Submitted:
26 September 2025
Posted:
30 September 2025
You are already at the latest version
Abstract
Nasotracheal Intubation (NTI) is a common route of airway management in many situations. Over the years, numerous techniques and approaches have been described in performing NTI safely and effectively, including many innovative techniques being published in recent years. However, there hasn’t been a summary of the recent approaches to NTI especially in an easy clinically applicable decision making format. In fact, the last algorithmic approach to nasal intubation in the literature was published by Backman et al. in 2008.
This comprehensive review details an updated analysis of NTI techniques along with a new adapted algorithmic outline to approach NTI in a methodical and stepwise manner (Figure 1). There is also an extensive review of techniques to control epistaxis which is the most commonly encountered complication during NTI.
The newly adapted NTI algorithm simplifies the initial approach to 3 options: Routine Asleep NTI, Awake NTI, and an Initial Orotracheal Intubation (OTI) followed by Conversion to NTI. Older techniques such as blind NTI, flexible intubation scope guided, “look before you leap” approach advocated by Piepho et al., and cuff inflation technique are discussed along with incorporation of newer techniques such as videolaryngoscope guided, hybrid, alignment approach and OTI to NTI conversion.
Uniquely, this manuscript reviews all published techniques for converting OTI to NTI and categorizes them into two pathways (Figure 2): direct conversion (with glottic visualization) or indirect conversion (without glottic visualization). Furthermore, original animated videos have been created and attached to help elucidate these conversion techniques visually.
Keywords:
nasotracheal intubation
; controlling epistaxis
; orotracheal to nasotracheal intubation conversion
1. Introduction
Nasotracheal Intubation (NTI) is a common route of airway management in numerous situations either to facilitate oral and maxillofacial surgery or in a difficult airway scenario.[1,2,3,4] Piepho et al. in 2005 developed a foundational algorithm for approaching NTI. He advocated for a “look before you leap” approach with direct laryngoscopy to assess the potential for a difficult intubation prior to passing the nasal endotracheal tube (NETT) through the nose.[5] Then in 2008 Backman et al. further adapted the NTI algorithm to include oral intubation as a consideration when an unanticipated grade 3 or 4 difficult Cormack-Lehane view was obtained during laryngoscopy. He also listed several techniques to subsequently convert an orotracheal intubation (OTI) over to a NTI including a novel approach using an Eschmann bougie.[6]
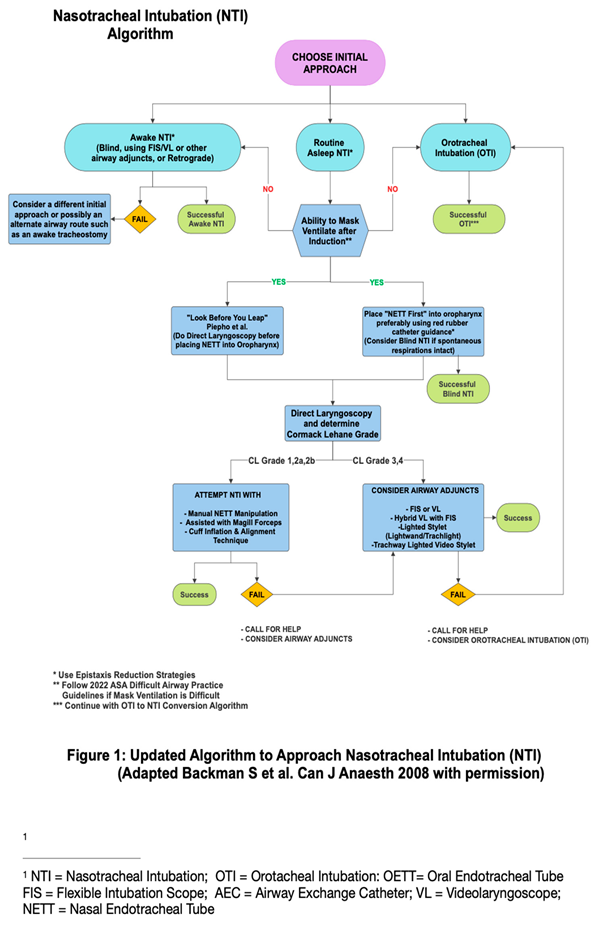
Since the last format of the NTI algorithm in 2008, more airway techniques, advanced airway equipment and more OTI to NTI conversion techniques have emerged prompting an update of the Piepho et al.and Backman et al. NTI algorithm. This clinical review details an analysis of NTI techniques old and new along with an updated clinical decision algorithm to approach NTI in a methodical and stepwise manner (Figure 1). The NTI algorithm has been updated to incorporate both resource poor locations around the world without access to modern devices such as a flexible intubation scope (FIS) or a videolaryngoscope (VL) along with more resource rich locations.
2. Choosing an Initial Nti Approach
One of the main adaptations of the updated NTI algorithm from the prior algorithms is first deciding on the initial approach. The most traditionally used is the “routine NTI”(RNTI) asleep approach with induction followed by mask ventilation and direct laryngoscopy (DL) often utilizing Magill forceps.[7] V (Video 1) https://m.youtube.com/watch?v=RxWc8JK0_iE A 2nd NTI approach available for a cooperative patient is an awake NTI with conscious sedation while maintaining spontaneous respiratory effort and intact airway reflexes.[8] Awake NTI is probably a safer approach when difficult ventilation or intubation is anticipated pre-induction and when mouth opening is mechanically limited such as in patients with temporomandibular joint ankylosis.[9] A 3rd NTI approach that can be considered INITIALLY in the algorithm (versus when a difficult intubation is encountered as Backman et al. suggested) is an orotracheal intubation (OTI) and a subsequent conversion to NTI. Since securing the airway orally is typically easier and quicker than a NTI, especially with utilization of new devices such as VL, this approach may be popular when a difficult RNTI is anticipated or there is desire to minimize mask ventilation during NTI. In addition, an initial asleep OTI is more comfortable for patients compared to an awake intubation, suitable for uncooperative patients and can give the clinician additional time to employ further nasal epistaxis reduction measures if desired.
2.1. Routine Asleep Nti (Rnti) Approach
One of the critical steps in the RNTI approach is the ability to adequately mask ventilate the patient after induction. Difficult and/or inadequate mask ventilation despite optimization maneuvers is probably best managed by quickly attempting an OTI, placing a supraglottic airway (SGA) or waking the patient up and attempting an awake NTI. The ASA 2022 Difficult Airway Practice Guidelines will assist the clinician to manage the patient safely until adequate ventilation and oxygenation is achieved.[10]
But if mask ventilation is adequate as it typically is, then the anesthesia clinician can consider 2 options:
- 1)“Look before you leap” option advocated by Piepho et al. which involves obtaining a glottic view with DL before placing the NETT into the oropharynx. Piepho et al. recommends passing the NETT through the nares only in patients with a grade 1 or 2 Cormack-Lehane (CL) view and using alternate adjunct guided techniques otherwise.[5] Lesser experienced clinicians may find this approach more reassuring.
- 2) More traditional option of placing the NETT into the oropharynx first (“NETT first”) before obtaining a glottic view with DL. The downside to this approach is the clinician may encounter a difficult 3/4 CL grade during subsequent DL, making it challenging to advance the NETT situated in the oropharynx through the glottis. Albeit rare, there is also potential for severe epistaxis with initial NETT insertion which may lead to aspiration of blood and render alternative options such as FIS assisted NTI difficult.[11] Telescoping the NETT with a red rubber catheter, amongst other epistaxis reduction measures, is strongly encouraged to reduce the possibility of severe epistaxis.[12]
2.1.1. RNTI Scenario with CL grade 1/2 view:
Often in this scenario with a complete or partial view of the glottis, the clinician will not have difficulty placing the NETT into the trachea either with manual manipulation or assisted with Magill forceps. Caution has to be used when using Magill forceps to avoid accidental injury to the delicate pharyngeal tissues, uvula and/or prevent damage to the NETT cuff which may lead to a cuff leak requiring NTI replacement.[13]
A commonly used technique to supplement manual manipulation and potentially avoid the use of Magill forceps is the cuff inflation technique, wherein the cuff of the NETT is inflated with ~10-20 mL of air to raise its tip until it’s aligned with the glottis, then the NETT tip is moved forward to partially enter the glottis followed by deflation of the cuff so that the NETT can be advanced further into the trachea to complete the NTI.[14] The cuff inflation technique technique is especially useful when thermosoftened NETTs are utilized which causes loss of the anterior curvature of the NETTs directing them posteriorly towards the esophagus.[15] A modification of the cuff inflation technique is the alignment approach , where in addition to cuff inflation, purposeful limitation of the glottic view to a CL grade 2 during laryngoscopy is undertaken to reduce chances of the abutment of the NETT on the anterior tracheal wall.[16]
90 degree counterclockwise rotation and Seldinger techniques using a bougie can be helpful to facilitate NETT advancement past the glottis if the NETT gets caught up on laryngeal structures or if resistance is encountered due to abutment against the tracheal wall.[17,18] In addition, the Chula formula [9 + (body height/10) cm] can help estimate the proper length for securing the NETT in the trachea at the right external naris.[19]
2.1.2. RNTI Scenario with CL grade 3/4 view:
When confronted with a difficult CL grade 3/4 view during RNTI, a clinician can quickly try simple maneuvers to improve the glottic view such as changing the DL blade, optimizing patient position and external manipulation of the larynx. Also if the patient desaturates while the NETT is already in the oropharynx, it can be used to ventilate and oxygenate the patient while closing the mouth and opposite nare similar to ventilating through a nasal airway.[20]
If simple maneuvers don’t improve the DL glottic view to CL 1/2, then adjunct devices will likely be needed to assist with the NTI. The most commonly used adjunct devices during a RNTI scenario with CL 3/4 view are probably a VL or FIS, which are especially useful when patients also have limited mouth opening making DL and RNTI difficult. When FIS is employed for NTI, the use of a “NETT first” option is recommended for a higher success with minimal attempts.[21,22] Furthermore, pre insertion of the NETT to a depth of 14 cm prior to insertion of the FIS, typically results in excellent visualization of the glottis to intubate the trachea easily and quickly.[23]
Many VLs have been used successfully to achieve NTI including non-channeled VLs such as Glidescope, CMAC and McGrath or channeled VLs such as Airtraq and Pentax Airway Scope.[24] VLs have been shown to provide better view of the laryngeal structures facilitating the ease and speed of NTI.[25,26,27] In fact, many clinicians in resource rich areas opt to use VL from the start to secure NTI rather than DL. When attempting NTI with a VL, use of SUZY/curved vascular forceps may be more effective (rather than Magill forceps) due to the increased curvature that better suits the hyperacute angle of VL blades and maintaining a neutral head position has also been found to be superior to the sniffing position.[28,29] In addition, cuff inflation and alignment techniques can also be employed together with VLs to help secure NTI.
Several case reports describe successful utilization of both FIS and VL during NTI (hybrid technique).[30,31,32] This hybrid technique is especially helpful following failed intubation attempts with FIS or VL alone. A variety of devices other than VLs and FIS have also been used to facilitate NTI when confronted with a difficult CL grade view 3/4. Among these, lighted stylet devices utilizing the transillumination technique such as the lightwand (Trachlight) and intubating lighted video stylets such as Trachway and Disposcope endoscope are prominent.[33,34,35]
2.2. Awake Nti Approach
When faced with a patient that may be potentially difficult to ventilate and/or intubate, clinicians may opt to perform an awake NTI if patient is cooperative. One of the old techniques that’s available to clinicians is to place a nasotracheal tube blindly (BNTI). Fritz Kuhn had used BNTI as early as 1902. BNTI can be done either in an awake cooperative patient with judicious sedation and airway topicalization or attempted asleep in a child or uncooperative patient while maintaining spontaneous respiration. Patient is usually positioned with neck flexed and head extended at the atlantoaxial joint (“sniffing position”) and the ETT is directed posteriorly along the nasal floor into the hypopharynx and advanced gently towards the glottis taking care to stay in the midline. Listening to air flow with breaths helps to advance the NETT. Once at the laryngeal inlet, the tube is advanced into the trachea as patient is asked to take a deep inspiration to abduct the vocal cords.[36,37] (Video 2) https://emedicine.medscape.com/article/1663655-technique?form=fpf#showall Over time, investigators have modified the original BNTI that “went by the ear” to make it “less blind” by adding features such as Beck Airway Airflow Monitor (BAAM) whistle, directional tip Endotrol tubes (Mallinckrodt, Hazelwood, MO), cuff inflation, lighted stylets, video stylets, and ETCO2 monitoring.[38,39,40]
The more popular approach for awake NTI is to use a FIS to guide the NETT into the trachea.[41] Adequate topical or regional anesthesia of the airway generally determines the ease and comfort of awake fiberoptic intubation.[42] Directional tip tubes such as EndoFlex tube can assist FIS to guide it towards the glottis and 90 degree anticlockwise pre-rotation of a standard nasal RAE tubes can help with a higher initial rate of successful railroading.[43,44,45] Judicious conscious sedation is also essential to reduce patient anxiety, enhance cooperativeness and decrease hemodynamic disturbances. Benzodiazepines, propofol, opioids, alpha2-adrenergic agonists such as dexmedetomodine, and ketamine are the main classes of drugs that have been described to facilitate awake NTI.[46]
Just as in the RNTI approach, other devices such as VLs & lighted video stylets and techniques such as cuff inflation and hybrid VL & FIS can also be used to assist awake NTI approach.[47,48] These devices and techniques are particularly handy for awake NTI when secretions and epistaxis make glottic visualization with a FIS indiscernible or when there is difficulty advancing a NETT over the FIS.
Another awake NTI approach available for difficult airways and/or maxillofacial trauma is retrograde nasal intubation technique. It involves the insertion of a guide wire through the cricothyroid membrane, which is then passed upward through the pharynx and delivered out of a nostril in a retrograde manner. A guiding Cook catheter followed by a NETT is then advanced into the trachea using the wire as a guide.[49,50]
2.3. Initial Orotracheal Intubation (Oti) Approach
An initial OTI has several situational advantages: 1) By securing ventilation and oxygenation, it can abate the need for intermittent mask ventilation which may occasionally be difficult during the RNTI approach or preferentially avoided with complicated mandibular fractures. 2) Since OTI can be accomplished quicker and easier than a NTI, this approach is especially useful in high aspiration risk situations by giving clinicians chance to protect the airway and decompress the stomach with a nasogastric tube (NGT) before conversion to NTI is attempted. 3) The initial OTI approach and conversion to NTI is also a favorable option when the patient arrives to the operating room already orally intubated from the field, emergency room or ICU. 4) Securing the airway orally allows ample time to employ additional epistaxis reduction measures (if desired) prior to placement of the NETT into the nasopharynx and protects the airway from aspiration of heme if severe epistaxis occurs. OTI can also be used as a backup option when difficulty is encountered during RNTI as noted by Backman et al.
3. Orotracheal Intubation (Oti) to Nasotracheal Intubation (Nti) Conversion:
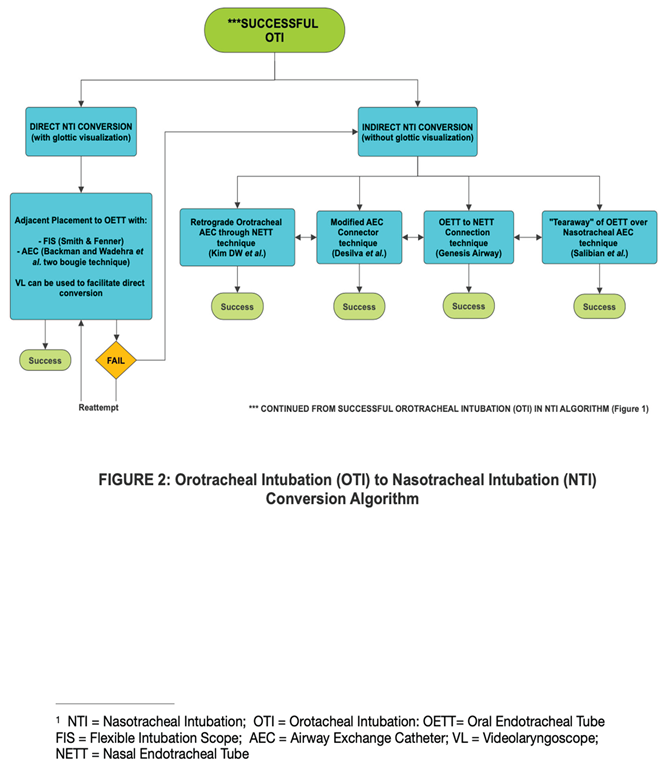
Successful conversion from OTI to NTI can be accomplished through a variety of techniques, offering the clinician with options suited to their preference and available equipment (Figure 2).
Once OTI is secured and confirmed, the clinician may proceed by two primary pathways:
3.1. Direct OTI to NTI Conversion with Glottic Visualization:
A major benefit of direct OTI to NTI conversion techniques is the continuation of ventilation and oxygenation up until the final step of advancing the NETT over a FIS or Airway Exchange Catheter (AEC). Such a reduction in apnea time is a very appealing feature especially for less experienced clinicians.
The Smith & Fenner FIS Guided direct conversion technique advances a FIS (loaded with a NETT) through the nasal passage and oropharynx, then guiding it through the vocal cords adjacent to the existing OETT. With slight deflation of the OETT cuff, the FIS is advanced into the trachea until carina is visualized, The OETT is then removed (either completely or over an AEC) and the NETT is advanced over the FIS into the trachea.[51] (Video 3) https://m.youtube.com/watch?v=z1hhHxMaAD0
The Backman & Wadhera “Two Bougie” direct conversion technique leverages two bougies (AECs) for continuous airway security. Initially, one bougie (AEC) is inserted nasally and guided into the trachea alongside the OETT under DL glottic visualization. The OETT is then removed over another bougie (AEC) leaving two bougies (AECs) in the airway transiently. The NETT is then threaded over the nasal bougie and ETCO2 confirmed to complete the NTI. The oral bougie (AEC) is subsequently removed but offers a guide to reinsert the OETT in case any unanticipated difficulties arise during advancement of the NETT into the trachea.[52,53] (Video 4) https://m.youtube.com/watch?v=9KgkQ7R9BB4
Challenges to direct conversion techniques may occur due to blood and secretions in the airway obscuring the FIS view or from a poor CL glottic view during DL. However, it can often be circumvented by using a VL to obtain a better view of the glottis during the OETT to NETT exchange.[54,55] Another consideration to improve the glottic view during these direct OTI to NTI conversion techniques is the posterior displacement of the OETT manually.[56]
3.2. Indirect OTI to NTI Conversion without Glottic Visualization
Indirect nasotracheal conversion, which avoids direct visualization of the glottis during the OTI to NTI conversion, offer flexibility when equipment inaccessibilty or challenging direct conversion attempts are encountered. Five innovative indirect OTI to NTI conversion techniques have been described in the literature:
The Retrograde AEC indirect conversion technique described by Kim DW et al. begins with an initial OTI after which a NETT together with an AEC is inserted into the oropharynx through a naris. The AEC and NETT is then retrieved outside the mouth from the oropharynx with Magill forceps. With the tip of the NETT now outside the mouth, the AEC is fully withdrawn from the NETT. The AEC is reinserted through the OETT and the OETT is extubated leaving the AEC in the trachea. The proximal end of the oral AEC is then inserted retrograde through the tip of the NETT, which was pulled out of the mouth earlier. Finally the NETT is railroaded or tracked over the nasotracheal AEC into the trachea, securing the NTI conversion.[57] (Video 5) https://m.youtube.com/watch?v=fz3REayMf8M
The Modified Connector indirect conversion technique by Desilva et al. is an innovative technique that revitalizes the original connector technique by Nakata & Nimii utilizing a Patil Connector.[58] After initial OTI, an 18 Fr NGT is inserted nasally and retrieved out of the mouth manually or using Magill forceps. Following a cut and slit modification of the NGT’s distal end, a 14 Fr AEC is advanced through the OETT and the OETT is extubated leaving the 14 Fr AEC in the trachea. The proximal end of the AEC is seated into the slit distal end of the NGT outside of the mouth and two silk sutures are placed through the walls of both the NGT and AEC to secure the connection. The NGT-AEC connection is then withdrawn nasally (being cautious not to extubate the distal end of the 14 Fr AEC from the trachea) establishing a nasotracheal AEC conduit to guide advancement of a NETT into the trachea.[59] (Video 6) https://m.youtube.com/watch?v=on9TgMstpsk
The Tear-Away indirect conversion technique by Salibian et al. involves initial OTI followed by insertion of a pediatric Cook AEC nasally until visualized in the oropharynx and retrieving the distal end of the AEC out of the mouth. After the OETT connector is removed, the AEC is inserted through the OETT into the trachea. The OETT without the connector is then cut longitudinally with a 10 blade in a “tear-away” fashion as it is withdrawn out over the AEC. This preserves the nasotracheal AEC conduit in place to advance a NETT into the trachea to complete the NTI conversion.[60] (Video 7) https://m.youtube.com/watch?v=_amqGHno5GI
The Genesis Interchangeable Oral-Nasal ETT Connection indirect conversion technique offers a reintubation-free transition unlike the other three indirect conversion options described above. The Genesis Airway ETT(Genesis Airway, Sunshine Coast, Australia) employs a reinforced endotracheal tube (RET) with a centered, posterior facing bevel and a curved tip similar to the Parker Flex-Tip tube (Parker Medical, Highlands Ranch, CO, USA).[61] The Parker Flex-Tip tube has been shown to reduce trauma and hang up during NETT insertion and advancement compared to a standard ETT.[62,63]
Starting with an OTI using the distal RET part of the the Genesis ONETT Airway, the proximal flexible part of the Genesis ONETT Airway, connected to a soft curved obturating introducer, is then inserted nasally into the oropharynx and pulled out of the mouth with Magill forceps. The ends of the flexible proximal part (after removal of the introducer) and distal RET part (after removal of the ETT connector) of the Genesis ONETT Airway have been manufactured to easily connect together firmly allowing for a continuous NETT. The NETT can then be slowly withdrawn out nasally until the proximal flexible part can be disconnected leaving behind the proximal end of the distal RET outside the nose securing the NTI conversion.[64] (Video 8) https://m.youtube.com/watch?v=LZ7XWWKS8yU
The downside of the Genesis technique is the rare availability of the Genesis Interchangeable Oral Nasal intubation kit in the operating room and also the fact that the pilot cuff of the NETT is left out of the mouth (as opposed to out of the nose away from the surgical field with the other indirect conversion techniques). The surgery team will have to either sink the pilot cuff in the oropharynx or maneuver the pilot cuff around as needed during surgery to avoid cuff damage.
Retrograde oral to nasal indirect conversion techniques have also been published in literature but predominantly in pediatric patients.[65,66] The smaller sizes of ETT employed in pediatric patients makes retrograding feasible through the narrow rigid nasal airway opening at the choanae. This approach is not so favorable in adults due to potential trauma to nasopharyngeal structures such as the Eustachian tube orifice from retrograding larger sized ETT’s.
An important caution to mention when using AECs in these conversion methods is to avoid inserting the AEC too far past the carina and potentially causing bronchial trauma. This can be avoided by paying attention to the markings on the AEC and making sure the AEC does not go in past the 20-25cm marking beyond the incisors of the mouth or past the 27-30cm marking at the nares depending on the height of the adult patient.[67]
4. Controlling Epistaxis
Epistaxis is a common complication during NTI due to the rich vascularity and friability of the nasal mucosa. Minimizing epistaxis improves visualization and enhances safety by allowing for more options to secure NTI and reduce possible aspiration of blood. Although severity of epistaxis during NTI is usually mild and transient, at times it can be severe.[68,69] So it is paramount that clinicians consider interventions to reduce this complication when NTI is attempted.
Foremost, it’s essential to recognize risk factors for severe epistaxis such as a history of frequent epistaxis, anticoagulant use or bleeding disorders in addition to other absolute contraindications for NTI.[70] For these patients, the deficient clotting factors or platelets must first be replenished, anticoagulant must be stopped for an adequate time and/or alternative airway options should be considered.
Nasal flow rate assessment, preoperative bilateral nasal fiberoptic endoscopy exam by an experienced otolaryngologist (ENT) or anesthesia provider and preoperative evaluation of paranasal sinuses on head Computed Tomography (CT)/skull radiograph imaging are helpful in identifying significant asymptomatic intranasal abnormalities such as bony spurs/septal deviations that impact patency and choice of nostril for NTI.[71,72,73] The right nostril appears to be generally more appropriate for NTI when both nostrils are symmetrically patent based on lower incidence/severity of epistaxis and faster intubation time but similar nasal passage time.[74,75,76] Keeping the bevel tip of a NETT on the lateral side of the nostril helps reduce epistaxis and the risk of middle turbinectomy.[77,78]
Clinicians have a slew of epistaxis reducing interventions to choose from. “Telescoping the NETT” with a red rubber Robinson/Jaques Nelaton catheter or “obturating the NETT” with a NGT/an esophageal stethoscope is conducive for safe navigational guidance through the nasal pathway and significantly decreases the incidence and severity of epistaxis during NTI.[79,80,81,82] (Supplementary 1). An additional benefit of the red rubber catheter guided technique is the reduction of NETT tip contamination by nasal mucosa and decreased transfer of tissue/bacteria from the nasal cavity into the lungs.[83]
Using the lower nasal pathway between the inferior turbinate and nasal floor is safer in comparison to the upper nasal pathway because the lower pathway is away from the middle turbinate and cribriform plate.[84,85] Both nasal tip lifting and use of a red rubber catheter or NGT as a guide during NETT insertion helps facilitate passage through the lower nasal pathway reducing the incidence and severity of epistaxis.[86]
Preparation of the nasal passage is useful to reduce epistaxis. Using vasoconstrictive agents such as oxymetazoline or phenylephrine can reduce vascular engorgement while lubrication with lidocaine jelly provides both lubrication and local anesthesia to minimize sympathetic response.[87] Progressive dilation of the naris with nasopharyngeal airways of increasing size can help dilate the nasal tissues and reduce the risk of mucosal damage, albeit with variable efficacy.[88] Thermosoftening NETT with warm saline (~35C) and controlling the hypertension induced by the autonomic sympathetic response during NTI with sedatives, antihypertensives and opioids can also help reduce the severity of epistaxis.[89,90] Finally, Combining NETT telescoping together with thermosoftening also has shown to be more efficacious than either technique alone.[91]
5. Conclusion
Nasotracheal intubation(NTI) is a critical airway management technique. The decision-making process for NTI begins with selection of an appropriate initial approach based on the clinical situation, likelihood of difficult ventilation or intubation pre-induction, patient cooperativeness as well as the clinician’s preference based on prior experience/comfort. Subsequent decision-making in the NTI pathway varies based on the initial approach chosen. Epistaxis reduction measures should always be applied to reduce the severity of this common complication and minimize its effect on NTI securement. By using the updated NTI Algorithm to guide them and having knowledge of the variety of techniques described in this manuscript, clinicians can not only start with a safe initial approach to secure NTI but also adapt to different clinical scenarios to optimize procedural success.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure Captions: Figure 1 illustrates an a nasotracheal intubation (NTI) algorithm including the 3 initial approaches and a decision making tree for the “routine NTI” (RNTI) pathway. Figure 2 illustrates published OTI to NTI conversion techniques to date including direct (with glottic visualization) and indirect (without glottic visualization) pathways. VIDEOS: (Video 1) https://m.youtube.com/watch?v=RxWc8JK0_iE (on page 1) illustrates the “routine Nasotracheal Intubation”(RNTI) approach which is an asleep NTI with the help of direct laryngoscopy (DL) and Magill forceps (Video 2) https://emedicine.medscape.com/article/1663655-technique?form=fpf#showall (Reference 26) illustrates the blind nasotracheal intubation technique courtesy of Therese Canares, MD, and Jonathan Valente, MD, Rhode Island Hospital, Brown University. (Video 3) https://m.youtube.com/watch?v=z1hhHxMaAD0 illustrates the Smith & FennerFIS Guided direct OTI to NTI conversion technique which advances a FIS (loaded with a NETT) through the vocal cords adjacent to the existing OETT. (Video 4) https://m.youtube.com/watch?v=9KgkQ7R9BB4 illustrates the Backman & Wadhera “Two Bougie” direct OTI to NTI conversion technique which leverages two bougies (AECs) for continuous airway security. (Video 5) https://m.youtube.com/watch?v=fz3REayMf8M illustrates the “Retrograde AEC” indirect OTI to NTI conversion technique described by Kim DW et al., where the proximal end of an oral AEC is inserted retrograde through the tip of a NETT withdrawn out of the mouth earlier. Then the NETT is railroaded or tracked over the nasotracheal AEC into the trachea. (Video 6) https://m.youtube.com/watch?v=on9TgMstpsk illustrates the “Modified Connector” indirect OTI to NTI conversion technique by Desilva et al., whereby the proximal end of an AEC is seated into the slit distal end of a NGT outside of the mouth and sutured together to establis a NGT-AEC connection and a nasotracheal AEC conduit to guide advancement of a NETT into the trachea (Video 7) https://m.youtube.com/watch?v=_amqGHno5GI illustrates the “Tear-Away” indirect OTI to NTI conversion technique by Salibian et al. whereby a nasal AEC is withdrawn out of the mouth and inserted through an OETT (after removal of the OETT connector) into the trachea. The OETT without the connector is then cut longitudinally in a “tear-away” fashion preserving the nasotracheal AEC conduit in place to advance a NETT into the trachea. (Video 8) https://m.youtube.com/watch?v=LZ7XWWKS8yU illustrates the “Genesis Interchangeable Oral-Nasal ETT Connection” indirect OTI to NTI conversion technique, where the distal end of a NETT (after removal of the introducer) and proximal OETT (after removal of the OETT connector) of the Genesis ONETT Airway have been manufactured to easily connect together firmly allowing for a continuous NETT. (Supplementary 1) https://doi.org/10.4236/ojanes.2017.78028 (Reference 11) illustrates the red rubber catheterguided technique for NTI and cites evidence for significant epistaxis reduction with this method.
Acknowledgements
Supplementary digital videos were created by graphic artist Phoenix Rose Hoffman based on Dr. Mahesh Desilva’s draft drawings and guidance.
Conflicts of Interest
No conflict of interest to disclose for any of the authors.
References
- Park DH, Lee CA, Jeong CY, Yang HS. Nasotracheal intubation for airway management during anesthesia. Anesth Pain Med (Seoul). 2021 Jul;16(3):232-247. [CrossRef]
- Hall CE, Shutt LE. Nasotracheal intubation for head and neck surgery. Anaesthesia. 2003 Mar;58(3):249-56. [CrossRef]
- Chauhan V, Acharya G. Nasal intubation: A comprehensive review. Indian J Crit Care Med. 2016 Nov;20(11):662-667. [CrossRef]
- Yoo H, Choi JM, Jo JY, Lee S, Jeong SM. Blind nasal intubation as an alternative to difficult intubation approaches. J Dent Anesth Pain Med. 2015 Sep;15(3):181-184. [CrossRef]
- Piepho T, Thierbach A, Werner C. Nasotracheal intubation: look before you leap. Br J Anaesth. 2005 Jun;94(6):859-60. [CrossRef]
- Backman SB, Uria M, Kost K, Schricker T. Case report: nasotracheal intubation--look before leaping to assess the laryngeal view. Can J Anaesth. 2008 May;55(5):302-5. [CrossRef]
- Prasanna D, Bhat S. Nasotracheal Intubation: An Overview. J Maxillofac Oral Surg. 2014 Dec;13(4):366-72. [CrossRef]
- Cincotta FA, Neidorff C. Blind awake nasotracheal intubation. Anesth Prog. 1977 Jan-Feb;24(1):15-7. PMCID: PMC2516107.
- Dhasmana S, Singh V, Pal US. Awake Blind Nasotracheal Intubation in Temporomandibular Joint Ankylosis Patients under Conscious Sedation Using Fentanyl and Midazolam. J Maxillofac Oral Surg. 2010 Dec;9(4):377-81. PMID: 22190828 . [CrossRef]
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, Fiadjoe JE, Greif R, Klock PA, Mercier D, Myatra SN, O’Sullivan EP, Rosenblatt WH, Sorbello M, Tung A. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022 Jan 1;136(1):31-81. [CrossRef]
- Jeon DG, Song J, Kim SK, Ji SH. Massive Epistaxis during Nasotracheal Intubation. J Korean Dent Soc Anesthesiol. 2013 Jun;13(2):51-54. [CrossRef]
- Lera, S. Lera, S., Machan, M. and Derefaka, G. (2017) A Safer Technique for Nasal Intubation: A Literature Review. Open Journal of Anesthesiology, 7, 275-285. [CrossRef]
- Nakamura S, Watanabe T, Hiroi E, Sasaki T, Matsumoto N. Hori T: [cuff damage during naso-tracheal intubation for general anesthesia in oral surgery]. Masui. 1997;46(11):1508–14. PMID: 9404138.
- Gorback, MS. Gorback MS. Inflation of the endotracheal tube cuff as an aid to blind nasal endotracheal intubation. Anesth Analg. 1987;66:916–7 PMID: 3619105.
- Kumar R, Gupta E, Kumar S, Rani Sharma K, Rani Gupta N. Cuff inflation-supplemented laryngoscope-guided nasal intubation: a comparison of three endotracheal tubes. Anesth Analg. 2013;116(3):619–24. [CrossRef]
- Goodine C, Sparrow K, Asselin M, Hung D, Hung O. The alignment approach to nasotracheal intubation. Can J Anaesth. 2016 Aug;63(8):991-2. [CrossRef]
- Choudhry DK, Brenn BR, Lutwin-Kawalec M, Sacks K, Nesargi S, He Z. Effect of 90° counterclockwise rotation of the endotracheal tube on its advancement through the larynx during nasal fiberoptic intubation in children: a randomized and blinded study. Paediatr Anaesth. 2016 Apr;26(4):378-83. [CrossRef]
- Abrons RO, Vansickle RA, Ouanes JP. Seldinger technique for nasal intubation: a case series. J Clin Anesth. 2016 Nov;34:609-11. PMID: 27687457. [CrossRef]
- Techanivate A, Kumwilaisak K, Worasawate W, Tanyong A. Estimation of the proper length of nasotracheal intubation by Chula formula. J Med Assoc Thai. 2008 Feb;91(2):173-80. PMID: 18389981.
- Use Of A Nasal Airway To Assist Ventilation During Fiberoptic Intubation. Anyone Can Intubate, 5th Edition, C. Whitten MD https://airwayjedi.com/2015/09/16/use-of-a-nasal-airway-to-assist-ventilation-during-fiberoptic-intubation/.
- Mohammadzadeh A, Haghighi M, Naderi B, Chaudhry A, Khan ZH, Rasouli MR, Saadat S. Comparison of two different methods of fiber-optic nasal intubation: conventional method versus facilitated method (NASAL-18). Ups J Med Sci. 2011 May;116(2):138-41. [CrossRef]
- Syal R, Parvez M, Kothari N, Abbas H, Kumar R, Singh S, Choudhary G. Comparison of Conventional Technique versus Modified Tube First Technique of Awake Nasotracheal Fiber-optic Intubation: A Randomized Control Open-Label Trial. Anesth Essays Res. 2020 Jul-Sep;14(3):395-400. [CrossRef]
- Spinella MK, Nathan H, Wilson T, Perez DE. A Reliable Protocol for Fiberoptic Nasal Intubation. J Oral Maxillofac Surg. 2025 Feb;83(2):148-155. [CrossRef]
- Ryoo SH, Park KN, Karm MH. The utilization of video laryngoscopy in nasotracheal intubation for oral and maxillofacial surgical procedures: a narrative review. J Dent Anesth Pain Med. 2024 Feb;24(1):1-17. [CrossRef]
- Tseng KY, Lu IC, Shen YC, Lin CH, Chen PN, Cheng KI. A comparison of the video laryngoscopes with Macintosh laryngoscope for nasotracheal intubation. Asian J Anesthesiol. 2017 Mar;55(1):17-21. [CrossRef]
- Jiang J, Ma DX, Li B, Wu AS, Xue FS. Videolaryngoscopy versus direct laryngoscopy for nasotracheal intubation: A systematic review and meta-analysis of randomised controlled trials. J Clin Anesth. 2019 Feb;52:6-16. [CrossRef]
- Kwak HJ, Lee SY, Lee SY, Cho SH, Kim HS, Kim JY. McGrath Video Laryngoscopy Facilitates Routine Nasotracheal Intubation in Patients Undergoing Oral and Maxillofacial Surgery: A Comparison With Macintosh Laryngoscopy. J Oral Maxillofac Surg. 2016. [CrossRef]
- Yeom JH, Oh MK, Shin WJ, Ahn DW, Jeon WJ, Cho SY. Randomized comparison of the effectiveness of nasal intubation using a GlideScope video laryngoscope with Magill forceps versus vascular forceps in patients with a normal airway. Can J Anaesth. 2017 Dec;64(12):1176-1181. [CrossRef]
- Kang R, Jeong JS, Ko JS, Ahn J, Gwak MS, Choi SJ, Hwang JY, Hahm TS. Neutral Position Facilitates Nasotracheal Intubation with a GlideScope Video Laryngoscope: A Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(3):671. [CrossRef]
- Nedrud SM, Baasch DG, Cabral JD, McEwen DS, Dasika J. Combined Video Laryngoscope and Fiberoptic Nasal Intubation. Cureus. 2021 Nov 11;13(11):e19482. PMID: 34912623 . [CrossRef]
- Hodgson RE, Gunning MDG. Oral to nasal endotracheal tube exchange using both video and flexible laryngoscopes. South Afr J Anesth Analg. 2018;24:168–169. [CrossRef]
- Douglas B, Stacey N, Salam S, Jayanth D. A hybrid nasal intubation technique for the head and neck surgical patient: a case series and review of the literature. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. Volume 131, Issue 1, 2021, Pages e38-e39.
- Dong Y, Li G, Wu W, Su R, Shao Y. Lightwand-guided nasotracheal intubation in oromaxillofacial surgery patients with anticipated difficult airways: a comparison with blind nasal intubation. Int J Oral Maxillofac Surg. 2013 Sep;42(9):1049-53. PMID: 23712007. [CrossRef]
- Kuang-I Cheng, Hung-T Hsu, Chia-H Lin, Kuang-Y Tseng, Ya-C Shen, Chung-H Chen, Wen-M Chuang, Trachway in Assistance of Nasotracheal Intubation with a Preformed Nasotracheal Tube in Patients Undergoing Oro-Maxillofacial Surgery, BJA: British Journal of Anaesthesia, Volume 113, Issue eLetters Supplement, 29 December 2014. [CrossRef]
- Yu J, Hu R, Wu L, Sun P, Zhang Z. A comparison between the Disposcope endoscope and fibreoptic bronchoscope for nasotracheal intubation: a randomized controlled trial. BMC Anesthesiol. 2019;19(1):163. [CrossRef]
- Morgan JP 3rd, Haug RH, Holmgreen WC. Awake blind nasoendotracheal intubation: a comprehensive review. J Oral Maxillofac Surg. 1994 Dec;52(12):1303-11. [CrossRef]
- Blind nasotracheal intubation video courtesy of Therese Canares, MD, and Jonathan Valente, MD, Rhode Island Hospital, Brown University https://emedicine.medscape.com/article/1663655-technique?form=fpf#showall.
- Dyson A, Saunders PR, Giesecke AH. Awake blind nasal intubation: use of a simple whistle. Anaesthesia. 1990 Jan;45(1):71-2. [CrossRef]
- King HK, Wooten JD. Blind nasal intubation by monitoring end-tidal CO2. Anesth Analg. 1989 Sep;69(3):412-3. PMID: 2505644.
- Asai, T. Asai T. Use of the endotrol endotracheal tube and a light wand for blind nasotracheal intubation. Anesthesiology. 1999 Nov;91(5):1557. [CrossRef]
- Tsukamoto M, Hitosugi T, Yokoyama T. Awake fiberoptic nasotracheal intubation for patients with difficult airway. J Dent Anesth Pain Med. 2018 Oct;18(5):301-304. [CrossRef]
- Ahmad, I. Ahmad, I. NYSORA: Regional and Topical Anesthesia for Awake Endotracheal Intubation. https://www.nysora.com/techniques/head-and-neck-blocks/airway/regional-topical-anesthesia-awake-endotracheal-intubation/#toc.
- Liu JH, Xue FS, Liao X, Zhang YM. Awake nasal intubation using a combination of the EndoFlex tube and fibreoptic bronchoscopy in patients with difficult airways. Acta Anaesthesiol Scand. 2010 Jan;54(1):121-2; author reply 122. [CrossRef]
- Sharma D, Bithal PK, Rath GP, Pandia MP. Effect of orientation of a standard polyvinyl chloride tracheal tube on success rates during awake flexible fibreoptic intubation. Anaesthesia. 2006 Sep;61(9):845-8. [CrossRef]
- Lomax SL, Johnston KD, Marfin AG, Yentis SM, Kathawaroo S, Popat MT. Nasotracheal fibreoptic intubation: a randomised controlled trial comparing the GlideRite® (Parker-Flex® Tip) nasal tracheal tube with a standard pre-rotated nasal RAE™ tracheal tube. Anaesthesia. 2011 Mar;66(3):180-4. [CrossRef]
- Johnston KD, Rai MR. Conscious sedation for awake fibreoptic intubation: a review of the literature. Can J Anaesth. 2013 Jun;60(6):584-99. [CrossRef]
- Kramer A, Müller D, Pförtner R, Mohr C, Groeben H. Fibreoptic vs videolaryngoscopic (C-MAC(®) D-BLADE) nasal awake intubation under local anaesthesia. Anaesthesia. 2015 Apr;70(4):400-6. [CrossRef]
- Gupta N, Garg R, Saini S, Kumar V. GlideScope video laryngoscope-assisted nasotracheal intubation by cuff-inflation technique in head and neck cancer patients. Br J Anaesth. 2016 Apr;116(4):559-60. [CrossRef]
- Kumar, A. Kumar A. Nasal Retrograde Intubation in Oromaxillofacial Surgery Patients with Limited Mouth Opening: A Cross- sectional Study. Int J Sci Stud 2018;6(3):57-61.
- Vadepally AK, Sinha R, Kumar AVSSS. Retrograde intubation through nasal route in patients with limited mouth opening undergoing oral and maxillofacial surgery. J Oral Biol Craniofac Res. 2018 Jan-Apr;8(1):30-34. [CrossRef]
- Smith JE, Fenner SG. Conversion of orotracheal to nasotracheal intubation with the aid of the fibreoptic laryngoscope. Anaesthesia. 1993 Nov;48(11):1016. [CrossRef]
- Backman SB, Uria M, Kost K, Schricker T. Case report: nasotracheal intubation--look before leaping to assess the laryngeal view. Can J Anaesth. 2008 May;55(5):302-5. [CrossRef]
- Wadehra A, Tandon MS, Ganjoo P. A two-bougie technique for safer oro- to nasotracheal tube exchange in a difficult airway. Anaesthesia. 2010 Dec;65(12):1231-2. [CrossRef]
- Yogo N, Sasaki T, Kozumi M, Kinoshita Y, Muto Y, Hirai K, Yoshino Y. Oral to nasal endotracheal tube exchange using tracheal tube guide and video laryngoscope in a pediatric patient with facial burns: a case report. Int J Emerg Med. 2022 Sep 5;15(1):42. [CrossRef]
- Ji S, Song J, Kim SK, Kim MY, Kim S. Fiberoptic bronchoscope and C-MAC video laryngoscope assisted nasal-oral tube exchange: two case reports. J Dent Anesth Pain Med. 2017 Sep;17(3):219-223. Epub 2017 Sep 25. [CrossRef]
- Gentry WB, Shanks CA. Reevaluation of a maneuver to visualize the anterior larynx after intubation. Anesth Analg. 1993 Jul;77(1):161-3. [CrossRef]
- Kim DW, Kim KN, Sun JE, Lim HJ. Conversion of an oral to nasal intubation in difficult nasal anatomy patients: two case reports. BMC Anesthesiol. 2021 Mar 9;21(1):72. [CrossRef]
- Nakata Y, Niimi Y. Oral-to-nasal endotracheal tube exchange in patients with bleeding esophageal varices. Anesthesiology. 1995 Dec;83(6):1380-1. [CrossRef]
- Desilva M, Maan R, Helwany ME, Bhuller AS. Oral to Nasal Endotracheal Tube Exchange: Modification to Enable Wider Applicability of an “Old Connector” Technique-A Case Report. A A Pract. 2023 Jul 21;17(7):e01703. [CrossRef]
- Salibian H, Jain S, Gabriel D, Azocar RJ. Conversion of an oral to nasal orotracheal intubation using an endotracheal tube exchanger. Anesth Analg. 2002 Dec;95(6):1822. [CrossRef]
- https://genesisairway.com/genesis-oral-nasal-endotracheal-tube-posterior-facing-bevel/.
- Sanuki T, Hirokane M, Matsuda Y, Sugioka S, Kotani J. The Parker Flex-Tip tube for nasotracheal intubation: the influence on nasal mucosal trauma. Anaesthesia. 2010 Jan;65(1):8-11. [CrossRef]
- Jafari A, Gharaei B, Kamranmanesh MR, Aghamohammadi H, Nobahar MR, Poorzamany M, Shahrabi M, Solhpour A. Wire reinforced endotracheal tube compared with Parker Flex-Tip tube for oral fiberoptic intubation: a randomized clinical trial. Minerva Anestesiol. 2014 Mar;80(3):324-9. PMID: 24193173.
- Vivian VH, Anaes D, L Pardon T, Van Zundert AAJ. Modified Retrograde Nasal Intubation: A New Airway Technique and Devices. Anesth Prog. 2021 Jun 1;68(2):107-113. [CrossRef]
- Dutta A, Chari P, Mohan RA, Manhas Y. Oral to nasal endotracheal tube exchange in a difficult airway: a novel method. Anesthesiology. 2002 Nov;97(5):1324-5. [CrossRef]
- De-Armendi A, Shukry M, Mayhew JF. Changing an oral endotracheal tube to a nasal tube in Pierre-Robin sequence. Paediatr Anaesth. 2009 Dec;19(12):1240-1. [CrossRef]
- Benumof JL, Augoustides JG. Rigorously Maintaining a “Targeted Depth of Insertion” for an Airway Exchange Catheter During Tracheal Tube Exchange. J Cardiothorac Vasc Anesth. 2019 Dec;33(12):3414-3415. [CrossRef]
- Jeon DG, Song J, Kim SK, Ji SH. Massive Epistaxis during Nasotracheal Intubation. J Korean Dent Soc Anesthesiol. 2013 Jun;13(2):51-54. [CrossRef]
- Inoue S, Fujimoto Y, Kawano Y, Furuya H. Difficult passage of the endotracheal tube and massive nasal bleeding during awake nasal fiberoptic intubation in a patient with airway obstruction caused by neck hematoma--a case report. Middle East J Anaesthesiol. 2011 Feb;21(1):125-7. PMID: 21991746.
- Sim WS, Chung IS, Chin JU, Park YS, Cha KJ, Lee SC, Kim YC. Risk factors for epistaxis during nasotracheal intubation. Anaesth Intensive Care. 2002 Aug;30(4):449-52. [CrossRef]
- Lim HS, Kim D, Lee J, Son JS, Lee JR, Ko S. Reliability of assessment of nasal flow rate for nostril selection during nasotracheal intubation. J Clin Anesth. 2012 Jun;24(4):270-4. [CrossRef]
- Tong JL, Tung A. A Randomized Trial Comparing the Effect of Fiberoptic Selection and Guidance Versus Random Selection, Blind Insertion, and Direct Laryngoscopy, on the Incidence and Severity of Epistaxis After Nasotracheal Intubation. Anesth Analg. 2018 Aug;127(2):485-489. [CrossRef]
- Thota RS, Doctor JR. Evaluation of paranasal sinuses on available computed tomography in head and neck cancer patients: An assessment tool for nasotracheal intubation. Indian J Anaesth. 2016 Dec;60(12):960-961. [CrossRef]
- Tan YL, Wu ZH, Zhao BJ, Ni YH, Dong YC. For nasotracheal intubation, which nostril results in less epistaxis: right or left?: A systematic review and meta-analysis. Eur J Anaesthesiol. 2021 Nov 1;38(11):1180-1186. [CrossRef]
- Boku A, Hanamoto H, Hirose Y, Kudo C, Morimoto Y, Sugimura M, Niwa H. Which nostril should be used for nasotracheal intubation: the right or left? A randomized clinical trial. J Clin Anesth. 2014 Aug;26(5):390-4. Epub 2014 Aug 10.. [CrossRef]
- Sanuki T, Hirokane M, Kotani J. Epistaxis during nasotracheal intubation: a comparison of nostril sides. J Oral Maxillofac Surg. 2010 Mar;68(3):618-21. Epub 2009 Nov 22. [CrossRef]
- Moore, Daniel C. M.D.. Middle Turbinectomy: A Complication of IMPROPER Nasal Intubation?. The Journal of the American Society of Anesthesiologists 92(5):p 1504, May 1, 2000. [CrossRef]
- Park JY, Yu J, Kim CS, Mun T, Jeong WS, Choi JW, Lee K, Kim YK. Reverse tube direction and epistaxis in left nasotracheal intubation: a randomized controlled trial. Korean J Anesthesiol. 2024 Dec;77(6):596-604. [CrossRef]
- Wong A, Subar P, Witherell H, Ovodov KJ. Reducing nasopharyngeal trauma: the urethral catheter-assisted nasotracheal intubation technique. Anesth Prog. 2011 Spring;58(1):26-30. Anesth Prog. 2011 Summer;58(2):107. [CrossRef]
- Lim CW, Min SW, Kim CS, Chang JE, Park JE, Hwang JY. The use of a nasogastric tube to facilitate nasotracheal intubation: a randomised controlled trial. Anaesthesia. 2014 Jun;69(6):591-7. Epub 2014 Apr 18. [CrossRef]
- Bahk JH, Ahn WS, Lim YJ. Use of esophageal stethoscope as an introducer during nasotracheal intubation. Anesthesiology. 2000 May;92(5):1503-4. PMID: 10781307. [CrossRef]
- Watt S, Pickhardt D, Lerman J, Armstrong J, Creighton PR, Feldman L. Telescoping tracheal tubes into catheters minimizes epistaxis during nasotracheal intubation in children. Anesthesiology. 2007 Feb;106(2):238-42. [CrossRef]
- Enk D, Palmes AM, Van Aken H, Westphal M. In Nasotracheal intubation: a simple and effective technique to reduce nasopharyngeal trauma and tube contamination. Anesth Analg. 2002 Nov; 95(5): 1432-6, table of contents. https://doi/10.1097/00000539-200211000-00061; 83. Enk D, Palmes AM, Van Aken H, Westphal M. Nasotracheal intubation: a simple and effective technique to reduce nasopharyngeal trauma and tube contamination. Anesth Analg. 2002 Nov;95(5):1432-6, table of contents. [Google Scholar] [CrossRef]
- Prasanna D, Bhat S. Nasotracheal Intubation: An Overview. J Maxillofac Oral Surg. 2014 Dec;13(4):366-72. Epub 2013 May 1. [CrossRef]
- Ahmed-Nusrath A, Tong JL, Smith JE. Pathways through the nose for nasal intubation: a comparison of three endotracheal tubes. Br J Anaesth. 2008 Feb;100(2):269-74. Epub 2007 Dec 14. [CrossRef]
- Kim H, Lee JM, Lee J, Hwang JY, Chang JE, No HJ, Won D, Choi S, Min SW. Influence of Nasal Tip Lifting on the Incidence of the Tracheal Tube Pathway Passing Through the Nostril During Nasotracheal Intubation: A Randomized Controlled Trial. Anesth Analg. 2018 Dec;127(6):1421-1426. [CrossRef]
- Katz RI, Hovagim AR, Finkelstein HS, Grinberg Y, Boccio RV, Poppers PJ. A comparison of cocaine, lidocaine with epinephrine, and oxymetazoline for prevention of epistaxis on nasotracheal intubation. J Clin Anesth. 1990 Jan-Feb;2(1):16-20. [CrossRef]
- Dhakate VR, Singam AP, Bharadwaj HS. Evaluation of Nasopharyngeal Airway to Facilitate Nasotracheal Intubation. Ann Maxillofac Surg. 2020 Jan-Jun;10(1):57-60. Epub 2020 Jun 8. [CrossRef]
- Kim YC, Lee SH, Noh GJ, Cho SY, Yeom JH, Shin WJ, Lee DH, Ryu JS, Park YS, Cha KJ, Lee SC. Thermosoftening treatment of the nasotracheal tube before intubation can reduce epistaxis and nasal damage. Anesth Analg. 2000 Sep;91(3):698-701. [CrossRef]
- Kim EM, Chung MH, Lee MH, Choi EM, Jun IJ, Yun TH, Ko YK, Kim JH, Jun JH. Is Tube Thermosoftening Helpful for Videolaryngoscope-Guided Nasotracheal Intubation?: A Randomized Controlled Trial. Anesth Analg. 2019 Sep;129(3):812-818. [CrossRef]
- Seo KS, Kim JH, Yang SM, Kim HJ, Bahk JH, Yum KW. A new technique to reduce epistaxis and enhance navigability during nasotracheal intubation. Anesth Analg. 2007 Nov;105(5):1420-4. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



