
Submitted:
22 September 2025
Posted:
23 September 2025
You are already at the latest version
Abstract
Background/Objectives: The inferior alveolar nerve block (IANB) is widely used for dental anesthesia; however, issues such as anatomical variation and inflammation can hinder effective pain control. Alternatives have been studied primarily in irreversible pulpitis, with limited data available for other procedures. Methods: In a retrospective analysis, data from 85 patients who underwent implantation, root resection, or osteotomy using QuickSleeper® intraosseous anesthesia (IO), infiltration (INF), or IANB were assessed. Results: IO, IANB, and INF produced similar pain levels during administration, procedure, and recovery; blood pressure and heart rate were comparable. IO and INF led to less lip numbness after 15 minutes and required less anesthetic. IO had a significantly shorter latency than IANB, allowing earlier surgery. Conclusions: Computer-guided IO is a viable alternative to IANB for implantation, root resection, and osteotomy, offering equal pain control, shorter latency, earlier surgery, and reduced injection volume.
Keywords:
anesthesia
; dental
; anesthetics
; local
; nerve block
; mandibular nerve
; pain perception
; dental implantation
; endosseous
; oral surgery
; articaine
; adverse effects
; humans
Introduction
Local anaesthesia is essential in modern dentistry, providing pain-free diagnostic and therapeutic procedures. Effective anesthesia improves patient comfort, cooperation, and treatment outcomes. However, the conventional inferior alveolar nerve block (IANB) can be challenging due to anatomical variability, inflammation, patient anxiety, or the operator's experience. Side effects include pain at the injection site, swelling, limited mouth opening, soft tissue injuries, and prolonged numbness. To address these challenges, alternative anesthesia techniques have been developed, such as buccal infiltration, Gow-Gates, closed-mouth nerve block, INF, intrapulpal injection, and intraosseous anesthesia (IO). Computer-guided systems, such as QuickSleeper®, facilitate IO delivery. Previously, we compared Anesto® IO with conventional methods in patients with irreversible pulpitis. Here, we compare IANB, INF, and Quicksleeper® IO in patients undergoing implantation, root resection, and osteotomy.
Materials and Methods
Study Design
This study was designed as a retrospective study using a convenience sample of consecutive patients in our practice. This study was authorized by the Committee for Ethics, Dresden University of Technology, Carl Gustav Carus, Case Ref. no: BO-EK- 389082022. All patients were informed thoroughly about the study and provided written informed consent. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Patients were seen between February 2022 and February 2024 at our dental clinic in Germany for implantation, root resection, and osteotomy procedures. A total of 85 patients were included in the study. The average age of the patients was 52.6 ± 19.9 years. 27 (31.8%) were male, the remainder were female (n=58, 68.2%). 12 patients (14.1%) used nicotine products, and 16 (18.8%) had preexisting cardiovascular disease. Distal teeth were present in 67 patients (78.8%).
The patients were undergoing implantation, root resection, or osteotomy, with some patients undergoing multiple procedures on different dates. Local anaesthesia methods were chosen for each procedure by the treating dentist, in accordance with clinical considerations and in consideration of the patient's wishes (IANB, INF, IO). Computer-guided IO was carried out using the QuickSleeper5 (Orcos Medical, Küsnacht, Switzerland) according to the manufacturer's instructions. For all procedures, we used 1.7 mL of articaine hydrochloride with 1:100,000 epinephrine hydrochloride (Ultracain D-S, Sanofi-Aventis, Frankfurt, Germany). Table 1 shows the number of procedures and anaesthesia methods employed. The location of the procedure in the lower or upper jaw is shown in Table 2.
Statistics
Statistical analysis was performed using the SPSS program (IBM, Armonk, NY, USA). Differences in categorical data were tested for significant difference using the Chi-square test, while continuous data were tested using the paired T-test.
Results
In all procedures, one or two perforations were required. Fewer patients in the IO and INF groups needed two perforations than in the IANB group; this difference reached statistical significance only in the comparison between IANB and INF (IO vs IANB, p = 0.0744; INF vs IANB, p = 0.0021, chi-square test). There was no significant difference in perforation between IO and INF (p = 0.0841).

Table 3.
Number of perforations for the main procedure according to anesthesia method.
| Number of Perforations | IO N=66 (%) | IANB N=43 (%) | INF N=37 (%) |
| 1 | 45 (68.2) | 22 (51.2) | 31 (83.8) |
| 2 | 21 (31.8) | 21 (48.8) | 6 (16.2) |
Table 3. Number of perforations required for the main procedure, comparing intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Needle obstruction was infrequent and occurred at similar rates for all anesthesia methods (Table 4, p > 0.05).
Needle changes were rare across all procedures and showed no significant difference between anesthesia methods (Table 5).
Lip numbness was common with IANB but rare with IO or INF at 15 minutes post-injection (Table 6). Differences between IANB and both IO and INF were statistically significant (p<0.0001).
Lip numbness rates were similar for IO and INF (p = 0.1706). Additional injections were needed in 14.0% to 21.6% of procedures, with no significant differences between anesthetic methods (Table 7, p > 0.005).
The IANB group received a significantly larger injection volume than the IO or INF groups (Figure 1, p < 0.001), with no volume difference between the IO and INF groups (p = 0.145). IO enabled a significantly earlier start compared to IANB (Figure 2, p<0.001), and showed no significant timing difference compared to INF (p = 0.140).
The difference in the start of the procedure after injection, when c omparing IANB and INF, was also not statistically significant (p = 0.078). The injection time was the same for all three local anaesthesia methods (Figure 3, p > 0.005, respectively). The latency of anesthesia was longest for IANB, with p-values of p < 0.001 for the comparison between IO and IANB and p = 0.017 for IANB and INF (Figure 4). There was no significant difference in latency of anaesthesia between IO and INF (p=0.605).
Patient-reported 10. point visual analogue scale, was compared for pain during infiltration, perforation, instillation, treatment, post-surgery, and one day post-surgery. There was no significant difference in these pain levels between IO, IANB, and INF (Table 8).
Other patient stress level-associated parameters that were compared between IO, IANB, and INF included systolic and diastolic blood pressure, as well as heart rate. The values were similar for all three anaesthesia types with no significant differences (Table 9).
Discussion
Local anaesthesia is an essential part of dentistry, with IANB being the most commonly used method [6]. However, due to various factors, reaching sufficient depths of anaesthesia using IANB can be challenging in some patients, and alternative anaesthesia methods have been investigated [4]. Typically, the success rate of IANB is around 70-90%. However, inflammation in the injection area and pulpitis severely reduce its efficacy [7,8,9,10,11].
Comparisons of the anesthetic efficacy of IANB with other local anaesthesia methods have been published [12,13,14]. However, published comparisons between IANB and IO, including a study conducted by our group, are limited to the treatment of irreversible symptomatic pulpitis [5,15,16]. Here, we compared IO, IANB, and INF as anaesthesia methods for implantation, root resection, and osteotomy procedures. All three anesthesia methods were comparable with respect to the number of perforations, needle obstructions, and the necessity of a needle change or additional injections, with only INF showing a slight, but statistically significant, lower average number of perforations.
Soft tissue numbness is a common side effect of local anesthesia in dental procedures and can lead to soft tissue injury due to bites or burns, especially in children [17,18]. In our comparison, lip numbness at 15 min was significantly more common in IANB. Local anaesthesia with a lower incidence or shorter duration of lip numbness might be a better choice for vulnerable populations such as children or people with developmental disabilities. The result might therefore indicate that both IO and INF might be better suited for these populations. A smaller injection volume used in both INF and IO compared to IANB might further contribute to its better suitability for vulnerable populations. However, the ultimate test for any anesthetic is the patient's perception of pain [19,20,21,22,23].
Our results for pain control during treatment and after the surgery showed comparable results for all three methods [8,12,14,15,16,17,24,25,26]. Other researchers have reported better efficacy for IO compared to IANB in the past . However, in the study by Farhad et al. (2018), the anesthetic was used on patients with irreversible pulpitis, a condition that is notorious for being associated with lower efficacy of IANB [8,16]. Pain during anesthesia administration was also comparable among the three methods, with a slightly lower average number for IO. However, there was a relatively high inter-patient variability, which might have contributed to the fact that significance levels were not reached.
Conclusion
Other measures indicating increased patient stress, such as systolic and diastolic blood pressure and heart rates, were also comparable among IO, IANB, and INF, indicating that the efficacy of these anesthetic methods was similar when treating patients undergoing implantation, root extraction, or osteotomy. Shorter overall procedures might be perceived as more comfortable by the patients. Therefore, an anaesthesia method with shorter latency and shorter waiting time to start surgery might be a better option when other parameters are similar. IO had the shortest latency and earliest start of the surgery while displaying similar efficacy, injection time, and pain during anaesthesia administration.
Our study using computer-assisted IO, IANB, and INF as local anaesthesia for implantation, root extraction, and osteotomy yielded similar pain control and patient stress levels for all three methods. The injection volume was lower for IO and INF compared to IANB, with shorter latency and earlier surgery start times, making IO a viable alternative to the standard IANB, with the potential benefit of shorter procedure times.
Author Contributions
M.H.N.: Conceptualization, methodology, validation, formal analysis, data curation, visualization, original draft preparation, writing—review, editing. M.N.: Conceptualization methodology, investigation, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Committee for Ethics, Dresden University of Technology, Carl Gustav Carus’ (protocol code BO-EK-389082022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data is not publicly available due to privacy restrictions.
Acknowledgments
The authors thank the staff of Niliusklinik for their assistance in data collection.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Abbreviations
| bpm | beats per minute |
| IANB | inferior alveolar nerve block |
| INF | infiltration anaesthesia |
| IO | computer-guided intraosseous anaesthesia |
| RR dia | diastolic blood pressure (mmHg) |
| RR sys | systolic blood pressure (mmHg) |
| SPSS | Statistical Package for the Social Sciences |
| StD | standard deviation |
References
- Akhtar, N.; Brizuela, M.; Stenhouse, P.D.; Local anesthetic drugs used in dentistry [Internet]. StatPearls Publishing; 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK610935/ (accessed on 19 August 2025).
- Bartholomew, O.; Hogden, C.; Randall, C.L.; et al. Challenges in achieving profound local anesthesia: Insights from a patient survey. J Am Dent Assoc. 2025, 156, 530–7. [Google Scholar] [CrossRef] [PubMed]
- Helmy, R.H.; Zeitoun, S.I.; El-Habashy, L.M. Computer-controlled intraligamentary local anesthesia in extraction of mandibular primary molars: Randomized controlled clinical trial. BMC Oral Health. 2022, 22, 594. [Google Scholar] [CrossRef]
- Lee, C.R.; Yang, H.J. Alternative techniques for failure of conventional inferior alveolar nerve block. J Dent Anesth Pain Med. 2019, 19, 125–34. [Google Scholar] [CrossRef]
- Nilius, M.; Mueller, C.; Nilius, M.H.; et al. Intraosseous anesthesia in symptomatic irreversible pulpitis: Impact of bone thickness on perception and duration of pain. J Dent Anesth Pain Med. 2020, 20, 367–74. [Google Scholar] [CrossRef]
- Johnson, T.M.; Badovinac, R.; Shaefer, J. Teaching alternatives to the standard inferior alveolar nerve block in dental education: Outcomes in clinical practice. J Dent Educ. 2007, 71, 1145–52. [Google Scholar] [CrossRef]
- Jung, I.Y.; Kim, J.H.; Kim, E.S.; et al. An evaluation of buccal infiltrations and inferior alveolar nerve blocks in pulpal anesthesia for mandibular first molars. J Endod. 2008, 34, 11–3. [Google Scholar] [CrossRef]
- Kanaa, M.D.; Whitworth, J.M.; Meechan, J.G. A prospective randomized trial of different supplementary local anesthetic techniques after failure of inferior alveolar nerve block in patients with irreversible pulpitis in mandibular teeth. J Endod. 2012, 38, 421–5. [Google Scholar] [CrossRef] [PubMed]
- Shakoui, S.; Ghodrati, M.; Ghasemi, N.; et al. Anesthetic efficacy of articaine/epinephrine plus mannitol in comparison with articaine/epinephrine anesthesia for inferior alveolar nerve block in patients with symptomatic irreversible pulpitis: A randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospects. 2019, 13, 321–6. [Google Scholar] [CrossRef]
- Wong, M.K.; Jacobsen, P.L. Reasons for local anesthesia failures. J Am Dent Assoc. 1992, 123, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Forbes, W.C. How to treat a difficult-to-anesthetize patient: Twelve alternatives to the traditional inferior alveolar nerve block. Todays FDA. 2010, 22, 27–33. [Google Scholar]
- Aggarwal, V.; Singla, M.; Kabi, D. Comparative evaluation of anesthetic efficacy of Gow-Gates mandibular conduction anesthesia, Vazirani-Akinosi technique, buccal-plus-lingual infiltrations, and conventional inferior alveolar nerve anesthesia in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010, 109, 303–8. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Aly Ahmed, H.M.; Pulikkotil, S.J.; et al. Anesthetic efficacy of Gow-Gates, Vazirani-Akinosi, and mental incisive nerve blocks for treatment of symptomatic irreversible pulpitis: A systematic review and meta-analysis with trial sequential analysis. J Endod. 2019, 45, 1175–83. [Google Scholar] [CrossRef]
- Goldberg, S.; Reader, A.; Drum, M.; et al. Comparison of the anesthetic efficacy of the conventional inferior alveolar, Gow-Gates, and Vazirani-Akinosi techniques. J Endod. 2008, 34, 1306–11. [Google Scholar] [CrossRef]
- Gaudin, A.; Clouet, R.; Boëffard, C.; et al. Comparing intraosseous computerized anesthesia with inferior alveolar nerve block in the treatment of symptomatic irreversible pulpitis: A randomized controlled trial. Int Endod J. 2023, 56, 922–31. [Google Scholar] [CrossRef]
- Farhad, A.; Razavian, H.; Shafiee, M. Effect of intraosseous injection versus inferior alveolar nerve block as primary pulpal anesthesia of mandibular posterior teeth with symptomatic irreversible pulpitis: A prospective randomized clinical trial. Acta Odontol Scand. 2018, 76, 442–7. [Google Scholar] [CrossRef]
- Brizuela, M.; Daley, J.O.; Inferior alveolar nerve block. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK564368/ (accessed on 27 August 2025).
- Tiwari, A. A traumatic ulcer caused by accidental lip biting following topical anesthesia: A case report. Cureus. 2023, 15, e38316. [Google Scholar] [CrossRef] [PubMed]
- Schmoeckel, J.; Mustafa Ali, M.; Wolters, P.; et al. Pain perception during injection of local anesthesia in pedodontics. Quintessence Int. 2021, 52, 706–12. [Google Scholar]
- Renton, T. Optimal local anesthesia for dentistry. Prim Dent J. 2019, 7, 51–61. [Google Scholar] [CrossRef]
- Solow, R.A. Local anesthesia for restorative dentistry. Gen Dent. 2014, 62, 18–20. [Google Scholar]
- Clark, T.M.; Yagiela, J.A. Advanced techniques and armamentarium for dental local anesthesia. Dent Clin North Am. 2010, 54, 757–68. [Google Scholar] [CrossRef]
- Matsuda, S.; Yoshida, H.; Yoshimura, H. A preliminary study on the assessment of pain using figures among patients administered with dental local anesthesia for mandibular third molar extraction. Medicine (Baltimore). 2023, 102, e34598. [Google Scholar] [CrossRef] [PubMed]
- Kary, A.L.; Gomez, J.; Raffaelli, S.D.; et al. Preclinical local anesthesia education in dental schools: A systematic review. J Dent Educ. 2018, 82, 1059–64. [Google Scholar] [CrossRef]
- Ogle, O.E.; Mahjoubi, G. Advances in local anesthesia in dentistry. Dent Clin North Am. 2011, 55, 481–99. [Google Scholar] [CrossRef] [PubMed]
- Bourke, K. Intra-osseous anaesthesia. Dent Anaesth Sedat. 1974, 3, 13–6. [Google Scholar] [PubMed]
Figure 1.
Mean injection volume (mL) for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation (StD). Significant differences between IANB and both IO and INF are indicated (p < 0.001).
Figure 1.
Mean injection volume (mL) for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation (StD). Significant differences between IANB and both IO and INF are indicated (p < 0.001).
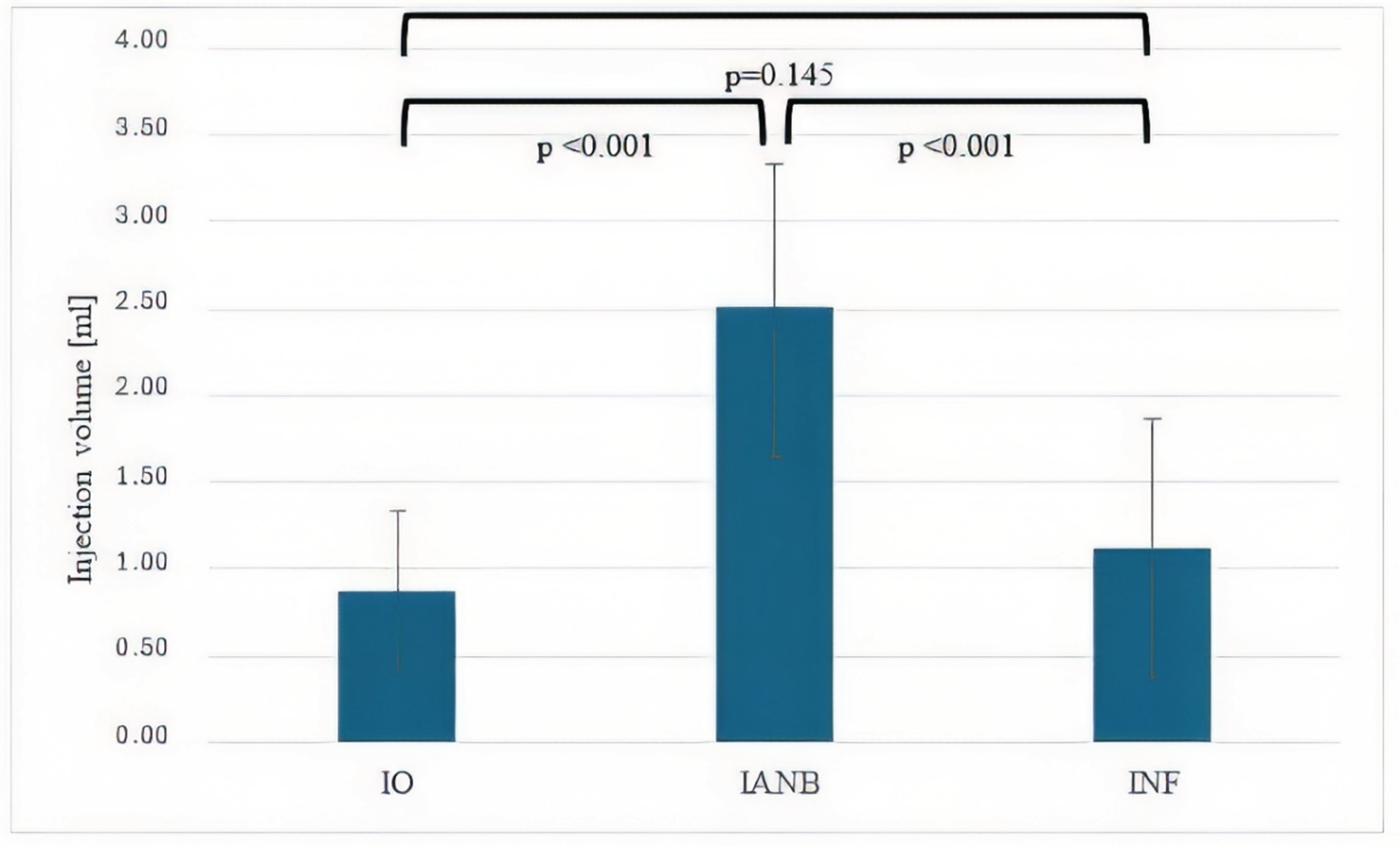
Figure 2.
Mean time (minutes) from anesthesia administration to the start of surgery for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation (StD). IO enabled significantly earlier procedure start compared with IANB (p < 0.001).
Figure 2.
Mean time (minutes) from anesthesia administration to the start of surgery for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation (StD). IO enabled significantly earlier procedure start compared with IANB (p < 0.001).
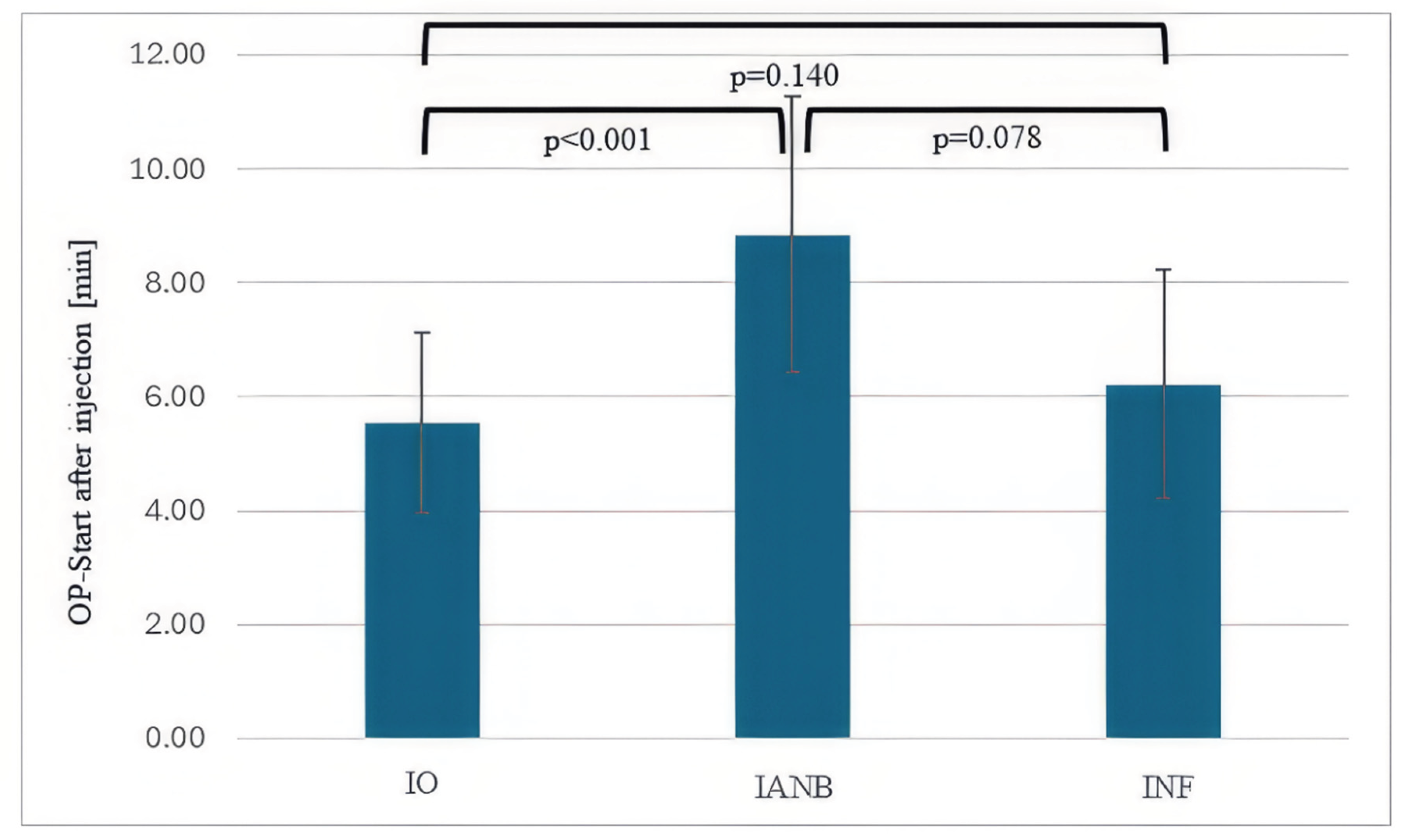
Figure 3.
Mean injection time (minutes) for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation (StD). No statistically significant differences were observed between the three techniques.
Figure 3.
Mean injection time (minutes) for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation (StD). No statistically significant differences were observed between the three techniques.
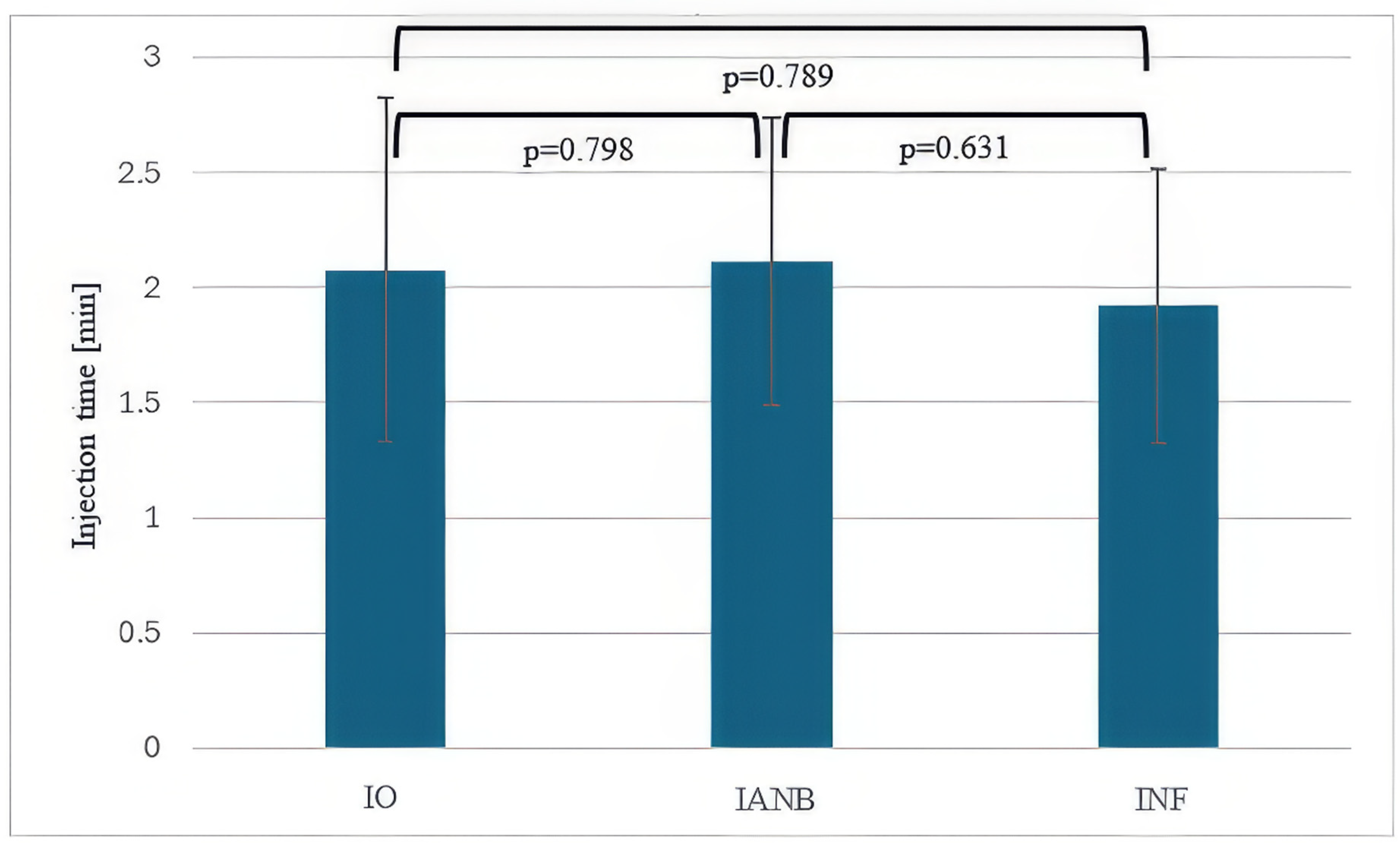
Figure 4.
Mean latency of anesthesia onset (minutes) for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation. Latency was significantly longer for IANB compared with IO (p < 0.001) and INF (p = 0.017).
Figure 4.
Mean latency of anesthesia onset (minutes) for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF). Error bars represent standard deviation. Latency was significantly longer for IANB compared with IO (p < 0.001) and INF (p = 0.017).
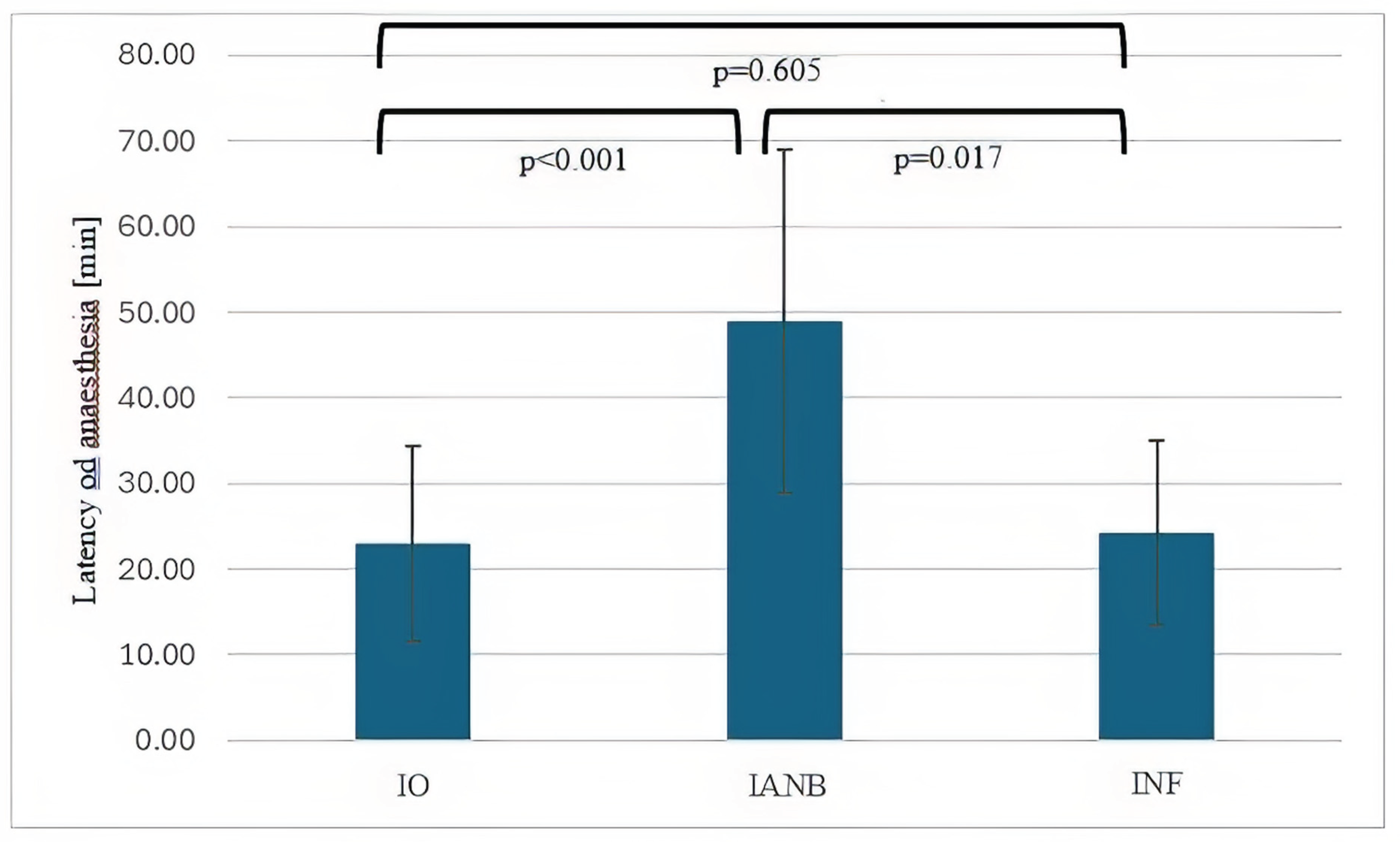
Table 1.
Surgical procedures and anesthesia methods used in 85 patients.
| Surgical procedure | IO N=66 (%) |
IANB N=43 (%) |
INF N=37 (%) |
Total N=85 |
| Osteotomy | 28 (42.4) | 20 (46.5) | 17 (45.9) | 65 (76.5) |
| Implantation | 29 (43.9) | 20 (46.5) | 12 (32.4) | 61 (71.8) |
| Root resection | 9 (13.6) | 3 (7.0) | 8 (21.6) | 20 (23.5) |
Table 1. Distribution of surgical procedures (osteotomy, implantation, and root resection) according to anesthesia method used: intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), or infiltration anesthesia (INF).
Table 2.
Location of surgical procedures in the upper or lower jaw.
| Location | IO N=66 (%) | IANB N=43 (%) | INF N=37 (%) | Total N=85 |
| Maxilla | 29 (43.9) | 5 (11.6) | 29 (78.4) | 65 (76.5) |
| Mandible | 37 (56.1) | 38 (88.4) | 8 (21.6) | 61 (71.8) |
Table 2. Location of surgical procedures in the maxilla or mandible stratified by anesthesia method: intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), or infiltration anesthesia (INF).
Table 4.
Occurrence of needle obstruction.
| Needle obstruction | IO N=66 (%) | IANB N=43 (%) | INF N=37 (%) |
| No | 57 (86.4) | 40 (93.0) | 33 (89.2) |
| Yes | 9 (13.6) | 3 (3.5) | 4 (10.8) |
Table 4. Occurrence of needle obstruction during intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Table 5.
Necessity of needle change.
| Needle change | IO N=66 (%) | IANB N=43 (%) | INF N=37 (%) |
| No | 58 (87.9) | 41 (95.3) | 34 (91.9) |
| Yes | 8 (12.1) | 2 (2.4) | 3 (8.1) |
Table 5. Necessity of needle change during intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Table 6.
Frequency of lip numbness 15 minutes after injection.
| Lip numbness | IO N=66 (%) | IANB N=43 (%) | INF N=37 (%) |
| No | 57 (86.4) | 9 (20.9) | 28 (75.7) |
| Yes | 9 (13.6) | 34 (79.1) | 9 (24.3) |
Table 6. Frequency of lip numbness 15 minutes after injection with intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Table 7.
Frequency of additional injections required.
| Additional injections | IO N=66 (%) | IANB N=43 (%) | INF N=37 (%) |
| No | 55 (83.3) | 37 (86.0) | 29 (78.4) |
| Yes | 11 (16.7) | 6 (14.0) | 8 (21.6) |
Table 7. Frequency of additional injections required during intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Table 8.
Average patient-reported pain scores (10-point visual analogue scale).
| Pain | IO Mean (StD) N=66 | IANB Mean (StD) N=43 |
INF Mean (StD) N=37 | P-value | P-value | P-value |
| Pain | IO Mean (StD) N=66 | IANB Mean (StD) N=43 |
INF Mean (StD) N=37 | IO vs. IANB | IO vs. INF |
IANB vs. INF |
| Infiltration | 2.19 (0.69) | 2.43 (0.77) | 2.33 (1.02) | 0.661 | 0.452 | 0.592 |
| Perforation | 2.41 (0.76) | 3.49 (7.01) | 4.52 (9.32) | 0.336 | 0.274 | 0.974 |
| Instillation | 2.49 (0.65) | 2.49 (0.65) | 2.67 (0.84) | 1.0 | 0.135 | 0.421 |
| Treatment | 1.11 (0.31) | 1.13 (0.06) | 1.11 (0.22) | 0.324 | 1.0 | 0.98 |
| Post surgery | 1.41 (0.50) | 1.46 (0.51) | 1.19 (0.40) | 0.160 | 0.162 | 0.96 |
| 1-day post-surgery | 1.57 (0.50) | 1.62 (0.08) | 1.57 (0.51) | 0.161 | 1.0 | 0.331 |
Table 8. Average patient-reported pain scores (10-point visual analogue scale) during infiltration, perforation, instillation, treatment, post-surgery, and one day post-surgery for intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Table 9.
Average systolic/diastolic blood pressure and heart rate.
| Pain | IO Mean (StD) N=66 | IANB Mean (StD) N=43 | INF Mean (StD) N=37 | P-value | P-value | P-value |
| Pain | IO Mean (StD) N=66 | IANB Mean (StD) N=43 | INF Mean (StD) N=37 | IO vs. IANB | IO vs. INF |
IANB vs. INF |
| (RR sys mmHg) | 141 (18) | 143 (19) | 142 (14) | 0.298 | 0.558 | 0.400 |
| (RR dia mmHG) | 76 (10) | 74 (8) | 74. (4) | 0.647 | 0.307 | 1.0 |
| Heart rate (bpm) | 80 (21) | 84 (22) | 81 (9) | 0.878 | 0.934 | 0.799 |
Table 9. Average systolic (RR sys) and diastolic blood pressure (RR dia) in mmHg and heart rate (bpm) measured during procedures using intraosseous anesthesia (IO), inferior alveolar nerve block (IANB), and infiltration anesthesia (INF).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



