
Submitted:
15 September 2025
Posted:
17 September 2025
You are already at the latest version
Abstract
Intimate partner violence (IPV) is a public health issue that produces significant psycho-logical and physiological consequences. This study examines whether sustaining a seri-ous physical injury increases the likelihood that IPV survivors experience emotional and physical symptoms. We analyzed nonfatal violence by an intimate partner reported in the U.S. National Crime Victimization Survey (2009–2019) and applied survey-adjusted lo-gistic regression models. We assessed two dichotomous outcomes: (1) whether respond-ents reported at least one emotional symptom (e.g., vulnerable, violated, distrustful, or unsafe) and (2) whether they reported at least one physical symptom (e.g., headaches, fa-tigue, or muscle tension). We define serious physical injury as broken bones, gunshot wounds, internal injuries, or loss of consciousness. We included demographic character-istics (age, race, sex, and educational attainment) and crime-related factors (sexual as-sault, simple assault, and aggravated assault) as control variables. The results show that IPV survivors who sustained serious injuries had significantly higher odds of reporting both emotional and physical symptoms than those who did not sustain such injuries. These findings underscore how serious injury compounds the burden of IPV and empha-size the need for comprehensive medical, legal, and psychosocial interventions to address its lasting health impacts.
Keywords:
intimate partner violence (IPV)
; traumatic brain injury (TBI)
; National Crime Victimization Survey (NCVS)
; emotional symptoms
; physical symptoms
; race/ethnicity
1. Introduction
Intimate partner violence (IPV) is a pervasive public health problem in the United States [1,2,3,4]. IPV affects people of all genders, sexual orientations, and relationship types, and includes threatened, attempted, or completed physical or sexual violence, emotional abuse, and stalking by a spouse, partner, or dating partner [1,5,6]. Although both men and women experience IPV, women bear a disproportionate burden, facing higher rates of victimization along with a much greater risk of injury and death [6,7]. Women are significantly more likely than men to report IPV-related rape, physical assault, or stalking, and they experience more chronic and injurious assaults, with more than 40% reporting injury during their most recent incident compared to fewer than 20% of men [5]. One of the most extreme forms of gender-based violence is pregnancy-associated femicide, where intimate partners murder women during or after pregnancy, accounting for up to 41% of maternal homicides [1,7]. Research further shows that between 6.7% and 17.2% of males experience IPV [8,9]. Nevertheless, males are frequently omitted from analyses, which complicates our understanding of the scope and consequences of IPV across genders.
Abused women face worse overall physical health, lower quality of life, and higher use of medical services compared to women who have not been abused [1,10,11]. Injuries frequently affect the head, face, and neck, but may also include lacerations, broken bones, and internal damage [12]. Beyond immediate harm, IPV produces chronic physical conditions such as headaches, back pain, and musculoskeletal issues [1]. Fatigue, insomnia, nightmares, and restless sleep commonly follow IPV, exacerbating depression and distress [13]. Longer-term consequences of IPV victimization include cardiovascular problems, hypertension [11], and disordered eating habits [6]. In the most severe cases, IPV causes traumatic brain injury (TBI), with symptoms ranging from loss of consciousness and headaches to long-term neurological impairment [12]. Women who experience sexual assault-related IPV face a higher risk of injuries, chronic pain, gastrointestinal and gynecological problems, sexually transmitted infections, and mental health conditions such as depression and PTSD [1,14]. A 2025 systematic review reported consistent associations between IPV and depression in 10 of 11 studies, most of which relied on hospital, shelter, or police samples. While these settings provide valuable insights, they limit generalizability because they exclude the many survivors who never seek formal services.
Experiencing violence at the hands of an intimate partner constitutes a betrayal of trust and represents a distinct form of emotional injury [15] This experience aligns with the concept of betrayal trauma [16]. Limited research on betrayal trauma suggests that it creates barriers to forming healthy relationships by fostering fear, shame, and low self-esteem. It also erodes trust and security, producing ongoing feelings of vulnerability, violation, unsafety, and shame [4]. Shame is defined as a negative emotion or painful experience that results in feelings of mistrust, vulnerability, fear of stigmatization, and self-blame [17,18,19,20]. Shame operates not only as an immediate emotional response but also as a longer-term psychosocial consequence of IPV, functioning as a barrier to help-seeking among female survivors [18]. When survivors do seek help, they often encounter individuals or institutions that reinforce rather than reduce this shame. Ethno-racial identity can compound these dynamics, as cultural and social identities shape how shame is experienced and expressed in help-seeking contexts [21].
Despite decades of research on IPV across medicine, psychology, and criminology, important gaps remain. Most studies have focused on general mental and physical health outcomes among survivors, documenting conditions such as depression, PTSD, or overall physical health restrictions. However, these outcomes are rarely linked directly to the IPV incident itself, making it difficult to understand the specific symptoms that emerge in the immediate weeks and months after victimization. A recent review highlights that although IPV affects women’s physical health well beyond acute injuries and mental health consequences, few studies validate these findings, underscoring the need for more research on the long-term effects of IPV, especially across different subtypes [22]. The review further notes that, despite challenges, such research is essential to establish links between IPV and chronic health conditions, thereby furthering the evidence base to establish IPV as a critical health issue.
To our knowledge, only one prior study has examined both emotional and physical symptoms following violent victimization using National Crime Victimization Survey (NCVS) data while incorporating IPV. Hullenaar et al. (2022) found that victims harmed by family members or intimate partners reported significantly higher levels of emotional and social distress, as well as long-term symptoms, than those harmed by strangers, with effects most pronounced among uninjured victims. In contrast, the present study focuses exclusively on IPV—defined as sexual or physical assault committed by a current or former intimate partner, consistent with the Bureau of Justice Statistics (BJS) classification—to assess how injury severity, particularly loss of consciousness as a marker of probable traumatic brain injury (pTBI), increases the risk of emotional and physical symptoms such as headaches, fatigue, gastrointestinal issues, anxiety, mistrust, and feelings of being unsafe that persist for at least one month following an IPV incident within the past six months. Consistent with a public health perspective, we also include both male and female survivors to examine patterns across genders. Unlike prior work, we estimate nationally representative prevalence and predicted probabilities of any symptom across sex, race/ethnicity, and injury status. By explicitly linking symptom onset to specific IPV incidents and establishing a temporal framework for outcomes, this study bridges the gap between research limited to immediate injuries and studies describing long-term health effects. This study provides the most comprehensive evidence to date on the short- to medium-term emotional and physical consequences of IPV in the United States and highlights implications for both public health and legal systems.
The current study uses nationally representative data from the National Crime Victimization Survey (NCVS) and defines IPV as a sexual or physical assault committed by a current or former intimate partner consistent with the Bureau of Justice Statistics (BJS) classification. Specifically, the study investigates the likelihood that victims report either emotional or physical symptoms, such as headaches, fatigue, gastrointestinal issues, anxiety, mistrust, and feelings of being unsafe, that persist for at least one month following an IPV incident that occurred within the past six months. By explicitly linking symptom onset to specific IPV events and establishing a temporal framework for outcomes, the study bridges the gap between research limited to immediate injuries and studies describing long-term, “lifetime” health effects. In addition, consistent with a public health perspective, we include both male and female survivors, ensuring that patterns across genders can be examined rather than assuming IPV is something that only affects health. This study has two primary objectives: first, to determine the national prevalence of emotional and physical symptoms following IPV across key sociodemographic groups; and second, to investigate whether injury, including potential traumatic brain injury, exacerbates these risks beyond sociodemographic characteristics. In doing so, this study provides the most comprehensive evidence to date on the short- to medium-term emotional and physical consequences of IPV in the United States.
2. Materials and Methods
Data for this study were analyzed from incident-level records from the NCVS public-use files. The NCVS is a nationally representative household survey administered by the BJS [23]. The NCVS interviews over 90,000 households twice annually, with sampled households remaining in the study for three years. Respondents aged 12 and older provide information on demographics, household composition, and victimizations that occurred in the past six months, along with follow-up questions about offender characteristics, incident context, injuries, police reporting, and victimization consequences. We limited our analysis to survey years 2009 through 2023, as questions about emotional and physical symptoms after victimization were fully included starting in 2009.
We followed the coding scheme of others [24] to identify incidents of IPV. Specifically, we coded cases in which offenders were reported as spouses, ex-spouses, or boyfriends/girlfriends, or when multiple offenders included a partner. We excluded victimizations committed solely by other family members or strangers. Following the BJS classification, we further limited the analytic sample to violent crimes, defined as sexual violence and assault (including both simple and aggravated assault). This resulted in a weighted, nationally representative sample of IPV incidents during the study period.
In the NCVS, only victims identified as having socio-emotional problems were asked about specific symptoms “for a month or more” following the crime. Emotional symptoms included feeling worried or anxious, angry, sad or depressed, vulnerable, violated, mistrustful, or unsafe. Physical symptoms included headaches, trouble sleeping, changes in eating or drinking, upset stomach, fatigue, high blood pressure, muscle tension, or back pain.
We constructed two binary outcome variables from these fourteen items, following previous research [25]. For the first dependent variable, we coded cases as one if victims reported at least one emotional symptom and zero otherwise. For the second dependent variable, we coded cases as one if victims reported at least one physical symptom and zero otherwise. Victims who were screened as not having socio-emotional problems, that is, they reported no or only mild distress and no problems at work, school, or with family and friends, were not asked the follow-up symptom items; for these cases, both outcomes were coded as 0. Following BJS practice, we also imputed outcomes as 0 for respondents who skipped the socio-emotional screening and therefore were not asked about emotional or physical symptoms (n = 2,545).
Our key predictors captured injury severity at the incident. We coded any injury as one if either of two injury items indicated injuries (codes 2–11) and zero otherwise. We also coded whether the victim was knocked unconscious during the incident. Because the NCVS does not include neuroimaging or clinical assessments, loss of consciousness serves as the closest available proxy for probable traumatic brain injury (pTBI), a clinical marker of head trauma with potential neurological consequences [16]. We controlled for a range of sociodemographic and contextual characteristics. Victim demographics included sex (female vs. male), age (modeled both continuously and categorically: <19, 19–39, 40–59, 60+), race/ethnicity (White [reference], Black, Hispanic, American Indian/Alaska Native, Asian/Pacific Islander, and multiracial), and education (high school or less vs. more than high school). Additional covariates included U.S. region (Northeast [reference], Midwest, South, West, and missing), population size of residence (<50,000 [reference], 50,000–250,000, ≥250,000), police reporting of the incident (yes/no), and survey year.
Analytic Strategy
We implemented all descriptive and model-based estimates using survey methods. Specifically, we applied NCVS victimization weights in survey designs with independent primary sampling units to generate nationally representative estimates. First, we summarized yearly totals for all victimizations, violent victimizations, and IPV victimizations. We also looked at the share of violent crimes caused by IPV and the proportion of IPV incidents that resulted in injury. Next, we used survey-weighted bivariate logistic regressions to estimate the odds ratios (ORs) for reporting one or more emotional or physical symptoms.
We fit multivariable survey-weighted logistic regressions separately for emotional and physical symptoms. We modeled age and year with restricted cubic splines to allow flexible nonlinear associations (age knots at 25, 40, and 65; year knots at 1999, 2007, and 2015) following [24]. Models included all covariates listed above, along with injury status and loss of consciousness. From the multivariable models, we generated predicted probabilities on the response scale under prespecified scenarios. We averaged predictions across year, region, and population size where indicated, and reported results by sex, injury status, and race/ethnicity. For an injured-only subset, we contrasted those who reported losing consciousness after the IPV victimization with those who were not by sex or race. We also visualized marginal effects for age and year with 95% confidence intervals.
3. Results
The NCVS public-use data from 2009 to 2023 revealed that violent victimizations ranged from 1.7 to 2.5 million annually. Depending on the operational definition, IPV accounted for between 14% and 22% of violent crimes per year under the broad definition (all violent partner victimizations) and 19% to 31% under the restricted definition (partner assaults and sexual violence only). The restricted definition produces a larger estimate of the national prevalence of IPV because it excludes robberies and threats by partners from both the numerator and denominator, which substantially reduces the pool of violent crimes against which IPV incidents are compared. Across the study period, 2% to 7% of IPV incidents under the restricted definition involved a coded injury, which equated to roughly 7,000 to 39,000 injury-causing IPV incidents per year (estimate not shown). It is important to note that NCVS data collection was severely limited during the COVID-19 pandemic, affecting the interpretation of 2020–2021 estimates.
Table 1 shows the percentage of IPV survivors reporting at least one symptom overall and by sociodemographic characteristics. Overall, 70.6% of IPV victims of assault and sexual violence reported at least one emotional symptom, and 53.6% reported at least one physical symptom lasting a month or longer. Symptom rates varied widely based on victim characteristics. Among females, 76.1% reported emotional symptoms and 60.5% reported physical symptoms, compared to 52.7% and 31.0% among males. Younger victims indicated somewhat lower symptom prevalence than middle-aged or older victims; in contrast, Native American/Alaska Native and Asian/Pacific Islander victims had the highest proportions of both emotional and physical symptoms. Injured victims had a notably higher prevalence: 81.4% reported emotional symptoms, and 72.6% reported physical symptoms.
The multivariable model results (Table 2) show that these differences remain after adjusting for covariates. Female sex was strongly linked to higher odds of symptoms (OR = 2.94 for emotional; OR = 3.61 for physical). Injury nearly doubled the odds of emotional symptoms (OR = 1.96) and tripled the odds of physical symptoms (OR = 2.79). Loss of consciousness was also significant, further increasing the likelihood of both outcomes. The effect of race/ethnicity was more variable. For example, Native American/Alaska Native victims had significantly higher odds of both outcomes, while Hispanic victims had lower odds of physical symptoms compared to non-Hispanic White victims. Education, region, and community size were not consistently related to symptoms.
We used post-estimation predictions from multivariable models to examine how the probability of experiencing each type of symptom varied by survey year and victim age (Figure 1). Predicted probabilities of both physical and emotional symptoms increased during early and middle adulthood and then leveled off or declined slightly at older ages. Temporal patterns were modest: symptom prevalence remained relatively stable across survey years, with only minor upward fluctuations in more recent years.
Predicted probabilities further illustrate the magnitude of effects across sociodemographic factors and injury status (Table 3, Table 4 and Table 5). Among White male victims without injury, the probability of reporting physical symptoms was 0.26 (95% CI: 0.18–0.33), compared to 0.76 (95% CI: 0.65–0.87) among White female victims with injury (Table 3). These patterns were consistent across racial and ethnic groups, with higher probabilities among females and those who sustained injuries.
For emotional symptoms, probabilities exceeded 0.80 among injured female victims across most racial and ethnic groups. Table 4 further demonstrates how race shapes symptom probabilities within sex and injury groups; for instance, injured Native American/Alaska Native females had predicted probabilities approaching 0.90 for both emotional and physical symptoms.
Table 5 shows that among injured victims, being rendered unconscious further increased predicted probabilities. This effect was especially pronounced among females, with more than 90% reporting either emotional or physical symptoms following loss of consciousness.
4. Discussion
This study examined the short- to medium-term health consequences of IPV by linking incident-level victimization data to survivors’ reports of physical and emotional symptoms lasting at least one month. Using a nationally representative sample, we found that more than two-thirds of IPV survivors experienced at least one emotional symptom, and more than half experienced at least one physical symptom after victimization. The risks were substantially higher for survivors who sustained injuries, and especially for those who lost consciousness, with predicted probabilities of symptoms often exceeding 80 to 90 percent. These findings provide some of the most substantial evidence to date that IPV-related injuries, including pTBI, compound both physical and emotional burdens, and that these burdens vary by sociodemographic characteristics.
Our findings align with prior research showing that IPV is closely linked to physical health problems, emotional distress, and long-lasting trauma symptoms [1,13,31]. Hullenaar et al. examined outcomes across victim–offender relationships (family/intimate partner, acquaintance, stranger) and found that IPV victims faced greater risks of adverse outcomes, with injury further increasing the likelihood of reporting physical and emotional symptoms [32]. We extend this work by focusing exclusively on IPV and by examining how injury severity and loss of consciousness, which serves as a marker of pTBI, compound the risk of both emotional and physical symptoms. In addition, we estimate the national prevalence and predicted probabilities of any symptom across survey years, sex, race and ethnicity, and injury status, providing a more detailed and population-level view of the consequences of IPV on emotional and physical health.
Consistent with previous research [7,33], our results demonstrate that sustaining a serious injury, particularly one involving loss of consciousness, substantially increases the risk of enduring adverse emotional and physical outcomes that persist for months after the incident. Betrayal trauma helps explain why these symptoms persist, manifesting in fear and avoidance, altered relationship expectations, shame and low self-esteem, and communication difficulties. Research also demonstrates that betrayal trauma extends beyond interpersonal relationships to include institutions: when systems fail to provide safety and fair treatment, trauma symptoms worsen in measurable ways. Our results align with [34], who surveyed 123 clients of two agencies serving IPV survivors and found that fear of being blamed, feelings of shame, and lack of community support were significant barriers to seeking help. Silence rooted in shame can easily be misinterpreted as guilt or a lack of credibility, while hesitation to take protective actions may reflect fear, mistrust, or feelings of being unsafe rather than disengagement.
Further, we found that the prevalence of emotional and physical health symptoms has remained relatively stable over time, with only modest increases in recent years. This suggests that, despite increased awareness of IPV and expanded services, there has been little measurable progress in reducing the health consequences survivors experience after victimization. Age differences were noted for physical symptoms, which peak between ages 30 and 50 before declining modestly at older ages. In contrast, emotional symptoms remain consistently high across adulthood, with predicted probabilities above 70% even into older age. Consistent with prior research, the higher predicted probabilities observed for females, Native American/Alaska Native, and Asian/Pacific Islander survivors are consistent with research documenting sex differences and racial/ethnic disparities in IPV exposure and general health outcomes [22], particularly surrounding experiences of shame [23,26]. Similarly, in the present study, the high prevalence of emotional symptoms among survivors of IPV, including worry, anxiety, anger, sadness, depression, vulnerability, violation, mistrust, and feeling unsafe, particularly among those who sustained injuries or pTBI, shows that IPV is not only a source of physical harm but also a deeply shame-inducing experience.
The increased likelihood of reporting emotional and physical symptoms may help explain why IPV survivors often experience disruptions in work, school, and family life [5,15]. Numerous studies show that exposure to interpersonal violence contributes to increased risks of depression, anxiety, and chronic health conditions later in life [1,35,36]. Our results add to this evidence by quantifying the additional risks associated with being injured or experiencing unconsciousness following an IPV-related physical or sexual assault, highlighting the importance of targeted screening and intervention for these high-risk groups.
Implications for Proactive Public Health Policy to Support IPV Survivors
The findings of this study underscore the need to integrate medical, neurological, and psychological screening into IPV response protocols, including within legal settings, especially for survivors who sustain injury, especially pTBI. Although federal initiatives encourage screening in healthcare settings, to date, no federal mandate requires IPV screening, and states maintain varied reporting laws, creating uneven requirements for providers [37,38], resulting in a lack of systematic screening [39]. Establishing a federal standard could help ensure consistency and equity in screening, which is critical, especially considering the variable definition of what constitutes IPV across states.
Betrayal trauma includes emotional symptoms that IPV survivors experience, such as feeling worried or anxious, angry, vulnerable, violated, mistrustful, or unsafe. These symptoms carry not only medical consequences, including heightened risks of chronic stress and mental health disorders, but also broader social consequences for relationships, family stability, and institutional involvement in areas such as schooling, employment, and the legal system [16]. To address the persistent health problems revealed in our findings, particularly among survivors with injuries or loss of consciousness, and to reduce disparities by sex and race/ethnicity, legal and medical systems should adopt shame-informed approaches in their responses to IPV. One such model is Blueprint for Safety, a program that coordinates how agencies respond to domestic violence crimes [28]. The program enhances control over offenders, facilitates rapid intervention, connects survivors with resources, and shifts the burden from survivors to the system. Building on its demonstrated success in Saint Paul, Minnesota, and other U.S. cities, implementation at the federal level would standardize protocols across states, strengthen consistency in practice, and reduce inequities in access to protection and support.
Institutions should be intentional about acknowledging the implications of institutional betrayal, also referred to as double betrayal [40]. Police reforms and courtroom procedures are especially important because law enforcement often serve as the frontline responders, and legal processes are the primary mechanisms for addressing IPV [41]. Trauma-informed approaches such as closed courtrooms, remote testimony, or private communication with judges can reduce shame and support survivor autonomy. Attorneys and advocates also need training to recognize emotional responses, such as shame, so that survivor protectiveness is not misinterpreted as apathy or dishonesty. Police interactions can also intensify distress when survivors anticipate disbelief, judgment, or blame, while courtrooms may become sites of re-traumatization when survivors must share space with their abuser or respond to questioning during hearings. Building trust, using survivor-centered language, and safeguarding privacy are essential for validating experiences and empowering survivors. Judges should enforce zero-tolerance policies for disrespectful conduct and adapt courtroom layouts to minimize involuntary contact. For example, providing private waiting areas, reducing reliance on mass hearings, and expanding the use of virtual platforms can all help reduce traumatic interactions. Abusers should never be allowed to confront or interrogate survivors directly, as such practices increase trauma and undermine dignity. Embedding these strategies into everyday practice can lessen stigma and emotional harm among IPV survivors and promote more equitable access to justice.
Despite being the first study to examine the national prevalence of emotional and physical symptoms following IPV-related injury, this study is not without limitations. Because the NCVS relies on self-reported data, estimates may be influenced by recall bias, underreporting, or social desirability effects [42]. While our models document associations between IPV-related injury and subsequent symptoms, we cannot establish causal relationships, as preexisting vulnerabilities may contribute to symptom reporting. The time frame for symptom measurement, within six months of the crime, may underestimate the full scope of long-term or delayed effects. The survey also lacks detailed information on injury severity, types of head trauma, and important covariates such as prior mental health conditions, which limits interpretation. Data collection disruptions during the COVID-19 lockdown also affected estimates for 2020–2021. Finally, observed temporal changes could reflect broader social dynamics, such as shifting cultural attitudes and increased support for survivors, which may have encouraged greater disclosure.
5. Conclusions
Overall, this study contributes to the growing body of research showing that violence—especially IPV is a significant risk factor for ongoing emotional and physical health issues, particularly among minoritized groups such as women. Understanding how injury severity and unconsciousness influence post-IPV health outcomes can help shape prevention strategies, early intervention efforts, and survivor-centered care models aimed at reducing the long-term impacts of IPV on individuals and communities. This section is mandatory.
Author Contributions
Conceptualization, G.B-S.; Methodology, G.B-S.; Software, G.B-S.; Validation, G.B-S., K.S.M., T.H., and A.W-G.; Formal Analysis, G.B-S.; Data Curation, G.B-S.; Writing—Original Draft Preparation, G.B-S., T.H., and K.S.M.; Writing—Review & Editing, K.S.M., T.H., and A.W-G.; Visualization, G.B-S.; Supervision, G.B-S. and K.S.M.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were not required for this study because it exclusively utilized deidentified, publicly available data, qualifying for exemption under 45 CFR 46.104(d)(4), which pertains to secondary research using identifiable private information or biospecimens that are publicly available.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original data presented in the study are openly available at the Bureau of Justice Statistics, National Crime Victimization Survey website: https://bjs.ojp.gov/data-collection/ncvs#7-0
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| IPV | Intimate partner violence |
| NCVS | National Crime Victimization Survey |
| BJS | Bureau of Justice Statistics |
| PTSD | Post-traumatic stress disorder |
| OR | Odds ratio |
References
- Campbell, J.C. Health Consequences of Intimate Partner Violence. Lancet Lond. Engl. 2002, 359, 1331–1336. [CrossRef]
- Carlyle, K.E.; Guidry, J.P.D.; Dougherty, S.A.; Burton, C.W. Intimate Partner Violence on Instagram: Visualizing a Public Health Approach to Prevention. Health Educ. Amp Behav. 2019, 46, 90S-96S. [CrossRef]
- Decker, M.R.; Wilcox, H.C.; Holliday, C.N.; Webster, D.W. An Integrated Public Health Approach to Interpersonal Violence and Suicide Prevention and Response. Public Health Rep. 2018, 133, 65S-79S. [CrossRef]
- Inslicht, S.S.; Marmar, C.R.; Neylan, T.C.; Metzler, T.J.; Hart, S.L.; Otte, C.; McCaslin, S.E.; Larkin, G.L.; Hyman, K.B.; Baum, A. Increased Cortisol in Women with Intimate Partner Violence-Related Posttraumatic Stress Disorder. Psychoneuroendocrinology 2006, 31, 825–838. [CrossRef]
- Tjaden, P.; Thoennes, N. Extent, Nature, and Consequences of Intimate Partner Violence: Findings from the National Violence against Women Survey; U.S. Department of Justice, Office of Justice Programs, National Institute of Justice: Washington, DC, 2000.
- Plichta, S.B. Intimate Partner Violence and Physical Health Consequences: Policy and Practice Implications. J. Interpers. Violence 2004, 19, 1296–1323. [CrossRef]
- Martin, S.L.; Macy, R.J.; Sullivan, K.; Magee, M.L. Pregnancy-Associated Violent Deaths: The Role of Intimate Partner Violence. Trauma Violence Abuse 2007, 8, 135–148. [CrossRef]
- Davidov, D.M.; Larrabee, H.; Davis, S.M. United States Emergency Department Visits Coded for Intimate Partner Violence. J. Emerg. Med. 2015, 48, 94–100. [CrossRef]
- Khurana, B.; Hines, D.A.; Johnson, B.A.; Bates, E.A.; Graham-Kevan, N.; Loder, R.T. Injury Patterns and Associated Demographics of Intimate Partner Violence in Men Presenting to U.S. Emergency Departments. Aggress. Behav. 2022, 48, 298–308. [CrossRef]
- Simmons, S.B.; Knight, K.E.; Menard, S. Long-Term Consequences of Intimate Partner Abuse on Physical Health, Emotional Well-Being, and Problem Behaviors. J. Interpers. Violence 2018, 33, 539–570. [CrossRef]
- Schollenberger, J.; Campbell, J.; Sharps, P.W.; O’Campo, P.; Gielen, A.C.; Dienemann, J.; Kub, J. African American HMO Enrollees: Their Experiences with Partner Abuse and Its Effect on Their Health and Use of Medical Services. Violence Women 2003, 9, 599–618. [CrossRef]
- Wilbur, L.; Higley, M.; Hatfield, J.; Surprenant, Z.; Taliaferro, E.; Smith, D.J.; Paolo, A. Survey Results of Women Who Have Been Strangled While in an Abusive Relationship. J. Emerg. Med. 2001, 21, 297–302. [CrossRef]
- Kendall-Tackett, K.A. Inflammation, Cardiovascular Disease, and Metabolic Syndrome as Sequelae of Violence Against Women: The Role of Depression, Hostility, and Sleep Disturbance. Trauma Violence Abuse 2007, 8, 117–126. [CrossRef]
- Leserman, J.; Drossman, D.A. Relationship of Abuse History to Functional Gastrointestinal Disorders and Symptoms: Some Possible Mediating Mechanisms. Trauma Violence Abuse 2007, 8, 331–343. [CrossRef]
- Camp, A.R. From Experiencing Abuse to Seeking Protection: Examining the Shame of Intimate Partner Violence. UC Irvine Rev 2022, 13, 103.
- St. Vil, N.M.; Carter, T.; Johnson, S. Betrayal Trauma and Barriers to Forming New Intimate Relationships Among Survivors of Intimate Partner Violence. J. Interpers. Violence 2021, 36, NP3495–NP3509. [CrossRef]
- Simmons, S.B.; Knight, K.E.; Menard, S. Long-Term Consequences of Intimate Partner Abuse on Physical Health, Emotional Well-Being, and Problem Behaviors. J. Interpers. Violence 2018, 33, 539–570. [CrossRef]
- Campbell, J.C. Health Consequences of Intimate Partner Violence. The Lancet 2002, 359, 1331–1336. [CrossRef]
- Plichta, S.B. Intimate Partner Violence and Physical Health Consequences: Policy and Practice Implications. J. Interpers. Violence 2004, 19, 1296–1323. [CrossRef]
- Villa, G.; Spena, P.R.; Marcomini, I.; Poliani, A.; Rosa, D.; Maculotti, D.; Manara, D.F. Factors Influencing the Feeling of Shame in Individuals with Incontinence: The INCOTEST Study. Kontakt 2025, 27, 97–102. [CrossRef]
- Stubbs, A.; Szoeke, C. The Effect of Intimate Partner Violence on the Physical Health and Health-Related Behaviors of Women: A Systematic Review of the Literature. Trauma Violence Abuse 2022, 23, 1157–1172. [CrossRef]
- U.S. Department of Justice, Bureau of Justice Statistics National Crime Victimization Survey, 2022–2009.
- Wheeler, A.P.; Piquero, A.R. Using Victimization Reporting Rates to Estimate the Dark Figure of Crime: A Case Study of Domestic Violence. Crime Delinquency 2025, 00111287251359210. [CrossRef]
- Vargas, E.W.; Hemenway, D. Emotional and Physical Symptoms after Gun Victimization in the United States, 2009–2019. Prev. Med. 2021, 143, 106374. [CrossRef]
- 25. R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023.
- Lumley, T. Survey: Analysis of Complex Survey Samples 2023.
- Harrell Jr, F.E. Rms: Regression Modeling Strategies; 2023.
- Wickham, H.; François, R.; Henry, L.; Müller, K.; Vaughan, D. Dplyr: A Grammar of Data Manipulation; 2023.
- Wickham; Chang, W.; Pedersen, T.; Takahashi, K.; Wilke, C.; Woo, K. Ggplot2: Create Elegant Data Visualisations Using the Grammar of Graphics 2018.
- Golding, J.M. Intimate Partner Violence as a Risk Factor for Mental Disorders: A Meta-Analysis. J. Fam. Violence 1999, 14, 99–132. [CrossRef]
- Hullenaar, K.L.; Rowhani-Rahbar, A.; Rivara, F.P.; Vavilala, M.S.; Baumer, E.P. Victim–Offender Relationship and the Emotional, Social, and Physical Consequences of Violent Victimization. Am. J. Prev. Med. 2022, 62, 763–769. [CrossRef]
- Kendall-Tackett, K.A. Inflammation, Cardiovascular Disease, and Metabolic Syndrome as Sequelae of Violence Against Women: The Role of Depression, Hostility, and Sleep Disturbance. Trauma Violence Abuse 2007, 8, 117–126. [CrossRef]
- Orpinas, P.; Choi, Y.J.; Han, J.-Y.; Chen, Y.; Ahn, K. Survivors of Intimate Partner Violence: Barriers to Seeking Help Among Asian Immigrants. J. Evid.-Based Soc. Work 2025, 1–16. [CrossRef]
- Black, M.C. Intimate Partner Violence and Adverse Health Consequences: Implications for Clinicians. Am. J. Lifestyle Med. 2011, 5, 428–439. [CrossRef]
- Dube, S.R.; Anda, R.F.; Felitti, V.J.; Edwards, V.J.; Croft, J.B. Adverse Childhood Experiences and Personal Alcohol Abuse as an Adult. Addict. Behav. 2002, 27, 713–725. [CrossRef]
- Esopenko, C.; Jain, D.; Adhikari, S.P.; Dams-O’Connor, K.; Ellis, M.; Haag, H. (Lin); Hovenden, E.S.; Keleher, F.; Koerte, I.K.; Lindsey, H.M.; et al. Intimate Partner Violence-Related Brain Injury: Unmasking and Addressing the Gaps. J. Neurotrauma 2024, 41, 2219–2237. [CrossRef]
- Houry, D.; Sachs, C.J.; Feldhaus, K.M.; Linden, J. Violence-Inflicted Injuries: Reporting Laws in the Fifty States. Ann. Emerg. Med. 2002, 39, 56–60. [CrossRef]
- Haag, H. (Lin); Jones, D.; Joseph, T.; Colantonio, A. Battered and Brain Injured: Traumatic Brain Injury Among Women Survivors of Intimate Partner Violence—A Scoping Review. Trauma Violence Abuse 2022, 23, 1270–1287. [CrossRef]
- Lahav, Y.; Avidor, S.; Gafter, L.; Lotan, A. A Double Betrayal: The Implications of Institutional Betrayal for Trauma-Related Symptoms in Intimate Partner Violence Survivors. Am. J. Orthopsychiatry 2025. [CrossRef]
- Serrano-Montilla, C.; Lozano, L.M.; Alonso-Ferres, M.; Valor-Segura, I.; Padilla, J.-L. Understanding the Components and Determinants of Police Attitudes Toward Intervention in Intimate Partner Violence Against Women: A Systematic Review. Trauma Violence Abuse 2023, 24, 245–260. [CrossRef]
- Isman, K.; Giorgi, S.; Ellis, J.; Huhn, A.S.; Liu, T.; Curtis, B. Perceived Stigma and Its Impact on Substance Use Disorder and Mental Health 2024.
Figure 1.
Age (right) and Temporal (left) Trends in Physical (top) and Emotional (bottom) Symptoms Following Intimate Partner Violence, 2009–2023. Note. Predicted probabilities of reporting at least one physical (top row) or emotional (bottom row) symptom among survivors of intimate partner violence in the United States, 2009–2023. Probabilities were estimated from survey-weighted logistic regression models and are shown as functions of survey year (left panels) and respondent age (right panels). Shaded bands represent 95% confidence intervals. Predictions were averaged across other covariates (sex, race/ethnicity, education, and region).
Figure 1.
Age (right) and Temporal (left) Trends in Physical (top) and Emotional (bottom) Symptoms Following Intimate Partner Violence, 2009–2023. Note. Predicted probabilities of reporting at least one physical (top row) or emotional (bottom row) symptom among survivors of intimate partner violence in the United States, 2009–2023. Probabilities were estimated from survey-weighted logistic regression models and are shown as functions of survey year (left panels) and respondent age (right panels). Shaded bands represent 95% confidence intervals. Predictions were averaged across other covariates (sex, race/ethnicity, education, and region).
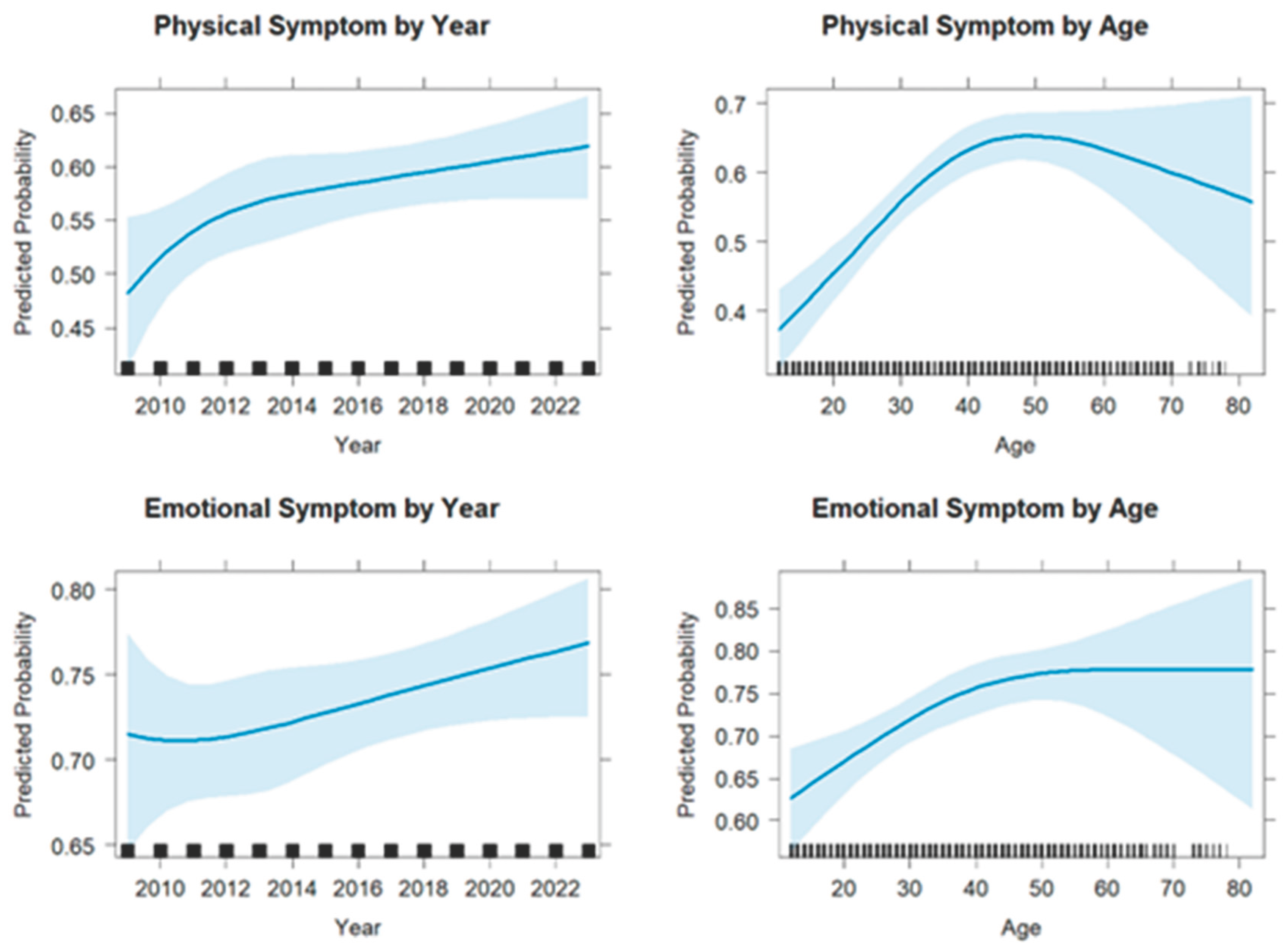

Table 1.
Percentage of IPV Survivors Reporting at Least One Symptom by Sociodemographic Characteristics.
Table 1.
Percentage of IPV Survivors Reporting at Least One Symptom by Sociodemographic Characteristics.
| Characteristic | Level | Denom N (unwtd) |
Denom N (wtd) |
Emotional n (unwtd) |
Emotional n (wtd) |
Emotional % (wtd) |
Physical n (unwtd) |
Physical n (wtd) |
Physical % (wtd) |
| Overall | All | 3,012 | 7,650,471 | 2,186 | 5,403,579 | 70.6 | 1,737 | 4,098,268 | 53.6 |
| Age | Under 19 | 302 | 1,027,762 | 185 | 617,999 | 60.1 | 119 | 379,341 | 36.9 |
| 19–39 | 1,693 | 4,410,926 | 1,227 | 3,141,339 | 71.2 | 976 | 2,380,037 | 54.0 | |
| 40–59 | 883 | 1,969,251 | 670 | 1,464,416 | 74.4 | 559 | 1,194,755 | 60.7 | |
| 60+ | 134 | 242,533 | 104 | 179,825 | 74.1 | 83 | 144,134 | 59.4 | |
| Race | Asian/PI | 56 | 155,529 | 46 | 126,607 | 81.4 | 43 | 112,920 | 72.6 |
| Black | 469 | 1,331,715 | 346 | 931,464 | 69.9 | 261 | 624,699 | 46.9 | |
| Hispanic | 492 | 1,304,346 | 357 | 933,534 | 71.6 | 270 | 648,830 | 49.7 | |
| White | 2,290 | 5,609,273 | 1,650 | 3,940,214 | 70.2 | 1,314 | 3,048,489 | 54.3 | |
| Multiracial | 145 | 428,951 | 102 | 307,380 | 71.7 | 82 | 226,389 | 52.8 | |
| Sex | Male | 668 | 1,800,398 | 372 | 949,016 | 52.7 | 237 | 558,707 | 31.0 |
| Female | 2,344 | 5,850,073 | 1,814 | 4,454,563 | 76.1 | 1,500 | 3,539,560 | 60.5 | |
| Highest Level of Education | HS diploma | 1,273 | 3,297,484 | 908 | 2,298,845 | 69.7 | 704 | 1,705,277 | 51.7 |
| > HS diploma | 1,720 | 4,311,041 | 1,260 | 3,065,499 | 71.1 | 1,019 | 2,366,506 | 54.9 | |
| Injury | No | 2,882 | 7,315,829 | 2,076 | 5,126,300 | 70.1 | 1,639 | 3,853,717 | 52.7 |
| Yes | 130 | 334,642 | 110 | 277,279 | 82.9 | 98 | 244,551 | 73.1 | |
| Potential TBI | No | 701 | 1,767,487 | 474 | 1,127,035 | 63.8 | 353 | 793,874 | 44.9 |
| Yes | 2,311 | 5,882,984 | 1,712 | 4,276,544 | 72.7 | 1,384 | 3,304,394 | 56.2 | |
| Region | Midwest | 914 | 1,988,216 | 668 | 1,398,200 | 70.3 | 541 | 1,072,526 | 53.9 |
| South | 1,008 | 2,720,715 | 716 | 1,875,129 | 68.9 | 567 | 1,458,077 | 53.6 | |
| West | 720 | 1,841,674 | 528 | 1,317,647 | 71.5 | 425 | 1,005,487 | 54.6 | |
| Northeast | 370 | 1,099,866 | 274 | 812,603 | 73.9 | 204 | 562,178 | 51.1 | |
| Population Size | Under 50K | 1,852 | 4,612,312 | 1,340 | 3,235,453 | 70.1 | 1,073 | 2,492,963 | 54.1 |
| 50K-250K | 631 | 1,630,186 | 477 | 1,193,815 | 73.2 | 387 | 931,333 | 57.1 | |
| Over 250K | 529 | 1,407,973 | 369 | 974,312 | 69.2 | 277 | 673,971 | 47.9 | |
| Police Report | No | 1,336 | 3,271,726 | 932 | 2,191,525 | 67.0 | 768 | 1,709,629 | 52.3 |
| Yes | 1,626 | 4,258,017 | 1,229 | 3,151,614 | 74.0 | 949 | 2,343,983 | 55.0 |
Note. Weighted estimates use the weight for victimization; percentages are survey-weighted. Key: “unwtd” = unweighted, “wtd” = weighted.
Table 2.
Emotional & Physical Symptoms After IPV Victimization (Multivariable ORs with Spline Terms).
Table 2.
Emotional & Physical Symptoms After IPV Victimization (Multivariable ORs with Spline Terms).
| Reporting ≥1 emotional symptom | Reporting ≥1 physical symptom | |||||
|---|---|---|---|---|---|---|
| Predictor | Odds Ratio | CI low | CI high | Odds ratio | CI low | CI high |
| — | — | — | — | — | — | — |
| s1(age) | 1.024 | 1.010 | 1.038 | 1.043 | 1.029 | 1.056 |
| s2(age) | 0.979 | 0.949 | 1.010 | 0.951 | 0.925 | 0.977 |
| s1(year) | 0.859 | 0.387 | 1.906 | 1.653 | 0.795 | 3.437 |
| s2(year) | 1.127 | 0.653 | 1.944 | 0.725 | 0.439 | 1.197 |
| Any Injury (Yes v No) | 1.955 | 1.132 | 3.376 | 2.794 | 1.687 | 4.627 |
| Female (Yes v No) | 2.943 | 2.352 | 3.681 | 3.610 | 2.887 | 4.515 |
| American Indian/Alaska Native (Yes v No) | 2.162 | 0.857 | 5.458 | 2.748 | 1.303 | 5.798 |
| Asian/Pacific Islander (Yes v No) | 1.620 | 0.680 | 3.858 | 1.986 | 0.913 | 4.319 |
| Black (Yes v No) | 1.054 | 0.784 | 1.415 | 0.786 | 0.607 | 1.017 |
| Hispanic (Yes v No) | 1.014 | 0.769 | 1.337 | 0.776 | 0.605 | 0.996 |
| Multiracial (Yes v No) | 1.182 | 0.745 | 1.874 | 0.998 | 0.666 | 1.497 |
| HS or Less (Yes v No) | 1.022 | 0.836 | 1.249 | 1.054 | 0.878 | 1.265 |
| Unconscious (Yes v No) | 1.495 | 1.196 | 1.869 | 1.503 | 1.221 | 1.849 |
| Population Size: 50k–250k | 1.200 | 0.932 | 1.545 | 1.254 | 0.997 | 1.577 |
| Population Size: ≥250k | 0.900 | 0.680 | 1.192 | 0.853 | 0.660 | 1.104 |
| Prepared Attack (Yes v No) | 1.448 | 1.187 | 1.768 | 1.121 | 0.934 | 1.346 |
| Region: Midwest | 0.890 | 0.637 | 1.244 | 1.252 | 0.929 | 1.688 |
| Region: South | 0.762 | 0.555 | 1.046 | 1.208 | 0.908 | 1.608 |
| Region: West | 0.953 | 0.671 | 1.355 | 1.316 | 0.966 | 1.793 |
Note. Survey-weighted logistic regression (svyglm, quasibinomial). year and age are modeled via restricted cubic splines with knots at (1999, 2007, 2015) and (25, 40, 65), respectively; spline basis terms shown as s1(year), s2(year), s1(age), s2(age). Reference levels: Region = Northeast; Population Size = <50k. Binary predictors are 1 vs 0. Weights: vic_weight.
Table 3.
Predicted Probabilities of Emotional Symptoms by Injury Present (Yes/No) and Race/Ethnicity.
Table 3.
Predicted Probabilities of Emotional Symptoms by Injury Present (Yes/No) and Race/Ethnicity.
| Outcome | Sex | Injury | Race | Predicted Probability (95% CI) |
| Physical symptom | Male | No Injury | American Indian/Alaska Native | 0.476 (0.275–0.677) |
| Asian/Pacific Islander | 0.399 (0.203–0.596) | |||
| Black | 0.213 (0.138–0.289) | |||
| Hispanic | 0.211 (0.135–0.288) | |||
| Multiracial | 0.255 (0.153–0.357) | |||
| White | 0.255 (0.179–0.332) | |||
| Injury | American Indian/Alaska Native | 0.709 (0.515–0.903) | ||
| Asian/Pacific Islander | 0.64 (0.423–0.858) | |||
| Black | 0.423 (0.265–0.581) | |||
| Hispanic | 0.42 (0.262–0.578) | |||
| Multiracial | 0.48 (0.306–0.653) | |||
| White | 0.48 (0.326–0.634) | |||
| Female | No Injury | American Indian/Alaska Native | 0.757 (0.607–0.907) | |
| Asian/Pacific Islander | 0.695 (0.523–0.867) | |||
| Black | 0.484 (0.381–0.586) | |||
| Hispanic | 0.481 (0.375–0.586) | |||
| Multiracial | 0.541 (0.412–0.67) | |||
| White | 0.541 (0.449–0.634) | |||
| Injury | American Indian/Alaska Native | 0.894 (0.803–0.986) | ||
| Asian/Pacific Islander | 0.86 (0.745–0.976) | |||
| Black | 0.715 (0.584–0.846) | |||
| Hispanic | 0.713 (0.581–0.844) | |||
| Multiracial | 0.76 (0.631–0.888) | |||
| White | 0.76 (0.647–0.873) | |||
| Emotional symptom | Male | No Injury | American Indian/Alaska Native | 0.606 (0.367–0.844) |
| Asian/Pacific Islander | 0.537 (0.309–0.765) | |||
| Black | 0.432 (0.311–0.553) | |||
| Hispanic | 0.423 (0.303–0.543) | |||
| Multiracial | 0.46 (0.307–0.613) | |||
| White | 0.42 (0.312–0.527) | |||
| Injury | American Indian/Alaska Native | 0.748 (0.534–0.962) | ||
| Asian/Pacific Islander | 0.691 (0.465–0.917) | |||
| Black | 0.594 (0.42–0.769) | |||
| Hispanic | 0.585 (0.411–0.76) | |||
| Multiracial | 0.621 (0.434–0.808) | |||
| White | 0.582 (0.415–0.749) | |||
| Female | No Injury | American Indian/Alaska Native | 0.816 (0.664–0.969) | |
| Asian/Pacific Islander | 0.769 (0.607–0.932) | |||
| Black | 0.686 (0.586–0.786) | |||
| Hispanic | 0.678 (0.576–0.78) | |||
| Multiracial | 0.71 (0.586–0.834) | |||
| White | 0.675 (0.583–0.767) | |||
| Injury | American Indian/Alaska Native | 0.896 (0.788–0.999) | ||
| Asian/Pacific Islander | 0.866 (0.742–0.99) | |||
| Black | 0.809 (0.698–0.92) | |||
| Hispanic | 0.803 (0.69–0.916) | |||
| Multiracial | 0.826 (0.71–0.941) | |||
| White | 0.801 (0.691–0.911) |
Note. Survey-weighted logistic regression. Predictions averaged over years, age, region, and population size.
Table 4.
Predicted Probabilities of Physical Symptoms by Sex, Injury Present (Yes/No), and Race/Ethnicity.
Table 4.
Predicted Probabilities of Physical Symptoms by Sex, Injury Present (Yes/No), and Race/Ethnicity.
| Outcome | Sex | Injury | Race | Predicted Probability (95% CI) |
| Physical symptom | Male | No Injury | White | 0.255 (0.179–0.332) |
| Hispanic | 0.211 (0.135–0.288) | |||
| Multiracial | 0.255 (0.153–0.357) | |||
| Asian/Pacific Islander | 0.399 (0.203–0.596) | |||
| American Indian/Alaska Native | 0.476 (0.275–0.677) | |||
| Black | 0.213 (0.138–0.289) | |||
| Injury | White | 0.48 (0.326–0.634) | ||
| Hispanic | 0.42 (0.262–0.578) | |||
| Multiracial | 0.48 (0.306–0.653) | |||
| Asian/Pacific Islander | 0.64 (0.423–0.858) | |||
| American Indian/Alaska Native | 0.709 (0.515–0.903) | |||
| Black | 0.423 (0.265–0.581) | |||
| Female | No Injury | White | 0.541 (0.449–0.634) | |
| Hispanic | 0.481 (0.375–0.586) | |||
| Multiracial | 0.541 (0.412–0.67) | |||
| Asian/Pacific Islander | 0.695 (0.523–0.867) | |||
| American Indian/Alaska Native | 0.757 (0.607–0.907) | |||
| Black | 0.484 (0.381–0.586) | |||
| Injury | White | 0.76 (0.647–0.873) | ||
| Hispanic | 0.713 (0.581–0.844) | |||
| Multiracial | 0.76 (0.631–0.888) | |||
| Asian/Pacific Islander | 0.86 (0.745–0.976) | |||
| American Indian/Alaska Native | 0.894 (0.803–0.986) | |||
| Black | 0.715 (0.584–0.846) | |||
| Emotional symptom | Male | No Injury | White | 0.42 (0.312–0.527) |
| Hispanic | 0.423 (0.303–0.543) | |||
| Multiracial | 0.46 (0.307–0.613) | |||
| Asian/Pacific Islander | 0.537 (0.309–0.765) | |||
| American Indian/Alaska Native | 0.606 (0.367–0.844) | |||
| Black | 0.432 (0.311–0.553) | |||
| Injury | White | 0.582 (0.415–0.749) | ||
| Hispanic | 0.585 (0.411–0.76) | |||
| Multiracial | 0.621 (0.434–0.808) | |||
| Asian/Pacific Islander | 0.691 (0.465–0.917) | |||
| American Indian/Alaska Native | 0.748 (0.534–0.962) | |||
| Black | 0.594 (0.42–0.769) | |||
| Female | No Injury | White | 0.675 (0.583–0.767) | |
| Hispanic | 0.678 (0.576–0.78) | |||
| Multiracial | 0.71 (0.586–0.834) | |||
| Asian/Pacific Islander | 0.769 (0.607–0.932) | |||
| American Indian/Alaska Native | 0.816 (0.664–0.969) | |||
| Black | 0.686 (0.586–0.786) | |||
| Injury | White | 0.801 (0.691–0.911) | ||
| Hispanic | 0.803 (0.69–0.916) | |||
| Multiracial | 0.826 (0.71–0.941) | |||
| Asian/Pacific Islander | 0.866 (0.742–0.99) | |||
| American Indian/Alaska Native | 0.896 (0.788–0.999) | |||
| Black | 0.809 (0.698–0.92) |
Note. Survey-weighted logistic regression. Predictions averaged over year, age, region, and population size.
Table 5.
Predicted Probabilities of Emotional & Physical Symptoms Among IPV Survivors with Injury by Sex, Probable TBI, and Race/Ethnicity.
Table 5.
Predicted Probabilities of Emotional & Physical Symptoms Among IPV Survivors with Injury by Sex, Probable TBI, and Race/Ethnicity.
| Outcome | Sex | Probable TBI | Race | Predicted Probability (95% CI) |
| Emotional symptom | Female | Yes | American Indian/Alaska Native | 0.928 (0.851–1) |
| Asian/Pacific Islander | 0.906 (0.816–0.996) | |||
| Black | 0.863 (0.781–0.945) | |||
| Hispanic | 0.858 (0.774–0.942) | |||
| Multiracial | 0.876 (0.792–0.96) | |||
| White | 0.857 (0.776–0.937) | |||
| No | American Indian/Alaska Native | 0.896 (0.788–0.999) | ||
| Asian/Pacific Islander | 0.866 (0.742–0.99) | |||
| Black | 0.809 (0.698–0.92) | |||
| Hispanic | 0.803 (0.69–0.916) | |||
| Multiracial | 0.826 (0.71–0.941) | |||
| White | 0.801 (0.691–0.911) | |||
| Male | Yes | American Indian/Alaska Native | 0.815 (0.647–0.983) | |
| Asian/Pacific Islander | 0.768 (0.582–0.955) | |||
| Black | 0.685 (0.534–0.836) | |||
| Hispanic | 0.677 (0.525–0.829) | |||
| Multiracial | 0.709 (0.55–0.868) | |||
| White | 0.674 (0.53–0.818) | |||
| No | American Indian/Alaska Native | 0.748 (0.534–0.962) | ||
| Asian/Pacific Islander | 0.691 (0.465–0.917) | |||
| Black | 0.594 (0.42–0.769) | |||
| Hispanic | 0.585 (0.411–0.76) | |||
| Multiracial | 0.621 (0.434–0.808) | |||
| White | 0.582 (0.415–0.749) | |||
| Physical symptom | Female | Yes | American Indian/Alaska Native | 0.927 (0.862–0.992) |
| Asian/Pacific Islander | 0.902 (0.818–0.986) | |||
| Black | 0.788 (0.685–0.891) | |||
| Hispanic | 0.786 (0.683–0.889) | |||
| Multiracial | 0.824 (0.726–0.923) | |||
| White | 0.825 (0.739–0.91) | |||
| No | American Indian/Alaska Native | 0.894 (0.803–0.986) | ||
| Asian/Pacific Islander | 0.86 (0.745–0.976) | |||
| Black | 0.715 (0.584–0.846) | |||
| Hispanic | 0.713 (0.581–0.844) | |||
| Multiracial | 0.76 (0.631–0.888) | |||
| White | 0.76 (0.647–0.873) | |||
| Male | Yes | American Indian/Alaska Native | 0.783 (0.625–0.941) | |
| Asian/Pacific Islander | 0.725 (0.538–0.911) | |||
| Black | 0.52 (0.364–0.675) | |||
| Hispanic | 0.517 (0.362–0.672) | |||
| Multiracial | 0.577 (0.413–0.74) | |||
| White | 0.577 (0.433–0.721) | |||
| No | American Indian/Alaska Native | 0.709 (0.515–0.903) | ||
| Asian/Pacific Islander | 0.64 (0.423–0.858) | |||
| Black | 0.423 (0.265–0.581) | |||
| Hispanic | 0.42 (0.262–0.578) | |||
| Multiracial | 0.48 (0.306–0.653) | |||
| White | 0.48 (0.326–0.634) |
Note. Survey-weighted logistic regression. Sample restricted to respondents reporting injury from IPV. ‘Probable TBI’ compares the loss of consciousness status. Predictions averaged over year, age, education, region, and population size.4. Discussion.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



