
Submitted:
25 September 2025
Posted:
26 September 2025
You are already at the latest version
Abstract
Background/Objectives: With increasing survival rates in pediatric oncology, late effects such as therapy-induced infertility are becoming more relevant. This study evaluated the management of fertility preservation in children and adolescents with cancer at the Medical University Innsbruck between 2000 and 2018. Methods: In this retrospective monocentric study, 552 patients (0–17 years) receiving chemotherapy were analyzed. Data was extracted from the Clinical Information System and the cryopreservation database. The assessed main variables included pubertal status, sex hormone levels and use of fertility preservation methods. Results: Fertility preservation was documented in 6.5% of patients, more frequently in males (8.9%) than females (3.2%). Sperm cryopreservation was performed in 28 males, ovarian tissue cryopreservation in six females and oocyte cryopreservation in three. Pubertal status at diagnosis was recorded in 4.9% of patients, and hormone levels in 29.7%. Conclusions: The findings highlight significant gaps in systematic fertility preservation, particularly in female patients. Consistent assessment of pubertal and hormonal parameters at diagnosis is essential to inform decision-making. Standardized procedures and closer interdisciplinary collaboration are needed to ensure equitable access to fertility preservation and safeguard long-term quality of life.
Keywords:
childhood cancer survivors
; gonadotoxicity
; cryopreservation
; survivorship
; infertility
; FertiProtekt
1. Introduction
With the increasing number of childhood cancer survivors (CCS), minimizing late effects and improving quality of life (QoL) have become increasingly important. In addition to physical limitations such as organ dysfunction, endocrine deficits, sterility/infertility, or psychosocial stressors also occur [1,2,3,4]. For survivors, fertility impairment is considered one of the most relevant long-term effects, the assessment of which is complicated by heterogeneous study populations and the frequent lack of long-term contact with oncologists [5].
In males, fertility disorders primarily arise from damage to spermatogenesis or the hypothalamic-pituitary-gonadal (HPG) axis. Hypogonadism and erectile dysfunction are other possible consequences [6,7,8]. Studies show a significantly increased risk of infertility in male CCS [9,10]. In women, the loss of primordial follicles, uterine damage, HPG disorders, and vaginal strictures can cause infertility resulting from chemotherapy or irradiation [11,12]. Female CCS have a lower pregnancy rate compared to the general population, mainly due to the development of premature ovarian insufficiency (POI) [13,14,15].
Rendtorff et al. reported that around one-third of CCS experience fertility limitations, although the desire to have children remains comparable to that of the general population [16]. Abortions are less common in CCS, which underscores the importance of the desire to have children [17].
The degree of fertility impairment depends on the type and dose of therapy, underlying disease, gender, and pubertal status. Chemotherapeutic agents, especially alkylating agents and platinum compounds are considered gonadotoxic and can cause long-term fertility impairment [18,19,20]. Men show dose-dependent disorders of spermatogenesis, including azoospermia, while women show a decrease in follicular reserve and an increased risk of POI [21,22,23,24]. Platinum compounds, especially cisplatin, also affect fertility in both sexes, although the data is heterogeneous [25,26,27,28].
Radiotherapy can impair fertility both through direct gonadal damage and through central effects on the HPG axis. Pelvic and whole-body irradiation in particular increase the risk of ovarian insufficiency, uterine dysfunction, or damage to spermatogenesis [10,14,16,28,29,30,31]. The results for cranial irradiation are contradictory, especially in male CCS [10,14,16,32,33].
Puberty status influences vulnerability to gonadotoxic therapies. Prepubertal children appear to be more resistant to certain chemotherapies, while postpubertal patients show a higher risk of fertility disorders [16,28,34].
Since there is no safe threshold above which infertility occurs after cancer therapy, all patients should be informed about the risks and offered fertility protection options depending on their gender, age, underlying disease, and therapy [35].
The options for fertility preservation in prepubertal boys are limited. In addition to testicular shielding during radiotherapy, testicular tissue cryopreservation (TTC) is being tested experimentally. Successful sperm maturation from stem cells has not yet been achieved in humans but is already possible in animal models [36,37,38].
Once spermarche has occurred, sperm cryopreservation (SC) can usually be performed in post-pubertal boys. Alternatively in rare cases, penile vibratory stimulation (PVS), electrostimulation, or testicular sperm extraction (TESE) can also be used if necessary [35,39,40]. It is important to obtain sperm before starting therapy, as sperm quality declines after therapy begins. Hormonal protective measures are not effective and are not recommended by professional societies [35,40].
The most promising option for prepubertal girls is ovarian tissue cryopreservation (OTC), which has already enabled puberty induction and live births after re-transplantation [41,42,43], although the risk of malignant cell contamination must be considered. Ovarian transposition or gonadal shielding may also be considered [35,44,45,46].
In addition, oocyte cryopreservation (OC) after controlled ovarian hyperstimulation (COH) and the use of gonadotropin-releasing hormone agonists (GnRHa) are established procedures in post-pubertal girls. OC achieves pregnancy rates of up to 50% in young women [47,48], but requires almost two weeks of preparation time. OTC is increasingly considered a standard procedure, although its invasiveness and higher resource requirements should be taken into account [40]. The administration of GnRHa is contradictory, but can be offered as a complementary option [35,40,49,50].
This study aimed to evaluate the current approach to fertility preservation for pediatric cancer patients at the Department of Pediatrics in Innsbruck between 2000 and 2018. The focus was on documenting the services offered and how they were implemented prior to the start of therapy, analyzing existing practices and identifying potential care gaps, with the aim of improving education about the long-term effects of gonadotoxicity.
2. Materials and Methods
This retrospective, monocentric study included 552 pediatric patients (305 male, 247 female) aged 0–17 years, treated for oncological diseases at the Department of Pediatrics I, Medical University of Innsbruck, between 2000 and 2018. All oncological patients receiving chemotherapy were included; those without such treatment or with incomplete records were excluded. The study period was limited to 2000–2018 to allow the use of an existing, comprehensive dataset of pediatric oncology patients who received chemotherapy, which served as the foundation for the systematic collection and analysis of additional clinical information by the authors. Data was collected from the Clinical Information System and the cryopreservation database. The data was pseudonymized via consecutive study numbers.
The parameters included demographics, diagnosis, treatment details, pubertal stage, hormone levels (FSH, AMH, estradiol, testosterone), menarche and spermarche age, and fertility preservation measures (SC, OTC, OC). Descriptive statistics were applied using IBM SPSS Statistics 26 and Microsoft Excel 365.
The study was approved by the local Ethics Committee of the Medical University of Innsbruck (1374/2023). The corresponding author will provide data upon reasonable request.
3. Results
3.1. Study population
From 2000 to 2018, a total of 552 pediatric patients (305 males [55.3%], 247 females [44.7%]) aged 0–17 years received chemotherapy for oncological diseases at the Department of Pediatrics I, Medical University of Innsbruck. At the time of data collection, 20.1% of patients were deceased. The most frequent diagnosis was acute lymphoblastic leukemia (ALL, n= 199), followed by extracranial solid tumors (n= 166, mainly neuroblastoma, Ewing sarcoma, osteosarcoma, rhabdomyosarcoma and Wilms tumor), central nervous system (CNS) tumors (n= 63), non-Hodgkin lymphoma (NHL, n= 37), acute myeloid leukemia (AML, n= 35), Hodgkin lymphoma (n= 32), and rare pediatric tumors (n= 20). At least one recurrence occurred in 22.5% of patients, and 29.3% received radiotherapy, including cranial (n= 57) and extracranial (n= 105) irradiation (see Table 1).
The median age at diagnosis was 6 years (IQR = 2-12). The highest frequency of diagnoses was observed in children aged 0–4 years (n = 240, 43.5%). The mean number of new oncological diagnoses that met the inclusion criteria was 29 per year (range: 16–38). Extracranial solid tumors, AML, CNS tumors and rare pediatric malignancies peaked in infancy and early childhood, while the incidence of ALL was highest between ages 2 and 4. NHL manifested at a consistent frequency across all age groups, while Hodgkin lymphoma was rarely diagnosed before the age of 10 and its incidence increased thereafter.
3.2. Indicators of puberty
The pubertal stage was documented in 27 patients (4.9%). Among the girls (n = 9), the development of breast and pubic hair was documented. The age or date of menarche was recorded in n = 44 patients. In 10 out of these girls, menarche occurred before the date of initial diagnosis. An evaluation of testicular development and pubic hair was conducted among a total of n = 18 males. The age of the patients, for whom puberty indicators were noted, ranged from 5 to 17 years (M = 11.7). Hormone levels were measured in 164 patients (29.7%), including FSH, estradiol, AMH, and testosterone. Evidence of hormonal activation consistent with puberty was observed in 30.6% of females and 20.2% of males, where sex hormones were documented (see Table 2).
3.3. Fertility preservation
The analysis revealed that fertility-preserving interventions were performed in 6.5% of all included patients (n= 36). Among patients aged ≥12 years, 25.4 % (36/142) received a fertility-preserving measure, with higher rates in males (31.8 %) than females (14.8 %). In the male subject group, 27 underwent sperm cryopreservation by masturbation, while one boy underwent TESE. Among the females, 6 underwent ovarian tissue cryopreservation, while 3 underwent oocyte cryopreservation. In one case, both OTC and OC were performed in the same patient (see Table 3).
The mean age at fertility preservation was 15.7 years for males (range 13–17) and 14.8 years for females (range 12–17). The proportion of interventions increased with age, reaching 50% among 17-year-old patients, with a male-to-female ratio of 10:1 (see Figure 1). No procedures were performed in patients under 12 years.
The highest frequency of interventions was observed in patients with extracranial solid tumors (n= 14, mainly Ewing sarcoma and osteosarcoma) and ALL (n= 8). Fertility preservation procedures were initiated in 2006, with a single exception in 2001. The mean number of interventions per year since 2006 was 2.4, with a maximum of five recorded in 2011 (see Figure 2).
4. Discussion
This monocentric, retrospective study assessed fertility preservation practices in pediatric oncology patients treated in Innsbruck between 2000 and 2018. The documentation of puberty status, hormone levels, and reproductive milestones (menarche and sperm-arche) was inconsistent, particularly in the early study period. This finding suggests that there was historically limited awareness of fertility risks. The analysis revealed that 6.5% of patients underwent fertility-preserving procedures, with a significantly higher uptake among males (8.9%) compared to females (3.2%). Among patients aged ≥12 years, 25.4% received such interventions, a proportion that was again higher among male patients (31.8%) than among female patients (14.8%). This gender imbalance is consistent with reports from other European centers, where SC is more accessible and logistically feasible than OCT or OC [51,52]. The invasiveness, prolonged preparation time, and elevated resource requirements (including specialized staff, facilities, and associated costs) of female procedures are likely to explain the observed differences. It must be noted that these interventions are not covered by public insurance in Austria. Consequently, the financial burden of these treatments therefore falls on the families of patients, which may further impact the number of patients undergoing preservation interventions. Furthermore, most diagnoses, particularly ALL and AML, require immediate treatment, often started within hours of diagnosis, making any delay for fertility preservation procedures challenging. At present, the safety and practicality of such procedures remain uncertain, as leukemic cells may infiltrate vital organs, including the ovaries and testes.
International data on fertility preservation in pediatric oncology is sparse and heterogeneous, which limits the comparability of results. A Swiss survey conducted from 2009 to 2013 reported a 9% uptake [51], which is slightly higher than the rate observed in our cohort. However, it should be noted that the inclusion criteria differed between the two studies, as they also included non-malignant diseases requiring HSCT as well as patients treated with radiotherapy alone. A European multicenter survey revealed significant variability, with sperm cryopreservation being offered in the majority of centers that supplied their data, while oocyte preservation was available in only one-third of the centers [52]. Beyond these examples, few systematic publications exist, highlighting the unique relevance of our findings: data on actual uptake and documentation practices is rarely reported and urgently needed to inform guidelines and improve equity in care.
It is important to acknowledge the limitations of the study. The single-center, retrospective design of the study limited its generalizability, and the absence of documentation (e.g., Tanner staging, hormone values) restricted the analysis. The results may be influenced by physician-dependent variation in awareness and counseling, as no SOPs were in place during the study period. Despite these limitations, the dataset provides valuable insights into historical practice and offers a rare reference point for international comparison.
4.1. Practical Implications
Our findings underline the need for structured, prospective approaches. Systematic documentation of puberty status, hormone levels (including AMH in girls and inhibin B in boys), and reproductive milestones should be standard at diagnosis. Interdisciplinary counseling involving pediatric oncologists and reproductive specialists can ensure individualized, risk-adapted recommendations. Awareness among physicians, patients, and families should be increased through standardized information at diagnosis. Finally, expanding fertility-preserving options for high-risk patients, including experimental approaches such as ovarian tissue cryopreservation for prepubertal girls, should be considered to prepare for future technological advances.
5. Conclusions
Fertility preservation in pediatric oncology patients at our center was inconsistently applied, with marked gender differences and incomplete documentation of reproductive parameters. Although uptake rates were comparable to the few international reports available, the scarcity of published data underscores the particular relevance of our findings.
Standardized documentation, interdisciplinary decision-making, and broader access to fertility preservation are essential to optimize care. As survival after childhood cancer improves, fertility preservation must become an integral component of survivorship care to safeguard long-term quality of life and future family planning.
Author Contributions
Conceptualization, Jonas Hafele, Gabriele Kropshofer, Roman Crazzolara, Bettina Toth and Bettina Böttcher; Data curation, Gabriele Kropshofer and Bettina Böttcher; Formal analysis, Jonas Hafele; Investigation, Jonas Hafele; Methodology, Jonas Hafele; Project administration, Gabriele Kropshofer and Roman Crazzolara; Resources, Gabriele Kropshofer, Roman Crazzolara, Bettina Toth and Bettina Böttcher; Supervision, Gabriele Kropshofer, Roman Crazzolara and Bettina Böttcher; Writing – original draft, Jonas Hafele and Bettina Böttcher; Writing – review & editing, Jonas Hafele, Gabriele Kropshofer, Roman Crazzolara, Bettina Toth and Bettina Böttcher.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the Medical University of Innsbruck (1374/2023, 26 March 2024).
Informed Consent Statement
Informed consent was waived by the ethics committee because of the retrospective design and anonymized data use.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to privacy and ethical restrictions. In accordance with institutional and national data protection regulations, individual-level patient data cannot be shared in an open repository. However, de-identified data may be made available from the corresponding author upon reasonable request and after review of compliance with applicable ethical and legal standards.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AMH | Anti-Müllerian Hormone |
| CCS | Childhood Cancer Survivors |
| COH | Controlled Ovarian Hyperstimulation |
| HPG | Hypothalamic-Pituitary-Gonadal Axis |
| HSCT | Hematopoietic Stem Cell Transplantation |
| NHL | Non-Hodgkin Lymphoma |
| OC | Oocyte Cryopreservation |
| OTC | Ovarian Tissue Cryopreservation |
| PVS | Penile Vibratory Stimulation |
| POI | Premature Ovarian Insufficiency |
| QoL | Quality of Life |
| SC | Sperm Cryopreservation |
| TESE | Testicular Sperm Extraction |
| TTC | Testicular Tissue Cryopreservation |
References
- Calaminus, G.; Langer, T.; Willich, N.; Beck, J.D. Lebensqualität Und Spätfolgen Bei Kindern Und Jugendlichen Mit Krebserkrankungen. Onkologe 2000, 6, 868–877.
- Phillips, S.M.; Padgett, L.S.; Leisenring, W.M.; Stratton, K.K.; Bishop, K.; Krull, K.R.; Alfano, C.M.; Gibson, T.M.; De Moor, J.S.; Hartigan, D.B.; et al. Survivors of Childhood Cancer in the United States: Prevalence and Burden of Morbidity. Cancer Epidemiol Biomarkers Prev 2015, 24, 653–663, doi:10.1158/1055-9965.EPI-14-1418.
- Bitsko, M.J.; Cohen, D.; Dillon, R.; Harvey, J.; Krull, K.; Klosky, J.L. Psychosocial Late Effects in Pediatric Cancer Survivors: A Report From the Children’s Oncology Group. Pediatr Blood Cancer 2016, 63, 337–343, doi:10.1002/pbc.25773.
- Zebrack, B.J.; Chesler, M.A. Quality of Life in Childhood Cancer Survivors. Psychooncology 2002, 11, 132–141, doi:10.1002/pon.569.
- Meacham, L.R.; Burns, K.; Orwig, K.E.; Levine, J. Standardizing Risk Assessment for Treatment-Related Gonadal Insufficiency and Infertility in Childhood Adolescent and Young Adult Cancer: The Pediatric Initiative Network Risk Stratification System. J Adolesc Young Adult Oncol 2020, 9, 662–666, doi:10.1089/jayao.2020.0012.
- Green, D.M.; Liu, W.; Kutteh, W.H.; Ke, R.W.; Shelton, K.C.; Sklar, C.A.; Chemaitilly, W.; Pui, C.H.; Klosky, J.L.; Spunt, S.L.; et al. Cumulative Alkylating Agent Exposure and Semen Parameters in Adult Survivors of Childhood Cancer: A Report from the St Jude Lifetime Cohort Study. Lancet Oncol 2014, 15, 1215–1223, doi:10.1016/S1470-2045(14)70408-5.
- Ritenour, C.W.M.; Seidel, K.D.; Leisenring, W.; Mertens, A.C.; Wasilewski-Masker, K.; Shnorhavorian, M.; Sklar, C.A.; Whitton, J.A.; Stovall, M.; Constine, L.S.; et al. Erectile Dysfunction in Male Survivors of Childhood Cancer-A Report from the Childhood Cancer Survivor Study. J Sex Med 2016, 13, 945–954, doi:10.1016/j.jsxm.2016.03.367.
- Romerius, P.; Ståhl, O.; Moëll, C.; Relander, T.; Cavallin-Ståhl, E.; Wiebe, T.; Giwercman, Y.L.; Giwercman, A. Hypogonadism Risk in Men Treated for Childhood Cancer. Clin Endocrinol Metab 2009, 94, 4180–4186, doi:10.1210/jc.2009-0337.
- Claessens, J.J.M.; Penson, A.; Bronkhorst, E.M.; Kremer, L.C.M.; van Dulmen-den Broeder, E.; van der Heiden-van der Loo, M.; Tissing, W.J.E.; van der Pal, H.J.H.; Blijlevens, N.M.A.; van den Heuvel-Eibrink, M.M.; et al. Desire for Children among Male Survivors of Childhood Cancer: A DCCSS LATER Study. Cancer 2023, 129, 1432–1442, doi:10.1002/cncr.34685.
- Green, D.M.; Kawashima, T.; Stovall, M.; Leisenring, W.; Sklar, C.A.; Mertens, A.C.; Donaldson, S.S.; Byrne, J.; Robison, L.L. Fertility of Male Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study. J Clin Oncol 2010, 28, 332–339, doi:10.1200/JCO.2009.24.9037.
- Green, D.M.; Sklar, C.A.; Boice, J.D.; Mulvihill, J.J.; Whitton, J.A.; Stovall, M.; Yasui, Y. Ovarian Failure and Reproductive Outcomes after Childhood Cancer Treatment: Results from the Childhood Cancer Survivor Study. J Clin Oncol 2009, 27, 2374–2381, doi:10.1200/JCO.2008.21.1839.
- Bath, L.E.; Critchley, H.O.D.; Chambers, S.E.; Anderson, R.A.; Kelnar, C.J.H.; Wallace, W.H.B. Ovarian and Uterine Characteristics after Total Body Irradiation in Childhood and Adolescence: Response to Sex Steroid Replacement. BJOG: Int. J. Obstet. Gynaecol. 1999, 106, 1265–1272, doi:10.1111/j.1471-0528.1999.tb08180.x.
- Torella, M.; Riemma, G.; De Franciscis, P.; Verde, M. La; Colacurci, N. Serum Anti-Müllerian Hormone Levels and Risk of Premature Ovarian Insufficiency in Female Childhood Cancer Survivors: Systematic Review and Network Meta-Analysis. Cancers (Basel) 2021, 13, 1–13, doi:10.3390/cancers13246331.
- Green, D.M.; Kawashima, T.; Stovall, M.; Leisenring, W.; Sklar, C.A.; Mertens, A.C.; Donaldson, S.S.; Byrne, J.; Robison, L.L. Fertility of Female Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study. J Clin Oncol 2009, 27, 2677–2685, doi:10.1200/JCO.2008.20.1541.
- Anderson, R.A.; Brewster, D.H.; Wood, R.; Nowell, S.; Fischbacher, C.; Kelsey, T.W.; Wallace, W.H.B. The Impact of Cancer on Subsequent Chance of Pregnancy: A Populationbased Analysis. Hum Reprod 2018, 33, 1281–1290, doi:10.1093/humrep/dey216.
- Rendtorff, R.; Hohmann, C.; Reinmuth, S.; Müller, A.; Dittrich, R.; Beyer, M.; Wickmann, L.; Keil, T.; Henze, G.; Borgmann-Staudt, A. Hormone and Sperm Analyses after Chemo- and Radiotherapy in Childhood and Adolescence. Klin Padiatr 2010, 222, 145–149, doi:10.1055/s-0030-1249658.
- Hohmann, C.; Borgmann, A.; Keil, T. Re: Induced Abortions in Danish Cancer Survivors: A Population-Based Cohort Study. . 2011;103(8):698. J Natl Cancer Inst 2011, 103, 698, doi:doi:10.1093/jnci/djr063.
- Donnez, J.; Martinez-Madrid, B.; Jadoul, P.; Van Langendonckt, A.; Demylle, D.; Dolmans, M.M. Ovarian Tissue Cryopreservation and Transplantation: A Review. Hum. Reprod. Update. 2006, 12, 519–535, doi:10.1093/humupd/dml032.
- Bedoschi, G.; Navarro, P.A.; Oktay, K. Chemotherapy-Induced Damage to Ovary: Mechanisms and Clinical Impact. Future Oncol. 2016, 12, 2333–2344, doi:10.2217/fon-2016-0176.
- Meistrich, M. Male Gonadal Toxicity. Pediatr Blood Cancer 2009, 53, 261–266, doi:10.1002/pbc.22004.
- Sonigo, C.; Beau, I.; Binart, N.; Grynberg, M. The Impact of Chemotherapy on the Ovaries: Molecular Aspects and the Prevention of Ovarian Damage. Int J Mol Sci 2019, 20, 1–17, doi:10.3390/ijms20215342.
- Soleimani, R.; Heytens, E.; Darzynkiewicz, Z.; Oktay, K. Mechanisms of Chemotherapy-Induced Human Ovarian Aging Double Strand DNA Breaks and Microvascular Compromise. Aging 2011, 3, 782–793.
- Poganitsch-Korhonen, M.; Masliukaite, I.; Nurmio, M.; Lähteenmäki, P.; Van Wely, M.; Van Pelt, A.M.M.; Jahnukainen, K.; Stukenborg, J.B. Decreased Spermatogonial Quantity in Prepubertal Boys with Leukaemia Treated with Alkylating Agents. Leukemia 2017, 31, 1460–1463, doi:10.1038/leu.2017.76.
- Ginsberg, J.P. New Advances in Fertility Preservation for Pediatric Cancer Patients. Curr. Opin. Pediatr 2011, 23, 9–13, doi:10.1097/MOP.0b013e3283420fb6.
- Tharmalingam, M.D.; Matilionyte, G.; Wallace, W.H.B.; Stukenborg, J.B.; Jahnukainen, K.; Oliver, E.; Goriely, A.; Lane, S.; Guo, J.; Cairns, B.; et al. Cisplatin and Carboplatin Result in Similar Gonadotoxicity in Immature Human Testis with Implications for Fertility Preservation in Childhood Cancer. 18:374. BMC Med 2020, 18, doi:10.1186/s12916-020-01844-y.
- Zhou, B.; Kwan, B.; Desai, M.J.; Nalawade, V.; Henk, J.; Viravalli, N.; Murphy, J.D.; Nathan, P.C.; Ruddy, K.J.; Shliakhtsitsava, K.; et al. Association of Platinum-Based Chemotherapy with Live Birth and Infertility in Female Survivors of Adolescent and Young Adult Cancer. Fertil Steril 2024, 121, 1020–1030, doi:10.1016/j.fertnstert.2024.01.039.
- Chow, E.J.; Stratton, K.L.; Leisenring, W.M.; Oeffinger, K.C.; Sklar, C.A.; Donaldson, S.S.; Ginsberg, J.P.; Kenney, L.B.; Levine, J.M.; Robison, L.L.; et al. Pregnancy after Chemotherapy in Male and Female Survivors of Childhood Cancer Treated between 1970 and 1999: A Report from the Childhood Cancer Survivor Study Cohort. Lancet Oncol 2016, 17, 567–576, doi:10.1016/S1470-2045(16)00086-3.
- Reinmuth, S.; Hohmann, C.; Rendtorff, R.; Balcerek, M.; Holzhausen, S.; Müller, A.; Henze, G.; Keil, T.; Borgmann-Staudt, A. Impact of Chemotherapy and Radiotherapy in Childhood on Fertility in Adulthood: The FeCt - Survey of Childhood Cancer Survivors in Germany. J Cancer Res Clin Oncol 2013, 139, 2071–2078, doi:10.1007/s00432-013-1527-9.
- Wallace, W.H.B.; Thomson, A.B.; Kelsey, T.W. The Radiosensitivity of the Human Oocyte. Hum. Reprod. 2003, 18, 117–121, doi:10.1093/humrep/deg016.
- Larsen, E.C.; Schmiegelow, K.; Rechnitzer, C.; Loft, A.; Müller, J.; Andersen, A.N. Radiotherapy at a Young Age Reduces Uterine Volume of Childhood Cancer Survivors. Acta Obstet Gynecol Scand 2004, 83, 96–102, doi:10.1111/j.1600-0412.2004.00332.x.
- De Felice, F.; Marchetti, C.; Marampon, F.; Cascialli, G.; Muzii, L.; Tombolini, V. Radiation Effects on Male Fertility. Andrology 2019, 7, 2–7, doi:10.1111/andr.12562.
- Koustenis, E.; Pfitzer, C.; Balcerek, M.; Reinmuth, S.; Zynda, A.; Stromberger, C.; Hohmann, C.; Keil, T.; Borgmann-Staudt, A. Impact of Cranial Irradiation and Brain Tumor Location on Fertility: A Survey. Klin Padiatr 2013, 225, 320–324, doi:10.1055/s-0033-1353206.
- Wasilewski-Masker, K.; Seidel, K.D.; Leisenring, W.; Mertens, A.C.; Shnorhavorian, M.; Ritenour, C.W.; Stovall, M.; Green, D.M.; Sklar, C.A.; Armstrong, G.T.; et al. Male Infertility in Long-Term Survivors of Pediatric Cancer: A Report from the Childhood Cancer Survivor Study. J. Cancer Surviv. 2014, 8, 437–447, doi:10.1007/s11764-014-0354-6.
- Thomas-Teinturier, C.; El Fayech, C.; Oberlin, O.; Pacquement, H.; Haddy, N.; Labbé, M.; Veres, C.; Guibout, C.; Diallo, I.; De Vathaire, F. Age at Menopause and Its Influencing Factors in a Cohort of Survivors of Childhood Cancer: Earlier but Rarely Premature. Hum. Reprod. 2013, 28, 488–495, doi:10.1093/humrep/des391.
- Lambertini, M.; Peccatori, F.A.; Demeestere, I.; Amant, F.; Wyns, C.; Stukenborg, J.B.; Paluch-Shimon, S.; Halaska, M.J.; Uzan, C.; Meissner, J.; et al. Fertility Preservation and Post-Treatment Pregnancies in Post-Pubertal Cancer Patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2020, 31, 1664–1678, doi:10.1016/j.annonc.2020.09.006.
- Fayomi, A.P.; Peters, K.; Sukhwani, M.; Valli-Pulaski, H.; Shetty, G.; Meistrich, M.L.; Houser, L.; Robertson, N.; Roberts, V.; Ramsey, C.; et al. Autologous Grafting of Cryopreserved Prepubertal Rhesus Testis Produces Sperm and Offspring. Science 2019, 363, 1314–1319, doi:doi:10.1126/science.aav2914.
- Goossens, E.; Jahnukainen, K.; Mitchell, R.T.; Van Pelt, A.M.M.; Pennings, G.; Rives, N.; Poels, J.; Wyns, C.; Lane, S.; Rodriguez-Wallberg, K.A.; et al. Fertility Preservation in Boys: Recent Developments and New Insights. Hum Reprod Open 2020, 2020, 1–18, doi:10.1093/hropen/hoaa016.
- Gül Siraz, Ü.; Hatipoğlu, N. Fertility Preservation Methods in Childhood and Adolescence Cancers: A Review. J Pediatr Acad 2021, 2, 91–96, doi:10.51271/jpea-2021-0145.
- Bahadur, G.; Ling, K.L.E.; Hart, R.; Ralph, D.; Riley, V.; Wafa, R.; Ashraf, A.; Jaman, N.; Oyede, A.W. Semen Production in Adolescent Cancer Patients. Hum. Reprod. 2002, 17, 2654–2656.
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001, doi:10.1200/JCO. 2018.78.1914.
- Poirot, C.; Abirached, F.; Prades, M.; Coussieu, C.; Bernaudin, F.; Piver, P. Induction of Puberty by Autograft of Cryopreserved Ovarian Tissue. Lancet 2012, 379, 588, doi:doi:10.1016/S0140-6736(11)61781-9.
- Matthews, S.; Picton, H.; Ernst, E.; Andersen, C. Successful Pregnancy in a Woman Previously Suffering from β-Thalassemia Following Transplantation of Ovarian Tissue Cryopreserved before Puberty. Minerva Ginecol. 2018, 70, 432–435.
- Demeestere, I.; Simon, P.; Dedeken, L.; Moffa, F.; Tsépélidis, S.; Brachet, C.; Delbaere, A.; Devreker, F.; Ferster, A. Live Birth after Autograft of Ovarian Tissue Cryopreserved during Childhood. Hum. Reprod. 2015, 30, 2107–2109, doi:10.1093/humrep/dev128.
- Kinderonkologische Erkrankungen. In Indikation und Durchführung fertilitätsprotektiver Maßnahmen bei onkologischen und nicht-onkologischen Erkrankungen; Balcerek, M., von Wolff, M., Borgmann-Staudt, A., Eds.; FertiPROTEKT: Kiel, Germany, 2020; pp. 117–131 ISBN 9783883121291.
- Mossa, B.; Schimberni, M.; Di Benedetto, L.; Mossa, S.; Schimberni, M. Ovarian Transposition in Young Women and Fertility Sparing. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3418–3425.
- Irtan, S.; Orbach, D.; Helfre, S.; Sarnacki, S. Ovarian Transposition in Prepubescent and Adolescent Girls with Cancer. Lancet Oncol. 2013, 14, e601–e608, doi:10.1016/S1470-2045(13)70288-2.
- Cobo, A.; García-Velasco, J.A.; Coello, A.; Domingo, J.; Pellicer, A.; Remohí, J. Oocyte Vitrification as an Efficient Option for Elective Fertility Preservation. Fertil Steril 2016, 105, 755–764, doi:10.1016/j.fertnstert.2015.11.027.
- von Wolff, M.; Bruckner, T.; Strowitzki, T.; Germeyer, A. Fertility Preservation: Ovarian Response to Freeze Oocytes Is Not Affected by Different Malignant Diseases—an Analysis of 992 Stimulations. J Assist Reprod Genet 2018, 35, 1713–1719, doi:10.1007/s10815-018-1227-0.
- Dolmans, M.M.; Taylor, H.S.; Rodriguez-Wallberg, K.A.; Blumenfeld, Z.; Lambertini, M.; von Wolff, M.; Donnez, J. Utility of Gonadotropin-Releasing Hormone Agonists for Fertility Preservation in Women Receiving Chemotherapy: Pros and Cons. Fertil Steril 2020, 114, 725–738, doi:10.1016/j.fertnstert.2020.08.011.
- Blumenfeld, Z. Fertility Preservation Using GnRH Agonists: Rationale, Possible Mechanisms, and Explanation of Controversy. Clin Med Insights Reprod Health 2019, 13, 1, doi:10.1177/1179558119870163.
- Diesch, T.; von der Weid, N.X.; Szinnai, G.; Schaedelin, S.; De Geyter, C.; Rovó, A. Fertility Preservation in Pediatric and Adolescent Cancer Patients in Switzerland: A Qualitative Cross-Sectional Survey. Cancer Epidemiol 2016, 44, 141–146, doi:10.1016/j.canep.2016.08.013.
- Terenziani, M.; Spinelli, M.; Jankovic, M.; Bardi, E.; Hjorth, L.; Haupt, R.; Michel, G.; Byrne, J. Practices of Pediatric Oncology and Hematology Providers Regarding Fertility Issues: A European Survey. Pediatr Blood Cancer 2014, 61, 2054–2058, doi:10.1002/pbc.25163.
Figure 1.
Fertility preservation measures in male and female patients as a percentage of the total age group.
Figure 1.
Fertility preservation measures in male and female patients as a percentage of the total age group.
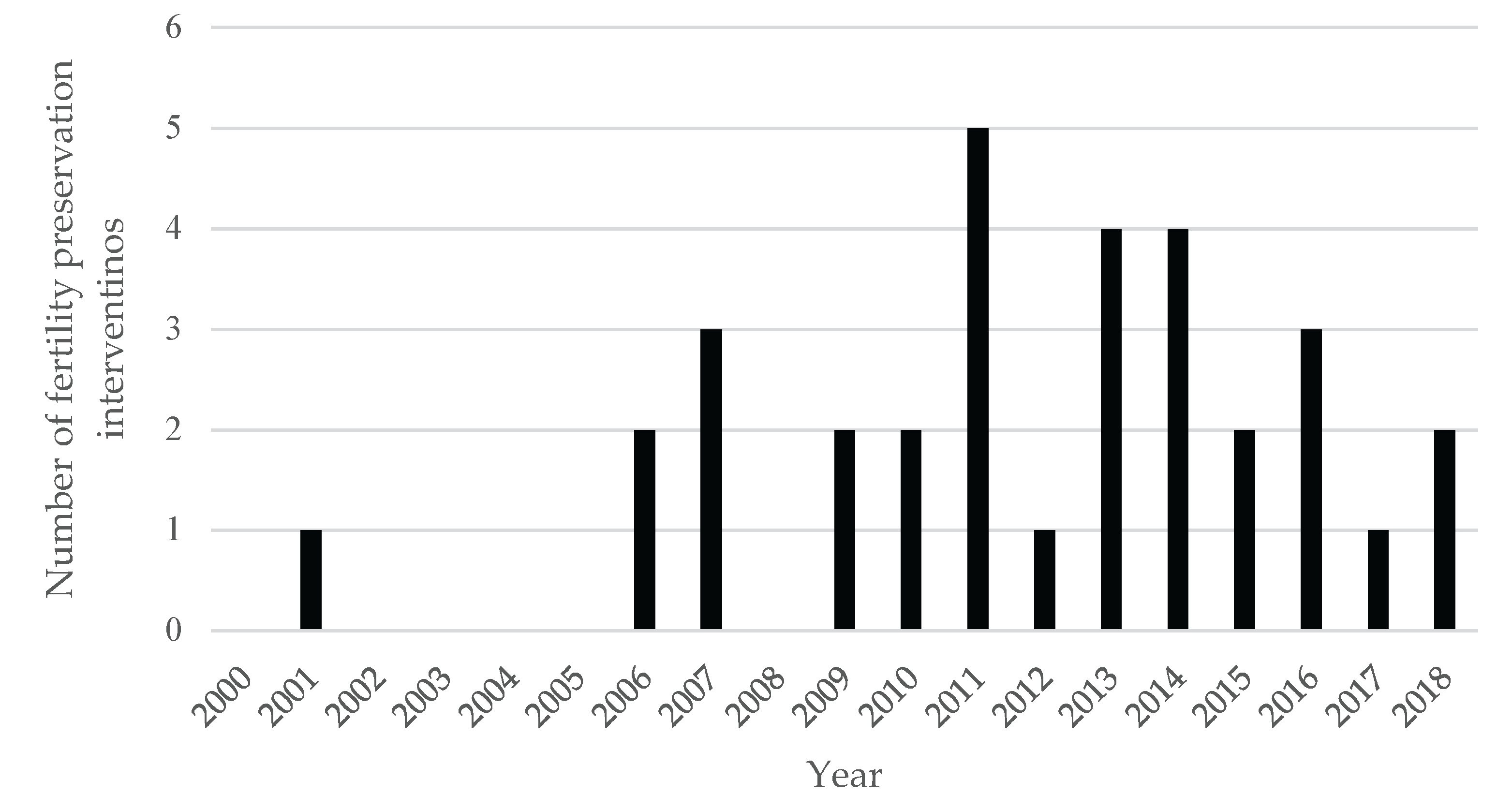
Figure 2.
Fertility preservation measures in male and female patients as a percentage of the total age group.
Figure 2.
Fertility preservation measures in male and female patients as a percentage of the total age group.
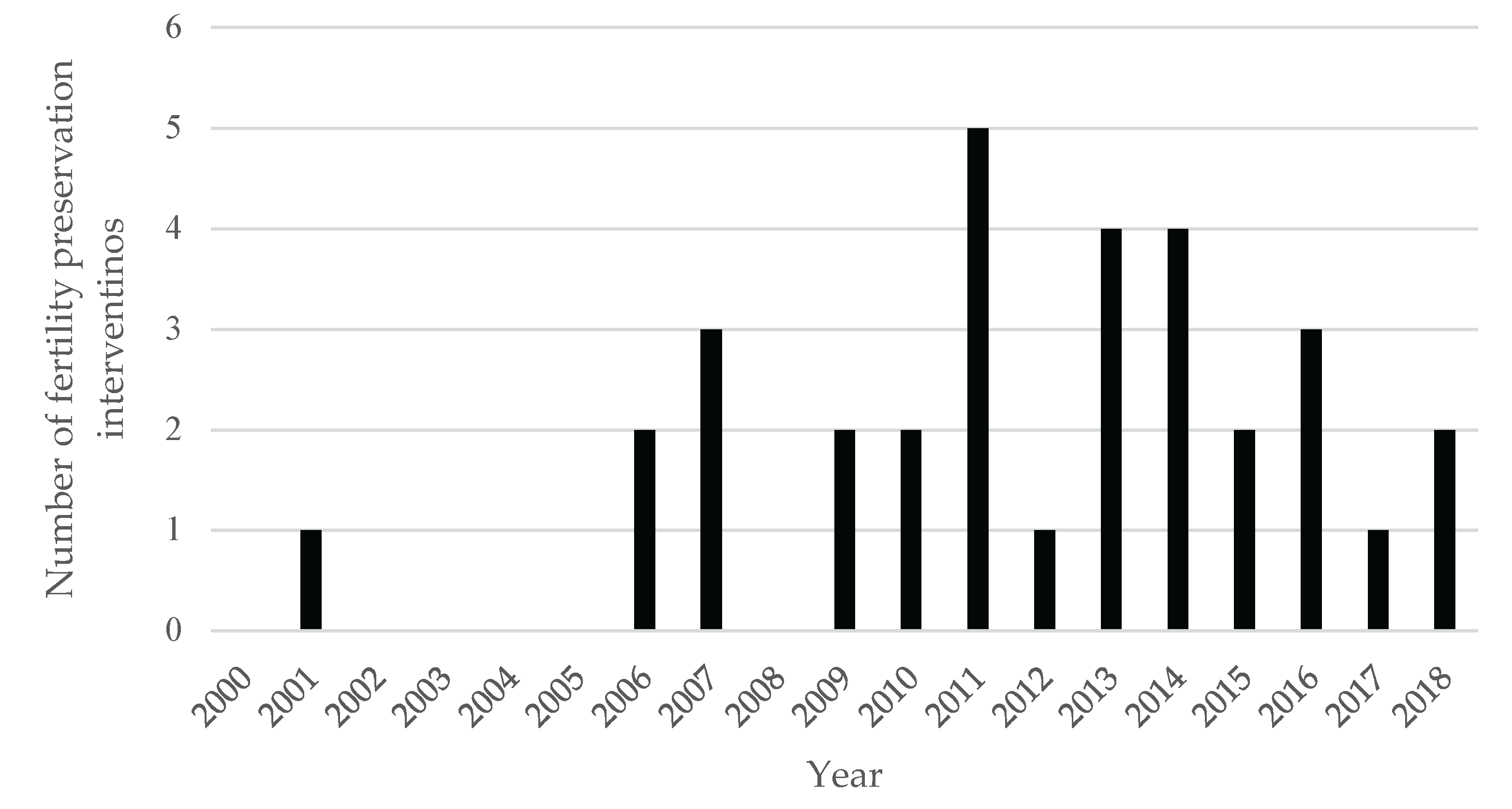

Table 1.
Patient characteristics, survival, recurrence, and radiotherapy status.
| Variable | n | Percentage (%)1 |
| Sex | ||
| Female | 247 | 44.7 |
| Male | 305 | 55.3 |
| Survival, recurrence, and radiation status | ||
| Alive | 441 | 79.9 |
| Deceased | 111 | 20.1 |
| Recurrence (min. 1) | 124 | 22.5 |
| Radiation | 162 | 29.3 |
| Extracranial Radiation | 105 | 19.0 |
| Cranial Radiation | 57 | 10.3 |
1 Percentage of the total sample.
Table 2.
Clinical documentation of sex hormone status.
| Variable | n | Percentage (%)1 |
| Total (female) | 75 | 30.4 |
| AMH | 4 | 1.6 |
| FSH | 73 | 29.6 |
| Estradiol | 72 | 29.1 |
| Hormonally active | 23 | 30.62 |
| Total (male) | 89 | 29.2 |
| FSH | 88 | 28.9 |
| Testosterone | 82 | 26.9 |
| Hormonally active | 18 | 20.22 |
1 Percentage of the total sample of same sex, 2 Percentage of the total number of patients with documented hormone levels of the same sex, in female patients estradiol ≥ 25 ng/L and age ≥ 9 years, in male patients testosterone ≥ 3.1 µg/L and age ≥ 9 years.
Table 3.
Application of SC, OC or OTC.
| Variable | n | Percentage (%)1 |
| Fertility preservation (female) | ||
| no | 239 | 96.8 |
| yes | 8 | 3.2 |
| OCT | 6 | 2.4 |
| OC | 3 | 1.2 |
| Fertility preservation (male) | ||
| no | 277 | 90.8 |
| yes | 28 | 9.2 |
| SC via masturbation | 27 | 8.9 |
| SC via TESE | 1 | 0.3 |
1 Percentage of the total sample of same sex.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



