systematic Review and Meta-Analysis. J Natl Cancer Inst. 2020 Nov 1;112(11):1089-1097. [CrossRef] [PubMed] [PubMed Central]
- Tripathy, D., Im, S. A., Colleoni, M., Franke, F., Bardia, A., Harbeck, N., Hurvitz, S. A., Chow, L., Sohn, J., Lee, K. S., Campos-Gomez, S., Villanueva Vazquez, R., Jung, K. H., Babu, K. G., Wheatley-Price, P., de Laurentiis, M., Im, Y. H., Kuemmel, S., El-Saghir, N., … Lu, Y. S. (2018). Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial. The Lancet Oncology, 19(7), 904–915. [CrossRef]
- Toda, E., Hoshino, M., Shimoi, T., Yamanaka, T., Kitadai, R., Saito, A., Kita, S., Kawachi, A., Maejima, A., Kojima, Y., Noguchi, E., Fujiwara, Y., Sudo, K., Koyama, T., & Yonemori, K. (2025). 66P Genetic insights into CDK4/6 inhibitor efficacy in invasive lobular carcinoma and invasive ductal carcinoma. ESMO Open, 10, 104620. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



