
Submitted:
23 May 2025
Posted:
26 May 2025
You are already at the latest version
Abstract
Background and objectives: Post-operative pain (POP) is a common complication after root canal treatment and is influenced by various clinical and patient-related factors. The present study evaluated the incidence and intensity of POP following root canal treatment using a bioceramic sealer, performed by operators with different levels of experience. Material and methods: A total of 115 patients were included in this prospective observational study. Patients were treated by operators with different levels of experience: postgraduate students (PGSs) and endodontic specialists (ESs). Standardized protocols were used in two distinct appointments: an instrumentation visit and an obturation visit. Obturation was performed using the continuous wave condensation technique and Total Fill Hi-Flow BC Sealer (TFHF). POP, mastication discomfort, and sleep disturbance were assessed at 24, 48, and 72 hours after the instrumentation and obturation phases using a numeric rating scale (NRS). Results: The results indicate significantly higher POP after the instrumentation phase, compared to the obturation phase (p < 0.001). The pain intensity progressively decreased over time for both phases. No significant differences were observed between the PGS and ES groups regarding POP, mastication discomfort, or sleep disturbance at any time. Sealer extrusion did not significantly impact POP (p > 0.05). Conclusions: This study found that operator experience does not significantly influence POP when a standardized protocol is followed. The use of TFHF with the continuous wave condensation technique was associated with minimal POP.
Keywords:
bioceramic sealer
; calcium silicate sealer
; operator experience
; postgraduate student
; endodontic obturation
1. Introduction
Root canal treatment is a procedure aimed at retaining the tooth through the treatment of dental pulp and peri-radicular diseases [1]. Endodontic pathologies are recognized to have a prevalence comparable to that of other dental disorders. Therefore, endodontology postgraduate training is needed for clinicians to provide high-quality care for patients undergoing endodontic therapy [2].
Post-operative pain (POP) is an unpleasant but frequent complication after root canal therapy. A systematic review has shown that POP has a prevalence of 3 to 58% in the investigated cases [3], while a clinical trial reported up to 19% of patients experiencing severe pain [4]. The anticipation and handling of POP is an essential part of the endodontic treatment, as it may be a stressful factor for both the patient and operator, and may require an unscheduled emergency appointment [3]. When pain occurs following treatment, it may hinder the trust of the patient towards the operator, even if it does not influence the long-term outcome [5]. A randomized clinical trial reported that sometimes POP can exceed the pre-operative level of pain [6]. This may be due to the progress of the inflammatory process due to apical instrumentation [7], as well as chemical or microbial injuries of periapical tissues [8]. Patient-related factors like initial diagnosis [9,10,11] or tooth type [4,12] and treatment-related factors like the number of visits [13,14,15,16], instrumentation or obturation techniques [17,18,19,20], or obturation material [21,22] are linked to POP.
Among root canal obturation techniques, warm vertical compaction using the continuous wave of condensation (CWC) technique is generally preferred by endodontists [23]. CWC softens and alters the gutta-percha phase, allowing a better fit to the root canal wall with fewer voids, and fewer radiographic translucencies [23,24,25].
The use of bioceramic sealers has become popular among operators due to their advantages such as bioactivity-enhancing periapical healing and biocompatibility [26]. A systematic review concluded that bioceramic sealers have good biological and physico-chemical properties, when compared to conventional sealers [27], with a retrospective analysis reporting an overall success rate of 90.9% [28]. Calcium silicate-based sealers were primarily developed for cold obturation techniques [29]. Consequently, Total Fill Hi-Flow BC Sealer(TFHF)—a pre-mixed and pre-loaded injectable sealer—was developed to allow the use of warm obturation techniques alongside bioceramic sealers [30], with better in vitro results compared to Total Fill BC Sealer [31].
A meta-analysis of nine randomized clinical trials showed that post-operative pain (POP) was significantly lower after root canal obturation with calcium silicate-based sealers, compared to resin-based sealers [32]; however, when compared directly, studies showed no difference between the two sealer types [33,34].
While several studies have analyzed POP after obturation using bioceramic sealers designed for cold obturation techniques [35,36], to the best of our knowledge, no study has investigated the pain after continuous wave condensation obturation along with TFHF. The operator’s experience has been shown to influence the POP after root canal treatment [4,21,37], but no study has analyzed the influence of the operator’s experience on POP after root canal obturation with bioceramic sealers. The influence of the obturation on POP can be clarified and evaluated by splitting the treatment into two visits and differentiating it from the POP associated with the pre-operative status [10] and the mechanical preparation of the root canal [38].
Therefore, this study aimed to evaluate and compare the incidence and intensity of POP after root canal treatment performed by two groups of operators with different experience levels using THFH and CWC.
The tested research hypotheses will be as follows:
a. There is no difference in the incidence and degree of POP after the instrumentation and obturation phases of root canal treatments performed by postgraduate students and endodontic specialists;
b. Pulpal and periapical diagnosis, case difficulty, and sealer extrusion have no significant effects on POP.
2. Materials and Methods
Patient selection
This prospective observational clinical cohort study was approved by the Ethics Committee of the University of Medicine and Pharmacy “Iuliu Hatieganu” Cluj-Napoca, Romania, under approval number AVZ38 from 12.03.2024. The “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) statement was used in preparing the study report (Table A1) [39]. All participants signed an informed consent form. All methods were performed in accordance with the Declaration of Helsinki.
Patients referred for endodontic treatment to the Endodontics Department of the University of Medicine and Pharmacy of Cluj-Napoca within a period of 12 months were selected for this prospective study. Before treatment, the medical and dental history of the patients was recorded. Gender, age, tooth number, periapical condition, pulp diagnosis, occlusion, and proximal contacts were registered. The exclusion criteria included immunosuppressed patients, patients under 18 or over 75 years old, pregnancy, consumption of antibiotic medication before treatment, teeth with previous root canal treatments, external or internal resorptions, open apexes, and root canals that made it impossible to negotiate to the apical constriction. The required sample size was calculated using G*Power 3.1 software (Kiel, Germany) for a statistical power of 0.8, with a significance threshold of 0.05 and a 0.3 effect size.
A total of 115 patients were considered eligible for this study (Figure 1). The patients were treated (as they presented or were referred to) by three endodontic specialists (ES) with at least 5 years of experience in this field or by three postgraduate students (PGSs) enrolled in the endodontics residency program. No randomization or blinding took place. A total of 59 patients were treated by ESs, while PGSs treated 56 patients. The treatments were performed in two visits: the instrumentation phase and the obturation phase. This protocol (i.e., in which patients require two visits) is commonly used in the endodontic department where the study took place, and it was used for all patients. Before the beginning of the study, a presentation was held for calibration, and training regarding the protocol was performed on extracted teeth by both ESs and PGSs. All of the PGSs were supervised by an operator accustomed to the protocol but did not interfere with the treatment.
2.1. First Visit—Instrumentation Phase
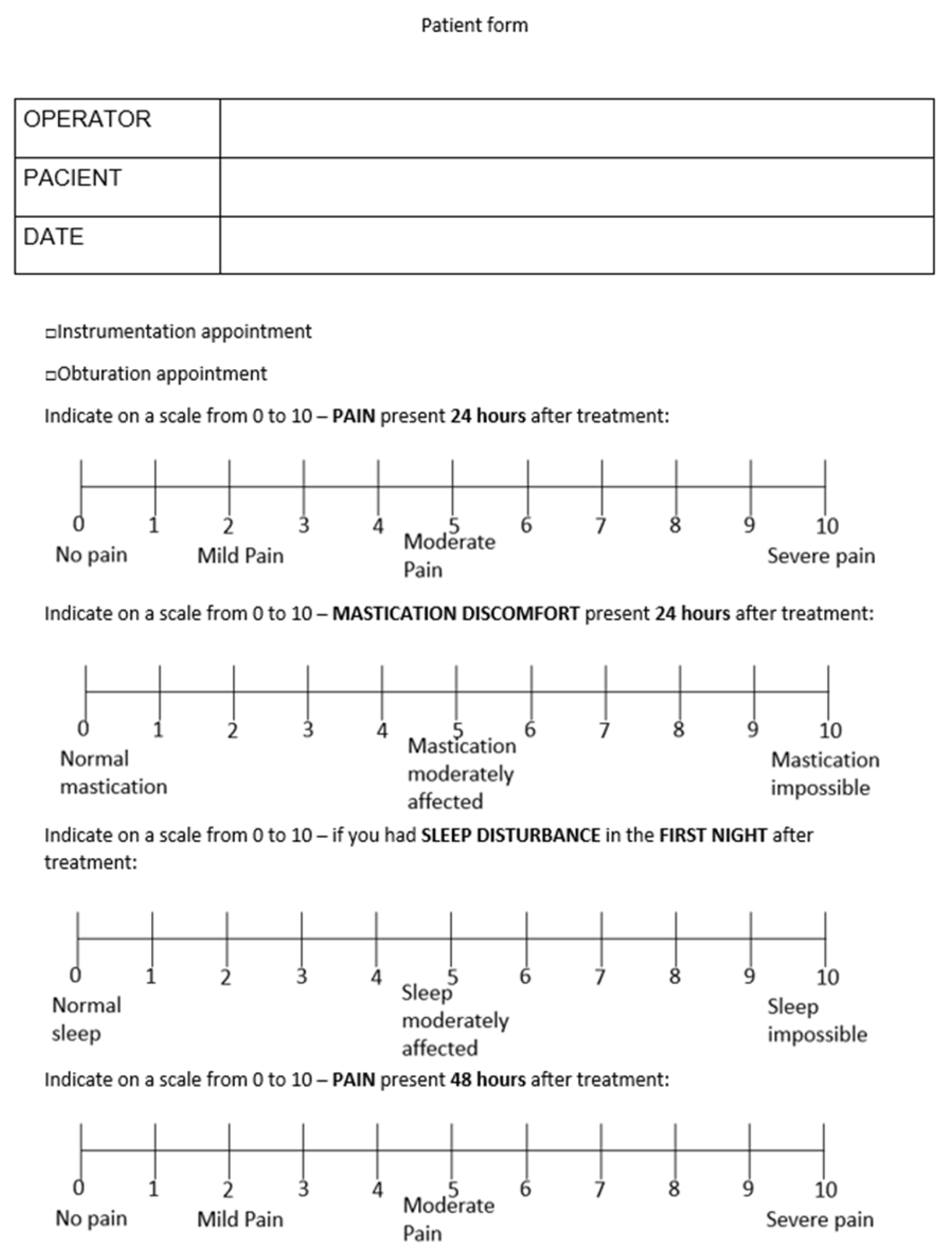
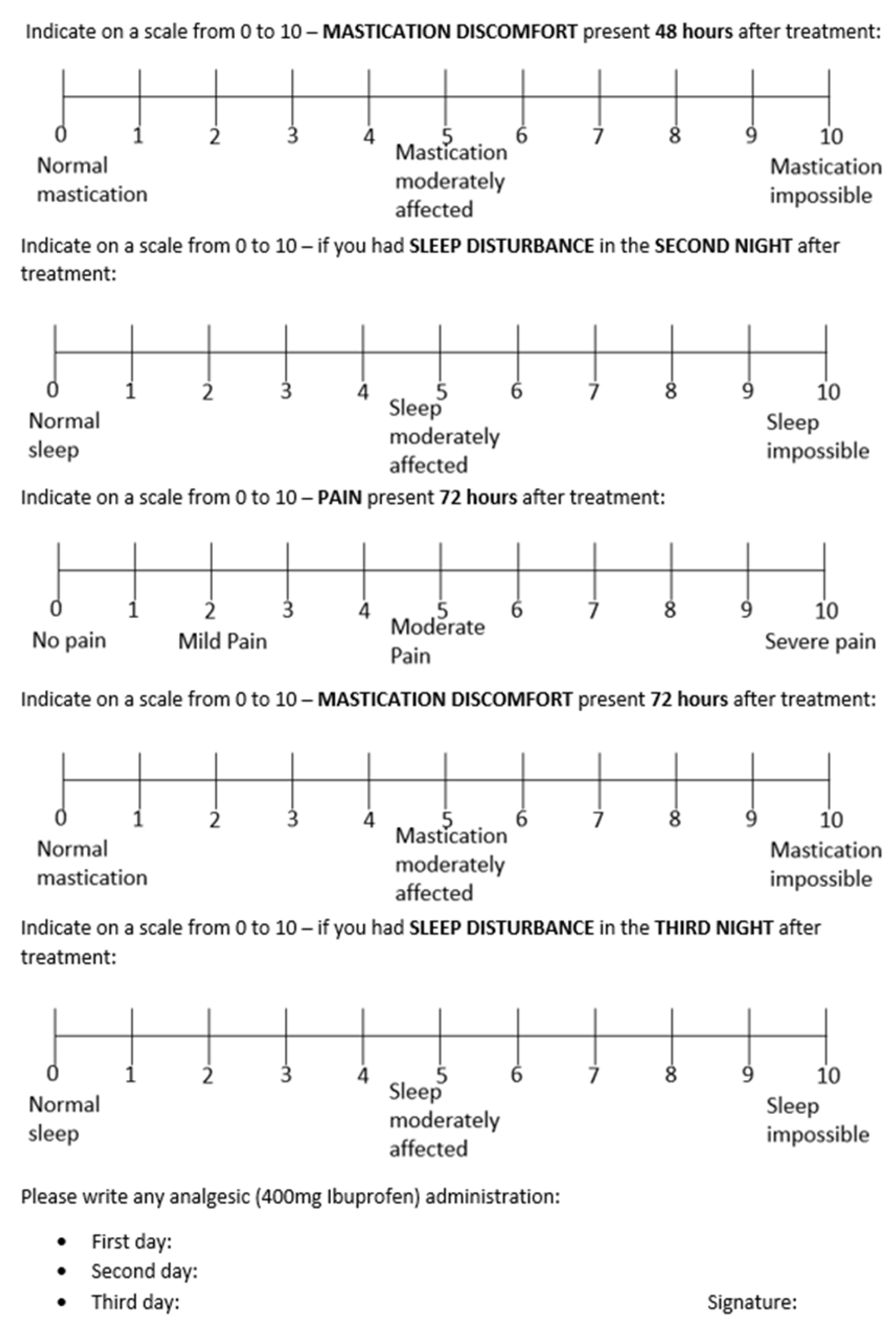
In the first visit, each patient underwent a periapical radiograph examination (Planmeca, Helsinki, Finland), which was analyzed by one of the ESs taking part in this study, and teeth were classified as having lesions of endodontic origin (LEO) when a loss of lamina dura and periodontal ligament enlargement bigger than 2 mm was present [6]. The pulpal status was assessed using the cold test (Cerkamed, Stalowa Wola, Poland) and classified as healthy pulp, reversible pulpitis, irreversible pulpitis, and pulp necrosis [40]. Teeth with reversible pulpitis were excluded from this study. The peri-radicular status was checked using percussion and palpation. The case difficulty was assessed using the American Association of Endodontists (AAE) endodontic case difficulty assessment form [41]. After anesthesia with articaine containing 2% adrenaline (Septodont, Saint Maur des Fosses, France) and rubber dam isolation, the access cavity was prepared using sterile round burs (Edenta, St. Gallen, Switzerland) and Endo-Z burs (Dentsply, Konstanz, Germany). The working length was determined via a 10 K-File (VDW, Munich, Germany) and an apex locator (Root ZX, Morita, Japan), using the middle green line on the display. The Pro Taper Ultimate (Dentsply, Konstanz, Germany) rotary system was used to prepare the root canals mechanically, following the manufacturer’s instructions. Root canal irrigation consisted of 2 ml NaOCl 5.25% (Cerkamed, Stalowa Wola, Poland) between each instrument. Apical patency was checked with a 10 K-File entering 0.5 mm longer than the working length [42]. The root canal was dried with paper points and dressed with temporary calcium hydroxide (Cerkamed, Stalowa Wola, Poland). Then, a sterile cotton pellet was put inside the pulp chamber, and a provisional filling (Coltosol, Coltene, Altstatten, Switzerland) was placed.Each patient received a POP assessment form (Figure A1). If needed, the patients were instructed to administer 400 mg of ibuprofen and record any analgesic administration on the form.
2.2. Second Visit—Obturation Phase
In the second visit, which took place 5 to 14 days after the first one, the current symptomatology of patients was assessed, and those with any degree of symptomatology at the second visit were excluded from the study. Anesthesia was again obtained using articaine containing 2% adrenaline (Septodont, Saint Maur des Fosses, France), and rubber dam isolation was performed. The provisional coronal filling was removed using an ultrasound scaler (Woodpecker, Guilin, China). Root canals were irrigated with 2 ml NaOCl (Cerkamed, Stalowa Wola, Poland), and the working length was reconfirmed using an electronic apex locator (Root ZX, Morita, Japan) and a 15 K-File (VDW, Munich, Germany). The apical diameter was measured with Ni-Ti K Files (Dentsply, Konstanz, Germany) using the following method: the Ni-Ti K File corresponding in size to the last Pro Taper Ultimate rotary file used was tried at the working length; if no resistance and binding sensation was found, the next Ni-Ti K File in size was used until a binding sensation was present [43]. The obturation technique used was the continuous wave condensation (CWC) technique, as described by Buchanan [44]. The corresponding Pro Taper Ultimate gutta-percha cone (Dentsply, Konstanz, Germany) was selected as a master cone and checked for tug-back at the working length, and then 0.5 mm was cut from the tip. Final irrigation consisted of 5 ml EDTA 17% (Cerkamed, Stalowa Wola, Poland), followed by 5 ml NaOCl (Cerkamed, Stalowa Wola, Poland). The root canal was dried using paper cones, and Total Fill BC Hi-Flow (FKG Dentaire, La Chaux-de-Fonds, Switzerland) sealer was applied inside the canal using the master cone. The gutta-percha cone was cut at the level of the root canal orifice using an electrically activated heated plugger (Kerr, Kloten, Switzerland) and condensed with a stainless-steel plugger (Kerr, Kloten, Switzerland). Next, the heat plugger was used to condense the master cone up to 4 to 6 mm shorter than the working length, followed by a pre-fitted stainless steel plugger. Next, backfill was performed using a gutta-percha injection gun (Kerr, Kloten, Switzerland). A provisional filling (Coltosol, Coltene, Altstatten, Switzerland) was placed, and a periapical radiograph was used to check the quality of the root canal (Figure 2). A blinded operator with at least 5 years of experience, who did not participate in patient treatment, assessed the radiographs and classified the outcome as short (>1 mm), adequate (<1 mm), correct, or over-obturation. The patient received a POP assessment form. If needed, the patients were instructed to administer 400 mg of ibuprofen and record any analgesic administration on the form.
2.3. Post-Operative Pain Assessment
Each patient received two forms (Figure A1) for POP assessment: one after the preparation phase and one after the obturation phase. Patients were instructed to mark the pain intensity on a numeric rating scale (NRS) on a horizontal line containing values from 0 to 10 [45]. The values were described as follows: 0, no pain; 1–3, mild pain; 4–6, moderate pain; 7–10, severe pain [45]. All values equal to or higher than 1 were considered as POP presence. Along with the pain intensity, the patient was asked to mark on an NRS the discomfort related to mastication and any degree of sleep disturbance caused by pain. These three indicators were assessed at 24, 48, and 72 hours after the treatment [46].
2.4. Statistical Analysis
One-way repeated analysis of variance (ANOVA) for independent samples was conducted to evaluate differences among groups regarding continuous variables. Tukey and Bonferroni post hoc tests were performed for pairwise comparisons between groups. In the case of categorical variables, the statistical difference was evaluated via the chi-squared test. For all analyses, the threshold for statistical significance was set at p < 0.05. All graphical representations and analyses were performed using the JASP software (JASP Team 2024, JASP version 0.19.0).
3. Results
A total of 103 selected patients were eligible for this study, and 12 patients were eliminated due to symptoms requiring an extra appointment, missed appointments, or failure to return pain assessment forms. The data belonging to excluded patients was removed from the analysis. Table 1 presents the demographic aspects of the two groups.
A total of 33 (32.3%) patients reported no POP after 24 hours from the instrumentation visit for the whole cohort, while 70 (67.6%) complained of POP. Following the obturation phase, 53 (51.9%) patients reported the absence of POP, while the rest experienced POP (Table 2).
POP, mastication discomfort, and sleep disturbance decreased from 24 to 72 h for the whole cohort (Figure 3); thus, the results of Tukey and Bonferroni post hoc tests for the whole cohort showed that the POP, mastication discomfort, and sleep disturbance were significantly higher (p < 0.001) after the instrumentation phase than after the obturation one. When evaluating POP during the three days, it was observed that it progressively diminished from 24 h to 48 h (p < 0.001) and from 48 h to 72 h (p = 0.02) after the instrumentation phase. The same was noticed for the obturation phase, with significant differences for 24 h POP level compared to those registered at 48 h (p < 0.001) and for 48 h compared to 72 h (p < 0.01). Mastication discomfort gradually decreased in both preparation and obturation phases from 24 h to 48 h (p < 0.001) and from 48 h to 72 h (p = 0.02 for the first appointment and p < 0.001 for the second one; Table 3). Significant differences were found between the two appointments for POP and mastication discomfort at 24 h (p < 0.001), 48 h, and 72 h (p < 0.01). The same was observed for sleep disturbance at 24 h (p < 0.01), 48 h, and 72 h (p < 0.05).
POP, mastication discomfort, and sleep disturbance at 24, 48, and 72 hours for the PGS and ES groups are presented in Figures 4a and 4b. The comparison between the PGS and ES groups regarding the instrumentation or obturation phases showed no significant differences for either POP, mastication discomfort, or sleep disturbance for the three days (p > 0.05). The same was observed when comparing results at 24, 48, and 72 hours (p > 0.05).
Within groups, a significant difference was observed in the ES category at 24 h between instrumentation and obturation phases for POP and mastication discomfort (p < 0.01), with the preparation phase having higher values. No difference was found for sleep disturbance. Within the PGS group, all three parameters (POP, mastication discomfort, and sleep disturbance) were significantly (p < 0.05) higher after the instrumentation appointment.
Regarding pre-operative percussion status, a positive response induced a significantly higher POP for all three days following the instrumentation visit (p < 0.001), while, when considering the obturation phase, the percussion test showed no statistical difference for POP (p = 0.67).
No significant differences were found for the two phases regarding the influence of the presence of LEO bigger or smaller than 2 mm on POP, mastication discomfort, or sleep disturbance (p > 0.05). The same was observed for the pulpal status (i.e., vital, pulpitis, or necrosis; p > 0.05).
Regarding sealer extrusion, no significant differences were found after the obturation phase (p = 0.33), regardless of the operator’s experience. Sealer extrusion incidence can be seen in Table 1 and was limited in all cases to the area close to the apical foramen. At the same time, gutta-percha over-obturation happened in 6 cases, all 1 mm or less, while a short obturation was reported only in 1 case. No significant differences (p > 0.05) in POP were observed at 24 h, 48 h, and 72 h after the obturation appointment, regardless of the obturation quality.
Concerning the AAE difficulty, regarding the obturation visit, a moderate difficulty revealed a significantly higher POP (p < 0.01) compared to minimum difficulty for the whole cohort. No differences between high and moderate (p = 0.069) or high and minimum (p = 0.499) difficulty were found. AAE difficulty did not influence the instrumentation visit (p > 0.05). When the PGS and ES groups were compared, no differences (p > 0.05) were found regarding POP, mastication discomfort, or sleep disturbance regarding the influence of the case difficulty in either of the two separate visits.
No differences between tooth types (i.e., anterior, premolar, molar) regarding POP, mastication discomfort, or sleep disturbance were found (p > 0.05).
Regarding analgesics, 20 patients used one dose of 400mg ibuprofen after the instrumentation phase, and 10 after the obturation visit. No significant influence (p > 0.05) was observed on POP evolution for the patients who took analgesics.
4. Discussion
Post-operative discomfort is a potentially distressing factor in endodontics, which sometimes exceeds the pre-treatment level of pain [32]. Our findings contribute to understanding factors influencing POP following endodontic treatment, particularly concerning the influence of operator experience and the choice of obturation materials. No significant differences were observed between the ES and PGS groups regarding the incidence and degree of POP after root canal treatment. Therefore, the first research hypothesis was accepted.
The POP level experienced after root canal treatment has been shown to be affected by a combination of treatment-dependent factors (ability of eliminating the infection/inflammation and of reducing pressure and swelling), including the type of rotary file, shaping techniques, irrigation solutions, and obturation technique used, as well as patient-dependent variables such as age, sex, general health condition (immune response, ability of repairing and regenerating the periapical tissues), pulpal and periapical diagnosis, pre-operative discomfort, and tooth anatomy [19,47].
Several clinical trials have studied POP following obturation with bioceramic sealers reporting similar pain values to those obtained in this study, despite differences in instrumentation and obturation protocols [21,34,48]. Meanwhile, Tan et al. reported a higher percentage of patients with no POP and fewer patients with mild or very mild POP, in contrast to the present study [33]. The reason might be the different POP assessment forms and the use of a single cone technique in Tan et al.’s research.
Endodontic treatment performed in multiple visits, as it was done in the present study, is common and allows for thorough cleaning of complex root anatomies [49]. Two systematic reviews have concluded that it may lead to lower immediate POP and flare-ups [13,15], though several studies have reported no significant differences compared to single-visit treatments[14,16,50]. Instrumentation can cause bacterial extrusion and apical injuries, leading to inflammation and POP. [51]. Different clinical trials have reported that mechanical glidepath [6] and 1.3% NaOCl irrigation could reduce POP [52], while rotary instrumentation was shown in a meta-analysis to exhibit less debris extrusion and lower POP [53].
The pulpal and periapical diagnosis has been demonstrated in other studies to affect the post-treatment pain following the endodontic procedure [9,47]. In our study, only positive percussion—an important procedure for deciding the diagnosis—significantly influenced POP for the instrumentation visit (p < 0.001). Therefore, the second research hypothesis was partially accepted. Tenderness to percussion tests before treatment has been found by several clinical trials to influence the intensity of POP after the instrumentation visit, despite different instrumentation protocols and POP assessment forms [9,11,54]. Regarding the POP following the obturation phase, no difference between positive and negative percussion tests was reported, similar to the results reported by Jang et al [9]. One study has reported no difference in the degree or duration of POP after the endodontic procedure between vital and non-vital teeth, despite dissimilar obturation techniques, confirming the present findings [55]. However, a prospective study using different instrumentation protocols reported that vital pulp might predict a higher POP [56]. In the present study, tooth vitality testing was performed using the cold test because of equipment limitations, even though the electric pulp test was reported to be more accurate in a systematic review [57]. Regarding periapical translucencies, some studies have shown that the presence of a radiolucent lesion might result in higher POP [10,58], while another study found a lower POP when the patients presented radiographic apical translucency [59]. Differences in treatment protocols, definitions of apical lesions, and POP assessment may be the causes for these discrepancies. In the present study, no differences were found when periapical lesions were present or not.
As in other studies [4,9], tooth type (anterior, premolar, or molar) did not influence POP, even though previous findings suggested that molars are associated with higher POP due to their complex root anatomy and increased likelihood of apical tissue disruption during instrumentation and obturation [12,47]. When AAE difficulty was compared in our research, the patients reported higher scores in medium-difficulty cases (compared to minimum difficulty) for the obturation phase, while no difference was observed for the instrumentation phase. Thus, the conflicting results may be due to different study designs and a uniform protocol applied in our study by practitioners with current or completed advanced endodontic training.
The CWC technique used for obturation in the present study was demonstrated to exhibit good dentinal tubule penetration and less void formation, particularly when used with TFHF [24]. However, another study reported that this technique could create thermal injuries in the peri-radicular tissues, produced by the temperature increase on the root surface, thus increasing the incidence of POP [60]. Similar to Ali et al.’s study, in this research, low POP levels were registered when asymptomatic teeth were obturated [20].
Regarding sealer extrusion, different studies have reported no difference in POP between Ah-Plus and Endosequence BC sealers [34,36], or between resin- and calcium silicate-based materials [61]. Although bioceramic sealers seem to exhibit more extrusion than other materials, several investigations have reported no correlation between calcium silicate-based sealer extrusion and POP [33,36,61], as observed in the present study (p > 0.05). In contrast, one prospective clinical trial has reported a direct correlation between sealer extrusion and POP [21]. These different results may be due to differences in study design, treatment protocol, number of visits, or obturation techniques.
When comparing the POP outcomes between the two groups of operators, no significant difference was observed between them (p > 0.05). The clinical implication of these findings could reflect the importance of careful supervision of less-experienced operators, which could minimize the risk of potential mistakes such as over-instrumentation and over-obturation that may lead to higher POP. This may suggest that training programs should instruct trainees to implement a consistent protocol to be used during treatment. The influence of the operator’s experience on the outcome and POP of endodontic treatments has been studied for a long time. A prospective study has reported that undergraduate students had better results in terms of flare-ups than those treated by postgraduate students or specialists, suggesting that the cause might be the longer duration spent cleaning and shaping [62]. In contrast, two studies comparing general dentists and endodontic specialists reported no difference in POP [4,63], while several studies have reported a low POP incidence and good treatment outcomes in treatments performed by postgraduate or undergraduate students [21,64].
The pain assessment in this study was conducted using a numeric rating scale (NRS)—a widely recognized and validated tool for quantifying subjective pain intensity [65]. This method has been shown to provide reliable and reproducible measurements of pain intensity across diverse clinical settings [66]. The simplicity of this scale allowed for the collection of data regarding several symptoms such as POP, mastication discomfort, and sleep disturbance. Assessments were conducted at 24, 48, and 72 hours after each treatment phase, in order to capture the evolution of the pain. This timeframe aligns with established recommendations for monitoring post-operative discomfort in endodontic studies, as the peak of inflammatory response and associated pain typically occurs within the first 24–48 hours [67].
Regarding pre-medication, a clinical trial has reported that the use of non-steroidal anti-inflammatory drugs (NSAIDs) prior to treatment reduced the POP following the endodontic treatment [68]. In the current study, before the obturation visit, no patient took any NSAID. Antibiotic medication has been found not to affect POP in a systematic review [69]; however, we excluded any patient who took antibiotics before the first and second visits.
When interpreting the results of this study, several limitations should be considered. The single-center design of this study may lead to potential biases, such as the characteristics and inadequate blinding of patients and operators, as well as equipment quality, potentially limiting the generalizability of the findings. The non-random allocation may have affected the consistency and comparability of the outcomes. The supervisor’s feedback to PGSs may positively impact the treatment quality. A long-term follow-up would also be necessary to obtain a broader perspective on these findings. The study design focused exclusively on a single type of bioceramic sealer and a specific obturation technique (CWC), which may not fully reflect the diverse clinical scenarios encountered in routine practice. Further, the reliance on patient-reported outcomes introduces a degree of reporting bias. Additionally, factors such as individual pain thresholds, pre-operative anxiety, and variations in anatomical complexity were not fully accounted for. Finally, the study’s exclusion criteria—such as the absence of symptomatic cases at the obturation phase—may not apply to all clinical conditions.
Future research should aim to address the limitations of this study by conducting randomized clinical trials and including multi-center trials to increase the generalizability of findings. Comparative studies exploring different bioceramic sealers, obturation techniques, and instrumentation systems are needed to establish optimal strategies for POP minimization. Additionally, investigations should focus on long-term outcomes, such as periapical healing and re-treatment success, when using bioceramic sealers. These could create a benchmark for proposing clinical guidelines regarding standardized protocols for trainee programs and usual clinical practice. Advanced imaging modalities such as cone-beam computed tomography (CBCT) could enable more precise evaluations of sealer extrusion and obturation quality. Furthermore, the role of adjunctive therapies—including pre-medication with NSAIDs, corticosteroids, or other analgesics—should be explored in greater detail. Studies that integrate patient-specific factors, such as pre-operative anxiety, anatomical variations, and genetic predispositions to pain sensitivity, would enable a more comprehensive understanding of POP in the endodontic context.
5. Conclusions
This study provides important insights into the factors influencing POP. The findings highlight the influence of treatment protocols, materials, and patient-specific factors. Operator experience did not affect POP when standardized protocols were followed. POP was more pronounced after the instrumentation phase than the obturation phase, emphasizing the potential impact of the shaping procedure and apical tissue injuries. Positive percussion influenced POP after the instrumentation phase, but not following the obturation phase, while sealer extrusion and case difficulty had no influence on POP. The use of a bioceramic sealer designed for warm obturation techniques, such as TFHF, demonstrated minimal POP, supporting its application in modern endodontic practice.
Author Contributions
Conceptualization, M.E.B. and A.G.D..; methodology, M.M., M.E.B., and S.I.C..; validation I.C.B.; formal analysis, S.I.C. and M.P.; investigation, M.M., S.I.C., I.S.P.C., R.C.P., O.C., and M.P.; resources, A.G.D.; data curation O.C.; writing—original draft preparation, M.M. and I.S.P.C.; writing—review and editing, M.M., S.I.C., and I.S.P.C; visualization, I.C.B. and R.C.P.; supervision, A.G.D. and M.E.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Medicine and Pharmacy “Iuliu Hatieganu” Cluj-Napoca, Romania (number AVZ38 from 12.03.2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request from the authors due to restrictions (privacy, ethics, patient data).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AAE | American Association of Endodontics |
| ESs | Endodontics specialists |
| CWC | Continuous wave condensation |
| LEO | Lesion of endodontic origin |
| NRS | Numeric rating scale |
| NSAID | Non-steroidal anti-inflammatory drug |
| POP | Post-operative pain |
| PGSs | Postgraduate students |
| SD | Standard deviation |
| TFHF | Total Fill Hi-Flow BC Sealer |
Appendix A

Table A1.
STROBE Statement Checklist – for cohort studies.
| Item No | Recommendation | Article section | |
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | Abstract - material and methods |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | Abstract | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 2nd, 6th paragraph |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 7th, 8th paragraph |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | Patient selection – 1st, 3rd paragraph |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | Patient selection 2nd ;3rd paragraph; Figure 1 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of follow-up | Patient selection – 2nd paragraph; POP assessment form |
| (b) For matched studies, give matching criteria and number of exposed and unexposed | n/a | ||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | First visit; POP assessment form |
| Data sources/ measurement | 8* | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | POP assessment form |
| Bias | 9 | Describe any efforts to address potential sources of bias | Patient selection – 3rd paragraph; Second visit; POP assessment form |
| Study size | 10 | Explain how the study size was arrived at | Patient selection – 3rd paragraph |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | Statistical analysis |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | Statistical analysis |
| (b) Describe any methods used to examine subgroups and interactions | Statistical analysis | ||
| (c) Explain how missing data were addressed | No missing data | ||
| (d) If applicable, explain how loss to follow-up was addressed | Results – 1st paragraph | ||
| (e) Describe any sensitivity analyses | None (low N) | ||
| Results | |||
| Participants | 13* | (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | Figure 1 |
| (b) Give reasons for non-participation at each stage | Results – 1st paragraph | ||
| (c) Consider use of a flow diagram | Figure 1 | ||
| Descriptive data | 14* | (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders | Table 2 |
| (b) Indicate number of participants with missing data for each variable of interest | Results – 1st paragraph | ||
| (c) Summarise follow-up time (eg, average and total amount) | Figure 1 | ||
| Outcome data | 15* | Report numbers of outcome events or summary measures over time | Results – 2nd paragraph |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval). Make clear which confounders were adjusted for and why they were included | No confounders/control variables. |
| (b) Report category boundaries when continuous variables were categorized | Results – 2nd paragraph | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | |||
| Other analyses | 17 | Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses | Patient selection – 3rd paragraph Power analysis |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | 1st paragraph; 5th paragraph |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 13th paragraph |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 1st paragraph; Conclusions |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | Discussions – 13th paragraph; 14th paragraph |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | None |
Figure A1.
a. POP patient assessment form—page 1. b. POP patient assessment form—page 2.
References
- Quality Guidelines for Endodontic Treatment: Consensus Report of the European Society of Endodontology - - 2006 - International Endodontic Journal - Wiley Online Library Available online: https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2591.2006.01180.x (accessed on 25 January 2024).
- Baaij, A.; Kruse, C.; Whitworth, J.; Jarad, F. EUROPEAN SOCIETY OF ENDODONTOLOGY Undergraduate Curriculum Guidelines for Endodontology. International Endodontic Journal 2024, 57, 982–995. [CrossRef]
- Sathorn, C.; Parashos, P.; Messer, H. The Prevalence of Postoperative Pain and Flare-up in Single- and Multiple-Visit Endodontic Treatment: A Systematic Review. International Endodontic Journal 2008, 41, 91–99. [CrossRef]
- Law, A.S.; Nixdorf, D.R.; Aguirre, A.M.; Reams, G.J.; Tortomasi, A.J.; Manne, B.D.; Harris, D.R. Predicting Severe Pain after Root Canal Therapy in the National Dental PBRN. J Dent Res 2015, 94, 37S-43S. [CrossRef]
- Siqueira, J.F. Microbial Causes of Endodontic Flare-Ups. Int Endod J 2003, 36, 453–463. [CrossRef]
- Pasqualini, D.; Mollo, L.; Scotti, N.; Cantatore, G.; Castellucci, A.; Migliaretti, G.; Berutti, E. Postoperative Pain after Manual and Mechanical Glide Path: A Randomized Clinical Trial. Journal of Endodontics 2012, 38, 32–36. [CrossRef]
- Pak, J.G.; White, S.N. Pain Prevalence and Severity before, during, and after Root Canal Treatment: A Systematic Review. Journal of Endodontics 2011, 37, 429–438. [CrossRef]
- Wang, C.; Xu, P.; Ren, L.; Dong, G.; Ye, L. Comparison of Post-obturation Pain Experience Following One-visit and Two-visit Root Canal Treatment on Teeth with Vital Pulps: A Randomized Controlled Trial. Int Endodontic J 2010, 43, 692–697. [CrossRef]
- Jang, Y.-E.; Kim, Y.; Kim, B.S. Influence of Preoperative Mechanical Allodynia on Predicting Postoperative Pain after Root Canal Treatment: A Prospective Clinical Study. Journal of Endodontics 2021, 47, 770-778.e1. [CrossRef]
- Sharma, A.; Sharma, R.; Sharma, M.; Jain, S.; Rai, A.; Gupta, S. Endodontic Flare-Ups: An Update. Cureus 2023, 15, e41438. [CrossRef]
- Parirokh, M.; Rekabi, A.R.; Ashouri, R.; Nakhaee, N.; Abbott, P.V.; Gorjestani, H. Effect of Occlusal Reduction on Postoperative Pain in Teeth with Irreversible Pulpitis and Mild Tenderness to Percussion. Journal of Endodontics 2013, 39, 1–5. [CrossRef]
- Arias, A.; de la Macorra, J.C.; Hidalgo, J.J.; Azabal, M. Predictive Models of Pain Following Root Canal Treatment: A Prospective Clinical Study. Int Endod J 2013, 46, 784–793. [CrossRef]
- Schwendicke, F.; Göstemeyer, G. Single-Visit or Multiple-Visit Root Canal Treatment: Systematic Review, Meta-Analysis and Trial Sequential Analysis. BMJ Open 2017, 7, e013115. [CrossRef]
- Wong, A.W.; Zhang, C.; Chu, C.-H. A Systematic Review of Nonsurgical Single-Visit versus Multiple-Visit Endodontic Treatment. Clin Cosmet Investig Dent 2014, 6, 45–56. [CrossRef]
- Mergoni, G.; Ganim, M.; Lodi, G.; Figini, L.; Gagliani, M.; Manfredi, M. Single versus Multiple Visits for Endodontic Treatment of Permanent Teeth - Mergoni, G - 2022 | Cochrane Library.
- Ince, B.; Ercan, E.; Dalli, M.; Dulgergil, C.T.; Zorba, Y.O.; Colak, H. Incidence of Postoperative Pain after Single- and Multi-Visit Endodontic Treatment in Teeth with Vital and Non-Vital Pulp. European Journal of Dentistry 2019, 03, 273–279. [CrossRef]
- Alonso-Ezpeleta, L.-O.; Gasco-Garcia, C.; Castellanos-Cosano, L.; Martín-González, J.; López-Frías, F.-J.; Segura-Egea, J.-J. Postoperative Pain after One-Visit Root-Canal Treatment on Teeth with Vital Pulps: Comparison of Three Different Obturation Techniques. Med Oral Patol Oral Cir Bucal 2012, 17, e721-727. [CrossRef]
- Monteiro, C.M.C.; Martins, A.C.R.; Reis, A.; de Geus, J.L. Effect of Endodontic Sealer on Postoperative Pain: A Network Meta-Analysis. Restor Dent Endod 2023, 48, e5. [CrossRef]
- Nagendrababu, V.; Gutmann, J.L. Factors Associated with Postobturation Pain Following Single-Visit Nonsurgical Root Canal Treatment: A Systematic Review. Quintessence Int 2017, 48, 193–208. [CrossRef]
- Alí, A.; Olivieri, J.G.; Duran-Sindreu, F.; Abella, F.; Roig, M.; García-Font, M. Influence of Preoperative Pain Intensity on Postoperative Pain after Root Canal Treatment: A Prospective Clinical Study. Journal of Dentistry 2016, 45, 39–42. [CrossRef]
- Yu, Y.-H.; Kushnir, L.; Kohli, M.; Karabucak, B. Comparing the Incidence of Postoperative Pain after Root Canal Filling with Warm Vertical Obturation with Resin-Based Sealer and Sealer-Based Obturation with Calcium Silicate-Based Sealer: A Prospective Clinical Trial. Clin Oral Investig 2021, 25, 5033–5042. [CrossRef]
- Rosen, E.; Goldberger, T.; Taschieri, S.; Del Fabbro, M.; Corbella, S.; Tsesis, I. The Prognosis of Altered Sensation after Extrusion of Root Canal Filling Materials: A Systematic Review of the Literature. J Endod 2016, 42, 873–879. [CrossRef]
- Jaha, H.S. Hydraulic (Single Cone) Versus Thermogenic (Warm Vertical Compaction) Obturation Techniques: A Systematic Review. Cureus 2024, 16, e62925. [CrossRef]
- Yang, R.; Tian, J.; Huang, X.; Lei, S.; Cai, Y.; Xu, Z.; Wei, X. A Comparative Study of Dentinal Tubule Penetration and the Retreatability of EndoSequence BC Sealer HiFlow, iRoot SP, and AH Plus with Different Obturation Techniques. Clin Oral Invest 2021, 25, 4163–4173. [CrossRef]
- Moccia, E.; Carpegna, G.; Dell’Acqua, A.; Alovisi, M.; Comba, A.; Pasqualini, D.; Berutti, E. Evaluation of the Root Canal Tridimensional Filling with Warm Vertical Condensation, Carrier-Based Technique and Single Cone with Bioceramic Sealer: A Micro-CT Study. Giornale Italiano di Endodonzia 2020, 34. [CrossRef]
- Ferreira, G.C.; Pinheiro, L.S.; Nunes, J.S.; de Almeida Mendes, R.; Schuster, C.D.; Soares, R.G.; Kopper, P.M.P.; de Figueiredo, J.A.P.; Grecca, F.S. Evaluation of the Biological and Physicochemical Properties of Calcium Silicate-Based and Epoxy Resin-Based Root Canal Sealers. J Biomed Mater Res B Appl Biomater 2022, 110, 1344–1353. [CrossRef]
- Almeida, L.H.S.; Moraes, R.R.; Morgental, R.D.; Pappen, F.G. Are Premixed Calcium Silicate–Based Endodontic Sealers Comparable to Conventional Materials? A Systematic Review of In Vitro Studies. Journal of Endodontics 2017, 43, 527–535. [CrossRef]
- Chybowski, E.A.; Glickman, G.N.; Patel, Y.; Fleury, A.; Solomon, E.; He, J. Clinical Outcome of Non-Surgical Root Canal Treatment Using a Single-Cone Technique with Endosequence Bioceramic Sealer: A Retrospective Analysis. Journal of Endodontics 2018, 44, 941–945. [CrossRef]
- Donnermeyer, D.; Dammaschke, T.; Schäfer, E. Hydraulic Calcium Silicate-Based Sealers: A Game Changer in Root Canal Obturation? 2020, 197–203.
- Rodríguez-Lozano, F.J.; López-García, S.; García-Bernal, D.; Tomás-Catalá, C.J.; Santos, J.M.; Llena, C.; Lozano, A.; Murcia, L.; Forner, L. Chemical Composition and Bioactivity Potential of the New Endosequence BC Sealer Formulation HiFlow. Int Endod J 2020, 53, 1216–1228. [CrossRef]
- Chen, B.; Haapasalo, M.; Mobuchon, C.; Li, X.; Ma, J.; Shen, Y. Cytotoxicity and the Effect of Temperature on Physical Properties and Chemical Composition of a New Calcium Silicate–Based Root Canal Sealer. Journal of Endodontics 2020, 46, 531–538. [CrossRef]
- Mekhdieva, E.; Del Fabbro, M.; Alovisi, M.; Comba, A.; Scotti, N.; Tumedei, M.; Carossa, M.; Berutti, E.; Pasqualini, D. Postoperative Pain Following Root Canal Filling with Bioceramic vs. Traditional Filling Techniques: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Clin Med 2021, 10, 4509. [CrossRef]
- Tan, H.S.G.; Lim, K.C.; Lui, J.N.; Lai, W.M.C.; Yu, V.S.H. Postobturation Pain Associated with Tricalcium Silicate and Resin-Based Sealer Techniques: A Randomized Clinical Trial. J Endod 2021, 47, 169–177. [CrossRef]
- Graunaite, I.; Skucaite, N.; Lodiene, G.; Agentiene, I.; Machiulskiene, V. Effect of Resin-Based and Bioceramic Root Canal Sealers on Postoperative Pain: A Split-Mouth Randomized Controlled Trial. J Endod 2018, 44, 689–693. [CrossRef]
- Aslan, T.; Dönmez Özkan, H. The Effect of Two Calcium Silicate-Based and One Epoxy Resin-Based Root Canal Sealer on Postoperative Pain: A Randomized Controlled Trial. Int Endod J 2021, 54, 190–197. [CrossRef]
- Fonseca, B.; Coelho, M.S.; Bueno, C.E. da S.; Fontana, C.E.; Martin, A.S.D.; Rocha, D.G.P. Assessment of Extrusion and Postoperative Pain of a Bioceramic and Resin-Based Root Canal Sealer. Eur J Dent 2019, 13, 343–348. [CrossRef]
- García-Font, M.; Duran-Sindreu, F.; Calvo, C.; Basilio, J.; Abella, F.; Ali, A.; Roig, M.; Olivieri, J.-G. Comparison of Postoperative Pain after Root Canal Treatment Using Reciprocating Instruments Based on Operator’s Experience: A Prospective Clinical Study. J Clin Exp Dent 2017, 9, e869–e874. [CrossRef]
- Oliveira, P.S.; Ferreira, M.C.; Paula, N.G.N.; Loguercio, A.D.; Grazziotin-Soares, R.; da Silva, G.R.; da Mata, H.C.S.; Bauer, J.; Carvalho, C.N. Postoperative Pain Following Root Canal Instrumentation Using ProTaper Next or Reciproc in Asymptomatic Molars: A Randomized Controlled Single-Blind Clinical Trial. Journal of Clinical Medicine 2022, 11, 3816. [CrossRef]
- STROBE Available online: https://www.strobe-statement.org/ (accessed on 6 February 2025).
- Endodontic Diagnosis Clinical Newsletter. American Association of Endodontists.
- AAE Endodontic Case Difficulty Assessment Form and Guidelines.
- Buchanan, L.S. Management of the Curved Root Canal. J Calif Dent Assoc 1989, 17, 18–25, 27.
- Dillon, J.S.; Amita, null; Gill, B. To Determine Whether the First File to Bind at the Working Length Corresponds to the Apical Diameter in Roots with Apical Curvatures Both before and after Preflaring. J Conserv Dent 2012, 15, 363–366. [CrossRef]
- Buchanan, L.S. Continuous Wave of Condensation Technique. Endod Prac 1998, 1, 7–10, 13–16, 18 passim.
- Sirintawat, N.; Sawang, K.; Chaiyasamut, T.; Wongsirichat, N. Pain Measurement in Oral and Maxillofacial Surgery. Journal of Dental Anesthesia and Pain Medicine 2017, 17, 253–263. [CrossRef]
- Demenech, L.S.; Freitas, J.V. de; Tomazinho, F.S.F.; Baratto-Filho, F.; Gabardo, M.C.L. Postoperative Pain after Endodontic Treatment under Irrigation with 8.25% Sodium Hypochlorite and Other Solutions: A Randomized Clinical Trial. Journal of Endodontics 2021, 47, 696–704. [CrossRef]
- Ng, Y.-L.; Glennon, J.P.; Setchell, D.J.; Gulabivala, K. Prevalence of and Factors Affecting Post-Obturation Pain in Patients Undergoing Root Canal Treatment. International Endodontic Journal 2004, 37, 381–391. [CrossRef]
- Drumond, J.P.S.C.; Maeda, W.; Nascimento, W.M.; Campos, D. de L.; Prado, M.C.; de-Jesus-Soares, A.; Frozoni, M. Comparison of Postobturation Pain Experience after Apical Extrusion of Calcium Silicate– and Resin–Based Root Canal Sealers. Journal of Endodontics 2021, 47, 1278–1284. [CrossRef]
- Olcay, K.; Eyüboglu, T.F.; Özcan, M. Clinical Outcomes of Non-Surgical Multiple-Visit Root Canal Retreatment: A Retrospective Cohort Study. Odontology 2019, 107, 536–545. [CrossRef]
- Nunes, G.P.; Delbem, A.C.B.; Gomes, J.M.L.; Lemos, C.A.A.; Pellizzer, E.P. Postoperative Pain in Endodontic Retreatment of One Visit versus Multiple Visits: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin Oral Invest 2021, 25, 455–468. [CrossRef]
- Villanueva, L.E.C.D.P. Fusobacterium Nucleatum in Endodontic Flare-Ups. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 2002, 93, 179–183. [CrossRef]
- Mostafa, M.E.H. a. A.; El-Shrief, Y. a. I.; Anous, W.I.O.; Hassan, M.W.; Salamah, F.T.A.; El Boghdadi, R.M.; El-Bayoumi, M. a. A.; Seyam, R.M.; Abd-El-Kader, K.G.; Amin, S. a. W. Postoperative Pain Following Endodontic Irrigation Using 1.3% versus 5.25% Sodium Hypochlorite in Mandibular Molars with Necrotic Pulps: A Randomized Double-Blind Clinical Trial. International Endodontic Journal 2020, 53, 154–166. [CrossRef]
- Hou, X.-M.; Su, Z.; Hou, B.-X. Post Endodontic Pain Following Single-Visit Root Canal Preparation with Rotary vs Reciprocating Instruments: A Meta-Analysis of Randomized Clinical Trials. BMC Oral Health 2017, 17, 86. [CrossRef]
- Segura-Egea, J.J.; Cisneros-Cabello, R.; Llamas-Carreras, J.M.; Velasco-Ortega, E. Pain Associated with Root Canal Treatment. International Endodontic Journal 2009, 42, 614–620. [CrossRef]
- Arias, A.; Azabal, M.; Hidalgo, J.J.; De La Macorra, J.C. Relationship between Postendodontic Pain, Tooth Diagnostic Factors, and Apical Patency. Journal of Endodontics 2009, 35, 189–192. [CrossRef]
- Gotler, M.; Bar-Gil, B.; Ashkenazi, M. Postoperative Pain after Root Canal Treatment: A Prospective Cohort Study. International Journal of Dentistry 2012, 2012, 310467. [CrossRef]
- Patro, S.; Meto, A.; Mohanty, A.; Chopra, V.; Miglani, S.; Das, A.; Luke, A.M.; Hadi, D.A.; Meto, A.; Fiorillo, L.; et al. Diagnostic Accuracy of Pulp Vitality Tests and Pulp Sensibility Tests for Assessing Pulpal Health in Permanent Teeth: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health 2022, 19, 9599. [CrossRef]
- Iqbal, M.; Kurtz, E.; Kohli, M. Incidence and Factors Related to Flare-Ups in a Graduate Endodontic Programme. International Endodontic Journal 2009, 42, 99–104. [CrossRef]
- Marshall, J.G.; Liesinger, A.W. Factors Associated with Endodontic Posttreatment Pain. Journal of Endodontics 1993, 19, 573–575. [CrossRef]
- Mc Cullagh, J.J.P.; Setchell, D.J.; Gulabivala, K.; Hussey, D.L.; Biagioni, P.; Lamey, P.-J.; Bailey, G. A Comparison of Thermocouple and Infrared Thermographic Analysis of Temperature Rise on the Root Surface during the Continuous Wave of Condensation Technique. International Endodontic Journal 2000, 33, 326–332. [CrossRef]
- Zamparini, F.; Lenzi, J.; Duncan, H.F.; Spinelli, A.; Gandolfi, M.G.; Prati, C. The Efficacy of Premixed Bioceramic Sealers versus Standard Sealers on Root Canal Treatment Outcome, Extrusion Rate and Post-Obturation Pain: A Systematic Review and Meta-Analysis. Int Endod J 2024, 57, 1021–1042. [CrossRef]
- Walton, R.; Fouad, A. Endodontic Interappointment Flare-Ups: A Prospective Study of Incidence and Related Factors. J Endod 1992, 18, 172–177. [CrossRef]
- Glennon, J.P.; Ng, Y.-L.; Setchell, D.J.; Gulabivala, K. Prevalence of and Factors Affecting Postpreparation Pain in Patients Undergoing Two-Visit Root Canal Treatment. Int Endod J 2004, 37, 29–37. [CrossRef]
- Llena, C.; Nicolescu, T.; Perez, S.; Gonzalez de Pereda, S.; Gonzalez, A.; Alarcon, I.; Monzo, A.; Sanz, J.L.; Melo, M.; Forner, L. Outcome of Root Canal Treatments Provided by Endodontic Postgraduate Students. A Retrospective Study. Journal of Clinical Medicine 2020, 9, 1994. [CrossRef]
- Bielewicz, J.; Daniluk, B.; Kamieniak, P. VAS and NRS, Same or Different? Are Visual Analog Scale Values and Numerical Rating Scale Equally Viable Tools for Assessing Patients after Microdiscectomy? Pain Res Manag 2022, 2022, 5337483. [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of Adult Pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken) 2011, 63 Suppl 11, S240-252. [CrossRef]
- Pak, J.G.; White, S.N. Pain Prevalence and Severity before, during, and after Root Canal Treatment: A Systematic Review. J Endod 2011, 37, 429–438. [CrossRef]
- Mokhtari, F.; Yazdi, K.; Mahabadi, A.M.; Modaresi, S.J.; Hamzeheil, Z. Effect of Premedication with Indomethacin and Ibuprofen on Postoperative Endodontic Pain: A Clinical Trial. Iran Endod J 2016, 11, 57–62. [CrossRef]
- Milani, A.S.; Froughreyhani, M.; Taghiloo, H.; Nouroloyouni, A.; Jafarabadi, M.A. The Effect of Antibiotic Use on Endodontic Post-Operative Pain and Flare-up Rate: A Systematic Review with Meta-Analysis. Evidence-Based Dentistry (EBD) 2022. [CrossRef]
Figure 1.
Flow chart of patient enrollment.
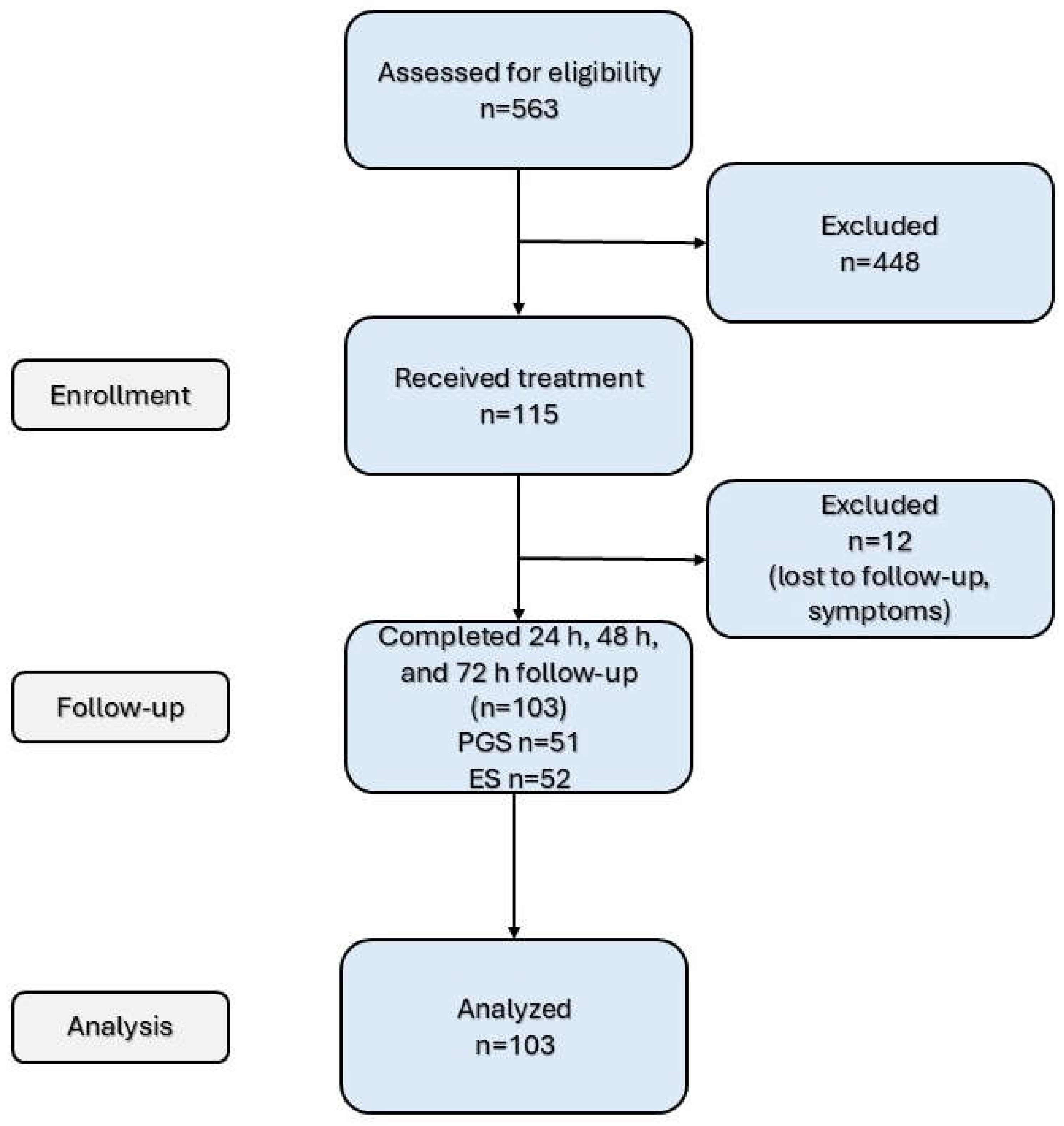
Figure 2.
Examples of cases performed by PGSs (a,c pre-operative radiograph; b,d post-operative radiograph) and ESs (c, pre-operative radiograph; d, post-operative radiograph).
Figure 2.
Examples of cases performed by PGSs (a,c pre-operative radiograph; b,d post-operative radiograph) and ESs (c, pre-operative radiograph; d, post-operative radiograph).

Figure 3.
Mean values for POP, mastication discomfort, and sleep disturbance evaluation at 24 h, 48 h, and 72 h after instrumentation and obturation phases for the whole cohort.
Figure 3.
Mean values for POP, mastication discomfort, and sleep disturbance evaluation at 24 h, 48 h, and 72 h after instrumentation and obturation phases for the whole cohort.
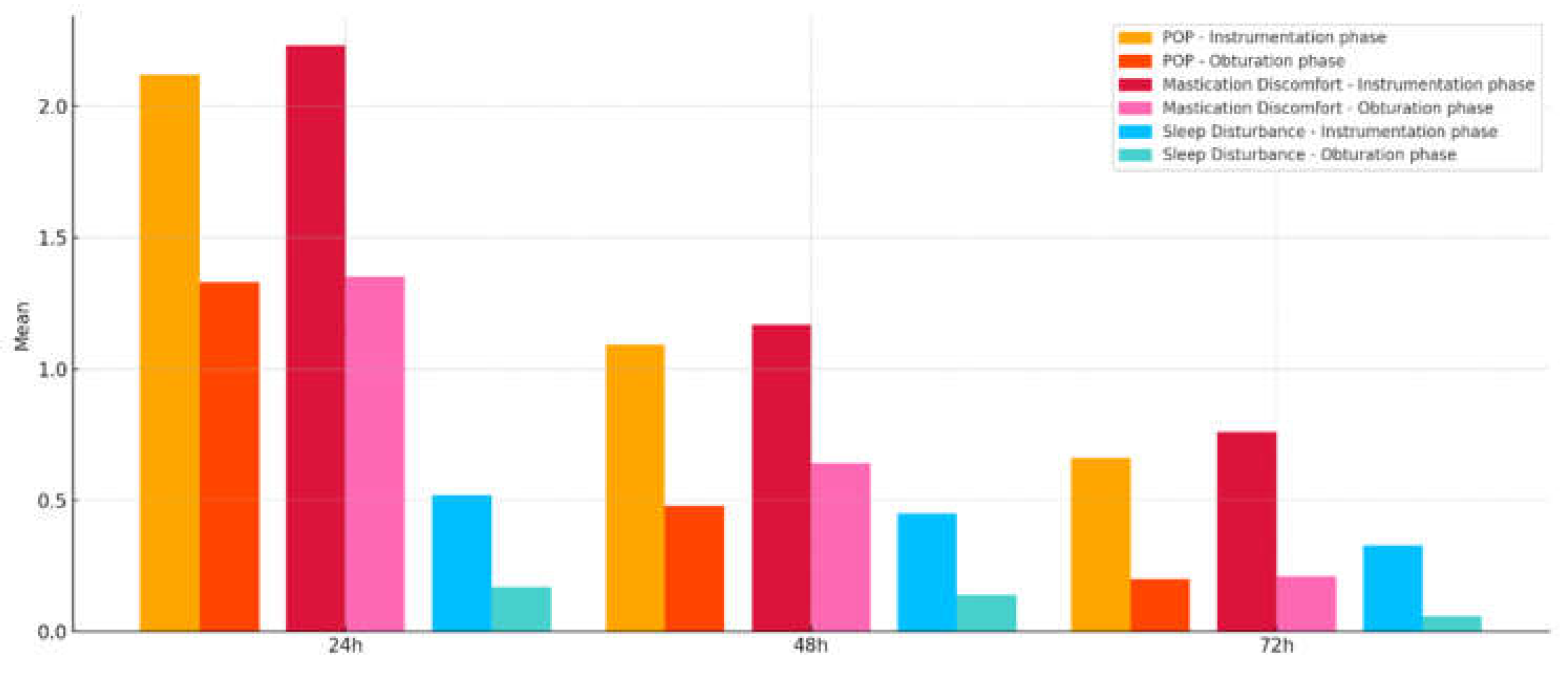
Figure 4.
a. POP, mastication discomfort, and sleep disturbance for PGSs and ESs at 24, 48, and 72 h following the instrumentation phase.
Figure 4.
a. POP, mastication discomfort, and sleep disturbance for PGSs and ESs at 24, 48, and 72 h following the instrumentation phase.
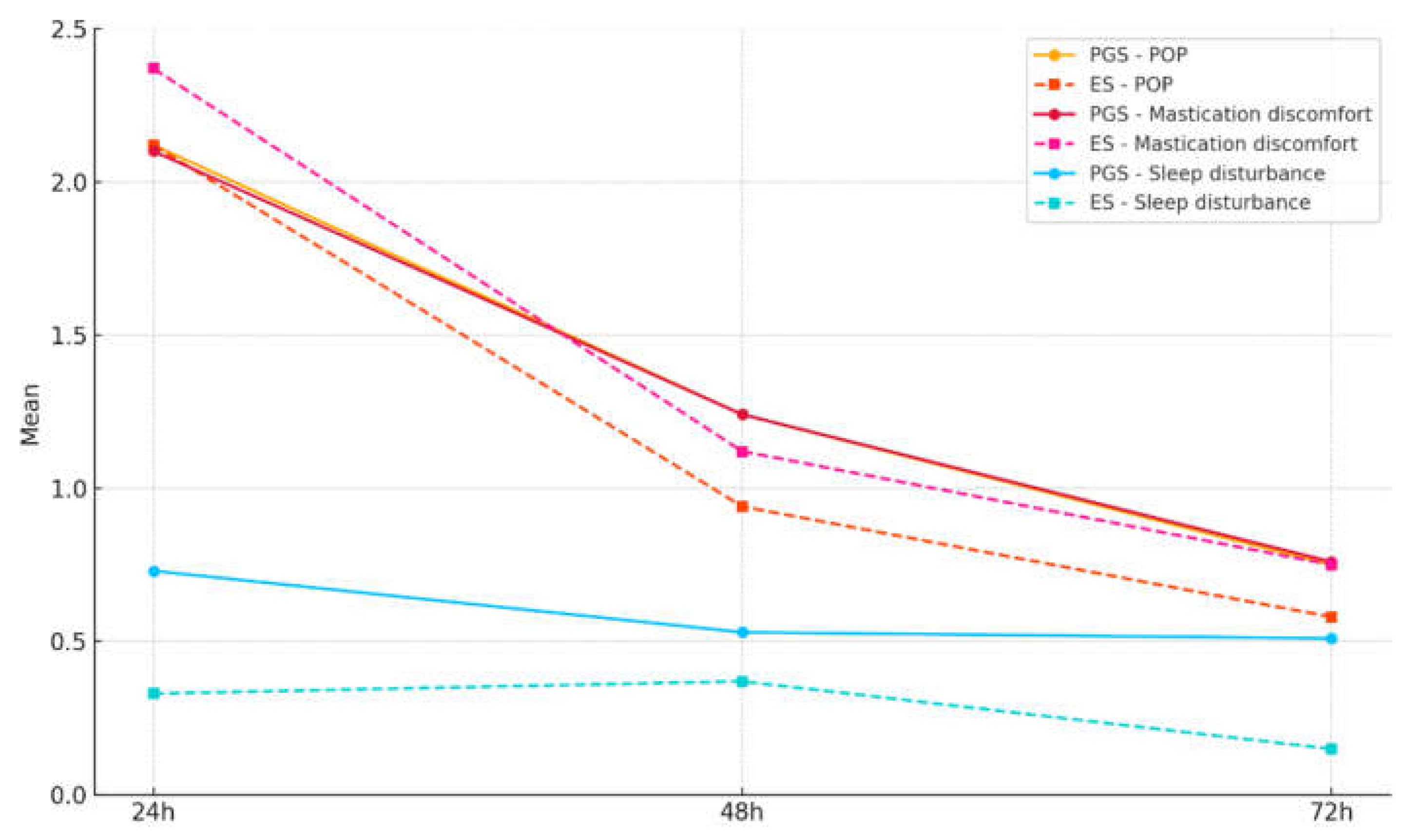
Figure 4.
b. POP, mastication discomfort, and sleep disturbance for PGSs and ESs at 24, 48, and 72 h following the obturation phase.
Figure 4.
b. POP, mastication discomfort, and sleep disturbance for PGSs and ESs at 24, 48, and 72 h following the obturation phase.
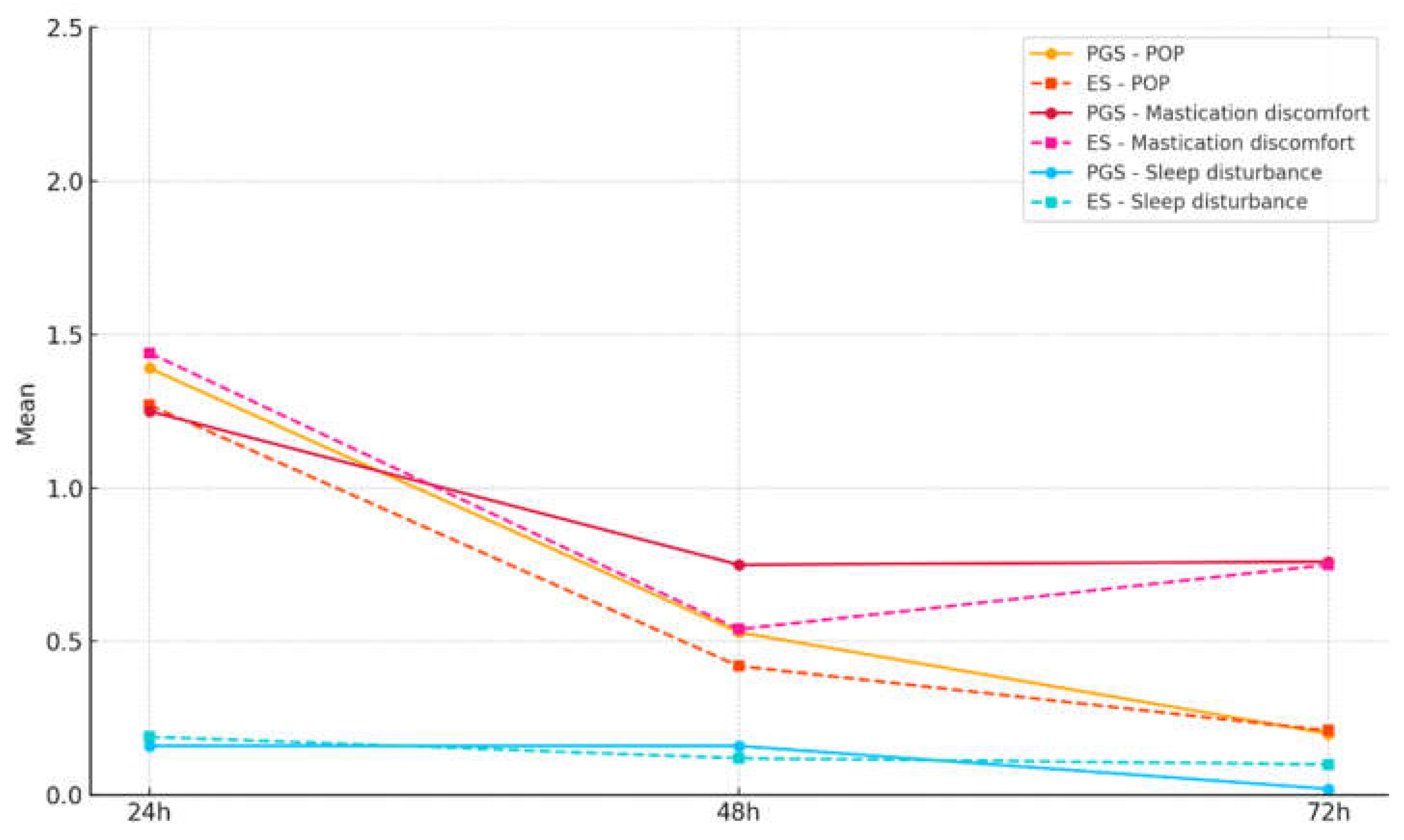
Table 1.
Demographics and distribution of clinical features.
| Factor | PGS | ES | Total | P a | |
|---|---|---|---|---|---|
| Age¹ | 42.3 ± 17.2 | 42.2 ± 15.3 | 42.3 ± 16.7 | 0.980 | |
| Gender | Female | 33 | 34 | 67 | 0.940 |
| Male | 18 | 18 | 36 | ||
| Tooth type | Anterior | 15 | 7 | 22 | 0.100 |
| Premolar | 10 | 9 | 19 | ||
| Molar | 26 | 36 | 62 | ||
| AAE Difficulty | Minimum | 19 | 14 | 33 | 0.500 |
| Moderate | 14 | 15 | 29 | ||
| High | 18 | 23 | 41 | ||
| Pulp status | Vital (healthy) | 8 | 8 | 16 | 0.990 |
| Pulpitis | 25 | 25 | 50 | ||
| Necrosis | 18 | 19 | 37 | ||
| Percussion | Positive | 15 | 20 | 35 | 0.330 |
| Negative | 36 | 32 | 68 | ||
| LEO | No | 34 | 34 | 68 | 0.700 |
| Leo < 2 mm | 9 | 12 | 10 | ||
| Leo > 2 mm | 8 | 6 | 14 | ||
| Extrusion | Yes | 11 | 20 | 31 | 0.060 |
| No | 40 | 32 | 72 | ||
| Obturation quality | Correct | 39 | 46 | 85 | 0.280 |
| Adequate | 8 | 3 | 11 | ||
| Short | 1 | 0 | 1 | ||
| Overfilling | 3 | 3 | 6 |
¹ Mean ± standard deviation (SD); p, significance between groups (PGS and ES); LEO, lesion of endodontic origin; a α < 0.05.
Table 2.
Presence or absence of POP 24 h after the instrumentation phase or obturation phase for the two groups.
Table 2.
Presence or absence of POP 24 h after the instrumentation phase or obturation phase for the two groups.
| POP | PGS | ES | total | P1,a | |
| Instrumentation phase | No | 17 (34.0%) | 16 (30.7%) | 33 (32.3%) | 0.946 |
| Yes | 34 (66.0%) | 36 (69.2%) | 70 (67.6%) | ||
| Obturation phase | No | 23 (46.0%) | 30 (57.6%) | 53 (51.9%) | 0.279 |
| Yes | 28 (54.0%) | 22 (42.3%) | 50 (48.0%) | ||
| P2,a | 0.311 | 0.010 |
p1, significance between groups (PGS and ES) for the two phases ; p2, significance between phases (instrumentation or obturation) for each group; a α < 0.05.
Table 3.
Mean difference and significance between different timepoints for instrumentation and obturation phases regarding POP, mastication discomfort, and sleep disturbance.
Table 3.
Mean difference and significance between different timepoints for instrumentation and obturation phases regarding POP, mastication discomfort, and sleep disturbance.
| Instrumentation phase | Obturation phase | ||
| POP | 24 h vs. 48 h | 1.03* | 0.85* |
| 24 h vs. 72 h | 1.46* | 1.13* | |
| 48 h vs. 72 h | 0.43*** | 0.27** | |
| Mastication discomfort | 24 h vs. 48 h | 1.06* | 0.71* |
| 24 h vs. 72 h | 1.48* | 1.14* | |
| 48 h vs. 72 h | 0.42*** | 0.43* | |
| Sleep disturbance | 24 h vs. 48 h | 0.08 | 0.04 |
| 24 h vs. 72 h | 0.19 | 0.12 | |
| 48 h vs. 72 h | 0.12 | 0.08 | |
*p < 0.001; **p < 0.01; ***p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



