Submitted:
24 September 2025
Posted:
25 September 2025
You are already at the latest version
Abstract
Background/Objectives: Bladder carcinoma (BC) is strongly associated with tobacco exposure, a major shared risk factor for several smoking-related diseases (SRDs), including pulmonary disorders and coronary atherosclerosis. However, the prevalence of SRDs in patients with high-grade (HGBC) or muscle-invasive bladder carcinoma (MIBC) has not been systematically investigated. We aimed to evaluate SRD prevalence and to assess the potential role of chest high-resolution computed tomography (HRCT) in a population with histologically confirmed HGBC or MIBC. Methods: We retrospectively analyzed 166 patients with histologically confirmed HGBC/MIBC who underwent staging HRCT. SRDs—including emphysema, suspicious pulmonary nodules, airway disease, interstitial lung disease (ILD), and coronary artery calcifications (CAC)—were assessed. Associations between smoking status and SRDs were evaluated using binary logistic regression, and odds ratios (OR) with 95% confidence intervals (CI) were calculated. Results: Overall, 60.2% of patients had at least one SRD. Smokers showed a significantly higher SRD prevalence than non-smokers (P< 0.05). Pulmonary SRDs were observed in 31.9% of patients, with emphysema being most strongly associated with smoking (P< 0.01). Suspicious pulmonary nodules (Lung-RADS ≥3) were detected in 6.6% of patients, more commonly among smokers (72.7%), though the difference was not statistically significant. Histological analysis confirmed all lesions as primary lung cancers rather than metastatic bladder carcinoma. Conclusions: Patients with HGBC/MIBC demonstrate a high prevalence of SRDs, supporting the integration of chest HRCT into staging protocols. HRCT may enable early detection of clinically relevant comorbidities and help identify candidates for lung cancer screening.
Keywords:
smoking-related diseases
; bladder cancer
; lung cancer
; lung cancer screening
1. Introduction
Bladder carcinoma (BC) is the tenth most frequently diagnosed malignancy worldwide. Its prevalence varies across regions, reflecting differences in exposure to risk factors and access to diagnostic resources. Globally, the estimated incidence is 9.5 per 100,000 person-years in men and 2.4 per 100,000 person-years in women [1]. Urothelial carcinoma accounts for approximately 95% of cases, although other histological variants—including squamous cell carcinoma, adenocarcinoma, and the rarer neuroendocrine or leiomyomatous tumors—have been described [2,3]. Clinically, BC most commonly presents with painless macroscopic hematuria, although abdominal pain and lower urinary tract symptoms such as dysuria and urgency may also occur [4]. Ultrasound is often used as the initial imaging modality in patients with hematuria, but its sensitivity is limited for small or anatomically hidden tumors [5]. Urine cytology offers high specificity (>90%) in high-grade BC or carcinoma in situ (CIS), yet sensitivity remains low in detecting low-grade lesions [6]. Definitive diagnosis relies on cystoscopy and, when indicated, transurethral resection of the bladder tumor (TURB) for histopathological evaluation. Histopathological assessment includes tumor grading, according to the World Health Organization system, which classifies lesions as papillary urothelial neoplasm of low malignant potential, low-grade (LG), or high-grade (HG) carcinoma [7]. Staging follows the TNM classification, and the presence of detrusor muscle invasion critically determines both treatment strategies and radiological follow-up. Non–muscle-invasive BC (NMIBC; stages Ta, T1, and CIS) occurs in about 75% of cases and is generally managed conservatively with TURB, with or without subsequent intravesical immunotherapy or chemotherapy. In contrast, muscle-invasive BC (MIBC; stage T2 or higher) carries a worse prognosis and requires radical treatment with cystectomy, systemic chemotherapy, and, in selected cases, radiotherapy [8]. Detrusor invasion is not only the key prognostic factor but also determines the need for staging investigations. According to the European Association of Urology (EAU) guidelines, cross-sectional imaging with CT or MRI is not routinely indicated in patients with NMIBC or LGBC. Instead, staging CT of the chest, abdomen, and pelvis is specifically recommended in patients with MIBC or HGBC, in order to evaluate lymph node involvement and distant metastases [8,9]. Both inherited and environmental factors contribute to BC development. Established risk factors include exposure to chemical agents such as aromatic amines or polycyclic aromatic hydrocarbons, pelvic radiotherapy, and chronic schistosomiasis. However, tobacco smoking remains the predominant acquired risk factor, accounting for a substantial proportion of BC cases worldwide [10,11,12]. Importantly, smoking is also strongly associated with other diseases, including atherosclerosis and pulmonary disorders such as pulmonary emphysema, interstitial lung diseases (ILDs) and lung cancer (LC) [13,14,15]. Despite these well-known associations, the prevalence of smoking-related diseases (SRDs) in patients with BC has not been systematically investigated. High-resolution computed tomography (HRCT) of the chest represents the diagnostic gold standard for SRDs, and low-dose HRCT has been shown to reduce LC mortality in large screening cohorts. These studies highlight the importance of selecting patients from high-risk populations, both to optimize screening efficacy and to minimize false positives and overdiagnosis, thereby improving the cost-effectiveness ratio of screening programs [16,17,18]. Given that BC and many SRDs share tobacco exposure as a common etiological factor, patients with BC may represent a population at particularly high risk for both prevalent SRDs and possibly for the development of primary LC. Investigating the prevalence of SRDs in this cohort may help clarify whether BC patients could represent an ideal target group for structured HRCT-based screening programs.
We retrospectively evaluated the prevalence of SRDs in a cohort of patients with histologically confirmed HGBC or MIBC. The risk of SRDs was compared among current smokers, former smokers, and non-smokers. As a secondary objective, we assessed the prevalence of pulmonary nodules suspicious for primary LC and compared the risk of LC across patient groups.
2. Materials and Methods
2.1. Population of the Study
This study was conducted at the Radiology Unit of Sant’Orsola University Hospital, Bologna, Italy. We included patients with MIBC OR HGBC who underwent staging CT between June 2021 and June 2025. The CT protocol comprised scans of the abdomen, pelvis, and chest, including HRCT, both before and after administration of intravenous contrast medium. Patients were excluded if chest CT was not included in the imaging protocol. The final study cohort consisted of 166 patients who had undergone at least one HRCT of the chest prior to cystectomy. When multiple CT scans were available, only the most recent examination was analyzed. Collected clinical data included sex, age, smoking status, histological grade and TNM stage of BC. Patients were categorized as current smokers, former smokers or non-smokers depending on their smoking habits. The presence of SRDs, including suspicious pulmonary nodules, pulmonary emphysema, airway disease, and ILD, was assessed for each patient. When available, histological data of suspicious pulmonary nodules, obtained either by bronchoscopic biopsy or surgical excision, were also collected. This study is an observational, retrospective single-center study and was approved by our local institution review board. Informed consent was waived by the institutional review board owning to the retrospective nature of the study.
2.2. Imaging Analysis
All CT scans were independently reviewed by two blinded radiologists with substantial expertise in chest imaging. Pulmonary nodules were considered suspicious for primary LC when no evidence of bladder carcinoma metastases or involvement of the common iliac lymph nodes (N3 stage) was present. In these cases, the radiological probability of pulmonary malignancy was further characterized according to the Lung-RADS criteria [19], and only nodules with a Lung-RADS score ≥3 were included in the estimation of LC prevalence. The severity of emphysema and airway disease was classified according to the Fleischner Society guidelines [20], with moderate to severe emphysema (grades 1C, 1D, 1E, or 3B) considered indicative of smoking-related disease. Coronary artery calcifications (CAC) were evaluated in accordance with the Society of Thoracic Radiology recommendations [21], and only moderate to severe CAC (grades 2 or 3) were included in the analysis. Interstitial abnormalities suggestive of ILD were also documented.
2.3. Statistical Analysis
Categorical variables were summarized as counts and percentages, while numerical variables were summarized as mean ± standard deviation, as well as minimum and maximum values. Binary logistic regression was employed to investigate associations between smoking status and each smoking-related disease. Smoking status was treated as the independent variable, while each disease was modeled as a binary outcome. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Statistical significance was set at p < 0.05. All analyses were performed using R (version 4.5.1).
3. Results
Of the 166 patients with muscle invasive or high-grade bladder carcinoma, 37 (22%) were female and 129 (78%) were male, with a mean age of 72.9 ± 10.3 years. Eighty-nine patients (53.6%) were non-smokers, while 77 (46.4%) had a history of smoking (28 current smokers and 49 former smokers). Overall, 100 patients (60.2%) had at least one SRD as defined by imaging criteria, including pulmonary disease or moderate to severe coronary artery calcification CAC. SRD prevalence did not differ significantly between male and female patients. Current smokers had a significantly higher risk of SRD compared with non-smokers (p < 0.05). When current and former smokers were combined, SRD prevalence remained significantly higher than in non-smokers (p < 0.05). Former smokers alone showed a higher SRD prevalence compared with non-smokers (65.3% vs 52.8%, OR 1.68), but this difference was not statistically significant. The prevalence of SRDs among smokers and non-smokers is summarized in Table 1 and visually represented in Figure 1.
Smoking-related pulmonary disease (p-SRD) was identified in 53 patients (31.9%), and moderate to severe CAC (grades 2 or 3, Society of Thoracic Radiology) was present in 86 (51.8%). Although CAC prevalence did not differ significantly between smokers and non-smokers, smokers had a significantly higher risk of p-SRD (p < 0.01). Moderate to severe centrilobular or paraseptal emphysema (grades 1C, 1D, 1E, or 3B, Fleischner Society) was significantly more frequent in smokers than in non-smokers (p < 0.01). Among smokers, current smokers had a higher risk of emphysema compared with former smokers (p < 0.01). An illustrative example of severe emphysema (grade 1D) diagnosed in one of our patients is shown in Figure 2.
Interstitial abnormalities suggestive of early interstitial lung disease (ILD) and airway pathology were found in 23 patients (13.9%) and 13 patients (7.8%), respectively, without significant differences between smokers and non-smokers. Nodules suspicious for LC (Lung-RADS score ≥ 3) were present in 11 patients (6.6%), each with a single lesion. Of these, 4 were current smokers, 4 were former smokers, and 3 were non-smokers. Although the prevalence was higher among patients with a smoking history (72.7% vs 27.3%, OR 3.32), the difference did not reach statistical significance. Histological data, obtained either via bronchoscopic biopsy or surgical excision, were available for five patients (45%). Importantly, all nodules were confirmed as primary lung cancers (three adenocarcinomas and two squamous cell carcinomas), excluding metastatic bladder carcinoma. A representative example of a suspicious pulmonary nodule (Lung-RADS score = 4B) detected in one of the patients is shown in Figure 3.
4. Discussion
Our study demonstrated a high prevalence (60.2%) of SRDs in patients with HGBC or MIBC, a population that shares tobacco exposure as a major risk factor. Both current smokers and the overall group of smokers showed a significantly increased risk of developing SRDs. However, SRD prevalence did not differ significantly between former smokers and never-smokers. This finding may be explained by the beneficial effects of early and sustained smoking cessation on pulmonary function, as demonstrated in previous studies [22,23,24]. A considerable prevalence of p-SRDs (31.9%) was observed, with emphysema emerging as the most frequent pulmonary disease and showing the strongest association with smoking status. Importantly, current smokers were significantly more affected than former smokers, highlighting the protective role of smoking cessation in limiting emphysema development [25]. Smoking is a well-established risk factor for both pulmonary emphysema and coronary atherosclerosis [26], and a strong relationship between these two conditions has been described [27]. Interestingly, in our cohort, smokers did not exhibit a significantly higher prevalence of moderate-to-severe CAC compared with non-smokers. This may be attributed to the multifactorial pathogenesis of atherosclerosis, which includes several cardiovascular risk factors beyond smoking [28], unlike pulmonary diseases, which show a more direct causal relationship with tobacco exposure.
In our population, 6.6% of patients presented with a solitary pulmonary nodule suspicious for primary LC, defined as Lung-RADS score ≥3. None of these patients had evidence of metastatic bladder carcinoma, and based on radiological features, patient history, and staging, pulmonary nodules were reasonably attributed to primary LC rather than BC metastases. Notably, histological analysis confirmed a primary lung origin for all nodules where data were available, reinforcing the diagnostic reliability of Lung-RADS criteria. The prevalence of suspicious nodules in our cohort was higher than reported in previous screening studies targeting high-risk smokers [16,17,18], which demonstrated the efficacy of LC screening in reducing LC mortality. Our observed prevalence (6.6%) is comparable to findings by O’Dwyer et al., who reported a LC prevalence of 6.4% in a screened population with a history of prior malignancies [29]. Although our results may be influenced by the relatively small sample size, they suggest that pulmonary comorbidities and prior cancer history should be considered when developing integrated risk-prediction models for LC. Previous studies have demonstrated that risk-prediction tools such as the PLCOM2012 model, which incorporates pulmonary comorbidities and prior malignancies, improve the efficiency of LC detection, and reduce false positives in screening programs [30,31]. Interestingly, 45% of patients with suspicious pulmonary nodules also presented with moderate-to-severe emphysema, reinforcing the value of incorporating comorbidities into LC screening eligibility criteria. These findings underscore the importance of carefully selecting high-risk patients for screening, both to reduce false positives and to optimize cost-effectiveness.
To our knowledge, this is the first study to systematically investigate the prevalence of SRDs in patients with HGBC/MIBC. Our results support the inclusion of HRCT among staging imaging examinations for BC, as currently recommended by the EAU guidelines [8,9]. Beyond detecting pulmonary nodules suggestive of metastases, HRCT may also identify early-stage, treatable LC, pulmonary diseases, and signs of coronary atherosclerosis requiring further pneumological or cardiological assessment. Given the shared etiological link with smoking habits and the observed high prevalence of SRDs and suspicious pulmonary nodules in our cohort, expanding HRCT surveillance to NMIBC patients with significant smoking histories could enable earlier detection of treatable pulmonary disease and primary LC. Future prospective studies are needed to evaluate the clinical utility and cost-effectiveness of such an approach.
This study has several limitations. The relatively small sample of our cohort may have led to an overestimation of the true prevalence of pulmonary nodules and data on their histological confirmation were available only in a minority of patients. Additionally, our population was relatively older and had, on average, lower cumulative tobacco exposure compared with previous studies, which may introduce selection bias. Finally, due to the retrospective design, we were unable to assess the impact of SRD diagnosis on quality of life or overall survival. Despite these limitations, our findings highlight the potential value of comprehensive chest HRCT in uncovering clinically relevant comorbidities in patients with HGBC and MIBC.
5. Conclusions
Patients with BC show a high prevalence of SRDs, particularly among current and former smokers. Among SRDs, emphysema, lung cancer, and coronary atherosclerosis are clinically relevant comorbidities that significantly impact patient prognosis and quality of life, and they particularly benefit from early detection and sustained smoking cessation. At present, HRCT is required only in the diagnostic workup of patients with NMIBC, who represent a minority of those presenting with bladder cancer. Our findings further support the utility of chest HRCT in detecting SRDs during staging in patients with HGBC/MIBC, but they also suggest that patients with NMIBC, particularly smokers, could also derive clinical benefit from HRCT-based assessment. Future research on larger, prospectively collected cohorts is warranted to validate these results and to evaluate the potential prognostic value of routine chest HRCT screening in current and former smokers, including those with NMIBC.
Author Contributions
The authors contributed to the various phases of the research as follows: conceptualization, Fe.C. and Fr.C.; methodology, Fe.C.; formal analysis, R.R.; investigation, Fe.C. and E.R.; data curation, R.R.; writing—original draft preparation, R.R.; writing—review and editing, S.P.; visualization, Fr.C.; supervision, C.G. and B.C.; project administration, R.S. and C.M. All authors have read and approved the final version of the manuscript. R.R. and Fe.C. contributed equally to this work and should be regarded as co–first authors, sharing the first position in the author list.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of IRCCS Sant’Orsola, Bologna, Italy (ID 7438 Cod. 299/2020/OSS/AOUBo).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
Data analyzed during the current study are available from the corresponding author upon reasonable request (data are not publicly available due to privacy restrictions).
Acknowledgments
During the preparation of this manuscript, the authors used a generative AI tool (ChatGPT-4.5, OpenAI) to assist in generating the graphics presented in Figure 1.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BC | Bladder Carcinoma |
| CAC | Coronary Artery Calcifications |
| CIS | Carcinoma In Situ |
| EAU | European Association of Urology |
| HGBC | High-Grade Bladder Carcinoma |
| HRCT | High-Resolution Computed Tomography |
| ILD | Interstitial Lung Disease |
| LC | Lung Cancer |
| LGBC | Low-Grade Bladder Carcinoma |
| MIBC | Muscle-Invasive Bladder Carcinoma |
| NMIBC | Non-Muscle-Invasive Bladder Carcinoma |
| p-SRD | Smoking-Related pulmonary Disease |
| SRD | Smoking Related Disease |
| TURB | Transurethral Resection of the Bladder |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J Clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Larkins, M.C.; Pasli, M.; Bhatt, A.; Burke, A. Squamous Cell Carcinoma of the bladder: Demographics and Outcomes associated with Surgery and Radiotherapy. Journal of Surgical Oncology 2024, 129, 649–658. [Google Scholar] [CrossRef]
- Mori, K.; Abufaraj, M.; Mostafaei, H.; Quhal, F.; Karakiewicz, P.I.; Briganti, A.; Kimura, S.; Egawa, S.; Shariat, S.F. A Systematic Review and Meta-Analysis of Variant Histology in Urothelial Carcinoma of the Bladder Treated with Radical Cystectomy. Journal of Urology 2020, 204, 1129–1140. [Google Scholar] [CrossRef]
- Reddy, A.C.; Gu, J.Z.; Koo, B.H.; Fruh, V.; Sax, A.J. Urothelial Carcinoma: Epidemiology and Imaging-Based Review. R I Med J (2013) 2024, 107, 26–32. [Google Scholar]
- Tan, W.S.; Sarpong, R.; Khetrapal, P.; Rodney, S.; Mostafid, H.; Cresswell, J.; Hicks, J.; Rane, A.; Henderson, A.; Watson, D.; et al. Can Renal and Bladder Ultrasound Replace Computerized Tomography Urogram in Patients Investigated for Microscopic Hematuria? Journal of Urology 2018, 200, 973–980. [Google Scholar] [CrossRef]
- Yafi, F.A.; Brimo, F.; Steinberg, J.; Aprikian, A.G.; Tanguay, S.; Kassouf, W. Prospective Analysis of Sensitivity and Specificity of Urinary Cytology and Other Urinary Biomarkers for Bladder Cancer. Urologic Oncology: Seminars and Original Investigations 2015, 33, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Compérat, E.; Amin, M.B.; Berney, D.M.; Cree, I.; Menon, S.; Moch, H.; Netto, G.J.; Rao, V.; Raspollini, M.R.; Rubin, M.A.; et al. What’s New in WHO Fifth Edition – Urinary Tract. Histopathology 2022, 81, 439–446. [Google Scholar] [CrossRef]
- De Jong, J.J.; Lotan, Y.; Boormans, J.L. Re: EAU Guidelines on Muscle-Invasive and Metastatic Bladder Cancer. European Urology 2024, 86, 480–481. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non–Muscle-Invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). European Urology 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Minami, T.; Fujita, K.; Hashimoto, M.; Nishimoto, M.; Adomi, S.; Banno, E.; Nozawa, M.; Nose, K.; Yoshimura, K.; Inada, M.; et al. External Beam Radiotherapy Combination Is a Risk Factor for Bladder Cancer in Patients with Prostate Cancer Treated with Brachytherapy. World J Urol 2023, 41, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Bayne, C.E.; Farah, D.; Herbst, K.W.; Hsieh, M.H. Role of Urinary Tract Infection in Bladder Cancer: A Systematic Review and Meta-Analysis. World J Urol 2018, 36, 1181–1190. [Google Scholar] [CrossRef]
- Freedman, N.D. Association Between Smoking and Risk of Bladder Cancer Among Men and Women. JAMA 2011, 306, 737. [Google Scholar] [CrossRef] [PubMed]
- Christenson, S.A.; Smith, B.M.; Bafadhel, M.; Putcha, N. Chronic obstructive pulmonary disease. Lancet 2022, 399, 2227–2242. [Google Scholar] [CrossRef]
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung Cancer. Med Clin North Am 2019, 103, 463–473. [Google Scholar] [CrossRef]
- Serrano Gotarredona, M.P.; Navarro Herrero, S.; Gómez Izquierdo, L.; Rodríguez Portal, J.A. Smoking-Related Interstitial Lung Disease. Radiologia (Engl Ed) 2022, 64 Suppl 3, 277–289. [Google Scholar] [CrossRef]
- Field, J.K.; Duffy, S.W.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Green, B.A.; Holemans, J.A.; Kavanagh, T.; Kerr, K.M.; et al. The UK Lung Cancer Screening Trial: A Pilot Randomised Controlled Trial of Low-Dose Computed Tomography Screening for the Early Detection of Lung Cancer. Health Technol Assess 2016, 20, 1–146. [Google Scholar] [CrossRef] [PubMed]
- Kramer, B.S.; Berg, C.D.; Aberle, D.R.; Prorok, P.C. Lung Cancer Screening with Low-Dose Helical CT: Results from the National Lung Screening Trial (NLST). J Med Screen 2011, 18, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Darrason, M.; Grolleau, E.; De Bermont, J.; Couraud, S. UKLS Trial: Looking beyond Negative Results. The Lancet Regional Health - Europe 2021, 10, 100184. [Google Scholar] [CrossRef]
- American College of Radiology Committee on Lung-RADS. Lung-RADS 2022. Available online: https://www.acr.org/-/media/ACR/Files/RADS/Lung-RADS/Lung-RADS-2022 (accessed on 19 September 2025).
- Lynch, D.A.; Austin, J.H.M.; Hogg, J.C.; Grenier, P.A.; Kauczor, H.-U.; Bankier, A.A.; Barr, R.G.; Colby, T.V.; Galvin, J.R.; Gevenois, P.A.; et al. CT-Definable Subtypes of Chronic Obstructive Pulmonary Disease: A Statement of the Fleischner Society. Radiology 2015, 277, 192–205. [Google Scholar] [CrossRef]
- Hecht, H.S.; Cronin, P.; Blaha, M.J.; Budoff, M.J.; Kazerooni, E.A.; Narula, J.; Yankelevitz, D.; Abbara, S. 2016 SCCT/STR Guidelines for Coronary Artery Calcium Scoring of Noncontrast Noncardiac Chest CT Scans: A Report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. Journal of Cardiovascular Computed Tomography 2017, 11, 74–84. [Google Scholar] [CrossRef]
- Wang, Z.; Qiu, Y.; Ji, X.; Dong, L. Effects of Smoking Cessation on Individuals with COPD: A Systematic Review and Meta-Analysis. Front. Public Health 2024, 12, 1433269. [Google Scholar] [CrossRef]
- Lai, H.; Liu, Q.; Ye, Q.; Liang, Z.; Long, Z.; Hu, Y.; Wu, Q.; Jiang, M. Impact of Smoking Cessation Duration on Lung Cancer Mortality: A Systematic Review and Meta-Analysis. Critical Reviews in Oncology/Hematology 2024, 196, 104323. [Google Scholar] [CrossRef] [PubMed]
- Pezzuto, A.; Ricci, A.; D’Ascanio, M.; Moretta, A.; Tonini, G.; Calabrò, N.; Minoia, V.; Pacini, A.; De Paolis, G.; Chichi, E.; et al. Short-Term Benefits of Smoking Cessation Improve Respiratory Function and Metabolism in Smokers. Int J Chron Obstruct Pulmon Dis 2023, 18, 2861–2865. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Aarsand, R.; Schotte, K.; Han, J.; Lebedeva, E.; Tsoy, E.; Maglakelidze, N.; Soriano, J.B.; Bill, W.; Halpin, D.M.G.; et al. Tobacco and COPD: Presenting the World Health Organization (WHO) Tobacco Knowledge Summary. Respir Res 2024, 25, 338. [Google Scholar] [CrossRef]
- Brassington, K.; Selemidis, S.; Bozinovski, S.; Vlahos, R. Chronic Obstructive Pulmonary Disease and Atherosclerosis: Common Mechanisms and Novel Therapeutics. Clinical Science 2022, 136, 405–423. [Google Scholar] [CrossRef]
- Kotlyarov, S. The Role of Smoking in the Mechanisms of Development of Chronic Obstructive Pulmonary Disease and Atherosclerosis. IJMS 2023, 24, 8725. [Google Scholar] [CrossRef]
- Libby, P. The Changing Landscape of Atherosclerosis. Nature 2021, 592, 524–533. [Google Scholar] [CrossRef]
- O’Dwyer, E.; Halpenny, D.F.; Ginsberg, M.S. Lung Cancer Screening in Patients with Previous Malignancy: Is This Cohort at Increased Risk for Malignancy? Eur Radiol 2021, 31, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Tammemägi, M.C.; Ruparel, M.; Tremblay, A.; Myers, R.; Mayo, J.; Yee, J.; Atkar-Khattra, S.; Yuan, R.; Cressman, S.; English, J.; et al. USPSTF2013 versus PLCOm2012 Lung Cancer Screening Eligibility Criteria (International Lung Screening Trial): Interim Analysis of a Prospective Cohort Study. The Lancet Oncology 2022, 23, 138–148. [Google Scholar] [CrossRef]
- Tammemägi, M.C.; Katki, H.A.; Hocking, W.G.; Church, T.R.; Caporaso, N.; Kvale, P.A.; Chaturvedi, A.K.; Silvestri, G.A.; Riley, T.L.; Commins, J.; et al. Selection Criteria for Lung-Cancer Screening. N Engl J Med 2013, 368, 728–736. [Google Scholar] [CrossRef]
Figure 1.
Odds ratios (ORs) with 95% confidence intervals (CIs) for smoking-related diseases (SRDs) in the study population. The red dashed line indicates the reference value (OR = 1). Asterisks represent statistical significance levels: ***p < 0.001; **p < 0.01; p < 0.05; ns = non-significant.
Figure 1.
Odds ratios (ORs) with 95% confidence intervals (CIs) for smoking-related diseases (SRDs) in the study population. The red dashed line indicates the reference value (OR = 1). Asterisks represent statistical significance levels: ***p < 0.001; **p < 0.01; p < 0.05; ns = non-significant.
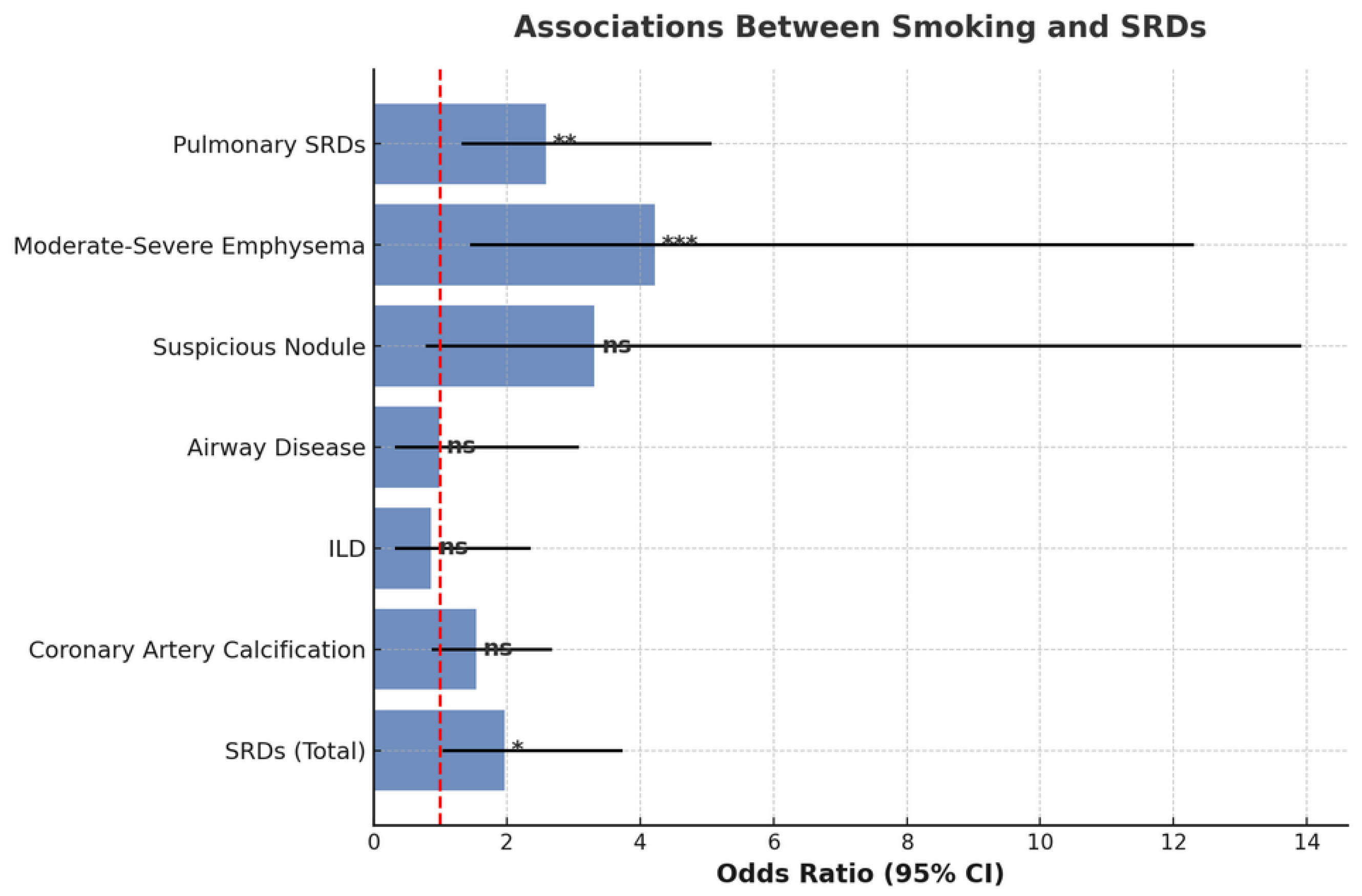
Figure 2.
Severe centrilobular and paraseptal emphysema (grade 1D) in both upper pulmonary lobes in a 67-year-old current male smoker.
Figure 2.
Severe centrilobular and paraseptal emphysema (grade 1D) in both upper pulmonary lobes in a 67-year-old current male smoker.
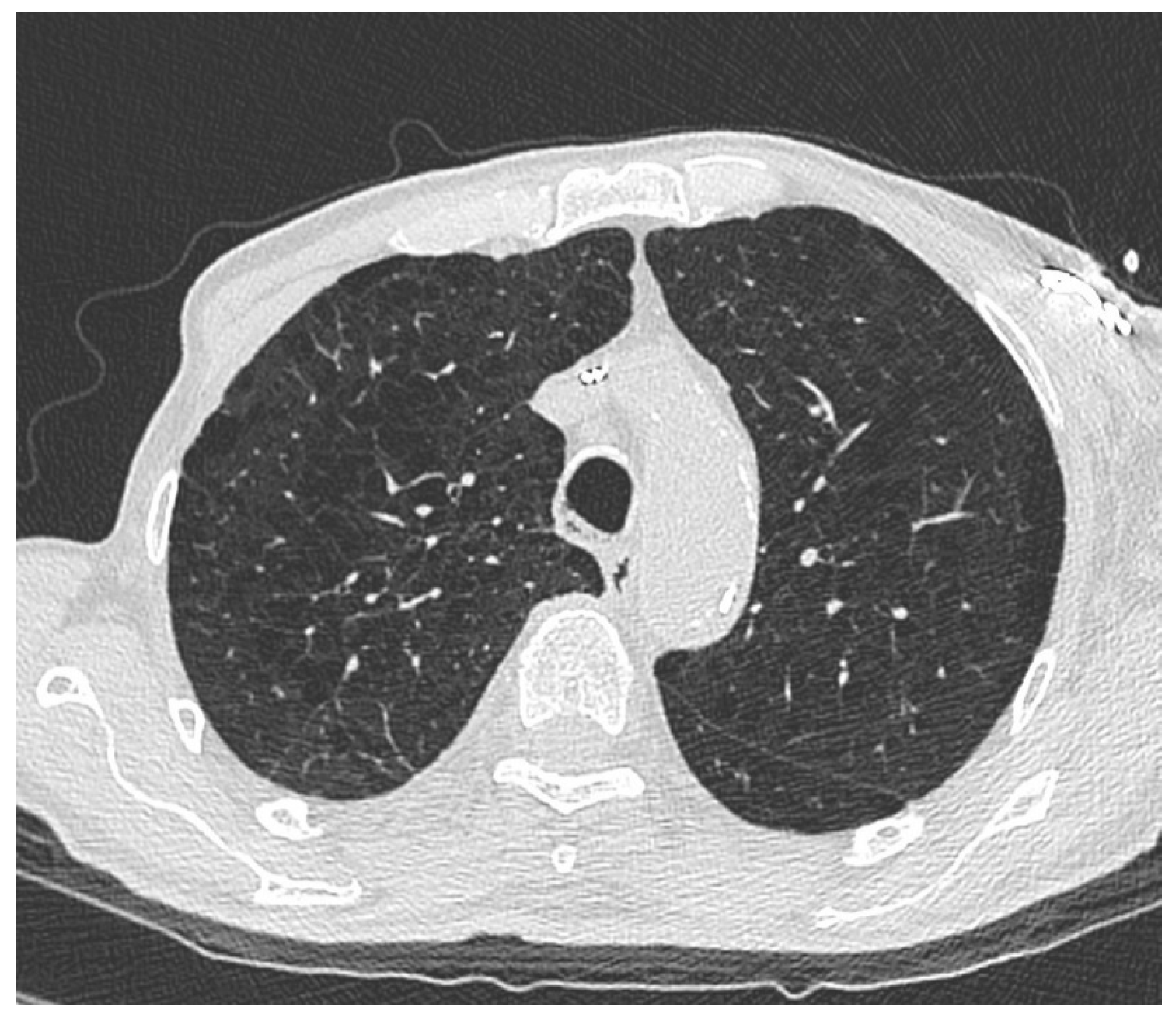
Figure 3.
Suspicious pulmonary nodule in the right upper lobe (20 mm, Lung-RADS 4B) in axial (a) and coronal (b) HRCT scan of a 75-year-old current male smoker.
Figure 3.
Suspicious pulmonary nodule in the right upper lobe (20 mm, Lung-RADS 4B) in axial (a) and coronal (b) HRCT scan of a 75-year-old current male smoker.
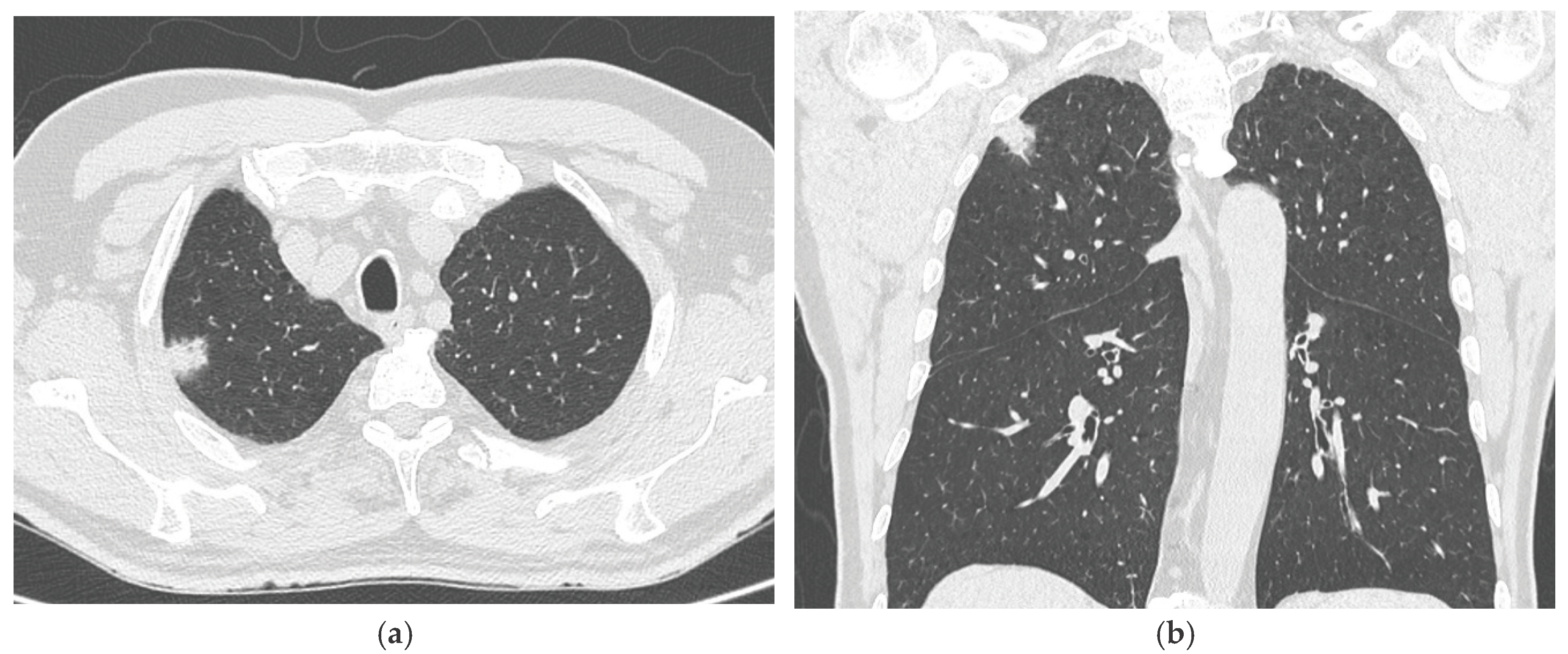

Table 1.
Prevalence and odds ratios (ORs) of smoking-related diseases (SRDs) in patients with histologically confirmed HGBC/MIBC.
Table 1.
Prevalence and odds ratios (ORs) of smoking-related diseases (SRDs) in patients with histologically confirmed HGBC/MIBC.
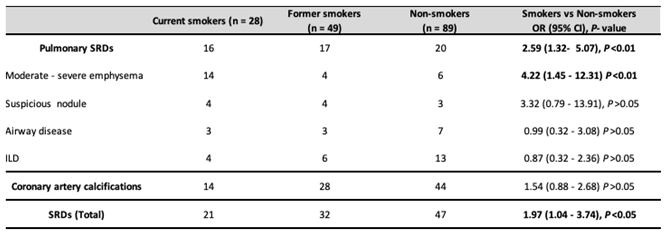 |
Statistically significant results are indicated in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



