
Submitted:
25 September 2025
Posted:
28 September 2025
You are already at the latest version
Abstract
Background/Objectives: Lactobacilli are recognized as indicators of vaginal health and probiotics represent a valuable approach to maintain or restore the homeostasis of the vaginal ecosystem. A randomized double-blind placebo-controlled study was conducted to confirm the health benefits of the orally administered probiotic Lacticaseibacillus rhamnosus CA15 strain, compared to placebo, in a large cohort of women with bacterial vaginosis (BV) and mixed vaginitis (MV), mainly related to mild aerobic vaginitis (AV) and vulvovaginal candidiasis (VVC). Methods: Two-hundred women, exhibiting signs and symptoms of bacterial vaginosis (BV) and mixed vaginitis (MV), were recruited, and randomly assigned in a 1:1 ratio to receive for 10 days, oral capsules containing 1x1010 colony forming units (cfu) of the L. rhamnosus CA15 strain (Active group) or a placebo (Placebo group). Clinical (leucorrhoea, burning, itching, vulvovaginal erythema/oedema, subjective vaginal discomfort, Nugent score, Amsel criteria, and Lactobacillary grade) and microbiological parameters (vaginal microbiota composition) were assessed at baseline (T0), 10 days after the start of the treatment (T1), and 30 days post-treatment (T2). In addition, quality of life was evaluated at baseline and 30 days post-treatment using the WHOQOL-BREF questionnaire. The study protocol was registered on clinicaltrials.gov (ID: NCT05796921). Results: The oral administration of the L. rhamnosus CA15 strain resulted in significant improvements in clinical characteristics of BV (leucorrhea, Nugent score, and Amsel criteria), AV (lactobacillary grade, discharge, and subjective vaginal discomfort), and VVC (leucorrhea, burning, itching, vulvovaginal erythema/oedema, and subjective vaginal discomfort) as well as changes in the vaginal microbiota composition. Furthermore, participants allocated to the Active group reported enhancements in physical and psychological health, social relations, environment, and overall quality of life. No significant changes in clinical and microbiological parameters nor in quality of life, were observed in the Placebo group. Conclusions: The randomized double-blind placebo-controlled study conducted on a large cohort of women highlighted the therapeutic value of the L. rhamnosus CA15 in the management of BV occurring with mixed infections. This probiotic strain represents a safe and effective strategy for restoring the balance of the vaginal microbiota, alleviating clinical symptoms, and enhancing the quality of life of subjects with co-occurring vaginal infections. This finding offers new perspectives for the treatment and prevention of common gynecological disorders.
Keywords:
probiotic
; vaginal dysbiosis
; quality of life
; women’s health
; Lacticaseibacillus rhamnosus
1. Introduction
Probiotics are widely recognized as health-promoting microorganisms that play a crucial role in preserving the health of the female reproductive tract, alleviating dysbiotic gynecological conditions, and boosting the vaginal immune response [1]. Advances in the study of vaginal microbiota composition and function have led to the widespread understanding that, under physiological conditions, this ecosystem is dominated by lactobacilli [2,3]. This group of bacteria is recognized as key indicator of vaginal health, being able to exert protective effects which are linked to the ability to produce antimicrobial compounds such as bacteriocins, bacteriocin-like inhibitory substances, organic acids, hydrogen peroxide (H2O2), siderophores, and biosurfactants [4]. Specifically, by hydrolyzing glycogen present in vaginal mucosal cells into glucose, and ultimately producing lactic acid, lactobacilli play a crucial role in restoring a healthy vaginal microbiome, since capable of inhibiting pathogen colonization and displacing pathogens already adhered to epithelial cells. Additionally, they act synergistically as a consortium in their probiotic activity [5,6,7]. A reduction in the proportion or abundance of lactobacilli is associated with various vaginal infections including bacterial vaginosis (BV), vulvovaginal candidiasis (VVC), aerobic vaginitis (AV), and infections caused by human papillomavirus (HPV), human immunodeficiency virus (HIV), herpes simplex virus 2 (HSV-2). Additionally, it is linked to other sexually transmitted infections (STIs) such as gonorrhea, trichomoniasis, Chlamydia, Mycoplasma, and Ureaplasma [8]. Among these, BV, VVC, and mixed vaginal infections are considered a common problem in women [9,10]. Recent systematic reviews and meta-analyses have confirmed the potential benefits of probiotics in managing these dysbiotic conditions, including improvements in clinical outcomes, restoration of a balanced vaginal microbiota, symptom relief, and a reduction in infection recurrence rate. Additional benefits of probiotic lactobacilli include the reduction of genital inflammation and the preservation of the vaginal epithelial barrier integrity. Probiotic lactobacilli offer a valuable alternative or complementary approach to conventional antimicrobial therapies [11,12]. In this perspective, significant progress has been made in the development of supplements aimed at restoring the homeostasis of the vaginal microbiome [1,13,14]. Among probiotic lactobacilli, the Lacticaseibacillus rhamnosus CA15 strain (DSM 33960) has emerged as a valuable probiotic, capable of restoring and maintaining a balanced vaginal microbiota. Isolated from the vaginal ecosystem of a healthy woman, the L. rhamnosus CA15 strain (patent number IT202200016542A) was previously tested both in vitro and in vivo for its probiotic features [15,16]. Along with safety standards, the L. rhamnosus CA15 strain, demonstrated strong adhesion to both vaginal and intestinal cell lines, the ability to antagonize a wide range of urogenital pathogens such as Escherichia coli, Candida spp., Gardnerella vaginalis, Pseudomonas aeruginosa, Staphylococcus aureus, and Streptococcus agalactiae. By measuring the scavenging activity of the superoxide radical generated by the self-oxidation of pyrogallol, the CA15 strain demonstrated antioxidant potential. This activity could be related to the production of bioactive metabolites able to mitigate oxidative stress in intestinal cells. In addition, the CA15 strain exerted anti-inflammatory activity as revealed by a decrease in the IL-6 and, in turn, an increase in the IL-2 in LPS-treated Caco-2 cells. This modulation indicates that the strain may influence immune responses by interacting with immune receptors, such as Toll-like receptors (TLRs), and activating signaling pathways that promote the production of anti-inflammatory cytokines. Due to these features, as well as its resilience under the harsh conditions of gastrointestinal passage, the L. rhamnosus CA15 was administered as a supplement in a randomized, double-blind, placebo-controlled trial involving 60 women evident signs and symptoms of BV, complicated by an overgrowth of microorganisms related to mixed vaginitis (MV) [16]. After 10 days of the L. rhamnosus CA15 strain administration, significant improvements were observed in both clinical signs and symptoms of vaginal dysbiosis (burning, itching, leucorrhea, subjective vaginal discomfort, and vulvo-vaginal erythema/edema), a notable reduction in vaginal pathogens, and a concomitant increase in lactobacilli. These effects were observed even 30 days post-treatment. In addition, the L. rhamnosus CA15 strain administration led to significant improvements in the perceived physical health, social relations, and environment of the enrolled participants [16]. On this basis, the present randomized double-blind placebo-controlled trial aimed to confirm the effectiveness of the orally administered L. rhamnosus CA15 strain, in treating BV with co-occurring vaginal infections in a large cohort of women.
2. Materials and Methods
2.1. Trial Population
The present single-center randomized double-blind placebo-controlled trial was conducted at the Department of General Surgery and Medical Surgical Specialties, Gynaecological Clinic, AOU Policlinico G. Rodolico-San Marco Hospital, Catania (Italy). Participants with evident signs and symptoms of BV and co-occurring mixed vaginal infections, who satisfy the inclusion and exclusion criteria outlined in Table 1, voluntarily participated in the study without any financial compensation. Information about the study protocol, procedures, and investigational product were provided to each participant and their right to withdraw from the study at any time. Written informed consent was obtained from all participants. All personal data were treated anonymously in accordance with Italian law, guaranteeing privacy.
2.2. Trial Design and Treatment
The study was conducted, from April 2023 to May 2025, according to the Good Clinical Practice and the World Medical Association (WMA) policy regarding Ethical Principles for Medical Research Involving Human Subjects, as stated in the Declaration of Helsinki. The study protocol was approved by the local Ethical Committee (registration number 163/2022/PO) and was registered on clinicaltrials.gov (ID: NCT05796921). All the design, analysis, interpretation of data, drafting, and revisions followed the CONSORT (CONsolidated Standards Of Reporting Trials) [17] and SPIRIT (Standard Protocol Items: Recommendation for Interventional Trials) Statements [18].
The primary efficacy outcomes included changes in the composition of vaginal microbiota, with a significant reduction of potential pathogenic bacteria and an increase of lactobacilli, as well as attenuation or resolution of signs and symptoms of vaginal dysbiosis. The secondary outcome was the improvement of quality of life (QoL). A priori power analysis was conducted to determine the appropriate sample size for detecting a clinically meaningful difference in the primary efficacy outcomes between Active and Placebo groups at the 30-day post-treatment evaluation (T2). Based on preliminary data from a pilot trial involving 60 participants [16], an effect size (Cohen’s d) of 0.6 was estimated for between-group differences in microbiological and clinical outcome scores. To achieve a power of 0.90 at an alpha level of 0.05 (two-tailed), a minimum sample size of 86 participants per group was required. Accounting for an anticipated dropout rate of 15–20%, a total of 200 participants (100 per group) were enrolled to ensure sufficient power and maintain statistical validity across all primary and secondary endpoints. Eligible participants, as defined by the inclusion and exclusion criteria (Table 1), were screened and enrolled sequentially. Following informed consent, participants were randomly assigned in a 1:1 ratio to receive either the Active or Placebo treatment, as illustrated in the CONSORT flow diagram (Figure 1). Randomization was implemented using a computer-generated sequence via a centralized, permuted block method with variable block sizes, ensuring allocation concealment. The randomization list was generated by an independent statistician not involved in the clinical aspects of the study. Allocation assignments were concealed in opaque, sequentially numbered envelopes and maintained by study personnel uninvolved in data collection or outcome assessment. Participants took one capsule per day for 10 consecutive days. The Active treatment consisted of a transparent vegetable capsule containing 10x1010 viable cells of the L. rhamnosus CA15 strain and corn starch. The placebo capsules were identical in appearance and composition, except for the absence of the bacterial strain. Capsules, manufactured by SYNBIOTEC srl (Camerino, Italy), were provided in standardized blisters of 15 units.
Blinding was maintained for participants, investigators, laboratory personnel, and data analysts throughout the study duration.
2.3. Visits and Assessment
After the baseline assessment (T0), follow-up visits were conducted at 10 days (T1) and 30 days post-treatment (T2). At baseline, demographic data were collected, including information on age, BMI, smoking habits, contraceptives use, history of vaginal infection, and sexual activity. At each sampling time (T0, T1, and T2), clinical signs and symptoms, Amsel criteria (homogenous vaginal discharge, presence of clue cells, positive amine test, and vaginal fluid pH) [19], Nugent score [20], Lactobacillary grade (LBG), and vaginal microbiota composition were evaluated. In detail, the clinical signs and symptoms leucorrhoea (associated to both BV and VVC); burning, itching and vulvovaginal erythema/oedema (associated to VVC); discharge and subjective vaginal discomfort (mainly associate to AV) were assessed on a severity scale ranging from 0 (absent or normal) to 3 (severe). The Nugent score was assessed using a 10-point scale based on microscope examination (1000× magnification, oil immersion) of Gram-stained vaginal smears. A score between 0 and 3, characterized by the dominance of lactobacilli, was considered as normal vaginal microbiota, a score of 4–6 was classified as intermediate, and a score of 7–10, dominated by Gram-negative and Gram-variable rods, was presumed as BV-like condition [20]. The lactobacillary grade (LBG) was evaluated according to the Donders classification, with LBG I, indicating normal microbiota dominated by lactobacilli, LBG II, indicating a reduced number of lactobacilli mixed with other bacteria, and LBG III, indicating the absence of lactobacilli and the presence of other bacteria [21].
The composition of the vaginal microbiota was evaluated at each sampling time (T0, T1, and T2) by plate count. In detail, vaginal swabs were collected from the lateral vaginal wall and the posterior vaginal fornix using sterile cotton-tipped swabs and were immediately transferred, under refrigerated conditions, to the Laboratory of ProBioEtna, spinoff of the University of Catania (Catania, Italy). Swabs were subjected to microbiological counting following the protocol and using the agar media and conditions reported by Rapisarda and co-workers [16]. The microbiological count was performed in triplicate and results were expressed as mean log10 cfu/ml with standard deviation.
In addition, both at baseline (T0) and 30 days post-treatment (T2), the quality of life (QoL), perceived by recruited subjects, was evaluated using the World Health Organization Quality of Life – BREF (WHOQOL-BREF) questionnaire [22]. The questionnaire includes 26 items, 24 of which assess four domains of the quality of life (physical health, psychological health, social relationships, environment) while the remaining two items, examined separately, are related to the individual’s perception of overall quality of life and general health.
Responses to each item are given on a 1–5 Likert-type scale, where 1 represents the lowest level of agreement and 5 indicates the highest level of agreement with a given statement. The scores for each of the four domains were converted into a scale ranging from 0 to 100 and expressed as means. Higher mean scores reflect a better perception of QoL.
2.4. Statistical Analysis
The Mann-Whitney U test was applied to evaluate baseline differences between Active and Placebo groups for variables such as age, body mass index (BMI), Nugent score, and LBG data. Baseline characteristics related to smoking habits, contraceptive use, history of vaginal dysbiosis, sexual activity, vulvovaginal signs and symptoms, and presence of Amsel criteria were analyzed using Fisher’s exact test. To assess intra-group changes over time in vulvovaginal signs and symptoms, Nugent score, LBG data, QoL, and vaginal microbiota composition, the Wilcoxon Signed-Rank Test was applied. Amsel criteria data were evaluated using the non-parametric McNemar test, specifically suited for paired nominal data, to detect differences within-group over time. Inter-group differences in vulvovaginal signs and symptoms, Nugent score, LBG data, quality of life, and vaginal microbiota composition were assessed through the Analysis of Covariance (ANCOVA), with baseline values as covariates. For inter-group comparisons related to Amsel criteria, logistic regression analysis was performed after baseline normalization. All statistical analyses were conducted using the SciPy library in Python (version 3.9.19, SciPy 1.13.1) and differences were considered statistically significant at p-value <0.05. P-values were corrected using the Benjamini-Hochberg method.
3. Results
3.1. Participant Flow
A total of 286 women, who met the inclusion and exclusion criteria, were initially assessed for eligibility. Among these, 10 were excluded for unconfirmed microbiological diagnosis of BV and of mixed vaginal infections and 20 declined to participate. The remaining participants were randomly assigned in a 1: 1 ratio, to either Active (n=128) or Placebo group (n=128). During the follow-up visits, scheduled 10 days (T1) and 30 days (T2) post-treatment, 56 participants dropped out for different reasons (lost to follow-up, discontinued adherence to the therapeutic regime, fever for seasonal flu, pregnancy, and others). Overall, 200 women completed the study. No severe adverse events were reported throughout the observational period, and none of the participants were excluded from the study due to adverse events.
3.2. Demographic and Baseline Clinical Characteristics
The baseline demographic and clinical characteristics of the enrolled subjects are reported in Table 2 and Table 3, respectively. Overall, the two groups were homogeneous in terms of demographic characteristics and baseline clinical data. The mean age of participants assigned to the Active or Placebo groups was 32.58 ± 5.74 and 32.13 ± 6.52, respectively (p-value=0.7727). The majority of the participants had a body mass index (BMI) within the healthy normal range (between 18.5 and 24.9), were sexually active (Active, n=68; Placebo, n=71), were contraceptive users (Active, n=76; Placebo, n=79), and had a history of vaginal dysbiosis (Active, n=61; Placebo, n=58). Only 24 subjects allocated to the Active group and 22 allocated to the Placebo group had smoking habits (Table 2). Concerning clinical characteristics (Table 3), leucorrhea, burning, and subjective vaginal discomfort were the most reported symptoms in both groups. Although all participants satisfied at least three Amsel criteria, the presence of homogeneous vaginal discharge and vaginal pH > 4.5 were the most frequently observed in both groups. Almost all participants had a Nugent score between 7 and 10 (Active, n=97; Placebo, n=95) and presented LBG III (Active, n=92; Placebo, n=89).
3.3. Effect of Probiotic and Placebo Treatment on Diagnostic Parameters
3.3.1. Clinical Signs and Symptoms
Data on clinical signs and symptoms (leucorrhea, burning, itching, vulvovaginal erythema/oedema, and subjective vaginal discomfort), evaluated using a 3-point severity score (0, absent or normal; 3, severe) in both Active and Placebo groups at baseline (T0), 10 days (T1) and 30 days post-treatment (T2), as well as intra-group and inter-groups differences are displayed in Figure 2 and detailed in Tables S1 and S2.
Concerning intra-group differences, compared to baseline, a statistically significant reduction in the mean severity score for all signs and symptoms was observed in the Active group both 10 days and 30 days post-treatment. In contrast, no statistically significant changes were observed in the Placebo group throughout the study.
Results on the differences between the Active and Placebo groups (inter-group differences), are reported in Figure 2 and detailed in Table S2. Statistically significant differences (p<0.05) were observed for all the signs and symptoms evaluated, indicating that the Active group experienced significantly greater changes in symptoms from baseline compared to the Placebo group.
3.3.2. Amsel Criteria
All subjects in the Active and Placebo groups met at least three Amsel criteria at baseline. Intra-group and inter-group differences were evaluated using the McNemar Test and logistic regression, respectively. As shown in Figure 3 and Table S3, statistically significant intra-group changes were observed only in the Active group. In fact, compared to baseline, a reduction in the average frequency of homogenous vaginal discharge, clue cells, positive amine test, and vaginal pH higher than 4.5 was revealed at both T1 and T2 sampling times. Interestingly, compared to T1, a statistically significant reduction in the average frequency of homogenous vaginal discharge (p=0.0059) and vaginal pH>4.5 (p=0.0455) was revealed at T2 (Table S3). In contrast, no statistically significant changes were observed in the Placebo group, throughout the study (Figure 3, Table S3). Concerning the inter-group analysis, after baseline normalization, statistically significant differences (p<0.05) were detected between Active and Placebo groups at both T1 and T2 sampling times (Figure 3; Table S4). Based on the treatment effect, a significant reduction in the number of participants meeting the Amsel criteria was observed only the Active group.
3.3.3. Nugent Score and Lactobacillary Grade
Data on the Nugent score are displayed in Figure 4 and in Table S5. The Wilcoxon Signed-Rank Test was applied to assess intra-group variations across sampling times (T0, T1, and T2). In the Active group, compared to baseline, a significant reduction in the Nugent score was observed both at T1 and T2, and no subjects had a Nugent score between 7 and 10. Differently, no statistically significant changes were observed in the Placebo group throughout the study (Figure 4, Table S5). After baseline normalization, statistically significant inter-group differences were revealed at both T1 and T2 sampling times (Figure 4, Table S5). Data on the Lactobacillary grade (LBG) are shown in Figure 5 and in Table S6. Statistically significant intra-group differences were observed only in the Active group at both T1 and T2 sampling times, compared to baseline (Figure 5, Table S6).
3.3.4. Effect of Probiotic and Placebo Treatment on the Vaginal Microbiota Composition
The composition of the vaginal microbiota of participants, allocated to Active and Placebo groups, was evaluated at T0, T1, and T2 sampling times by plate count and results, expressed as mean log10 cfu/mL and standard deviation, are reported in Table 4. Overall, at baseline (T0) participants of both Active and Placebo groups showed a dysbiotic microbiota, characterized by an overabundance of pathogenic bacteria and a reduced presence of lactobacilli. In comparison to T0, a statistically significant reduction of all pathogens and a significant increase of lactobacilli, was achieved in the Active group at both T1 and T2 sampling time (Table 4), revealing the ability of the Lacticaseibacillus rhamnosus CA15 strain to maintain a balanced vaginal microbiota till 30 days post-treatment. In contrast, the Placebo group showed a different trend with a vaginal microbiota imbalance throughout the study. The observed statistically significant changes were related to an increase in the cell density of almost all the investigated potential pathogens and a weak increase of lactobacilli (Table 4). As reported in Table 5, the Analysis of Covariance (ANCOVA) revealed inter-group differences, at both T1 and T2 sampling times, for all the investigated microbial groups, demonstrating that only the treatment was associated with significant beneficial changes in the vaginal microbiota composition.
3.4. Effect of Probiotic and Placebo Treatment on the Perceived Quality of Life
Results on the perceived quality of life (QoL), assessed at baseline and 30 days post-treatment, using the WHOQOL-BREF questionnaire, are reported in Figure 6 and Figure 7 and in Table S7. Compared to baseline, the Wilcoxon signed-rank test revealed in the Active group statistically significant changes in all the QoL domains (physical health, psychological health, social relations, environment) (Figure 6). In addition, a significant improvement in the overall perception of quality of life (p=4.73x10-17) was shown (Figure 7, Table S7). In comparison, among the different domains, no significant variations were detected in the Placebo group (Figure 6 and Figure 7, Table S7). The ANCOVA analysis, used to compare the treatment effect between the Active and Placebo groups after baseline normalization, showed significant differences in all the QoL domains (Table S7).
4. Discussion
The imbalance of the vaginal microbiota, frequently accompanied by symptoms that cause discomfort, represents the main cause of vaginal dysbiosis, with BV, VVC, AV, and mixed vaginal infections being the most common conditions [23]. Antifungal and antibiotic treatments generally used in clinical practice, althought selective against target pathogens, can suppress beneficial lactobacilli, causing a vaginal pH increase, and recurrent rate of infection [24]. Hence, the use of probiotic lactobacilli has emerged as an alternative or supplementary therapy for vaginal infections, garnering increasing interest from both clinicians and patients dealing with vaginal disorders [25]. Both vaginal and oral administration routes have been explored. Research investigating the underlying mechanism by which oral probiotics impact the vaginal microbiota hypothesizing that probiotic orally administered can translocate from the rectum to the vagina, therefore, promoting specific clinical effects (e.g., via alleviating dysbiosis). Moreover, emerging studies suggest that the gastrointestinal microbiota is interconnected with the vagina through the “vagina-gut axis” which facilitate a bidirectional microbial translocation [24,26,27]. In this context, several hypotheses have been put forward about the ascending pathway, as the rectum can act as a reservoir for vaginal lactobacilli and facilitate microbial exchange between adjacent sites, significantly impacting the vaginal health [26,27,28]. In addition to bidirectional translocation, indirect interactions between the vagina and gut, through hematogenous route, lymph node transfer, or hormonal pathways have been suggested [26,28]. These pathways are not mutually exclusive and future studies, combining longitudinal fecal, rectal, vaginal, and systemic sampling, will be necessary to clarify the dynamics of this process.
The present study aimed to evaluate, in a large cohort of participants, the ability of the probiotic L. rhamnosus CA15 strain, orally administered, to treat BV and co-occurring vaginitis. Previously, Rapisarda and co-workers [16], by conducting a randomized double-blind placebo-controlled study on a cohort of 60 women with vaginal dysbiosis, highlighted the ability of the L. rhamnosus CA15 strain, orally administered, to significantly improve both clinical signs and symptoms and to modulate the vaginal microbiota. In this contest, Rapisarda and colleagues [16] revealed a significant reduction of co-occurring pathogens (e.g., Gardnerella, E. coli, staphylococci and Candida spp), and an increase in the cell density of lactobacilli both 10 days after the start of the treatment and 30 days post- treatment.
In line with this evidence, the present study confirmed the ability of the L. rhamnosus CA15 strain to balance the vaginal microbiota even 30 days post-treatment, demonstrating a lasting effect over time. In fact, a further increase of lactobacilli and a concomitant decrease of enterococci, staphylococci, and Gardnerella spp. was observed 30 days post-treatment. This feature could be associated with the strong adhesion properties and the ability to co-aggregate with pathogens, exhibited in vitro [15], thereby preventing their adhesion to vaginal epithelial cells and reducing colonization. The CA15 strain is also able to produce high amount of lactic acid which, by lowering the vaginal pH, creates an unfavorable environment for pathogenic microorganisms. Furthermore, the ability to synthesizes exopolysaccharides (EPS) may contribute to the exerted antimicrobial activity while the biofilm formation could enhance its persistence in the vaginal ecosystem.
Along with microbiological parameters, the L. rhamnosus CA15 strain, administeredfor 10 days, positively affected both clinical signs and symptoms caused by several pathogens, which are involved in BV and vaginal co-infections, as previously reported by Xiao and co-workers [29]. In the last years, great attention was focused on the increasing prevalence of mixed vaginal infections, a syndrome combining symptoms of different pathogenic processes, mediated by at least two types of vaginal pathogens that cause vaginal inflammation. Similar results were achieved by Vaccalluzzo and co-workers [30] who evaluated the efficacy of the L. rhamnosus TOM 22.8 strain, orally administered for 10 days, to restore the physiological conditions of the vaginal microbiota in women with BV and mixed vaginal dysbiosis. The authors, in fact, revealed a significant improvement of all the vaginal signs and symptoms both 10 days and 30 days after the start of the treatment [30]. A single-arm uncontrolled open-label trial evaluating the blend SYNBIO®, a combination of L. rhamnosus IMC501® and Lacticaseibacillus paracasei IMC502®, revealed that the oral administration of the probiotic blend for 15 days determined a statistically significant decrease in itching and vulvo-vaginal erythema/oedema. The severity score attributed to leucorrhea showed an increase whereas no significant effects on both burning and subjective vaginal discomfort were observed. Moreover, seven days after the end of the treatment, both itching and vulvo-vaginal erythema/oedema were characterized by an increasing trend, reaching values similar to those observed at baseline [31].
The evidence of the present study clearly demonstrates the ability of the L. rhamnosus CA15 strain to support the reestablishment of a balanced vaginal microbiota and to increase the cure rate without the need of antimicrobial drugs. Actually, several clinical trials evaluated the effect of oral probiotics after or during antifungal or antimicrobial treatments sometimes with conflicting results. In this context, L. rhamnosus GR-1 and Limosilactobacillus reuteri RC-14 have been extensively assessed as female orally consumed probiotic although evidence for their oral administration efficacy in the prevention and treatment of vaginal infection conditions, such as BV, remains highly debated [32]. Recently, Zhang and co-workers [33], evaluating the effectiveness of metronidazole and oral L. rhamnosus GR-1 and L. reuteri RC-14 probiotics, adjunct to metronidazole in the treatment of bacterial vaginosis, revealed that the oral probiotic adjunctive treatment did not increase the cure rate of Chinese BV patients compared to metronidazole alone [33]. Consistent with this study, the rates of BV did not differ between the probiotic and placebo groups after oral administration of L. rhamnosus GR-1 and L. reuteri RC-14 to pregnant women. Additionally, there were no differences in the α-diversity or the composition of the vaginal microbiota between or within the probiotic and placebo groups at different time points [34], nor in the cytokine and chemokine levels, as shown by Yang and colleagues [35]. Differently, the efficacy of these two probiotic strains was demonstrated in Black African and Brazilian among others [36,37]. A randomized, double-blind, placebo-controlled trial conducted in a cohort of 125 black African premenopausal women diagnosed with BV, revealed that the administration of metronidazole (500 mg) twice daily for 7 days, plus oral L. rhamnosus GR-1 and L. reuteri RC-14 twice daily for 30 days, determined negative sialidase and a shift in Nugent scores to normal values. Few patients, subjected to probiotic administration, experienced mild irritative symptoms, a weakly positive sialidase score and intermediate Nugent score. In addition, at the end of the study, a higher count of Lactobacillus spp. was observed in vaginal samples from probiotic-treated subjects compared to controls [36]. The hypothesis that the probiotics L. rhamnosus GR-1 and L. reuteri RC-14 might provide an adjunct to antimicrobial treatment and improve cure rates of BV was evaluated by Martinez and co-workers [37] on sixty-four Brazilian women. Based on the study design, enrolled patients were randomly assigned to receive a single dose of tinidazole (2 g) supplemented with either 2 placebo capsules or 2 capsules containing L. rhamnosus GR-1 and L. reuteri RC-14 for 4 weeks. At the end of treatment, according to the Gram-stain Nugent score, a significantly higher cure rate of BV was revealed in the placebo group [37].
Among probiotics suitable for oral administration, the Lactobacillus acidophilus La-14 (La-14) and L. rhamnosus HN001 (HN001) strains showed promising beneficial effects for vaginal health in randomized placebo-controlled clinical trials [38,39,40,41]. Generally, the blend mentioned above was tested in combination with lactoferrin, a glycoprotein with a well-known ability to beneficially affect the vaginal microbiota. Only one clinical trial used the blend of La-14 and HN001 devoid of lactoferrin in premenopausal Caucasian women without vaginal complaints (Nugent score 0–3 and vaginal pH ≤ 4.5) [42]. Although the therapeutic effect of the probiotic blend was not under investigation, the study revealed the ability of the probiotic blend to colonize the vagina, supporting a stable and healthy commensal vaginal microbiota, and to significantly decrease specific immune markers contributing to immunological homeostasis [42].
It is well known that symptomatic vaginal dysbiosis may have a negative impact on quality-of-life causing embarrassment, stigmatization, anxiety, and low work productivity [43,44,45,46,47]. Moreover, it is also recognized that recurrent urogenital infections also contribute to stress and can influence mental health [47]. In the present study, by using the WHO-QOL BRIEF questionnaire, a significant improvement in the quality of life was experienced by women subjected to the L. rhamnosus CA15 strain administration. In particular, improvement in environment, social relations, and physical health domains as well as in the overall perception of quality of life were revealed, confirming the results previously reported by Rapisarda and co-workers [16]. Interestingly, in the present study, a significant improvement in the psychological health domain was also achieved. Actually, few studies evaluated, in women with vaginal dysbiosis, the effects of probiotic administration on the quality of life [30,31,48]. Vaccalluzzo and co-workers [30], through The Short Form-36 (SF-36) questionnaire, demonstrated the ability of the L. rhamnosus TOM 22.8 strain to improve physical and emotional limitations as well as social functioning. Similarly, Ang and colleagues [48], by using the vulvovaginal symptom questionnaire (VSQ), revealed that the administration of a blend of lactobacilli (SynForU-HerCare) in pregnant women determined a reduction in emotional and social stress. Differently, Pino and co-workers [31], by using the WHO-QOL BRIEF questionnaire, revealed that the oral administration of SYNBIO® did not provide any significant improvement in the quality of life.
This study was limitated mainly by the short follow-up period and the lack of participant stratification based on the diagnosed vaginal infection. A part from this, ongoing studies are focusing on the detection of the L. rhamnosus CA15 strain in both vaginal and fecal samples, which could provide valuable insights into its therapeutic potential.
5. Conclusions
In conclusion, the administration of the Lacticaseibacillus rhamnosus CA15 (DSM 33960) probiotic strain can be considered an effective and safe strategy to re-establish the balance of the vaginal microbiota, to manage clinical signs and symptoms and to improve the quality-of-life of women with BV and co-occurring vaginal infections.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1. Clinical signs and symptoms reported in both Active and Placebo groups at baseline (T0), 10 days (T1) and 30 days (T2) after the end of the treatment. Data are reported as mean values related to the score obtained by the assessment of the intensity of signs and symptoms and standard deviation. Table S2. Inter-groups differences, related to the mean score values obtained by the assessment of the intensity of clinical signs and symptoms. Table S3. Amsel criteria evaluated in both Active and Placebo groups at baseline (T0), 10 days (T1) and 30 days (T2) after the end of the treatment. Data are reported as average frequency. Table S4. Inter-groups differences, related to the number of patients satisfying the Amsel criteria, based on logistic regression analysis. Table S5. Nugent score evaluated in both Active and Placebo groups at baseline (T0), 10 days (T1) and 30 days (T2) after the end of the treatment. Data are reported as number of subjects allocated to each score (0-3, normal; 4-6, intermediate; 7-10, dysbiotic). Intra-group differences were evaluated by Wilcoxon Signed-Rank Test for paired data; inter-group differences, at T1 and T2 sampling times, were evaluated by Analysis of Covariance (ANCOVA), after baseline (T0) normalization. Table S6. Lactobacillary grade (LBG) evaluated in both Active and Placebo groups at baseline (T0), 10 days (T1) and 30 days (T2) after the end of the treatment. Data are reported as number of subjects allocated to each grade (LBG I, normal; LBG II, mixed flora; LBG III, suppression of lactobacilli). Intra-group differences were evaluated by Wilcoxon Signed-Rank Test for paired data; inter-group differences, at T1 and T2 sampling times, were evaluated by Analysis of Covariance (ANCOVA), after baseline (T0) normalization. Table S7. Quality of life (QoL) evaluated through the WHOQOL-BREF questionnaire, assessed at baseline (T0) and 30 days (T2) after the end of the treatment.
Author Contributions
Conceptualization, C.L.R; methodology, A.P. and S.C.; software, A.V.; validation, S.C.; M.P. and C.C.; formal analysis, A.P. and A.V.; investigation, S.C.; M.P. and G.C.; resources, C.L.R.; data curation, A.P.; writing—original draft preparation, A.P. and A.V.; writing—review and editing, S.C.; M.P.; G.C.; C.C.; and C.L.R.; visualization, G.C.; supervision, M.P. and C.L.R.; project administration, C.L.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the or Ethics Committee Comitato Etico Catania 1, Azienda Ospedaliero-Universitaria “G. Rodolico-San Marco” Catania, (registration number 163/2022/PO).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
Authors thanks Dr. Emanuela Bartolo for the valuable contribution in the participants recruitment.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mei, Z. , Li, D. The role of probiotics in vaginal health. Front Cell Infect Microbiol. 2022, 12, 963868. [Google Scholar] [CrossRef] [PubMed]
- Cappello, C. , Acin-Albiac, M., Pinto, D., Polo, A., Filannino, P., Rinaldi, F., Gobbetti, M., Di Cagno, R. Do nomadic lactobacilli fit as potential vaginal probiotics? The answer lies in a successful selective multi-step and scoring approach. Microb Cell Fact, 22.
- Shen, X. , Xu, L., Zhang, Z., Yang, Y., Li, P., Ma, T., Guo, S., Kwok, L.Y., Sun, Z. Postbiotic gel relieves clinical symptoms of bacterial vaginitis by regulating the vaginal microbiota. Front Cell Infect Microbiol. 2023, 13, 1114364. [Google Scholar] [CrossRef] [PubMed]
- Pino, A. , Hiippala, K., Ronkainen, A., Vaccalluzzo, A., Caggia, C., Satokari, R., Randazzo, C.L. Adhesion Properties and Pathogen Inhibition of Vaginal-Derived Lactobacilli. Probiotics Antimicrob Proteins. [CrossRef]
- Das, S. , Bhattacharjee, M.J., Mukherjee, A.K., Khan, M.R. Recent advances in understanding of multifaceted changes in the vaginal microenvironment: implications in vaginal health and therapeutics. Crit Rev Microbiol, 49.
- Chee, W.J.Y. , Chew, S.Y., Than, L.T.L. Vaginal microbiota and the potential of Lactobacillus derivatives in maintaining vaginal health. Microb Cell Fact. 2020, 19, 203. [Google Scholar] [CrossRef] [PubMed]
- Tachedjian, G. , Aldunate, M., Bradshaw, C.S., Cone, R.A. The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Res Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Han, Y. , Liu, Z., Chen, T. Role of vaginal microbiota dysbiosis in gynecological diseases and the potential interventions. Front. Microbiol. 2021, 12, 643422. [Google Scholar] [CrossRef] [PubMed]
- Paladine, H.L. , Desai, U.A. Vaginitis: Diagnosis and Treatment. Am Fam Physician, 97.
- Qi, W. , Li, H., Wang, C., Li, H., Zhang, B., Dong, M., Fan, A., Han, C., Xue, F. Recent Advances in Presentation, Diagnosis and Treatment for Mixed Vaginitis. Front Cell Infect Microbiol, 7597; 11. [Google Scholar]
- Zuñiga Vinueza, A.M. Probiotics for the Prevention of Vaginal Infections: A Systematic Review. Cureus. 2024, 16, e64473. [Google Scholar] [CrossRef] [PubMed]
- Abavisani, M. , Sahebi, S., Dadgar, F., Peikfalak, F., Keikha, M. The role of probiotics as adjunct treatment in the prevention and management of gynecological infections: An updated meta-analysis of 35 RCT studies. Taiwan J Obstet Gynecol, 63.
- Stavropoulou, E. , Bezirtzoglou, E. Probiotics in Medicine: A Long Debate. Front Immunol, 2192; 11. [Google Scholar]
- Magalhães, C. , Lima, M., Trieu-Cuot, P., Ferreira, P. To give or not to give antibiotics is not the only question. Lancet Infect Dis. 2021, 21, e191–e201. [Google Scholar] [CrossRef] [PubMed]
- Pino, A. , Vaccalluzzo, A., Caggia, C., Balzaretti, S., Vanella, L., Sorrenti, V., Ronkainen, A., Satokari, R., Randazzo, C.L. Lacticaseibacillus rhamnosus CA15 (DSM 33960) as a Candidate Probiotic Strain for Human Health. Nutrients. 2022, 14, 4902. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, A.M.C. , Pino, A., Grimaldi, R.L., Caggia, C., Randazzo, C.L., Cianci, A. Lacticaseibacillus rhamnosus CA15 (DSM 33960) strain as a new driver in restoring the normal vaginal microbiota: A randomized, double-blind, placebo-controlled clinical trial. Front Surg, 5612. [Google Scholar]
- Hopewell, S. , Chan, A.W., Collins, G.S., Hróbjartsson, A., Moher, D., Schulz, K.F., Tunn, R., Aggarwal, R., Berkwits, M., Berlin, J.A., Bhandari, N., Butcher, N.J., Campbell, M.K., Chidebe, R.C.W., Elbourne, D., Farmer, A., Fergusson, D.A., Golub, R.M., Goodman, S.N., Hoffmann, T.C., Ioannidis, J.P.A., Kahan, B.C., Knowles, R.L., Lamb, S.E., Lewis, S., Loder, E., Offringa, M., Ravaud, P., Richards, D.P., Rockhold, F.W., Schriger, D.L., Siegfried, N.L., Staniszewska, S., Taylor, R.S., Thabane, L., Torgerson, D., Vohra, S., White, I.R., Boutron, I. CONSORT 2025 statement: updated guideline for reporting randomized trials. Nat Med. 1776. [Google Scholar]
- Chan, A.W. , Boutron, I., Hopewell, S., Moher, D., Schulz, K.F., Collins, G.S., Tunn, R., Aggarwal, R., Berkwits, M., Berlin, J.A., Bhandari, N., Butcher, N.J., Campbell, M.K., Chidebe, R.C.W., Elbourne, D.R., Farmer, A.J., Fergusson, D.A., Golub, R.M., Goodman, S.N., Hoffmann, T.C., Ioannidis, J.P.A., Kahan, B.C., Knowles, R.L., Lamb, S.E., Lewis, S., Loder, E., Offringa, M., Ravaud, P., Richards, D.P., Rockhold, F.W., Schriger, D.L., Siegfried, N.L., Staniszewska, S., Taylor, R.S., Thabane, L., Torgerson, D.J., Vohra, S., White, I.R., Hróbjartsson, A. SPIRIT 2025 statement: updated guideline for protocols of randomized trials. Nat Med, 1784; 31. [Google Scholar]
- Amsel, R. , Totten, P.A., Spiegel, C.A., Chen, K.C., Eschenbach, D., Holmes, K.K. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med. 1983, 74, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Nugent, R.P. , Krohn, M.A., Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G. Definition and classification of abnormal vaginal flora. Best Pract Res Clin Obstet Gynaecol. 2007, 21, 355–73. [Google Scholar] [CrossRef] [PubMed]
- Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. 1998, 28, 551–8. [Google Scholar]
- Sobel, J.D. , Vempati, Y.S. Bacterial Vaginosis and Vulvovaginal Candidiasis Pathophysiologic Interrelationship. Microorganisms. 2024, 12, 108. [Google Scholar] [CrossRef] [PubMed]
- López-Moreno, A. , Aguilera, M. Vaginal Probiotics for Reproductive Health and Related Dysbiosis: Systematic Review and Meta-Analysis. J Clin Med. 2021, 10, 1461. 10, 1461.
- Liu, P. , Lu, Y., Li, R., Chen, X. Use of probiotic lactobacilli in the treatment of vaginal infections: In vitro and in vivo investigations. Front Cell Infect Microbiol, 1153; 13. [Google Scholar]
- Takada, K. , Melnikov, V.G., Kobayashi, R., Komine-Aizawa, S., Tsuji, N.M., Hayakawa, S. Female reproductive tract-organ axes. Front Immunol, 1110; 14. [Google Scholar]
- McDonald, B.D. , Jabri, B., Bendelac, A. Diverse developmental pathways of intestinal intraepithelial lymphocytes. Nat Rev Immunol. 2018, 18, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Salazar, A.M. , Neugent, M.L., De Nisco, N.J., Mysorekar, I.U. Gut-bladder axis enters the stage: Implication for recurrent urinary tract infections. Cell Host Microbe, 1066; 30. [Google Scholar]
- Xiao, B. , A, D. , Qin, H., Mi, L., & Zhang, D. Correlation analysis of vaginal microbiome changes and bacterial vaginosis plus vulvovaginal candidiasis mixed vaginitis prognosis. Front. Cell. Infect. Microbiol. 2022, 2022. 12, 860589. [Google Scholar]
- Vaccalluzzo, A. , Pino, A., Grimaldi, R.L., Caggia, C., Cianci, S., Randazzo, C.L. Lacticaseibacillus rhamnosus TOM 22.8 (DSM 33500) is an effective strategy for managing vaginal dysbiosis, rising the lactobacilli population. J Appl Microbiol. 2024, 135, lxae110. [Google Scholar] [CrossRef] [PubMed]
- Pino, A. , Rapisarda, A.M.C., Vaccalluzzo, A., Sanfilippo, R.R., Coman, M.M., Grimaldi, R.L., Caggia, C., Randazzo, C.L., Russo, N., Panella, M.M., Cianci, A., Verdenelli, M.C. Oral Intake of the Commercial Probiotic Blend Synbio® for the Management of Vaginal Dysbiosis. J Clin Med.
- Chen, C. , Hao, L., Zhang, Z., Tian, L., Zhang, X., Zhu, J., Jie, Z., Tong, X., Xiao, L., Zhang, T., Jin, X., Xu, X., Yang, H., Wang, J., Kristiansen, K., Jia, H. Cervicovaginal microbiome dynamics after taking oral probiotics. J Genet Genomics. 2021, 48, 716–726. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. , Lyu, J., Ge, L., Huang, L,. Peng, Z., Liang, Y., Zhang, X., Fan, S. Probiotic Lacticaseibacillus rhamnosus GR-1 and Limosilactobacillus reuteri RC-14 as an Adjunctive Treatment for Bacterial Vaginosis Do Not Increase the Cure Rate in a Chinese Cohort: A Prospective, Parallel-Group, Randomized, Controlled Study. Front Cell Infect Microbiol.
- Husain, S. , Allotey, J., Drymoussi, Z., Wilks, M., Fernandez-Felix, B.M., Whiley, A., Dodds, J., Thangaratinam, S., McCourt, C., Prosdocimi, E.M., Wade, W.G., de Tejada, B.M., Zamora, J., Khan, K., Millar, M. Effects of oral probiotic supplements on vaginal microbiota during pregnancy: a randomised, double-blind, placebo-controlled trial with microbiome analysis. BJOG.
- Yang, S. , Reid, G., Challis, J.R.G., Gloor, G.B., Asztalos, E., Money, D., Seney, S., Bocking, A.D. Effect of Oral Probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 on the Vaginal Microbiota, Cytokines and Chemokines in Pregnant Women. Nutrients.
- Anukam, K. , Osazuwa, E., Ahonkhai, I., Ngwu, M., Osemene, G., Bruce, A.W., Reid, G. Augmentation of antimicrobial metronidazole therapy of bacterial vaginosis with oral probiotic Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14: randomized, double-blind, placebo controlled trial. Microbes Infect.
- Martinez, R.C. , Franceschini, S.A., Patta, M.C., Quintana, S.M., Gomes, B.C., De Martinis, E.C., Reid, G. Improved cure of bacterial vaginosis with single dose of tinidazole (2 g), Lactobacillus rhamnosus GR-1, and Lactobacillus reuteri RC-14: a randomized, double-blind, placebo-controlled trial. Can J Microbiol.
- De Alberti, D. , Russo, R., Terruzzi, F., Nobile, V., Ouwehand, A.C. Lactobacilli vaginal colonisation after oral consumption of Respecta(®) complex: a randomised controlled pilot study. Arch Gynecol Obstet.
- Russo, R. , Edu, A., De Seta, F. Study on the effects of an oral lactobacilli and lactoferrin complex in women with intermediate vaginal microbiota. Arch Gynecol Obstet. 2018, 298, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Russo, R. , Superti, F., Karadja, E., De Seta, F. Randomised clinical trial in women with Recurrent Vulvovaginal Candidiasis: Efficacy of probiotics and lactoferrin as maintenance treatment. Mycoses, 62.
- Russo, R. , Karadja, E., De Seta, F. Evidence-based mixture containing Lactobacillus strains and lactoferrin to prevent recurrent bacterial vaginosis: a double blind, placebo controlled, randomised clinical trial. Benef Microbes, 10.
- Lyra, A. , Ala-Jaakkola, R., Yeung, N., Datta, N., Evans, K., Hibberd, A., Lehtinen, M.J., Forssten, S.D., Ibarra, A., Pesonen, T., Junnila, J., Ouwehand, A.C., Baranowski, K., Maukonen, J., Crawford, G., Lehtoranta, L. A Healthy Vaginal Microbiota Remains Stable during Oral Probiotic Supplementation: A Randomised Controlled Trial. Microorganisms, 11.
- Chapple, A. Vaginal thrush: perceptions and experiences of women of south Asian descent. Health Educ Res. 2001, 16, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Aballéa, S. , Guelfucci, F., Wagner, J., Khemiri, A., Dietz, J.P., Sobel, J., Toumi, M. Subjective health status and health-related quality of life among women with Recurrent Vulvovaginal Candidosis (RVVC) in Europe and the USA. Health Qual Life Outcomes.
- Zhu, Y.X. , Li, T., Fan, S.R., Liu, X.P., Liang, Y.H., Liu, P. Health-related quality of life as measured with the Short-Form 36 (SF-36) questionnaire in patients with recurrent vulvovaginal candidiasis. Health Qual Life Outcomes. 2016, 14, 65. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Y. , Lee, A., Fischer, G. Quality of life in patients with chronic vulvovaginal candidiasis: A before and after study on the impact of oral fluconazole therapy. Australas J Dermatol, 58.
- Thomas-White, K. , Navarro, P., Wever, F., King, L., Dillard, L.R., Krapf, J. Psychosocial impact of recurrent urogenital infections: a review. Womens Health, 2023; 19. [Google Scholar]
- Ang, X.Y. , Chung, F.Y., Lee, B.K., Azhar, S.N.A., Sany, S., Roslan, N.S., Ahmad, N., Yusof, S.M., Abdullah, N., Nik Ab Rahman, N.N., Abdul Wahid, N., Deris, Z.Z., Oon, C.E., Wan Adnan, W.F., Liong, M.T. Lactobacilli reduce recurrences of vaginal candidiasis in pregnant women: a randomized, double-blind, placebo-controlled study. J Appl Microbiol, 3168. [Google Scholar]
Figure 1.
CONSORT flow diagram of the study.
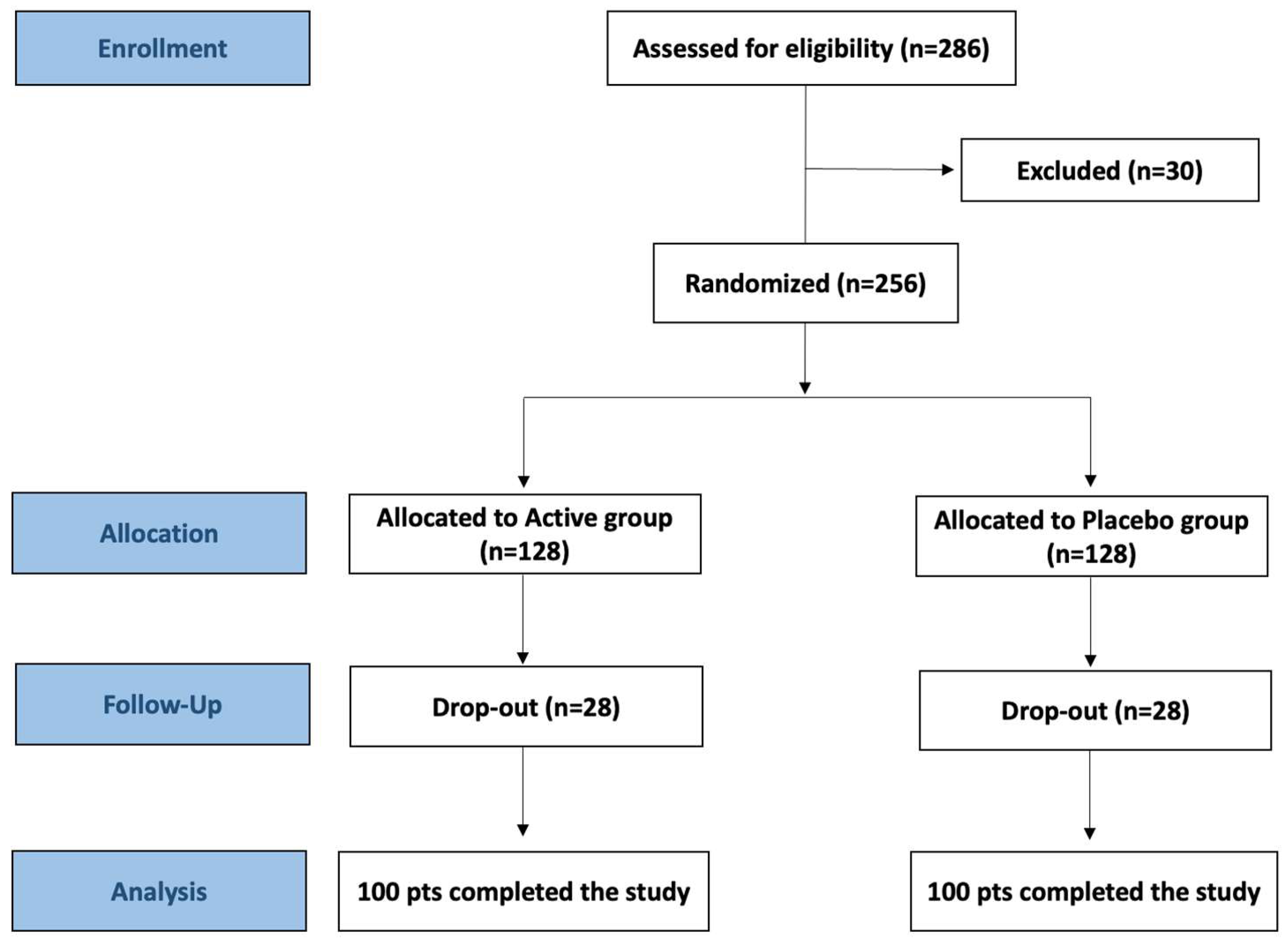
Figure 2.
Average changes in clinical signs and symptoms in both Active and Placebo groups. Intra-group comparisons (T1 vs T0) and inter-group comparisons at T1 (Panel A); Intra-group comparisons (T0 vs T2) and inter-group comparisons at T2 (Panel B); Intra-group comparisons (T2 vs T1) (Panel C). All inter-group comparisons were performed after baseline (T0) normalization. Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** = p ≤ 0.01, *** = p ≤ 0.001.
Figure 2.
Average changes in clinical signs and symptoms in both Active and Placebo groups. Intra-group comparisons (T1 vs T0) and inter-group comparisons at T1 (Panel A); Intra-group comparisons (T0 vs T2) and inter-group comparisons at T2 (Panel B); Intra-group comparisons (T2 vs T1) (Panel C). All inter-group comparisons were performed after baseline (T0) normalization. Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** = p ≤ 0.01, *** = p ≤ 0.001.
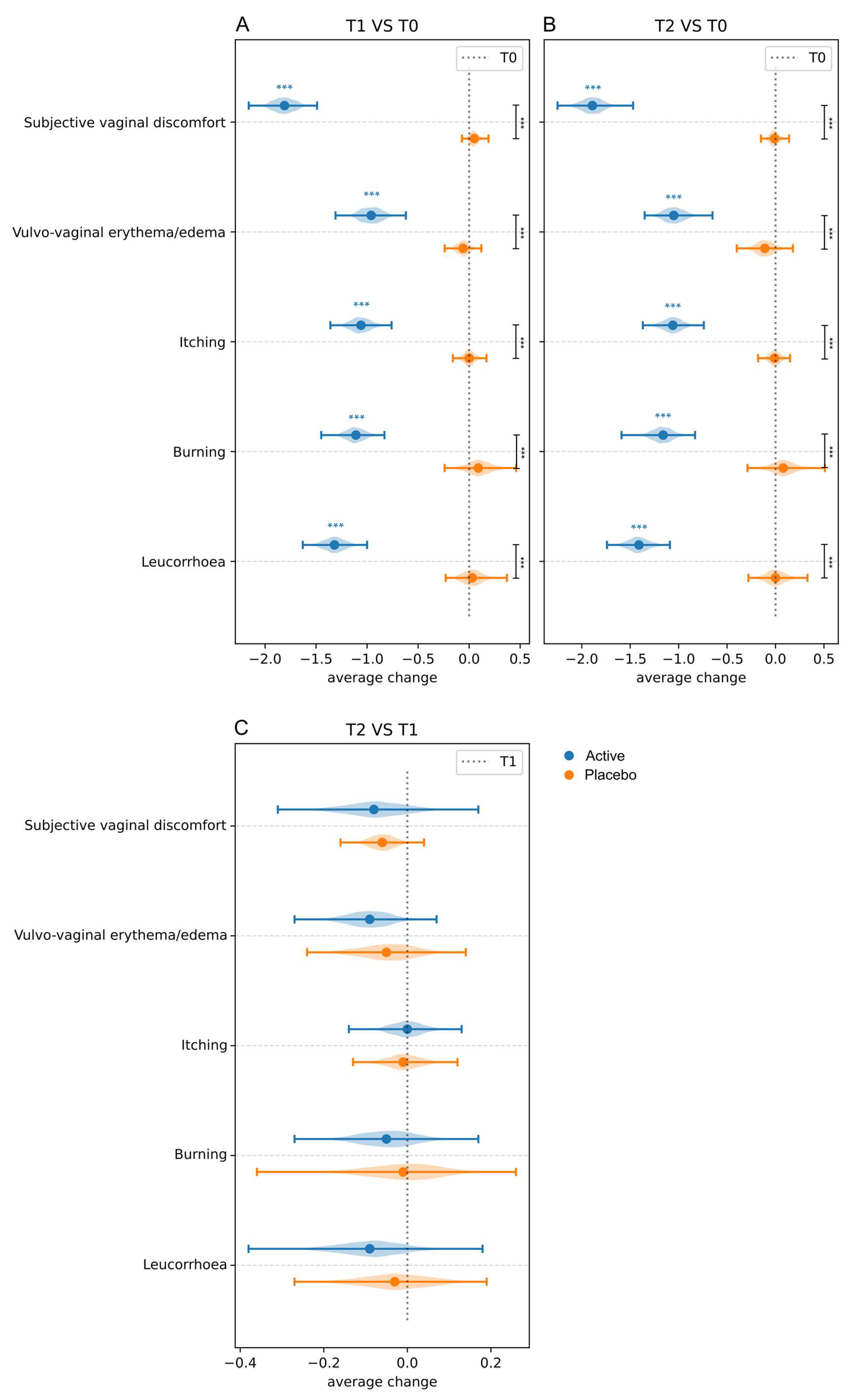
Figure 3.
Amsel criteria evaluated in both Active and Placebo groups at baseline (T0), 10 days (T1), and 30 days (T2) after the end of the treatment. Data are reported as average frequency. Intra-group comparison and inter-group comparisons, after baseline (T0) normalization, are displayed. * = p ≤ 0.05, ** = p ≤ 0.01, *** = p ≤ 0.001.
Figure 3.
Amsel criteria evaluated in both Active and Placebo groups at baseline (T0), 10 days (T1), and 30 days (T2) after the end of the treatment. Data are reported as average frequency. Intra-group comparison and inter-group comparisons, after baseline (T0) normalization, are displayed. * = p ≤ 0.05, ** = p ≤ 0.01, *** = p ≤ 0.001.
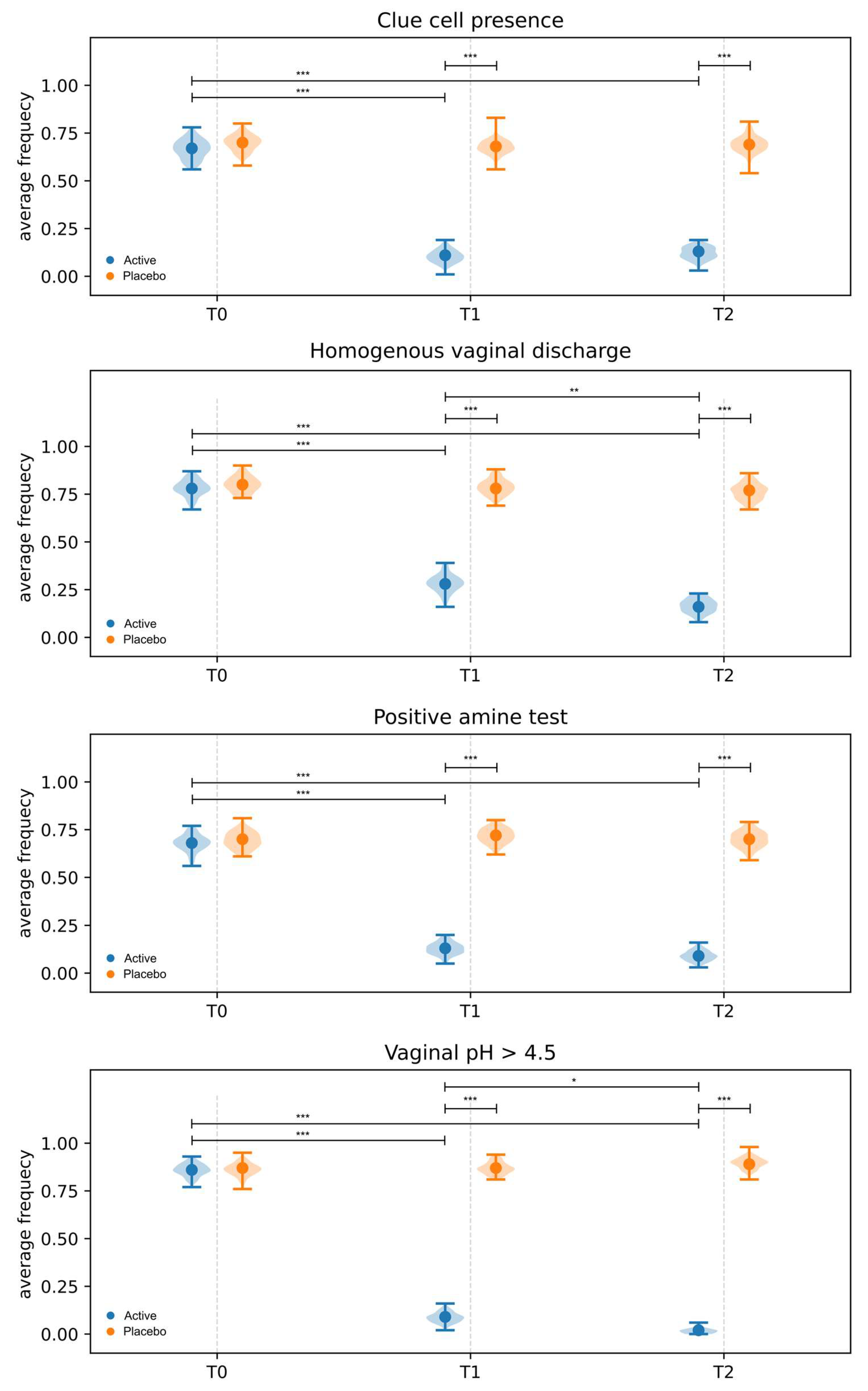
Figure 4.
Intra-group and inter-group comparison of Nugent score. Data are reported as average change. Intra-group comparison (T0 vs T1) and inter-group comparisons at T1 (Panel A); Intra-group comparisons (T0 vs T2) and inter-group comparisons at T2 (Panel B); Intra-group comparisons (T2 vs T1) (Panel C). Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** =p ≤ 0.01, *** = p ≤ 0.001.
Figure 4.
Intra-group and inter-group comparison of Nugent score. Data are reported as average change. Intra-group comparison (T0 vs T1) and inter-group comparisons at T1 (Panel A); Intra-group comparisons (T0 vs T2) and inter-group comparisons at T2 (Panel B); Intra-group comparisons (T2 vs T1) (Panel C). Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** =p ≤ 0.01, *** = p ≤ 0.001.
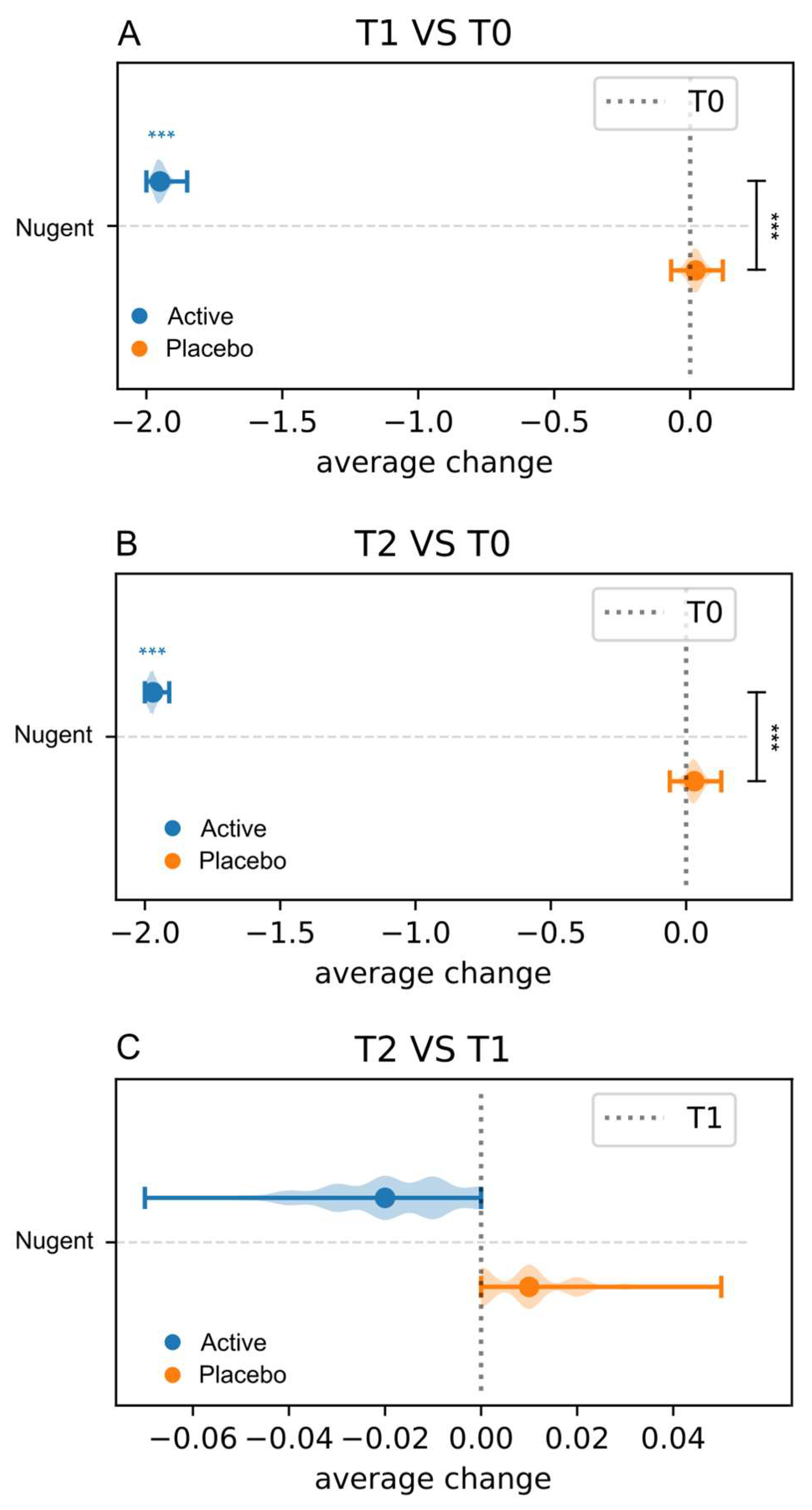
Figure 5.
Intra-group and inter-group comparison of LBG data. Data are reported as average change. Intra-group comparisons (T0 vs T1) and inter-group comparisons at T1 (Panel A); Intra-group comparisons (T0 vs T2) and inter-group comparisons at T2 (Panel B); Intra-group comparisons (T2 vs T1) (Panel C). Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** =p ≤ 0.01, *** = p ≤ 0.001.
Figure 5.
Intra-group and inter-group comparison of LBG data. Data are reported as average change. Intra-group comparisons (T0 vs T1) and inter-group comparisons at T1 (Panel A); Intra-group comparisons (T0 vs T2) and inter-group comparisons at T2 (Panel B); Intra-group comparisons (T2 vs T1) (Panel C). Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** =p ≤ 0.01, *** = p ≤ 0.001.
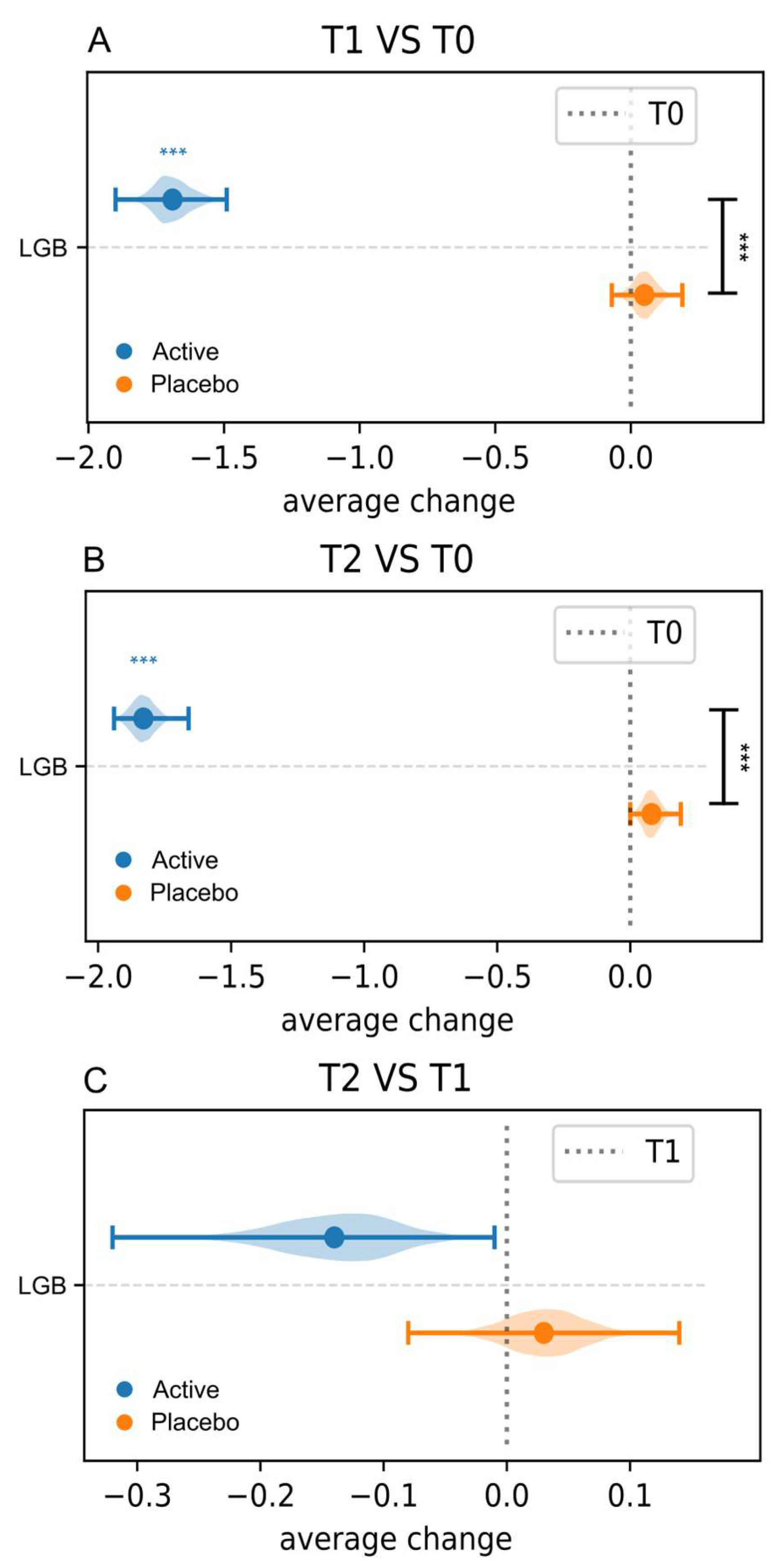
Figure 6.
Intra-group and inter-group comparison of physical health, psychological health, social relations, and environment domains of the quality of life. Data are reported as average change. Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p≤0.05, ** =p≤ 0.01, *** = p≤ 0.001.
Figure 6.
Intra-group and inter-group comparison of physical health, psychological health, social relations, and environment domains of the quality of life. Data are reported as average change. Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p≤0.05, ** =p≤ 0.01, *** = p≤ 0.001.
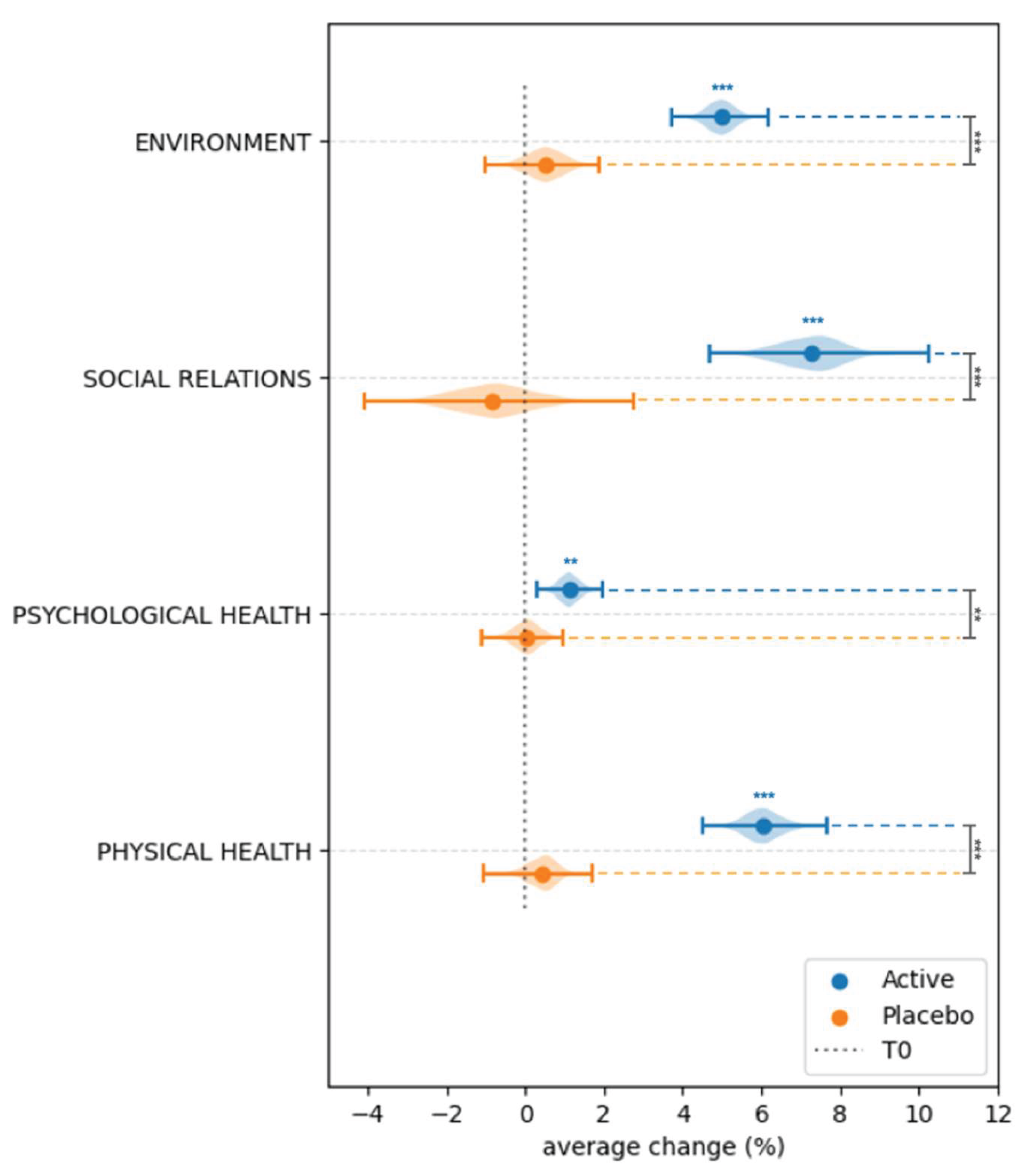
Figure 7.
Intra-group and inter-group comparison of general health and overall quality of life domains of the quality of life. Data are reported as average change. Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** = p ≤ 0.01, *** = p ≤ 0.001.
Figure 7.
Intra-group and inter-group comparison of general health and overall quality of life domains of the quality of life. Data are reported as average change. Blue and black stars are related to intra- and inter-group comparisons, respectively. * = p ≤ 0.05, ** = p ≤ 0.01, *** = p ≤ 0.001.
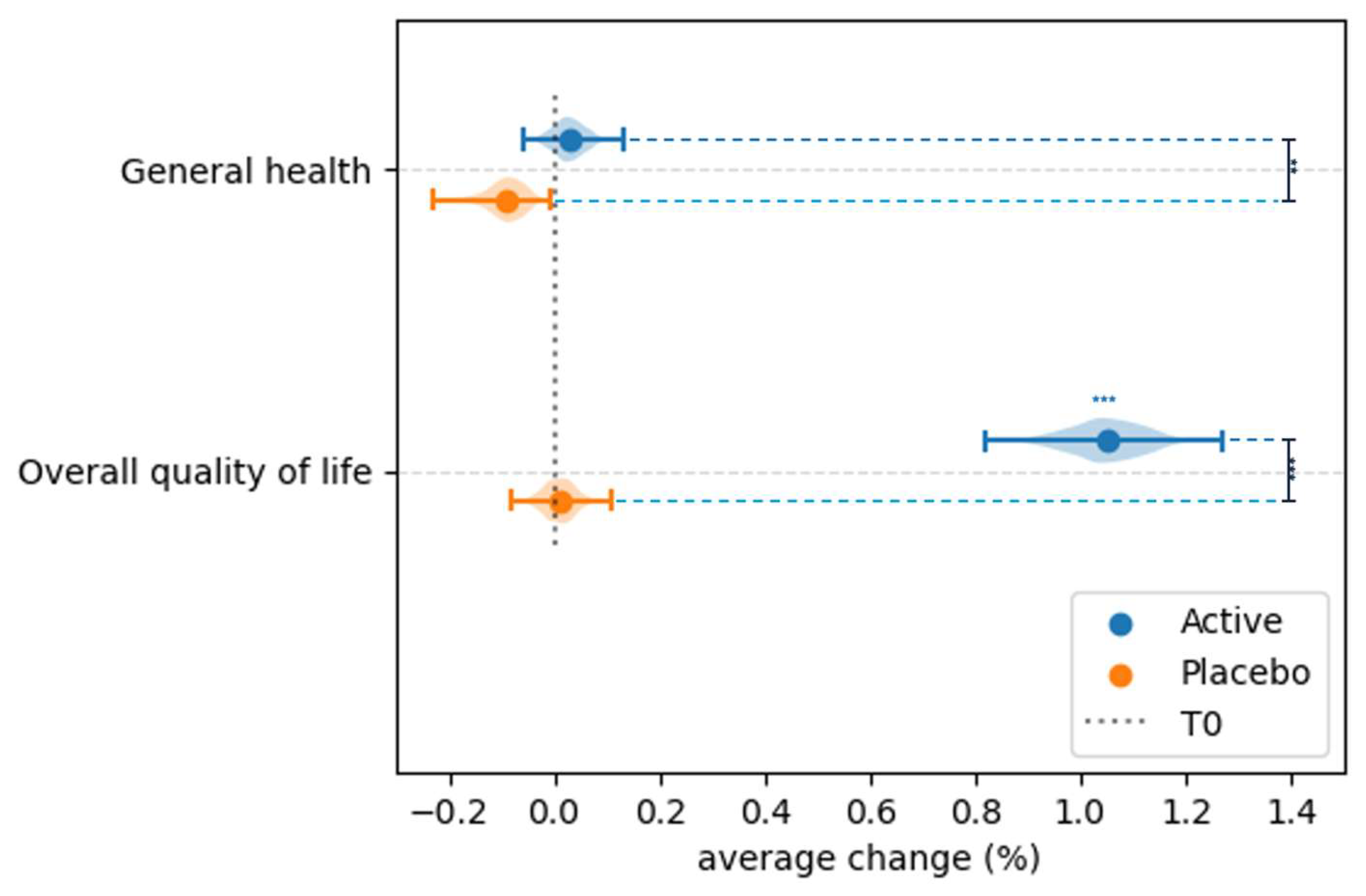

Table 1.
Inclusion and exclusion criteria.
| Inclusion criteria |
| Fertile age (18-45 years); regular menstruation; presence of BV (at least 3 Amsel criteria; Nugent score ≥7); co-occurring of AV (diagnosed based on the Donders’ score) and VVC (clinical picture and yeast culture); presence of at least one vaginal symptom (leucorrhea, burning, itching, erythema/oedema or subjective vaginal discomfort); no participation in other clinical studies; consent to participate; willingness to collaborate in completing the study procedures, non-lactating status, appropriate personal hygiene, the cognitive ability for collaboration. |
| Exclusion Criteria |
| Presence of sexually transmitted disease due to Chlamydia, Neisseria gonorrhoeae or Trichomonas vaginalis; presence of specific vaginitis related to acute AV and VVC; clinically apparent herpes simplex infection; precancerous lesions due to Human papillomavirus; human immunodeficiency virus infection; confirmed diagnosis of pelvic inflammatory disease (PID); recent use of antibiotic and/or antifungal drugs (less than one month); recent consumption of probiotics or food containing probiotics; recent use of immunosuppressive drugs (less than one month); pregnancy or breastfeeding; use of douching; hypersensitivity or allergy to any ingredient of investigational product or placebo; chronic diseases; neoplastic disease; diabetes; genital tract bleeding. |
Table 2.
Baseline demographic characteristics of recruited subjects allocated to Active and Placebo groups.
Table 2.
Baseline demographic characteristics of recruited subjects allocated to Active and Placebo groups.
| Demographic characteristics | Active group (n=100) | Placebo group (n=100) | p-value |
|---|---|---|---|
| Age | 32.58 ± 5.74 | 32.13 ± 6.52 | 0.7727 |
| Body mass index | |||
| <18.5 | 4 | 5 | 0.7369 |
| 18.5 – 24.9 | 81 | 81 | |
| 25 – 29.9 | 8 | 8 | |
| ≥ 30 | 7 | 6 | |
| Smoking habits | 24 | 22 | 0.8667 |
| Contraceptive use | |||
| Oral | 12 | 15 | 0.6796 |
| Barrier | 28 | 30 | 0.8762 |
| Others | 36 | 34 | 0.8822 |
| History of vaginal dysbiosis | 61 | 58 | 0.7733 |
| Sexual activity | 68 | 71 | 0.7588 |
Data related to age are presented as means ± SD. All the other characteristics are reported as number of patients. Statistical significance between Active and Placebo groups was set at p < 0.05.
Table 3.
Baseline clinical characteristics of recruited subjects allocated to Active and Placebo groups.
Table 3.
Baseline clinical characteristics of recruited subjects allocated to Active and Placebo groups.
| Clinical characteristics | Active group (n=100) | Placebo group (n=100) | p-value | |
|---|---|---|---|---|
| Signs and symptoms | Leucorrhoea | 95 | 97 | 0.7209 |
| Burning | 92 | 89 | 0.6306 | |
| Itching | 79 | 82 | 0.7214 | |
| Vulvovaginal Erythema/Oedema | 90 | 88 | 0.8217 | |
| Subjective vaginal discomfort | 95 | 97 | 0.7209 | |
| Amsel Criteria | Homogenous vaginal discharge | 78 | 80 | 0.8623 |
| Clue cell presence | 67 | 70 | 0.7609 | |
| Positive amine test | 68 | 70 | 0.8785 | |
| Vaginal pH > 4.5 | 86 | 87 | 1.0000 | |
| Nugent score | 0–3 | 0 | 0 | 0.4738 |
| 4–6 | 3 | 5 | ||
| 7–10 | 97 | 95 | ||
| Lactobacillary grade | I | 0 | 0 | 0.4719 |
| II | 8 | 11 | ||
| III | 92 | 89 | ||
Data are reported as number of patients. Statistical significance between Active and Placebo groups was set at p < 0.05.
Table 4.
Vaginal microbiota composition at baseline (T0), 10 days (T1) and 30 days (T2) after the end of the treatment evaluated by plate count.
Table 4.
Vaginal microbiota composition at baseline (T0), 10 days (T1) and 30 days (T2) after the end of the treatment evaluated by plate count.
| Microbial groups | Active group (n=100) | Placebo group (n=100) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 |
p-value T0vsT1 |
p-value T0vsT2 |
p-value T1vsT2 |
T0 | T1 | T2 |
p-value T0vsT1 |
p-value T0vsT2 |
p-value T1vsT2 |
|
| Lactobacillus spp. | 3.49 ± 0.08 | 7.19 ± 0.71 | 7.21 ± 0.76 | 3.89 x 10-18* | 3.89 x 10-18* | 0.0033* | 3.51 ± 0.12 | 3.52 ± 0.14 | 3.53 ± 0.34 | 0.1760 | 0.0039* | 0.0216* |
| Enterococcus spp. | 4.93 ± 0.57 | 2.17 ± 0.99 | 2.14 ± 0.86 | 3.89 x 10-18* | 3.89 x 10-18* | 0.0026* | 4.90 ± 0.59 | 4.99 ± 0.57 | 4.98 ± 0.58 | 0.0001* | 0.0000* | 0.7258 |
| Staphylococcus spp. | 3.70 ± 0.36 | 1.83 ± 0.22 | 1.76 ± 0.24 | 3.89 x 10-18* | 3.89 x 10-18* | 0.0023* | 3.69 ± 0.29 | 3.78 ± 0.32 | 3.79 ± 0.33 | 0.0000* | 0.0000* | 0.0237* |
| Gardnerella spp. | 4.41 ± 0.50 | 1.93 ± 0.47 | 1.92 ± 0.21 | 3.89 x 10-18* | 3.89 x 10-18* | 0.0005* | 4.43 ± 0.44 | 4.53 ± 0.36 | 4.44 ± 0.43 | 0.0007* | 0.9014 | 0.0098* |
| Candida spp. | 3.83 ± 0.29 | 1.32 ± 0.81 | 1.34 ± 0.78 | 3.89 x 10-18* | 3.89 x 10-18* | 0.6996 | 3.87 ± 0.42 | 3.95 ± 0.41 | 3.92 ± 0.43 | 0.0006* | 0.0510 | 0.8231 |
| Escherichia coli | 4.02 ± 0.68 | 1.11 ± 0.82 | 1.09 ± 0.81 | 3.89 x 10-18* | 3.89 x 10-18* | 0.1492 | 4.17 ± 0.48 | 4.05 ± 0.52 | 4.11 ± 0.54 | 0.0000* | 0.0890 | 0.0078* |
Data are shown as mean log10 cfu/ml and standard deviation. *Intra-group statistical significance, at p<0.05, based on Wilcoxon Signed-Rank Test.
Table 5.
Inter-group differences, at T1 and T2 sampling times, evaluated by Analysis of Covariance (ANCOVA) after baseline (T0) normalization, related to the composition of the vaginal microbiota composition.
Table 5.
Inter-group differences, at T1 and T2 sampling times, evaluated by Analysis of Covariance (ANCOVA) after baseline (T0) normalization, related to the composition of the vaginal microbiota composition.
| Microbial groups | Sampling time | ANCOVA | |
|---|---|---|---|
| Effect† | p-value | ||
| Lactobacillus spp. | T1 | 3.6978 | 6.23 x 10-117* |
| T2 | 3.6905 | 8.40 x 10-105* | |
| Enterococcus spp. | T1 | -2.8436 | 1.87 x 10-72* |
| T2 | -2.8546 | 5.31 x 10-78* | |
| Staphylococcus spp. | T1 | -1.9538 | 6.66 x 10-118* |
| T2 | -2.0379 | 4.44 x 10-118* | |
| Gardnerella spp. | T1 | -2.5927 | 1.09 x 10-116* |
| T2 | -2.5226 | 5.11 x 10-123* | |
| Candida spp. | T1 | -2.6082 | 1.58 x 10-75* |
| T2 | -2.5624 | 2.95 x 10-74* | |
| Escherichia coli | T1 | -2.8240 | 8.47 x 10-95* |
| T2 | -2.9056 | 9.29 x 10-93* | |
†Effect of the treatment on microbiota composition changes, after baseline normalization; *Statistical significance at p<0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



